
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol., 04 March 2020
Sec. Cancer Epidemiology and Prevention
Volume 10 - 2020 | https://doi.org/10.3389/fonc.2020.00145
 Ronilson Oliveira Durães1,2
Ronilson Oliveira Durães1,2 Gustavo Noriz Berardinelli1
Gustavo Noriz Berardinelli1 Allini Mafra da Costa3
Allini Mafra da Costa3 Cristovam Scapulatempo-Neto1,4
Cristovam Scapulatempo-Neto1,4 Rui Pereira5,6
Rui Pereira5,6 Marco Antônio Oliveira7
Marco Antônio Oliveira7 Denise Peixoto Guimarães1,8
Denise Peixoto Guimarães1,8 Rui Manuel Reis1,9,10*
Rui Manuel Reis1,9,10*Background: Colorectal cancer (CRC) is the third most frequent and the second deadliest cancer worldwide. The ethnic structure of the population has been gaining prominence as a cancer player. The purpose of this study was to determine the genetic ancestry of Brazilian CRC patients. Moreover, we intended to interrogate its impact on patients' clinicopathological features.
Methods: Retrospective observational cohort study with 1,002 patients with CRC admitted from 2000 to 2014 at Barretos Cancer Hospital. Following tumor DNA isolation, genetic ancestry was assessed using a specific panel of 46 ancestry informative markers. Survival rates were obtained by the Kaplan–Meier method, and the log-rank test was used to compare the survival curves. Multivariable Cox proportional regression models were used to estimate hazard ratios (HRs).
Results: We observed considerable admixture in the genetic composition, with the following average proportions: European 74.2%, African 12.7%, Asian 6.5%, and Amerindian 6.6%. The multivariate analysis for cancer-specific survival showed that clinical stage, lymphovascular invasion, and the presence of recurrence were associated with an increased relative risk of death from cancer (p < 0.05). High African proportion was associated with younger age at diagnosis, while high Amerindian proportion was associated with the mucinous histological subtype.
Conclusions: This represents the larger assessment of genetic ancestry in a population of Brazilian patients with CRC. Brazilian CRC patients exhibited similar clinicopathological features as described in Western countries.
Impact: Genetic ancestry components corroborated the significant admixture, and importantly, patients with high African proportion develop cancer at a younger age.
Colorectal cancer (CRC) represents more than 1,849,518 new cases, accounting for approximately 10.2% of all neoplasms worldwide (1). CRC is the third most common neoplasm in men and the second in women (1–4). CRC mortality is also high, with 880,792 deaths having been estimated for 2018, corresponding to 9.2% of the total, with higher rates (52%) being observed in less developed regions of the world (1). The incidence of CRC varies more than 10-fold worldwide (1). The highest detection rates are observed in Australia, New Zealand, and countries of Europe and North America, and the lowest are found in the countries of Africa, South America, and Asia (1, 2). In Brazil, according to the National Cancer Institute (INCA), an estimated 17,380 new cases of colon and rectum cancer in men and 18,980 in women are expected for 2018, which occupies the third position in men and the second among women (4).
Several reasons account for these discrepancies, including distinct risk factors. Age is the primary risk factor, yet many other factors contribute to CRC development including a previous history of colorectal neoplasia and/or adenomas or family history of CRC; a diet rich in red meat and saturated fats, fruits, and vegetables; obesity and sedentary lifestyle; smoking; diabetes mellitus; CRC-associated syndromes such as familial adenomatous polyposis, hereditary non-polyposis colorectal cancer (HNPCC or Lynch syndrome); and inflammatory diseases of the colon (2, 3, 5, 6). Besides the risk factors abovementioned, patient ethnicity has been reported as a risk and prognostic factor (7–12). The ethnic structure becomes more pressing in the Brazilian population due to its great admixture (13–17). Currently, genetic markers are available that determine, with more assertiveness than the self-declared form or based on physical traits, the ethnic structure of each individual (14, 18).
Despite the high incidence and mortality rate of CRC in Brazil, few studies have comprehensively described and characterized the main clinicopathological features of Brazilian patients with CRC (19, 20). Therefore, this study aimed to characterize the clinicopathological aspects of CRC patients, to determine their genetic ancestry, and to identify whether the genetic ancestry can influence patients' clinicopathological features and disease outcome.
We conducted a retrospective observational cohort study enrolling 1,002 patients with CRC admitted from 2000 to 2014 at Barretos Cancer Hospital, Barretos, São Paulo, Brazil. Of the total of 1,002 cases, 96.3% (965/1,002) were selected from the Department of Low-Digestive and 3.7% (37/1,002) were oncogenetic-based cases, being 1.8% (18/1,002) confirmed Lynch syndrome cases, 1.5% (15/1,002) confirmed familial adenomatous polyposis (FAP) syndrome cases, and 0.4% (4/1,002) of unclassified hereditary syndrome (21). Clinicopathological and treatment data of CRC patients were collected from patient medical records. The present study evaluated 21 variables. The seventh edition of the American Joint Committee on Cancer (AJCC) was used for tumor staging. The Institutional Ethics Committee approved the study (protocol number: 600/2012-CAAE: 02468812.30000.5437).
DNA samples were recovered from formalin-fixed paraffin-embedded (FFPE) tissue of tumor specimens obtained from surgical or endoscopic procedures. The DNA was isolated using the DNA Micro kit (Qiagen), according to the method previously established by our group (22).
The ancestry of the patients was determined using ancestry informative markers (AIMs) as previously reported (14, 23–25). Briefly, 46 small insertion–deletion (INDEL) polymorphisms were ascertained to maximize the divergence between four human major population groups: Amerindian (AME), European (EUR), African (AFR), and East Asian (ASN). These markers were selected due to their high allele frequency divergence between different ancestral or geographically distant populations, including more than 1,000 individuals from 40 reference populations from the Human Genome Diversity Project (HGDP)-Centre d/Etude du Polymorphisme (CEPH), plus individuals from Angola, Portugal, Taiwan, and indigenous Brazilian, which allowed to establish the ancestral proportions in high admixture individuals and populations, like the Brazilian one (14). Moreover, they were assembled in a simple multiplex reaction following a short amplicon strategy, adequate for challenging samples such as FFPE (15, 26, 27). The primer sequences and PCR conditions were according to Giolo et al. (14).
After DNA extraction, and multiplex PCR with 46 primers, the amplified products were further subjected to capillary electrophoresis and fragment analysis on an ABI 3500 Genetic Analyzer (Applied Biosystems) according to the manufacturer's instructions. These 46 INDELs are used mainly to estimate ancestry proportions in admixed populations and assess the structure of those populations. Two observers independently analyzed the electropherograms, and the genotypes were automatically assigned with GeneMapper Software v4.1 (Applied Biosystems).
The ancestry ratios were evaluated using the Structure Software v2.3.4 (23, 24, 28, 29), considering the four main population groups, AME, EUR, AFR, and ASN, as possible contributors to the current Brazilian genetic composition. Briefly, the data available for the HGDP-CEPH panel were used as a reference for the ancestral populations, and a supervised analysis was performed to estimate ancestry relationship proportions of the individuals involved in the study. The Structure software runs considering K = 4 consisted of 100,000 burning steps followed by 100,000 Markov Chain Monte Carlo iterations. The option “Use population information to test for migrants” was used with the admixture model, considering allele frequencies correlated, and updating allele frequencies using only individuals with POPFLAG = 1.
