 Bastiaan M. Privé1*
Bastiaan M. Privé1* Constantijn H. J. Muselaers2Inge M. van Oort2Marcel J. R. Janssen1Steffie M. B. Peters1Willemijn A. M. van Gemert1Maike J. M. Uijen1Melline M. G. Schilham1
Constantijn H. J. Muselaers2Inge M. van Oort2Marcel J. R. Janssen1Steffie M. B. Peters1Willemijn A. M. van Gemert1Maike J. M. Uijen1Melline M. G. Schilham1 J. P. Michiel Sedelaar2
J. P. Michiel Sedelaar2 Harm Westdorp3
Harm Westdorp3 Niven Mehra3
Niven Mehra3 Martin Gotthardt1Jelle O. Barentsz1Winald R. Gerritsen3J. Alfred Witjes2
Martin Gotthardt1Jelle O. Barentsz1Winald R. Gerritsen3J. Alfred Witjes2 James Nagarajah1
James Nagarajah1- 1Department of Radiology and Nuclear Medicine, Radboudumc, Nijmegen, Netherlands
- 2Department of Urology, Radboudumc, Nijmegen, Netherlands
- 3Department of Medical Oncology, Radboudumc, Nijmegen, Netherlands
177Lu-PSMA-617 radioligand therapy is a novel treatment for end-stage prostate cancer, which could also be applied to patients with hormone-sensitive prostate cancer with high expression levels of prostate-specific membrane antigen (PSMA). In this perspective, we review the recent results of toxicity, radiation doses, and treatment effect of 177Lu-PSMA in patients with low volume metastatic hormone-sensitive prostate cancer. Moreover, we present long-term follow-up data, such as toxicity and time without androgen deprivation therapy (ADT), of the patients who participated in this trial. Overall, 177Lu-PSMA appeared to be a feasible and safe treatment modality in this setting, as well as in long-term follow-up. We observed that men with a prostate-specific antigen (PSA) response of more than 50% seemed to especially benefit from this therapy by postponing ADT and thus preserving the quality of life.
Perspective
Between 27 and 53% of patients with prostate cancer undergoing radical surgery or external beam radiotherapy (EBRT) will develop disease recurrence (1). If salvage surgery or EBRT is no option, androgen deprivation therapy (ADT) is recommended, particularly in patients with high prostate-specific antigen (PSA) velocity (e.g., PSA doubling time <6 months) (1). Despite favorable responses to ADT and novel drug combinations, there is an increasing interest in metastases-directed therapies (MDT) for oligometastatic disease, mainly because these treatments can postpone ADT-related side effects and thus preserve a good quality of life (1–4). Therefore, there is a need for more treatment options to control recurrent tumor progression while maintaining a good quality of life.
[177Lu]Lu-PSMA-617 (177Lu-PSMA) radioligand therapy is a novel treatment for patients with end-stage castrate-resistant prostate cancer (mCRPC) with promising efficacy and acceptable toxicity profile (5–8). This has resulted in an international registration trial for use of 177Lu-PSMA in patients with mCRPC, which recently reported positive outcomes with a 30–40% reduction in death from any cause (9). However, 177Lu-PSMA was yet unexplored in the (metastatic) hormone-sensitive setting (mHSPC). Recently, we evaluated if 177Lu-PSMA could become a potential effective MDT for patients with mHSPC harboring low tumor load (≤ 10 metastases on [68Ga]Ga-PSMA-PET imaging [PSMA-PET]) in a prospective pilot study (10). This article reports on long-term follow-up data, including toxicity, progression-free survival, and time without ADT.
