


94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Oncol. , 29 October 2012
Sec. Cancer Immunity and Immunotherapy
Volume 2 - 2012 | https://doi.org/10.3389/fonc.2012.00147
This article is part of the Research Topic Anti-idiotype antibodies in cancer treatment View all 12 articles
Active immunotherapy is an interesting field from the industry's perspective and in the last years, regulatory agencies and the medical community have showed renewed expectations and interest in cancer vaccines. The development of new immune therapies offers many challenges, and this is reflected in the small number of phase III trials showing clear benefits. Traditional concepts applied in clinical trials for the development of chemotherapeutic agents may be inadequate for immunotherapies and a new paradigm is emerging. It is possible that organized efforts and funding will accelerate the development of therapeutically effective cancer vaccines. This article reviews the attributes of cancer vaccines which make them attractive from the industry's perspective, and focuses especially in the characteristics of Racotumomab, an anti-idiotype antibody vaccine.
There are different immunotherapeutic approaches in cancer, including passive and active immunotherapy, adoptive T cell transfer, and non-specific immunotherapy, amongst others.
Active immunotherapy is an interesting field because vaccines usually have a favorable side effect profile and are well-tolerated and can be used in combination with other therapies.
However, the development of these new immune therapies offers many challenges, and this is reflected in the small number of phase III trials showing clear benefits. Immune response may not always translate into clinical benefit, and for solid tumors, traditional criteria for evaluation of tumor response may not be appropriate or relevant (Tuma, 2006; Hoos et al., 2007; Schlom et al., 2007).
In the last years, the regulatory agencies and the medical community have increased their expectations regarding these therapeutic strategies. The FDA released in October 2011a guidance document for the industry addressing the challenges and particular issues with the development of cancer vaccines such as monitoring for immune response, disease progression/recurrence immediately or shortly after the start of the vaccine, delayed effects of the vaccines when evaluating time to event endpoints, etc (Guidance for Industry, 2011). This shows that in the development phases of vaccines and immunotherapies, some of the traditional concepts applied in oncology clinical trials for chemotherapeutic agents are at least controversial or inappropriate and a new paradigm is emerging for immunotherapies.
The NCI recently recognized the untapped potential of therapeutic cancer vaccines and set a pilot project for identification and prioritization of cancer antigens (Cheever et al., 2009). There is increasing interest in the cancer vaccine field, and it is possible that organized efforts and funding will accelerate the development of therapeutically effective cancer vaccines.
The successful development of a vaccine for cancer treatment is influenced by several factors. Some of them are related to the product, type of tumor, expression of the target, and also to the patient characteristics, such as performance status or stage of the disease, play an important role.
An anti-idiotype monoclonal antibody (mAb) is the mirror image of the original antibody formed against specific surface antigens. Thus, anti-idiotype antibodies can act as antigens, inducing a response against the original antigen.
Racotumomab is an anti-idiotype antibody used as a therapeutic vaccine. Although it is as mAb, it is administered in small amounts, intradermally, and acts as an active specific immunotherapeutic agent.
Racotumomab was formerly known as 1E10 anti-idiotype vaccine and is a good example of a candidate for development because it holds many positive characteristics:
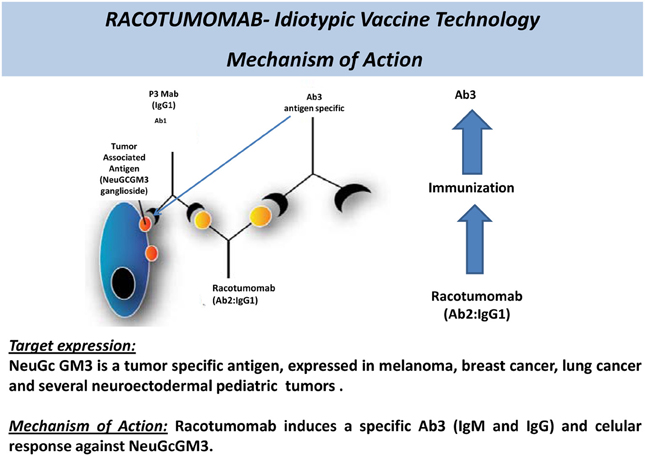
Figure 1. Racotumomab—mechanism of action of an anti-idiotype antibody.
