
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 26 April 2019
Sec. Women's Cancer
Volume 9 - 2019 | https://doi.org/10.3389/fonc.2019.00303
This article is part of the Research Topic New Approaches to Classification and Diagnostic Prediction of Breast Cancers View all 18 articles
 Tomás Pascual1,2
Tomás Pascual1,2 Miguel Martin3,4,5
Miguel Martin3,4,5 Aranzazu Fernández-Martínez6Laia Paré1,2Emilio Alba4,5,7Álvaro Rodríguez-Lescure4,8Giuseppe Perrone9Javier Cortés10,11Serafín Morales12Ana Lluch4,5,13,14,15Ander Urruticoechea16Blanca González-Farré2,17Patricia Galván1Pedro Jares17Adela Rodriguez1
Aranzazu Fernández-Martínez6Laia Paré1,2Emilio Alba4,5,7Álvaro Rodríguez-Lescure4,8Giuseppe Perrone9Javier Cortés10,11Serafín Morales12Ana Lluch4,5,13,14,15Ander Urruticoechea16Blanca González-Farré2,17Patricia Galván1Pedro Jares17Adela Rodriguez1 Nuria Chic1Daniela Righi9Juan Miguel Cejalvo1Giuseppe Tonini9Barbara Adamo1
Nuria Chic1Daniela Righi9Juan Miguel Cejalvo1Giuseppe Tonini9Barbara Adamo1 Maria Vidal1Patricia Villagrasa2Montserrat Muñoz1
Maria Vidal1Patricia Villagrasa2Montserrat Muñoz1 Aleix Prat1,2*
Aleix Prat1,2*Background: In hormone receptor-positive (HR+)/HER2-negative breast cancer, the HER2-enriched and Basal-like intrinsic subtypes are associated with poor outcome, low response to anti-estrogen therapy and high response to chemotherapy. To date, no validated biomarker exists to identify both molecular entities other than gene expression.
Methods: PAM50 subtyping and immunohistochemical data were obtained from 8 independent studies of 1,416 HR+/HER2-negative early breast tumors. A non-luminal disease score (NOLUS) from 0 to 100, based on percentage of estrogen receptor (ER), progesterone receptor (PR) and Ki67 tumor cells, was derived in a combined cohort of 5 studies (training dataset) and tested in a combined cohort of 3 studies. The performance of NOLUS was estimated using Area Under the ROC Curve (AUC).
Results: In the training dataset (n = 903) and compared to luminal disease, non-luminal disease had lower percentage of ER-positive cells (median 65.2 vs. 86.2%, p < 0.01) and PR-positive cells (33.2 vs. 56.4%, p < 0.01) and higher percentage of Ki67-positive cells (18.2 vs. 13.1%, p = 0.01). A NOLUS formula was derived: −0.45*ER −0.28*PR +0.27*Ki67 + 73.02. The proportion of non-luminal tumors in NOLUS-positive (≥51.38) and NOLUS-negative (<51.38) groups was 52.6 and 8.7%, respectively. In the testing dataset (n = 514), NOLUS was found significantly associated with non-luminal disease (p < 0.01) with an AUC 0.902. The proportion of non-luminal tumors in NOLUS-positive and NOLUS-negative groups was 76.9% (56.4–91.0%) and 2.6% (1.4–4.5%), respectively. The sensitivity and specificity of the pre-specified cutoff was 59.3 and 98.7%, respectively.
Conclusions: In the absence of gene expression data, NOLUS can help identify non-luminal disease within HR+/HER2-negative breast cancer.
Gene expression profiling has had a considerable impact on our understanding of hormone receptor-positive (HR+)/HER2-negative breast cancer biology (1, 2). During the last decade, two intrinsic molecular subtypes within HR+/HER2-negative disease (i.e., Luminal A and Luminal B) have been identified and intensively studied (3–5). These studies have led to well-validated prognostic gene expression-based tests such as Prosigna (6), OncotypeDX (7), MammaPrint (8), Breast Cancer Index (9),and EndoPredict (10). The implementation of these 4 platforms in the clinical practice has been essential in order to identify a subset of Luminal A tumors that can safely spare (neo)adjuvant chemotherapy treatments because of their good prognostic (11–13).
At the same time, cumulative evidence from recent studies suggests that 5–30% of HR+/HER2-negative tumors are not Luminal A or B by gene expression and fall into the HER2-enriched (HER2-E) and Basal-like categories (14). From a clinical perspective, these non-luminal tumors have been associated with low estrogen dependency (15–17), high chemo-sensitivity (18–20), potential lower activity of CDK4/6 inhibitors (21, 22) and poor outcome in both early and the advanced/metastatic breast cancer (22–24). Thus, clinical utility of the identification of the two non-luminal subtypes within HR+/HER2-negative disease is now being pursued.
In this study, we sought to validate a simple pathology-based model to help clinicians and researchers identify non-luminal disease within HR+/HER2-negative breast cancer in the absence of gene expression data.