All study procedures and in- and exclusion criteria were previously described (10). In short, men (age > 50 years) with histologically proven prostate cancer (PCa) and progressive disease after local therapy (PSA > 0.2 μg/l), with a PSA doubling time of <6 months and no curable treatment options left (e.g., surgery or external beam radiotherapy), were eligible for this trial. Moreover, patients needed to have low volume metastatic disease (≥1 but ≤ 10 positive lesions) on PSMA-PET with high tumor prostate-specific membrane antigen (PSMA) uptake. At the start of the study, none of the patients were allowed to use ADT. The study was approved by the Medical Review Ethics Committee Region Arnhem-Nijmegen (NL62774.091.17), was registered on clinicaltrials.gov (NCT03828838), and performed in accordance with the principles of Good Clinical Practice and the Declaration of Helsinki. The included patients received two cycles containing 3 and ~6 GBq 177Lu-PSMA 8 weeks in between. Patients were monitored up to 6 months after the last cycle. After the study, patients had regular appointments with their treating oncologist, including laboratory testing for PSA. The progression-free survival was reported following Prostate Cancer Working Group (PCWG3), wherein the time from the start of therapy to the date of first PSA had an increase of ≥25% and ≥2 ng/ml from nadir or date of start systemic treatment.
Since the start of treatment with 177Lu-PSMA-617, the median long-term follow-up of the cohort was 28 months (range 11–39 months). At this time, the median progression-free survival was 11 months (range 4–39 months). In line with this, the median androgen deprivation-free survival of the studied cohort was 16 months (range 7–39 months). Importantly, three of the ten patients are still postponing ADT (median 29 months [range 28–39 months]) (Figure 1). Prior to inclusion, all patients had PSA-doubling time <6 months. However, all of the patients showed a stabilization of the PSA-increase velocity following [177Lu]Lu-PSMA-617, with five of ten patients achieving a PSA decline of > 50% (Figure 1). The five patients with a >50% PSA response showed a longer ADT-free survival compared to patients with a <50% PSA response (Figure 1).
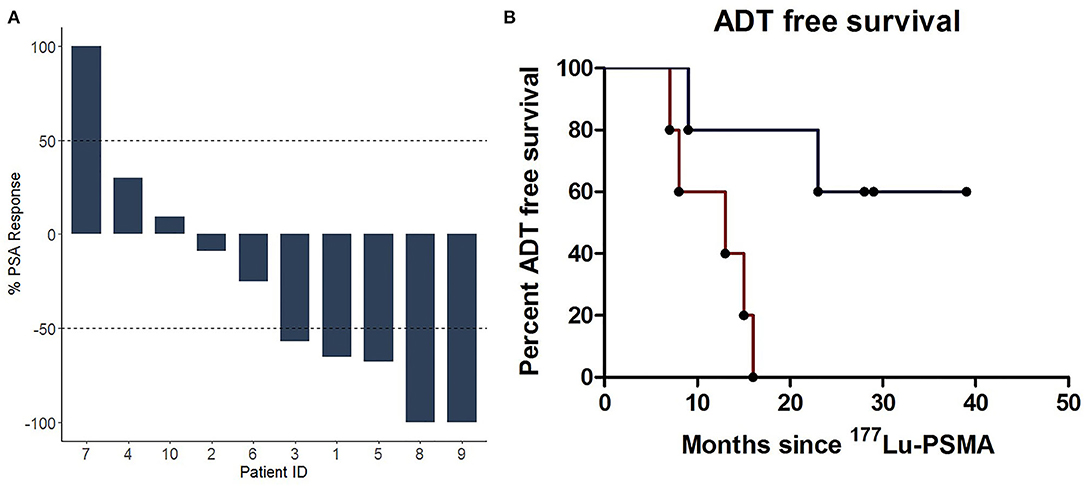
Figure 1. (A) Waterfall plot of the best prostate-specific antigen (PSA) response after two cycles of 177Lu-PSMA. (B) Kaplan-Meier plot showing the time without testosterone suppressing drugs (e.g., dutasteride, bicalutamide, LHRH agonists/antagists, enzalutamide, and abiraterone) grouped according to their PSA response. ADT, androgen deprivation therapy; LHRH, gonadotropin-releasing hormone; PSA, Prostate Specific Antigen; PSMA, Prostate Specific Membrane Antigen.
