 Sebastian J. Stolte
Sebastian J. Stolte Hanna Geiger1,†
Hanna Geiger1,† Flavio Forrer
Flavio Forrer Joachim Müller
Joachim Müller
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Nucl. Med. , 17 May 2023
Sec. PET and SPECT
Volume 3 - 2023 | https://doi.org/10.3389/fnume.2023.1150143
Intraosseous hibernoma (IOH) mimicking osseous metastasis is a rare and little-known pitfall in nuclear medicine and radiology. Referring to a clinical case, we show imaging features in FDG-PET and CT as well as pathological characteristics and discuss MRI and differential diagnoses. A 73-year-old woman was assigned for an FDG-PET/CT examination after the incidental finding of a suspicious pulmonary nodule. The FDG-PET/CT examination detected a small slightly FDG-avid pulmonary nodule suspicious for malignancy and a small slightly sclerotic lesion with mild FDG-uptake in the upper pubic bone. Histopathology revealed an intraosseous hibernoma, a rare benign soft-tissue tumor arising from brown fat. In the sparse literature available, intraosseous hibernomas may or may not be positive on bone scans. As in our case, most are slightly sclerotic on CT but lytic lesions have also been described. On MRI, they are T1 hypointense to subcutaneous fat and hyperintense to skeletal muscle; they are usually T2 hyperintense and may show peripheral contrast enhancement. According to the literature, IOHs are mostly incidental findings with solitary lesions in the spine, pelvis, ribs, or, very rarely, in the extremities with low to moderately increased glucose metabolism. IOHs present as painless tumors in general; a few painful cases could be successfully treated with radiofrequency ablation or surgery. Differential diagnoses include metastases, lymphoma, fibrous dysplasia, and non-ossifying fibroma among others. Intraosseous hibernoma is a rare benign tumor that can mimic metastases in FDG-PET, CT, bone scan, and MRI. IOHs might be indistinguishable from metastases or malignant lesions, which makes a biopsy or follow-up mandatory in clinically relevant cases. Given the benign nature of IOHs, radiofrequency ablation or surgery is only an option in symptomatic cases.
It is well known that F-18-FDG (fluorodeoxyglucose) is far from being tumor-specific; nevertheless, FDG is the most commonly used PET tracer in nuclear medicine today. Many benign pathologies or anomalies in FDG-PET/CT can be, with some certainty, distinguished from metastases by their location, CT morphology, or distribution, such as sarcoidosis or activated brown adipose tissue. We present a rare pitfall in FDG-PET/CT that is not very well known and is difficult to distinguish from osseous metastases: intraosseous hibernoma (IOH), a rare benign tumor consisting of brown adipose tissue. In our case, the IOH appeared as a roundish sclerotic lesion with mild FDG-uptake, initially suspicious for metastasis. In the sparse literature available, intraosseous hibernomas may or may not be positive on bone scans. As in our case, most are slightly sclerotic on CT but lytic lesions have also been described (1). On MRI, they are T1 hypointense to subcutaneous fat and hyperintense to skeletal muscle; they are usually T2 hyperintense and may show peripheral contrast enhancement (2). On FDG-PET/CT, they have a low to moderately increased FDG-uptake (3). IOHs are mostly asymptomatic; nevertheless, radiofrequency ablation (RFA) and surgery are described in painful cases (2).
A 73-year-old woman was assigned for an FDG-PET/CT examination after the incidental finding of a suspicious pulmonary nodule in a CT examination performed because of prolonged dyspnea in the context of an infection-related chronic obstructive pulmonary disease exacerbation without clinical improvement after 8 days of Prednisone therapy.
FDG-PET/CT revealed a small slightly FDG-avid pulmonary nodule in the upper lobe of the left lung with spiculated margins suspicious for malignancy, which later turned out to be a non-small-cell lung carcinoma. There was no evidence for FDG-avid or enlarged lymph nodes but a small, slightly sclerotic lesion with mild FDG-uptake (SUVmax 3.2) in the upper left pubic bone was detected (Figure 1). After finding adenocarcinoma metastases in a primarily unsuspicious infracarinal lymph node, the thoracic tumor board opted for a biopsy of the bone lesion. Histological work-up found regular hematopoietic bone marrow with an accumulation of moderately big, foamy cells with central small and inconspicuous nuclei (Figure 2). The possibility of foamy macrophages was ruled out in regard to their negativity for histiocyte markers CD11c and CD68.