Patient and cancer characteristics were reported as frequencies (number and percentage). First, the continuous variables of genetic ancestry component were summarized as mean [standard deviation (SD)]. For the association of the genetic ancestry component (AFR, EUR, ASN, AME) by AIMs panel with patient and clinical characteristics, the chi-square test or Fisher's exact test was used. For this step, ancestry proportions were further categorically defined as low, intermediate, and high based on tercile distribution (Table 1 and Supplementary Table 1).
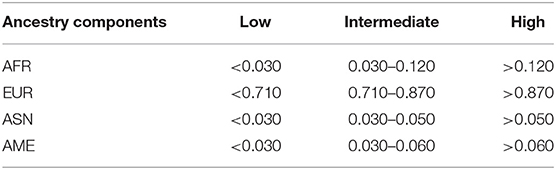
Table 1. Ancestry background categorization according to tercile based on percentage proportions for all four ethnic groups.
The overall survival (OS) and the cancer-specific survival (CSS) rates were obtained using the Kaplan–Meier method. Survival rates were estimated in months. Survival was defined as the period from diagnosis to the date of death or the time at which information was last obtained. For the analysis, the event of interest was death by any cause for OS and death related to cancer for CSS. Cases that were alive were censored for OS, and cases that were alive or dead from other causes were censored for CSS. Such information was obtained through direct consultation to the death certificate or medical records. The follow-up median of our sample was 62.0 months. The log-rank test was used to compare survival curves, and results were considered significant when the p < 0.05.
Multiple confirmatory models were used to check whether genetic ancestry component (AFR, EUR, ASN, AME) by AIMs panel was related to the prognosis of CRC. Multivariable Cox proportional hazards regression models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs) for the variables with p < 0.20 in univariate analyses and adjusted with treatment period and genetic ancestry components by AIMs panel. Fisher exact test was used for association analysis.
For tabulation and statistical analysis, the IBM® SPSS® Statistics 21.0 software for Windows (IBM Corporation, Route 100, Somers, NY 10589) was used. The level of statistical significance was set at 0.05 for all analyses.
The present study included 1,002 cases, and the main clinicopathological features are summarized in Table 2. A detailed description of therapeutic regimens is shown in Supplementary Table 2. There were more men than women in the population (51.9%), most patients were between 50 and 75 years old at diagnosis (60.5%), and the majority lived in the South or Southeast regions of Brazil (82%). The distribution of the CRC patients according to the Brazilian state of origin is plotted in Supplementary Figure 1. The left colon was the leading primary tumor site, representing 46% of the cases, and adenocarcinoma was the main histological type, representing 93.5% of the cases. The cases were distributed in all stages, but clinical stages II and III were the most common, representing together 70.8% of the cases.
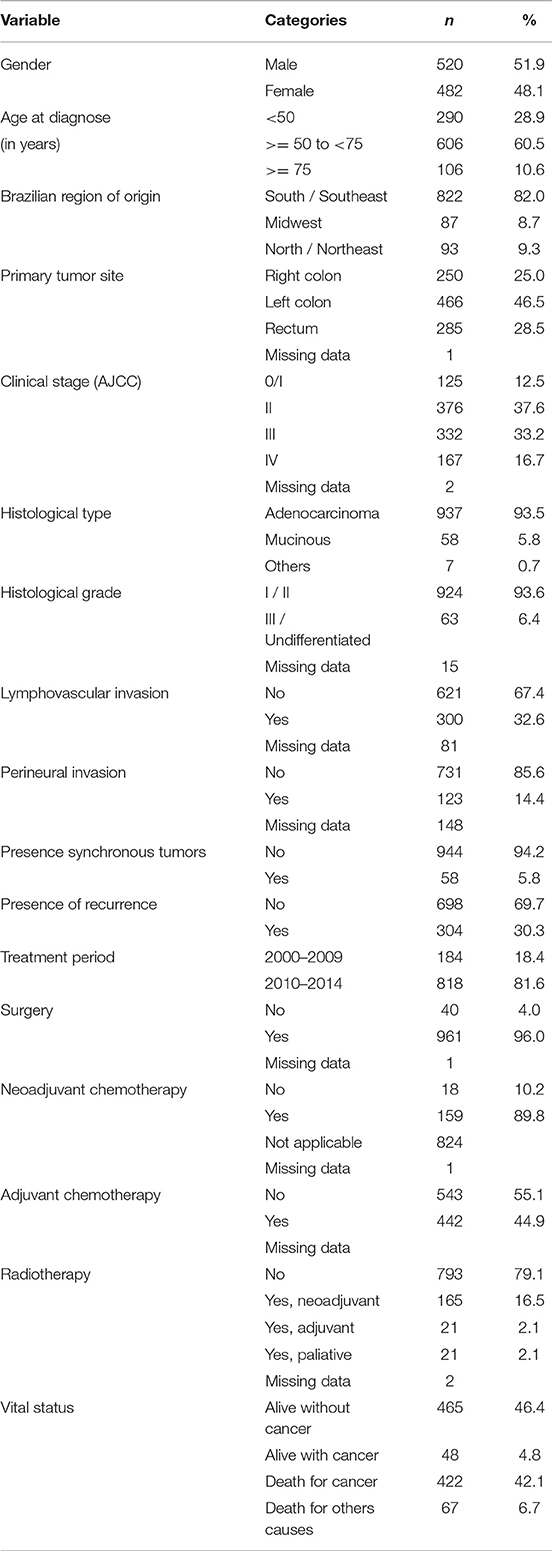
Table 2. Clinicopathological features of Brazilian colorectal cancer patients (n = 1,002).
The present study also aimed to evaluate the genetic ancestry of the patients, which was performed in 934/1,002 (93.2%) of the cases. In a small subset of cases (n = 68), the genetic ancestry could not be evaluated due to low quantity and poor-quality DNA. We observed a great admixture in genetic composition, with the following averages of ancestral proportions: AFR 12.7% (SD = 15.7%), EUR 74.2% (SD = 20.6%), ASN 6.5% (SD = 11.3%), and AME 6.6% (SD = 7.1%) (Figure 1). The average of each genetic ancestry component according to the Brazilian state of origin is plotted in Figure 2. The ancestry proportions were further categorically defined as low, intermediate, and high based on tercile distribution (Table 1 and Supplementary Table 1).
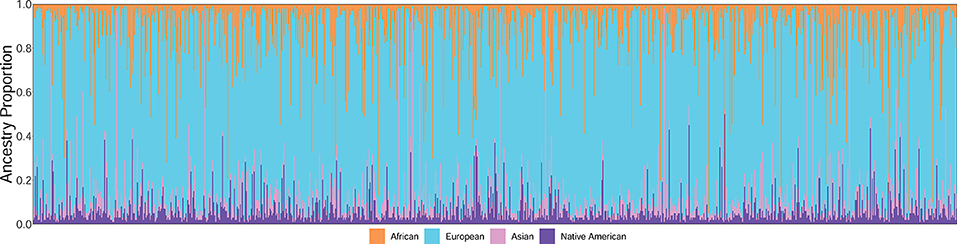
Figure 1. Individual ancestry estimates for the Brazilian colorectal cancer patients (n = 934).
