 Xiaoping Lin
Xiaoping Lin Zizheng Xiao1,2
Zizheng Xiao1,2 Steven H. Liang
Steven H. Liang Huiqin Guo
Huiqin Guo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Oncol., 06 March 2020
Sec. Molecular and Cellular Oncology
Volume 10 - 2020 | https://doi.org/10.3389/fonc.2020.00317
This article is part of the Research TopicImpact of Cancer Plasticity on Drug Resistance and Treatment in Solid Tumors.View all 33 articles
Malignant cells support tumor proliferation and progression by adopting to metabolic changes. Tumor cells altered metabolism by increasing glucose uptake and fermentation of glucose to lactate, even in the aerobic state and the presence of functioning mitochondria. Glucose metabolism in tumor plasticity has attracted great interests by clinicians and scientists in the past decades. This review discusses the previous and emerging researches on the tumor plasticity altered by changing glucose metabolism in different cancer cells, including cancer stem cells (CSCs). In addition, we summarize the rising applications of glucose metabolism in tumor diagnosis and treatment. Our objective is to direct future investigation on this altered metabolic phenotype and its application in patient care.
The characteristics of malignant cells, including sustaining cell proliferation, escaping cell death, attaining immortality by inducing new blood vessel formation and promoting tumor cell invasion and metastasis, were summarized in the year 2000 (1). After one decade of conceptual advance, two emerging traits were added—altering energy metabolism and evading immune demolition (2). In recent years, increasing number of studies focus on the alteration of energy metabolism, that allows tumor cells to survive and spread even in challenging conditions. However, a paradigm shift has occurred adding to our knowledge of the function of glycolysis in glucose metabolism over the last decade (3). In this review, we attempt to provide a better understanding of glucose metabolism in tumor plasticity which may contribute to the design and outcome of novel diagnostics and treatment strategies.
Normally, glucose is processed by glycolysis to generate ATP and pyruvate. Then the ribose 5-phosphate and NADPH were produced through the pentose phosphate pathway (PPP), or enter into the tricarboxylic acid (TCA) cycle in mitochondrion. Glucose-derived citrate is converted to acetyl-CoA, oxaloacetate (OAA), or a-ketoglutarate (a-KG). Glutamine is deaminated to form glutamate, which is processed to produce a-KG for use in the TCA cycle.
The main pathway of glucose metabolism in cancer cells is aerobic glycolysis, termed Warburg effect (4). In cancer cells, glucose uptake and the production of lactate was dramatically increased, even in the presence of oxygen and fully functioning mitochondria (5). This classic type of metabolic change provides substrates required for cancer cell proliferation and division, which is involved in tumor growth, metastatic progression and long-term survival (5–8). It must be emphasized that both glycolysis and mitochondrial metabolism are crucial to cancer cells in the Warburg Effect (5).
Glucose metabolism in tumor is governed by both oncogenes and cancer-producing factors (6). Metabolic reprogramming of cancer cells is regulated by transcription factors that include c-Myc, p53 and hypoxia-inducible factor (HIF) 1α (9). The reprogramming is a complex interaction of various signaling pathways, such as Notch, Akt, phosphoinositide-3-kinase (PI3K), PTEN, mammalian target of rapamycin (mTOR), and AMP-activated protein kinase (AMPK) (10, 11).
c-Myc can stimulate glycolysis, glutaminolysis, and nucleotide synthesis (12). c-Myc mediated glucose metabolic reprogramming primarily on mitochondrial aerobic metabolism (13). Glycolysis can be promoted by c-Myc through direct induction of glycolytic-associated enzymes (14). Besides, mitochondrial biogenesis can be promoted by c-Myc with stable function and the number of mitochondria in tumor cells.
p53 is the main adverse regulator during tumor metabolic reprogramming (15). p53 inhibits glycolysis by inducing glycolysis and apoptosis regulator (TIGAR), inhibiting phosphoglycerate mutase (PGM) to upregulate expression of TP53, and repressing glucose transporter (GLUT)-1 and GLUT -4 (6, 16–18). Also, p53 can alter oxygen consumption and the synthesis of cytochrome c oxidase 2 (SCO2) protein, which is critical for regulating the cytochrome c oxidase(COX) complex (19). Moreover, p53 promotes mitochondrial glutaminase (GLS2) and limits glutaminolysis in response to oxidative stress or DNA damage (20).
HIF-1 is a heterodimeric protein that could alter various genes coded for enzymes involved in glucose metabolism. The phosphatidylinositol 3-kinase (PI3K) and ERK mitogen-activated protein kinase (MAPK) pathways affect HIF-1α protein synthesis. In glucose metabolism, glyceraldehyde-3-P-dehydrogenase (GAPDH), GLUT-1, hexokinase (including HK1 and HK2), autocrine motility factor/ (AMF/GPI), enolase 1(ENO1), plasminogen activator receptor (TPI), Pyruvate kinase(PKM), 6-phosphofructo-2-kinase/fructose-2,6-biphosphatase-3(PFKBF3, PFKL, PGK1), and LDHA can be transcriptionally activated by HIF-1 (21).
Tumor cells need to survive drastic changes in the microenvironment such as hypoxia, nutrient storage, and acidic pH (22). A huge number of cancer cells show remarkable plasticity in metabolic adaptation. The reprogrammed glucose metabolism allows cancer cells to satisfy high proliferation requests. In addition, it provides some survival and growth advantages, including high carbon source for anabolism, rapid ATP availability to supply the energy, abundant lactic acid to increase the redox status (NADPH) via the glycine–serine pathway (6–8). Lactic acid induces metabolic “dormancy” and is involved in EMT and tumor immune response by reducing pH in the tumor environment (5, 8, 23–25). To manage all the situations above, cancer cells must maintain a balance to deliver adequate energy with constrained resources and to meet the biosynthetic demands of proliferation. Though oxidative phosphorylation(OXPHOS) would be the best energy provider, the physiological reality is that both OXPHOS and glycolysis collaborate to produce ATP under the local oxygen concentration. Coordinate results are net increments in glucose utilization and lactic acid secretions. This process is known as the glycolytic switch, which is corresponding to uncoupling glycolysis from OXPHOS (26).
Cell proliferation requires expanded uptake of supplements, lifted flux through biosynthetic pathways, support of metabolic intermediates, and proceeded recovery of cofactors required to supply energy or reducing equivalents for reactions. Cancer cells preferred aerobic glycolysis for cell proliferation. In addition, aerobic glycolysis produces metabolic precursors that are essential for rapid cell proliferation (25). As proliferation is the key feature of cancer cells, aerobic glycolysis allows cancer cells to meet the requirements of generating enough ATP and biosynthetic precursors. The goal of aerobic glycolysis is to preserve high levels of glycolytic intermediates to maintain anabolic reactions in cells instead of generating lactate and ATP. Thus, it may explain why increased glucose metabolism happens in proliferating cancer cells (26).
The biosynthesis in proliferating cells requires building blocks for the synthesis of nucleotides, lipids, and non-essential amino acids—those that glycolytic intermediates can supply (27). The PPP can produce the reducing equivalents in the form of NADPH molecules and generates nucleotide and lipid precursors. The TCA cycle can generate acetyl-CoA and glutamine and drive them into the cytosol. As a result, the anabolic metabolism of amino acids and lipids is supplied by both glycolysis and the TCA cycle within mitochondria (27). NAD+ is an essential cofactor of nucleotide and amino acid biosynthesis. The maintenance of biosynthesis in proliferating cells demands the regeneration of NAD+. The conversion of pyruvate to lactate can partially produce NAD+ (28). Because cells use as much as 10% of their entire proteome and half of all of their metabolic genes to produce proteins involved in glycolysis, the cost of using Warburg Effect in aerobic glycolysis as a tradeoff to promote biosynthesis is vast (29). Mitochondrial functions occur concomitantly with the aerobic glycolysis and limiting mitochondrial activity may not occur during the Warburg Effect (5). Under energy stress conditions, the apparent shift from glycolysis to OXPHOS by mitochondrial elongation contribute to tumor survival. Remodeling of mitochondrial morphology is a remarkable protection of tumor cells from stress (30).