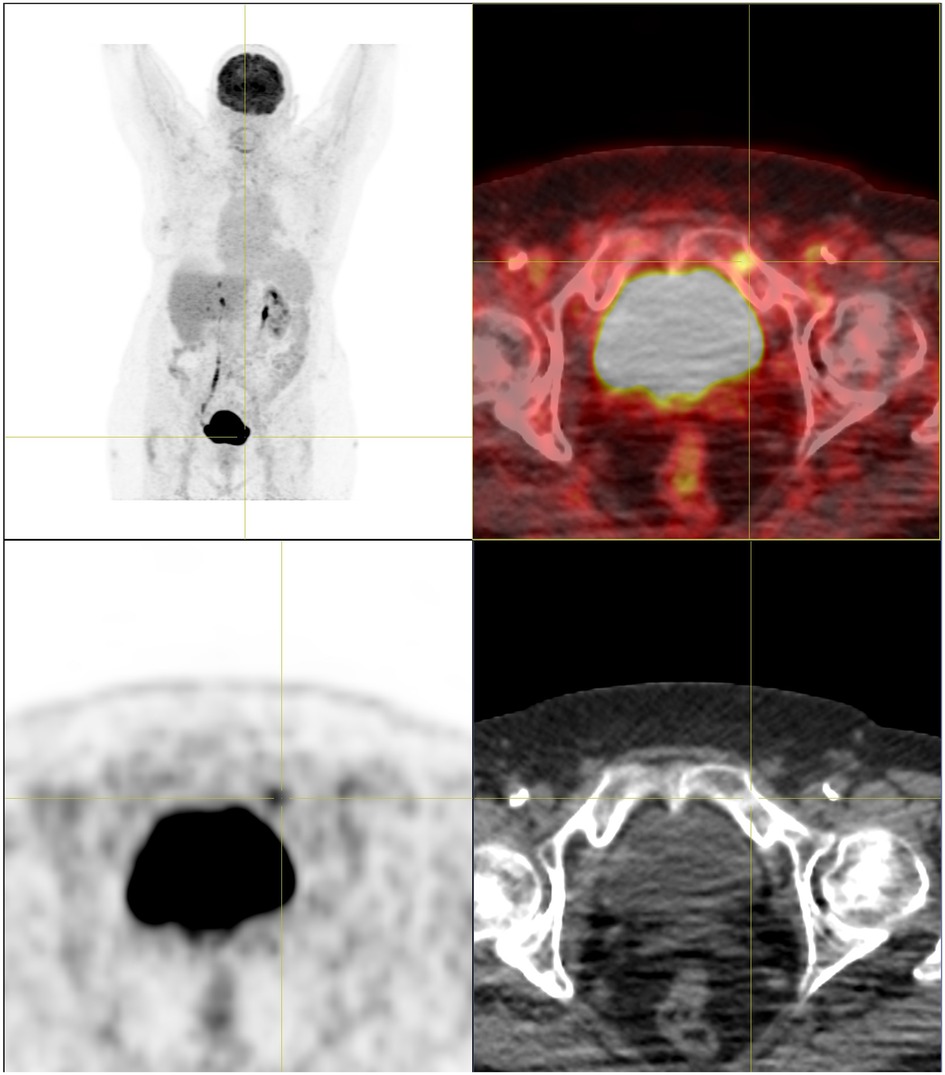
Figure 1. FDG-PET/CT. Roundish sclerosing lesion with low FDG-uptake in the upper left pubic branch.
