 Vincent Rebière1
Vincent Rebière1 Meriem Maajem2
Meriem Maajem2 Ronan Le Calloch3
Ronan Le Calloch3 Leela Raj4
Leela Raj4 Anne-Sophie Le Bris5Mohamed Malou6François Salmon7
Anne-Sophie Le Bris5Mohamed Malou6François Salmon7 Isabelle Quintin-Roué8
Isabelle Quintin-Roué8 Adrian Tempescul1
Adrian Tempescul1 David Bourhis2Laura Samaison9
David Bourhis2Laura Samaison9 Hussam Saad1
Hussam Saad1 Pierre-Yves Salaun2Christian Berthou1Jean-Christophe Ianotto1
Pierre-Yves Salaun2Christian Berthou1Jean-Christophe Ianotto1 Ronan Abgral2
Ronan Abgral2 Jean-Richard Eveillard1*
Jean-Richard Eveillard1*- 1Department of Hematology, Brest University Hospital, Brest, France
- 2Department of Nuclear Medicine, Brest University Hospital, Brest, France
- 3Department of Internal Medicine, Blood and Infectious Diseases, Cornouaille Hospital Center, Quimper, France
- 4Faculty of Health Science, McMaster University, Hamilton, ON, Canada
- 5Department of Internal Medicine, Michel Mazéas Hospital Center, Douarnenez, France
- 6Department of Hematology and Oncology, Morlaix Hospital Center, Morlaix, France
- 7Department of Nuclear Medicine, Cornouaille Hospital Center, Quimper, France
- 8Department of Anatomo-Pathology, Brest University Hospital, Brest, France
- 9Department of Anatomo-Pathology, Cornouaille Hospital Center, Quimper, France
Currently, prognostic models in diffuse large B-cell lymphoma (DLBCL) fail to closely reflect patients' biological, clinical, and survival heterogeneity. We, therefore, assessed the impact of clinical, biological, immunohistochemical (IHC), baseline (0), and interim (after 2 and 4 treatment cycles) PET (PET0, PET2, and PET4) data not yet included in any scoring system on DLBCL outcome. The analysis was conducted on 89 previously untreated adult patients of the Finistere Observatory Cohort (O.Ly.Fin) with documented DLBCL, recruited between January 2010 and December 2017, with progression-free survival (PFS) and overall survival (OS) as primary and secondary endpoints, respectively. Seventy-eight patients were treated with rituximab, cyclophosphamide, hydroxyadriamycin, vincristine, and prednisone (R-CHOP), while 11 received R-dose-adjusted etoposide, prednisone, vincristine, cyclophosphamide, and hydroxyadriamycin (EPOCH). Patients were followed up until June 20, 2020. On multivariate analysis, Ki67 ≥ 70% on IHC (K), bulky presentation ≥7.5 cm (B), meningeal lymphomatosis (M), and PET0–PET4 ΔSUVmax <71% (P4) were identified as strong independent predictors of PFS, and all variables but bulky disease also strongly and independently predicted OS. Using these 4 parameters, we designed a scoring model named KBMP4 stratifying patients into low- (0 parameter), intermediate- (1 or 2), and high-risk (≥3) subgroups by the Kaplan–Meier analysis. At a median follow-up of 43 months, PFS and OS were both 100% in the low-risk subgroup, 71.4 and 90.5%, respectively, in the intermediate-risk subgroup, and 0 and 55.5%, respectively, in the high-risk subgroup. Use of the KBMP4 model in clinical practice may improve accuracy in prognostic prediction and treatment decisions in de novo DLBCL patients.