PAM50 gene expression and pathology-based data from 1,416 HR+/HER2-negative early breast tumors were obtained from 8 independent studies that are summarized in Table 1 (20, 25–30). The GEICAM/9906 is a phase III adjuvant trial in women with lymph node-positive disease that compared treatment with fluorouracil, epirubicin, and cyclophosphamide (FEC) or with FEC followed by weekly paclitaxel (FEC-P) (25). A total of 531 HR+/HER2-negative tumor samples were analyzed (26). SOLTI-1007 NeoEribulin trial is a neoadjuvant trial within HER2-negative breast cancer, where patients were treated with eribulin monotherapy for 4 cycles (20). A total of 93 HR+/HER2-negative baseline tumor samples were analyzed. Pre-operative endocrine treatment (PETx) cohort is a retrospective Spanish registry of 56 patients with HR+/HER2-negative disease treated with neoadjuvant endocrine therapy. From this study, baseline samples were analyzed (30). From GEICAM/2009-03_CONVERTHER, a study that aimed to compared pathology and gene expression data between primary and metastatic tumor samples, we obtained 50 HR+/HER2-negative primary tumor samples (28, 31). GEICAM/2012-09 is a prospective study of the Spanish Breast Cancer Research Group to characterize the impact of Prosigna assay in adjuvant treatment decision of postmenopausal patients with HR+/HER2-negative breast cancer without nodal involvement (27). A total of 174 primary tumor samples were included. Hospital Clinic of Barcelona (HCB) cohort is a consecutive series of 194 tumor samples where Prosigna has been performed as routine clinical care (29). Università Campus Bio-Medico di Roma (CBM) cohort is a consecutive series of 145 tumor samples where Prosigna has been performed as routine clinical care (29). Instituto de Investigación Biomédica de Málaga (IBIMA) cohort includes 180 HR+/HER2-negative baseline tumors treated with neoadjuvant chemotherapy as routine clinical practice (18).
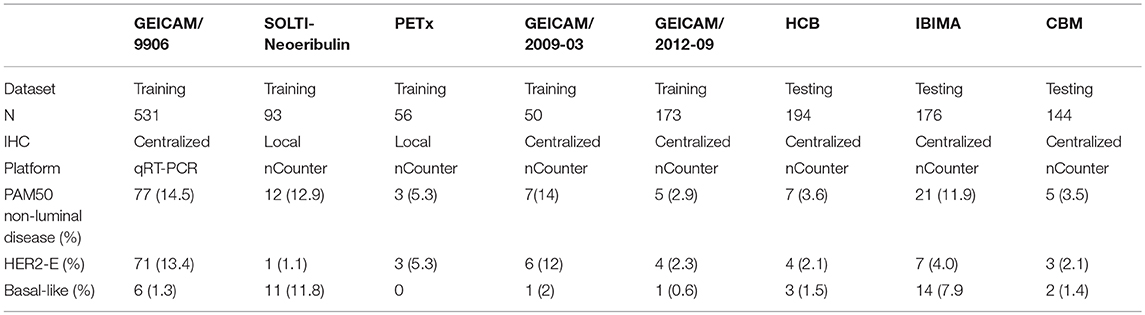
Table 1. Main features of the cohorts analyzed in this study.
The formalin-fixed paraffin-embedded tumor samples analyzed met the following criteria: (1) they were obtained from untreated primary tumors, (2) estrogen receptor (ER) and progesterone receptor (PR) positivity was defined as >1% positive tumor cells according to the ASCO/CAP guidelines (32), (3) HER2-negativity was defined according to the 2013 ASCO/CAP guidelines (33). Ki67 IHC was quantified according to the 2011 Guidelines developed by the International Ki67 in Breast Cancer working group (34).
A research-based PAM50 subtyping assay was performed using the nCounter as previously described (24, 35, 36), except in GEICAM/9906, where a research-based PAM50 qRT-PCR-based assay was used, and GEICAM/2012-09, HCB, IBIMA, and CBM datasets, which used the standardized and commercial version of the PAM50 assay (i.e., Prosigna®). Original subtype calls obtained from each study were used. From the research-based PAM50 version, we eliminated any tumor samples identified as normal-like.
A combined score to identify non-luminal disease by PAM50 was derived from a combined dataset of 5 studies (i.e., training dataset) using ER, PR, and Ki67 levels (i.e., % of positive tumor cells). The optimal cutoff was defined as the point with the most significant (Fisher's exact test) split between Luminal and non-Luminal disease. Once NOLUS was developed, the final model and cutoff were tested in 513 HR+/HER2-negative tumors (i.e., testing set) from 3 independent databases: HCB, IBIMA, and CBM studies.
Univariate and multivariable logistic regression analyses were done to investigate the association of each IHC biomarkers with non-luminal disease. Odds ratios (ORs) and 95% confidence intervals (CI) were calculated for each variable. The performance of NOLUS was estimated using Area Under the ROC Curve (AUC). 10-fold cross-validation was conducted (37). The significance level was set to a two-sided α of 0.05. We used R version 3.3.1 for all the statistical analyses.
A total of 903 HR+/HER2-negative tumor samples from 5 studies were used as the training dataset (Table 1). In this cohort, non-luminal subtypes represented 11.6% (105/903) of the cases, ranging from 2.9% in GEICAM/2012-09 to 14.5% in GEICAM/9906. As expected, a relationship between chemotherapy cohorts and higher proportion of non-luminal disease was found. The 3 chemotherapy cohorts had proportions of non-luminal disease >10%, whereas the 2 hormonotherapy cohorts, the Spanish neoadjuvant endocrine therapy registry (PETx) and the GEICAM/2012-09 prospective study, had 2.9 and 5.4% of non-luminal tumors, respectively.
ER, PR, and Ki67 were found differentially expressed (p < 0.001) between PAM50 luminal (n = 798) and non-luminal (n = 105) disease. Non-luminal disease had lower percentage of ER-positive cells (median 65.2 vs. 86.2%, p < 0.01) and PR-positive cells (33.2 vs. 56.4%, p < 0.01) and higher percentage of Ki67-positive cells (18.2 vs. 13.1%, p = 0.01) compared to luminal disease (Figure 1).
