
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
DATA REPORT article
Front. Oncol. , 31 October 2018
Sec. Cancer Genetics
Volume 8 - 2018 | https://doi.org/10.3389/fonc.2018.00490
This article is part of the Research Topic Accomplishments, Collaborative Projects and Future Initiatives in Breast Cancer Genetic Predisposition View all 13 articles
 Fabienne Lesueur1*
Fabienne Lesueur1* Noura Mebirouk1
Noura Mebirouk1 Yue Jiao2Laure Barjhoux3Muriel Belotti2Maïté Laurent2Mélanie Léone4Claude Houdayer2Brigitte Bressac-de Paillerets5
Yue Jiao2Laure Barjhoux3Muriel Belotti2Maïté Laurent2Mélanie Léone4Claude Houdayer2Brigitte Bressac-de Paillerets5 Dominique Vaur6Hagay Sobol7Catherine Noguès7Michel Longy8Isabelle Mortemousque9Sandra Fert-Ferrer10Emmanuelle Mouret-Fourme2Pascal Pujol11Laurence Venat-Bouvet12Yves-Jean Bignon13Dominique Leroux14Isabelle Coupier11Pascaline Berthet6Véronique Mari15Capucine Delnatte16Paul Gesta17Marie-Agnès Collonge-Rame18Sophie Giraud4Valérie Bonadona19,20Amandine Baurand21Laurence Faivre21Bruno Buecher2Christine Lasset19,20Marion Gauthier-Villars2Francesca Damiola3Sylvie Mazoyer22
Dominique Vaur6Hagay Sobol7Catherine Noguès7Michel Longy8Isabelle Mortemousque9Sandra Fert-Ferrer10Emmanuelle Mouret-Fourme2Pascal Pujol11Laurence Venat-Bouvet12Yves-Jean Bignon13Dominique Leroux14Isabelle Coupier11Pascaline Berthet6Véronique Mari15Capucine Delnatte16Paul Gesta17Marie-Agnès Collonge-Rame18Sophie Giraud4Valérie Bonadona19,20Amandine Baurand21Laurence Faivre21Bruno Buecher2Christine Lasset19,20Marion Gauthier-Villars2Francesca Damiola3Sylvie Mazoyer22 Sandrine M. Caputo2
Sandrine M. Caputo2 Nadine Andrieu1Dominique Stoppa-Lyonnet2,23 and GEMO Study Collaborators
Nadine Andrieu1Dominique Stoppa-Lyonnet2,23 and GEMO Study CollaboratorsWomen carrying a pathogenic variant (PV) in the BRCA1 or BRCA2 (BRCA1/2) genes are at high lifetime risk of developing breast cancer (BC) and ovarian cancer (OC), but estimation of the cumulative risk of cancer to age 70 years varies substantially between studies and populations. Initial estimations were obtained from selected high-risk families with multiple cases, such as those ascertained through the Breast Cancer Linkage Consortium used to identify disease loci (1). In the first retrospective studies conducted on such families, estimates for BC ranged from 40 to 87% for BRCA1 PV carriers and from 27 to 84% for BRCA2 PV carriers and estimates for OC ranged from 16 to 68% for BRCA1 PV carriers and from 11 to 27% for BRCA2 PV carriers (1–4). Recently, the largest prospective cohort conducted to date reported cumulative risks of BC to age 80 years of 72% for BRCA1 PV carriers and 69% for BRCA2 PV carriers (5). In the same study, cumulative risks of OC to age 80 years were 44% for BRCA1 PV carriers and 17% for BRCA2 PV carriers. Variation in cancer risks within or between BRCA1/2 families, with respect to age at diagnosis or type of cancer, can be explained by other genetic factors and/or lifestyle and reproductive factors (6–10). Genome-wide association studies (GWAS) conducted by the Breast Cancer Association Consortium (BCAC) have identified 172 common single-nucleotide polymorphisms (SNPs) associated with small increases in breast and/or ovarian cancer risk in the general population (11). A subset of these SNPs modifies the risk of breast and ovarian cancer risk for BRCA1/2 PV carriers (12–14) but most of the variability has not been explained yet (15). Breast and ovarian cancer risks in BRCA1/2 PV carriers might also vary according to the location of the variant and/or its origin (14, 16–19).
Genetic testing for BRCA1 and BRCA2 has been part of genetic counseling in European Union countries and North America since their discovery in the 90's, and has greatly improved recommendations about clinical management options and the most appropriate treatments. Nonetheless, both retrospective and prospective studies on large datasets of BRCA1/2 PV carrier families are still very much needed to refine individual cancer risk estimates by considering other genetic and lifestyle/environmental factors, and they will also contribute to a better understanding of the correlation between mutant BRCA1/2 alleles and phenotype. In particular, accurate age-specific risk estimates for the different types of cancer would be useful when choosing risk reduction strategies such as prophylactic bilateral mastectomy or salphingo-oophorectomy.
The Genetic Modifiers of BRCA1 and BRCA2 (GEMO) Group is the French multidisciplinary, collaborative framework for the investigation of genetic factors modifying cancer risk in Hereditary Breast and Ovarian cancer (HBOC) families segregating BRCA1/2 PVs. Its primary aims are to contribute to large-scale national and international projects to identify genetic modifiers and to facilitate the translation of research results to the clinical setting. This is achieved by establishing a resource of blood DNA samples from individuals carrying a PV together with family and clinical data through the nation-wide network of cancer genetic clinics. Here we report on the progress of the GEMO study, the characteristics of the 5,303 actual participants and the prevalence and spectrum of BRCA1/2 cancer-associated variants identified so far.
GEMO investigators include molecular geneticists, clinicians, genetic counselors, and epidemiologists who are involved in the Genetic and Cancer Group (GGC), a consortium with support of UNICANCER whose objectives are to define optimal testing practices both in terms of genetic counseling and laboratory techniques, and to contribute to the estimation of individual's cancer risks (http://www.unicancer.fr/en/cancer-and-genetic-group). GGC has contributed to the national development of BRCA1/2 screening tests and genetic consultations and, therefore improved management of subjects at high-risk of cancer.
