
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Oncol. , 28 March 2019
Sec. Women's Cancer
Volume 9 - 2019 | https://doi.org/10.3389/fonc.2019.00193
This article is part of the Research Topic New Approaches to Classification and Diagnostic Prediction of Breast Cancers View all 18 articles
 Elisabet Cuyàs1,2†
Elisabet Cuyàs1,2† Maria Buxó2†Maria José Ferri Iglesias3
Maria Buxó2†Maria José Ferri Iglesias3 Sara Verdura1,2
Sara Verdura1,2 Sonia Pernas4Joan Dorca5Isabel Álvarez6,7Susana Martínez8Jose Manuel Pérez-Garcia9Norberto Batista-López10César A. Rodríguez-Sánchez11,12Kepa Amillano13Severina Domínguez14Maria Luque15Idoia Morilla4Agostina Stradella4Gemma Viñas5Javier Cortés16Jorge Joven17Joan Brunet5,18,19Eugeni López-Bonet20Margarita Garcia21Samiha Saidani22
Sonia Pernas4Joan Dorca5Isabel Álvarez6,7Susana Martínez8Jose Manuel Pérez-Garcia9Norberto Batista-López10César A. Rodríguez-Sánchez11,12Kepa Amillano13Severina Domínguez14Maria Luque15Idoia Morilla4Agostina Stradella4Gemma Viñas5Javier Cortés16Jorge Joven17Joan Brunet5,18,19Eugeni López-Bonet20Margarita Garcia21Samiha Saidani22 Xavier Queralt Moles3Begoña Martin-Castillo22*
Xavier Queralt Moles3Begoña Martin-Castillo22* Javier A. Menendez1,2*
Javier A. Menendez1,2*Background: The minor allele (C) of the single-nucleotide polymorphism (SNP) rs11212617, located near the ataxia telangiectasia mutated (ATM) gene, has been associated with an increased likelihood of treatment success with metformin in type 2 diabetes. We herein investigated whether the same SNP would predict clinical response to neoadjuvant metformin in women with early breast cancer (BC).
Methods: DNA was collected from 79 patients included in the intention-to-treat population of the METTEN study, a phase 2 clinical trial of HER2-positive BC patients randomized to receive either metformin combined with anthracycline/taxane-based chemotherapy and trastuzumab or equivalent regimen without metformin, before surgery. SNP rs11212617 genotyping was assessed using allelic discrimination by quantitative polymerase chain reaction.
Results: Logistic regression analyses revealed a significant relationship between the rs11212617 genotype and the ability of treatment arms to achieve a pathological complete response (pCR) in patients (odds ratio [OR]genotype×arm = 10.33, 95% confidence interval [CI]: 1.29–82.89, p = 0.028). In the metformin-containing arm, patients bearing the rs11212617 C allele had a significantly higher probability of pCR (ORA/C,C/C = 7.94, 95%CI: 1.60–39.42, p = 0.011). Conversely, no association was found between rs11212617 and clinical response in the reference arm (ORA/C,C/C = 0.77, 95%CI: 0.20–2.92, p = 0.700). After controlling for tumor size and hormone receptor status, the rs11212617 C allele remained a significant predictor of pCR solely in the metformin-containing arm.
Conclusions: If reproducible, the rs11212617 C allele might warrant consideration as a predictive clinical biomarker to inform the personalized use of metformin in BC patients.
Trial Registration: EU Clinical Trials Register, EudraCT number 2011-000490-30. Registered 28 February 2011, https://www.clinicaltrialsregister.eu/ctr-search/trial/2011-000490-30/ES.
The minor allele C of the noncoding single nucleotide polymorphism (SNP) rs11212617, which is located near the ataxia telangiectasia mutated (ATM) gene, was found to be associated with the metabolic response to the biguanide metformin in the first genome-wide association study (GWAS) carried out in 3,912 Europeans with type 2 diabetes (T2D) (1). Although lack of replication occurred in some studies aiming to verify the association between rs11212617 and the effect of metformin in multiple ethnic groups (2), a meta-analysis in smaller cohorts suggested that the rs11212617 C allele might be considered as the first robustly replicated common susceptibility locus associated with metformin treatment success in patients with T2D (3). Moreover, rs11212617 remained a top signal with no other genome-significant hits in a more recent GWAS of 13,123 participants of different ancestries, but failed to associate with glycemic response to metformin in a systematic three-stage replication study (4). However, rs11212617 has recently been shown to significantly affect not only the response to metformin in terms of insulin Z score, but also metformin plasma concentration (5). Mechanistic studies have shown that rs11212617 increases enhancer activity and could lead to elevated expression of several target genes including ATM itself (6). Yet, almost nothing is known about the impact of the rs11212617 C allele on the clinical efficacy of metformin in several ongoing clinical trials aiming to evaluate its potential benefits in a cancer setting (7).
A potential anti-cancer effect of metformin has gained considerable epidemiological and pre-clinical support over the last decade (7–10). First, a large number of population-based observational and cohort studies have suggested a cancer-preventive advantage associated with metformin usage among T2D patients (11). Second, diabetic patients with breast cancer receiving metformin during neoadjuvant chemotherapy were reported to benefit from a 3-fold greater pathological complete response (pCR) when compared with those who did not receive metformin (12). Third, an ever-growing number of pre-clinical studies have proposed numerous cell-autonomous (e.g., AMPK/mTOR-related) and non-cell-autonomous (e.g., insulin/IGF-1-related) molecular mechanisms that have enthusiastically endorsed the clinical development of metformin as a novel anti-cancer drug (13–15). However, one should acknowledge that a metformin-driven cancer-preventive advantage does not necessarily imply an effective therapeutic efficacy in non-diabetic patients with established cancers, and it remains unclear whether the adjuvant use of metformin in combination with standard cancer therapy could translate into better clinical outcomes (16–19). Indeed, recent randomized studies reporting the use of metformin in cancer treatment have yielded mixed results in patients with advanced disease (20, 21). Although the results of much larger randomized studies, such as NCIC CTG MA.32, the most advanced adjuvant trial investigating the effects of metformin vs. placebo on invasive disease-free survival and other outcomes on early breast cancer in 3,649 women (22), will be of great interest to confirm or reject the causal nature of the suggested correlation between metformin use and survival benefit in cancer patients, it is also true that companion biomarker studies are urgently needed to refine tumor and patient selection when using metformin as an adjuvant to established cancer therapeutics.