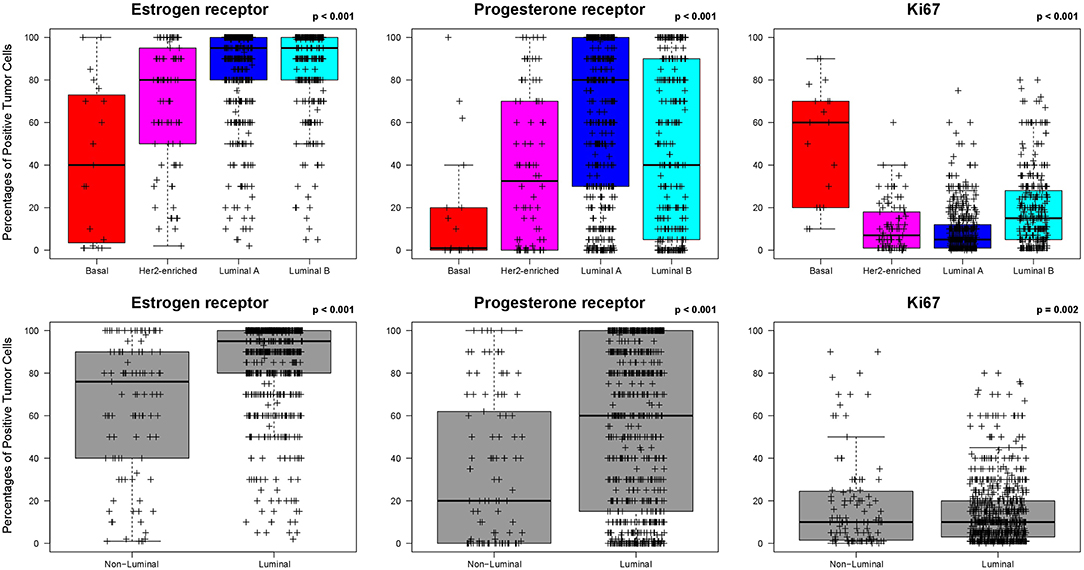
Figure 1. Levels of estrogen receptor (ER), progesterone receptor (PR) and Ki67-positive cells across the PAM50 intrinsic subtypes in HR+/HER2-negative breast cancer. Data was obtained from the training dataset.
To evaluate if ER, PR, and Ki67 (measured as continuous variables) provide independent information from each other regarding the identification of non-luminal disease, a multivariable logistic regression model was applied (Table S1). Interestingly, the expression of the 3 biomarkers was found independently associated with non-luminal disease. Using this multivariable result, we developed a combined score, called non-luminal disease score (NOLUS), that weights the value of each biomarker to identify non-luminal disease. The estimated coefficient of each variable in the logistic model was used to derive NOLUS (0–100) = −0.45*ER% −0.28*PR% + 0.27*Ki67% + 73, where ER, PR, and Ki67 are measured as continuous variables based on the percentage of positive tumor cells by immunohistochemistry.
Next, we identified a NOLUS cutoff to identify non-luminal disease based on the most significant split using a Fisher's exact test. Using this cutoff of 51.38, the proportion of NOLUS-positive (≥51.38) tumors and NOLUS-negative (<51.38) tumors was 6.3 and 93.7%, respectively. In addition, the proportion of non-luminal tumors in NOLUS-positive and NOLUS-negative groups was 52.6% (95% CI 38.9–66.0) and 8.7% (95 CI 6.97–10.77), respectively (p < 0.001) (Figure 2).
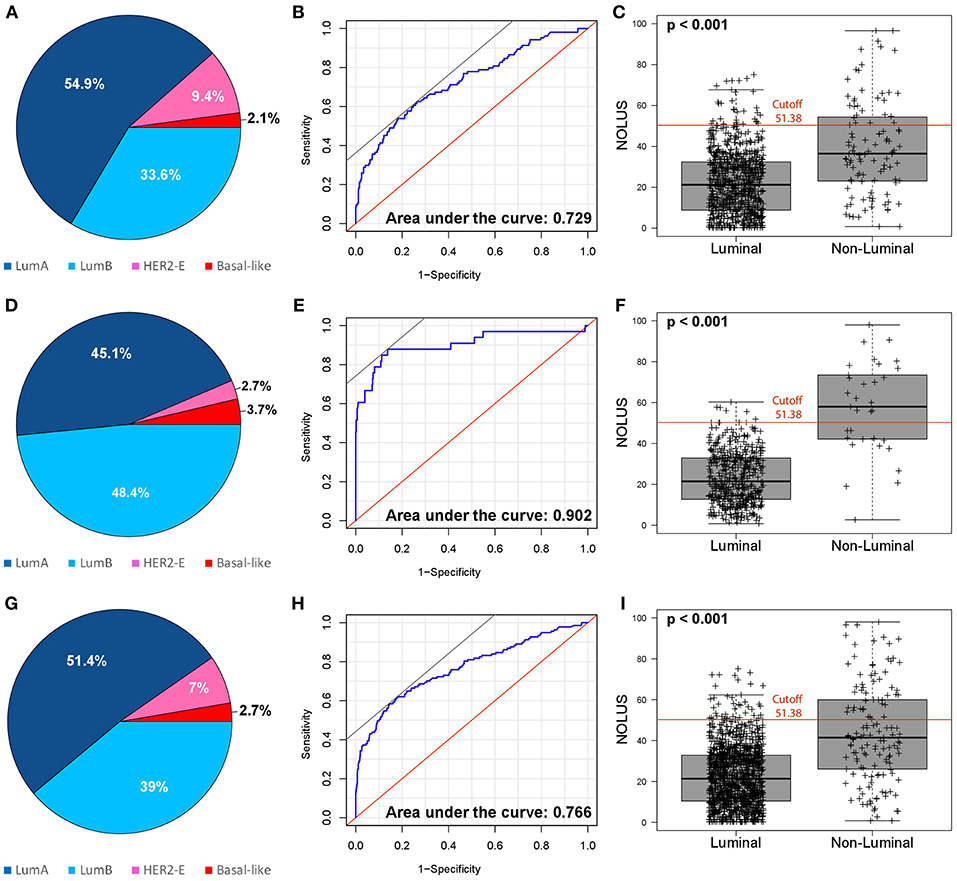
Figure 2. Performance of NOLUS score to predict non-luminal subtype. (A) Distribution of the intrinsic subtypes in the training dataset; (B) NOLUS score to predict non-luminal disease in the training dataset; (C) Expression of NOLUS in luminal vs. non-luminal tumors with the pre-specified cutoff in the training dataset; (D) Distribution of the intrinsic subtypes in testing dataset; (E) NOLUS score to predict non-luminal disease in the testing dataset; (F) Expression of NOLUS in luminal vs. non-luminal tumors with the pre-specified cutoff in the testing dataset; (G) Distribution of the intrinsic subtypes in all patients; (H) NOLUS score to predict non-luminal subtype in all patients; (I) Expression of NOLUS in luminal vs. non-luminal tumors with the pre-specified cutoff in all patients.