Currently, there are 145 cancer genetic counseling units and 17 laboratories performing BRCA1/2 testing (or panel testing of multiple cancer susceptibility genes) in France (see Supplementary Data for methods used by laboratories for PV identification).
Eligibility criteria for BRCA1/2 testing according to the current national clinical guidelines are (i) at least 3 first or second degree relatives affected with breast or ovarian cancer in the same family branch, (ii) 2 first-degree relatives with BC, one of them having been diagnosed before age 41, or one before age 51 and the other before age 71, (iii) 2 first-degree relatives with BC, one of them being a male, (iv) 1 BC case before age 36, or before age 51 if triple negative tumor, (v) 1 case with bilateral BC, the first one before age 50, (vi) 1 male BC, (vii) 1 OC before age 71, or at any age if high-grade serous OC.
By 2016, 17,821 probands (i.e., the first individual tested in the family) were tested for BRCA1/2, and 1,670 (9.4%) were found to carry a PV. A similar number of probands carried a variant of uncertain clinical significance (VUS). A total of 6,417 relatives (essentially first-degree relatives of probands) underwent targeted screening tests and about 39% of them were found to carry the PV identified in the proband (http://www.e-cancer.fr).
GEMO participants are from HBOC families ascertained prospectively through family cancer clinics and tested positive for a confirmed PV in BRCA1/2. The GEMO study was initiated in 2006 and is still ongoing. Initially, only female PV carriers aged 18 or older, affected or unaffected with cancer were invited to participate in the study by geneticists. Adult male PV carriers have been invited to participate since 2013. Today, GEMO involves 32 clinics and the 17 diagnostics laboratories from the GGC.
The GEMO coordinating center was located at Centre Léon Bérard (Lyon) until September 2015 and is currently held at Institut Curie (Paris). All data and biospecimens are stored without personal identifiers. The GEMO case report form (CRF) includes information on participants' family history, gyneco-obstetrics risk factors (age at menarche, number of pregnancies, age at menopause), preventive surgery and tumor pathology (histology, grade, tumor size, hormone receptors status). Data on socio-demographic variables (age at inclusion, sex, ethnicity/population ancestry) and medical history of cancer (laterality, other cancer prior recruitment into study) are also collected.
Geneticists invite BRCA1/2 PV carriers, whether affected with cancer or not, to participate in GEMO during the consultation informing them of their BRCA1/2 positive test results. After completing the CRF with the participant, the geneticist sends it to the coordinating center, and requests that an aliquot of the blood DNA sample (at least 10 μg) that was used for genetic testing is shipped from the testing laboratory to the coordinating center. The study protocol is illustrated in Supplementary Figure 1.
Recently, an upgraded electronic database on FileMaker Pro 16 (FileMaker Inc., Santa Clara, California, USA) was developed to collate, manage and distribute core data and DNA samples, and to facilitate inter-operability with the GGC BRCA1/2 (ex-UMD-BRCA1/BRCA2) database (20) and that of the prospective cohort on BRCA1/2 PV carriers GENEPSO (21).
The study is performed in compliance with the Helsinki Declaration and received a favorable review of the French National Committees for personal data protection in medical research (CCTIRS N°07223 and CNIL agreement N°1245228). GEMO has human ethics approval at all the participating institutions where subjects are recruited. All research projects making use of data and/or materials collected by GEMO are required to have independent ethical approval from their host institutions. Participants give written informed consent during genetic counseling sessions and understand that as a result of participation, personal details will be recorded and stored in a coded format on a database. They consent to samples of DNA material prepared from blood cells being stored in a central location and to de-identified information and samples being made available for scientifically and ethically approved research projects. Informed consent agreements signed by participants are kept in the clinics.
Investigators wishing to use the GEMO DNA collection and related clinical and family data submit a brief expression of interest to principal investigators (gemo@curie.fr) who then circulate the proposal to the GEMO steering committee with a 10-day opportunity given to highlight any major issues, especially duplication of, or complementarity to, existing projects. If favorably reviewed, a full application is then submitted and verified to ensure that sufficient resources to conduct the project exist, the amount of DNA requested is appropriate, and that the proposal has any required ethics approvals. When the project is accepted, a material transfer agreement and/or a data transfer agreement are signed between the coordinating center and the research institution of the applicant. DNA samples along with related data are sent to the applicants who commit to providing annual progress reports. To further enrich the GEMO resource, applicants are required to supply their research data to GEMO after publication, and/or 12 months after completion of their projects.
The description of the genetic variants follows recommendations proposed by the Human Genome Variation Society (22). Variants are denoted using the cDNA reference sequences NM_007294.3 (BRCA1) and NM_000059.3 (BRCA2). Only carriers of a clear BRCA1/2 PV are included in GEMO. PVs are defined as variants considered as pathogenic by the GGC (20), the Evidence-based Network for the Interpretation of Germline Mutant Alleles consortium (23), the Consortium of Investigators of Modifiers of BRCA1/2 (CIMBA) (24) and/or published variants classified as pathogenic using multifactorial likelihood approaches (25, 26).
As of April 2018, 5,303 participants with available DNA sample had been enrolled in GEMO. Participants included 3,087 BRCA1 PV carriers (2,877 women and 210 men) and 2,216 BRCA2 PV carriers (2,005 women and 211 men) belonging to 2,190 and 1,544 families, respectively. The mean number of participants per family was 1.4 (range: 1–11). For 600 families, DNA samples were collected from three or more family members. While no individuals in the dataset carried more than a single PV, four families segregated two PV in two branches of the family (family 1: BRCA1:c.5137del and BRCA2:c.2808_2811del; family 2: BRCA1:c.1480C>T and BRCA1:c.3839_3843delinsAGGC; family 3: BRCA1:c.3841C>T and BRCA2:c.4889C>G; family 4: BRCA1:c.4391_4393delinsTT and BRCA2:c.7680dup).