We herein investigated whether the presence of the rs11212617 C allele could predict the pathological complete response (pCR) in the METTEN study (23, 24), a randomized, open-label, multicenter, phase 2 trial of neoadjuvant metformin in combination with trastuzumab and chemotherapy in women with early HER2-positive breast cancer.
The METTEN study was registered with the EU Clinical Trials Register and is available online (https://www.clinicaltrialsregister.eu/ctr-search/trial/2011-000490-30/ES). Patients were randomly assigned to receive daily metformin (850 mg twice-daily) for 24 weeks concurrently with 12 cycles of weekly paclitaxel (80 mg/m2) plus trastuzumab (4 mg/kg loading dose followed by 2 mg/kg) followed by four cycles of 3 weekly fluorouracil (600 mg/m2), epirubicin (75 mg/m2), cyclophosphamide (600 mg/m2) with concomitant trastuzumab (6 mg/kg) (arm A), or equivalent sequential chemotherapy plus trastuzumab without metformin (arm B), followed by surgery. Patients had surgery within 4–5 weeks of the last cycle of neoadjuvant treatment (24). Post-surgery, patients received thrice-weekly trastuzumab to complete 1 year of neoadjuvant-adjuvant therapy. Genotyping of SNP rs11212617 was carried out in the intention-to-treat (ITT) population (n = 79), which included all randomly assigned patients who received at least one dose of study medication.
pCR was defined as absence of invasive tumor cells on hematoxylin and eosin evaluation of the complete resected breast specimen (and all sample regional lymph nodes if lymphadenectomy was performed) following the completion of neoadjuvant systemic therapy. Residual ductal carcinoma in situ (DCIS) only was included in the definition of pCR (ypT0/is, ypN0) (24).
Blood was drawn after an overnight fast. Serum glucose was measured in duplicate using the glucose oxidase method and serum insulin was measured in duplicate using the Human Insulin ELISA (Cat. # EZHI-14K, Merck Millipore, Billerica, MA). The lowest level of insulin that can be detected by this assay is 2 μU/mL when using a 20 μL sample size. Intra- and inter-assay coefficients of variation were below 6 and 11%, respectively. Fasting insulin resistance was calculated using the homeostasis model assessment (HOMA) using the following formula: HOMA-IR = fasting glucose (mmol/L) × fasting insulin (mU/L)/22.5.
The ATM rs11212617 SNP variants were determined using the 5′ exonuclease TaqMan-based allelic discrimination method (Applied Biosystems, assay ID C_134213_10).
Descriptive data were summarized using percentages, medians or means with their respective 25 and 75 percentiles or standard deviations as appropriate. Clinical baseline characteristics between groups (non-pCR and pCR) were assessed using Chi-square or Fisher's exact test for categorical variables, student t-test for continuous variables with normal distribution, or Mann-Whitney U test for non-normal distributions. The assumption of normality was evaluated with the Shapiro-Wilk test. Changes in glucose, insulin, and HOMA-IR between pre and post treatment were compared using the Wilcoxon test. The R package Hardy-Weinberg (http://www.jstatsoft.org/v64/i03/) was employed to check whether the Hardy-Weinberg equilibrium holds among study population. Binary logistic regression was used to assess the prognostic effect of baseline rs11212617 genotype on pCR. Unadjusted and adjusted odds ratios (ORs) with their relative 95% confidence intervals (CIs) were reported as a measure of association. All tests were 2- sided and P ≤ 0.05 was set as statistically significant. Statistical analyses were carried out using SPSS (IBM Corp. released 2017. IBM SPSS Statistics for Windows, Version 25.0; Armonk, NY) and STATA (StataCorp. 2013. Stata Statistical Software: Release 13; StataCorp LP, College Station, TX).
This study was designed to evaluate the clinical relevance of the SNP rs11212617 C allele with respect to its potential to predict a pCR in breast cancer patients with HER2 overexpression treated with metformin-containing neoadjuvant systemic therapy (Figure 1). We conducted the study with patients belonging to the ITT population of the METTEN trial, which included all randomly assigned patients who received at least one dose of study medication (n = 79) (24). A flowchart describing the formation of each cohort in the study is shown in Figure 1. The baseline characteristics of those ITT patients who achieved pCR after neoadjuvant therapy and those who did not are shown in Table 1. The comparison of clinical-pathological variables at diagnosis between patients of each non-pCR/pCR cohort revealed no significant differences, except for hormone receptor status. The non-pCR group tended to have more estrogen receptor-negative and/or progesterone-positive tumors (p = 0.056).