The testing dataset was composed of 514 HR+/HER2-negative tumor samples from 3 independent studies (HCB, IBIMA and CBM). The proportion of non-luminal disease here was 6.2% (33/514). NOLUS as a continuous variable was found significantly associated with non-luminal disease (p < 0.01) with an AUC 0.902 (Figure 2). The proportion of non-luminal tumors in NOLUS-positive and NOLUS-negative groups was 76.9% (56.4–91.0) and 2.6% (1.4–4.5), respectively (p < 0.01). The sensitivity was 59.3 and the specificity was 98.7%. To identify only HER2-E, the sensitivity was 42.8 and the specificity was 96.0%. To identify only Basal-like, the sensitivity was 53.9 and the specificity was 99.0%.
We explored NOLUS in all datasets combined. The odds of being non-luminal subtype increase 6.8% for every point increase (OR = 1.068, 95% CI 1.06–1.08, p < 0.001). The rates of non-luminal in NOLUS-negative and NOLUS-positive were 6.52 and 60.24%, respectively (Adjusted OR = 23.82, 95% CI 13.97–40.61, p < 0.001) (Figure 3).
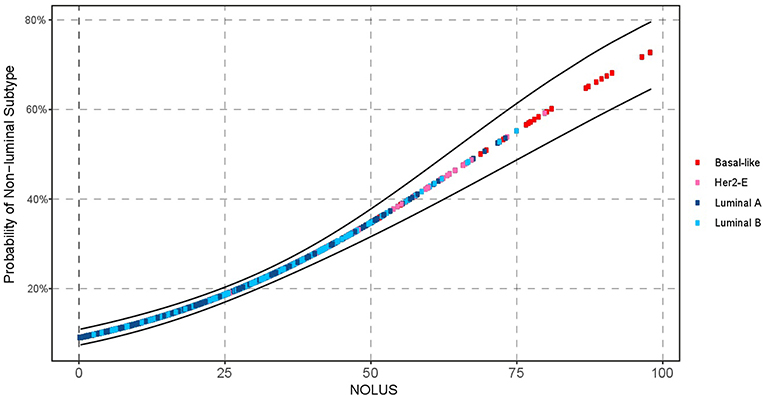
Figure 3. Probability of non-luminal disease as a function of NOLUS in all patients.
Finally, the model was validated using 10-fold cross validation. The data was separated into 10 sets, each set containing 10% of the data. For each validation round, 9 sets were used as training data, and the other set was used as testing data to validate the model using the linear discriminant analysis method. The accuracy of the model with 10-fold cross-validation was 0.97 (Cohen's kappa coefficient = 0.83).
In this study, we aimed to identify a pathology-based model that is easy, fast and with the potential to be widely implemented to identify non-luminal disease within HR+/HER2-negative breast cancer when gene expression data is not available. The main reasons are that there is accumulating evidence that non-luminal disease within HR+/HER2-negative disease represents a distinct biological and clinical entity (14) that deserves substantial attention and that gene expression-based assays are not always readily available in daily clinical practice. To our knowledge, this is the first report to attempt to derive a pathology-based predictive model to identify PAM50 non-luminal disease within HR+/HER2-negative disease.
The importance of intrinsic subtyping was highlighted in one of the most complete molecular characterization studies that has ever been performed in breast cancer (4). In this study, led by The Cancer Genome Atlas Project (TCGA), more than 500 primary breast cancer were extensively profiled at the DNA (i.e., methylation, chromosomal copy-number changes and somatic and germline mutations), RNA (i.e., miRNA and mRNA expression) and protein (i.e., protein and phosphor-protein expression) levels using the most recent technologies (4). In a particular analysis of over 300 primary tumors, 5 different data-types (i.e., all except DNA mutations) were combined together in a cluster of clusters in order to identify how many biological homogenous groups of tumors one can identify in breast cancer. The consensus clustering results showed the presence of 4 main entities of breast cancer but, more importantly, these 4 entities were found to be very-well recapitulated by the 4 main intrinsic subtypes (Luminal A, Luminal B, HER2-E, and Basal-like) as defined by mRNA expression only (3, 5, 6, 36, 38–40). Overall, these results suggest that intrinsic subtyping captures the vast majority of the biological diversity occurring in breast cancer.
Although the incidence of the Basal-like and HER2-E subtypes within HR+/HER2-negative tumors is below 10% in the primary disease setting (4), current evidence suggest that this frequency is much larger in the advanced/metastatic setting, specially following endocrine treatment (14). The increase proportion of the HER2-E subtype in the metastatic setting may be due to setting selection, a change in the biology of the tumor due to the inherent evolution of the tumor or the effects of the treatment, or a combination of both. Current evidence supports this latter possibility. Patients with early HR+/HER2-negative/HER2-E breast cancer have a higher probability of relapse than luminal disease. Therefore, it is likely that a given population of patients with metastatic disease is more enriched for the HER2-E subtype compared to patients with early breast cancer. Moreover, using 123 pairs of primary vs. metastatic tumor samples with a high proportion of HR+/HER2-negative tumors, Cejalvo et al. (28) showed that the HER2-E signature and HER2-E subtype are enriched in the metastatic samples compared to primary tumors. For example, 13% of primary Luminal A and B tumors were identified as HER2-E in the relapsed tumor sample. Overall, the proportion of HER2-E tumors in primary vs. metastatic was 11.4 vs. 22%, respectively. Moreover, in a retrospective analysis of tumor samples from the BOLERO-2 study, where patients with HR+/HER2-negative advanced disease resistant to an aromatase inhibitor, the proportion of HER2-E in primary vs. metastatic tumors was 19 vs. 32% (41). Recently, gene expression data from the PALOMA-2 clinical trial have been presented (21, 22). In this retrospective analysis, which included 68% (445/666) of the tumors of both primary and metastatic tumors within the clinical trial population, the HER2-E population represented 19 and the Basal-like population represented 1%.