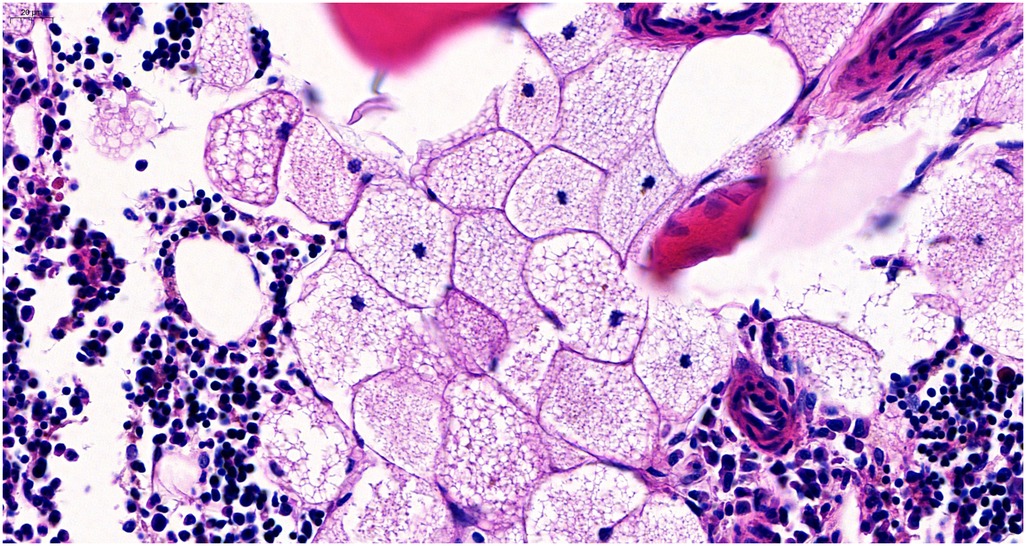
Figure 2. Histology. Histopathologic examination revealed brown fat cells in the bone marrow, solitary and with focal clustering. The cells typically show multiple small cytoplasmic vacuoles with a central, small nucleus slightly deformed by the homogeneous, small fat vacuoles. Bone remodeling or stromal changes could not be shown.
The nodule was finally diagnosed as an IOH, a rare benign soft-tissue tumor composed of brown adipose tissue, which was indistinguishable from metastases during imaging.
The hibernoma is named after the brown adipose tissue that can be found in hibernating (winter-sleeping) animals (4). The brown adipose tissue is important for thermoregulation and is normally found in the head and neck region, paravertebral of the thoracic spine, and even in the region of the adrenal glands, predominantly in infants and young adults but can also be found in adults up to the ages of 40–50 years. When activated, as a response to the sympathetic activation via norepinephrine, the cells metabolize lipids and glucose, which consequently makes them avid for FDG (5).
The soft-tissue hibernoma is an uncommon but actually well-known tumor and is predominantly located in the subcutaneous and (less frequently) muscle tissue (6–8).
A hibernoma in general is a rare finding (9), first described in around 1906, with its function discovered later in 1914 (2). Intraosseous hibernoma, in contrast, only recently came to light in the literature. Hence, a Medline search revealed only 19 publications, nearly all of them being case reports, with 27 cases; a few more can be found in Google Scholar.
Lesion localizations are mostly in the spine and pelvis but also in the ribs and rarely in the extremities. Only one case report described two lesions in one patient; the other cases have been solitary lesions.
They are usually found incidentally during medical imaging for other reasons, mostly for the staging of carcinomas or orthopedic symptoms. That may be why the typical age of diagnosis is 40–85 years (10). IOHs are generally considered to be painless tumors, although they might occasionally present with pain. Surgery and radiofrequency ablation have been described only in three symptomatic patients.
Differential diagnoses include metastases, lymphoma, degenerative changes (e.g., sclerotic lesions at the iliosacral joint), healing fractures or bone contusions (e.g., of the ribs), fibrous dysplasia, non-ossifying fibroma, chordoma, liposarcoma, and more.
An IOH is a potential mimic of malignant lesions and can cause false-positive findings in FDG-PET scans. PET scans performed in seven reported cases showed variable metabolism, ranging from no hypermetabolism to mildly/moderately increased glucose avidity (SUV 2.5–4.6) (3). It has been hypothesized that this might be due to temperature-dependent activity of the adipocytes, with higher activity in cold temperatures and higher adrenaline levels (11).
An absolutely certain diagnosis is not possible by imaging alone. A follow-up or histological confirmation must be considered individually.