At inclusion, 56.3% of BRCA1 female PV carriers were diagnosed with BC (mean age at diagnosis: 41.3, range 22–81), 18.3% were diagnosed with OC or fallopian tube cancer (mean age at diagnosis: 51.9, range 16–92) and 33.2% were free of these cancers (mean age at inclusion: 40.5, range 18–101). With respect to BRCA2, 61.1% of female PV carriers had BC (mean age at diagnosis: 43.6, range 21–90), 10.1% had OC or fallopian tube cancer (mean age at diagnosis: 57.9, range 31–99) and 32.9% were free of these cancers (mean age at inclusion: 42.1, range 19–91). Among the 421 male participants, 2.9% of BRCA1 PV carriers and 6.2% of BRCA2 PV carriers were diagnosed with prostate cancer at inclusion (mean age at diagnosis for BRCA1: 61.5, range 48–71 and 64.1, range 50–78 for BRCA2). Ten percent of males carrying a BRCA2 PV had BC (mean age at diagnosis: 58.8, range 44–77) vs. none in male BRCA1 PV carriers. Detailed characteristics of participants (probands and relatives) according to their cancer status are shown in Table 1. Parity, age at menarche and age at menopause (natural or artificial) for female PV carriers are shown in Supplementary Table 1. Female participants reported an average number of live births of 1.7 and a mean age at menarche of 12.9 years. No difference in parity or age at menarche was observed between women affected and unaffected with cancer, and no differences were observed between probands and relatives. Mean age at menopause (natural or artificial) was 45.7 and 47.8 years in BRCA1 and BRCA2 PV carriers, respectively. Information on prophylactic mastectomy or salphingo-oophorectomy is not systematically recorded in GEMO. However, based on available data, we identified 600 out of 4,882 female participants (12.3%) who had had bilateral or unilateral mastectomy. For 50 of them mastectomy was prophylactic as they had not developed BC at inclusion (1.0%). Among the 1,496 women (30.6%) who had had bilateral oophorectomy at inclusion, 1,005 (20.5%) had not developed OC or fallopian tube cancer and this surgery was likely prophylactic.
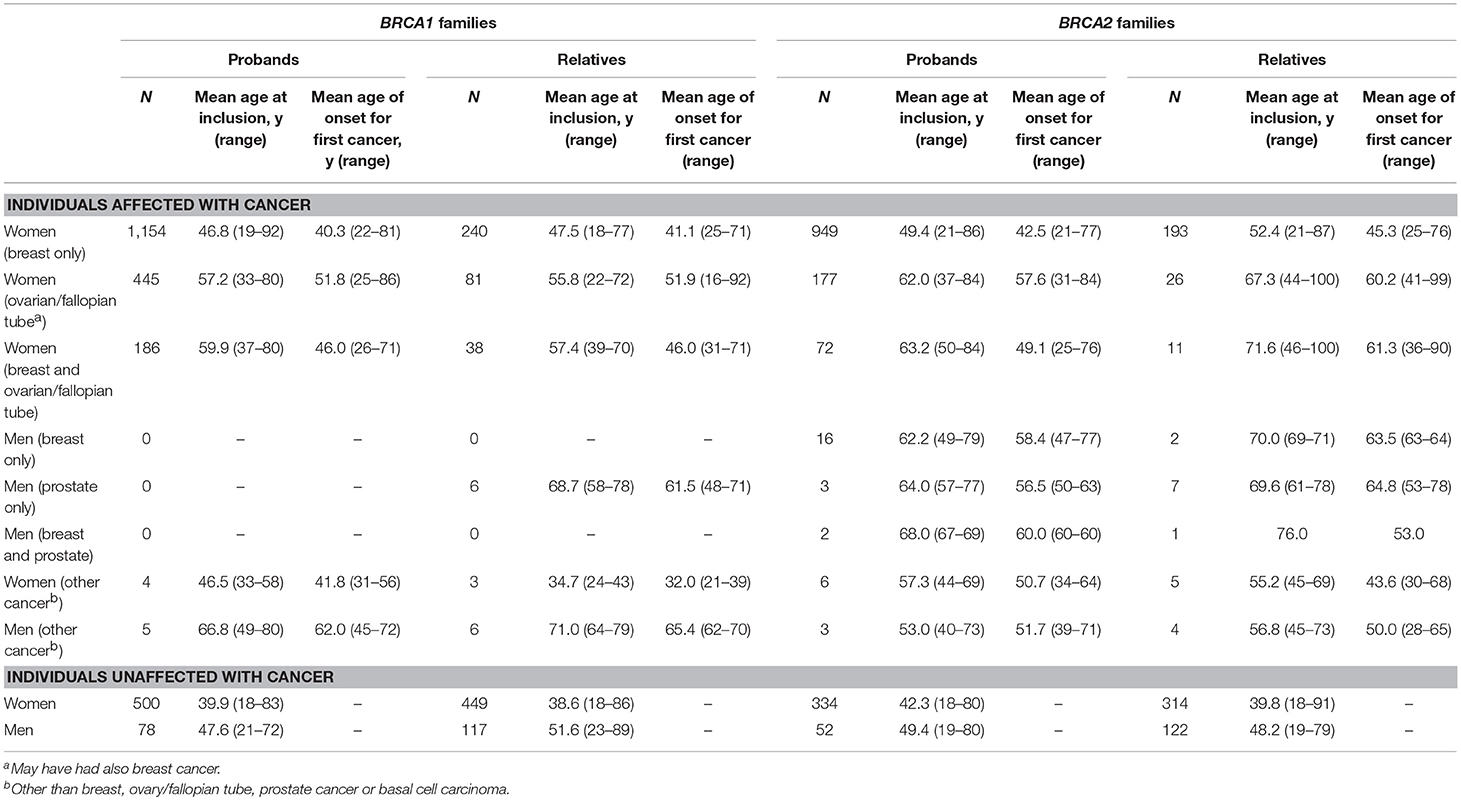
Table 1. Characterisitics of the GEMO subjects.