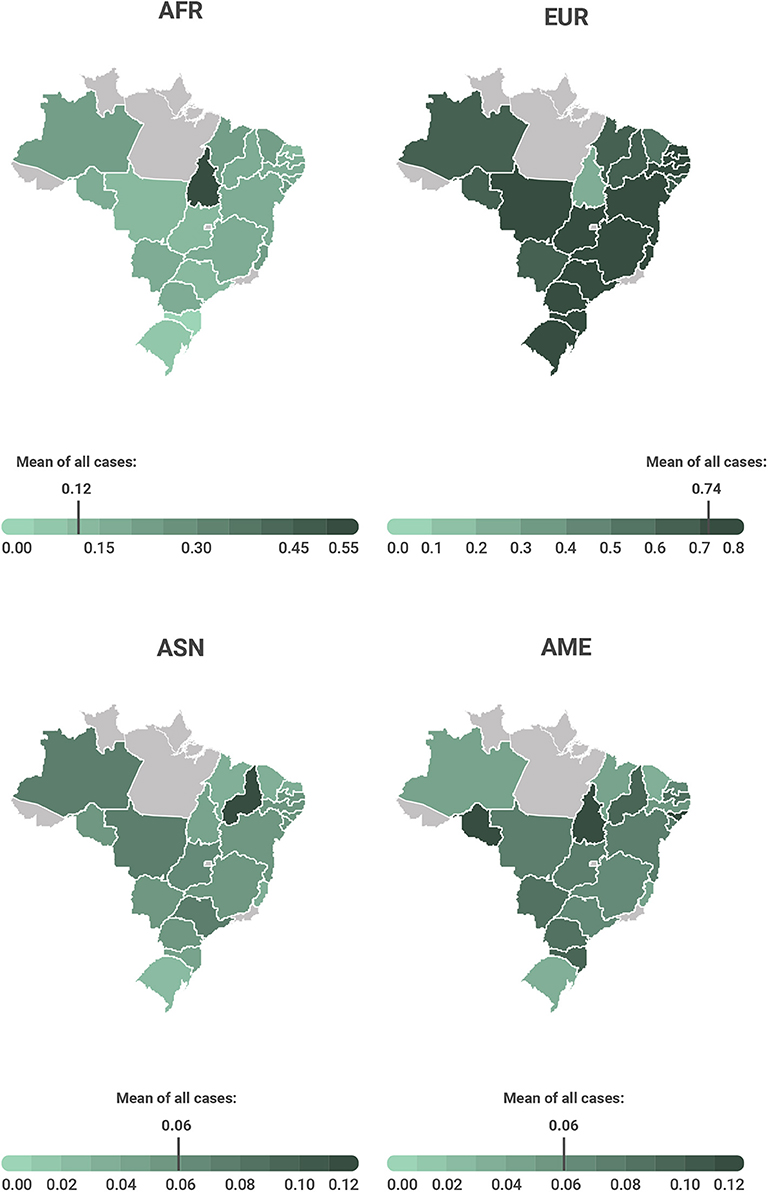
Figure 2. Average of each genetic ancestry component according to the Brazilian state of origin. AFR- African; EUR- European; ASN- Asian; AME- Amerindian (Native American).
We further investigated the association of genetic ancestry with patients' clinicopathological characteristics (Table 3). We observed significant associations between the AFR component and younger age at diagnosis (p = 0.013), Brazilian region of origin (p < 0.001), and recurrence of the disease (p = 0.034). For the EUR component, we found significant associations with the region of origin (p < 0.001), adenocarcinoma (p = 0.023), higher histological grade (p = 0.040), and presence of synchronous tumors (p = 0.012). For the AME component, a significant association with the mucinous histological type (p = 0.033) was observed.
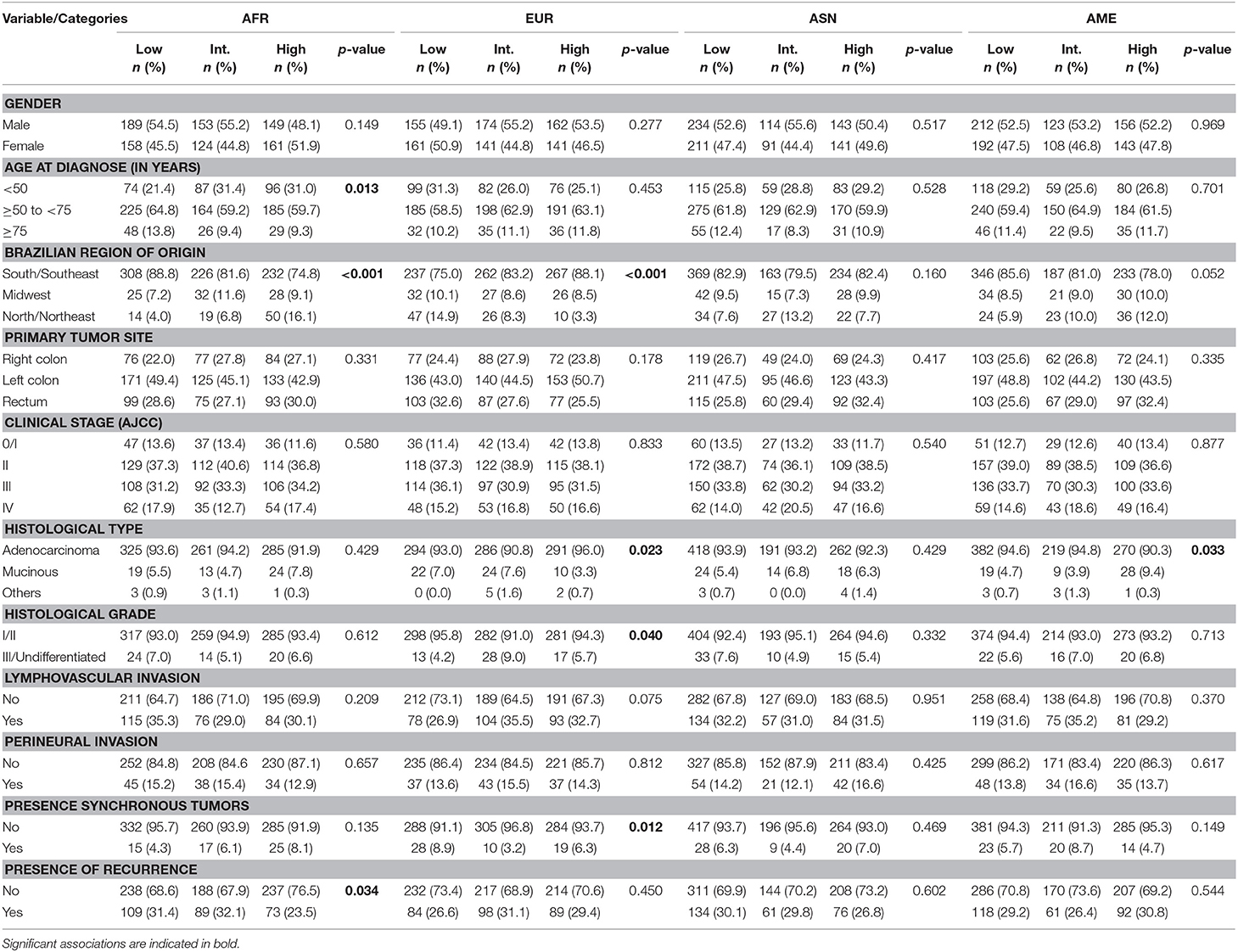
Table 3. Association between clinicopathological and genetic ancestry components by AIM-INDEL panel (n = 934).