In histology, (intraosseous) hibernomas present as moderately big, foamy cells with unsuspicious nuclei and a high number of homogeneous, small lipid vacuoles, as they are found in physiological brown adipose tissue. Genetic analyses have identified some genetic alterations contributing to the development of hibernomas, such as an increase of UCP1 (3).
However, molecular criteria play a minor role in the diagnostic process as the histological morphology is fairly characteristic.
An intraosseous hibernoma is a rare benign tumor that can mimic metastases during FDG-PET, CT, bone scan, and MRI.
Even though there are benign features in medical imaging, it might be indistinguishable from metastases or malignant lesions, especially since many IOHs are found incidentally during the work-up of malignancies. Consequently, a biopsy or follow-up examination must be taken into account to exclude malignancy depending on the situation of the individual patient.
Given the benign nature of IOHs, no treatment is necessary. RFA or surgery might be an option only in symptomatic cases (with localized pain).
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethical review and approval were not required for the study on human participants in accordance with the local legislation and institutional requirements. The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
SS and HG equally contributed to the writing of the article and the conducting of the literature search under the supervision of JM. RR provided the pathological expertise and described the pathological features in our case. FF, as head of the department of nuclear medicine, also provided his expertise and contributed to the final corrections before submission. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Yahia M, Laabidi B, M'sakni I, Bougrine F, Bouziani A. Intraosseous hibernoma: a case report and review of the literature. Tunis Med. (2016) 94(8–9):622–5.
2. Bonar SF, Watson G, Gragnaniello CSeex K, Magnussen J, Earwaker J. Intraosseous hibernoma: characterization of five cases and literature review. Skeletal Radiol. (2014) 43:939–46. doi: 10.1007/s00256-014-1868-8
3. Weiss SN, Mohla A, Zhu GG, Gutowski C, Kim TWB, Amin R. Intraosseous hibernoma: two case reports and a review of the literature. Radiol Case Rep. (2022) 17(7):2477–83. doi: 10.1016/j.radcr.2022.01.079
5. Cannon B, Nedergaard J. Brown adipose tissue: function and physiological significance. Physiol Rev. (2004) 84(1):277–359. doi: 10.1152/physrev.00015.2003
6. Miettinen M. Modern soft tissue pathology, tumor and non-neoplastic conditions. Cambridge: Cambridge University Press (2010).
7. Baghaie H, Chan E, Francisco S, Rasheed H, Puhalla H. Intramuscular abdominal hibernoma: case report of a rare tumour and a review of the literature. J Surg Case Rep. (2021) 2021(2):rjaa304. doi: 10.1093/jscr/rjaa304
8. Wardelmann E, Hartmann W. Tumoren mit prädominant adipozytärer morphologie. Pathologe. (2019) 40:339–52. doi: 10.1007/s00292-019-0624-1
9. Schmidt F, Cathomas R, Stallmach T, Putora PM, Mueller J. Have you ever heard of hibernoma? A rare but important pitfall in FDG-PET/CT. Nuklearmedizin. (2010) 49(6):N71–3. doi: 10.1055/s-0038-1626519
10. Ko A, Rowell CC, Vogler JB 4th, Samoilov DE. Intraosseous hibernoma: a metastatic mimicker to consider on the differential. Radiol Case Rep. (2020) 15(12):2677–80. doi: 10.1016/j.radcr.2020.10.014
Keywords: intraosseous hibernoma, hibernoma, FDG-PET/CT, osseous metastasis, adipocytic tumor, brown fat
Citation: Stolte SJ, Geiger H, Forrer F, Rodriguez R and Müller J (2023) Case report: Intraosseous hibernoma (IOH) mimics osseous metastasis: another rare pitfall in FDG-PET-CT. Front. Nucl. Med. 3:1150143. doi: 10.3389/fnume.2023.1150143
Received: 23 January 2023; Accepted: 4 April 2023;
Published: 17 May 2023.
Edited by:
Mario Petretta, IRCCS SYNLAB SDN, ItalyReviewed by:
Jules Zhang-Yin, Clinique Sud Luxembourg, Belgium© 2023 Stolte, Geiger, Forrer, Rodriguez and Müller. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Joachim Müller am9hY2hpbS5tdWVsbGVyQGtzc2cuY2g=
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.