 Tania Crombet Ramos
Tania Crombet Ramos Orestes Santos Morales
Orestes Santos Morales Grace K. Dy2
Grace K. Dy2 Kalet León Monzón
Kalet León Monzón Agustín Lage Dávila
Agustín Lage Dávila- 1Research Direction, Center of Molecular Immunology, Havana, Cuba
- 2Department of Medicine, Roswell Park Comprehensive Cancer Center, Buffalo, NY, United States
Advanced non-small cell lung cancer (NSCLC) has faced a therapeutic revolution with the advent of tyrosine kinase inhibitors (TKIs) and immune checkpoints inhibitors (ICIs) approved for first and subsequent therapies. CIMAvax-EGF is a chemical conjugate between human-recombinant EGF and P64, a recombinant protein from Neisseria meningitides, which induces neutralizing antibodies against EGF. In the last 15 years, it has been extensively evaluated in advanced NSCLC patients. CIMAvax-EGF is safe, even after extended use, and able to keep EGF serum concentration below detectable levels. In a randomized phase III study, CIMAvax-EGF increased median overall survival of advanced NSCLC patients with at least stable disease after front-line chemotherapy. Patients bearing squamous-cell or adenocarcinomas and serum EGF concentration above 870 pg/ml had better survival compared to control patients treated with best supportive care as maintenance, confirming tumors’ sensitivity to the EGF depletion. This manuscript reviews the state-of-the-art NSCLC therapy and proposes the most promising scenarios for evaluating CIMAvax-EGF, particularly in combination with TKIs or ICIs. We hypothesize that the optimal combination of CIMAvax-EGF with established therapies can further contribute to transform advanced cancer into a manageable chronic disease, compatible with years of good quality of life.
Introduction
Advanced non-small cell lung cancer (NSCLC) remains a major health problem. Despite all scientific advances of the last decades, a substantial fraction of lung cancer patients are diagnosed at advanced stages of disease, accounting for roughly 1.2 million deaths per year worldwide (1).
During the last decade, the high heterogeneity of advanced NSCLC has been confirmed (2, 3). Aside from histologic subtypes, molecular characterization of the disease is a critical step in the classification of the disease, making management of NSCLC much more complex (2–6). In this context, oncogene addiction to the epidermal growth factor receptor (EGFR) pathway is widely accepted (7, 8). Indeed, the dependence of some tumors on aberrant EGFR signaling supports the successful use of EGFR tyrosine kinase inhibitors (TKI) in tumors with known activating mutations (9, 10).
Epidermal growth factor (EGF) is one of the most important ligands of the EGFR, which is produced mainly in a paracrine fashion (11). EGF concentration in human serum is largely variable, both in healthy and lung cancer patients, but it tends to be higher in patients (12, 13). A high EGF amount plus EGFR overexpression in lung cancer cells (14), create conditions for the growth of some EGF-dependent tumors, even in the absence of specific EGFR driver mutations. Our group has shown that high EGF concentration in serum is a poor prognostic factor for advanced NSCLC individuals (15). CIMAvax-EGF is a growth factor-depleting immunotherapy intended to reduce EGF concentration, both in serum and in the tumor microenvironment (16–18).
Advanced NSCLC has recently faced a therapeutic revolution with the advent of new drugs registered for first and subsequent therapies (19, 20). The introduction of innovative treatments, particularly TKIs and immunotherapies, evolves so fast that the therapeutic landscape is constantly changing (21). In this setting, medical progress relies not only on the discovery of new drugs but also on the smart positioning of the novel medications among the other choices. In this complex scenario, we would like to discuss novel clinical trials with CIMavax-EGF, which could better potentiate other registered therapeutics.
CIMAvax-EGF Immunotherapy
CIMAvax-EGF is a chemical conjugate between human-recombinant EGF and P64, a recombinant protein from Neisseria meningitides (16, 17) (Figure 1A). CIMAvax-EGF induces neutralizing antibodies that trap EGF and reduces its concentration in serum, achieving an immunological “castration” of the growth factor (Figure 1B). Indeed, sera of patients immunized with CIMAvax-EGF block the binding between EGF and its receptor, inhibiting the EGFR phosphorylation and cell proliferation in vitro (22) (Figure 1C)
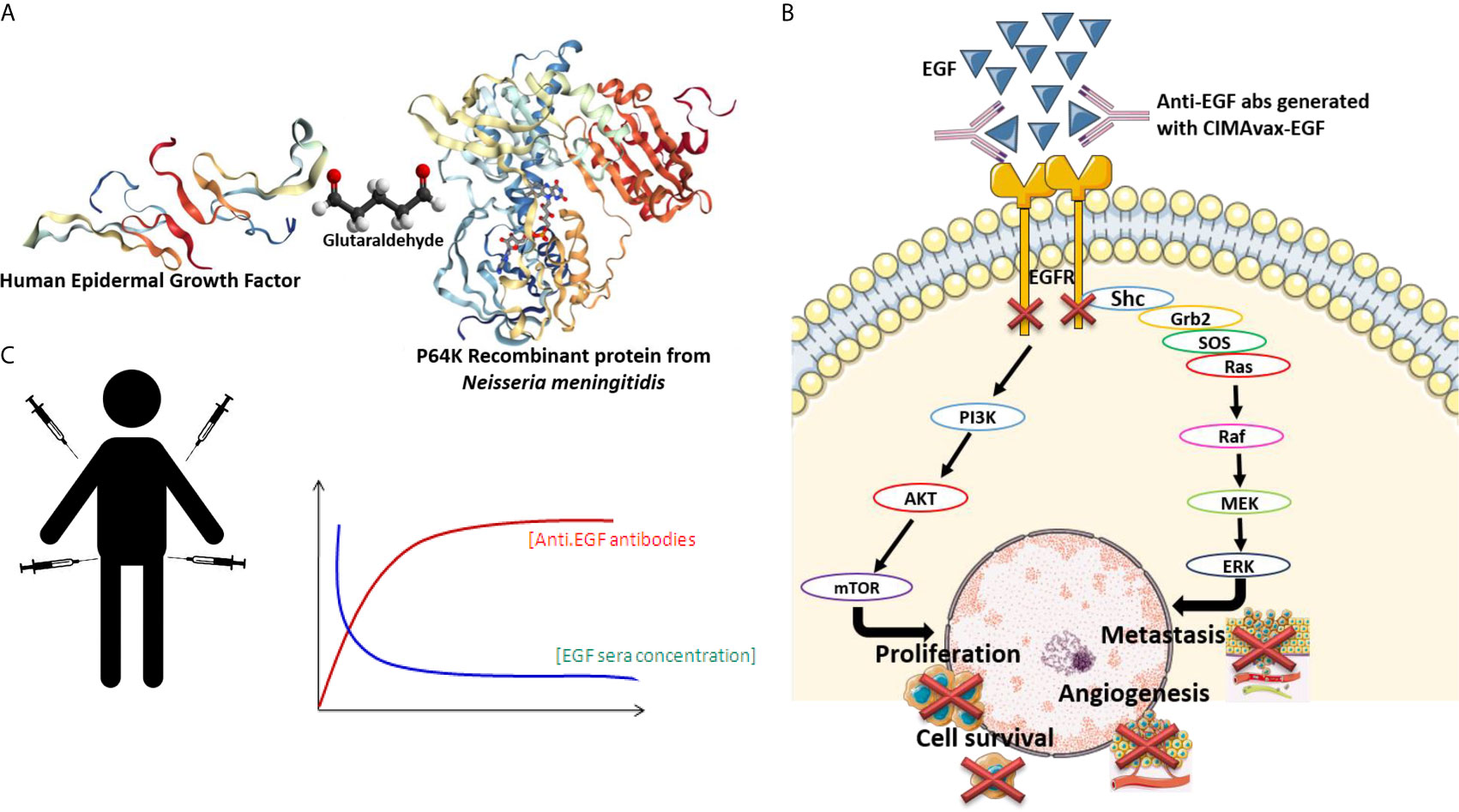
Figure 1 (A) Cimavax composition: CIMAvax-EGF is a chemical conjugate between human-recombinant EGF and P64, a recombinant protein from Neisseria meningitides. (B) CIMAvax-EGF induces neutralizing antibodies that trap EGF and reduces its concentration in serum, achieving an immunological “castration” of the growth factor. (C) Sera of patients immunized with CIMAvax-EGF block the binding between EGF and its receptor, inhibiting the EGFR phosphorylation and cell proliferation in vitro.
In the last 15 years, CIMAvax-EGF has been extensively evaluated in advanced NSCLC patients. CIMAvax-EGF has proven to be safe, even after extended use, and capable to keep EGF serum concentration below detectable levels (23, 24). The anti-EGF antibody response did not cross-react with other EGFR ligands, such as TGF alpha and amphiregulin (22, 25). Notably, in some patients, TGF alpha augmented after 6 months of CIMAvax-EGF, while amphiregulin concentration did not change overtime (25). The increase of one or more ligands after effective EGFR blockade has been reported before (26, 27).
In a phase III randomized clinical trial conducted between 2008 and 2012 in 405 patients, CIMAvax-EGF increased the median overall survival (OS) of the advanced NSCLC patients that had at least stable disease after front-line chemotherapy (15). Median OS was 12.43 months in the vaccinated patients that completed induction vs. 9.43 months in the control arm (15). Survival advantage was larger in patients with high-serum EGF concentration. In patients with EGF levels >870 pg/ml, absolute survival gain was 5 months (15). Moreover, long-term survival rates were higher in vaccinated vs. control patients: 37% vs 20% (2-year survival rate) and 23% vs 0% (5-year survival rate) (15).
Other clinical and tumor characteristics have been associated with longer survival after CIMAvax-EGF (15). Notably, benefit was larger in patients with squamous cell carcinoma (HR 0.524) than in adenocarcinoma (HR 0.835), probably linked to the higher expression of wild type EGFR in the squamous histology (28). In addition, patients with a better immune status benefited more: OS was larger individuals with higher anti-EGF antibodies or lower markers of immune-senescence (29). The proportion of CD8+CD28− T cells, CD4 T cells, and the CD4/CD8 ratio after chemotherapy correlated with the clinical benefit of CIMAvax-EGF. Vaccinated patients with CD4+ T cells counts greater than 40%, CD8+CD28− T cells counts lower than 24% and a CD4/CD8 ratio > 2 after first-line platinum-based therapy, achieved a significantly larger survival, as compared to controls with the same phenotype (29). Other biomarkers associated with the inflammatory response (neutrophil to lymphocyte ratio, NLR) as well as the neutrophil and monocyte counts were useful to predict response to CIMAvax-EGF (30).
One of the key findings of the CIMAvax-EGF trials is the presence of a subgroup of patients with long-term survival, even in the absence of subsequent therapy (29, 31). These long-term survivors frequently exhibit a persistent but almost dormant or very slow-growth tumor (Figure 2), which resembles the behavior of prostate or breast tumors treated with hormone-depleting therapies (32, 33).