EMT is a process that involves a high level of cellular plasticity. EMT is often activated during cancer cell invasion, systemic dissemination, and metastasis (31, 32). EMT is an important step preceding to invasion and metastasis in tumor cells. Epithelial cells lose the junctions among cells and their polarized organization during EMT. They change cytoskeletal organization, transform the shape, and acquire mesenchymal characteristics, such as fibroblast-like cell morphology and increased capability of invasion and migration (32, 33).
The plasticity of glucose metabolism is important in EMT (34). The genes and biochemical mechanisms impact glucose metabolism during EMT of cancer cells. Crosstalk network has been explored between EMT and cancer metabolism (35). PI3K-AKT-mTOR, EGFR-RAS-MAPKs, and JAK2-STAT3 signaling pathways can mediate EMT (36). HIF1α, Myc and FOXM1 regulate both metabolism and EMT (37). LKB1 / AMPK (Liver kinase B1/AMP-activated protein kinase) downregulates SNAIL and ZEB1and inhibits the invasion and migration of tumor cells, by regulating FOXO3, TGF- β, NF-κB, AKT, and mTOR signaling pathways (34).
Glucose transporters, especially GLUT-1 and GLUT-3, promote tumor progression by increasing glucose influx and activating downstream molecular pathways (38). GLUT-1 increases matrix metalloproteinase 2 (MMP-2) in vitro and in vivo, which contributes to EMT and cellular invasiveness (34, 39). GLUT-3 gene could be activated by ZEB1, which is an EMT marker (34). HK2 is a well-known hypoxia-inducible gene that can induce EMT (34). PFK increases glycolytic flux and EMT by maintaining this glycolytic phenotype in cancer cells in vitro. Pyruvate kinase M2 (PKM2) can prompt EMT both by metabolic and non-metabolic mechanisms (40). PKM2 increases glucose uptake and lactate production to support cell survival and invasion (41).
Besides the enzymes involved glucose metabolism, altered mitochondrial function also contributes to EMT induction (34). Tumor cell migration and metastasis was stimulated by abnormal TCA cycling coupled with mitochondrial superoxide production (42).
Cancer consists of mainly stem cells (CSCs) and non-CSCs (2). CSCs have the potentials of self-renew and tumor initiation (43, 44). CSCs adapt to metabolic plasticity, which is determined by the factors present in the tumor microenvironment (TME). Metabolic plasticity allows these cancer stem cells to switch between OXPHOS and glycolysis (45). Only complete oxidation through the TCA cycle cannot supply enough anabolic precursors such as pyruvate and glutamine. CSCs prefer to rely on glycolysis and the PPP and devolve mitochondrial infrastructure and function. This predominantly glycolytic metabolism offers sufficient energy to support the basic needs of CSCs. The maturation of metabolic network matches the increasing energy demands of specialized progeny cells. The oxidative metabolism infrastructure contains mitochondrial biogenesis and maturation, and networks of the TCA cycle and electron transport chain. A concurrent rise in mitochondrial ROS may prime CSCs for lineage differentiation (46). The main difference between cancer cells and CSCs is the metabolic shift and mitochondrial resetting. CSCs display the metabolic change and mitochondrial resetting into precise bioenergetic states and lose the unique metabolic phenotypes after differentiation. Compared with differentiated neoplastic cells, CSCs exhibit a more prominent Warburg effect. Aerobic glycolysis may produce enough glycolytic intermediates into the PPP to supply molecules that are necessary for anabolic metabolism and growth of CSCs (47). In CSCs, the oxidative metabolism and mitochondrial structure are altered to commit glycolysis (48). Aerobic glycolysis is one of the important aspects in maintaining CSCs and inducing their differentiation. Specifically, aerobic glycolysis is critical in preserving the stemness of CSCs, while switching to oxidative metabolism is the characteristic of stem cell differentiation. Besides, aerobic glycolysis is essential to the properties of CSCs (46). Multiple regulatory factors including metabolic enzymes promoted the metabolic plasticity of stem cells in breast cancers. The metabolism-regulating genes and epigenetic factors that regulate glucose metabolism might also regulate the expression of EMT (49). An enhanced Warburg effect was observed in metastatic prostate cancers (44).
Moreover, metabolic flexibility diverge the fates CSCs, which include dormancy to minimize stress damage, proliferation and self-renewal to preserve progenitor pools, and pedigree specification for tissue regeneration (48). Depending on the metabolic characteristics of the tumor cells of origin, isogenic glioma stem cells (GSCs) exhibits heterogeneity in metabolic characteristics. They can be divided into mitochondrial and glycolytic phenotypes. Cells of the mitochondrial type consume more oxygen and maintain a higher ATP content; those of the glycolytic type consume more glucose and produce more lactate. Both metabolic phenotypes are independent and stable. They can coexist within a given tumor. The environmental factors further influence the metabolic preferences of these cells. For example, CSCs that rely on OXPHOS can switch to aerobic glycolysis in response to metabolic stress (50).
In addition to the inherent alterations in the tumor cells, the metabolic competition and cooperation among the TME components support tumor proliferation, progression, and therapeutic resistance (9). TME consist of different types of cells, that include cancer associated fibroblasts (CAFs), non-cancer cell stroma, immune cells, and endothelial cells (51). The TME forms a pro-tumorigenic cocoon around the tumor cells. Intrinsic traits (e.g., genetic programs in cancer cells) and extrinsic factors (e.g., nutrient availability, oxygen tension, pH) contribute to the deregulated metabolism in TME. TME enforces metabolic plasticity to adapt to hypoxic and acidic environment, nutrient deprivation and competition, oxidative stress, and immune surveillance (52). Reprogramming of the metabolism occurs in tumor and non-tumor cells. The interactions and competitions in TME components guarantee the steady supply of nutrients and molecules for tumor growth even under hypoxic conditions. Metabolic reprogramming also affects TME. Hypoxia inhibits this process by upregulating PDK1 and LDHA (53, 54). When HIF1α is activated in CAFs, the activity of mitochondria drops and lactate production increases. This is consistent with a glycolytic phenotype. It leads to slow down metabolism in the microenvironment (55). Lactate accumulation resulted from continuous activation of glycolytic and LDHA enzymes leads to a low-pH microenvironment during tumor progression. Nutrient deficiency is another microenvironment stress that cancer cell often encounters. Numerous studies have shown that reprogramming of glucose metabolism upon nutrient starvation in tumor cells occurs in order to use energy to support their growth (56–61).
The reverse Warburg Effect was proposed in the last decade (62). The energy-rich metabolites of aerobic glycolysis, such as lactate and pyruvate, are generated by cancer associated fibroblasts and taken up and used in the TCA cycle in mitochondria of epithelial cancer cells. Thus, efficient energy production such as ATP generation, which leads to increase cell proliferation and reduce cell death (62). The reverse Warburg effect can benefit tumor cells by cooperative utilization of oxygen between stromal cells and tumor cells (55). Cancer cells induce stromal cells to undergo “aerobic glycolysis.” Their products are returned to the cancer cells to be used for mitochondrial OXPHOS (63). The metabolic heterogeneity in TME allows cancer and stromal cells to exchange metabolites between them to maintain maximal cellular growth (18).
The immune system plays an important role in TME. The immune cells in the TME can detect and eliminate the abnormal cells or tumor cells and protect the body from damage caused by tumor cells (64). Tumor cells activate immune cells, and the activated innate or adaptive immune cells can maintain homeostasis (9, 65). The immune system affects cancer survival and progression (23, 66). Tumor cells develop different mechanisms to escape the immune response. They include strategies at the genetic, epigenetic and metabolic levels. It implements to resist immune recognition and decrease apoptosis (67).
There is a complex interaction between malignant cells and immune cells in the tumor stroma (66). Metabolism regulates tumor cells to escape immune surveillance and to coexist with stroma cells. Tumor and other different types of cells in the TME compete for nutrient. Inflammation induced by oncogene in the tumors promotes adaptive metabolic changes in the surrounding non-tumor cells to secrete metabolites. Tumors use these metabolites as alternative nutrient sources to meet their increasing demands for anabolic function (68).