Introduction
Diffuse large B-cell lymphoma (DLBCL) is the most common subtype of B-cell lymphoma in western countries, accounting for 30% of non-Hodgkin's lymphomas (NHL) in adults (1). The major prognostic scores for de novo DLBCL are the International Prognostic Index (IPI) and the age-adjusted (aa) IPI for patients under 60 years (2). IPI is based on clinical and biological factors including age >60 years, Ann Arbor stage III or IV, serum lactate dehydrogenase (LDH) above the upper normal limit, Eastern Cooperative Oncology Group (ECOG) Performance Status (PS) ≥2, and >1 extranodal site involvement. Each factor is attributed one point. Patients are stratified into low (0–1 point), low-intermediate (2 points), high-intermediate (3 points), and high-risk (≥4 points) categories accordingly with respective 3-year overall survival (OS) of 91%, 81%, 65%, and 60%.
High-grade B-cell lymphomas (HGBL) are a new category of aggressive B-cell lymphomas introduced by the WHO in 2016 (1). Specifically, HGBL may be subclassified as “double hit” (DH), involving chromosomal breakpoints on MYC and BCL2 or BCL6 genes on molecular analysis, or as “triple hit” (TH), implying concomitant chromosomal breakpoints on MYC, BCL2, and BCL6 genes. In patients presenting with overexpression of MYC and BCL2 proteins on immunohistochemical (IHC) analysis, some DLBCLs not otherwise specified (NOS) have been defined as dual-expressor (DE) lymphoma. In all cases, DH, TH, and DE statuses portend a poor prognosis (3–8).
Additional evidence predicts unfavorable outcomes and chemoresistance in DLBCL patients. This includes subclassification into the germinal center (GC) or non-GC DLBCL based on the cell of origin (COO) (9–11), high SUVmax (12), high total metabolic tumor volume (TMTV) (13), and high total lesion glycolysis (TLG) (14) on baseline PET imaging and failure to reach complete metabolic response as assessed by visual [International Harmonization Project (IHP) and Deauville 5-point scale (5-PS)] (15) or semiquantitative (ΔSUVmax) methods with interim PET evaluation after 2 and 4 treatment cycles (16). Regarding interim PET, although IHP, Deauville 5-PS, and ΔSUVmax have shown significant predictive value, ΔSUVmax was reported as an independent prognostic factor and is presumed to offer more advantages (17, 18).
Despite widely recognized pathobiological heterogeneity across cases, R-CHOP (rituximab, cyclophosphamide, hydroxyadriamycin, vincristine, and prednisone) regimen remains the primary approach in most DLBCL patients as uniform first-line immunochemotherapy (19). However, while 60% of patients treated with R-CHOP are considered cured without early or late relapse, 10% are primary refractory with a very poor prognosis, and 25% of those under 65 years are considered late responders and candidates for intensification followed by autologous stem cell transplantation (ASCT) (20). Important uncertainty remains regarding the 30–35% of patients who failed to respond to R-CHOP as the first line. Infusional R-dose adjusted (DA)-EPOCH (rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and hydroxyadriamycin) regimen, once considered a better upfront option in patients with MYC-rearranged DLBCL (21), finally showed no superiority in survival to R-CHOP in this population in a recent large retrospective review (22). The optimal management of such patients remains debatable, and no reliable prognostic scoring systems based on the above-mentioned biomarkers currently exist to identify them early (23–25).
In the present study, we explored the prognostic value of several variables in DLBCL patients, including demographic, clinical, biological, and IHC data, as well as PET biomarkers at baseline and following 2 and 4 courses of immunochemotherapy. Based on our results, we designed a prognostic scoring model in DLBCL named KBMP4, which appears promising for earlier and more effective identification of patients susceptible to be unresponsive to R-CHOP.
Methods
Design
This is a retrospective multicenter observational study involving the West Brittany Inter-Hospital Federation (FIHBO) (Brest University Hospital, Quimper Hospital Center, and Douarnenez Hospital Center) and the Finistere Observatory Cohort (O.Ly.Fin).
This study was approved by our institution's ethics committee and conducted in accordance with the Declaration of Helsinki.
Eligible patients had documented de novo DLBCL (26) for which they had undergone PET at baseline and interim assessment after 2 and 4 cycles of chemotherapy.
Among 251 patients, identified consecutively from January 2010 to December 2017, 89 were eligible for inclusion in the analysis (Figure 1).