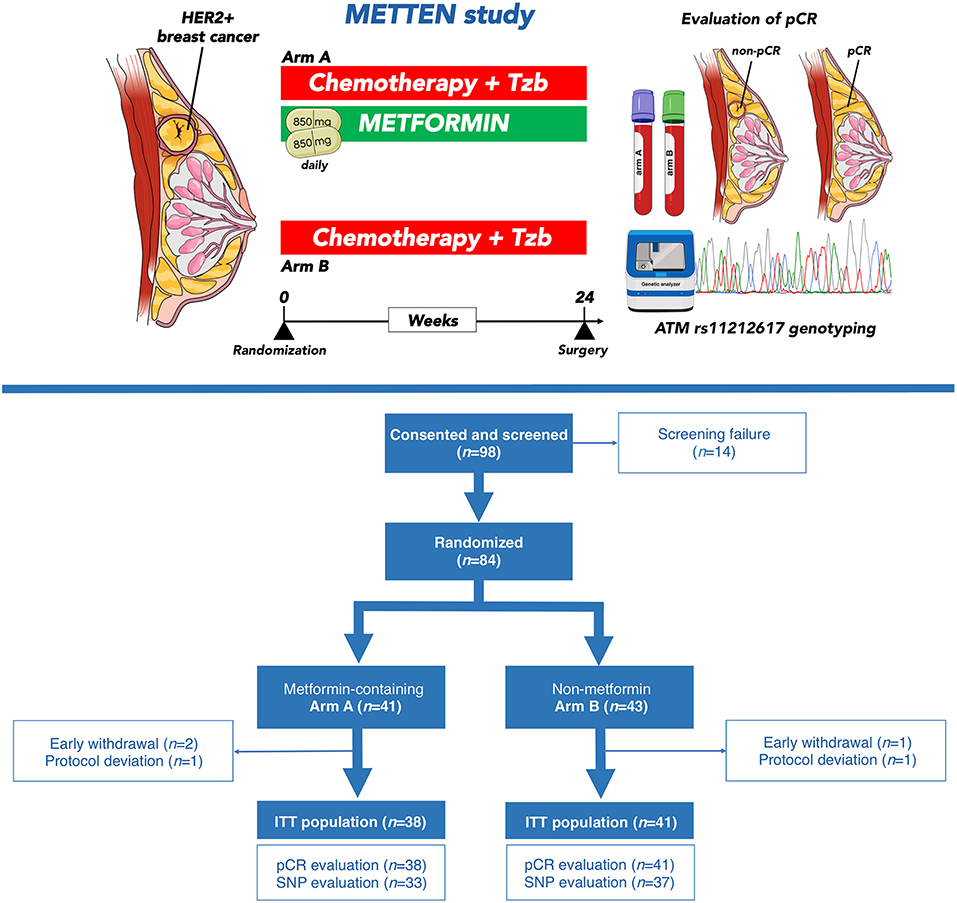
Figure 1. The METTEN study. (Top) The open-label, multicenter, phase II randomized METTEN study was designed to evaluate the clinical activity, tolerability, and safety of adding metformin to neoadjuvant chemotherapy plus trastuzumab in operable, locally advanced, or inflammatory HER2-positive BC (23, 24). Women with primary, non-metastatic HER2-positive BC were randomly assigned (1:1) to receive daily metformin (850 mg twice-daily) for 24 weeks concurrently with 12 cycles of weekly paclitaxel plus trastuzumab followed by four cycles of 3 weekly fluorouracil, epirubicin, cyclophosphamide plus trastuzumab (arm A) or equivalent sequential chemotherapy plus trastuzumab without metformin (arm B), followed by surgery. The primary end point was pCR, defined as absence of invasive tumor cells on hematoxylin and eosin evaluation of the complete resected breast specimen (and all sample regional lymph nodes if lymphadenectomy was performed) following the completion of neoadjuvant systemic therapy. Residual ductal carcinoma in situ (DCIS) only was included in the definition of pCR (ypT0/is, ypN0). Between June 1, 2012 and March 17, 2016, 98 patients at 10 centers in Spain were recruited into the METTEN study. DNA sample collection was not included in the original study design and was added as addendum #3 in April 2012 to re-consent patients for an additional blood draw for germ line DNA extraction. DNA samples from 70 patients (89% of the full ITT cohort) were subsequently collected and genotyped for SNP rs11212617. (Bottom) Modified CONSORT diagram showing the 70 cases of HER2-positive BC patients used for the analysis of clinical response analysis to neoadjuvant metformin by the minor allele C of the SNP rs11212617.
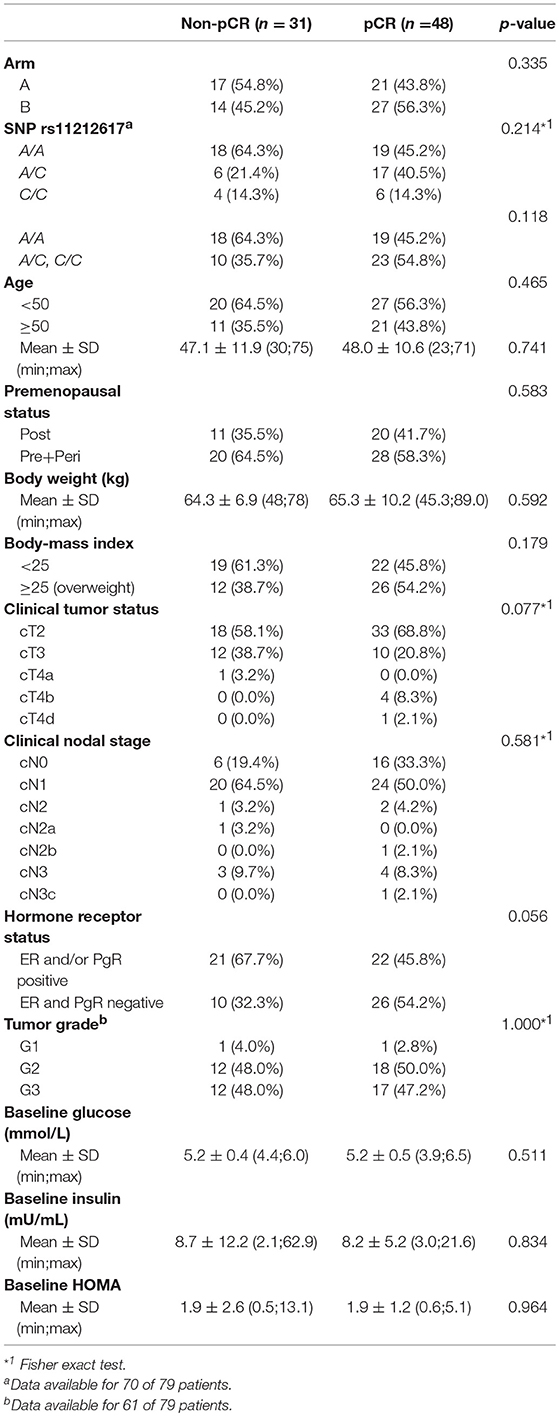
Table 1. Clinical characteristics of patients at baseline according to pathological complete response (pCR) status.