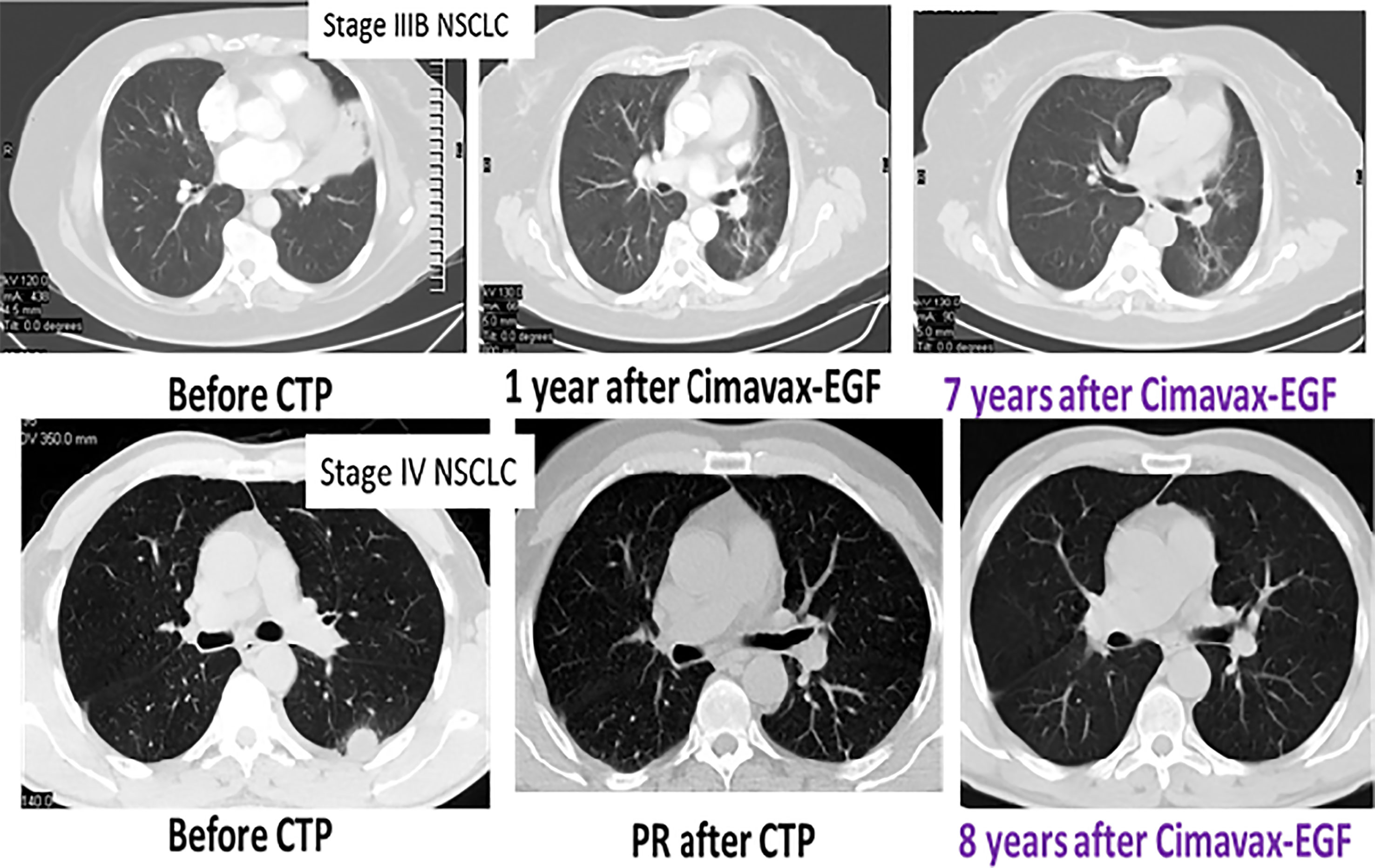
Figure 2 Long-lasting disease control after CIMAvax-EGF. CT scan series of two representative patients.
A recent update of the Cimavax-EGF Phase III clinical trial confirmed this previous finding. The 5-year survival rate was high in patients with adenocarcinoma or squamous cell carcinomas with serum EGF concentration above 870 pg/ml, confirming sensitivity of the tumors to the EGF depletion (Figure 3).
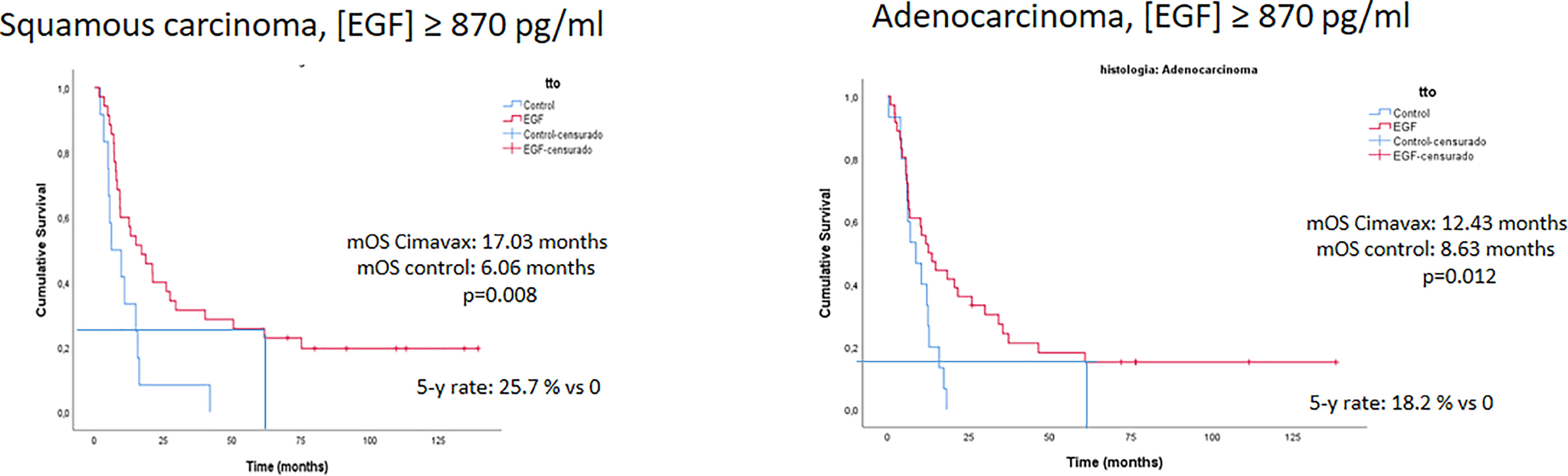
Figure 3 Survival advantage of EGF deprivation therapy over best supportive care according to serum EGF concentration and tumor histology: 5 years update of the phase III trial.
CIMAvax-EGF was initially approved as switch maintenance for all advanced NSCLC patients not progressing after first platinum-based chemotherapy. Later on, label was amended to include patient selection according the EGF concentration in serum.
The Evolving Landscape of Advanced NSCLC Treatment
Over the past two decades, chemotherapy and, in particular, platinum-based combinations provided a modest survival advantage and symptom palliation for inoperable NSCLC patients (34). At the end of the 20th century, controlled clinical trials comparing doublet regimens (platinum plus taxanes, vinca alkaloids, or etoposide) found equal efficacy among treatment arms. Indeed, it seemed that a survival plateau (40% 1-year survival rate) was reached with traditional cytotoxic drug combinations (2).
In this context, efforts for obtaining an EGF-depleting therapy began. Epidermal growth factor was discovered in 1962, and the first clues on the role of EGF/EGFR in cancer cell biology appeared in the 1980s (35, 36). Several pieces of evidence showing the wide applicability of the cancer hormone-dependence concept to the emerging field of peptide growth factors came out from our team (37, 38).
CIMAvax-EGF treatment showed survival improvement as switch maintenance for NSCLC patients with disease control after platinum doublets. However, in parallel, two major scientific advances emerged, which led to radical changes in the standard treatment protocols for advanced NSCLC. These were the following:
1. The identification of genetic driver mutations (39) and the introduction of targeted therapies, such as tyrosine kinase inhibitors (TKI). TKIs are specific for mutated oncogenic proteins and have the advantage of being oral pills with reduced toxicity (40). Particularly, TKIs targeting specific EGFR and ALK/ROS1 mutations are widely used (41, 42).
2. The discovery of the immune “checkpoints,” which can be targeted with specific monoclonal antibodies (immune checkpoint inhibitors [ICI]). ICI lessens the control loops of the immune system, allowing the expansion of the antitumor immune response (43–45). The cytotoxic T lymphocyte–associated antigen 4 (CTLA-4) and programmed death 1 (PD-1) immune checkpoints are negative regulators of immune function. CTLA-4 regulates T-cell proliferation early in the immune response, mainly in lymph nodes, whereas PD-1 limits T cells later in an immune response, primarily in the peripheral tissues (46). Particularly, antibodies targeting programmed death molecule-1 (PD1) or their main ligands (PD-L1) are extensively used in the first-line setting (47).
The evolving landscape of advanced NSCLC therapy from conventional chemotherapy to EGFR TKIs and checkpoint inhibitors is depicted in Figure 4.
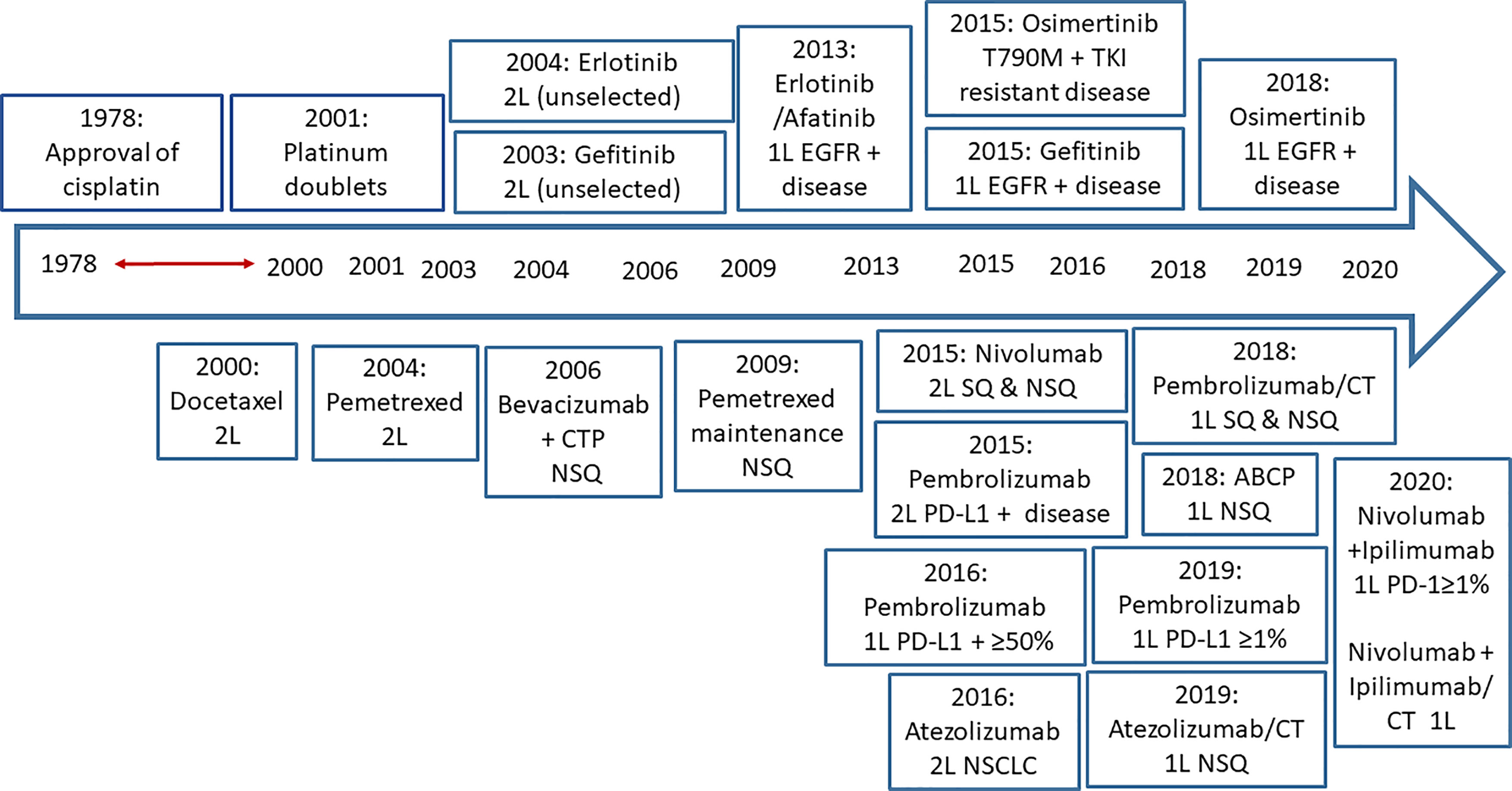
Figure 4 The evolving setting of advanced NSCLC therapy: From conventional chemotherapy to EGFR TKIs and checkpoint inhibitors. SOC, standard of care; 1L, first line; 2L, second line; SQ, squamous; NSQ, non-squamous; ABCP, atezolizumab-bevacizumab-carboplatin and paclitaxel.