Metabolism is essential to lymphocyte for its development, function and inducing tolerance (69). T cells prefer glycolysis upon activation, though they had lower glycolytic flux when resting. Activated by TCR- and CD28-mediated co-stimulation, T cells switch to a rapid increase in glucose uptake and glycolysis (69–71), as well as glutaminolysis (69, 72, 73). In contrast, the activation of T cells and dendritic cells can be inhabited by lactate accumulation (74, 75). Lactate prevents cytokine release and monocyte migration, while promotes the formation of tumor-associated macrophage 2 (TAM2) phenotype. It leads to upregulate the expression of arginase 1, promote immune escape and tumor progression (25, 76–78). Lactate reduces the production of IFN-γ from T cells and NK cells, and decreases the level of nuclear factor of activated T cells (NFAT), which also contributes to immune escape and tumor progression (79, 80). As antigen presenting cells and a source of cytokines, B lymphocytes also have a critical role in antitumor immunity (81, 82). B cells upon activation use both glycolysis and OXPHOS, which is different from T cells. However, the deletion of GLUT-1 or inhibition of glycolysis in B cells suppresses antibody production in vivo (69, 70).
Attempts to target the glucose metabolism, especially on Warburg effect, for cancer diagnosis and therapy emerges in the past decades and is still in developing.
Many different types of human tumors dramatically enhanced uptake and use of glucose. Since 1976, positron emission tomography (PET) with a radiolabeled analog of glucose (18F-fluorodeoxyglucose, FDG) was applied to non-invasively visualize glucose uptake in human body. This tracer is the most impressively clinical utility of the Warburg effect (2, 6). Increased FDG implies high glucose uptake which is an indication of the glycolytic switch. It provides information about the pathologic differentiation and precise stageing of tumors, predicts treatment response and gives an indication of overall prognosis (83). The positron-emitting radionuclide fluorine-18 replaces the normal hydroxyl group at the C-2 position in the glucose molecule. After injection into the body, the tracer is transported into cells by glucose transporters, especially GLUT-1 and GLUT-3, followed by phosphorylation with the hexokinase, especially HK2, to produce 18F-FDG-6-phosphate (18F-FDG-6-p). 18F-FDG-6-p cannot be released from the cell and is trapped in the cytoplasm. Because of the lack of the 2'hydroxyl group, 18F-FDG-6-p cannot further proceed to glycolytic pathway (84). PET scanner detects the radioactive decay of 18F-FDG-6-p and form the body images of the distribution of 18F-FDG. Thus, the presence of living malignance can be identified by the accumulated amounts of 18F-FDG-6-p (84, 85). The sites and the semi-quantitative analysis of high glucose uptake (e.g., standard uptake value, SUV) in the whole body can be identified. In the vast majority of malignance, glucose is trapped in cancer cells more than normal tissues with the exception of the brain and brown fat. It relates to the metabolic characteristics at the tumor site (42). Owing to the limitation of spatial resolution and some particular pathology subtypes(e.g., signet ring cell carcinoma, well-differentiated cancer), the sensitivity and specificity varied across different applications using18F-FDG–PET (26, 85).
PET imaging tracers are able to detect the PKM2, such as N,N-diarylsulfonamide (DASA) compounds bind to PKM2. 11C-labeled analog of DASA-23 was applied to the orthotopic U87 and GBM39 patient-derived tumors in preclinical models of glioblastoma multiforme and to monitor the response of the PKM2 activator TEPP-46 in GBM39 tumors (86).
An analog of glutamine, 4-18F-(2S,4R)-fluoroglutamine (18F-FGln), is taken up by cancer cells in vitro and its specific uptake can be detected on PET imaging in mouse xenograft model in vivo. Thus, the glutamine metabolism in gliomas and its uptake can be evaluated (87). Other investigational PET agent, such as 5-11C-(2S)-glutamine (87, 88), was also exploited for its ability to take up and retain glutamine in some tumors (87).
As another device in molecular imaging, a few agents have been developed to detect the glucose metabolism in magnetic resonance (MR). The hyperpolarized agents can form the better imaging for remarkable enhancement compared to conventional MR imaging. Magnetic resonance spectroscopy(MRS) can image the conversion of 13C-labeled pyruvate to lactate in patients (83). It is possible to identify malignance and monitor treatment response by evaluating the distribution of 13C-pyruvate and the altered 13C -lactate/13C -pyruvate in preclinical MRS study in prostate cancer and glioma (83, 89). Some other targetable processes in glucose metabolism, such as the detection of 2HG, can also be used for new imaging technology (90, 91).
To date, various agents involved in glucose metabolism are actively investigated as novel targets with therapeutic potential (Table 1). It helps to overcome drug resistance or increase the efficacy of current combination therapy (88, 109). Compared to diagnosis, targeting glucose metabolism in treatment seems faint due to their efficacy or safety concern. Several drugs with efficacy confirmed and multi-targets, as well as some old non-chemotherapeutic drugs with new aspects of inhabiting tumor glucose metabolism will be discussed below.
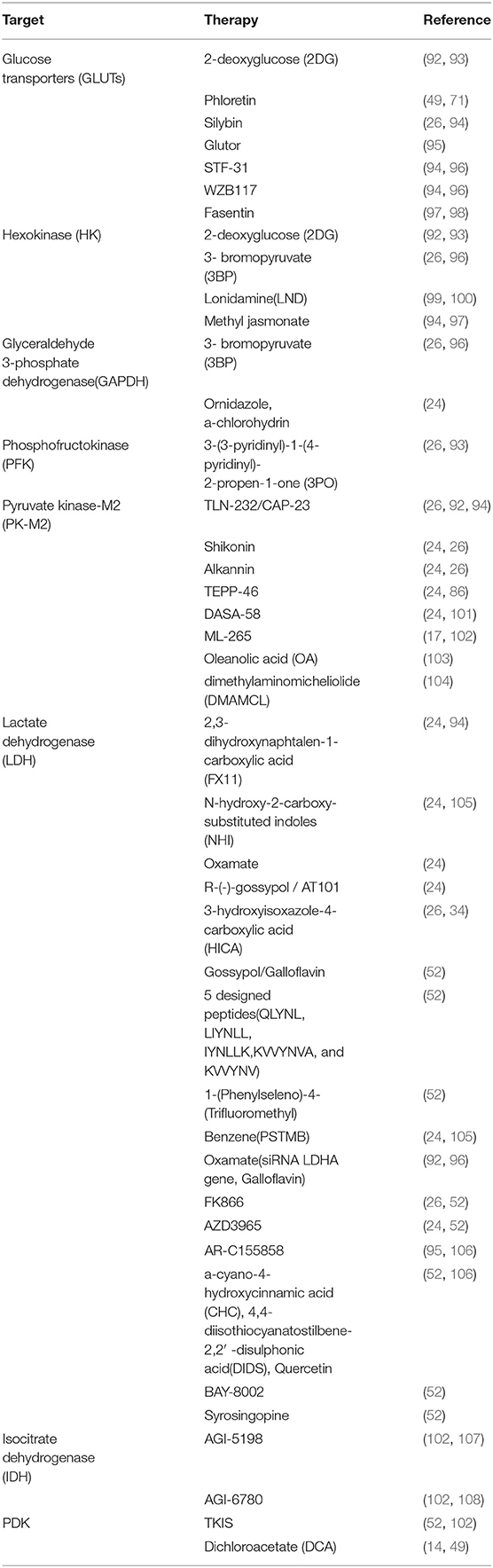
Table 1. Metabolic modulators arising from the metabolic theory of cancer.
GLUTs control the influx of glucose, especially GLUT-1. Several GLUT-1 inhibitory agents, including WZB117 and STF-31 have been tested (94, 105). STF-31 was effective in decreasing glucose uptake, inducing cell apoptosis and inhibiting tumor progression. However, STF-31 has a narrow therapeutic potential due to its molecular restriction (110, 111). WZB117 can effectively inhibit glucose uptake, cell proliferation, and tumor progression both in vivo and in vitro. However, its efficacy remains in doubt (105). A glucose-conjugated LDH inhibitor, glucose-conjugated methyl ester (NHI-Glc-2), is a promising compound. It is a weaker inhibitor than the N-OH methyl ester (NHI-2) on the isolated enzyme. It can increase the glucose uptake by exploiting the GLUT-1 overexpression, reduce lactate production and decrease proliferation of cancer cells (105).