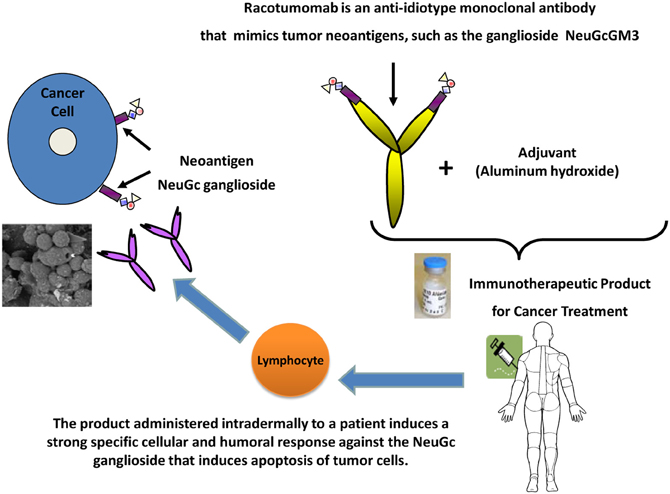
Figure 2. Immune response to vaccination with Racotumomab.
In summary, Racotumomab is a well-tolerated, immunogenic cancer vaccine which has shown to prolong survival in NSCLC and is currently being evaluated in a multinational, phase III trial.
Full time employee at Laboratorio ELEA SACIFyA.
Alfonso, M., Díaz, A., Hernández, A. M., Pérez, A., Rodríguez, E., and Bitton, R. (2002). An anti-idiotype vaccine elicits a specific response to N-glycolyl sialic acid residues of glycoconjugates in melanoma patients. J. Immunol. 168, 2523–2529.
Alfonso, S., Díaz, R. M., de la Torre, A., Santiesteban, E., Aguirre, F., and Pérez, K. (2007). 1E10 anti-idiotype vaccine in non-small cell lung cancer. Experience in stage IIIb/IV patients. Cancer Biol. Ther. 6, 1847–1852.
Balducci, L. (2001). Hematopoietic growth factors in the older cancer patient. Curr. Opin. Hematol. 8, 170–187.
Balducci, L., and Repetto, L. (2004). Increased risk of myelotoxicity in elderly patients with non-Hodgkin lymphoma. Cancer 100, 6–11.
Belani, C. P. (2005). Elderly subgroup analysis of a randomized phase III study of docetaxel plus platinum combinations versus vinorelbine plus cisplatin for first-line treatment of advanced nonsmall cell lung carcinoma (TAX 326). Cancer 104, 2766–2774.
Cheever, A. M., Allison, J. P., Ferris, A. S., Finn, O. J., Hastings, B. M., and Hecht, T. T. (2009). The prioritization of cancer antigens: a national cancer institute pilot project for the acceleration of translational research. Clin. Cancer Res. 15, 5323–37.
Díaz, A., Alfonso, M., Alonso, R., Saurez, G., Troche, M., and Catalá, M. (2003). Immune responses in breast cancer patients immunized with an anti-idiotype antibody mimicking NeuGc-containing gangliosides. Clin. Immunol. 107, 80–89.
Gridelli, C. (2008). Treatment of advanced non–small-cell lung cancer in the elderly: from best supportive care to the combination of platin-based chemotherapy and targeted therapies; editorial. J. Clin. Oncol. 26, 13–15.
Guidance for Industry. (2011). Clinical considerations for therapeutic cancer vaccines. Available online at: http://www.fda.gov/downloads/biologicsbloodvaccines/guidancecomplianceregulatoryinformation/guidances/vaccines/ucm278673.pdf
Guthmann, M. D., Bitton, R. J., Carnero, A. J., Gabri, M. R., Cinat, G., and Koliren, L. (2004). Active specific immunotherapy of melanoma with a GM3 ganglioside-based vaccine: a report on safety and immunogenicity. J. Immunother. 27, 442–451.
Guthmann, M. D., Castro, M. A., Cinat, G., Venier, C., Koliren, L., and Bitton, R. J. (2006). Cellular and humoral immune response to N-Glycolyl-GM3 elicited by prolonged immunotherapy with an anti-idiotypic vaccine in high-risk and metastatic breast cancer patients. J. Immunother. 29, 215–223.
Hernández, A. M., Rodríguez, N., González, J. E., Reyes, E., Rondón, T., and Griñán, T. (2011). Anti-NeuGcGM3 antibodies, actively elicited by idiotypic vaccination in nonsmall cell lung cancer patients, induce tumor cell death by an oncosis-like mechanism. J. Immunol. 186, 3735–3744.