Progressively, molecular stratification according to driver mutations (actionable mutations) and PD-L1 expression has gained preeminence, even over the classical histological classification. The identification of actionable mutations and the level of expression of PD-L1 have divided the current landscape of NSCLC into several therapeutic scenarios (Figure 5) apart from traditional chemotherapies. Moreover, the lower toxicities of the new drugs allow maintenance or even their use as consolidation therapies, such as after concurrent chemo-radiation in unresectable stage III NSCLC (48, 49). In the next sections, we briefly describe and comment the main therapeutic scenarios illustrated in Figure 5.
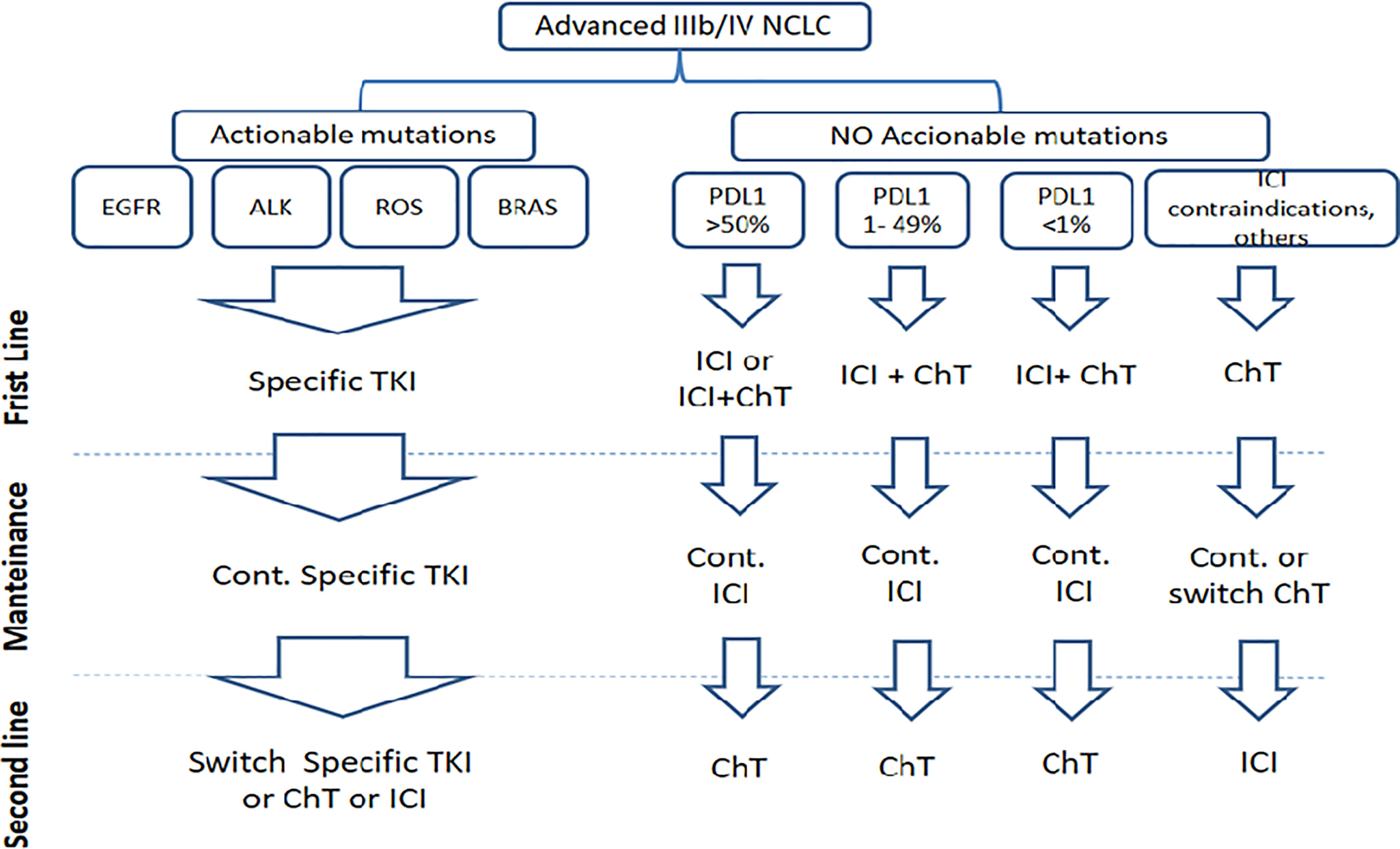
Figure 5 Current landscape of NSCLC according actionable mutations and PD-L1 expression.
Tumors With Actionable Mutations
Actionable mutations appear in roughly 40% to 50% of adenocarcinoma patients and are rare in squamous cell carcinomas (50). EGFR, ALK, ROS1, BRAF, MET, RET mutations are the most relevant for current lung cancer therapy, although many other mutations are still under active clinical investigation (51). The detection of such driver mutations determines the use of specific targeted therapy. In this manuscript, we focus on the current therapeutic alternatives for tumors bearing EGFR mutations (see Table 1).
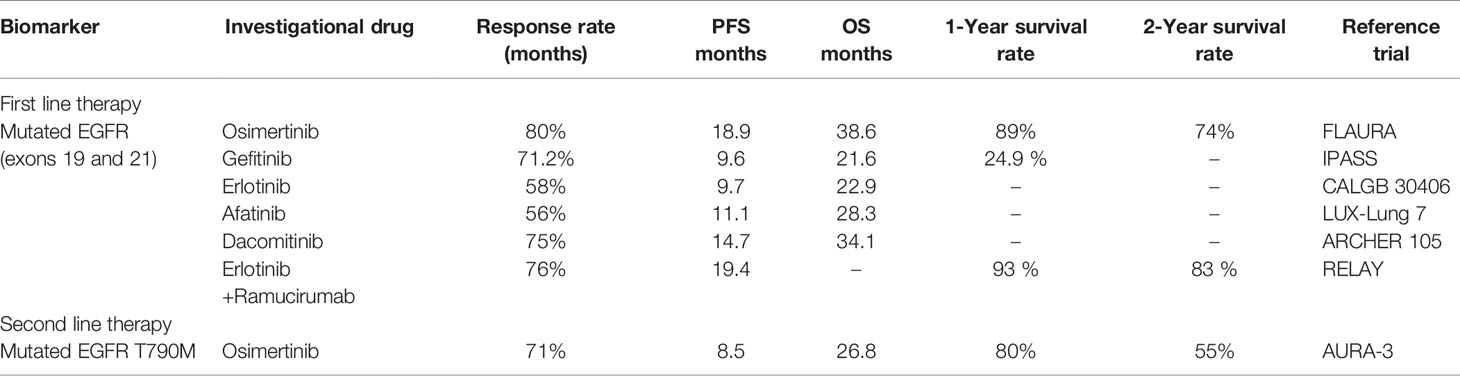
Table 1 Therapeutics options for patients with actionable mutations of the EGFR, regardless histology.
In patients with EGFR-mutated tumors, the use of specific TKI as first line has significantly increased the response rate and progression free survival (PFS) when compared with standard chemotherapy. First- and second-generation TKIs, such as gefitinib, erlotinib, afatinib, and dacomitinib, are used continuously until evidence of tumor resistance, which happen frequently by the selection of a secondary mutation in the kinase domain of the EGFR, particularly T790M (52). Osimertinib is a third-generation TKI, which is specific for EGFR mutations, including the T790M mutation. It has shown the best response rate and PFS observed so far in the first-line setting among patients with sensitizing EGFR mutations (53). For this patient population, subsequent therapy with cytotoxic drugs should be used only after exhausting all TKI possibilities. ICIs as initial or subsequent monotherapies are not recommended, since there is evidence of resistance of EGFR mutated tumors to the PD1/PD-L1 blockade, despite their frequently elevated PD-L1 expression (54, 55).
Combination of ramucirumab, an anti-VEGFR2 monoclonal antibody (MAb), with erlotinib has also shown significant PFS improvement as compared with single first- and second-generation TKI therapies in the first line (56). However, safety must be considered due to the higher frequency of grade 4 or serious adverse events (SAEs) observed with this combination (56). Recently, several preclinical and early clinical trials were performed to assess the combined effect of EGFR TKIs and PD1/PD-L1 targeting drugs. According Han and co-workers, treatment schedule would be crucial to increase the efficacy and safety of EGFR TKI and immunotherapy. ICIs can synergize better with hypo-fractionated TKI to achieve complete response of late-stage cancer. However, high-dose EGFR TKI can not only elicit a greater innate response but also increase the PD-L1 expression in tumors, contributing to resistance (57). According the initial trials, combination of TKIs and ICIs in patients with EGFR mutations could be toxic and had failed to show clinical benefit (58). Pembrolizumab plus erlotinib was feasible; however, pembrolizumab plus gefitinib provoked grade 3/4 liver toxicity in five of seven patients, leading to permanent treatment discontinuation in four individuals (58). In addition, PD-L1 blockade followed by osimertinib was associated with severe immune-related adverse events, particularly pneumonitis (59).
Tumors With No Actionable Mutation
In tumors with unknown or no actionable mutations, ICIs blocking the interaction between PD-1 and PD-L1 ligand, ICI alone, or in combination with chemotherapy dominate the therapeutic landscape currently (Figure 5). Therapeutic interventions are largely guided by PD-L1 expression levels regardless of the classical NSCLC histological sub-classification. However, overall efficacy of the treatments and the specific choice of the chemotherapy regimen vary depending on histology.
Tumors With PD-L1>50%
Tumors with high expression of PD-L1 represent 30% to 40% of all advanced NSCLC (60) and are highly sensitive to ICI provided there are no EGFR/ALK/ROS1 genetic alterations. Pembrolizumab, an anti-PD1 antibody, is the preferred first-line therapy for this type of tumors. This antibody can be used either alone or in combination with platinum-based chemotherapy based on the data from KEYNOTE 24, 42, 189, and 407 clinical trials (Table 2) (44, 60–63). However, an open debate remains in the literature regarding which patients should receive pembrolizumab alone vs its combination with chemotherapy (64, 65). Some authors suggest that clinical efficacy of pembrolizumab monotherapy is mainly demonstrated in patients with very high expression of PD-L1 (PDL-1>90%) (65). Atezolizumab has also shown benefits in comparison with chemotherapy as first-line monotherapy. The trial demonstrated a statistically significant improvement in OS for patients with high PD-L1 tumor expression (as defined by SP142 immunohistochemistry assay) receiving atezolizumab compared to those treated with platinum-based chemotherapy. Efficacy signals were very similar even with using DAKO 22C3 immunohistochemical stain to derive cutoff point of >/= 50% (used as companion diagnostic for pembrolizumab). Median OS was 20.2 months for patients in the atezolizumab arm compared with 13.1 months in the control arm (66).