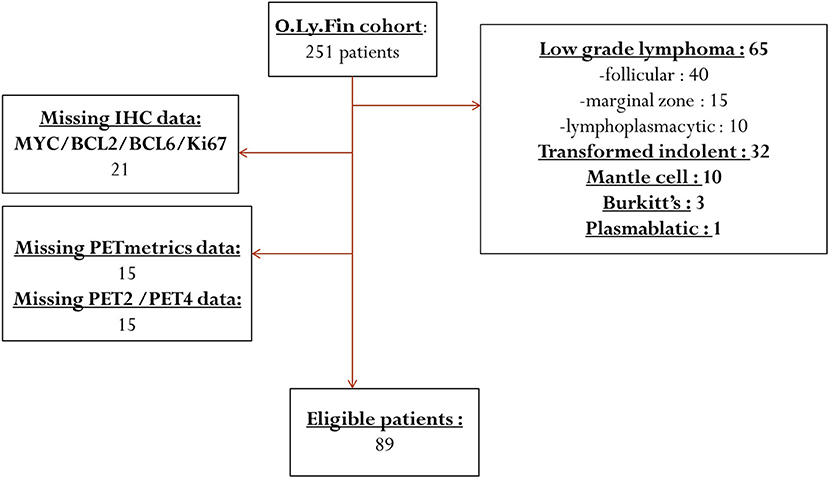
Figure 1. Flow chart of the exclusion process of initially selected patients.
Optimal treatment for each patient was determined by a board of expert clinicians based on age, PS, IPI score, and evidence of poor prognostic features (MYC-positive IHC staining, bulky presentation defined as a tumoral lesion with diameter ≥7.5 cm, and extranodal involvement).
All responding patients received 6 R-CHOP-based immunochemotherapy cycles. Patients having tested positive for MYC received R-(DA)-EPOCH.
Demographic, clinical, biological, PET, and follow-up (FU) data were collected from patient files (see Supplementary Material for details).
Patients were followed up for at least 6 months, or until the occurrence of an event, to calculate progression-free survival (PFS) and OS. Clinical FU visits were scheduled and recorded according to European Society for Medical Oncology (ESMO) guidelines (27).
Imaging Techniques and Analysis
CT was initially cranio-caudally performed with a whole-body protocol and injection of iodized contrast material (1.5 ml/kg) in the absence of contraindication. Whole-body PET/CT data were acquired in 3D mode and included both emission images (2 to 3 min per step) and transmission images required for attenuation correction (see Supplementary Material for details).
Quantitative SUV-based parameters were collected for each patient (see Online Supplementary Data for details).
PET/CT scanners in our institutions have EANM Research Ltd. (EARL) accreditation, in accordance with our policy regarding compliance with best clinical and technical guidelines, in daily practice as well as within the frame of international clinical trials.
Statistical Methods
Continuous variables were compared using Student's t-test, ANOVA, or Mann–Whitney non-parametric test. Categorical variables were compared using the chi-squared test or Fisher's exact test, as appropriate.
PFS was measured from the date of diagnosis to the date of relapse, death, or last FU. OS was calculated from the date of diagnosis to the date of death or last FU. The ΔSUVmax PET0–PET2 <66% and ΔSUVmax PET0–PET4 <71% thresholds, as defined in a recently reported phase 3 study by LYSA, were used, but we did not apply the Deauville 5-PS as recommended by the 2011 Menton workshop, as <10% of patients met the criterion of PET0 SUVmax <10 (28).
Variables significant (p < 0.10) on univariate analysis were included in the multivariate analysis. PFS and OS were calculated for all patients and for patient subgroups, divided through receiver operating characteristic (ROC) analysis, using the Kaplan–Meier survival analysis, and compared between subgroups using a log-rank test.
A multivariate Cox regression analysis was performed to test the association between variables and survival rates. All tests were two-sided, and a p < 0.05 was considered statistically significant.