Only 26.9% of participants self-reported their population ancestry/ethnicity. Among them, 90.8% were European, 3.5% were African, 0.3% were Asian and 4.1% were of other or mixed origin. Ashkenazi Jewish (AJ) ancestry was reported by 1.3% of participants.
Currently, 506 BRCA1 and 494 BRCA2 unique PVs are described in the GEMO database. The number of families in which each PV was observed is shown in Supplementary Table 2 and the distribution of PVs across the gene sequences is shown in Figure 1. The five most common PVs accounted for 21.3% of all PVs in BRCA1 and 14.9% of all BRCA2 PVs. The most common BRCA1 PVs were c.5266dup (7.5%) and c.68_69del (3.9%), originally described as founder PVs in the AJ population (30), the c.3481_3491del founder PV from North-Eastern France (4.9%) (31, 32), and the two common European PVs c.4327C>T (2.7%) and c.3839_3843delinsAGGC (2.2%) (33). The most common BRCA2 PVs were c.2808_2811del (3.3%), c.5946del (3.2%), a Western European PV of AJ origin (34), c.4889C>G (2.2%), c.8364G>A (2.1%), c.5645C>A (1.9%), and c.7680dup (1.9%). There were 267 BRCA1 PVs and 265 BRCA2 PVs observed only once in GEMO.
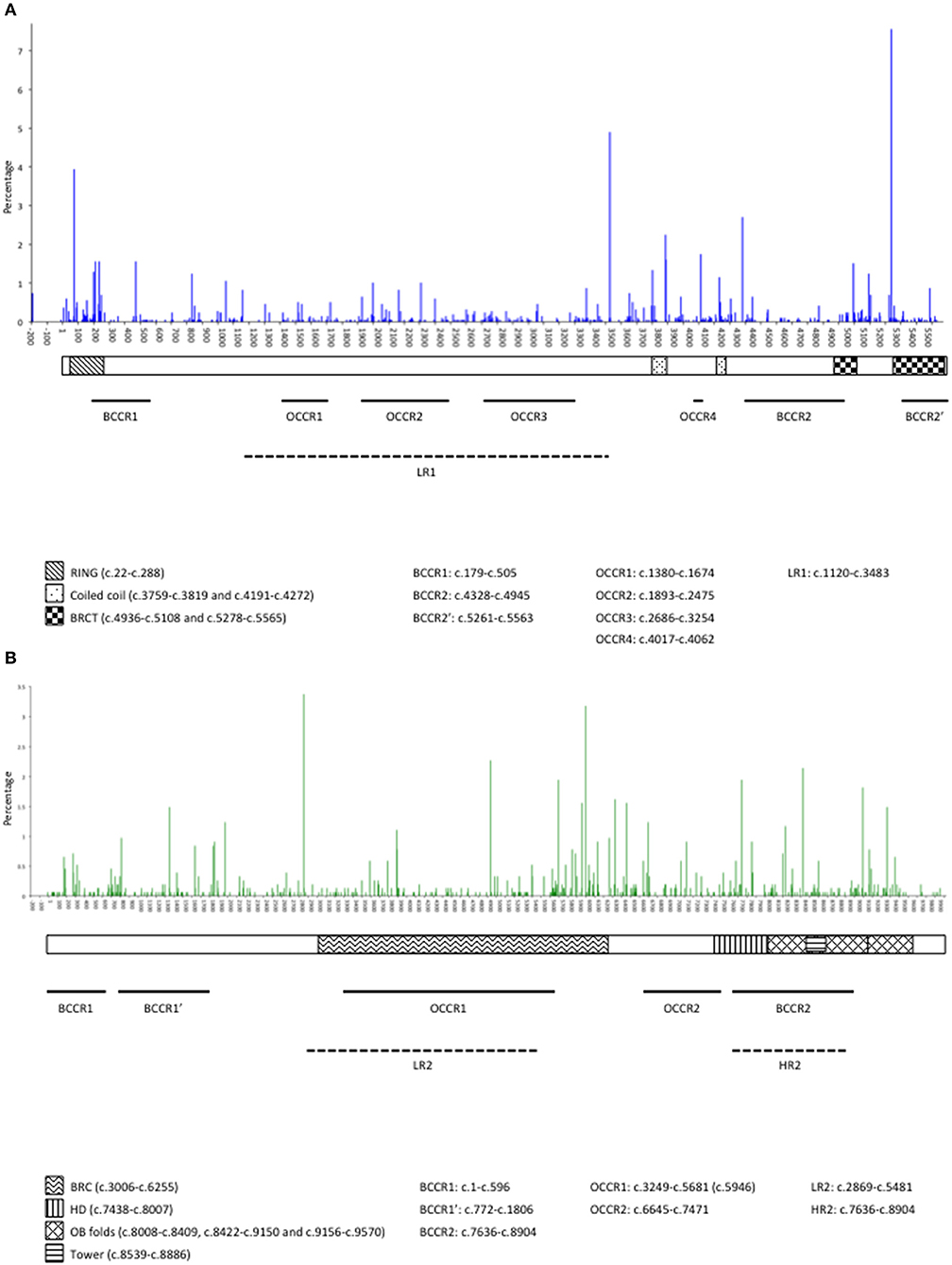
Figure 1. Distribution and occurrence of pathogenic variants along BRCA1 (A) and BRCA2 (B) in probands in the GEMO study. BRCA1 domains are: RING domain, Coiled Coil domains, BRCT (BRCA1 C-terminal) domains (14, 27). BRCA2 domains are: BRC repeats, helical domain (HD), OB fold binding domains, tower alpha (14, 28). Breast cancer risk regions: LR1, lower risk region in BRCA1, LR2 lower risk region in BRCA2, HR2, higher risk region in BRCA2 (29); BCCR, breast cancer cluster region (14); Ovarian cancer risk regions: OCCR, ovarian cancer cluster region (14).