The rs11212617 polymorphism was evaluable in most of the patient samples, and 70 of 79 patients (89%) were genotyped (Figure 1, Table 2). The A and C allelic frequencies of rs11212617 in our patients were 69 and 31%, respectively. The frequencies of three genotypes in all the patients were 14.3% (C/C), 32.9% (A/C), and 52.9% (A/A). These genotype frequencies were very similar to those predicted by the Ensembl genome database for a Tuscany, in Italy (TSI) population, and slightly different to those observed in Europeans and the Iberian population in Spain (Table 2). Despite the small population size, there was no significant deviation in rs11212617 genotype frequencies in our population from the Hardy-Weinberg expectation [HWE; Sum Equally Likely or More Extreme [SELOME] p = 0.0879]. No significant differences were observed in the genotype frequencies of SNP rs11212617 between the non-pCR and pCR cohorts in the ITT population (Table 1).
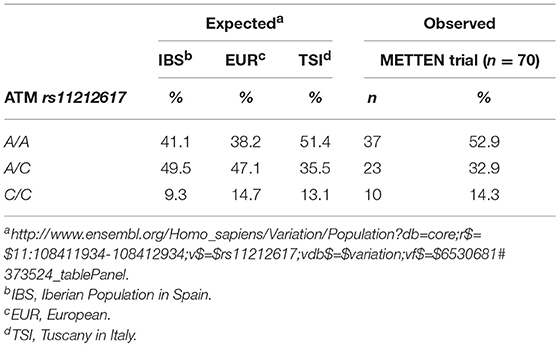
Table 2. Expected and observed SNP rs11212617 prevalence (%).
Frequency distributions of SNP rs11212617 were similar between treatment arms (Table S1). Of the patients in the metformin-containing arm A, 81.2% of homo or heterozygous patients for the rs11212617 C allele achieved a pCR, whereas 64.7% of non-carrier patients did not achieve a pCR (Figure 2, top panels). Of the patients in the reference arm B, 58.8% of homo or heterozygous patients for the rs11212617 C allele and 65% of non-carrier patients achieved a pCR, respectively (Figure 2, top panels). We employed logistic binary regression analyses to investigate the association between arm, ATM rs11212617 genotype, and pCR. In bivariate analysis, we failed to show predictive capacity of either the arm treatment or rs11212617 genotype with the probability of achieving pCR (Table S2). However, we observed a significant relationship between rs11212617 genotype and the ability of treatment arms to achieve pCR (ORgenotype×arm = 10.33, 95%CI: 1.29–82.89, p = 0.028; Table 3). This finding suggested that the direction and/or intensity of the relationship between rs11212617 genotype and pCR significantly varied in each treatment arm. Accordingly, the patients bearing the rs11212617 C allele in the metformin-containing arm had a significantly higher probability of pCR (ORA/C, C/C = 7.94, 95%CI: 1.60–39.42, p = 0.011; Figure 2, bottom panel). Conversely, no association was found between the presence of the rs11212617 C allele and clinical response in the (non-metformin) reference arm (ORA/C, C/C = 0.77, 95%CI: 0.20–2.92, p = 0.700; Figure 2, bottom panel). After additional adjusting for potential confounding tumor characteristics such as tumor size and hormone receptor (HR) status, a relationship between the rs11212617 genotype and the ability of treatment arms to achieve a pCR in patients remained significant (adjusted ORgenotype×arm = 20.53, 95%CI: 1.97–213.79, p = 0.011; Table S3). In the metformin-containing arm, the positive association between the presence of the rs11212617 C allele and pCR remained significant after accounting for tumor size and HR status (adjusted ORA/C, C/C = 28.88, 95%CI: 2.20–378.73, p = 0.010; Table S4). The lack of association between the rs11212617 C allele and pCR in the (non-metformin) reference arm was not altered after adjusting for these factors (Table S5).