Based on the results, we stratified patients into three prognostic subgroups according to the number of risk factors: 0 (A), 1 or 2 (B), or ≥3 (C).
Statistical analyses were performed using Addinsoft 2020 XLSTAT 2020.
Results
Patient Characteristics
Demographic, Clinical, Biological, and Prognostic Characteristics
Table 1 summarizes patients' baseline demographic, clinical, and biological characteristics in addition to lymphoma IHC, bio-clinical, baseline and interim PET features, and IPI-based prognostic profiles at diagnosis.
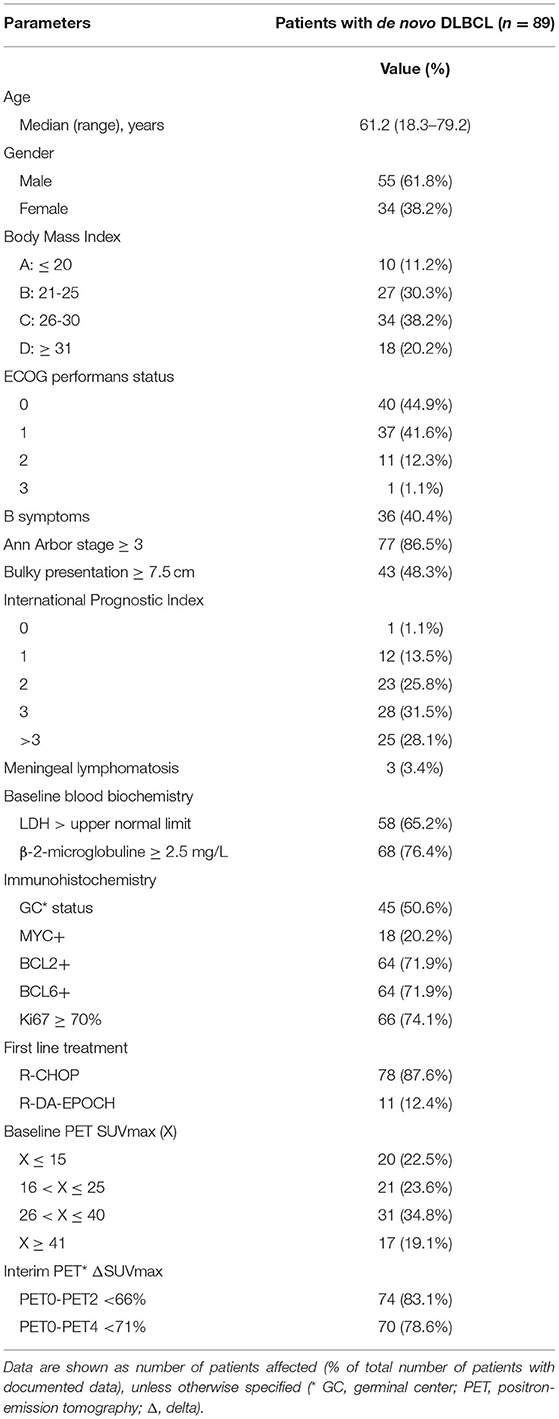
Table 1. Patients baseline demographic, clinical, biological, PET and prognostic characteristics.
Immunohistochemical Characteristics
According to the Hans algorithm, 45 patients (51.7%) had GC-subtype DLBCL. Through IHC expression, MYC was positive in 18 (20.2%), BCL2 in 64 (71.9%), and BCL6 in 64 (71.9%). Median IHC positivity for Ki67 was 80%, ranging from 20 to 100%, and in 66 patients (74.1%), Ki67 positivity was ≥70%.
