
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Nucl. Med. , 26 October 2023
Sec. PET and SPECT
Volume 3 - 2023 | https://doi.org/10.3389/fnume.2023.1273967
 Henri Pasquesoone1*†
Henri Pasquesoone1*† Aurélien Callaud1
Aurélien Callaud1 Thibaut Carsuzaa1Thomas Chalopin2
Thibaut Carsuzaa1Thomas Chalopin2 Maria-Joao Santiago-Ribeiro1,3
Maria-Joao Santiago-Ribeiro1,3
TEMPI syndrome (TEMPI) compounds telangiectasias and polycythemia with elevated erythropoietin levels, monoclonal gammopathy, perirenal fluid collections, and intrapulmonary shunt. Although the pathophysiology of this syndrome remains unclarified, prior research has been established that it is a plasma cell neoplasm, often containing less than 10% bone marrow plasma cells. 18F-FDG PET serves as a valuable instrument for initial staging and treatment monitoring in multiple myeloma management. Thus, 18F-FDG PET can be legitimately applied for TEMPI assessment. Here, we present the first 18F-FDG PET images for the initial evaluation and treatment monitoring of TEMPI in a 51-year-old woman, who exhibited polycythemia (EPO:5,448 mIU/ml) without JAK2 mutation, telangiectasias, monoclonal IgG lambda gammopathy (13.9) g/L and 7% dysmorphic plasma cells (CD38 + CD138+), occasionally clustered, in favor of tumoral plasmacytomas. The first PET scan exhibited hypermetabolic diffuse bone marrow, potentially related to polycythemia, accompanied by non-lytic bone hypermetabolic lesions in the femoral and humeral diaphysis, and ametabolic peri-renal fluid collections, brown fat, and pleural talcoma. Post-treatment 18F-FDG PET (Daratumumab Bortezomib Thalidomide Dexamethasone) revealed a completely reduced signal of bone lesions, suggesting a complete response, which was substantiated both clinically and biologically, with the concurrent disappearance of telangiectasia and the monoclonal component, and the normalization of the EPO level. In future, additional data will be required to confirm the added value of 18F-FDG PET with TEMPI. Nevertheless, 18F-FDG PET can be a preferred tool for the extension workup and therapeutic evaluation of TEMPI syndrome.
We’re discussing here a TEMPI syndrome case, which is a condition characterised by a syndrome compound by telangiectasias and polycythemia with elevated erythropoietin levels, monoclonal gammopathy, perirenal fluid collections, and intrapulmonary shunt (1–4). Although the pathophysiology of this syndrome remains unclarified, prior research has been established that it is a plasma cell neoplasm, often containing less than 10% bone marrow plasma cells. 18F-FDG PET serves as a valuable instrument for initial staging and treatment monitoring in multiple myeloma management. Thus, 18F-FDG PET can be legitimately applied for TEMPI assessment.
Here, we present the first 18F-FDG PET images for the initial evaluation and treatment monitoring of TEMPI in a 51-year-old woman, with history of splenic artery thrombosis in 2017, leading to the discovery of JAK2-negative polycythemia, with monoclonal IgG lambda gammopathy (13.9 g/L), low bone marrow plasmacytosis (5%), and telangiectasias leading to the diagnosis of TEMPI syndrome with 3 major criteria and one minor criteria (2). No exploration for shunt were performed at this time, and pluri-disciplinary decision was made for surveillance with anticoagulant therapy only. In October 2021, the patient presented fever spikes and suspected pneumopathy leading to hospitalization, with persistent telangiectasias and a preserved general condition. She exhibited polycythemia (EPO:5,448 mUI/ml) and a plasmacytosis at 7% with 0.23% of dysmorphic plasma cells (CD38 + CD138 +), occasionally clustered, in favor of tumoral plasma cells (5). A first 18F-FDG PET scan was performed for infectious etiological assessment, and it exhibited hypermetabolic diffuse bone marrow, potentially related to polycythemia, accompanied by non-lytic bone hypermetabolic lesions in the femoral and humeral diaphysis, ametabolic peri-renal fluid collections, brown fat, and pleural talcoma (Figure 1: maximal intensity projection (MIP) (A), sagittal PET (B), fusion (C), and CT (D)). These lesions were similar to lesions associated to bone marrow hyperplasia (6), lymphomas, myelomas, POEMS syndrome (7) or other hematologic malignancy (8), but through the overall clinical presentation, its character direcly related to TEMPI was retained. Thus, considering anemia and hypermetabolic foci, pluridisciplinary decision was made to initiate a treatment with 6 cycles of Daratumumab (1,800 mg), Bortezomib (2.25 mg), Thalidomide (100 mg) and Dexamethasone (40 mg) (9–11) (D-VTD treatment). It was started in November 2021, for 6 cycle each 3 weeks, and stopped in August 2022, without any severe side effect, adverse or unanticipated events.