An initial univariate analysis of survival was performed, including 1,002 individuals: 489 events occurred in OS, and 422 events occurred in CSS. The probability of patients living for more than 5 years was 58.2% for OS and 62.3% for CSS (Table 4). Several significant associations were observed between OS and CSS and patients' features, including gender, clinical stage, histological type, histological grade, lymphovascular invasion, perineural invasion, presence of recurrence, treatment period, neoadjuvant chemotherapy, adjuvant chemotherapy, and radiotherapy (Table 3 and Supplementary Figure 2). On the univariate survival analyses (OS and CSS), the genetic ancestry categorically defined as low, intermediate, and high based on terciles was not associated with CRC survival (Table 4).
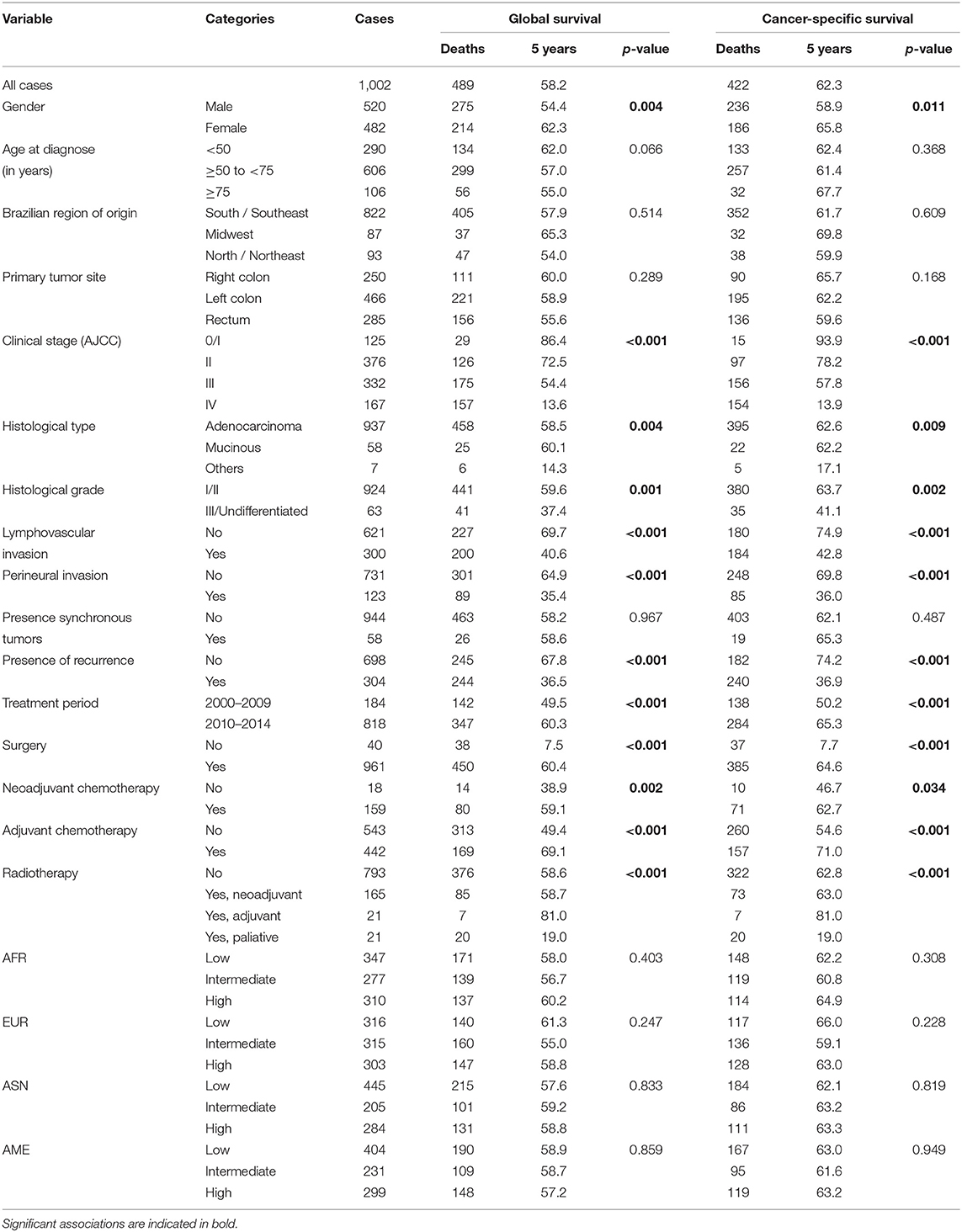
Table 4. Kaplan-Meier estimates of overall survival and cancer-specific survival of colorectal cancer patients (n = 1,002).
The multivariate analysis for CSS adjusted by treatment period and genetic ancestry components showed that clinical stage, lymphovascular invasion, and the presence of recurrence were associated with an increased relative risk of death from cancer (p < 0.05), whereas adjuvant chemotherapy was associated with a lower risk of death (Table 5). These results are explained by the different therapeutic approaches used in distinct clinical stages (Supplementary Tables 3, 4).
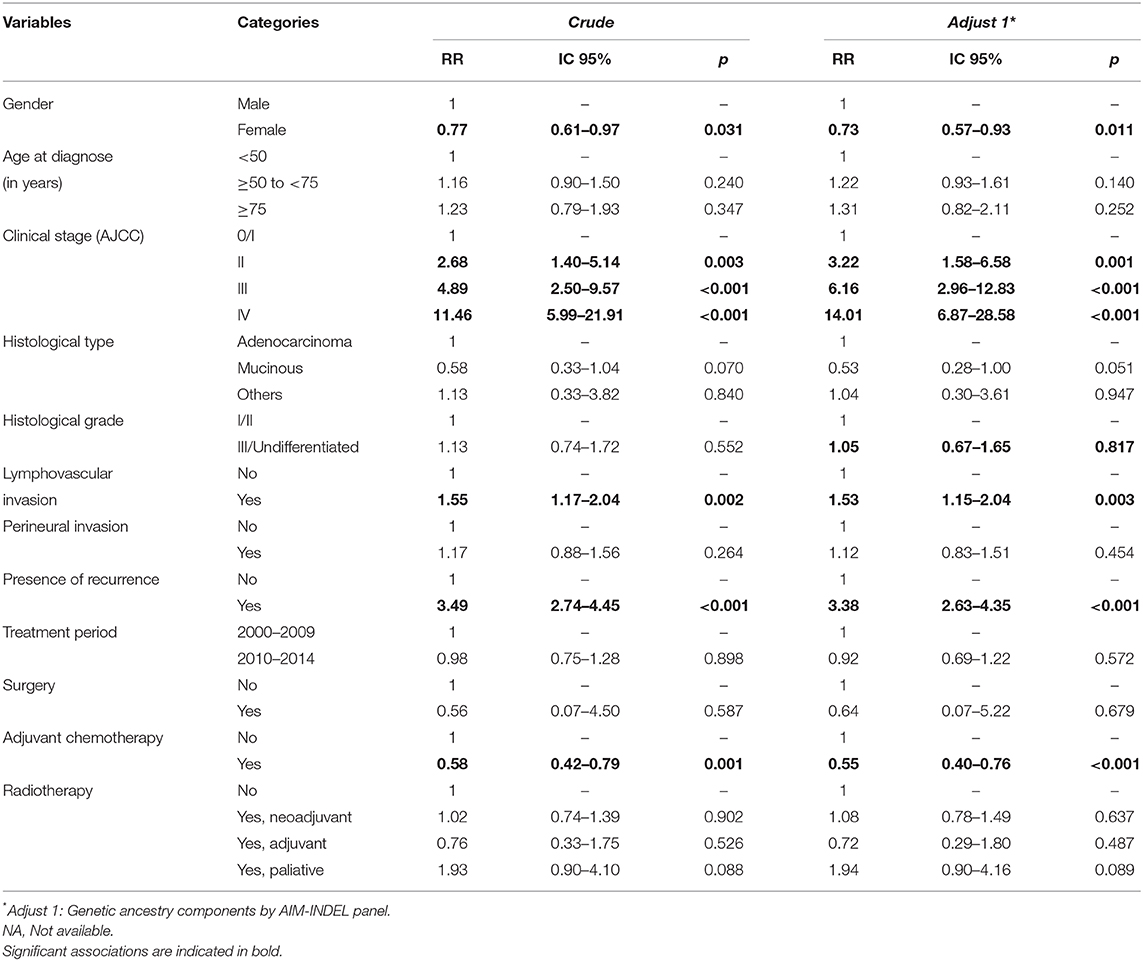
Table 5. Multivariate analysis of cancer-specific survival associated with different clinicopathological characteristics and treatment of patients with colorectal cancer.