PET Characteristics
The mean baseline SUVmax was 30.85, ranging from 2 to 57. Mean PET0–PET2 ΔSUV was 74.7% (0–97.4%), and 74 patients (83.1%) were above the cutoff of <66%. Mean PET0–PET4 ΔSUV was 78.1% (0–98.1%), and 70 patients (78.6%) were above the cutoff of <71%. Of note, among 19 patients whose PET0–PET4 ΔSUVmax was <71%, histological assessment and PET4 proofreading were undertaken in 6 who were in fact and are still in complete response (CR) without additional treatment, while 13 others were not in CR and underwent salvage therapy. For the avoidance of doubt in these 19 patients, the response was also assessed according to Deauville 5-PS and was reported as follows: of the six responders, 5-PS was estimated to be 5 in 1, 4 in 1, 3 in 1, and 2 in 3; of the 13 nonresponders, it was evaluated to be 5 in 6, 4 in 2, 2 in 1, and 1 in 4.
Treatment Outcome and Follow-Up
As detailed below, 84 (92%) patients responded to treatment, 76 patients were in CR following the first line, and 8 experienced CR after salvage treatment.
First-line treatment with R-CHOP in 78 patients (87.6%) and R-(DA)-EPOCH in 11 (12.4%) resulted in CR in 76 (85.4%), partial response (PR) in 6 (6.7%), and failure in 7 (7.9%). The six patients in PR proceeded to ASCT, after R-DHAP as salvage treatment in three and no salvage in three; after the procedure, two were in failure and four advanced to CR. Among the seven patients in failure, four advanced to CR: one after R-DHAP followed by ASCT as salvage strategy and three after rescue by rituximab, dexamethasone, high-dose aracytine, platinol (cisplatin) (R-DHAP), rituximab, etoposide, solumedrol, aracytine, platinol (cisplatin) (R-ESAP), and rituximab, dexamethasone, high-dose aracytine, oxaliplatin (R-DHAOX); the other three remained in failure after two or three further treatment lines. No ASCT was performed in patients over 68 years old.
Patients were followed up until June 20, 2020. Median FU was 43 months, ranging from 6.9 to 101.1 months. FU length was >36 months in 60 (67.4%), >48 months in 40 (45%), and >60 months in 26 (29.2%). No patients were lost to FU.
A total of 27 relapse events were observed. Overall median time to relapse was 8.2 months, ranging from 1.9 to 65.9. Early relapse, defined as disease recurrence within the year of diagnosis or 6 months after the end of treatment, was observed in 16 patients (59.3%), whereas late relapse, defined as disease recurrence later than 1 year after diagnosis, occurred in 11 (40.7%).
A total of 11 patients died during FU: nine from disease-related causes (five in primary failure, one in early relapse, and three in late relapse) and two from unrelated causes. Overall median time to death was 14.5 months, ranging from 6.9 to 69.8.
Survival Analysis
Progression-Free Survival
On multivariate Cox model, bulky presentation (p = 0.030), meningeal lymphomatosis (p = 0.020), Ki67 ≥ 70% (p = 0.007), and PET0–PET4 ΔSUV <71% (p = 0.005) demonstrated statistical significance for PFS (Table 2). Despite a p-value of 0.083 in univariate analysis, IPI > 2 failed to show statistical significance while aaIPI > 1, MYC status, and GC/non-GC profile were not eligible for multivariate analysis.
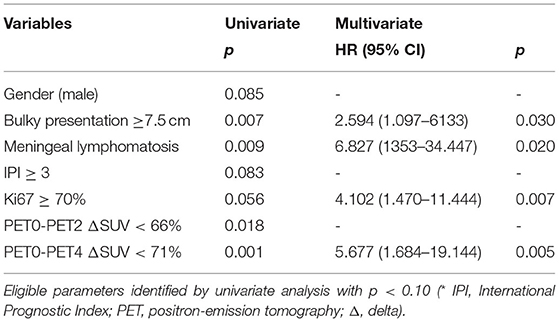
Table 2. Multivariate Cox model analysis for PFS.