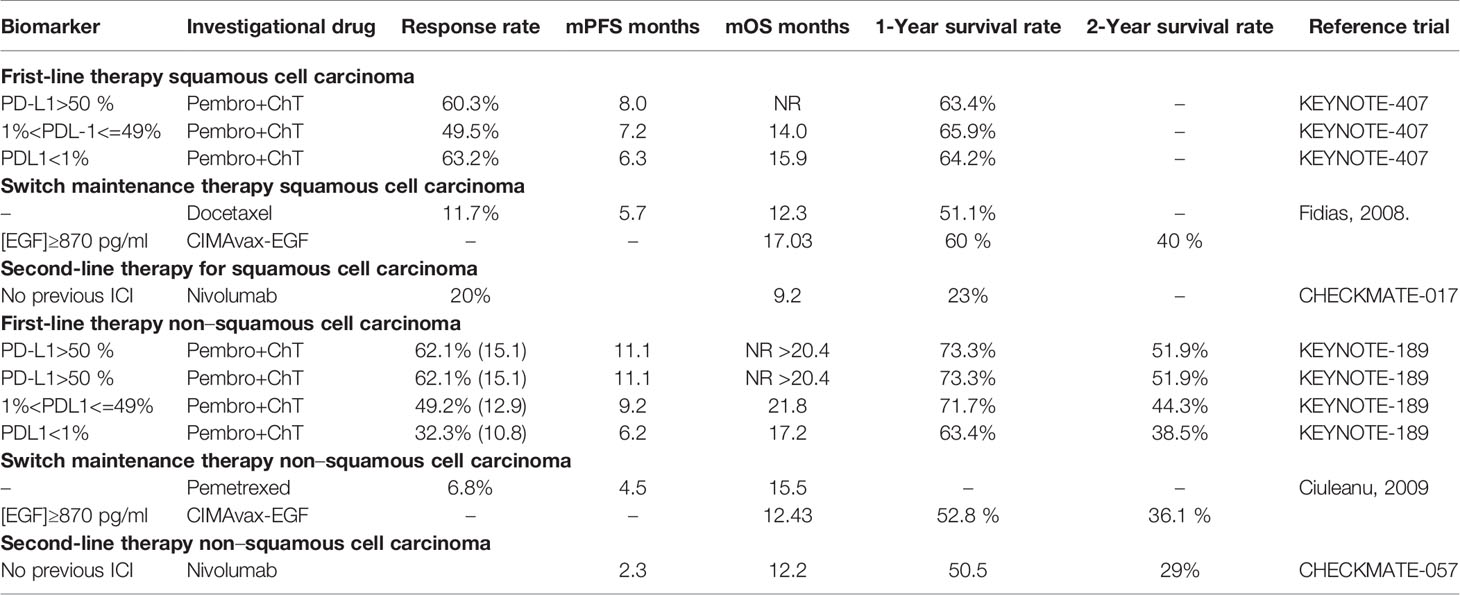
Table 2 Most used therapeutic schemes in advanced NSCLC and no actionable mutations, according histology.
Other recommended combinations for non-squamous tumors consist of atezolizumab/carboplatin plus paclitaxel/bevacizumab or nab-paclitaxel and nivolumab/ipilimumab plus platinum/pemetrexed (64). The bevacizumab-containing combination was also the first and only regimen to date to demonstrate superior survival outcomes in patients with EGFR/ALK mutations who had disease progression on TKI prior to enrollment in the study. For squamous tumors, nivolumab/ipilimumab plus platinum/paclitaxel also seems to be efficacious (64). For both histologies, nivolumab + ipilimumab significantly prolonged progression-free survival vs chemotherapy in patients with high tumor mutational burden (67).
Tumors With 1% < PD-L1 <= 49%
Tumors with intermediate expression of PD-L1 represent between 30% and 40% of all advanced NSCLC (63) and respond better to the combination of ICI and chemotherapy (64). For non-squamous, the best alternative is pembrolizumab + platinum/pemetrexed. Other accepted treatments are atezolizumab/carboplatin combined with paclitaxel/bevacizumab or nab-paclitaxel and nivolumab/ipilimumab plus platinum/pemetrexed. For squamous, the preferred choice is pembrolizumab/carboplatin plus paclitaxel or nab-paclitaxel. Nivolumab/ipilimumab plus carboplatin/paclitaxel can also be prescribed (64).
As in the previous subset, nivolumab and ipilimumab can be used in patients with high-mutation tumors.
Tumors With PD-L1<=1%
Tumors with low or negative expression of PD-L1 represent roughly 30% of all advanced NSCLC (68), and they are not sensitive to ICIs alone. However, chemotherapy and ICI, as described in the previous subset, can be used for ECOG performance status 0-1 patients (64). The mechanistic explanation for this effect remains unclear, but it could reflect immune sensitization of the tumors by the applied chemotherapy.
ICI Contraindicated, Patient Refusal, or Product Not Affordable
Despite PD-L1 expression level, several contraindications could prevent the use of ICI: active or documented history of autoimmune diseases, current use of immunosuppressive agents and ECOG > 2 (62, 63, 67, 69). Furthermore, there is a significant questioning in the literature regarding cost effectiveness of the combination of ICI + chemotherapy in PD-L1 low or negative tumors (70, 71). The high cost of ICIs in contrast to its clinical impact could lead to negative pharmacoeconomic evaluations, even for rich countries like US, Japan, or Europe, but definitely for many middle and low-income countries (72–75). Therefore, some national and/or private health insurances might choose not to cover ICI + chemotherapy in patients with PD-L1 < 1%, at least until a significant price reduction for ICIs takes place. Accordingly, a significant number of advanced NSCLC patients might not have access to ICIs in first-line or in even second-line setting. For this group of patients, traditional platinum-based chemotherapy (Table 2) remains the standard of care (76–78).
Subsequent Therapy (Maintenance and Second Line)
In patients receiving ICI alone or in combination with chemotherapy in first-line, continuation maintenance with pembrolizumab alone or combined with pemetrexed (63, 68), atezolizumab alone, or combined with bevacizumab (69, 79) are the recommended schemes in the adenocarcinoma histology. For the squamous setting, pembrolizumab or atezolizumab monotherapies can be used as maintenance therapies (62, 66).
Prior to the advent of ICIs, switch or continuation maintenance chemotherapy is the standard of care (76–78). However, some concerns have been raised about the advantage of switch maintenance in advanced NSCLC due to the toxicity and modest survival benefit (76) (Table 2).
CIMAvax-EGF Opportunities
There is an unquestionable clinical benefit of the newly adopted therapies and protocols for NSCLC (Figure 5 and Tables 1, 2). Indeed, beyond the statistical significance and differences in median survival, there was a modification of the shape of the survival curves. Cumulative survival curves of patients receiving ICIs did not show only better overall survival, but also a tail suggesting very prolonged survival and transition to chronicity of a subset of patients (63). Patients live longer with good quality of life (80). However, these undeniable improvements are still far from raising the bar of survival expectancies long enough in a larger fraction of patients to achieve substantial reduction in mortality rates, or major decreases in the mortality/incidence index, as already happened for hematologic malignancies, prostate and breast cancer (81, 82). The vast majority of lung cancer patients will eventually succumb from their disease (81). Therefore, the addition of CIMAvax-EGF and other new drugs that might further increase survival is warranted.
What could be the place of CIMAvax-EGF inside this new therapeutic landscape? Which strategies seem more promising for its rapid practical application and/or for designing new clinical trials?
The most straightforward positioning of CIMAvax-EGF is as switch maintenance in the subgroup of patients who are not candidates for ICI maintenance and have higher serum EGF levels. As explained, clinical trials with CIMAvax-EGF started prior to the adoption of mutation testing, targeted therapies, and ICI as standards. Under these circumstances, a clear survival advantage was demonstrated in advanced NSCLC patients treated with CIMAvax-EGF as switch-maintenance (Figure 3 and Table 2). Particularly, a large benefit was seen in patients with high-serum EGF concentration, with a noteworthy 5-year survival rate of 18% and 26% for ADC and SCC histology, respectively (15) (Figure 3).
Given the low access to ICIs, the current standard for advanced NSCLC in Cuba for patients without actionable mutations and EGF concentration above 870 pg/ml consists of platinum doublets followed by switch maintenance with CIMavax-EGF. Moreover, given its low toxicity and the need of monthly re-immunizations, patients can receive booster vaccination at the primary care setting, under the supervision of trained family medicine physicians. However, this niche of patients will be contracted, both in Cuba and worldwide, as the access to ICIs increases.
Therefore, the larger opportunities of CIMAvax-EGF come from its potential use in combination with established therapies. In 2011, Hanahan and Weinberg proposed eight “hallmarks of cancer” (sustaining proliferative signaling, evading growth suppressors, resisting cell death, enabling replicative immortality, inducing angiogenesis, activating invasion and metastasis, reprogramming of cellular energy metabolism, and active evasion from attack by immune cells) in an attempt to explain the complexity of cancer biology (83). These hallmarks of cancer can become targets of therapeutic interventions and rational combinations.
EGF immune deprivation (with CIMAvax-EGF) targets the extracellular domain of EGFR, while TKIs recognize the intracellular cascade controlling cell proliferation and resistance to apoptosis. ICIs target the capacity of cancer cells to evade the immune system control. In the following sections, we debate potential combinations of CIMAvax-EGF with TKI or ICI in the treatment of advanced NSCLC.
Combining CIMAvax-EGF and EGFR-TKI
For a long time, oncologists thought that tumors bearing EGFR-activating mutations in the intracellular domain were mostly independent from external ligand stimulation. However, recent in vitro studies showed that this might not be absolute. Codony-Servat et al. showed that EGF induces a basal signal on EGFR mutated tumors, even while treated with potent TKI, such as gefitinib, erlotinib, afatinib, and osimertinib (Figure 6) (84). Such basal EGFR signaling sustains slow tumor proliferation and survival, contributing to the escape of the cancer cells under TKI therapy. These in vitro observations explain previous findings of a worse response to TKI in patients with high serum levels of EGFR ligands, such as amphiregulin, TGFα, and EGF (85). Indeed, treatment of the EGFR mutant cell lines with anti-EGF polyclonal antibodies enhanced the antitumor activity of TKIs and delayed the appearance of resistant clones (84).
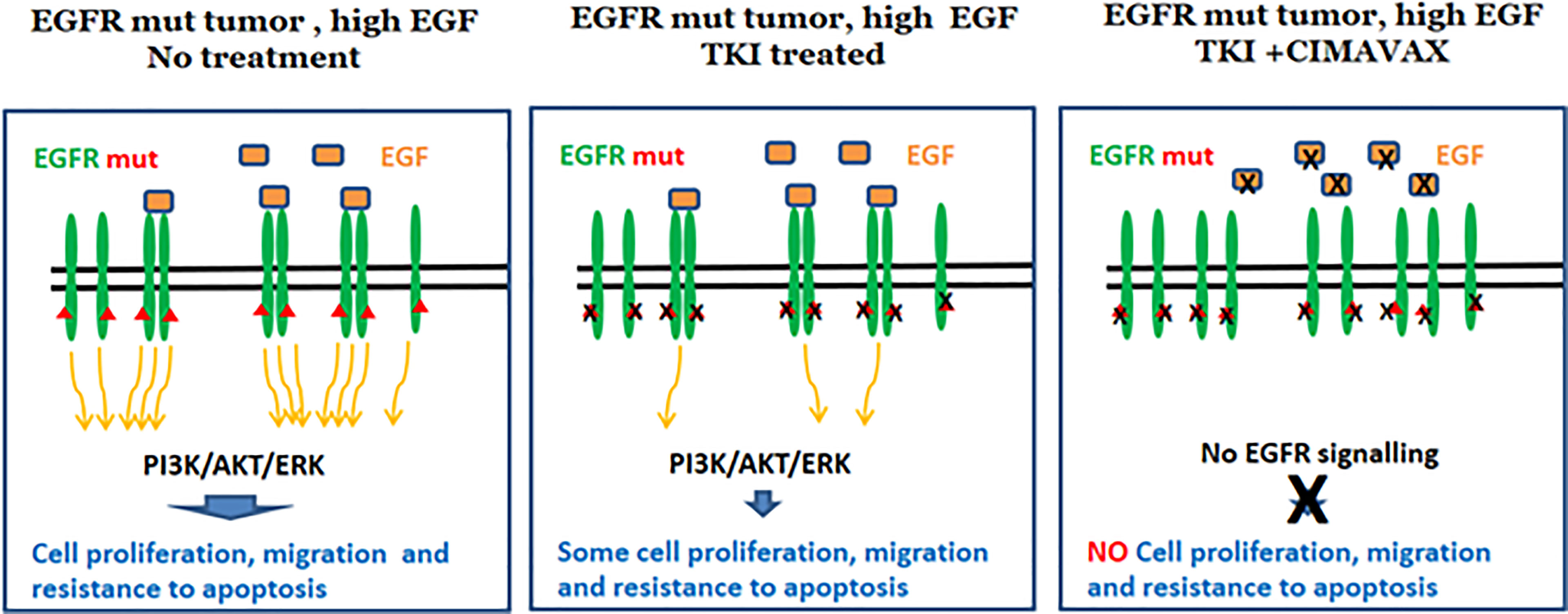
Figure 6 Rationale for CIMAvax-EGF combination with EGFR-TKI. Dual inhibition potentiates EGFR signaling inhibition.