Currently, inhibition of lactate transport is being tested as an alternative approach. But LDHA inhibitors had some limitations, such as high toxicity, low drug exposure or a lack of LDHA dependence in human tumor inhibitors (112). Nevertheless, an inhibitor of human LDH isoforms, Galloflavin is a natural phenol derivative and a product of gallic acid oxidation (105, 113). The analogs of Gossypol, a natural component extracted from the cotton seeds has been screened for small molecular inhibitors specific for LDHA. 3-dihydroxy-6-methyl-7-(phenylmethyl)-4-propylnaphthalene-1-carboxylic acid (FX11) was proved to effectively inhibit proliferation of cancer cells in vitro and in vivo by enhancing the levels of oxidative stress. Another isoform-specific inhibitors of LDHA, N-hydroxyindole-based compounds, can compete with its substrate pyruvate and the cofactor, NADH (92, 97).
The reversal reprogramming in IDH mutant tumors seems more successful (114, 115). The mechanism of 2HG-mediated transformation may vary in different kinds of tumors. It may inhibit the dual metabolic flux of glycolysis and oxidative PPP (88, 116). In preclinical studies, the inhibition of mutant IDH has been shown to dramatically decrease the generation of 2HG and cause cancer cells to differentiate into normal cells (107, 108). An inhibitor of mutant IDH2, AG-221, has been put forward in early phase clinical trials (113).
New compounds also target dual inhibition, such as the inhibition of metabolic plasticity and metabolic rescue in cancer cells. Compounds targeting glucose, glutamine and lactate metabolism have been found to exert anticancer effects by inhibiting growth of tumor-associated endothelial cells (24). A new glucose uptake inhibitor, Glutor, targets GLUTs (GLUT-1, -2, and -3), diminishes glycolytic flux and selectively suppresses growth of a variety of cancer cells. Glutor combined with glutaminase inhibitor CB-839 synergistically inhibits the proliferation of colon cancer cells (95).
Compared to conventional cytotoxic therapy, modulation of particular targets with altered glycolytic metabolism would reduce treatment toxicity. A number of studies show that treatment combined with vitamin C leads to interfering with glycolysis and the TCA cycle and inhibits ATP and NADPH production. It can kill cancer cells by increasing oxidative stress and further inhibition in cancer cell survival and invasion. (117–122). Preclinical studies have shown that vitamin C at the concentration below 5 mM could prevent proliferation of cancer cells (123–125). Because of the anti-oxidant capacity, vitamin C can prevent the growth of circulating tumor cells (CTCs). Vitamin C also reduces pyruvate and glutathione (GSH). Extracellular matrix remodeling and cancer cell motility were reduced by vitamin C by boosting ROS levels. It can increase expression of E-cadherin, decrease expression of Snail and inhibit matrix metalloproteinases (MMPs) (105, 126, 127).
Metformin is a common drug for diabetes. The metformin/hypoglycemia combination has synergistic anti-neoplastic effects to decrease the pro-survival protein MCL-1 and cause cell death (128). Metformin combined with ritonavir targets OXPHOS, in particular, GLUT-4. It can effectively inhibit the AKT and mTORC1 phosphorylation and pro-survival mitochondrial complex I (MCL1) (116, 129).
Aspirin is a common pain reliever and anti-inflammatory drug. It also inhibits MCL1 activity (130). In the past two decades, its anti-neoplastic action has been investigated against different malignancies and tumor cell lines. Dalton's lymphoma (T-cell lymphoma) cells obtained from tumor-bearing mice treated by aspirin showed a change of expression of pH regulators MCT-1 and V-ATPase, as well as change in cell survival regulatory molecules including GLUT-1 (131). Aspirin can also modulate glucose uptake by depressing GLUT-1 through targeting NF-κB or NF κB/HIF1α signaling to inhibit proliferation (132).
Despite the extensive study on cancer metabolism with interesting results accumulated in the last decades, questions are still arising. The key process of balance among glycolysis, TCA and other pathways of the glucose metabolism in tumor remains unclear, as it is the essential mechanism of Warburg effect. In addition, it should be considered to develop more tumor-specific tracers and drugs based on the metabolic switch in tumor cells, cancer stem cells or the interaction with immune system. The ideal drugs should only applied in tumor by blocking specific pathway(s) for its metabolic plasticity but not in normal tissues. Despite the emerging of metabolic enzymes or transporters inhibitors, the efficiency of targeting tumor glucose metabolism is being challenged. To explore the metabolic plasticity in cancer under intrinsic and extrinsic influences, tumorous glucose metabolism should be addressed. Nevertheless, with technological advances, it is expected that we will uncover many other unknown aspects of glucose metabolism in cancer and use them to benefit patient care.
XL and HG conceived and designed the study. XL wrote the first draft. ZX, TC, and SL wrote some sections of the article. HG edited the article. All authors read and approved the final version of submission.
This work was supported by the Fund of Natural Science Foundation of Guangdong Province, China, No. 2018A030310239.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Hanahan D, Weinberg RA. The hallmarks of cancer. Cell. (2000) 100:57–70. doi: 10.1016/S0092-8674(00)81683-9
2. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. (2011) 144:646–74. doi: 10.1016/j.cell.2011.02.013
3. Semenza GL. Hypoxia-inducible factors: coupling glucose metabolism and redox regulation with induction of the breast cancer stem cell phenotype. EMBO J. (2017) 36:252–9. doi: 10.15252/embj.201695204
4. Warburg O. On the origin of cancer cells. Science. (1956) 123:309–14. doi: 10.1126/science.123.3191.309
5. Liberti MV, Locasale JW. The Warburg effect: how does it benefit cancer cells? Trends Biochem Sci. (2016) 41:211–8. doi: 10.1016/j.tibs.2015.12.001
6. Levine AJ, Puzio-Kuter AM. The control of the metabolic switch in cancers by oncogenes and tumor suppressor genes. Science. (2010) 330:1340–4. doi: 10.1126/science.1193494
7. Locasale JW. Serine, glycine and one-carbon units: cancer metabolism in full circle. Nat Rev Cancer. (2013) 13:572–83. doi: 10.1038/nrc3557
8. Zdralevic M, Vucetic M, Daher B, Marchiq I, Parks SK, Pouyssegur J. Disrupting the 'Warburg effect' re-routes cancer cells to OXPHOS offering a vulnerability point via 'ferroptosis'-induced cell death. Adv Biol Regul. (2018) 68:55–63. doi: 10.1016/j.jbior.2017.12.002
9. Gupta S, Roy A, Dwarakanath BS. Metabolic cooperation and competition in the tumor microenvironment: implications for therapy. Front Oncol. (2017) 7:68. doi: 10.3389/fonc.2017.00068
10. Masui K, Tanaka K, Ikegami S, Villa GR, Yang H, Yong WH, et al. Glucose-dependent acetylation of Rictor promotes targeted cancer therapy resistance. Proc Natl Acad Sci USA. (2015) 112:9406–11. doi: 10.1073/pnas.1511759112
11. Koczula KM, Ludwig C, Hayden R, Cronin L, Pratt G, Parry H, et al. Metabolic plasticity in CLL: adaptation to the hypoxic niche. Leukemia. (2016) 30:65–73. doi: 10.1038/leu.2015.187
12. Maher EA, Marin-Valencia I, Bachoo RM, Mashimo T, Raisanen J, Hatanpaa KJ, et al. Metabolism of [U-13 C]glucose in human brain tumors in vivo. NMR Biomed. (2012) 25:1234–44. doi: 10.1002/nbm.2794
13. Murphy TA, Dang CV, Young JD. Isotopically nonstationary 13C flux analysis of Myc-induced metabolic reprogramming in B-cells. Metab Eng. (2013) 15:206–17. doi: 10.1016/j.ymben.2012.07.008
14. Kim JW, Gao P, Liu YC, Semenza GL, Dang CV. Hypoxia-inducible factor 1 and dysregulated c-Myc cooperatively induce vascular endothelial growth factor and metabolic switches hexokinase 2 and pyruvate dehydrogenase kinase 1. Mol Cell Biol. (2007) 27:7381–93. doi: 10.1128/MCB.00440-07
15. Shi L, Jackstadt R, Siemens H, Li H, Kirchner T, Hermeking H. p53-induced miR-15a/16-1 and AP4 form a double-negative feedback loop to regulate epithelial-mesenchymal transition and metastasis in colorectal cancer. Cancer Res. (2014) 74:532–42. doi: 10.1158/0008-5472.CAN-13-2203
16. Yang X, Ye H, He M, Zhou X, Sun N, Guo W, et al. LncRNA PDIA3P interacts with c-Myc to regulate cell proliferation via induction of pentose phosphate pathway in multiple myeloma. Biochem Biophys Res Commun. (2018) 498:207–213. doi: 10.1016/j.bbrc.2018.02.211
17. Mendez-Lucas A, Li X, Hu J, Che L, Song X, Jia J, et al. Glucose catabolism in liver tumors induced by c-MYC can be sustained by various PKM1/PKM2 ratios and pyruvate kinase activities. Cancer Res. (2017) 77:4355–4364. doi: 10.1158/0008-5472.CAN-17-0498
18. Wilde L, Roche M, Domingo-Vidal M, Tanson K, Philp N, Curry J, et al. Metabolic coupling and the Reverse Warburg Effect in cancer: Implications for novel biomarker and anticancer agent development. Semin Oncol. (2017) 44:198–203. doi: 10.1053/j.seminoncol.2017.10.004
19. Kondoh H, Lleonart ME, Gil J, Wang J, Degan P, Peters G, et al. Glycolytic enzymes can modulate cellular life span. Cancer Res. (2005) 65:177–85.