Kaplan–Meier analysis showed a statistically significant difference in PFS between patients with and without bulky presentation ≥7.5 cm (p = 0.004) (Figure 2A), with and without meningeal lymphomatosis (p = 0.002) (Figure 2B), with and without Ki67 ≥ 70% (p = 0.049) (Figure 2C), and with and without PET0–PET4 ΔSUV <71% (p = 0.000) (Figure 2D). PFS at 24 months of FU (PFS24) was 65 vs. 89% in patients with or without bulky presentation, 70 vs. 87.5% in patients with or without Ki67 ≥ 70%, 0 vs 79% in patients with or without meningeal lymphomatosis, and 47.3 vs. 85.7% in patients with or without PET0–PET4 ΔSUV <71%.
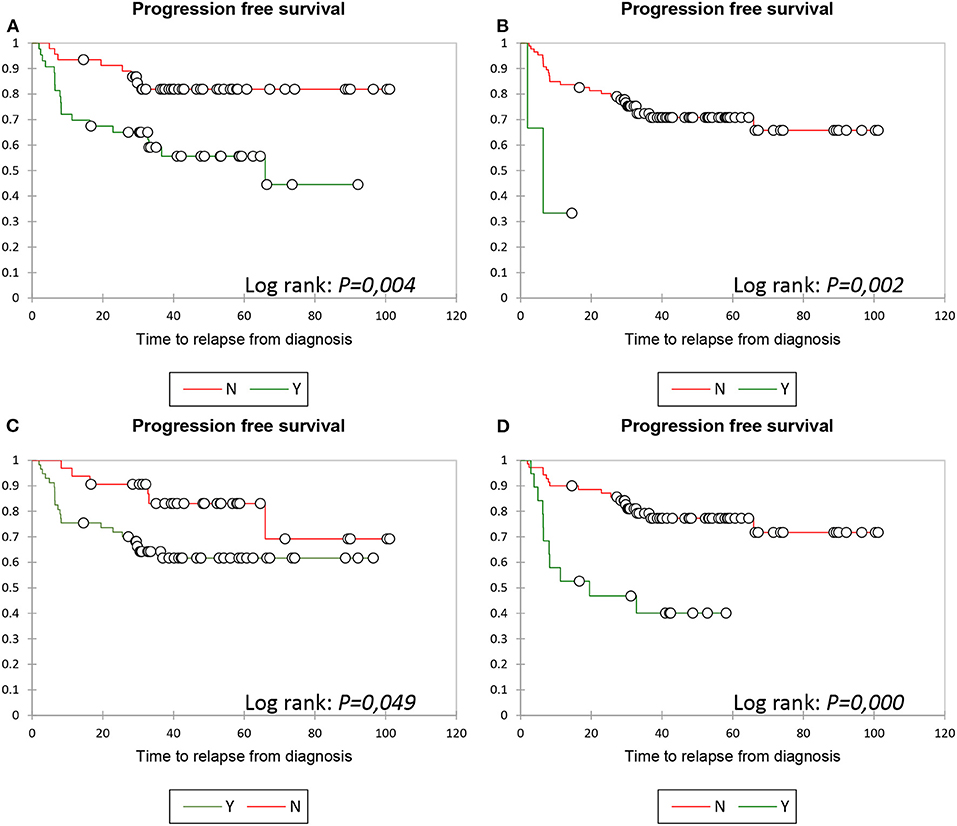
Figure 2. PFS: Kaplan Meier analysis. PFS according to bulky presentation ≥7.5 cm (A), meningeal lymphomatosis (B), Ki67 ≥70% (C) and PETO-PET4 ΔSUV <66% (D), respectively.
A prognostic scoring model, based on the identified predictors, was designed and named KBMP4 (Ki67, Bulky, Meningeal disease, PET4). No patients had all 4 parameters. With the use of Kaplan–Meier analysis (Figure 4 left), three distinct subgroups were identified based on the number of risk factors: in subgroup A (low-risk with 0 parameters), no relapse was observed in 17 patients (0%); in subgroup B (intermediate risk with 1 or 2 parameters), relapse occurred in 18/63 patients (28.6%), with a median time of 21.1 months, ranging from 2.4 to 65.9; in subgroup C (high risk with ≥3 factors), relapse was observed in 9/9 patients (100%), with a median time of 6.3 months, ranging from 1.9 to 8.2. A significant difference was noticed when subgroup A was compared to subgroup B (p = 0.014), subgroup A to group C (p < 0.0001), and subgroup B to subgroup C (p < 0.0001). PFS24 was 100% in subgroup A, 81% in subgroup B, and 0% in subgroup C.