The prognostic value of the Basal-like and HER2-E intrinsic subtypes in HR+/HER2-negative breast cancer has been evaluated in several studies (22–24). For example, intrinsic subtyping performed in a cohort of 1,380 patients with ER+ early breast cancer treated with 5 years of adjuvant tamoxifen-only (23) demonstrated the presence of a 7% of non-Luminal disease. These patients showed a statistically significant worse outcome compared to Luminal A subpopulation. The prognostic value of the HER2-E intrinsic subtype has been evaluated also in 3 retrospective studies involving HR+/HER2-negative metastatic patients (22, 24, 41). In the EGF30008 Phase III clinical trial, intrinsic subtyping was performed in a cohort of 821 patients with HR-positive disease (644 HER2-negative and 157 HER2+) treated in the first-line metastatic setting with either letrozole or letrozole plus lapatinib (24). Patients with HER2-E and Basal-like disease showed worse outcome in terms of progression free survival (PFS) and overall survival (OS) compared to Luminal A disease regardless of the HER2 status and treatment. Compared with the Luminal A subtype, the non-luminal subtypes showed a significantly decreased PFS independently of other clinical-pathological variables. Patients with HER2-E, and Basal-like subtypes had a 2.87, and 2.26 times higher risk of tumor progression, respectively. Median PFS differed across the intrinsic subtypes: Luminal A (16.9 months), Luminal B (11.0 months), HER2-E (4.7 months), and Basal-like (4.1 months). In the second study, PAM50 was performed in 261 tumor samples from the BOLERO-2 phase III trial (41). The subtype distribution was: 46.7% Luminal A, 21.5% HER2-negativeE, 15.7% Luminal B, 14.2% Normal-like and 1.9% Basal-like. Non-luminal disease was independently associated with poor PFS and OS compared to the luminal subtypes. In the third study, PAM50 was performed in 465 tumor samples from the PALOMA-2 phase III trial. Both non-luminal subtypes were associated with worse PFS compared to Luminal A subtype. These results support that non-luminal HR+/HER2-negative tumors are aggressive and require novel therapeutic approaches.
The ability of the Basal-like and HER2-E subtype to predict benefit from anti-estrogen therapy has been evaluated in the neoadjuvant setting. In the Z1031 neoadjuvant trial (16) within ER+/HER2-negative disease, patients with HER2-E or Basal-like disease had persistently high surgical Ki67 levels (20%) after 4–6 months of treatment with an aromatase inhibitor, consistent with high-level estrogen-independent growth. In another retrospective study of 112 postmenopausal women with stages I–IIIB ER+ early breast cancer before and after 2-weeks' anastrozole treatment in a neoadjuvant trial, patients with HER2-E subtype (n = 9 [8.0%]) or Basal-like subtype (n = 3 [2.7%]) showed a poorer Ki67 response (mean Ki-67 change of−50.7 and +15.3%) compared to Luminal A or B subtypes (mean Ki-67 change of−75%). Interestingly, this study also profiled post-treatment samples. As expected, the vast majority of Luminal A samples (31/32, 97%) continued being Luminal A. However, although the majority of Luminal B tumors became Luminal A (9/17, 53%), 12% (2/17) became HER2-E. Overall, this data, together with the poor PFS of the HER2-E subtype following endocrine therapy in EGF30008, BOLERO-2 and PALOMA 2 trials (22, 24, 41), suggest that both non-luminal subtypes within HR-positive disease might not benefit substantially from anti-estrogen therapy.
The ability of the Basal-like and HER2-E subtype to predict benefit from palbociclib has been recently evaluated in 465 samples of the PALOMA-2 study (22). The increase in median PFS in the HER2-E subtype was modest (2.8 months), compared to the increase in median PFS of 13.4 and 8.6 months in Luminal A and B subtypes, respectively. Regarding Basal-like, only 1 patient was identified and progressed at 6.4 months following letrozole plus palbociclib. This data suggest that non-luminal subtypes do not benefit much from CDK4/6 inhibition. In the neoadjuvant setting, Ma and colleagues conducted the NEOPALANA clinical trial with anastrozole and palbociclib. Two non-luminal tumors were identified by PAM50 (1 HER2-E and 1 Basal-like) and, interestingly, none of the 2 patients responded to the combined treatment (17).
The ability of the Basal-like and HER2-E subtype to predict chemotherapy sensitivity within HR+/HER2- disease has been evaluated in the neoadjuvant setting. In one study, we evaluated the pathological complete response (pCR) rated in 451 patients with HR+/HER2-negative disease treated with standard multi-agent neoadjuvant chemotherapy (42). The pCR rates in the non-luminal subtype was 23.2% compared to 15% in Luminal B and 5% in Luminal A tumors. In another neoadjuvant study, Prat and colleagues evaluated the residual cancer burden (RCB) 0/1 rates of the intrinsic subtypes in 180 patients with HR+/HER2-negative disease treated with anthracycline/taxane-based chemotherapy (18). Concordant with the first study, the RCB0/1 rates were higher in the non-luminal subtypes (38.1%) compared to Luminal B (20.0%) and Luminal A (9.3%). Overall, this data suggests that within HR+/HER2-negative disease, non-luminal tumors are highly chemo-sensitive.