The GGC database was designed to compile information on all BRCA1/2 variants (pathogenic, neutral and VUS), except common polymorphisms, identified probands in the 17 French licensed laboratories (20). This database is therefore considered as the reference database for BRCA1/2 variants in France. In June 2018, it contained PV from 6,385 BRCA1 and 4,839 BRCA2 families (Sandrine Caputo, personal communication), and about one third of the population recorded in the GGC database had been enrolled in GEMO. The distribution of PVs along the genes sequence in GEMO and the GGC BRCA1/2 database overlaps (Supplementary Table 2), although a few variants were under-represented in GEMO reflecting a recruitment bias in the study due to the absence of participating cancer clinics in some regions (e.g., BRCA1:c.5260G>T is identified mostly in families from Western France). Other differences can be attributable to a different dynamics between the GEMO and the national registry (some PVs observed in GEMO had not been yet recorded in the GGC database).
Over 5,300 participants have been enrolled in GEMO to date, which provides an overview of BRCA1/2 PVs in a well-characterized sample of French counseled HBOC families. The GEMO resource is available to internal and external researchers who can apply for blood DNA and data for use in ethically approved, peer reviewed collaborative and interdisciplinary projects on the genetic epidemiology of cancer in BRCA1/2 families. Its overall goal is to facilitate the translation of research results to the clinical setting.
As an example, GEMO contributes massively to the CIMBA effort involving centers on six continents that have recruited BRCA1/2 PV carriers with associated clinical, risk factors, and genetic data (24). GEMO is one of the three most important contributors to CIMBA projects in terms of number of samples, phenotypic and pathology data. In total, 2,868 subjects (53.9% of the GEMO population) had been genotyped using the iCOGS and/or the Oncoarray chips in the context of large-scale GWAS (35, 36). In brief, these international initiatives led to the identification of 26 and 16 SNPs associated with BC risk for BRCA1 and BRCA2 PV carriers respectively, and the corresponding numbers for OC risk are 11 and 13 (15). The combined effect of these SNPs, modeled as Polygenic Risk Scores (PRS) is currently being investigated to improve individualized cancer risk predictions. Other goals of the Consortium are to precise age-specific cancer risk estimates considering position and functional effects of the PV, family history of cancer and genetic and lifestyle/hormonal modifier risk factors in order to integrate findings on SNPs into the genetic counseling process. GEMO study collaborators co-authored 43 CIMBA publications. Publications and summary results for iCOGS SNPs are accessible via http://cimba.ccge.medschl.cam.ac.uk/.
At the national level, the GEMO group is aiming to develop specific PRS in the French counseled families in order to assess the clinical utility of incorporating such scores in risk prediction models. Indeed, improvement in the performance of such models for risk stratification and personalized decision-making (e.g., prophylactic mastectomy/salphingo-oophorectomy or frequency of BC screening) has important clinical implications. Efforts are also being made to render the GEMO database interoperable with other national databases including that of GENEPSO, which is a prospective cohort initiated in 1999, where BRCA1/2 PV carriers are followed over time to observed prospectively characteristics of subjects who develop either primary or secondary cancers (5). To date, about 1,400 individuals have been enrolled in both GEMO and GENEPSO.
Clinical management of healthy women with a BRCA1/2 PV involves a combination of frequent screening, especially of the breasts, risk-reducing surgeries and possibly chemoprevention (37). For these women, important decisions include whether or not to undergo preventive mastectomy and the age at which to undergo risk-reducing salphingo-oophorectomy. These choices are invasive, have substantial side effects, and are associated with adverse psychological effects (38). It is therefore important to have precise estimates of associated age-specific cancer risks to provide optimal advices to women carrying a PV. Hence, women at particularly high risk or with a high risk of disease at early ages may benefit from early intervention, and women at lower risk may opt to delay surgery or chemoprevention.
FL, FD, SM, and DS-L coordinated the GEMO study. CN, MiL, IM, SF-F, EM-F, PP, LV-B, Y-JB, DL, IC, PB, VM, CD, PG, M-AC-R, SG, VB, LF, BB, CL, and MG-V invited GEMO participants. CH, BB-dP, DV, HS, NM, LB, MéL, FD, and FL managed the DNA samples. NM, LB, MB, FD, FL, MaL, and YJ managed family and clinical data. NM, LB, MéL, FD, YJ, SMC, and FL curated the variants databases. FL and YJ analyzed the data. FL and NA wrote the paper. All authors read and approved the final manuscript.