Following the two cycles of 177Lu-PSMA, none of the ten patients had severe treatment-related toxicities, and even the grades I-II toxicities (e.g., fatigue) recovered within a few weeks (10). Importantly, only mild and transient xerostomia was reported. Additionally, during long-term follow-up, none of the patients developed a dry mouth. However, one patient died 11 months after the study due to a cerebral vascular incident. This was deemed unrelated to 177Lu-PSMA-617 but may have been associated with the ADT that was started following the study. No clinically relevant changes in quality of life were observed applying a standardized questionnaire (EORTC QLQ-C30) before and after treatment of 177Lu-PSMA-617. In accordance with these outcomes, the dosimetry showed that patients could receive higher doses of 177Lu-PSMA and up to 38 GBq of 177Lu-PSMA-617 before organ-related toxicity occurred in this early setting (11). Importantly, doses to tumor lesions were consistently higher compared to the doses to the organs at risk (salivary glands, kidneys, and bone marrow).
Although the study consisted of a small cohort of selected patients, the results suggest a favorable outcome after 177Lu-PSMA in approximately half of the patients. These findings have encouraged us to initiate a larger prospective randomized multicenter study to provide stronger evidence for first-line 177Lu-PSMA in patients with oligometastatic mHSPC (e.g., NCT04443062) (12).
To conclude, 177Lu-PSMA appeared to be a feasible and safe treatment modality in low volume metastatic hormone-sensitive prostate cancer patients, also at long-term follow-up. In particular, those men with a PSA response of more than 50% seemed to benefit from this therapy by postponing ADT and preserving good quality of life.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Statement
The studies involving human participants were reviewed and approved by Medical Review Ethics Committee Arnhem-Nijmegen. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
BP, CM, JW, and JN: conceptualization. BP, SP, CM, IO, MJ, WG, NM, JB, MG, JW, and JN: methodology. BP, SP, and JN: formal analysis and data curation. BP, CM, IO, MJ, MU, MS, WGem, HW, NM, JB, MG, JW, and JN: resources. BP and JN: writing—original draft preparation and visualization. BP, CM, IO, SP, MJ, JS, HW, NM, WGem, JB, MG, JW, and JN: writing—review and editing. WGer, JW, and JN: supervision. BP, SP, CM, and JN: project administration. MJ, WGer, JW, and JN: funding acquisition. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by the Radboud Oncology Foundation and the Dutch Prostate Cancer Foundation (Prostaatkankerstichting).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We thank all the investigators of the study, the patients, and their families.
References
1. Cornford P, van den Bergh RCN, Briers E, Van den Broeck T, Cumberbatch MG, De Santis M, et al. EAU-EANM-ESTRO-ESUR-SIOG Guidelines on Prostate Cancer. Part II-2014-2020 Update: Treatment of Relapsing and Metastatic Prostate Cancer. Eur Urol. (2021) 79:263–82. doi: 10.1016/j.eururo.2020.09.046
2. Ost P, Reynders D, Decaestecker K, Fonteyne V, Lumen N, De Bruycker A, et al. Surveillance or metastasis-directed therapy for oligometastatic prostate cancer recurrence: a prospective, randomized, multicenter phase II trial. J Clin Oncol. (2018) 36:446–53. doi: 10.1200/JCO.2017.75.4853