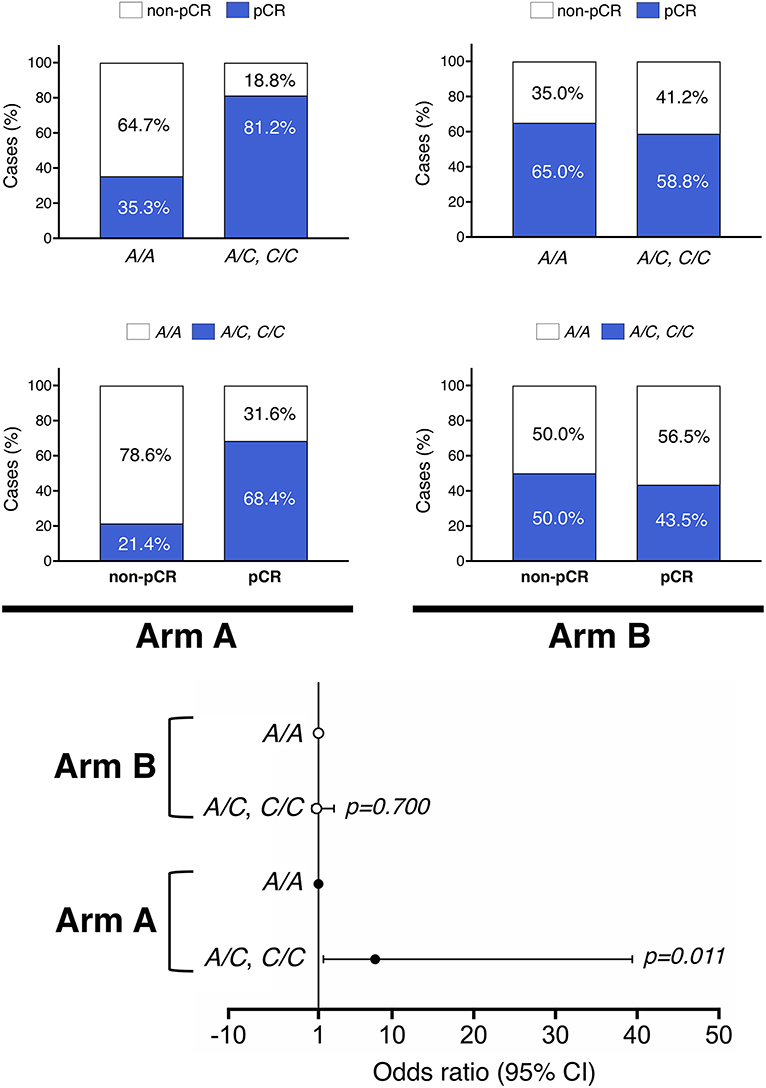
Figure 2. Association of ATM rs11212617 genotype and pCR by treatment arm. (Top) Rates of pCR stratified by the (C) rs11212617 genotype in patients randomized to receive either metformin combined with anthracycline/taxane-based chemotherapy and trastuzumab (arm A) or equivalent regimen without metformin (arm B). (Bottom) Relationship between the (C) rs11212617 genotype and the ability of treatment arms to achieve pCR.
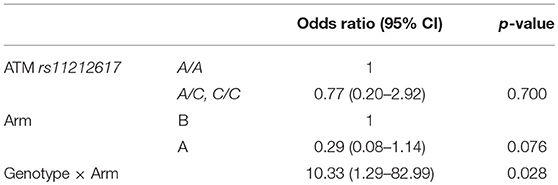
Table 3. Association of the interaction between ATM rs11212617 genotype and pCR by treatment arm.
A Wilcoxon test was conducted to evaluate whether there was a significant relationship between the rs11212617 C allele and the metabolic response to each arm. In the reference arm, no significant relationship between rs11212617 C allele and reductions in glucose, insulin, or HOMA-IR index was evident (Table 4). In the metformin arm, however, there was a near-significant trend between the rs11212617 C allele and the metabolic response to metformin in terms of insulin reduction (p = 0.069; Table 4).
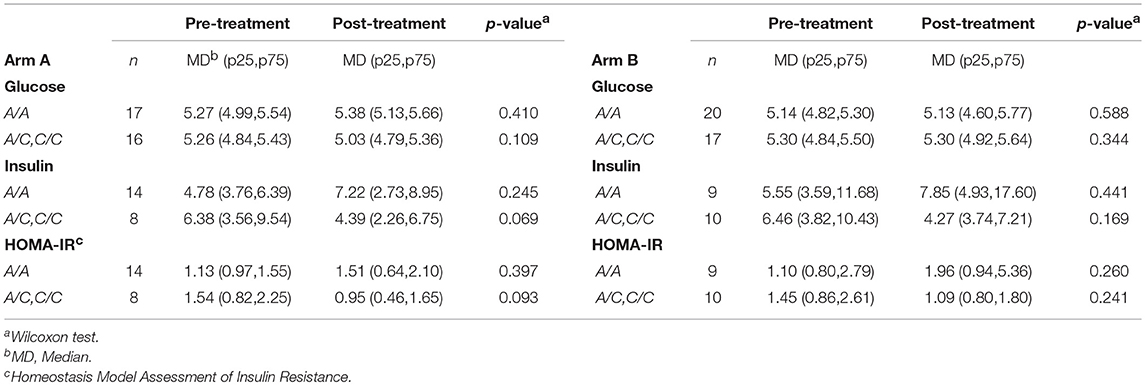
Table 4. Association of ATM rs11212617 genotype with changes in glucose, insulin, and HOMA-IR pre- and post-treatment.
A significant number of neoadjuvant, adjuvant, and advanced disease trials are currently ongoing or have been proposed to elucidate whether metformin, when used at doses established for diabetes control, has the potential to be used in preventive and treatment settings as an adjuvant to established cancer therapeutics. In this scenario, companion biomarker studies are urgently needed to define metformin efficacy and refine the tumor types and/or patient populations that are most likely to benefit from metformin-containing interventions.