Our study has several limitations worth noting. For example, determination of ER, PR and Ki67 was not performed centrally in a single lab and, in 2 studies, IHC data was obtained from local pathology reports. In addition, each study used different pathology-based assays. Although this heterogeneity is a limitation, its effects must not be large since the proportion of non-luminal disease across studies was similar and the fact that NOLUS was able to predict non-luminal disease in both the training and testing sets with similar performance. Another limitation is that NOLUS is not a standardized assay; thus, analytical validity is lacking. However, the biomarkers that compose NOLUS (i.e., ER, PR, and Ki67) have not been standardized; thus, NOLUS will suffer from lack of standardization as well. Another aspect is that we did not aim to derive a model that could further distinguish Basal-like from HER2-E subtypes within non-luminal disease. The main reason is that at this point it is unclear what are the clinical implications of each of these entities both from a prognostic and predictive point of view. However, as more data is gathered, NOLUS could be updated in the future to further distinguish these 2 non-luminal subtypes. Finally, we do not provide clinical validation of the NOLUS predictor.
To conclude, NOLUS is a tool that, in the absence of gene expression-based assays, may help identify non-luminal disease within HR+/HER2-negative breast cancer. Overall, the data clearly suggest that both non-luminal subtypes provide additional prognostic and predictive information beyond HR and HER2 status and may support more informed treatment decisions (1). For example, to identify patients who are not good candidates for endocrine therapy alone. Pivotal and large studies evaluating prognosis and treatment benefits can now apply NOLUS and further define the clinical validity and clinical utility of this biomarker.
All authors participated in the design and/or interpretation of the reported results and participated in the acquisition and/or analysis of data. In addition, all authors participated in drafting and/or revising the manuscript and provided administrative, technical, or supervisory support.
This work was supported by Instituto de Salud Carlos III - PI16/00904 (to AP), Banco Bilbao Vizcaya Argentaria Foundation (to AP), Pas a Pas (to AP), Save the Mama (to AP), Breast Cancer Research Foundation (to AP), Fundación Mutua Madrileña- Investigación en Salud 2018 (to AP), SEOM Translational Research Grant (to AF-M.), Banca d'Italia (to GP), and by T.C.I. telecomunicazioni (to GP).
AP reports consulting and lecture fees from Nanostring Technologies outside the submitted work. ÁR-L reports Clinical Research from Amgen, Astra Zeneca, Boehringer-Ingelheim, GSK, Novartis, Pfizer, Roche/Genentech, Eisai, Celgene, and Pierre Fabre and Advisory Boards and Consulting from Novartis, Pfizer, Roche/Genentech, Eisai, and Celgene, outside the submitted work. GP reports lecture fees from Nanostring Technologies and Clinical Research funds from Astrazeneca, outside the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank all the patients and their family members for participating in the studies.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2019.00303/full#supplementary-material
1. Prat A, Perou CM. Deconstructing the molecular portraits of breast cancer. Mol Oncol. (2011) 5:5–23. doi: 10.1016/j.molonc.2010.11.003
2. Prat A, Pineda E, Adamo B, Galvan P, Fernandez A, Gaba L, et al. Clinical implications of the intrinsic molecular subtypes of breast cancer. Breast. (2015) 24 (Suppl. 2):S26–35. doi: 10.1016/j.breast.2015.07.008
3. Prat A, Parker JS, Karginova O, Fan C, Livasy C, Herschkowitz JI, et al. Phenotypic and molecular characterization of the claudin-low intrinsic subtype of breast cancer. Breast Cancer Res. (2010) 12:R68. doi: 10.1186/bcr2635
4. Network CGA. Comprehensive molecular portraits of human breast tumours. Nature. (2012) 490:61. doi: 10.1038/nature11412
5. Prat A, Parker JS, Fan C, Perou CM. PAM50 assay and the three-gene model for identifying the major and clinically relevant molecular subtypes of breast cancer. Breast Cancer Res Treat. (2012) 135:301–6. doi: 10.1007/s10549-012-2143-0
6. Parker JS, Mullins M, Cheang MC, Leung S, Voduc D, Vickery T, et al. Supervised risk predictor of breast cancer based on intrinsic subtypes. J Clin Oncol. (2009) 27:1160–7. doi: 10.1200/JCO.2008.18.1370
7. Sparano JA, Gray RJ, Makower DF, Pritchard KI, Albain KS, Hayes DF, et al. Prospective Validation of a 21-Gene Expression Assay in Breast Cancer. N Engl J Med. (2015) 373:2005–14. doi: 10.1056/NEJMoa1510764
8. Cardoso F, Van't Veer LJ, Bogaerts J, Slaets L, Viale G, Delaloge S, et al. 70-Gene Signature as an Aid to treatment decisions in early-stage breast cancer. N Engl J Med. (2016) 375:717–29. doi: 10.1056/NEJMoa1602253