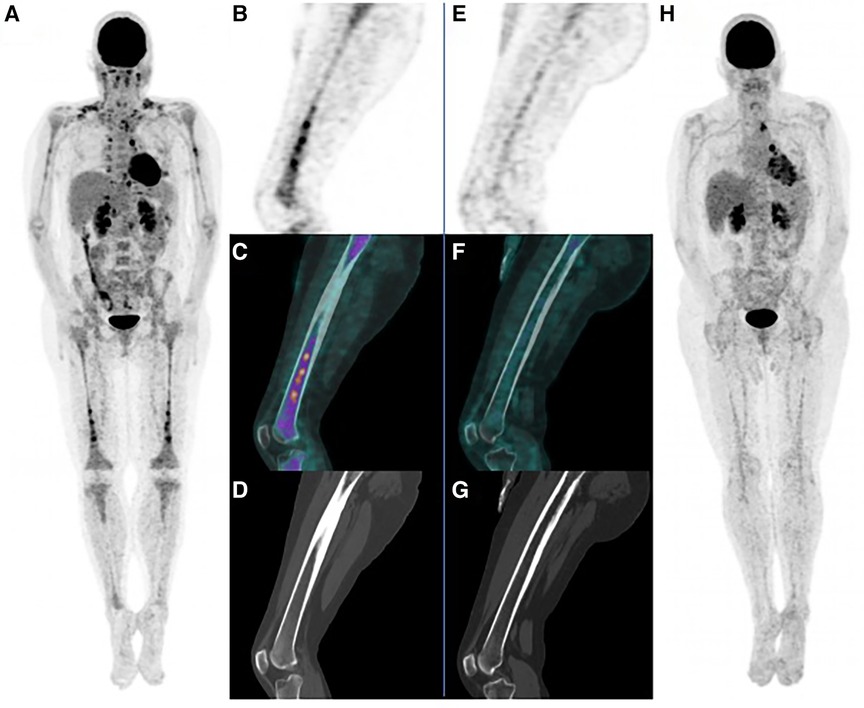
Figure 1. First PET scan with maximal intensity projection (MIP) (A), sagittal PET (B), fusion (C), and CT (D). Final post treatment PET scan with MIP (H), sagittal PET (E), fusion (F), and CT (G), showing completely reduced signal of bone lesions, and almost complete peri-renal collection response.
In September 2022, a post-treatment 18F-FDG PET was performed to evaluate metabolic lesions response to treatment. showed a completely reduced signal of bone lesions, suggesting a complete response (Figure 1: MIP (H), sagittal PET (E), fusion (F), and CT (G)), which was substantiated both clinically and biologically, with the concurrent disappearance of telangiectasia and the monoclonal component, and the normalization of the EPO level (12). Peri-renal collection had an almost complete response with only a thin strip of left perirenal non hypermetabolic effusion remaining.
Chronology of markers and SUVmax evolution during treatment is summarized in Figure 2. There is a need for additional data, that will be required to confirm the potential added value of 18F-FDG PET with TEMPI. Nevertheless, 18F-FDG PET can be a preferred tool for the extension workup and therapeutic evaluation of TEMPI syndrome. The patient was reassured by the hypermetabolic lesion's disappearance on 18F-FDG PET scan, with a reported added value for her, compared with only clinical and biological assessment.