3. Isbarn H, Boccon-Gibod L, Carroll PR, Montorsi F, Schulman C, Smith MR, et al. Androgen deprivation therapy for the treatment of prostate cancer: consider both benefits and risks. Eur Urol. (2009) 55:62–75. doi: 10.1016/j.eururo.2008.10.008
4. Phillips R, Shi WY, Deek M, Radwan N, Lim SJ, Antonarakis ES, et al. Outcomes of observation vs stereotactic ablative radiation for oligometastatic prostate cancer: the ORIOLE phase 2 randomized clinical trial. JAMA Oncol. (2020) 6:650–9. doi: 10.1001/jamaoncol.2020.0147
5. Hofman MS, Violet J, Hicks RJ, Ferdinandus J, Thang SP, Akhurst T, et al. [(177)Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): a single-centre, single-arm, phase 2 study. Lancet Oncol. (2018) 19:825–33. doi: 10.1016/S1470-2045(18)30198-0
6. Heck MM, Tauber R, Schwaiger S, Retz M, D'Alessandria C, Maurer T, et al. Treatment outcome, toxicity, and predictive factors for radioligand therapy with 177Lu-PSMA-I T in metastatic castration-resistant prostate cancer. Eur Urol. (2019) 75:920–6. doi: 10.1016/j.eururo.2018.11.016
7. Hofman MS, Emmett L, Sandhu S, Iravani A, Joshua AM, Goh JC, et al. [177Lu]Lu-PSMA-617 versus cabazitaxel in patients with metastatic castration-resistant prostate cancer (TheraP): a randomised, open-label, phase 2 trial. Lancet. (2021) 397:797–804. doi: 10.1016/S0140-6736(21)00237-3
8. Privé BM, Slootbeek PHJ, Laarhuis BI, Naga SP, van der Doelen MJ, van Kalmthout LWM, et al. Impact of DNA damage repair defects on response to PSMA radioligand therapy in metastatic castration-resistant prostate cancer. Prostate Cancer Prostatic Dis. (2021) 1–8. doi: 10.1038/s41391-021-00424-2
9. Sartor O, de Bono J, Chi KN, Fizazi K, Herrmann K, Rahbar K, et al. Lutetium-177–PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. (2021). doi: 10.1056/NEJMoa2107322
10. Privé BM, Peters SMB, Muselaers CHJ, van Oort IM, Janssen MJR, Sedelaar M, et al. Lutetium-177-PSMA-617 in low-volume hormone sensitive metastatic prostate cancer, a prospective pilot study. Clin Cancer Res. (2021) 27:3595–601. doi: 10.1055/s-0040-1708448
11. Peters SMB, Privé BM, de Bakker M, de Lange F, Jentzen W, Eek A, et al. Intra-therapeutic dosimetry of [177Lu]Lu-PSMA-617 in low-volume hormone-sensitive metastatic prostate cancer patients and correlation with treatment outcome. Eur J Nuclear Med Mol Imaging. (2020) 20:884. doi: 10.1007/s00259-021-05471-4
Keywords: hormone sensitive, prostate cancer, lutetium-177-PSMA-617, radioligand therapy, urologic oncology, metastases-directed therapies
Citation: Privé BM, Muselaers CHJ, van Oort IM, Janssen MJR, Peters SMB, van Gemert WAM, Uijen MJM, Schilham MMG, Sedelaar JPM, Westdorp H, Mehra N, Gotthardt M, Barentsz JO, Gerritsen WR, Witjes JA and Nagarajah J (2022) An Update to the Pilot Study of 177Lu-PSMA in Low Volume Hormone-Sensitive Prostate Cancer. Front. Nucl. Med. 2:863101. doi: 10.3389/fnume.2022.863101
Received: 26 January 2022; Accepted: 16 March 2022;
Published: 03 May 2022.
Edited by:
Markus Luster, University of Marburg, GermanyReviewed by:
Francesco Ceci, European Institute of Oncology (IEO), ItalyCopyright © 2022 Privé, Muselaers, van Oort, Janssen, Peters, van Gemert, Uijen, Schilham, Sedelaar, Westdorp, Mehra, Gotthardt, Barentsz, Gerritsen, Witjes and Nagarajah. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bastiaan M. Privé, YmFzdGlhYW4ucHJpdmVAcmFkYm91ZHVtYy5ubA==