To our knowledge, this is the first prospective study evaluating the relationship between the ATM SNP rs11212617 C allele, which has been associated with an increased likelihood of metformin treatment success in T2D (1, 3, 5), and the clinical benefit of adding metformin to well-established neoadjuvant treatment regimens in breast cancer patients. Logistic regression analyses revealed a significant relationship between the rs11212617 genotype and the ability of treatment arms to achieve a pCR. In the metformin-containing arm, patients bearing the rs11212617 C allele had a significantly higher probability of pCR. Conversely, no association was found between rs11212617 and clinical response in the reference arm. Because greater benefits from HER2-targeted neoadjuvant treatment in breast cancer are achieved in patients with small HR-negative tumors compared with patients with large HR-positive tumors (25), it is noteworthy that the capacity of the ATM rs11212617 C allele to predict a higher chance of achieving a pCR in patients treated with neoadjuvant metformin was not altered after accounting for factors like tumor size and HR status.
A previous report by Reni et al. (21) failed to observe any association between the C allele of rs11212617 and the clinical response to metformin in pancreatic cancer, but a significant relationship between the highest reduction of fasting plasma glucose and the CC genotype was observed. Our study suggests that the presence of the minor C allele of rs11212617 might associate with a significant improvement in insulin sensitivity in HER2-positive breast cancer patients subjected to neoadjuvant metformin in combination with trastuzumab and chemotherapy. This was evidenced by a near significant reduction of circulating insulin levels and HOMA-IR index—which fairly correlates with the insulin sensitivity index calculated using the minimal model approach (26), solely in those patients bearing SNP rs11212617 C allele in the metformin-containing arm despite maintenance of blood glucose levels.
Limitations of this study are inherent in the design; in particular, the open-label nature of the study, and a relatively modest sample size. Further, because a concurrent analysis of well-characterized breast cancer biomarkers relevant for the putative mechanism of metformin was not achievable, it might be argued that the outcome predicted by the “favorable” C allele could be partially biased. Cancer cells expressing constitutively active phosphatidylinositol-3 kinase (PI3K) are proliferative regardless of the absence of insulin, and they can form dietary restriction (DR)-resistant tumors in vivo (27). Accordingly, because the binding of insulin to its receptors activates the PI3K/AKT/mammalian target of rapamycin (mTOR) signaling cascade, activating mutations in the PIK3CA oncogene might be expected to determine tumor response to DR-like pharmacological strategies targeting the insulin and mTOR pathways (27, 28). In our hands, however, breast cancer xenografts harboring the insulin-unresponsive, DR-resistant, PIK3CA-activating mutation H1047R remained largely sensitive to the anti-tumoral effects of metformin (29). Given that new groundbreaking research has shown how dietary approaches such as carb-restricted ketogenic diets can prevent the systemic glucose-insulin feedback that impairs the efficacy of PI3K inhibitors (30), our current findings, together with the ability of metformin to significantly augment the circulating the levels of the ketone body beta-hydroxybutyrate in the metformin-containing arm of the METTEN study (manuscript in preparation), might have a significant impact on the design of future trials evaluating the potential of combining metformin with targeted therapy.
In summary, we have genotyped a subset of patients included in a neoadjuvant breast cancer trial to explore the effect of rs11212617 variants on the clinical endpoint pCR, a powerful predictor of long-term outcome of patients with HER2-positive disease treated with neoadjuvant therapy with or without HER2-targeted agents (31–33). The present findings, although limited by the small effect size, suggest that further analyses using a larger number of breast cancer patients treated with metformin should verify whether a pharmacogenomic profile including the analysis of ATM SNP rs11212617 genotype might deserve consideration as a predictive clinical biomarker to inform the personalized use of metformin in a cancer setting.
Association with a significantly augmented pCR rate was found in metformin-treated breast cancer patients that have a “favorable” C allele-containing ATM SNP rs11212617 genotype. Because achievement of pCR is an appropriate surrogate for significantly improved long-term clinical outcomes in high-risk breast cancer subtypes (34), future studies validating this association of favorable ATM rs11212617 genotype with improvements in relapse-free survival after surgery in the METTEN study (and retrospective outcome analyses for other clinical trials) should definitely determine whether the rs11212617 C allele may lead to actionable modifications for prospective clinical planning in metformin-based anti-breast cancer approaches.
The datasets generated and analyzed during the current study are available from the corresponding authors on reasonable request.
The hospital (Dr. Josep Trueta Hospital, Girona, Spain) ethics committee (Clinical Investigation Ethic Committee, CIEC) and independent institutional review boards at each site participating in the METTEN study approved the protocol and any amendments. All procedures were in accordance with the ethical standards of the institutional research committees and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all individual participants included in the study. The authors declared that they have no competing interests.
BM-C and JM: conceptualization, supervision, and funding acquisition; BM-C, MB, and JM: methodology; MB, JM, and EC: formal analysis and visualization; EC, SV, MF, SP, JD, IA, SM, JP-G, NB-L, CR-S, KA, SD, ML, AS, IM, GV, JC, and JJ: investigation; JB, EL-B, MG, SS, and XQ: resources; EC, SS, and MB: data curation; JM: writing-original draft preparation; JM, JP-G, EC, and BM-C: writing-review and editing; BM-C: project administration.