The GEMO resource was initially funded by the French National Institute of Cancer (INCa, PHRC Ile de France, AOR 01 082, DS-L 2001–2003), the Association Le cancer du sein, parlons-en! Award (SM, O. Sinilnikova, DS-L 2004) and the Association for International Cancer Research (O. Sinilnikova; 2008–2010). It also received support from the Canadian Institute of Health Research for the CIHR Team in Familial Risks of Breast Cancer program (J. Simard; 2008–2013), and the European commission FP7, Project Collaborative Ovarian, breast and prostate Gene-environment Study (COGS), Large-scale integrating project (D. Easton, Per Hall; 2009–2013). GEMO is currently supported by the INCa AAP 2013 Bases Clinico-Biologiques (CANSOP grant 2013-1-BCB-01-ICH-1, DS-L) and the Fondation ARC pour la recherche sur le cancer (grant PJA 20151203365, FL).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Genetic Modifiers of Cancer Risk in BRCA1/2 Mutation Carriers (GEMO) study is a study from the National Cancer Genetics Network UNICANCER Genetic Group, France. We wish to pay a tribute to Olga M. Sinilnikova, who with DS-L initiated and coordinated GEMO until she sadly passed away on the 30th June 2014. The team in Lyon (Olga Sinilnikova, ML, LB, Carole Verny-Pierre, SM, FD, Valérie Sornin) managed the GEMO samples until the biological resource center was transferred to Paris in December 2015 (NM, FL, DS-L). We want to thank all the GEMO collaborating groups for their contribution to this study. Coordinating Center: Service de Génétique, Institut Curie, Paris: MB, Ophélie Bertrand, Anne-Marie Birot, BB, SMC, Chrystelle Colas, Anaïs Dupré, Emmanuelle Fourme, MG-V, Lisa Golmard, CH, Marine Le Mentec, Virginie Moncoutier, Antoine de Pauw, Claire Saule, DS-L, and Inserm U900, Institut Curie, Paris: FL, NM. Contributing Centers: Unité Mixte de Génétique Constitutionnelle des Cancers Fréquents, Hospices Civils de Lyon-Centre Léon Bérard, Lyon: Nadia Boutry-Kryza, Alain Calender, SG, ML. Institut Gustave Roussy, Villejuif: BB-dP, Olivier Caron, Marine Guillaud-Bataille. Centre Jean Perrin, Clermont–Ferrand: Y-JB, Nancy Uhrhammer. Centre Léon Bérard, Lyon: VB, CL. Centre François Baclesse, Caen: PB, Laurent Castera, DV. Institut Paoli Calmettes, Marseille: Violaine Bourdon, CN, Tetsuro Noguchi, Cornel Popovici, Audrey Remenieras, HS. CHU Arnaud-de-Villeneuve, Montpellier: IC, Pierre-Olivier Harmand, PP, Paul Vilquin. Centre Oscar Lambret, Lille: Aurélie Dumont, Françoise Révillion. Centre Paul Strauss, Strasbourg: Danièle Muller. Institut Bergonié, Bordeaux: Emmanuelle Barouk-Simonet, Françoise Bonnet, Virginie Bubien, ML, Nicolas Sévenet. Institut Claudius Regaud, Toulouse: Laurence Gladieff, Rosine Guimbaud, Viviane Feillel, Christine Toulas. CHU Grenoble: Hélène Dreyfus, DL, Magalie Peysselon, Christine Rebischung. CHU Dijon: AB, Geoffrey Bertolone, Fanny Coron, LF, Vincent Goussot, Caroline Jacquot, Caroline Sawka. CHU St-Etienne: Caroline Kientz, Marine Lebrun, Fabienne Prieur. Hôtel Dieu Centre Hospitalier, Chambéry: SF-F. Centre Antoine Lacassagne, Nice: VM. CHU Limoges: LV-B. CHU Nantes: Stéphane Bézieau, CD. CHU Bretonneau, Tours and Centre Hospitalier de Bourges: IM. Groupe Hospitalier Pitié-Salpétrière, Paris: Florence Coulet, Florent Soubrier, Mathilde Warcoin. CHU Vandoeuvre-les-Nancy: Myriam Bronner, Sarab Lizard, Johanna Sokolowska. CHU Besançon: M-AC-R, Alexandre Damette. CHU Poitiers, Centre Hospitalier d'Angoulême and Centre Hospitalier de Niort: PG. Centre Hospitalier de La Rochelle: Hakima Lallaoui. CHU Nîmes Carémeau: Jean Chiesa. CHI Poissy: Denise Molina-Gomes. CHU Angers: Olivier Ingster. CHRU de Lille: Sylvie Manouvrier-Hanu, Sophie Lejeune. We wish to acknowledge the work of Gustave Roussy Biobank (BB-0033-00074) in providing DNA resources.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fonc.2018.00490/full#supplementary-material
Supplementary Table 1. Age at menarche, age at menopause and parity for women affected and unaffected with cancer.
Supplementary Table 2. Unique pathogenic variants and number of families in which each variant was observed. Variants are called using the cDNA reference sequences NM_007294.3 (BRCA1) and NM_000059.3 (BRCA2).
Supplementary Figure 1. Protocol of the study.
Supplementary Data. Methods used for identification of BRCA1/2 pathogenic variants.
BC, Breast Cancer; BCAC, Breast Cancer Association Consortium; BRCA1, BReast CAncer 1; BRCA2, BReast CAncer 2; CRF, Case Report Form; CIMBA, Consortium of Investigators of Modifiers of BRCA1/2; GWAS, Genome-Wide Association Study; HBOC, Hereditary Breast and Ovarian Cancer; OC, Ovarian Cancer; PRS, Polygenic Risk Score; SNP, Single Nucleotide Polymorphism, VUS, Variant of Uncertain Clinical Significance.
1. Ford D, Easton DF, Stratton M, Narod S, Goldgar D, Devilee P, et al. Genetic heterogeneity and penetrance analysis of the BRCA1 and BRCA2 genes in breast cancer families. Breast Cancer Linkage Consort Am J Hum Genet. (1998) 62:676–89. doi: 10.1086/301749
2. Hopper JL, Southey MC, Dite GS, Jolley DJ, Giles GG, Mccredie MR, et al. Population-based estimate of the average age-specific cumulative risk of breast cancer for a defined set of protein-truncating mutations in BRCA1 and BRCA2. Aust Breast Cancer Family Study Cancer Epidemiol Biomarkers Prev. (1999) 8:741–7.