Hernández, A. M., Toledo, D., Martínez, D., Griñán, T., Brito, V., and Macías, A. (2008). Characterization of the antibody response against NeuGcGM3 ganglioside elicited in non-small cell lung cancer patients immunized with an anti-idiotype antibody. J. Immunol. 181, 6625–6634.
Hoos, A., Parmiani, G., Hege, K., Sznol, M., Loibner, H., and Eggermont, A. (2007). A clinical development paradigm for cancer vaccines and related biologics. J. Immunother. 30, 1–15.
Irie, A., Koyama, S., Kozutsumi, Y., Kawasaki, T., and Suzuki, A. (1998). The molecular basis for the absence of N-glycolylneuraminic acid in humans. J. Biol. Chem. 273, 15866–15871.
Lynn, A., Ries, G., Reichman, M. E., Riedel Lewis, D., Hankey, B. F., and Edwards, B. K. (2003). Cancer survival and incidence from the surveillance, epidemiology, and end results (SEER) program. Oncologist 8, 541–552.
Moreno, E., Lanne, B., Vázquez, A. M., Kawashima, I., Tai, T., and Fernández, L. E. (1998). Delineation of the epitope recognized by an specific antibody for N-glycolylneuraminic acid-containing gangliosides. Glycobiology 8, 695.
Muchmore, E. A., Diaz, S., and Varki, A. (1998). A structural difference between the cell surfaces of humans and the great apes. Am. J. Phys. Anthropol. 107, 187–198.
Neninger, E., Díaz, R. M., de la Torre, A., Rives, R., Díaz, A., and Saurez, G. (2007). Active immunotherapy with 1E10 anti-idiotype vaccine in patients with small cell lung cancer: report of a phase I trial. Cancer Biol. Ther. 6, 145–150.
Schlom, J., Arlen, P., and Gulley, J. (2007). Cancer vaccines: moving beyond current paradigms. Clin. Cancer Res. 13, 3776–3782.
Scursoni, A. M., Galluzzo, L., Camarero, S., Lopez, J., Lubieniecki, F., and Sampor, C. (2011). Detection of N-Glycolyl GM3 ganglioside in neuroectodermal tumors by immunohistochemistry: an attractive vaccine target for aggressive pediatric cancer. Clin. Dev. Immunol. 2011, 245181.
Scursoni, A. M., Galluzzo, L., Camarero, S., Pozzo, N., Gabri, M. R., and Mateo de Acosta, C. (2012). Detection and characterization of N-glycolyated gangliosides in Wilms tumor by immunohistochemistry. Pediatr. Dev. Pathol. 13, 18–23.
Tuma, R. S. (2006). Sometimes size doesn't matter: reevaluating RECIST and tumor response rate endpoints. J. Natl. Cancer Inst. 98, 1272–1274.
van Cruijsen, H., Ruiz, M. G., van der Valk, P., de Gruijl, T. D., and Giaccone, G. (2009). Tissue micro array analysis of ganglioside N-glycolyl GM3 expression and signal transducer and activator of transcription (STAT)-3 activation in relation to dendritic cell infiltration and microvessel density in non-small cell lung cancer. BMC Cancer 9:180. doi: 10.1186/1471-2407-9-180
Keywords: lung cancer, Racotumomab, cancer vaccines, immunotherapy, pediatric tumor
Citation: Gómez RE and Ardigo ML (2012) Anti-idiotype antibodies in cancer treatment: the pharmaceutical industry perspective. Front. Oncol. 2:147. doi: 10.3389/fonc.2012.00147
Received: 03 August 2012; Accepted: 01 October 2012;
Published online: 29 October 2012.
Edited by:
Daniel Gomez, Universidad Nacional de Quilmes, ArgentinaReviewed by:
Viktor Umansky, German Cancer Research Center (DKFZ), GermanyCopyright © 2012 Gómez and Ardigo. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits use, distribution and reproduction in other forums, provided the original authors and source are credited and subject to any copyright notices concerning any third-party graphics etc.
*Correspondence: Roberto E. Gómez, Medical Affairs, Laboratorio ELEA SACIFyA, Buenos Aires, Argentina. e-mail:Z29tZXpyQGVsZWEuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.