CRC is one of the most common neoplasms in men and women worldwide (3, 30, 31). Although its incidence is declining in the US and other western countries (32); in others, including Brazil, we are still witnessing an increase in the number of cases, and it is a major public health problem. In this study, we intended to characterize the genetic ancestry of an extensive series of 1,002 CRC patients admitted at the Barretos Cancer Hospital. Knowing that the Brazilian population is ethnically one of the most heterogeneous in the world (14, 18), with an essential contribution from the main ethnicities that formed the background of our population, we also intended to correlate the ancestry components (EUR, AFR, ASN, and AME) measured genetically with the different clinical–pathological factors and its prognostic role.
There was a slight male predominance, with an incidence of 1.08. In all regions of the world, despite the similarities between genders, the rates were higher for males (vs. females, 1.3) in the American population (2, 33), as well as in Europe (1) and Asia (34). Others have a higher incidence among women in the colon (4, 35).
The main studies divide the samples into three age categories: below 50, between 50 and 75, and above 75 years old. The age of 50 years old is critical to differentiate between hereditary and sporadic CRC cases. This age limit has been used in the Amsterdam criteria (36, 37) and also to recommend screening colonoscopic examination for people at average risk for CRC (38, 39). Although it has been reported that 21 to 33% of patients are older than 75 years [Surveillance Epidemiologic and End Results (SEER)] (40), they may account for more than 40% and are underrepresented in the clinical studies. These clinical studies use in their inclusion criteria an age group of up to 75 years old as a limit to be treated (41–44), mainly due to comorbidities. Therefore, we adopted the upper limit range as those with 75 or more years old (45).
The mean age at diagnosis in our population was 57.7 years (SD = 13.8), below the American age of 68 years (31) and the European age of 72 years (45). The predominant age group in our population was between 50 and 75 years old (60.5%), similar to that in the SEER (31) data.
Our population had a high incidence of patients younger than 50 years old (28.9%), higher than the 20% reported in studies including North American populations (31) and Asian patients (3–14%) (46). This finding can be due to the inclusion criteria and to the potential presence of some hereditary cases in the present analysis. In the present study, patients with a known and genetically confirmed familial history of Lynch or APC represented <4% of cases (21); however, we cannot rule out the existence of hereditary cases in the cohort. Since 1992, the incidence in cases under 50 has increased by 1.5% per year (3, 45), especially from 20 to 34 years. According to the American College of Gastroenterology (39), colorectal cancer screening begins at age 50, except for those of African origin, where it is recommended to start at age 45 (47). Moreover, some studies even question to initiate at 40 years old (48). In concordance with these findings, we observed that Brazilian CRC patients depicting higher African proportion were associated with younger age of disease onset.
The importance of primary tumor location, being associated with distinct clinical–pathological features, as well as a differential prognostication has been widely discussed. For this, we performed the categorization of the cases included into the right colon, left colon, and rectum (49–53). In our population, 25% of the tumors were in the right colon. This percentage is within the average of other studies that ranged from 22.7 to 39% (49). However, in contrast, we did not find that laterality was associated with disease outcome.
Another critical variable is the TNM staging. In our study, the majority of cases were stage II (37.6%), followed by III (33.2%) and IV (16.7%). The percentage of stage IV at diagnosis is in agreement with several regions of the world (31, 45, 54).
Another goal of our study was to evaluate the main prognostic factors in our CRC patients. To this end, we estimated the OS and CSS and correlated with the different variables collected and selected in the multivariate analysis. The follow-up median of our sample was 62.0 months, very similar to the SEER that was 65.2 months (31). In the study of OS and CSS, we interrogated whether the variables selected in the multivariate analysis would be influenced by other variables such as the treatment period and the genetic ancestry components. Therefore, following adjustment of both variables, namely, treatment period (patients treated from 2000 to 2009 and from 2010 to 2014, where the introduction of the molecular target drugs, such as cetuximab, were included by the Department of Oncology of the Barretos Cancer Hospital), and ancestry, a multivariate analysis was performed.
The multivariate analysis for OS and CSS adjusted by genetic ancestry showed that the clinical stage, lymphovascular invasion, and recurrence of the disease were associated with an increased relative risk of death from cancer. In contrast, adjuvant chemotherapy was associated with a better outcome, as expected.
About 1/3 of our patients had lymphovascular invasion. The association of lymphovascular dissemination and adverse outcomes (55, 56) is well-described, besides being a known definer regarding therapeutics, especially in stage II (3).
The ancestry of the individuals assumes importance concerning its association with specific pathologies, immunological, and therapeutic responses, yet in the vast majority of studies, it is not evaluated (57, 58). Currently, with the availability of molecular tools for genetic studies, self-declaration and/or family origin can no longer be a proxy/authentication of the ancestral origin of an individual or population, especially in regions with a high degree of population admixture such as Brazil (57). However, in a large number of studies, skin color alone is used to assert ethnical origin of CRC patients (7–9, 12, 59). There is an extensive amount of studies, based on self-declaration, suggesting that black skin color patients have a higher incidence and lower survival of CRC (7, 12). However, it is unclear whether the ancestral component alone would influence survival or whether there are other confounding factors, such as less reference to screening methods (60), presence of a higher number of comorbidities diagnosis (7), lack of access to treatment services (61), or low educational/economic level, which can justify this fact (11, 60).
There are several ways to analyze the genetic composition of a particular population, and the selection criteria of genetic markers may diverge between studies, originating different values of the ethnic groups (62) for the Brazilian population. In our study, we analyzed four major ethnic compositions (EUR, AFR, ASN, and AME) using AIMs according to previous studies (13, 14, 18, 63). The present study was retrospective, dependent on the collection of information in medical records, and there was no mention of self-declaration of skin color. Therefore, our data collection instrument did not contemplate this aspect. If we had this information, we could have carried out a cross-referencing of information between the genotype and the phenotype to try to evaluate the fidelity of the latter.