20. Wegiel B, Vuerich M, Daneshmandi S, Seth P. Metabolic switch in the tumor microenvironment determines immune responses to anti-cancer therapy. Front Oncol. (2018) 8:284. doi: 10.3389/fonc.2018.00284
21. Semenza GL. Targeting HIF-1 for cancer therapy. Nat Rev Cancer. (2003) 3:721–32. doi: 10.1038/nrc1187
22. Oizel K, Chauvin C, Oliver L, Gratas C, Geraldo F, Jarry U, et al. Efficient mitochondrial glutamine targeting prevails over glioblastoma metabolic plasticity. Clin Cancer Res. (2017) 23:6292–304. doi: 10.1158/1078-0432.CCR-16-3102
23. Damgaci S, Ibrahim-Hashim A, Enriquez-Navas PM, Pilon-Thomas S, Guvenis A, Gillies RJ. Hypoxia and acidosis: immune suppressors and therapeutic targets. Immunology. (2018) 154:354–62. doi: 10.1111/imm.12917
24. Polet F, Feron O. Endothelial cell metabolism and tumour angiogenesis: glucose and glutamine as essential fuels and lactate as the driving force. J Intern Med. (2013) 273:156–65. doi: 10.1111/joim.12016
25. Colegio OR, Chu NQ, Szabo AL, Chu T, Rhebergen AM, Jairam V, et al. Functional polarization of tumour-associated macrophages by tumour-derived lactic acid. Nature. (2014) 513:559–63. doi: 10.1038/nature13490
26. Porporato PE, Dhup S, Dadhich RK, Copetti T, Sonveaux P. Anticancer targets in the glycolytic metabolism of tumors: a comprehensive review. Front Pharmacol. (2011) 2:49. doi: 10.3389/fphar.2011.00049
27. Lunt SY, Vander Heiden MG. Aerobic glycolysis: meeting the metabolic requirements of cell proliferation. Annu Rev Cell Dev Biol. (2011) 27:441–64. doi: 10.1146/annurev-cellbio-092910-154237
28. Harris RA, Tindale L, Cumming RC. Age-dependent metabolic dysregulation in cancer and Alzheimer's disease. Biogerontology. (2014) 15:559–77. doi: 10.1007/s10522-014-9534-z
29. Madhukar NS, Warmoes MO, Locasale JW. Organization of enzyme concentration across the metabolic network in cancer cells. PLoS ONE. (2015) 10:e0117131. doi: 10.1371/journal.pone.0117131
30. Li J, Huang Q, Long X, Guo X, Sun X, Jin X, et al. Mitochondrial elongation-mediated glucose metabolism reprogramming is essential for tumour cell survival during energy stress. Oncogene. (2017) 36:4901–12. doi: 10.1038/onc.2017.98
31. Tiwari N, Gheldof A, Tatari M, Christofori G. EMT as the ultimate survival mechanism of cancer cells. Semin Cancer Biol. (2012) 22:194–207. doi: 10.1016/j.semcancer.2012.02.013
32. Mani SA, Guo W, Liao MJ, Eaton EN, Ayyanan A, Zhou AY, et al. The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell. (2008) 133:704–15. doi: 10.1016/j.cell.2008.03.027
33. Payen VL, Porporato PE, Baselet B, Sonveaux P. Metabolic changes associated with tumor metastasis, part 1: tumor pH, glycolysis and the pentose phosphate pathway. Cell Mol Life Sci. (2016) 73:1333–48. doi: 10.1007/s00018-015-2098-5
34. Kang H, Kim H, Lee S, Youn H, Youn B. Role of metabolic reprogramming in Epithelial? Mesenchymal Transition (EMT). Int J Mol Sci. (2019) 20:E2042. doi: 10.3390/ijms20082042
35. Thiery JP, Sleeman JP. Complex networks orchestrate epithelial-mesenchymal transitions. Nat Rev Mol Cell Biol. (2006) 7:131–42. doi: 10.1038/nrm1835
36. Xu W, Yang Z, Lu N. A new role for the PI3K/Akt signaling pathway in the epithelial-mesenchymal transition. Cell Adh Migr. (2015) 9:317–24. doi: 10.1080/19336918.2015.1016686
37. Huang R, Zong X. Aberrant cancer metabolism in epithelial-mesenchymal transition and cancer metastasis: Mechanisms in cancer progression. Crit Rev Oncol Hematol. (2017) 115:13–22. doi: 10.1016/j.critrevonc.2017.04.005
38. Macheda ML, Rogers S, Best JD. Molecular and cellular regulation of glucose transporter (GLUT) proteins in cancer. J Cell Physiol. (2005) 202:654–62. doi: 10.1002/jcp.20166
39. Phillips RM, Lam C, Wang H, Tran PT. Bittersweet tumor development and progression: emerging roles of epithelial plasticity glycosylations. Adv Cancer Res. (2019) 142:23–62. doi: 10.1016/bs.acr.2019.01.002
40. Hamabe A, Konno M, Tanuma N, Shima H, Tsunekuni K, Kawamoto K, et al. Role of pyruvate kinase M2 in transcriptional regulation leading to epithelial-mesenchymal transition. Proc Natl Acad Sci USA. (2014) 111:15526–31. doi: 10.1073/pnas.1407717111
41. Li C, Zhao Z, Zhou Z, Liu R. PKM2 promotes cell survival and invasion under metabolic stress by enhancing warburg effect in pancreatic ductal adenocarcinoma. Dig Dis Sci. (2016) 61:767–73. doi: 10.1007/s10620-015-3931-2
42. Porporato PE, Payen VL, Perez-Escuredo J, De Saedeleer CJ, Danhier P, Copetti T, et al. A mitochondrial switch promotes tumor metastasis. Cell Rep. (2014) 8:754–66. doi: 10.1016/j.celrep.2014.06.043
43. Park CY, Tseng D, Weissman IL. Cancer stem cell-directed therapies: recent data from the laboratory and clinic. Mol Ther. (2009) 17:219–30. doi: 10.1038/mt.2008.254
44. Aguilar E, Marin de Mas I, Zodda E, Marin S, Morrish F, Selivanov V, et al. Metabolic reprogramming and dependencies associated with epithelial cancer stem cells independent of the epithelial-mesenchymal transition program. Stem Cells. (2016) 34:1163–76. doi: 10.1002/stem.2286
45. Sancho P, Barneda D, Heeschen C. Hallmarks of cancer stem cell metabolism. Br J Cancer. (2016) 114:1305–12. doi: 10.1038/bjc.2016.152
46. Jang H, Yang J, Lee E, Cheong JH. Metabolism in embryonic and cancer stemness. Arch Pharm Res. (2015) 38:381–8. doi: 10.1007/s12272-015-0558-y
47. Shen YA, Wang CY, Hsieh YT, Chen YJ, Wei YH. Metabolic reprogramming orchestrates cancer stem cell properties in nasopharyngeal carcinoma. Cell Cycle. (2015) 14:86–98. doi: 10.4161/15384101.2014.974419
48. Folmes CD, Dzeja PP, Nelson TJ, Terzic A. Metabolic plasticity in stem cell homeostasis and differentiation. Cell Stem Cell. (2012) 11:596–606. doi: 10.1016/j.stem.2012.10.002
49. Walsh HR, Cruickshank BM, Brown JM, Marcato P. The flick of a switch: conferring survival advantage to breast cancer stem cells through metabolic plasticity. Front Oncol. (2019) 9:753. doi: 10.3389/fonc.2019.00753
50. Shibao S, Minami N, Koike N, Fukui N, Yoshida K, Saya H, et al. Metabolic heterogeneity and plasticity of glioma stem cells in a mouse glioblastoma model. Neuro Oncol. (2018) 20:343–54. doi: 10.1093/neuonc/nox170
51. Lyssiotis CA, Kimmelman AC. Metabolic interactions in the tumor microenvironment. Trends Cell Biol. (2017) 27:863–75. doi: 10.1016/j.tcb.2017.06.003
52. de la Cruz-López KG, Castro-Muñoz LJ, Reyes-Hernández DO, García-Carranca A, Manzo-Merino J. Lactate in the regulation of tumor microenvironment and therapeutic approaches. Front Oncol. (2019) 9:1143. doi: 10.3389/fonc.2019.01143
53. Kim JW, Tchernyshyov I, Semenza GL, Dang CV. HIF-1-mediated expression of pyruvate dehydrogenase kinase: a metabolic switch required for cellular adaptation to hypoxia. Cell Metab. (2006) 3:177–85. doi: 10.1016/j.cmet.2006.02.002
54. Semenza GL, Roth PH, Fang HM, Wang GL. Transcriptional regulation of genes encoding glycolytic enzymes by hypoxia-inducible factor 1. J Biol Chem. (1994) 269:23757–63.