Overall Survival
Multivariate Cox model identified age at diagnosis (p = 0.005), meningeal lymphomatosis (p = 0.000), Ki67 ≥ 70% (p = 0.007), PET0–PET2 ΔSUV <66% (p = 0.045), and PET0–PET4 ΔSUV <71% (p = 0.008) as the statistically significant parameters negatively influencing OS as shown in Table 3. Despite a p-value of 0.0041 and 0.121, respectively, in univariate analysis, MYC status and IPI > 2 failed to show statistical significance, while aaIPI > 1 and GC/non-GC profile were not eligible for multivariate analysis.
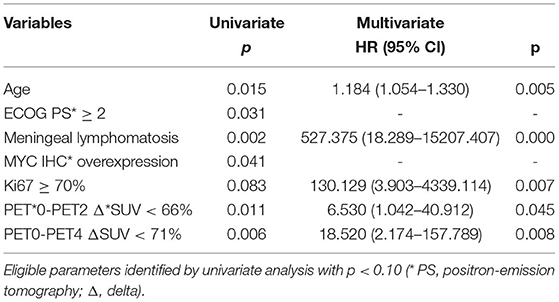
Table 3. Multivariate Cox model analysis for OS.
The Kaplan–Meier analysis showed a statistical significance in OS regarding age (p = 0.017) and a statistically significant difference between patients with or without meningeal lymphomatosis (p < 0.0001), with or without Ki67 ≥ 70% (p = 0.047), with or without PET0–PET2 (P2) ΔSUV <66% (p = 0.005), and with or without PET0–PET4 ΔSUV <71% (p = 0.002) (Figure 3; data regarding age not shown).
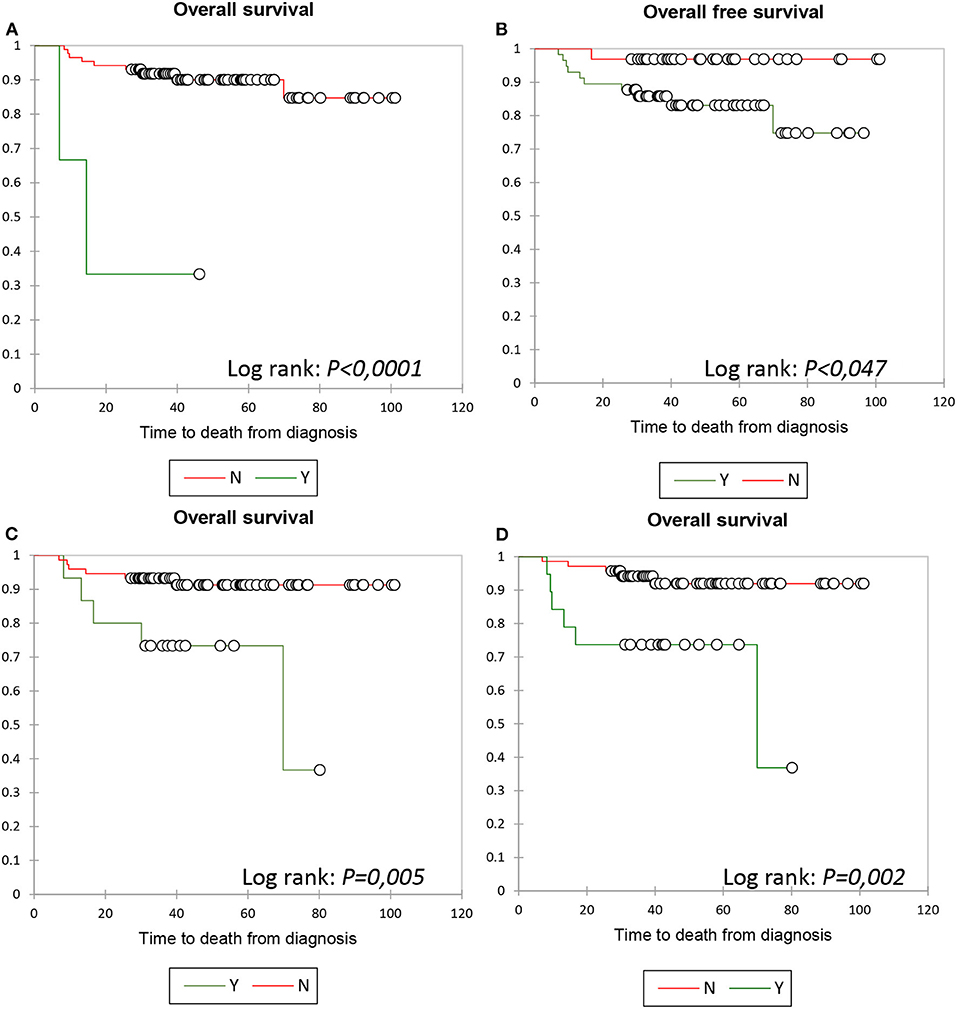