Overall, the latter findings provide a novel rationale for combining CIMAvax-EGF with EGFR TKI (Figure 6). Limited clinical data exist on the use of dual targeting of EGFR in patients with mutated NSCLC. Cetuximab, an anti-EGFR mAb, was combined with afatinib in a phase I study, in patients with acquired resistance to gefitinib/erlotinib. The combination of afatinib with cetuximab as second line of treatment demonstrated modest clinical activity with a median PFS of 4.7 months, a response rate of 29%, and 44% of grade 3 related adverse events (86). Combination treatment of afatinib and nimotuzumab demonstrated an acceptable safety profile and encouraging antitumor activity in advanced NSCLC patients with acquired resistance to gefitinib or erlotinib. The median PFS and overall survival were 4.0 and 11.7 months, respectively (87).
Potential caveats of this approach are safety concerns mainly associated with the use of high-affinity antibodies (cetuximab or panitumumab) and the lack of a strategy for selecting patients most likely to benefit. Therefore, the addition of CIMAvax-EGF to TKI is an appealing alternative, given CIMAvax-EGF excellent safety profile and the possibility of preselecting patients with high EGF concentration in serum (Table 3). Combination of CIMAvax-EGF in first line with TKI (EPICAL study) was launched in 2018. The trial will be completed in June 2021 (NCT03623750).
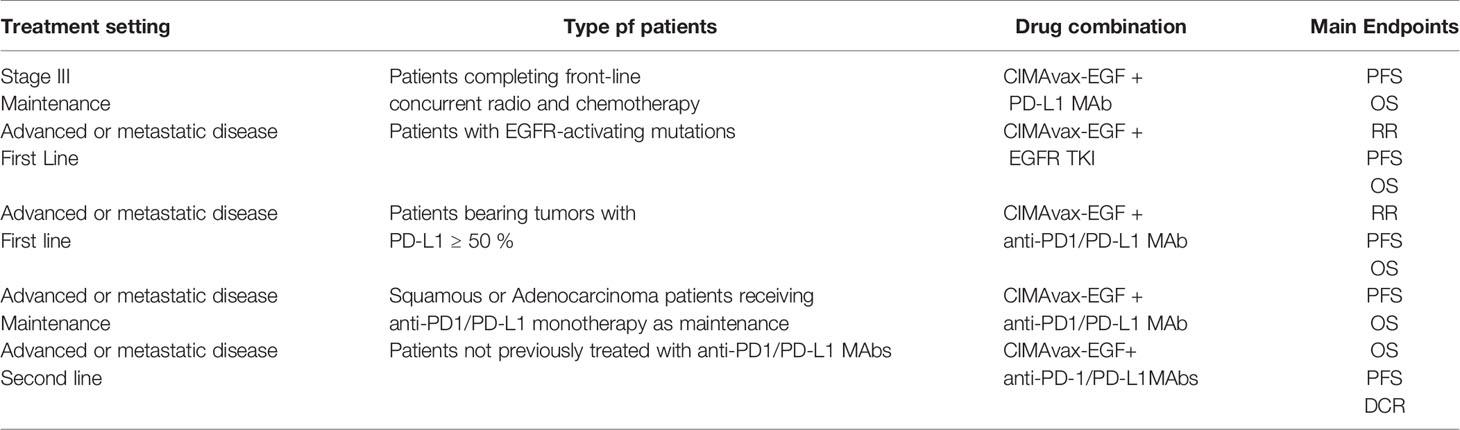
Table 3 Potential combination trials of CIMAvax-EGF plus EGFR TKIs or ICIs.
Combining CIMAvax-EGF and ICI
Immune evasion and growth factor dependence are two hallmarks of cancer, which can be targeted by ICI and CIMAavax-EGF or anti-EGFR MAbs. However, these two properties are clearly connected at the molecular level. EGFR activation has been associated with a down regulation of MHC-I and the antigen processing machinery (Figure 7), making tumor cells less sensitive to the immune system attack (88). For instance, treatment of cancer cells lines with the anti-EGFR MAb nimotuzumab in vitro induced the upregulation MHC class I expression (89). EGFR activation has also been associated with the induction of an immunosuppressive environment by the tumor cells, via up-regulation of pro-inflammatory cytokine secretion (90, 91). Transcription factors, like Stat3, NF-Кβ, and HIF-1α, link oncogene activation signaling pathways with these molecular mechanisms (92). Therefore, the use of ICI on tumors with a strong active signaling via EGFR might be less effective, given that the cancer cells impair, at least partially, the therapeutic effect of the activated CD8 T cells (Figure 7).
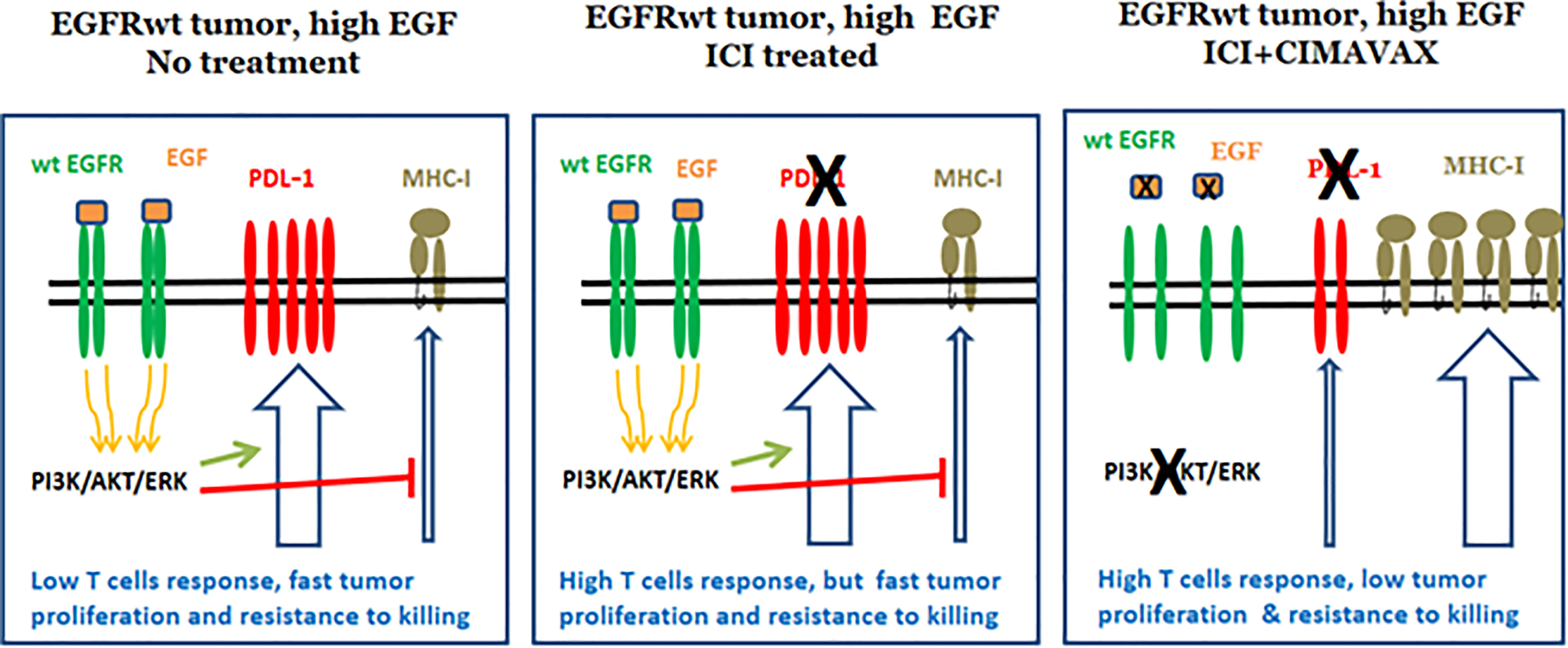
Figure 7 Reduction of PD-L1 expression after EGF depletion.
Furthermore, compelling evidences on the relationship between EGFR and PD-L1 expression in tumors are progressively accumulating (93–95). EGFR activation, through the interaction with natural ligands or by the existence of activating mutations, upregulates the expression of PD-L1 in cancer cells in vitro (96). Moreover, in lung cancer patients, there is a positive correlation between EGFR and PD-L1 expression (97). Therefore, the inhibition of EGFR signaling might reduce PD-L1 expression in the tumor cells, further reducing PD-L1–mediated tumor evasion. This effect enhances the effectiveness of the CD8 T cell response potentiated by ICI treatment (Figure 7). ICI treatments would inhibit PD1-PD-L1 interaction in the tumor cells, but also in the antigen presenting cells inside the tumor and lymph nodes, further promoting CD8 T cells activation.
Overall, the latter findings provide a novel rationale for the combination of CIMAvax-EGF with ICI (Figure 7). Combining checkpoint inhibitors and EGF deprivation would restore the immune system activation, presumably with higher sensitivity as a result of the EGFR signaling inhibition. Moreover, EGFR inhibition shall have a direct antitumor effect mediated by the blockade of the tumor proliferation and apoptosis induction.
Recently, the first results of combining an anti-EGFR antibody with an ICI in advanced NSCLC were reported. Necitumumab, an anti-EGFR mAb, was combined with pembrolizumab in 64 stage IV NSCLC patients who had progressed after platinum-based doublet, irrespective of PD-L1 expression and histology. The authors argue a manageable safety with SAEs in 42% of the patients. Median PFS was 4.1 months, and OS at 6 months was 74.7% (98) (Table 2).
CIMAvax-EGF is able to inhibit EGFR-mediated signaling without the well-recognized toxicities associated with the use of high affinities anti-EGFR mAb (15, 31, 99). Thus, it offers an attractive alternative to produce a synergistic effect between EGFR signaling inhibition and PD1 blockade without major toxicity concerns (Table 3). Below we discuss three different scenarios to do so:
Combination of CIMAvax-EGF and Nivolumab in Second Line
A phase I/II clinical trial combining CIMAvax-EGF with nivolumab, as second line in NSCLC is open and recruiting patients at the Roswell Park Comprehensive Cancer Center (NCT02955290). Safety profile was good with no significant toxicities added by CIMAvax-EGF to the anti-PD1. A fast induction of anti-EGF antibodies and a reduction of EGF concentration in patient’s serum were also observed (100). Remarkably, overall response rate was 30% among PD-L1–negative patients and a median OS of 22.4 months was reported for patients with wild type KRAS (101). These figures compare well with those reported for nivolumab alone as second-line treatment (102).
However, this specific niche of patients (ICI second line, Figure 5) will be progressively reduced as the use of ICIs in first line becomes widely implemented. Therefore, there is a need to relocate the combination of CIMAvax-EGF with ICI in the context of first-line or maintenance scenarios.
Combination of CIMAvax-EGF and ICI in Maintenance
CIMAvax-EGF can be used for prolonged periods as maintenance treatment without cumulative toxicity (31). This finding could support the use of CIMAvax-EGF in the maintenance setting, with pembrolizumab or atezolizumab in the squamous scenario (Table 3). This strategy can also apply to adenocarcinoma patients that would receive maintenance therapy with checkpoint inhibitors alone. This could be the case of patients with high PD-L1 expression, receiving chemo-immunotherapy in the front line, but maintenance therapy with ICI monotherapy. Preselection of patients with high EGF concentration and KRAS-wild type would be highly recommended. This combination shall increase response duration and PFS, increasing the proportion of long-term survivors.
Combination of CIMAvax-EGF and ICI in First Line
Other alternative is to position CIMAvax-EGF in combination with pembrolizumab or atezolizumab, as starting therapy in stage IV NSCLC with 50% overexpression of PD-L1, irrespective of histology (Table 3). Preselecting patients with high EGF serum concentration and KRAS wild type will be crucial to potentiate combination. The benefit of using the combination as first line shall increase objective response as well as response duration and PFS.
Combination of CIMAvax-EGF and Durvalumab in Stage III Tumors
The last alternative would be to combine CIMAvax-EGF with durvalumab in stage III NSCLC after completing front-line concurrent radio and chemotherapy (Table 3). In this scenario, median progression-free survival from randomization was 17.2 months with durvalumab versus 5.6 months with placebo (48). We hypothesize that combining CIMAvax-EGF with the anti-PDL1 can further increase PFS and overall survival in this patient subset.