9. Sgroi DC, Sestak I, Cuzick J, Zhang Y, Schnabel CA, Schroeder B, et al. Prediction of late distant recurrence in patients with oestrogen-receptor-positive breast cancer: a prospective comparison of the breast-cancer index (BCI) assay, 21-gene recurrence score, and IHC4 in the TransATAC study population. Lancet Oncol. (2013) 14:1067–76. doi: 10.1016/S1470-2045(13)70387-5
10. Varga Z, Sinn P, Fritzsche F, Von Hochstetter A, Noske A, Schraml P, et al. Comparison of EndoPredict and Oncotype DX test results in hormone receptor positive invasive breast cancer. PLoS ONE. (2013) 8:e58483. doi: 10.1371/annotation/f715f38e-7aee-4d2b-8bbf-da0411dc6ef3
11. Dowsett M, Sestak I, Lopez-Knowles E, Sidhu K, Dunbier AK, Cowens JW, et al. Comparison of PAM50 risk of recurrence score with oncotype DX and IHC4 for predicting risk of distant recurrence after endocrine therapy. J Clin Oncol. (2013) 31:2783–90. doi: 10.1200/JCO.2012.46.1558
12. Gnant M, Filipits M, Greil R, Stoeger H, Rudas M, Bago-Horvath Z, et al. Predicting distant recurrence in receptor-positive breast cancer patients with limited clinicopathological risk: using the PAM50 Risk of Recurrence score in 1478 postmenopausal patients of the ABCSG-8 trial treated with adjuvant endocrine therapy alone. Ann Oncol. (2014) 25:339–45. doi: 10.1093/annonc/mdt494
13. Kwa M, Makris A, Esteva FJ. Clinical utility of gene-expression signatures in early stage breast cancer. Nat Rev Clin Oncol. (2017) 14:595–610. doi: 10.1038/nrclinonc.2017.74
14. Cejalvo JM, Pascual T, Fernandez-Martinez A, Braso-Maristany F, Gomis RR, Perou CM, et al. Clinical implications of the non-luminal intrinsic subtypes in hormone receptor-positive breast cancer. Cancer Treat Rev. (2018) 67:63–70. doi: 10.1016/j.ctrv.2018.04.015
15. Dunbier AK, Anderson H, Ghazoui Z, Salter J, Parker JS, Perou CM, et al. Association between breast cancer subtypes and response to neoadjuvant anastrozole. Steroids. (2011) 76:736–40. doi: 10.1016/j.steroids.2011.02.025
16. Ellis MJ, Suman VJ, Hoog J, Lin L, Snider J, Prat A, et al. Randomized phase II neoadjuvant comparison between letrozole, anastrozole, and exemestane for postmenopausal women with estrogen receptor-rich stage 2 to 3 breast cancer: clinical and biomarker outcomes and predictive value of the baseline PAM50-based intrinsic subtype–ACOSOG Z1031. J Clin Oncol. (2011) 29:2342–9. doi: 10.1200/JCO.2010.31.6950
17. Ma CX, Gao F, Luo J, Northfelt DW, Goetz M, Forero A, et al. NeoPalAna: Neoadjuvant Palbociclib, a Cyclin-Dependent Kinase 4/6 Inhibitor, and Anastrozole for Clinical Stage 2 or 3 Estrogen Receptor-Positive Breast Cancer. Clin Cancer Res. (2017) 23:4055–65. doi: 10.1158/1078-0432.CCR-16-3206
18. Prat A, Galvan P, Jimenez B, Buckingham W, Jeiranian HA, Schaper C, et al. Prediction of Response to Neoadjuvant Chemotherapy Using Core Needle Biopsy Samples with the Prosigna Assay. Clin Cancer Res. (2016) 22:560–6. doi: 10.1158/1078-0432.CCR-15-0630
19. Fujii T, Kogawa T, Dong W, Sahin AA, Moulder S, Litton JK, et al. Revisiting the definition of estrogen receptor positivity in HER2-negative primary breast cancer. Ann Oncol. (2017) 28:2420–8. doi: 10.1093/annonc/mdx397
20. Prat A, Ortega V, Villagrasa P, Paré L, Galván P, Oliveira M, et al. Abstract P1-09-09: efficacy and gene expression results from SOLTI1007 NEOERIBULIN phase II clinical trial in HER2-negative early breast cancer. Cancer Res. (2017) 77:P1-09-09. doi: 10.1158/1538-7445.SABCS16-P1-09-09
21. Finn RS, Martin M, Rugo HS, Jones S, Im S-A, Gelmon K, et al. Palbociclib and letrozole in advanced breast cancer. New Engl J Med. (2016) 375:1925–36. doi: 10.1056/NEJMoa1607303
22. Finn R, Liu Y, Martin M, Rugo H, Dieras V, Im S, et al. “Abstract P2-09-10: Comprehensive gene expression biomarker analysis of CDK 4/6 and endocrine pathways from the PALOMA-2 study”. Cancer Res. (2018) 78. doi: 10.1158/1538-7445.SABCS17-P2-09-10
23. Prat A, Parker JS, Fan C, Cheang MC, Miller LD, Bergh J, et al. Concordance among gene expression-based predictors for ER-positive breast cancer treated with adjuvant tamoxifen. Ann Oncol. (2012) 23:2866–73. doi: 10.1093/annonc/mds080
24. Prat A, Cheang MC, Galvan P, Nuciforo P, Pare L, Adamo B, et al. Prognostic value of intrinsic subtypes in hormone receptor-positive metastatic breast cancer treated with letrozole with or without lapatinib. JAMA Oncol. (2016) 2:1287–94. doi: 10.1001/jamaoncol.2016.0922
25. Martín M, Rodríguez-Lescure Á, Ruiz A, Alba E, Calvo L, Ruiz-Borrego M, et al. Randomized phase 3 trial of fluorouracil, epirubicin, and cyclophosphamide alone or followed by paclitaxel for early breast cancer. J Natl Cancer Inst. (2008) 100:805–14. doi: 10.1093/jnci/djn151
26. Martín M, Prat A, Rodríguez-Lescure Á, Caballero R, Ebbert MT, Munárriz B, et al. PAM50 proliferation score as a predictor of weekly paclitaxel benefit in breast cancer. Breast Cancer Res Treat. (2013) 138:457–66. doi: 10.1007/s10549-013-2416-2
27. Martín M, González-Rivera M, Morales S, De La Haba-Rodriguez J, González-Cortijo L, Manso L, et al. Prospective study of the impact of the Prosigna assay on adjuvant clinical decision-making in unselected patients with estrogen receptor positive, human epidermal growth factor receptor negative, node negative early-stage breast cancer. Curr Med Res Opin. (2015) 31:1129–37. doi: 10.1185/03007995.2015.1037730