This work was supported by grants from the Ministerio de Sanidad, Servicios Sociales e Igualdad (EC10-125, Ayudas para el Fomento de la Investigación Clínica Independiente to BM-C). Work in the Menendez laboratory is supported by the Ministerio de Ciencia e Innovación [Grant SAF2016-80639-P, Plan Nacional de l+D+I, founded by the European Regional Development Fund (EU FEDER), Spain] and by an unrestricted research grant from the Fundació Oncolliga Girona (Lliga catalana d'ajuda al malalt de càncer, Girona).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The METTEN study was conceived and designed by BM-C and JM, and was sponsored by the Consortium for the Support of Biomedical Research Network (CAIBER) and the Catalan Institute of Oncology (ICO). The Unit of Clinical Research at the ICO in Girona and the Unit for Statistical and Methodological Assessment at the Girona Biomedical Research Institute (IDIBGI) were responsible for central data gathering and analysis. All authors had responsibility for the decision to submit for publication. The authors would like to thank Dr. Kenneth McCreath for editorial support.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2019.00193/full#supplementary-material
1. Zhou K, Bellenguez C, Spencer CC, Bennett AJ, Coleman RL, Tavendale R, et al. Common variants near ATM are associated with glycemic response to metformin in type 2 diabetes. Nat Genet. (2011) 43:117–20. doi: 10.1038/ng.735
2. Florez JC, Jablonski KA, Taylor A, Mather K, Horton E, White NH, et al. The C allele of ATM rs11212617 does not associate with metformin response in the Diabetes Prevention Program. Diabetes Care. (2012) 35:1864–7. doi: 10.2337/dc11-2301
3. van Leeuwen N, Nijpels G, Becker ML, Deshmukh H, Zhou K, Stricker BH, et al. A gene variant near ATM is significantly associated with metformin treatment response in type 2 diabetes: a replication and meta-analysis of five cohorts. Diabetologia. (2012) 55:1971–7. doi: 10.1007/s00125-012-2537-x
4. Zhou K, Yee SW, Seiser EL, van Leeuwen N, Tavendale R, Bennett AJ, et al. Variation in the glucose transporter gene SLC2A2 is associated with glycemic response to metformin. Nat Genet. (2016) 48:1055–9. doi: 10.1038/ng.3632
5. Out M, Becker ML, van Schaik RH, Lehert P, Stehouwer CD, Kooy A. A gene variant near ATM affects the response to metformin and metformin plasma levels: a post hoc analysis of an RCT. Pharmacogenomics. (2018) 19:715–26. doi: 10.2217/pgs-2018-0010
6. Luizon MR, Eckalbar WL, Wang Y, Jones SL, Smith RP, Laurance M, et al. Genomic characterization of metformin hepatic response. PLoS Genet. (2016) 12:e1006449. doi: 10.1371/journal.pgen.1006449
7. Chae YK, Arya A, Malecek MK, Shin DS, Carneiro B, Chandra S, et al. Repurposing metformin for cancer treatment: current clinical studies. Oncotarget. (2016) 7:40767–80. doi: 10.18632/oncotarget.8194
8. Gonzalez-Angulo AM, Meric-Bernstam F. Metformin: a therapeutic opportunity in breast cancer. Clin Cancer Res. (2010)16:1695–700. doi: 10.1158/1078-0432.CCR-09-1805
9. Thompson AM. Molecular pathways: preclinical models and clinical trials with metformin in breast cancer. Clin Cancer Res. (2014) 20:2508–15. doi: 10.1158/1078-0432.CCR-13-0354
10. Heckman-Stoddard BM, DeCensi A, Sahasrabuddhe VV, Ford LG. Repurposing metformin for the prevention of cáncer and cáncer recurrence. Diabetologia. (2017) 60:1639–47. doi: 10.1007/s00125-017-4372-6
11. Xu H, Chen K, Jia X, Tian Y, Dai Y, Li D, et al. Metformin use is associated with better survival of breast cáncer patients with diabetes: a meta-analysis. Oncologist. (2015) 20:1236–44. doi: 10.1634/theoncologist.2015-0096
12. Jiralerspong S, Palla SL, Giordano SH, Meric-Bernstam F, Liedtke C, Barnett CM, et al. Metformin and pathologic complete responses to neoadjuvant chemotherapy in diabetic patients with breast cancer. J Clin Oncol. (2009) 27:3297–302. doi: 10.1200/JCO.2009.19.6410
13. Goodwin PJ, Stambolic V, Lemieux J, Chen BE, Parulekar WR, Gelmon KA, et al. Evaluation of metformin in early breast cancer: a modification of the traditional paradigm for clinical testing of anti-cancer agents. Breast Cancer Res Treat. (2011) 126:215–20. doi: 10.1007/s10549-010-1224-1
14. Del Barco S, Vazquez-Martin A, Cufí S, Oliveras-Ferraros C, Bosch-Barrera J, Joven J, et al. Metformin: multi-faceted protection against cancer. Oncotarget. (2011) 2:896–917. doi: 10.18632/oncotarget.387
15. Foretz M, Guigas B, Bertrand L, Pollak M, Viollet B. Metformin: from mechanisms of action to therapies. Cell Metab. (2014) 20:953–66. doi: 10.1016/j.cmet.2014.09.018
16. Dowling RJ, Goodwin PJ, Stambolic V. Understanding the benefit of metformin use in cancer treatment. BMC Med. (2011) 9:33. doi: 10.1186/1741-7015-9-33
17. Dowling RJ, Niraula S, Stambolic V, Goodwin PJ. Metformin in cancer: translational challenges. J Mol Endocrinol. (2012) 48:R31–43. doi: 10.1530/JME-12-0007
18. Chandel NS, Avizonis D, Reczek CR, Weinberg SE, Menz S, Neuhaus R, et al. Are metformin doses used in murine cancer models clinically relevant? Cell Metab. (2016) 23:569–70. doi: 10.1016/j.cmet.2016.03.010
19. Menendez JA, Martin-Castillo B, Joven J. Metformin and cancer: Quo vadis et cui bono? Oncotarget. (2016) 7:54096–101. doi: 10.18632/oncotarget.10262
20. Kordes S, Pollak MN, Zwinderman AH, Mathôt RA, Weterman MJ, Beeker A, et al. Metformin in patients with advanced pancreatic cancer: a double-blind. randomised. placebo-controlled phase 2 trial. Lancet Oncol. (2015) 16:839–47. doi: 10.1016/S1470-2045(15)00027-3
21. Reni M, Dugnani E, Cereda S, Belli C, Balzano G, Nicoletti R, et al. (Ir)relevance of metformin treatment in patients with metastatic pancreatic cancer: an open-label. randomized phase II trial. Clin Cancer Res. (2016) 22:1076–85. doi: 10.1158/1078-0432.CCR-15-1722
22. Goodwin PJ, Parulekar WR, Gelmon KA, Shepherd LE, Ligibel JA, Hershman DL, et al. Effect of metformin vs placebo on and metabolic factors in NCIC CTG MA.32. J Natl Cancer Inst. (2015) 107:djv006. doi: 10.1093/jnci/djv006
23. Martin-Castillo B, Dorca J, Vazquez-Martin A, Oliveras-Ferraros C, Lopez-Bonet E, Garcia M, et al. Incorporating the antidiabetic drug metformin in HER2-positive breast cancer treated with neo-adjuvant chemotherapy and trastuzumab: an ongoing clinical-translational research experience at the Catalan Institute of Oncology. Ann Oncol. (2010) 21:187–9. doi: 10.1093/annonc/mdp494
24. Martin-Castillo B, Pernas S, Dorca J, Álvarez I, Martínez S, Pérez-Garcia JM, et al. A phase 2 trial of neoadjuvant metformin in combination with trastuzumab and chemotherapy in women with early HER2-positive breast cancer: the METTEN Study. Oncotarget. (2018) 9:35687–704. doi: 10.18632/oncotarget.26286.