When ancestry was measured genetically, we did not evaluate the data individually, but rather the four ancestor components that form the demographic base of Brazil. Our study did not intend to assess the causal relationship between genetic ancestry and CRC cancer as already done in other studies (64), but rather to correlate them with the various clinical–pathological characteristics of the patients.
As expected, the predominant ancestral component was the EUR one, with an average of 74% followed by the AFR with 13%, and by the ASN and AME with 7%, agreeing with previous studies of the Brazilian population (13, 63, 65). In agreement with other studies (62), a predominance of the European ancestral component in the Southeast and South regions was observed (63). Some differences in our study were observed, for example, the African component concentrated more strongly in the north region, unlike other studies based on the mitochondrial DNA (mtDNA) and not on autosomal AIM-INDELs, where this happened more in the Northeast Brazilian region (13, 17, 62, 63). The contribution of Asian ancestry in the northeast region of 5% is very close to that of the regions known to be colonized by Asians, but this may perhaps be explained first by the small sample size representing this region in our study and/or the proximity of the gene pool between Amerindians and eastern Asians considering the modern history of these human groups (14). The high SDs identified in our study show how miscegenated our Brazilian population is.
When we evaluated the individual components separately, we found that the European ancestral component was significantly associated with the absence of synchronous tumors. The African component was associated with younger patients, in agreement with other international studies (7, 8, 10). The Amerindian component predominated in the Northern region which correlates with other studies and is corroborated by the IBGE (Brazilian Institute of Geography and Statistics) self-declaration assessment (13, 18, 63, 66). Interestingly, we observed an association of the Amerindian component with mucinous histological type.
In our study, there was no correlation between the different ancestry proportions and patient survival. However, some North American studies reported an association of African ancestry based on self-declaration with tumors located in the right colon (67) and that these would be associated with more aggressive behavior histopathology, which would lead to worse survival (7, 11, 12).
Finally, despite the exciting and important findings, this study harbors some limitations, such as the retrospective nature of the study, based on the analysis of medical records, which often do not have complete and accurate information. The extent of the AIM panel could also be arguably higher. Nonetheless, the employed AIM indel set harbors a sufficient number of markers sparsely distributed throughout the genome and is simply analyzed in a multiplexed short-amplicon strategy, which are desirable characteristics considering the challenging nature of the source tumor samples included in our study. Despite the large number of patients and their diverse geographic origin, it does not represent all Brazilian states and the fully ethnical diversity of the Brazilian population, so further studies are warranted to extend our findings.
This pioneering work determined the genetic ancestry profile of more than 1,000 Brazilian patients diagnosed with CRC from a single oncology reference center. We described the main clinicopathological features of the population and observed that patients with a high African proportion develop cancer at a younger age. The present study can contribute to drawing a nationwide portrait of Brazilian CRC patient and may help in the design of management strategies for these patients.
The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
The studies involving human participants were reviewed and approved by Barretos Cancer Hospital Ethics Committee. Written informed consent was not provided because this was a retrospective study.
RD participated in study design, collection of the data, analyzed the data, and prepared the manuscript. GB participated in the collection of the data, carried out the ancestry experiments, and analyzed the data. AC participated in the collection of the data, analyzed the data, and preparation of the manuscript. CS-N participated in the collection of the data, re-evaluation of the diagnosis, and participated in the ancestry experiments. RP participated in the ancestry experiments and analyzed the data. MO participated in the statistical analysis and analysis of the results. DG participated in study design and analysis of the results. RR participated in study design, coordination, analysis of the results, and prepared the manuscript. All authors read and approved the final manuscript.
This study was partially supported by Barretos Cancer Hospital Internal Research Funds (PAIP) of participant authors and Public Ministry of Labor Campinas (Research, Prevention and Education of Occupational Cancer). RR was the recipient of a National Council of Technological and Scientific Development (CNPq) scholarship. AC is recipient of a FAPESP post-doc fellowship (2018/22097-0).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank the Hospital-Based Cancer Registry of Barretos Cancer Hospital (São Paulo, Brazil) for the collaboration in updating the follow-up status of the patients.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2020.00145/full#supplementary-material
AIMs, ancestry informative markers; AFR, African; AME, Amerindian; ASN, Eastern Asian; CCR, colorectal cancer; CI, confidence interval; DNA, deoxyribonucleic acid; EUR, European; FFPE, formalin-fixed paraffin-embedded; HNPCC, hereditary non-polyposis colorectal cancer; HR, hazard ratio; INCA, National Cancer Institute; OS, overall survival; CSS, cancer-specific survival; D, standard deviation.
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. (2018) 68:394–424. doi: 10.3322/caac.21492
2. Devita V, Lawrence T. Cancer: Principles and Practice of Oncology. Philladelphia, PA: LWW (2015).
3. National Comprehensive Cancer Network (NCCN) (2016). Available online at: http://www.nccn.org/professionals/physician_gls/pdf/colon.pdf.
4. Instituto Nacional De Câncer (INCA). Estimativa 2018: Incidência de Câncer no Brasil. Coordenação Geral de Ações Estratégicas. Coordenação de Prevenção e Vigilância. Rio de Janeiro: Ministerio da Saúde (2018).
5. Huxley RR, Ansary-Moghaddam A, Clifton P, Czernichow S, Parr CL, Woodward M. The impact of dietary and lifestyle risk factors on risk of colorectal cancer: a quantitative overview of the epidemiological evidence. Int J Cancer. (2009) 125:171–80. doi: 10.1002/ijc.24343
6. Slattery ML, Fitzpatrick FA. Convergence of hormones, inflammation, and energy-related factors: a novel pathway of cancer etiology. Cancer Prev Res. (2009) 2:922–30. doi: 10.1158/1940-6207.CAPR-08-0191
7. Wallace K, Sterba KR, Gore E, Lewin DN, Ford ME, Thomas MB, et al. Prognostic factors in relation to racial disparity in advanced colorectal cancer survival. Clin Colorectal Cancer. (2013) 12:287–93. doi: 10.1016/j.clcc.2013.08.001
8. Wassira LN, Pinheiro PS, Symanowski J, Hansen A. Racial-ethnic colorectal cancer survival disparities in the mountain west region: the case of Blacks compared to Whites. Ethn Dis. (2013) 23:103–9.