Discussion
CIMAvax-EGF is a new class of therapy aiming to induce antibodies against self-growth factors. It targets the EGF-EGFR pathway, a validated target on tumorigenesis. However, its larger impact will depend on the smart insertion of immune EGF deprivation into the complex algorithm of lung cancer management. Exploring the overlapping zone between interventions in the control of cell proliferation and immune evasion should be a priority of the current therapeutic algorithms.
Understanding the therapeutic potential of CIMAvax-EGF will demand a series of clinical trials devoted to identify the highest impact niches, potentiation with other treatment, optimal schedules, and new biological markers. The potential role of CIMAvax-EGF in increasing the clinical response achieved with other treatments like TKI or ICI is particularly attractive. Alternatively, CIMAvax-EGF can also help subgroups of patients who are not benefiting from the current therapies, like PD-L1 negative or EGFR wild type individuals.
In summary, CIMAvax-EGF is a therapeutic approach that has already been proven to be safe and efficacious, mainly in patients with high EGF levels and wild-type KRAS. We hypothesize that the smart combination of CIMAVax-EGF with the established EGFR TKI and ICIs can further contribute to the transition of advanced cancer to a chronic disease, compatible with years of quality life.
Author Contributions
All authors contributed to the article and approved the submitted version.
Funding
This research was funded by the Center of Molecular Immunology and the Cuban Ministry of Health.
Conflict of Interest
Authors TC, OS, KL, AL currently work for the Center of Molecular Immunology, the institution that generated and originally patented CIMAvax-EGF.
The remaining author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Xu Y, Zong S, Gao X, Zhang H, Wang B, Li P, et al. Combined Treatment of ABT199 and Irinotecan Suppresses KRAS-Mutant Lung Cancer Cells. Gene (2019) 688:1–6. doi: 10.1016/j.gene.2018.11.018
2. Lynch T Jr., Kim E. Optimizing Chemotherapy and Targeted Agent Combinations in NSCLC. Lung Cancer (2005) 50S2:S25–32. doi: 10.1016/S0169-5002(05)81570-3
3. Zito Marino F, Bianco R, Accardo M, Ronchi A, Cozzolino I, Morgillo F, et al. Molecular Heterogeneity in Lung Cancer: From Mechanisms of Origin to Clinical Implications. Int J Med Sci (2019) 16(7):981–9. doi: 10.7150/ijms.34739
4. Hodkinson P, Mackinnon A, Sethi T. Targeting Growth Factors in Lung Cancer. Chest (2008) 133:1209–16. doi: 10.1378/chest.07-2680
5. Friedlaender A, Tsantoulis P, Chevallier M, De Vito C, Addeo A. The Impact of Variant Allele Frequency in EGFR Mutated NSCLC Patients on Targeted Therapy. Front Oncol (2021) 11:644472. doi: 10.3389/fonc.2021.644472
6. Jamal-Hanjani M, Wilson GA, McGranahan N, Birkbak NJ, Watkins TBK, Veeriah S, et al. Tracking the Evolution of Non-Small-Cell Lung Cancer. N Engl J Med (2017) 376(22):2109–21. doi: 10.1056/NEJMoa1616288
7. Evan G. Can’t Kick That Oncogene Habit. Cancer Cell (2006) 10:345–7. doi: 10.1016/j.ccr.2006.10.013
8. Hynes NE LH. ERBB Receptors and Cancer: The Complexity of Targeted Inhibitors. Nat Rev Cancer (2005) 5:341–54. doi: 10.1038/nrc1609
9. Mendelsohn J. Targeting the Epidermal Growth Factor Receptor for Cancer Therapy. J Clin Oncol (2002) 20:1S–13S.
10. Paez J, Janne P, Lee J, Tracy S, Greulich H, Gabriel S, et al. EGFR Mutations in Lung Cancer: Correlation With Clinical Response to Gefitinib Therapy. Sci (New York NY) (2004) 304:1497–500. doi: 10.1126/science.1099314
11. Wilson KJ, Mill C, Lambert S, Buchman J, Wilson TR, Hernandez-Gordillo V, et al. EGFR Ligands Exhibit Functional Differences in Models of Paracrine and Autocrine Signaling. Growth Factors (2012) 30(2):107–16. doi: 10.3109/08977194.2011.649918
12. Blanco-Prieto S, Vázquez L, Rodríguez M, Barcia L, Fernández A, Botana M, et al. Serum Calprotectin, CD26 and EGF to Establish a Panel for the Diagnosis of Lung Cancer. PLoSONE (2015) 10(5):1–17. doi: 10.1371/journal.pone.0127318
13. Rosell R, Neninger E, Nicolson M, Huber RM, Thongprasert S, Parikh PM, et al. Pathway Targeted Immunotherapy: Rationale and Evidence of Durable Clinical Responses With A Novel, EGF-Directed Agent for Advanced Nsclc. J Thorac Oncol (2016) 11(11):1954–61. doi: 10.1016/j.jtho.2016.08.132
14. Hirsch F, Scaglioti G, Langer C, Varella-Garcia M, Franklin W. Epidermal Growth Factor Family of Receptors in Preneoplasia and Lung Cancer, Perspectives for Targeted Therapies. Lung Cancer (2003) 41(Suppl 1):S29–42. doi: 10.1016/S0169-5002(03)00137-5
15. Rodriguez PC, Popa X, Martinez O, Mendoza S, Santiesteban E, Crespo T, et al. A Phase III Clinical Trial of the Epidermal Growth Factor Vaccine CIMAvax-EGF as Switch Maintenance Therapy in Advanced Non-Small Cell Lung Cancer Patients. Clin Cancer Res (2016) 22(15):3782–90. doi: 10.1158/1078-0432.CCR-15-0855
16. Gonzalez G, Crombet T, Catala M, Mirabal V, Hernandez JC, Gonzalez Y, et al. A Novel Cancer Vaccine Composed of Human-Recombinant Epidermal Growth Factor Linked to A Carrier Protein: Report of a Pilot Clinical Trial. Ann Oncol (1998) 9(4):431–5. doi: 10.1023/A:1008261031034
17. Gonzalez G, Crombet T, Neninger E, Viada C, Lage A. Therapeutic Vaccination With Epidermal Growth Factor (EGF) in Advanced Lung Cancer: Analysis of Pooled Data From Three Clinical Trials. Hum Vaccin (2007) 3(1):8–13. doi: 10.4161/hv.3.1.3537
18. Gonzalez G, Lage A. Cancer Vaccines for Hormone/Growth Factor Immune Deprivation: A Feasible Approach for Cancer Treatment. Curr Cancer Drug Targets (2007) 7(3):229–41. doi: 10.2174/156800907780618310
19. Dafni U, Tsourti Z, Vervita K, Peters S. Immune Checkpoint Inhibitors, Alone or in Combination With Chemotherapy, as First-Line Treatment for Advanced Non-Small Cell Lung Cancer. A Syst Rev Netw Meta Anal Lung Cancer (2019) 134:127–40. doi: 10.1016/j.lungcan.2019.05.029
20. Franek J, Cappelleri JC, Larkin-Kaiser KA, Wilner KD, Sandin R. Systematic Review and Network Meta-Analysis of First-Line Therapy for Advanced EGFR-Positive Non-Small-Cell Lung Cancer. Future Oncol (2019) 15(24):2857–71. doi: 10.2217/fon-2019-0270
21. Sun MLM, Hee H, Hye RK. Immunotherapy for Non-Small Cell Lung Cancer: Current Landscape and Future Perspectives. Immune Netw (2020) 20(1):1–14. doi: 10.4110/in.2020.20.e10
22. Garcia B, Neninger E, de la Torre A, Leonard I, Martinez R, Viada C, et al. Effective Inhibition of the Epidermal Growth Factor/Epidermal Growth Factor Receptor Binding by Anti-Epidermal Growth Factor Antibodies Is Related to Better Survival in Advanced Non-Small-Cell Lung Cancer Patients Treated With the Epidermal Growth Factor Cancer Vaccine. Clin Cancer Res (2008) 14(3):840–6. doi: 10.1158/1078-0432.CCR-07-1050
23. Neninger Vinageras E, de la Torre A, Osorio Rodriguez M, Catala Ferrer M, Bravo I, Mendoza del Pino M, et al. Phase II Randomized Controlled Trial of an Epidermal Growth Factor Vaccine in Advanced Non-Small-Cell Lung Cancer. J Clin Oncol (2008) 26(9):1452–8. doi: 10.1200/JCO.2007.11.5980
24. Rodriguez PC, Gonzalez I, Gonzalez A, Avellanet J, Lopez A, Perez R, et al. Priming and Boosting Determinants on the Antibody Response to An Epidermal Growth Factor-Based Cancer Vaccine. Vaccine (2008) 26(36):4647–54. doi: 10.1016/j.vaccine.2008.07.003
25. Popa X, Garcia B, Fuentes KP, Huerta V, Alvarez K, Viada CE, et al. Anti-EGF Antibodies as Surrogate Biomarkers of Clinical Efficacy in Stage IIIB/IV Non-Small-Cell Lung Cancer Patients Treated With An Optimized CIMAvax-EGF Vaccination Schedule. Oncoimmunology (2020) 9(1):1762465. doi: 10.1080/2162402X.2020.1762465
26. Hobor S, Van Emburgh BO, Crowley E, Misale S, Di Nicolantonio F, Bardelli A. Tgfalpha and Amphiregulin Paracrine Network Promotes Resistance to EGFR Blockade in Colorectal Cancer Cells. Clin Cancer Res (2014) 20(24):6429–38. doi: 10.1158/1078-0432.CCR-14-0774
27. Mutsaers AJ, Francia G, Man S, Lee CR, Ebos JM, Wu Y, et al. Dose-Dependent Increases in Circulating TGF-alpha and Other EGFR Ligands Act as Pharmacodynamic Markers for Optimal Biological Dosing of Cetuximab and Are Tumor Independent. Clin Cancer Res (2009) 15(7):2397–405. doi: 10.1158/1078-0432.CCR-08-1627
28. Tagliamento M, Genova C, Rijavec E, Rossi G, Biello F, Dal Bello MG, et al. Afatinib and Erlotinib in the Treatment of Squamous-Cell Lung Cancer. Expert Opin Pharmacother (2018) 19(18):2055–62. doi: 10.1080/14656566.2018.1540591
29. Saavedra D, Garcia B, Lorenzo-Luaces P, Gonzalez A, Popa X, Fuentes KP, et al. Biomarkers Related to Immunosenescence: Relationships With Therapy and Survival in Lung Cancer Patients. Cancer Immunol Immunother (2016) 65(1):37–45. doi: 10.1007/s00262-015-1773-6
30. Lorenzo-Luaces P, Sanchez L, Saavedra D, Crombet T, van der Elst W, Alonso A, et al. Identifying Predictive Biomarkers of CIMAvaxEGF Success in Non-Small Cell Lung Cancer Patients. BMC Cancer (2020) 20(1):772. doi: 10.1186/s12885-020-07284-4
31. Saavedra D, Neninger E, Rodriguez C, Viada C, Mazorra Z, Lage A, et al. Cimavax-EGF: Toward Long-Term Survival of Advanced NSCLC. Semin Oncol (2018) 45(1-2):34–40. doi: 10.1053/j.seminoncol.2018.04.009
32. Berthelet E, Pickles T, Lee KW, Liu M, Truong PT, Prostate Cancer Outcomes I. Long-Term Androgen Deprivation Therapy Improves Survival in Prostate Cancer Patients Presenting With Prostate-Specific Antigen Levels > 20 Ng/Ml. Int J Radiat Oncol Biol Phys (2005) 63(3):781–7. doi: 10.1016/j.ijrobp.2005.02.034
33. Fan P, Maximov PY, Curpan RF, Abderrahman B, Jordan VC. The Molecular, Cellular and Clinical Consequences of Targeting the Estrogen Receptor Following Estrogen Deprivation Therapy. Mol Cell Endocrinol (2015) 418 Pt 3:245–63. doi: 10.1016/j.mce.2015.06.004
34. Johnson DH. Evolution of Cisplatin-Based Chemotherapy in non-Small Cell Lung Cancer: A Historical Perspective and the Eastern Cooperative Oncology Group Experience. Chest (2000) 117(4 Suppl 1):133S–7S. doi: 10.1378/chest.117.4_suppl_1.133S
35. Cooper JA, Hunter T. Similarities and Differences Between the Effects of Epidermal Growth Factor and Rous Sarcoma Virus. J Cell Biol (1981) 91(3 Pt 1):878–83. doi: 10.1083/jcb.91.3.878
36. Osborne CK, Hamilton B, Titus G, Livingston RB. Epidermal Growth Factor Stimulation of Human Breast Cancer Cells in Culture. Cancer Res (1980) 40(7):2361–6.