55. Shan M, Dai D, Vudem A, Varner JD, Stroock AD. Multi-scale computational study of the Warburg effect, reverse Warburg effect and glutamine addiction in solid tumors. PLoS Comput Biol. (2018) 14:e1006584. doi: 10.1371/journal.pcbi.1006584
56. Huang Li T, Wang L, Zhang L, Yan R, Li K, et al. Hepatocellular carcinoma redirects to ketolysis for progression under nutrition deprivation stress. Cell Res. (2016) 26:1112–30. doi: 10.1038/cr.2016.109
57. Sun L, Song L, Wan Q, Wu G, Li X, Wang Y, et al. cMyc-mediated activation of serine biosynthesis pathway is critical for cancer progression under nutrient deprivation conditions. Cell Res. (2015) 25:429–44. doi: 10.1038/cr.2015.33
58. Ma L, Tao Y, Duran A, Llado V, Galvez A, Barger JF, et al. Control of nutrient stress-induced metabolic reprogramming by PKCzeta in tumorigenesis. Cell. (2013) 152:599–611. doi: 10.1016/j.cell.2012.12.028
59. Daye D, Wellen KE. Metabolic reprogramming in cancer: unraveling the role of glutamine in tumorigenesis. Semin Cell Dev Biol. (2012) 23:362–9. doi: 10.1016/j.semcdb.2012.02.002
60. Boroughs LK, DeBerardinis RJ. Metabolic pathways promoting cancer cell survival and growth. Nat Cell Biol. (2015) 17:351–9. doi: 10.1038/ncb3124
61. Valencia T, Kim JY, Abu-Baker S, Moscat-Pardos J, Ahn CS, Reina-Campos M, et al. Metabolic reprogramming of stromal fibroblasts through p62-mTORC1 signaling promotes inflammation and tumorigenesis. Cancer Cell. (2014) 26:121–35. doi: 10.1016/j.ccr.2014.05.004
62. Pavlides S, Whitaker-Menezes D, Castello-Cros R, Flomenberg N, Witkiewicz AK, Frank PG, et al. The reverse Warburg effect: aerobic glycolysis in cancer associated fibroblasts and the tumor stroma. Cell Cycle. (2009) 8:3984–4001. doi: 10.4161/cc.8.23.10238
63. Xu XD, Shao SX, Jiang HP, Cao YW, Wang YH, Yang XC, et al. Warburg effect or reverse Warburg effect? A review of cancer metabolism. Oncol Res Treat. (2015) 38:117–22. doi: 10.1159/000375435
64. Davies M. New modalities of cancer treatment for NSCLC: focus on immunotherapy. Cancer Manag Res. (2014) 6:63–75. doi: 10.2147/CMAR.S57550
65. Gonzalez H, Hagerling C, Werb Z. Roles of the immune system in cancer: from tumor initiation to metastatic progression. Genes Dev. (2018) 32:1267–84. doi: 10.1101/gad.314617.118
66. Bremnes RM, Al-Shibli K, Donnem T, Sirera R, Al-Saad S, Andersen S, et al. The role of tumor-infiltrating immune cells and chronic inflammation at the tumor site on cancer development, progression, and prognosis: emphasis on non-small cell lung cancer. J Thorac Oncol. (2011) 6:824–33. doi: 10.1097/JTO.0b013e3182037b76
67. Liu Y, Cao X. Immunosuppressive cells in tumor immune escape and metastasis. J Mol Med. (2016) 94:509–22. doi: 10.1007/s00109-015-1376-x
68. Ahmed N, Escalona R, Leung D, Chan E, Kannourakis G. Tumour microenvironment and metabolic plasticity in cancer and cancer stem cells: Perspectives on metabolic and immune regulatory signatures in chemoresistant ovarian cancer stem cells. Semin Cancer Biol. (2018) 53:265–81. doi: 10.1016/j.semcancer.2018.10.002
69. Caro-Maldonado A, Wang R, Nichols AG, Kuraoka M, Milasta S, Sun LD, et al. Metabolic reprogramming is required for antibody production that is suppressed in anergic but exaggerated in chronically BAFF-exposed B cells. J Immunol. (2014) 192:3626–36. doi: 10.4049/jimmunol.1302062
70. Romero-Garcia S, Moreno-Altamirano MMB, Prado-Garcia H, Sánchez-García FJ. Lactate contribution to the tumor microenvironment: mechanisms, effects on immune cells and therapeutic relevance. Front Immunol. (2016) 7:52. doi: 10.3389/fimmu.2016.00052
71. Jacobs SR, Herman CE, Maciver NJ, Wofford JA, Wieman HL, Hammen JJ, et al. Glucose uptake is limiting in T cell activation and requires CD28-mediated Akt-dependent and independent pathways. J Immunol. (2008) 180:4476–86. doi: 10.4049/jimmunol.180.7.4476
72. Wang R, Dillon CP, Shi LZ, Milasta S, Carter R, Finkelstein D, et al. The transcription factor Myc controls metabolic reprogramming upon T lymphocyte activation. Immunity. (2011) 35:871–82. doi: 10.1016/j.immuni.2011.09.021
73. Wang R, Green DR. Metabolic reprogramming and metabolic dependency in T cells. Immunol Rev. (2012) 249:14–26. doi: 10.1111/j.1600-065X.2012.01155.x
74. Gottfried E, Kunz-Schughart LA, Ebner S, Mueller-Klieser W, Hoves S, Andreesen R, et al. Tumor-derived lactic acid modulates dendritic cell activation and antigen expression. Blood. (2006) 107:2013–21. doi: 10.1182/blood-2005-05-1795
75. Fischer K, Hoffmann P, Voelkl S, Meidenbauer N, Ammer J, Edinger M, et al. Inhibitory effect of tumor cell-derived lactic acid on human T cells. Blood. (2007) 109:3812–9. doi: 10.1182/blood-2006-07-035972
76. Goetze K, Walenta S, Ksiazkiewicz M, Kunz-Schughart LA, Mueller-Klieser W. Lactate enhances motility of tumor cells and inhibits monocyte migration and cytokine release. Int J Oncol. (2011) 39:453–63. doi: 10.3892/ijo.2011.1055
77. Carmona-Fontaine C, Bucci V, Akkari L, Deforet M, Joyce JA, Xavier JB. Emergence of spatial structure in the tumor microenvironment due to the Warburg effect. Proc Natl Acad Sci USA. (2013) 110:19402–7. doi: 10.1073/pnas.1311939110
78. Ohashi T, Aoki M, Tomita H, Akazawa T, Sato K, Kuze B, et al. M2-like macrophage polarization in high lactic acid-producing head and neck cancer. Cancer Sci. (2017) 108:1128–34. doi: 10.1111/cas.13244
79. Brand A, Singer K, Koehl GE, Kolitzus M, Schoenhammer G, Thiel A, et al. LDHA-associated lactic acid production blunts tumor immunosurveillance by T and NK cells. Cell Metab. (2016) 24:657–71. doi: 10.1016/j.cmet.2016.08.011
80. Sun L, Suo C, Li ST, Zhang H, Gao P. Metabolic reprogramming for cancer cells and their microenvironment: beyond the Warburg Effect. Biochim Biophys Acta Rev Cancer. (2018) 1870:51–66. doi: 10.1016/j.bbcan.2018.06.005