9. Carethers JM, Murali B, Yang B, Doctolero RT, Tajima A, Basa R, et al. Influence of race on microsatellite instability and CD8+ T cell infiltration in colon cancer. PLoS ONE. (2014) 9:e100461. doi: 10.1371/journal.pone.0100461
10. Xicola RM, Gagnon M, Clark JR, Carroll T, Gao W, Fernandez C, et al. Excess of proximal microsatellite-stable colorectal cancer in African Americans from a multiethnic study. Clin. Cancer Res. (2014) 20:4962–70. doi: 10.1158/1078-0432.CCR-14-0353
11. Tawk R, Abner A, Ashford A, Brown CP. Differences in colorectal cancer outcomes by race and insurance. Int J Environ Res Public Health. (2015) 13:ijerph13010048. doi: 10.3390/ijerph13010048
12. Holowatyj AN, Ruterbusch JJ, Rozek LS, Cote ML, Stoffel EM. Racial/ethnic disparities in survival among patients with young-onset colorectal cancer. J Clin Oncol. (2016) 34:2148–56. doi: 10.1200/JCO.2015.65.0994
13. Pena SD, Di Pietro G, Fuchshuber-Moraes M, Genro JP, Hutz MH, Kehdy Fde S, et al. The genomic ancestry of individuals from different geographical regions of Brazil is more uniform than expected. PLoS ONE. (2011) 6:e17063. doi: 10.1371/journal.pone.0017063
14. Giolo SR, Soler JM, Greenway SC, Almeida MA, de Andrade M, Seidman JG, et al. Brazilian urban population genetic structure reveals a high degree of admixture. Eur J Hum Genet. (2012) 20:111–6. doi: 10.1038/ejhg.2011.144
15. Pereira R, Phillips C, Pinto N, Santos C, dos Santos SE, Amorim A, et al. Straightforward inference of ancestry and admixture proportions through ancestry-informative insertion deletion multiplexing. PLoS ONE. (2012) 7:e29684. doi: 10.1371/journal.pone.0029684
16. Manta FS, Pereira R, Caiafa A, Silva DA, Gusmao L, Carvalho EF. Analysis of genetic ancestry in the admixed Brazilian population from Rio de Janeiro using 46 autosomal ancestry-informative indel markers. Ann Hum Biol. (2013) 40:94–8. doi: 10.3109/03014460.2012.742138
17. Lima-Costa MF, Rodrigues LC, Barreto ML, Gouveia M, Horta BL, Mambrini J, et al. Genomic ancestry and ethnoracial self-classification based on 5,871 community-dwelling Brazilians (The Epigen Initiative). Sci Rep. (2015) 5:9812. doi: 10.1038/srep09812
18. Santos NP, Ribeiro-Rodrigues EM, Ribeiro-Dos-Santos AK, Pereira R, Gusmão L, Amorim A, et al. Assessing individual interethnic admixture and population substructure using a 48-insertion-deletion (INSEL) ancestry-informative marker (AIM) panel. Hum Mutat. (2010) 31:184–90. doi: 10.1002/humu.21159
19. Piazzolla LP, de Almeida RM, dos Santos AC, de Oliveira PG, da Silva EF, de Sousa JB. Does Age Influence Treatment and Oncological Outcomes in Individuals with Sporadic Colorectal Cancer? J Am Geriatr Soc. (2015) 63:2190–1. doi: 10.1111/jgs.13680
20. Dos Santos LV, Faria TM, Lima AB, Abdalla KC, de Moraes ED, Cruz MR, et al. Timing of adjuvant chemotherapy in colorectal cancer. Colorectal Dis. (2016) 18:871–6. doi: 10.1111/codi.13306
21. Rossi BM, Palmero EI, Lopez-Kostner F, Sarroca C, Vaccaro CA, Spirandelli F, et al. A survey of the clinicopathological and molecular characteristics of patients with suspected Lynch syndrome in Latin America. BMC Cancer. (2017) 17:623. doi: 10.1186/s12885-017-3599-4
22. Berardinelli GN, Scapulatempo-Neto C, Duraes R, Antonio de Oliveira M, Guimaraes D, Reis RM. Advantage of HSP110 (T17) marker inclusion for microsatellite instability (MSI) detection in colorectal cancer patients. Oncotarget. (2018) 9:28691–701. doi: 10.18632/oncotarget.25611
23. Pritchard JK, Stephens M, Donnelly P. Inference of population structure using multilocus genotype data. Genetics. (2000) 155:945–59.
24. Falush D, Stephens M, Pritchard JK. Inference of population structure using multilocus genotype data: dominant markers and null alleles. Mol Ecol Notes. (2007) 7:574–8. doi: 10.1111/j.1471-8286.2007.01758.x
25. Campanella NC, Berardinelli GN, Scapulatempo-Neto C, Viana D, Palmero EI, Pereira R, et al. Optimization of a pentaplex panel for MSI analysis without control DNA in a Brazilian population: correlation with ancestry markers. Eur J Hum Genet. (2014) 22:875–80. doi: 10.1038/ejhg.2013.256
26. Romanini C, Romero M, Salado Puerto M, Catelli L, Phillips C, Pereira R, et al. Ancestry informative markers: inference of ancestry in aged bone samples using an autosomal AIM-Indel multiplex. Foren Sci Int Genet. (2015) 16:58–63. doi: 10.1016/j.fsigen.2014.11.025
27. Leal LF, de Paula FE, De Marchi PL, de Souza Viana, Pinto GDJ, Carlos CD, et al. Mutational profile of Brazilian lung adenocarcinoma unveils association of EGFR mutations with high Asian ancestry and independent prognostic role of KRAS mutations. Sci Rep. (2019) 9:3209. doi: 10.1038/s41598-019-39965-x
28. Falush D, Stephens M, Pritchard JK. Inference of population structure using multilocus genotype data: linked loci and correlated allele frequencies. Genetics. (2003) 164:1567–87.
29. Hubisz MJ, Falush D, Stephens M, Pritchard JK. Inferring weak population structure with the assistance of sample group information. Mol Ecol Resour. (2009) 9:1322–32. doi: 10.1111/j.1755-0998.2009.02591.x
30. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. (2015) 65:5–29. doi: 10.3322/caac.21254
31. SEER. Surveillance, Epidemiology, and End Results Program. (2016). Available online at: www.seer.cancer.gov/ (accessed August 08, 2016).
32. Welch HG, Robertson DJ. Colorectal cancer on the decline–why screening can't explain it all. N Engl J Med. (2016) 374:1605–7. doi: 10.1056/NEJMp1600448
33. WHO. World Health Organization. (2020). Available online at: www.who.int (accessed 07, 2019).
34. Chen W, Zheng R, Baade PD, Zhang S, Zeng H, Bray F, et al. Cancer statistics in China, 2015. CA Cancer J Clin. (2016) 66:115–32. doi: 10.3322/caac.21338
35. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2017. CA Cancer J Clin. (2017) 67:7–30. doi: 10.3322/caac.21387
36. Vasen HF, Moslein G, Alonso A, Bernstein I, Bertario L, Blanco I, et al. Guidelines for the clinical management of Lynch syndrome (hereditary non-polyposis cancer). J Med Genet. (2007) 44:353–62. doi: 10.1136/jmg.2007.048991
37. Bellizzi AM, Frankel WL. Colorectal cancer due to deficiency in DNA mismatch repair function: a review. Adv Anat Pathol. (2009) 16:405–17. doi: 10.1097/PAP.0b013e3181bb6bdc
38. Center MM, Jemal A, Smith RA, Ward E. Worldwide variations in colorectal cancer. CA Cancer J Clin. (2009) 59:366–78. doi: 10.3322/caac.20038
39. American College of Gastroenterology (ACG) (2016). Available online at: http://gi.org/ (accessed 09, 2016).
40. Dienstmann R, Salazar R, Tabernero J. Personalizing colon cancer adjuvant therapy: selecting optimal treatments for individual patients. J Clin Oncol. (2015) 33:1787–96. doi: 10.1200/JCO.2014.60.0213
41. Twelves C, Wong A, Nowacki MP, Abt M, Burris H, Carrato A, et al. Capecitabine as adjuvant treatment for stage III colon cancer. N Engl J Med. (2005) 352:2696–704. doi: 10.1056/NEJMoa043116
42. Andre T, Boni C, Navarro M, Tabernero J, Hickish T, Topham C, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol. (2009) 27:3109–16. doi: 10.1200/JCO.2008.20.6771
43. Van Cutsem E, Labianca R, Bodoky G, Barone C, Aranda E, Nordlinger B, et al. Randomized phase III trial comparing biweekly infusional fluorouracil/leucovorin alone or with irinotecan in the adjuvant treatment of stage III colon cancer: PETACC-3. J Clin Oncol. (2009) 27:3117–25. doi: 10.1200/JCO.2008.21.6663
44. Sauer R, Liersch T, Merkel S, Fietkau R, Hohenberger W, Hess C, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. (2012) 30:1926–33. doi: 10.1200/JCO.2011.40.1836