25. Zhao B, Zhao H. Impact of clinicopathological characteristics on the efficacy of neoadjuvant therapy in patients with human epidermal growth factor receptor-2-positive breast cancer. Int J Cancer. (2018) 142:844–53. doi: 10.1002/ijc.31097
26. Fernandez-Real JM, Pugeat M, Grasa M, Broch M, Vendrell J, Brun J, et al. Serum corticosteroid-binding globulin concentration and insulin resistance syndrome: a population study. J Clin Endocrinol Metab. (2002) 87:4686–90. doi: 10.1210/jc.2001-011843
27. Kalaany NY, Sabatini DM. Tumours with PI3K activation are resistant to dietary restriction. Nature. (2009) 458:725–31. doi: 10.1038/nature07782
29. Cufí S, Corominas-Faja B, Lopez-Bonet E, Bonavia R, Pernas S, López IÁ, et al. Dietary restriction-resistant human tumors harboring the PIK3CA-activating mutation H1047R are sensitive to metformin. Oncotarget. (2013) 4:1484–95. doi: 10.18632/oncotarget.1234
30. Hopkins BD, Pauli C, Du X, Wang DG, Li X, Wu D, et al. Suppression of insulin Feedback enhances the efficacy of PI3K inhibitors. Nature. (2018) 560:499–503. doi: 10.1038/s41586-018-0343-4
31. Cortazar P, Zhang L, Untch M, Mehta K, Costantino JP, Wolmark N, et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet. (2014) 384:164–72. doi: 10.1016/S0140-6736(13)62422-8
32. Broglio KR, Quintana M, Foster M, Olinger M, McGlothlin A, Berry SM, et al. Association of pathologic complete response to neoadjuvant therapy in HER2-positive breast cancer with long-term outcomes: a meta-analysis. JAMA Oncol. (2016) 2:751–60. doi: 10.1001/jamaoncol.2015.6113
33. Untch M, von Minckwitz G, Gerber B, Schem C, Rezai M, Fasching PA, et al. Survival analysis after neoadjuvant chemotherapy with trastuzumab or lapatinib in patients with human epidermal growth factor receptor 2-positive breast cancer in the GeparQuinto (G5) Study (GBG 44). J Clin Oncol. (2018) 36:1308–16. doi: 10.1200/JCO.2017.75.9175
Keywords: metformin, breast cancer, neoadjuvancy, HER2, ATM, rs11212617
Citation: Cuyàs E, Buxó M, Ferri Iglesias MJ, Verdura S, Pernas S, Dorca J, Álvarez I, Martínez S, Pérez-Garcia JM, Batista-López N, Rodríguez-Sánchez CA, Amillano K, Domínguez S, Luque M, Morilla I, Stradella A, Viñas G, Cortés J, Joven J, Brunet J, López-Bonet E, Garcia M, Saidani S, Queralt Moles X, Martin-Castillo B and Menendez JA (2019) The C Allele of ATM rs11212617 Associates With Higher Pathological Complete Remission Rate in Breast Cancer Patients Treated With Neoadjuvant Metformin. Front. Oncol. 9:193. doi: 10.3389/fonc.2019.00193
Received: 18 December 2018; Accepted: 06 March 2019;
Published: 28 March 2019.
Edited by:
Aleix Prat, Hospital Clínic de Barcelona, SpainReviewed by:
Tarah Ballinger, Indiana University, Purdue University Indianapolis, United StatesCopyright © 2019 Cuyàs, Buxó, Ferri Iglesias, Verdura, Pernas, Dorca, Álvarez, Martínez, Pérez-Garcia, Batista-López, Rodríguez-Sánchez, Amillano, Domínguez, Luque, Morilla, Stradella, Viñas, Cortés, Joven, Brunet, López-Bonet, Garcia, Saidani, Queralt Moles, Martin-Castillo and Menendez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Begoña Martin-Castillo, Ym1hcnRpbkBpY29uY29sb2dpYS5uZXQ=
Javier A. Menendez, am1lbmVuZGV6QGljb25jb2xvZ2lhLm5ldA==; am1lbmVuZGV6QGlkaWJnaS5vcmc=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.