Figure 2. Timeline.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
HP: Formal analysis, Writing – original draft, Writing – review & editing. AC: Writing – original draft, Writing – review & editing. TBC: Writing – original draft, Writing – review & editing. TC: Data curation, Writing – review & editing. MS-R: Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author MS-R declared that he was an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Xu Z-F, Ruan J, Chang L, Wu S, Lin J, Wang W, et al. Case report: TEMPI syndrome: report of three cases and treatment follow-up. Front Oncol. (2022) 12:949647. doi: 10.3389/fonc.2022.949647
2. Sykes DB, Schroyens W, O’Connell C. The TEMPI syndrome–a novel multisystem disease. N Engl J Med. (2011) 365:475–7. doi: 10.1056/NEJMc1106670
3. Sykes DB, O’Connell C, Schroyens W. The TEMPI syndrome. Blood. (2020) 135:1199–203. doi: 10.1182/blood.2019004216
4. Xu J, Liu W, Fan F, Zhang B, Zhao F, Hu Y, et al. TEMPI syndrome: update on clinical features, management, and pathogenesis. Front Endocrinol (Lausanne). (2022) 13:886961. doi: 10.3389/fendo.2022.886961
5. Zhang X, Fang M. TEMPI syndrome: erythrocytosis in plasma cell dyscrasia. Clin Lymphoma Myeloma Leuk. (2018) 18:724–30. doi: 10.1016/j.clml.2018.07.284
6. Kwee TC, De Klerk JMH, Nix M, Heggelman BGF, Dubois SV, Adams HJA. Benign bone conditions that may be FDG-avid and mimic malignancy. Semin Nucl Med. (2017) 47:322–51. doi: 10.1053/j.semnuclmed.2017.02.004
7. Pan Q, Li J, Li F, Zhou D, Zhu Z. Characterizing POEMS syndrome with 18F-FDG PET/CT. J Nucl Med. (2015) 56:1334–7. doi: 10.2967/jnumed.115.160507
8. Adams HJA, De Klerk JMH, Heggelman BGF, Dubois SV, Kwee TC. Malignancy rate of biopsied suspicious bone lesions identified on FDG PET/CT. Eur J Nucl Med Mol Imaging. (2016) 43:1231–8. doi: 10.1007/s00259-015-3282-4
9. Kwok M, Korde N, Landgren O. Bortezomib to treat the TEMPI syndrome. N Engl J Med. (2012) 366:1843–5. doi: 10.1056/NEJMc1202649
10. Kawamura S, Tamaki M, Nakamura Y, Kawamura M, Takeshita J, Yoshino N, et al. Successful treatment of the TEMPI syndrome with pomalidomide plus dexamethasone followed by autologous stem cell transplantation. Acta Haematol. (2022) 145:553–9. doi: 10.1159/000525056
11. Undar L, Atas U, Iltar U, Salim O, Yucel OK, Alpsoy E. Long-term complete clinical and hematological response with bortezomib: the report of a case with TEM(P)I syndrome and a review of the literature. Clin Lymphoma Myeloma Leuk. (2022) 22:702–7. doi: 10.1016/j.clml.2022.04.018
Keywords: TEMPI, 18F-FDG, PET, multifocal hypermetabolic bone lesions, case report
Citation: Pasquesoone H, Callaud A, Carsuzaa T, Chalopin T and Santiago-Ribeiro M-J (2023) First use of 18F-FDG PET in TEMPI syndrome: can it be used for treatment assessment? A case report. Front. Nucl. Med. 3:1273967. doi: 10.3389/fnume.2023.1273967
Received: 7 August 2023; Accepted: 3 October 2023;
Published: 26 October 2023.
Edited by:
Ismaheel Lawal, Emory University, United StatesReviewed by:
Stuart More, University of Cape Town, South Africa© 2023 Pasquesoone, Callaud, Carsuzaa, Chalopin and Santiago-Ribeiro. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Henri Pasquesoone aGVucmkucGFzcXVlc29vbmVAZ21haWwuY29t
†ORCID Henri Pasquesoone orcid.org/0009-0001-4892-6692
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.