28. Cejalvo JM, Martinez De Duenas E, Galvan P, Garcia-Recio S, Burgues Gasion O, Pare L, et al. Intrinsic subtypes and gene expression profiles in primary and metastatic breast cancer. Cancer Res. (2017) 77:2213–21. doi: 10.1158/0008-5472.CAN-16-2717
29. Fernandez-Martinez A, Pascual T, Perrone G, Morales S, De La Haba J, Gonzalez-Rivera M, et al. Limitations in predicting PAM50 intrinsic subtype and risk of relapse score with Ki67 in estrogen receptor-positive HER2-negative breast cancer. Oncotarget. (2017) 8:21930–7. doi: 10.18632/oncotarget.15748
30. Larburu L, Pare L, Rezola R, Carrera M, Buch E, Gimenez J, et al. Abstract P4-04-05: primary endocrine therapy (PETx) induces PAM50 intrinsic subtype migration with prognostic implications. Cancer Res. (2018) 78:P4-04-05. doi: 10.1158/1538-7445.SABCS17-P4-04-05
31. De Dueñas EM, Hernández AL, Zotano ÁG, Carrión RMP, López-Muñiz JIC, Novoa SA, et al. Prospective evaluation of the conversion rate in the receptor status between primary breast cancer and metastasis: results from the GEICAM 2009-03 ConvertHER study. Breast Cancer Res Treat. (2014) 143:507–15. doi: 10.1007/s10549-013-2825-2
32. Hammond MEH, Hayes DF, Dowsett M, Allred DC, Hagerty KL, Badve S, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer (unabridged version). Arch Pathol Lab Med. (2010) 134:e48–72. doi: 10.1043/1543-2165-134.7.e48
33. Wolff AC, Hammond MEH, Hicks DG, Dowsett M, Mcshane LM, Allison KH, et al. Recommendations for human epidermal growth factor receptor 2 testing in breast cancer: American Society of Clinical Oncology/College of American Pathologists clinical practice guideline update. Arch Pathol Lab Med. (2013) 138:241–56. doi: 10.1200/JCO.2013.50.9984
34. Dowsett M, Nielsen TO, A'hern R, Bartlett J, Coombes RC, Cuzick J, et al. Assessment of Ki67 in breast cancer: recommendations from the International Ki67 in Breast Cancer working group. J Natl Cancer Inst. (2011)103:1656–64. doi: 10.1093/jnci/djr393
35. Vidal M, Peg V, Galvan P, Tres A, Cortes J, Ramon Y Cajal S, et al. Gene expression-based classifications of fibroadenomas and phyllodes tumours of the breast. Mol Oncol. (2015) 9:1081–90. doi: 10.1016/j.molonc.2015.01.003
36. Llombart-Cussac A, Cortés J, Paré L, Galván P, Bermejo B, Martínez N, et al. HER2-enriched subtype as a predictor of pathological complete response following trastuzumab and lapatinib without chemotherapy in early-stage HER2-positive breast cancer (PAMELA): an open-label, single-group, multicentre, phase 2 trial. Lancet Oncol. (2017) 18:545–54. doi: 10.1016/S1470-2045(17)30021-9
37. Peters A. Improved predictors (2018) Available online at: http://www2.uaem.mx/r-mirror/web/packages/ipred/ipred.pdf
38. Cheang MC, Voduc KD, Tu D, Jiang S, Leung S, Chia SK, et al. Responsiveness of intrinsic subtypes to adjuvant anthracycline substitution in the NCIC.CTG MA.5 randomized trial. Clin Cancer Res. (2012) 18:2402–12. doi: 10.1158/1078-0432.CCR-11-2956
39. Prat A, Cheang MC, Martin M, Parker JS, Carrasco E, Caballero R, et al. Prognostic significance of progesterone receptor-positive tumor cells within immunohistochemically defined luminal A breast cancer. J Clin Oncol. (2013) 31:203–9. doi: 10.1200/JCO.2012.43.4134
40. Cheang MC, Martin M, Nielsen TO, Prat A, Voduc D, Rodriguez-Lescure A, et al. Defining breast cancer intrinsic subtypes by quantitative receptor expression. Oncologist. (2015) 20:474–82. doi: 10.1634/theoncologist.2014-0372
41. Prat A, Brase J, Cheng Y, Nuciforo P, Paré L, Pascual T, et al. PAM50 intrinsic subtype in hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2-) advanced breast cancer (ABC) treated with exemestane (EXE) in combination with everolimus (EVE) or placebo (PBO): A correlative analysis of the phase III BOLERO-2 trial. Eur J Cancer. (2018) 92:S117–8. doi: 10.1016/S0959-8049(18)30574-4
Keywords: intrinsic subtype, non-luminal, PAM50, breast cancer, gene expression
Citation: Pascual T, Martin M, Fernández-Martínez A, Paré L, Alba E, Rodríguez-Lescure Á, Perrone G, Cortés J, Morales S, Lluch A, Urruticoechea A, González-Farré B, Galván P, Jares P, Rodriguez A, Chic N, Righi D, Cejalvo JM, Tonini G, Adamo B, Vidal M, Villagrasa P, Muñoz M and Prat A (2019) A Pathology-Based Combined Model to Identify PAM50 Non-luminal Intrinsic Disease in Hormone Receptor-Positive HER2-Negative Breast Cancer. Front. Oncol. 9:303. doi: 10.3389/fonc.2019.00303
Received: 14 January 2019; Accepted: 02 April 2019;
Published: 26 April 2019.
Edited by:
Raquel Nunes, Johns Hopkins University, United StatesReviewed by:
Tomas Reinert, Federal University of Rio Grande do Sul, BrazilCopyright © 2019 Pascual, Martin, Fernández-Martínez, Paré, Alba, Rodríguez-Lescure, Perrone, Cortés, Morales, Lluch, Urruticoechea, González-Farré, Galván, Jares, Rodriguez, Chic, Righi, Cejalvo, Tonini, Adamo, Vidal, Villagrasa, Muñoz and Prat. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Aleix Prat, YWxwcmF0QGNsaW5pYy5jYXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.