37. Lombardero J, Perez R, Lage A. Epidermal Growth Factor Inhibits Thymidine Incorporation in Ehrlich Ascites Tumor Cells In Vivo. Neoplasma (1986) 33(4):423–9.
38. Perez R, Pascual M, Macias A, Lage A. Epidermal Growth Factor Receptors in Human Breast Cancer. Breast Cancer Res Treat (1984) 4(3):189–93. doi: 10.1007/BF01806484
39. Hirsch FR. The Role of Genetic Testing in the Prediction of Response to EGFR Inhibitors in NSCLC. Oncogene (2009) 28:S1–3. doi: 10.1038/onc.2009.195
40. Tsao MS, Sakurada A, Cutz JC, Zhu CQ, Kamel-Reid S, Squire J, et al. Erlotinib in Lung Cancer - Molecular and Clinical Predictors of Outcome. N Engl J Med (2005) 353(2):133–44. doi: 10.1056/NEJMoa050736
41. da Cunha Santos G, Shepherd FA, Tsao MS. EGFR Mutations and Lung Cancer. Annu Rev Pathol (2011) 6:49–69. doi: 10.1146/annurev-pathol-011110-130206
42. Rossi A, Maione P, Sacco PC, Sgambato A, Casaluce F, Ferrara ML, et al. ALK Inhibitors and Advanced Non-Small Cell Lung Cancer (Review). Int J Oncol (2014) 45(2):499–508. doi: 10.3892/ijo.2014.2475
43. Fehrenbacher L, Spira A, Ballinger M, Kowanetz M, Vansteenkiste J, Mazieres J, et al. Atezolizumab Versus Docetaxel for Patients With Previously Treated Non-Small-Cell Lung Cancer (POPLAR): A Multicentre, Open-Label, Phase 2 Randomised Controlled Trial. Lancet (2016) 387(10030):1837–46. doi: 10.1016/S0140-6736(16)00587-0
44. Herbst R. Pembrolizumab Versus Docetaxel for Previously Treated, PD-L1-Positive, Advanced Non-Small-Cell Lung Cancer (KEYNOTE-010): A Randomised Controlled Trial. Lancet (2016) 387:1540–50. doi: 10.1016/S0140-6736(15)01281-7
45. Horn L, Spigel DR, Vokes EE, Holgado E, Ready N, Steins M, et al. Nivolumab Versus Docetaxel in Previously Treated Patients With Advanced Non-Small-Cell Lung Cancer: Two-Year Outcomes From Two Randomized, Open-Label, Phase Iii Trials (CheckMate 017 and CheckMate 057). J Clin Oncol (2017) 35(35):3924–33. doi: 10.1200/JCO.2017.74.3062
46. Buchbinder EI, Desai A. CTLA-4 and PD-1 Pathways: Similarities, Differences, and Implications of Their Inhibition. Am J Clin Oncol (2016) 39(1):98–106. doi: 10.1097/COC.0000000000000239
47. Yamada T, Uchino J, Chihara Y, Shimamoto T, Iwasaku M, Tamiya N, et al. Rationale and Design of A Phase II Trial of Durvalumab Treatment in Patients With NSCLC Ineligible for Stage III Chemoradiotherapy Following Radiation Monotherapy (SPIRAL-RT Study). Ther Adv Med Oncol (2020) 12:1758835920927841. doi: 10.1177/1758835920927841
48. Antonia SJ, Ozguroglu M. Durvalumab in Stage III Non-Small-Cell Lung Cancer. N Engl J Med (2018) 378(9):869–70. doi: 10.1056/NEJMc1716426
49. Gray JE, Villegas A, Daniel D, Vicente D, Murakami S, Hui R, et al. Three-Year Overall Survival With Durvalumab After Chemoradiotherapy in Stage Iii NSCLC-Update From PACIFIC. J Thorac Oncol (2020) 15(2):288–93. doi: 10.1016/j.jtho.2019.10.002
50. Jordan EJ, Kim HR, Arcila ME, Barron D, Chakravarty D, Gao J, et al. Prospective Comprehensive Molecular Characterization of Lung Adenocarcinomas for Efficient Patient Matching to Approved and Emerging Therapies. Cancer Discovery (2017) 7(6):596–609. doi: 10.1158/2159-8290.CD-16-1337
51. Nagano T, Tachihara M, Nishimura Y. Molecular Mechanisms and Targeted Therapies Including Immunotherapy for Non-Small Cell Lung Cancer. Curr Cancer Drug Targets (2019) 19(8):595–630. doi: 10.2174/1568009619666181210114559
52. Santarpia MG,N, Rosell R. Strategies to Overcome Resistance to Tyrosine Kinase Inhibitors in Non-Small-Cell Lung Cancer. Expert Rev Clin Pharmacol (2015) 8:461–77. doi: 10.1586/17512433.2015.1055252
53. Soria JC, Ohe Y, Vansteenkiste J, Reungwetwattana T, Chewaskulyong B, Lee KH, et al. Osimertinib in Untreated Egfr-Mutated Advanced Non-Small-Cell Lung Cancer. N Engl J Med (2018) 378(2):113–25. doi: 10.1056/NEJMoa1713137
54. Lee CK, Man J, Lord S, Links M, Gebski V, Mok T, et al. Checkpoint Inhibitors in Metastatic Egfr-Mutated Non-Small Cell Lung Cancer-a Meta-Analysis. J Thorac Oncol (2017) 12(2):403–7. doi: 10.1016/j.jtho.2016.10.007
55. Cavanna L, Citterio C, Orlandi E. Immune Checkpoint Inhibitors in EGFR-mutation Positive TKI-treated Patients With Advanced Non-Small-Cell Lung Cancer Network Meta-Analysis. Oncotarget (2019) 10(2):209–15. doi: 10.18632/oncotarget.26541
56. Nakagawa K, Garon EB, Seto T, Nishio M, Ponce Aix S, Paz-Ares L, et al. Ramucirumab Plus Erlotinib in Patients With Untreated, EGFR-mutated, Advanced Non-Small-Cell Lung Cancer (RELAY): A Randomised, Double-Blind, Placebo-Controlled, Phase 3 Trial. Lancet Oncol (2019) 20(12):1655–69. doi: 10.1016/S1470-2045(19)30634-5
57. Han C, Zhang A, Liu Z, Moore C, Fu YX. Small Molecular Drugs Reshape Tumor Microenvironment to Synergize With Immunotherapy. Oncogene (2021) 40(5):885–98. doi: 10.1038/s41388-020-01575-7
58. Yang JC, Gadgeel SM, Sequist LV, Wu CL, Papadimitrakopoulou VA, Su WC, et al. Pembrolizumab in Combination With Erlotinib or Gefitinib as First-Line Therapy for Advanced Nsclc With Sensitizing EGFR Mutation. J Thorac Oncol (2019) 14(3):553–9. doi: 10.1016/j.jtho.2018.11.028
59. Schoenfeld AJ, Arbour KC, Rizvi H, Iqbal AN, Gadgeel SM, Girshman J, et al. Severe Immune-Related Adverse Events are Common With Sequential PD-(L)1 Blockade and Osimertinib. Ann Oncol (2019) 30(5):839–44. doi: 10.1093/annonc/mdz077
60. Mok TSK, Wu YL, Kudaba I, Kowalski DM, Cho BC, Turna HZ, et al. Pembrolizumab Versus Chemotherapy for Previously Untreated, PD-L1-Expressing, Locally Advanced or Metastatic Non-Small-Cell Lung Cancer (KEYNOTE-042): A Randomised, Open-Label, Controlled, Phase 3 Trial. Lancet (2019) 393(10183):1819–30. doi: 10.1016/S0140-6736(18)32409-7
61. Gadgeel S, Rodriguez-Abreu D, Speranza G, Esteban E, Felip E, Domine M, et al. Updated Analysis From KEYNOTE-189: Pembrolizumab or Placebo Plus Pemetrexed and Platinum for Previously Untreated Metastatic Nonsquamous Non-Small-Cell Lung Cancer. J Clin Oncol (2020) 38(14):1505–17. doi: 10.1200/JCO.19.03136
62. Paz-Ares L, Vicente D, Tafreshi A, Robinson A, Parra HS, Mazieres J, et al. A Randomized, Placebo-Controlled Trial of Pembrolizumab Plus Chemotherapy in Patients With Metastatic Squamous Non-Small-Cell Lung Cancer: Protocol-Specified Final Analysis of KEYNOTE-407. J Thorac Oncol (2020) 15(10):1657–69. doi: 10.1016/j.jtho.2020.06.015
63. Reck M, Rodriguez-Abreu D, Robinson AG, Hui R, Csoszi T, Fulop A, et al. Updated Analysis of KEYNOTE-024: Pembrolizumab Versus Platinum-Based Chemotherapy for Advanced Non-Small-Cell Lung Cancer With Pd-L1 Tumor Proportion Score of 50% or Greater. J Clin Oncol (2019) 37(7):537–46. doi: 10.1200/JCO.18.00149
64. Gravara LD, Battiloro C, Cantile R, Letizia A, Vitiello F, Montesarchio V, et al. Chemotherapy and/or Immune Checkpoint Inhibitors in NSCLC First-Line Setting: What is the Best Approach? Lung Cancer Manag (2020) 9(1):LMT22. doi: 10.2217/lmt-2019-0018
65. Pacheco JM. Keynote-407: Changing the Way We Treat Stage IV Squamous non-Small Cell Lung Cancer. Transl Lung Cancer Res (2020) 9(1):148–53. doi: 10.21037/tlcr.2020.01.12
66. Spigel D, de Marinis F, Giaccone G, Reinmuth N, Vergnenegre A, Barrios C, et al. Lba78 IMpower110: Interim Overall Survival (OS) Analysis of a Phase III Study of Atezolizumab (Atezo) vs Platinum-Based Chemotherapy (Chemo) as First-Line (1L) Treatment (Tx) in PD-L1–selected Nsclc. Annals of Oncology (2019) 30(Supplement_5):v915. doi: 10.1093/annonc/mdz293
67. Reck M, Schenker M, Lee KH, Provencio M, Nishio M, Lesniewski-Kmak K, et al. Nivolumab Plus Ipilimumab Versus Chemotherapy As First-Line Treatment in Advanced Non-Small-Cell Lung Cancer With High Tumour Mutational Burden: Patient-Reported Outcomes Results From the Randomised, Open-Label, Phase III CheckMate 227 Trial. Eur J Cancer (2019) 116:137–47. doi: 10.1016/j.ejca.2019.05.008
68. Gandhi L, Rodriguez-Abreu D, Gadgeel S, Esteban E, Felip E, De Angelis F, et al. Pembrolizumab Plus Chemotherapy in Metastatic Non-Small-Cell Lung Cancer. N Engl J Med (2018) 378(22):2078–92. doi: 10.1056/NEJMoa1801005
69. Reck M, Jotte RM, Socinski MA. Atezolizumab Treatment of Nonsquamous Nsclc. N Engl J Med (2018) 379(12):1188. doi: 10.1056/NEJMc1809195
70. Aguiar PN Jr., Perry LA, Penny-Dimri J, Babiker H, Tadokoro H, de Mello RA, et al. The Effect of PD-L1 Testing on the Cost-Effectiveness and Economic Impact of Immune Checkpoint Inhibitors for the Second-Line Treatment of NSCLC. Ann Oncol (2017) 28(9):2256–63. doi: 10.1093/annonc/mdx305
71. She L, Hu H, Liao M, Xia X, Shi Y, Yao L, et al. Cost-Effectiveness Analysis of Pembrolizumab Versus Chemotherapy as First-Line Treatment in Locally Advanced or Metastatic Non-Small Cell Lung Cancer With PD-L1 Tumor Proportion Score 1% or Greater. Lung Cancer (2019) 138:88–94. doi: 10.1016/j.lungcan.2019.10.017