81. Nelson BH. CD20+ B cells: the other tumor-infiltrating lymphocytes. J Immunol. (2010) 185:4977–82. doi: 10.4049/jimmunol.1001323
82. Linnebacher M, Maletzki C. Tumor-infiltrating B cells: the ignored players in tumor immunology. Oncoimmunology. (2012) 1:1186–8. doi: 10.4161/onci.20641
83. Bohndiek SE, Brindle KM. Imaging and 'omic' methods for the molecular diagnosis of cancer. Expert Rev Mol Diagn. (2010) 10:417–34. doi: 10.1586/erm.10.20
84. Wadsak W, Mitterhauser M. Basics and principles of radiopharmaceuticals for PET/CT. Eur J Radiol. (2010) 73:461–9. doi: 10.1016/j.ejrad.2009.12.022
85. Gambhir SS. Molecular imaging of cancer with positron emission tomography. Nat Rev Cancer. (2002) 2:683–93. doi: 10.1038/nrc882
86. Witney TH, James ML, Shen B, Chang E, Pohling C, Arksey N, et al. PET imaging of tumor glycolysis downstream of hexokinase through noninvasive measurement of pyruvate kinase M2. Sci Transl Med. (2015) 7:310ra169. doi: 10.1126/scitranslmed.aac6117
87. Venneti S, Dunphy M, Zhang H, Pitter KL, Zanzonico P, Campos C, et al. Glutamine-based PET imaging facilitates enhanced metabolic evaluation of gliomas in vivo. Sci Transl Med. (2015) 7:274ra217. doi: 10.1126/scitranslmed.aaa1009
88. Vander Heiden MG, DeBerardinis RJ. Understanding the intersections between metabolism and cancer biology. Cell. (2017) 168:657–669. doi: 10.1016/j.cell.2016.12.039
89. Nelson SJ, Kurhanewicz J, Vigneron DB, Larson PE, Harzstark AL, Ferrone M, et al. Metabolic imaging of patients with prostate cancer using hyperpolarized [1-13C]pyruvate. Sci Transl Med. (2013) 5:198ra108. doi: 10.1126/scitranslmed.3006070
90. Andronesi OC, Kim GS, Gerstner E, Batchelor T, Tzika AA, Fantin VR, et al. Detection of 2-hydroxyglutarate in IDH-mutated glioma patients by in vivo spectral-editing and 2D correlation magnetic resonance spectroscopy. Sci Transl Med. (2012) 4:116ra114. doi: 10.1126/scitranslmed.3002693
91. Choi C, Ganji SK, DeBerardinis RJ, Hatanpaa KJ, Rakheja D, Kovacs Z, et al. 2-hydroxyglutarate detection by magnetic resonance spectroscopy in IDH-mutated patients with gliomas. Nat Med. (2012) 18:624–9. doi: 10.1038/nm.2682
92. Cheong H, Lu C, Lindsten T, Thompson CB. Therapeutic targets in cancer cell metabolism and autophagy. Nat Biotechnol. (2012) 30:671–8. doi: 10.1038/nbt.2285
93. Veys K, Alvarado-Diaz A, De Bock K. Measuring glycolytic and mitochondrial fluxes in endothelial cells using radioactive tracers. Methods Mol Biol. (2019) 1862:121–36. doi: 10.1007/978-1-4939-8769-6_9
94. Granja S PC, Reis RM, Martinho O, Baltazar F. Glucose addiction in cancer therapy advances and drawbacks. Curr Drug Metab. (2015) 16:221–42. doi: 10.2174/1389200216666150602145145
95. Reckzeh ES, Karageorgis G, Schwalfenberg M, Ceballos J, Nowacki J, Stroet MCM, et al. Inhibition of glucose transporters and glutaminase synergistically impairs tumor cell growth. Cell Chem Biol. (2019) 26:1214–28.e25. doi: 10.1016/j.chembiol.2019.06.005
96. Muschen M. Metabolic gatekeepers to safeguard against autoimmunity and oncogenic B cell transformation. Nat Rev Immunol. (2019) 19:337–48. doi: 10.1038/s41577-019-0154-3
97. Talekar M, Boreddy SR, Singh A, Amiji M. Tumor aerobic glycolysis: new insights into therapeutic strategies with targeted delivery. Expert Opin Biol Ther. (2014) 14:1145–59. doi: 10.1517/14712598.2014.912270
98. Sabnis HS, Somasagara RR, Bunting KD. Targeting MYC dependence by metabolic inhibitors in cancer. Genes. (2017) 8:114. doi: 10.3390/genes8040114
99. Fang J, Quinones QJ, Holman TL, Morowitz MJ, Wang Q, Zhao H, et al. The H+-linked monocarboxylate transporter (MCT1/SLC16A1): a potential therapeutic target for high-risk neuroblastoma. Mol Pharmacol. (2006) 70:2108–15. doi: 10.1124/mol.106.026245
100. Goldman A, Khiste S, Freinkman E, Dhawan A, Majumder B, Mondal J, et al. Targeting tumor phenotypic plasticity and metabolic remodeling in adaptive cross-drug tolerance. Sci Signal. (2019) 12:eaas8779. doi: 10.1126/scisignal.aas8779
101. Chen TJ, Wang HJ, Liu JS, Cheng HH, Hsu SC, Wu MC, et al. Mutations in the PKM2 exon-10 region are associated with reduced allostery and increased nuclear translocation. Commun Biol. (2019) 2:105. doi: 10.1038/s42003-019-0343-4
102. Kinnaird A, Michelakis ED. Metabolic modulation of cancer: a new frontier with great translational potential. J Mol Med. (2015) 93:127–42. doi: 10.1007/s00109-014-1250-2
103. Guerra F, Arbini AA, Moro L. Mitochondria and cancer chemoresistance. Biochim Biophys Acta Bioenerg. (2017) 1858:686–99. doi: 10.1016/j.bbabio.2017.01.012
104. Guo J, Xue Q, Liu K, Ge W, Liu W, Wang J, et al. Dimethylaminomicheliolide (DMAMCL) suppresses the proliferation of glioblastoma cells via targeting pyruvate kinase 2 (PKM2) and rewiring aerobic glycolysis. Front Oncol. (2019) 9:993. doi: 10.3389/fonc.2019.00993
105. El Hassouni B, Granchi C, Vallés-Marti A, Supadmanaba IGP, Bononi G, Tuccinardi T, et al. The dichotomous role of the glycolytic metabolism pathway in cancer metastasis: interplay with the complex tumor microenvironment and novel therapeutic strategies. Semin Cancer Biol. (2019):S1044-579X(19)30180-4. doi: 10.1016/j.semcancer.2019.08.025
106. Colen CB, Seraji-Bozorgzad N, Marples B, Galloway MP, Sloan AE, Mathupala SP. Metabolic remodeling of malignant gliomas for enhanced sensitization during radiotherapy: an in vitro study. Neurosurgery. (2006) 59:1313–23; discussion 1323–4. doi: 10.1227/01.NEU.0000249218.65332.BF
107. Rohle D, Popovici-Muller J, Palaskas N, Turcan S, Grommes C, Campos C, et al. An inhibitor of mutant IDH1 delays growth and promotes differentiation of glioma cells. Science. (2013) 340:626–30. doi: 10.1126/science.1236062
108. Wang F, Travins J, DeLaBarre B, Penard-Lacronique V, Schalm S, Hansen E, et al. Targeted inhibition of mutant IDH2 in leukemia cells induces cellular differentiation. Science. (2013) 340:622–6. doi: 10.1126/science.1234769