45. European Society for Medical Oncology (ESMO) (2014). Available online at: http://www.esmo.org/.
46. Wang R, Wang MJ, Ping J. Clinicopathological features and survival outcomes of colorectal cancer in young versus elderly: a population-based cohort study of SEER 9 Registries data (1988-2011). Medicine. (2015) 94:e1402. doi: 10.1097/MD.0000000000001402
47. Rex DK, Johnson DA, Anderson JC, Schoenfeld PS, Burke CA, Inadomi JM, et al. American College of Gastroenterology guidelines for colorectal cancer screening 2009. Am J Gastroenterol. (2009) 104:739–50. doi: 10.1038/ajg.2009.104
48. Davis DM, Marcet JE, Frattini JC, Prather AD, Mateka JJ, Nfonsam VN. Is it time to lower the recommended screening age for colorectal cancer?” J Am Coll Surg. (2011) 213:352–61. doi: 10.1016/j.jamcollsurg.2011.04.033
49. Meza R, Jeon J, Renehan AG, Luebeck EG. Colorectal cancer incidence trends in the United States and United kingdom: evidence of right- to left-sided biological gradients with implications for screening. Cancer Res. (2010) 70:5419–29. doi: 10.1158/0008-5472.CAN-09-4417
50. Huang CW, Tsai HL, Huang MY, Huang CM, Yeh YS, Ma CJ, et al. Different clinicopathologic features and favorable outcomes of patients with stage III left-sided colon cancer. World J Surg Oncol. (2015) 13:257. doi: 10.1186/s12957-015-0640-4
51. Lee GH, Malietzis G, Askari A, Bernardo D, Al-Hassi HO, Clark SK. Is right-sided colon cancer different to left-sided colorectal cancer? - a systematic review Eur J Surg Oncol. (2015) 41:300–8. doi: 10.1016/j.ejso.2014.11.001
52. Loupakis F, Yang D, Yau L, Feng S, Cremolini C, Zhang W, et al. Primary tumor location as a prognostic factor in metastatic colorectal cancer. J Natl Cancer Inst. (2015) 107:dju427. doi: 10.1093/jnci/dju427
53. Price TJ, Beeke C, Ullah S, Padbury R, Maddern G, Roder D, et al. “Does the primary site of colorectal cancer impact outcomes for patients with metastatic disease?” Cancer. (2015) 121:830–5. doi: 10.1002/cncr.29129
54. Brenner H, Kloor M, Pox CP. Colorectal cancer. Lancet. (2014) 383:1490–502. doi: 10.1016/S0140-6736(13)61649-9
55. Lim SB, Yu CS, Jang SJ, Kim TW, Kim JH, Kim JC. Prognostic significance of lymphovascular invasion in sporadic colorectal cancer. Dis Colon Rectum. (2010) 53:377–84. doi: 10.1007/DCR.0b013e3181cf8ae5
56. Zhong J. W., Yang S. X., Chen RP, Zhou YH, Ye MS, et al. Prognostic value of lymphovascular invasion in patients with stage iii colorectal cancer: a retrospective study. Med Sci Monit. (2019) 25:6043–50. doi: 10.12659/MSM.918133
57. Rotimi CN, Jorde LB. Ancestry and disease in the age of genomic medicine. N Engl J Med. (2010) 363:1551–8. doi: 10.1056/NEJMra0911564
58. Ramos BR, D'Elia MP, Amador MA, Santos NP, Santos SEE, da Cruz Castelli, et al. Neither self-reported ethnicity nor declared family origin are reliable indicators of genomic ancestry. Genetica. (2016) 144:259–65. doi: 10.1007/s10709-016-9894-1
59. Yoon HH, Shi Q, Alberts SR, Goldberg RM, Thibodeau SN, Sargent DJ, et al. Racial differences in BRAF/KRAS mutation rates and survival in stage III colon cancer patients. J Natl. Cancer Inst. (2015) 107:djv186. doi: 10.1093/jnci/djv186
60. Coleman Wallace DA, Baltrus PT, Wallace TC, Blumenthal DS, Rust GS. Black white disparities in receiving a physician recommendation for colorectal cancer screening and reasons for not undergoing screening. J Health Care Poor Underserv. (2013) 24:1115–24. doi: 10.1353/hpu.2013.0132
61. Teng A, Lee DY, Cai J, Patel SS, Bilchik AJ, Goldfarb MR. Patterns and outcomes of colorectal cancer in adolescents and young adults. J Surg Res. (2016) 205:19–27. doi: 10.1016/j.jss.2016.05.036
62. Moura RR, Coelho AV, Balbino Vde Q, Crovella S, Brandao LA. Meta-analysis of Brazilian genetic admixture and comparison with other Latin America countries. Am J Hum Biol. (2015) 27:674–80. doi: 10.1002/ajhb.22714
63. Saloum de Neves Manta F, Pereira R, Vianna RA, Rodolfo Beuttenmuller de Araujo D, Leite Goes Gitai D, et al. Revisiting the genetic ancestry of Brazilians using autosomal AIM-Indels. PLoS ONE. (2013) 8:e75145. doi: 10.1371/journal.pone.0075145
64. Hernandez-Suarez G, Sanabria MC, Serrano M, Herran OF, Perez J, Plata JL, et al. Genetic ancestry is associated with colorectal adenomas and adenocarcinomas in Latino populations. Eur J Hum Genet. (2014) 22:1208–16. doi: 10.1038/ejhg.2013.310
65. Andrade RB, Amador MAT, Cavalcante GC, Leitao LPC, Fernandes MR, Modesto AAC, et al. Estimating Asian contribution to the Brazilian population: a new application of a validated set of 61 ancestry informative markers. G3. (2018) 8:3577–82. doi: 10.1534/g3.118.200650
66. IBGE (2016). Available online at: http://www.ibge.gov.br/ (accessed April 10, 2016).
Keywords: colorectal cancer, genetic ancestry, cancer outcome, colorectal cancer survival, prognostic factors
Citation: Durães RO, Berardinelli GN, da Costa AM, Scapulatempo-Neto C, Pereira R, Oliveira MA, Guimarães DP and Reis RM (2020) Role of Genetic Ancestry in 1,002 Brazilian Colorectal Cancer Patients From Barretos Cancer Hospital. Front. Oncol. 10:145. doi: 10.3389/fonc.2020.00145
Received: 05 September 2019; Accepted: 27 January 2020;
Published: 04 March 2020.
Edited by:
Maria Paula Curado, ACCamargo Cancer Center, BrazilReviewed by:
Hamidullah Khan, University of Wisconsin-Madison, United StatesCopyright © 2020 Durães, Berardinelli, da Costa, Scapulatempo-Neto, Pereira, Oliveira, Guimarães and Reis. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rui Manuel Reis, cnVpcmVpcy5oY2JAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.