72. Aguiar P Jr., Giglio AD, Perry LA, Penny-Dimri J, Babiker H, Tadokoro H, et al. Cost-Effectiveness and Budget Impact of Lung Cancer Immunotherapy in South America: Strategies to Improve Access. Immunotherapy (2018) 10(10):887–97. doi: 10.2217/imt-2017-0183
73. Criss SD, Palazzo L, Watson TR, Paquette AM, Sigel K, Wisnivesky J, et al. Cost-Effectiveness of Pembrolizumab for Advanced Non-Small Cell Lung Cancer Patients With Varying Comorbidity Burden. PloS One (2020) 15(1):e0228288. doi: 10.1371/journal.pone.0228288
74. Hu X, Hay JW. First-Line Pembrolizumab in PD-L1 Positive Non-Small-Cell Lung Cancer: A Cost-Effectiveness Analysis From the UK Health Care Perspective. Lung Cancer (2018) 123:166–71. doi: 10.1016/j.lungcan.2018.07.012
75. Wan N, Zhang TT, Hua SH, Lu ZL, Ji B, Li LX, et al. Cost-Effectiveness Analysis of Pembrolizumab Plus Chemotherapy With PD-L1 Test for the First-Line Treatment of NSCLC. Cancer Med (2020) 9(5):1683–93. doi: 10.1002/cam4.2793
76. Fidias PM, Dakhil SR, Lyss AP, Loesch DM, Waterhouse DM, Bromund JL, et al. Phase III Study of Immediate Compared With Delayed Docetaxel After Front-Line Therapy With Gemcitabine Plus Carboplatin in Advanced Non-Small-Cell Lung Cancer. J Clin Oncol (2009) 27(4):591–8. doi: 10.1200/JCO.2008.17.1405
77. Ciuleanu T, Brodowicz T, Zielinski C, Kim JH, Krzakowski M, Laack E, et al. Maintenance Pemetrexed Plus Best Supportive Care Versus Placebo Plus Best Supportive Care for Non-Small-Cell Lung Cancer: A Randomised, Double-Blind, Phase 3 Study. Lancet (2009) 374(9699):1432–40. doi: 10.1016/S0140-6736(09)61497-5
78. Burdett S, Stehphens R, Stewart L, Tierney J, Auperin A, Le Chevalier T, et al. Chemotherapy in Addition to Supportive Care Improves Survival in Advanced Non-Small-Cell Lung Cancer: A Systematic Review and Meta-Analysis of Individual Patient Data From 16 Randomized Controlled Trials. J Clin Oncol (2008) 26:4617– 25. doi: 10.1200/JCO.2008.17.7162
79. Socinski MA, Jotte RM, Cappuzzo F, Orlandi F, Stroyakovskiy D, Nogami N, et al. Atezolizumab for First-Line Treatment of Metastatic Nonsquamous Nsclc. N Engl J Med (2018) 378(24):2288–301. doi: 10.1056/NEJMoa1716948
80. Reck M, Brahmer J, Bennett B, Taylor F, Penrod JR, DeRosa M, et al. Evaluation of Health-Related Quality of Life and Symptoms in Patients With Advanced Non-Squamous Non-Small Cell Lung Cancer Treated With Nivolumab or Docetaxel in CheckMate 057. Eur J Cancer (2018) 102:23–30. doi: 10.1016/j.ejca.2018.05.005
81. Allemani C, Matsuda T, Di Carlo V, Harewood R, Matz M, Niksic M, et al. Global Surveillance of Trends in Cancer Survival 2000-14 (Concord-3): Analysis of Individual Records for 37 513 025 Patients Diagnosed With One of 18 Cancers From 322 Population-Based Registries in 71 Countries. Lancet (2018) 391(10125):1023–75. doi: 10.1016/S0140-6736(17)33326-3
82. Santucci C, Carioli G, Bertuccio P, Malvezzi M, Pastorino U, Boffetta P, et al. Progress in Cancer Mortality, Incidence, and Survival: A Global Overview. Eur J Cancer Prev (2020) 29(5):367–81. doi: 10.1097/CEJ.0000000000000594
83. Hanahan D, Weinberg RA. Hallmarks of Cancer: The Next Generation. Cell (2011) 144(5):646–74. doi: 10.1016/j.cell.2011.02.013
84. Codony-Servat J, García-Roman S, Molina-Vila M, Bertran-Alamillo J, Giménez-Capitán A, Viteri S, et al. Anti-Epidermal Growth Factor Vaccine Antibodies Enhance the Efficacy of Tyrosine Kinase Inhibitors and Delay the Emergence of Resistance in EGFR Mutant Lung Cancer Cells. J Thorac Oncol (2018) 13(9):1324–37. doi: 10.1016/j.jtho.2018.04.030
85. Moya-Horno I, Viteri S, Karachaliou N, Rosell R. Combination of Immunotherapy With Targeted Therapies in Advanced Non-Small Cell Lung Cancer (NSCLC). Ther Adv Med Oncol (2018) 10:1758834017745012. doi: 10.1177/1758834017745012
86. Janjijian Y. Dual Inhibition of EGFR With Afatinib and Cetuximab in Kinase Inhibitor–Resistant EGFR-Mutant Lung Cancer With and Without T790M Mutations. Cancer Discovery (2014) 4:1036–45. doi: 10.1158/2159-8290.CD-14-0326
87. Lee JY, Sun JM, Lim SH, Kim HS, Yoo KH, Jung KS, et al. A Phase Ib/Ii Study of Afatinib in Combination With Nimotuzumab in Non-Small Cell Lung Cancer Patients With Acquired Resistance to Gefitinib or Erlotinib. Clin Cancer Res (2016) 22(9):2139–45. doi: 10.1158/1078-0432.CCR-15-1653
88. Watanabe S, Hayashi H, Haratani K, Shimizu S, Tanizaki J, Sakai K, et al. Mutational Activation of the Epidermal Growth Factor Receptor Down- Regulates Major Histocompatibility Complex Class I Expression via the Extracellular Signal-Regulated Kinase in Non–Small Cell Lung Cancer. Cancer Sci (2018) 1–9. doi: 10.1111/cas.13860
89. Garrido G, Rabasa A, Garrido C, Chao L, Garrido F, García-Lora ÁM, et al. Upregulation of HLA Class I Expression on Tumor Cells by the Anti-EGFR Antibody Nimotuzumab. Front Pharmacol (2017) 8:595. doi: 10.3389/fphar.2017.00595
90. Huang WC, Hung CM, Wei CT, Chen TM, Chien PH, Pan HL, et al. Interleukin-6 Expression Contributes to Lapatinib Resistance Through Maintenance of Stemness Property in HER2-positive Breast Cancer Cells. Oncotarget (2016) 7(38):62352–63. doi: 10.18632/oncotarget.11471
91. Husain H, Scur M, Murtuza A, Bui N, Woodward B, Kurzrock R. Strategies to Overcome Bypass Mechanisms Mediating Clinical Resistance to EGFR Tyrosine Kinase Inhibition in Lung Cancer. Mol Cancer Ther (2017) 16(2):265–72. doi: 10.1158/1535-7163.MCT-16-0105
92. Shostak K, Chariot A. EGFR and NF-kappaB: Partners in Cancer. Trends Mol Med (2015) 21(6):385–93. doi: 10.1016/j.molmed.2015.04.001
93. Azuma K, Ota K, Kawahara A, Hattori S, Iwama E, Harada T, et al. Association of PD-L1 Overexpression With Activating EGFR Mutations in Surgically Resected Nonsmall-Cell Lung Cancer. Ann Oncol (2014) 25(10):1935–40. doi: 10.1093/annonc/mdu242
94. Lastwika KJ, Wilson W 3rd, Li QK, Norris J, Xu H, Ghazarian SR, et al. Control of PD-L1 Expression by Oncogenic Activation of the AKT-mTOR Pathway in Non-Small Cell Lung Cancer. Cancer Res (2016) 76(2):227–38. doi: 10.1158/0008-5472.CAN-14-3362
95. Ota K, Azuma K, Kawahara A, Hattori S, Iwama E, Tanizaki J, et al. Induction of PD-L1 Expression by the EML4-ALK Oncoprotein and Downstream Signaling Pathways in Non-Small Cell Lung Cancer. Clin Cancer Res (2015) 21(17):4014–21. doi: 10.1158/1078-0432.CCR-15-0016
96. Zhang N, Zeng Y, Du W, Zhu J, Shen D, Liu Z, et al. Pd-L1 is Regulated by EGFR Through IL-6/JAK/STAT3 Signaling Pathway. Int J Oncol (2016) 49:1360–8. doi: 10.3892/ijo.2016.3632
97. Okita R, Maeda A, Shimizu K, Nojima Y, Saisho S, Nakata M. Pd-L1 Overexpression is Partially Regulated by EGFR/HER2 Signaling and Associated With Poor Prognosis in Patients With Non-Small-Cell Lung Cancer. Cancer Immunol Immunother (2017) 66(7):865–76. doi: 10.1007/s00262-017-1986-y
98. Besse B, Garrido P, Cortot AB, Johnson M, Murakami H, Gazzah A, et al. Efficacy and Safety of Necitumumab and Pembrolizumab Combination Therapy in Patients With Stage IV Non-Small Cell Lung Cancer. Lung Cancer (2020) 142:63–9. doi: 10.1016/j.lungcan.2020.02.003
99. Saavedra D, Crombet T. Cimavax-EGF: A New Therapeutic Vaccine for Advanced Non-Small Cell Lung Cancer Patients. Front Immunol (2017) 8:269. doi: 10.3389/fimmu.2017.00269
100. Dy G, Crombet T, Leon K, Mazzora Z, Hernandez D, Lage A, et al. Ep1. 04-23 Ongoing Phase II Trial of Anti-PD1 Therapy in Combination With CIMAvax-EGF in Patients With Advanced NSCLC or Squamous Cell Head and Neck Cancer. J Thorac Oncol (2019) 14: (10):S970. doi: 10.1016/j.jtho.2019.08.2126
101. Crombet T MJ, Mesa C, Evans R, Saavedra D, Lorenzo P, Mazorra Z, et al. Abstract CT130: Evidence for Synergistic Immune Responses in the First-in-Human (FIH) Combination of B Cell-Activating Immunotherapy (IO) with Anti-PD1 Immune Checkpoint Inhibitor nivolumab (N) as 2nd-Line Therapy in Patients (pts) with Advanced Non-Small Cell Lung Cancer (aNSCLC). Cancer Res AACR (2020). CT130. doi: 10.1158/1538-7445.AM2020-CT130
102. Vokes EE, Ready N, Felip E, Horn L, Burgio M, Antonia S, et al. Nivolumab Versus Docetaxel in Previously Treated Advanced Non-Small-Cell Lung Cancer (CheckMate 017 and CheckMate 057): 3-Year Update and Outcomes in Patients With Liver Metastases. Ann Oncol (2018) 29: (4):959–65. doi: 10.1093/annonc/mdy041
Keywords: CIMAvax-EGF, NSCLC, EGFR, immune checkpoint inhibitors, tyrosine kinase inhibitors
Citation: Crombet Ramos T, Santos Morales O, Dy GK, León Monzón K and Lage Dávila A (2021) The Position of EGF Deprivation in the Management of Advanced Non-Small Cell Lung Cancer . Front. Oncol. 11:639745. doi: 10.3389/fonc.2021.639745
Received: 09 December 2020; Accepted: 17 May 2021;
Published: 15 June 2021.
Edited by:
Benjamin Frey, University Hospital Erlangen, GermanyReviewed by:
Rafael Rosell, Catalan Institute of Oncology, SpainDennis O. Adeegbe, Moffitt Cancer Center, United States
Copyright © 2021 Crombet Ramos, Santos Morales, Dy, León Monzón and Lage Dávila. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tania Crombet Ramos, dGFuaWFjQGNpbS5zbGQuY3U=