3. Antoniou AC, Cunningham AP, Peto J, Evans DG, Lalloo F, Narod SA, et al. The BOADICEA model of genetic susceptibility to breast and ovarian cancers: updates and extensions. Br J Cancer (2008a) 98:1457–66. doi: 10.1038/sj.bjc.6604305
4. Brohet RM, Velthuizen ME, Hogervorst FB, Meijers-Heijboer HE, Seynaeve C, Collee MJ, et al. Breast and ovarian cancer risks in a large series of clinically ascertained families with a high proportion of BRCA1 and BRCA2 Dutch founder mutations. J Med Genet. (2014) 51:98–107. doi: 10.1136/jmedgenet-2013-101974
5. Kuchenbaecker KB, Hopper JL, Barnes DR, Phillips KA, Mooij TM, Roos-Blom MJ, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA (2017) 317:2402–16. doi: 10.1001/jama.2017.7112
6. Narod SA. Modifiers of risk of hereditary breast cancer. Oncogene (2006) 25:5832–6. doi: 10.1038/sj.onc.1209870
7. Antoniou AC, Spurdle AB, Sinilnikova OM, Healey S, Pooley KA, Schmutzler RK, et al. Common breast cancer-predisposition alleles are associated with breast cancer risk in BRCA1 and BRCA2 mutation carriers. Am J Hum Genet. (2008) 82:937–48. doi: 10.1016/j.ajhg.2008.02.008
8. Milne RL, Antoniou AC. Genetic modifiers of cancer risk for BRCA1 and BRCA2 mutation carriers. Ann Oncol. (2011) 22(Suppl. 1):i11–7. doi: 10.1093/annonc/mdq660
9. Kotsopoulos J, Lubinski J, Lynch HT, Kim-Sing C, Neuhausen S, Demsky R, et al. Oophorectomy after menopause and the risk of breast cancer in BRCA1 and BRCA2 mutation carriers. Cancer Epidemiol Biomarkers Prev. (2012) 21:1089–96. doi: 10.1158/1055-9965.EPI-12-0201
10. Friebel TM, Domchek SM, Rebbeck TR. Modifiers of cancer risk in BRCA1 and BRCA2 mutation carriers: systematic review and meta-analysis. J Natl Cancer Inst. (2014) 106:dju091. doi: 10.1093/jnci/dju091
11. Michailidou K, Lindstrom S, Dennis J, Beesley J, Hui S, Kar S, et al. Association analysis identifies 65 new breast cancer risk loci. Nature (2017) 551:92–4. doi: 10.1038/nature24284
12. Couch FJ, Wang X, Mcguffog L, Lee A, Olswold C, Kuchenbaecker KB, et al. Genome-wide association study in BRCA1 mutation carriers identifies novel loci associated with breast and ovarian cancer risk. PLoS Genet. (2013) 9:e1003212. doi: 10.1371/journal.pgen.1003212
13. Gaudet MM, Kuchenbaecker KB, Vijai J, Klein RJ, Kirchhoff T, Mcguffog L, et al. Identification of a BRCA2-specific modifier locus at 6p24 related to breast cancer risk. PLoS Genet. (2013) 9:e1003173. doi: 10.1371/journal.pgen.1003173
14. Rebbeck TR, Mitra N, Wan F, Sinilnikova OM, Healey S, Mcguffog L, et al. Association of type and location of BRCA1 and BRCA2 mutations with risk of breast and ovarian cancer. JAMA (2015) 313:1347–61. doi: 10.1001/jama.2014.5985
15. Milne RL, Antoniou AC. Modifiers of breast and ovarian cancer risks for BRCA1 and BRCA2 mutation carriers. Endocr Relat Cancer (2016) 23:T69–84. doi: 10.1530/ERC-16-0277
16. Thompson D, Easton D, Breast Cancer Linkage C. Variation in cancer risks, by mutation position, in BRCA2 mutation carriers. Am J Hum Genet. (2001) 68:410–9. doi: 10.1086/318181
17. Thompson D, Easton D, Breast Cancer Linkage Consortium. Variation in BRCA1 cancer risks by mutation position. Cancer Epidemiol Biomarkers Prev. (2002) 11:329–36. Available online at: http://cebp.aacrjournals.org/content/11/4/329.long
18. Lecarpentier J, Nogues C, Mouret-Fourme E, Gauthier-Villars M, Lasset C, Fricker JP, et al. Variation in breast cancer risk associated with factors related to pregnancies according to truncating mutation location, in the French National BRCA1 and BRCA2 mutations carrier cohort (GENEPSO). Breast Cancer Res. (2012) 14:R99. doi: 10.1186/bcr3218
19. Lecarpentier J, Nogues C, Mouret-Fourme E, Buecher B, Gauthier-Villars M, Stoppa-Lyonnet D, et al. Breast cancer risk associated with estrogen exposure and truncating mutation location in BRCA1/2 carriers. Cancer Epidemiol Biomarkers Prev. (2015) 24:698–707. doi: 10.1158/1055-9965.EPI-14-0884
20. Caputo S, Benboudjema L, Sinilnikova O, Rouleau E, Beroud C, Lidereau R. Description and analysis of genetic variants in French hereditary breast and ovarian cancer families recorded in the UMD-BRCA1/BRCA2 databases. Nucleic Acids Res. (2012) 40:D992–1002. doi: 10.1093/nar/gkr1160
21. Andrieu N, Easton DF, Chang-Claude J, Rookus MA, Brohet R, Cardis E, et al. Effect of chest X-rays on the risk of breast cancer among BRCA1/2 mutation carriers in the international BRCA1/2 carrier cohort study: a report from the EMBRACE, GENEPSO, GEO-HEBON, and IBCCS Collaborators' Group. J Clin Oncol. (2006) 24:3361–6. doi: 10.1200/JCO.2005.03.3126
22. Den Dunnen JT, Dalgleish R, Maglott DR, Hart RK, Greenblatt MS, Mcgowan-Jordan J, et al. HGVS recommendations for the description of sequence variants: 2016 update. Hum Mutat. (2016) 37:564–9. doi: 10.1002/humu.22981
23. Spurdle AB, Healey S, Devereau A, Hogervorst FB, Monteiro AN, Nathanson KL, et al. ENIGMA–evidence-based network for the interpretation of germline mutant alleles: an international initiative to evaluate risk and clinical significance associated with sequence variation in BRCA1 and BRCA2 genes. Hum Mutat. (2012) 33:2–7. doi: 10.1002/humu.21628