109. Martinez-Outschoorn UE, Peiris-Pages M, Pestell RG, Sotgia F, Lisanti MP. Cancer metabolism: a therapeutic perspective. Nat Rev Clin Oncol. (2017) 14:11–31. doi: 10.1038/nrclinonc.2016.60
110. Liu Y, Cao Y, Zhang W, Bergmeier S, Qian Y, Akbar H, et al. A small-molecule inhibitor of glucose transporter 1 downregulates glycolysis, induces cell-cycle arrest, and inhibits cancer cell growth in vitro and in vivo. Mol Cancer Ther. (2012) 11:1672–82. doi: 10.1158/1535-7163.MCT-12-0131
111. Chan DA, Sutphin PD, Nguyen P, Turcotte S, Lai EW, Banh A, et al. Targeting GLUT1 and the Warburg effect in renal cell carcinoma by chemical synthetic lethality. Sci Transl Med. (2011) 3:94ra70. doi: 10.1126/scitranslmed.3002394
112. Boudreau A, Purkey HE, Hitz A, Robarge K, Peterson D, Labadie S, et al. Metabolic plasticity underpins innate and acquired resistance to LDHA inhibition. Nat Chem Biol. (2016) 12:779–86. doi: 10.1038/nchembio.2143
113. Kishton RJ, Rathmell JC. Novel therapeutic targets of tumor metabolism. Cancer J. (2015) 21:62–9. doi: 10.1097/PPO.0000000000000099
114. Losman JA, Kaelin WG Jr. What a difference a hydroxyl makes: mutant IDH, (R)-2-hydroxyglutarate, and cancer. Genes Dev. (2013) 27:836–52. doi: 10.1101/gad.217406.113
115. Tateishi K, Wakimoto H, Iafrate AJ, Tanaka S, Loebel F, Lelic N, et al. Extreme vulnerability of IDH1 mutant cancers to NAD+ depletion. Cancer Cell. (2015) 28:773–84. doi: 10.1016/j.ccell.2015.11.006
116. de Padua MC, Delodi G, Vučetić M, Durivault J, Vial V, Bayer P, et al. Disrupting glucose-6-phosphate isomerase fully suppresses the “Warburg effect” and activates OXPHOS with minimal impact on tumor growth except in hypoxia. Oncotarget. (2017) 8:87623–37. doi: 10.18632/oncotarget.21007
117. Ngo B, Van Riper JM, Cantley LC, Yun J. Targeting cancer vulnerabilities with high-dose vitamin C. Nat Rev Cancer. (2019) 19:271–82. doi: 10.1038/s41568-019-0135-7
118. Park S, Ahn S, Shin Y, Yang Y, Yeom CH. Vitamin C in cancer: a metabolomics perspective. Front Physiol. (2018) 9:762. doi: 10.3389/fphys.2018.00762
119. Polireddy K, Dong R, Reed G, Yu J, Chen P, Williamson S, et al. High dose parenteral ascorbate inhibited pancreatic cancer growth and metastasis: mechanisms and a phase I/IIa study. Sci Rep. (2017) 7:17188. doi: 10.1038/s41598-017-17568-8
120. Schoenfeld JD, Sibenaller ZA, Mapuskar KA, Wagner BA, Cramer-Morales KL, Furqan M, et al. O2·− and H2O2-mediated disruption of Fe metabolism causes the differential susceptibility of NSCLC and GBM cancer cells to pharmacological ascorbate. Cancer Cell. (2017) 31:487–500.e8. doi: 10.1016/j.ccell.2017.07.008
121. Yun J, Mullarky E, Lu C, Bosch KN, Kavalier A, Rivera K, et al. Vitamin C selectively kills KRAS and BRAF mutant colorectal cancer cells by targeting GAPDH. Science. (2015) 350:1391–6. doi: 10.1126/science.aaa5004
122. Uetaki M, Tabata S, Nakasuka F, Soga T, Tomita M. Metabolomic alterations in human cancer cells by vitamin C-induced oxidative stress. Sci Rep. (2015) 5:13896. doi: 10.1038/srep13896
123. Chen Q, Espey MG, Sun AY, Pooput C, Kirk KL, Krishna MC, et al. Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice. Proc Natl Acad Sci USA. (2008) 105:11105–9. doi: 10.1073/pnas.0804226105
124. Shenoy N, Creagan E, Witzig T, Levine M. Ascorbic acid in cancer treatment: let the phoenix fly. Cancer Cell. (2018) 34:700–6. doi: 10.1016/j.ccell.2018.07.014
125. Mikirova N, Casciari J, Riordan N, Hunninghake R. Clinical experience with intravenous administration of ascorbic acid: achievable levels in blood for different states of inflammation and disease in cancer patients. J Transl Med. (2013) 11:191. doi: 10.1186/1479-5876-11-191
126. Cha J, Roomi MW, Ivanov V, Kalinovsky T, Niedzwiecki A, Rath M. Ascorbate supplementation inhibits growth and metastasis of B16FO melanoma and 4T1 breast cancer cells in vitamin C-deficient mice. Int J Oncol. (2013) 42:55–64. doi: 10.3892/ijo.2012.1712
127. Sajadian SO, Tripura C, Samani FS, Ruoss M, Dooley S, Baharvand H, et al. Vitamin C enhances epigenetic modifications induced by 5-azacytidine and cell cycle arrest in the hepatocellular carcinoma cell lines HLE and Huh7. Clin Epigenetics. (2016) 8:46. doi: 10.1186/s13148-016-0213-6
128. Elgendy M, Ciro M, Hosseini A, Weiszmann J, Mazzarella L, Ferrari E, et al. Combination of hypoglycemia and metformin impairs tumor metabolic plasticity and growth by modulating the PP2A-GSK3β-MCL-1 axis. Cancer Cell. (2019) 35:798–815.e5. doi: 10.1016/j.ccell.2019.03.007
129. Dalva-Aydemir S, Bajpai R, Martinez M, Adekola KU, Kandela I, Wei C, et al. Targeting the metabolic plasticity of multiple myeloma with FDA-approved ritonavir and metformin. Clin Cancer Res. (2015) 21:1161–71. doi: 10.1158/1078-0432.CCR-14-1088
130. Dang CV. Links between metabolism and cancer. Genes Dev. (2012) 26:877–90. doi: 10.1101/gad.189365.112
131. Kumar A, Vishvakarma NK, Tyagi A, Bharti AC, Singh SM. Anti-neoplastic action of aspirin against a T-cell lymphoma involves an alteration in the tumour microenvironment and regulation of tumour cell survival. Biosci Rep. (2012) 32:91–104. doi: 10.1042/BSR20110027
Keywords: metabolism, tumor, plasticity, glucose, Warburg effect, diagnosis, treatment
Citation: Lin X, Xiao Z, Chen T, Liang SH and Guo H (2020) Glucose Metabolism on Tumor Plasticity, Diagnosis, and Treatment. Front. Oncol. 10:317. doi: 10.3389/fonc.2020.00317
Received: 27 December 2019; Accepted: 21 February 2020;
Published: 06 March 2020.
Edited by:
Dong-Hua Yang, St. John's University, United StatesCopyright © 2020 Lin, Xiao, Chen, Liang and Guo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xiaoping Lin, Z3VvaHVpcWluMkAxNjMuY29t; Huiqin Guo, bGlueHBAc3lzdWNjLm9yZy5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.