24. Chenevix-Trench G, Milne RL, Antoniou AC, Couch FJ, Easton DF, Goldgar DE. An international initiative to identify genetic modifiers of cancer risk in BRCA1 and BRCA2 mutation carriers: the Consortium of Investigators of Modifiers of BRCA1 and BRCA2 (CIMBA). Breast Cancer Res. (2007) 9:104. doi: 10.1186/bcr1670
25. Goldgar DE, Easton DF, Deffenbaugh AM, Monteiro AN, Tavtigian SV, Couch FJ, et al. Integrated evaluation of DNA sequence variants of unknown clinical significance: application to BRCA1 and BRCA2. Am J Hum Genet. (2004) 75:535–44. doi: 10.1086/424388
26. Easton DF, Deffenbaugh AM, Pruss D, Frye C, Wenstrup RJ, Allen-Brady K, et al. A systematic genetic assessment of 1,433 sequence variants of unknown clinical significance in the BRCA1 and BRCA2 breast cancer-predisposition genes. Am J Hum Genet. (2007) 81:873–83. doi: 10.1086/521032
27. Millot GA, Carvalho MA, Caputo SM, Vreeswijk MP, Brown MA, Webb M, et al. A guide for functional analysis of BRCA1 variants of uncertain significance. Hum Mutat. (2012) 33:1526–37. doi: 10.1002/humu.22150
28. Yang H, Jeffrey PD, Miller J, Kinnucan E, Sun Y, Thoma NH, et al. BRCA2 function in DNA binding and recombination from a BRCA2-DSS1-ssDNA structure. Science (2002) 297:1837–48. doi: 10.1126/science.297.5588.1837
29. Lecarpentier J, Noguès C, Mouret-Fourme E, Stoppa-Lyonnet D, Lasset C, Caron O, et al. Variation in breast cancer risk with mutation position, smoking, alcohol, and chest X-ray history, in the French National BRCA1/2 carrier cohort (GENEPSO). Breast Cancer Res Treat. (2011) 130:927–38. doi: 10.1007/s10549-011-1655-3
30. Hamel N, Feng BJ, Foretova L, Stoppa-Lyonnet D, Narod SA, Imyanitov E, et al. On the origin and diffusion of BRCA1 c.5266dupC (5382insC) in European populations. Eur J Hum Genet. (2011) 19:300–6. doi: 10.1038/ejhg.2010.203
31. Stoppa-Lyonnet D, Laurent-Puig P, Essioux L, Pages S, Ithier G, Ligot L, et al. BRCA1 sequence variations in 160 individuals referred to a breast/ovarian family cancer clinic. Inst Curie Breast Cancer Group Am J Hum Genet. (1997) 60:1021–30.
32. Muller D, Bonaiti-Pellie C, Abecassis J, Stoppa-Lyonnet D, Fricker JP. BRCA1 testing in breast and/or ovarian cancer families from northeastern France identifies two common mutations with a founder effect. Fam Cancer (2004) 3:15–20. doi: 10.1023/B:FAME.0000026819.44213.df
33. Rebbeck TR, Friebel TM, Friedman E, Hamann U, Huo D, Kwong A, et al. Mutational spectrum in a worldwide study of 29,700 families with BRCA1 or BRCA2 mutations. Hum Mutat. (2018) 39:593–620. doi: 10.1002/humu.23406
34. Hall MJ, Reid JE, Burbidge LA, Pruss D, Deffenbaugh AM, Frye C, et al. BRCA1 and BRCA2 mutations in women of different ethnicities undergoing testing for hereditary breast-ovarian cancer. Cancer (2009) 115:2222–33. doi: 10.1002/cncr.24200
35. Kuchenbaecker KB, Neuhausen SL, Robson M, Barrowdale D, Mcguffog L, Mulligan AM, et al. Associations of common breast cancer susceptibility alleles with risk of breast cancer subtypes in BRCA1 and BRCA2 mutation carriers. Breast Cancer Res. (2014) 16:3416. doi: 10.1186/s13058-014-0492-9
36. Milne RL, Kuchenbaecker KB, Michailidou K, Beesley J, Kar S, Lindstrom S, et al. Identification of ten variants associated with risk of estrogen-receptor-negative breast cancer. Nat Genet. (2017) 49:1767–78. doi: 10.1038/ng.3785
37. Evans DG, Graham J, O'connell S, Arnold S, Fitzsimmons D. Familial breast cancer: summary of updated NICE guidance. BMJ (2013) 346:f3829. doi: 10.1136/bmj.f3829
Keywords: breast cancer, BRCA1/2 mutation carriers, pathogenic variant (PV), DNA banking, genetic epidemiology
Citation: Lesueur F, Mebirouk N, Jiao Y, Barjhoux L, Belotti M, Laurent M, Léone M, Houdayer C, Bressac-de Paillerets B, Vaur D, Sobol H, Nogués C, Longy M, Mortemousque I, Fert-Ferrer S, Mouret-Fourme E, Pujol P, Venat-Bouvet L, Bignon Y-J, Leroux D, Coupier I, Berthet P, Mari V, Delnatte C, Gesta P, Collonge-Rame M-A, Giraud S, Bonadona V, Baurand A, Faivre L, Buecher B, Lasset C, Gauthier-Villars M, Damiola F, Mazoyer S, Caputo SM, Andrieu N, Stoppa-Lyonnet D and GEMO Study Collaborators (2018) GEMO, a National Resource to Study Genetic Modifiers of Breast and Ovarian Cancer Risk in BRCA1 and BRCA2 Pathogenic Variant Carriers. Front. Oncol. 8:490. doi: 10.3389/fonc.2018.00490
Received: 01 July 2018; Accepted: 11 October 2018;
Published: 31 October 2018.
Edited by:
Nandita Mitra, University of Pennsylvania, United StatesReviewed by:
Florentia Fostira, National Centre of Scientific Research Demokritos, GreeceCopyright © 2018 Lesueur, Mebirouk, Jiao, Barjhoux, Belotti, Laurent, Léone, Houdayer, Bressac-de Paillerets, Vaur, Sobol, Nogués, Longy, Mortemousque, Fert-Ferrer, Mouret-Fourme, Pujol, Venat-Bouvet, Bignon, Leroux, Coupier, Berthet, Mari, Delnatte, Gesta, Collonge-Rame, Giraud, Bonadona, Baurand, Faivre, Buecher, Lasset, Gauthier-Villars, Damiola, Mazoyer, Caputo, Andrieu, Stoppa-Lyonnet and GEMO Study Collaborators. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fabienne Lesueur, ZmFiaWVubmUubGVzdWV1ckBjdXJpZS5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.