Figure 3. PFS: Kaplan Meier analysis according to the KBMP4 scoring model. OS according to meningeal lymphomatosis (A), Ki67 ≥70% (B), PETO-PET2 ΔSUV <66% (C) and PETO-PET4 ΔSUV <71% (D), respectively.
As KBMP4 parameters, except for bulky presentation ≥7.5 cm, were found statistically significant in multivariate analysis, the model was tested and showed prognostic significance for OS: in subgroup A, no patient out of 17 died (0%); in subgroup B, 6/63 patients (9.5%) died, with a median time to death of 21.9 months, ranging from 9.3 to 69.8; and in subgroup C, 4/9 patients (44.4%) died, with a median time to death of 9 months, ranging from 6.9 to 13.2. No statistical significance was noticed when subgroup A was compared to subgroup B (p = 0.140), while a significant difference was observed when comparing subgroup A to subgroup C (p = 0.002) and subgroup B to subgroup C (p = 0.002) (Figure 4 right).
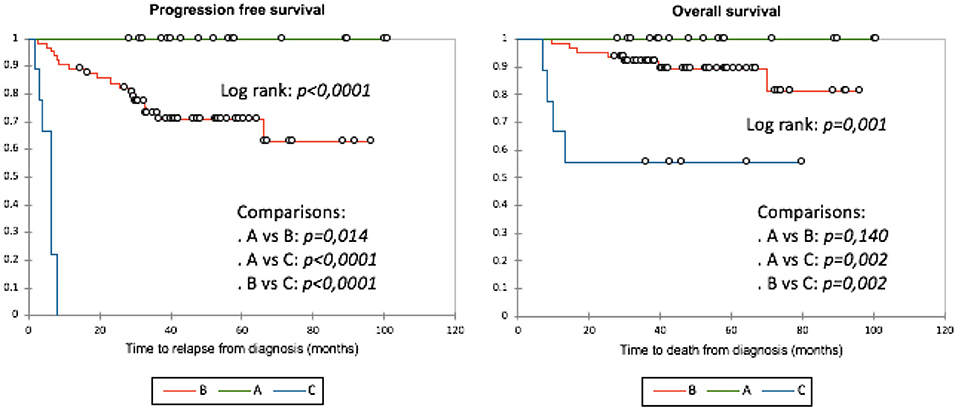
Figure 4. PFS and OS according to KBMP4 scoring models: Kaplan Maier analysis. KBMP4 scoring model identified three distint prognostic low-(A: O parameter), intermediate- (B: 1 or 2 parameters) and high risk (C: ≥3 parameters) subgroup regarding PFS (left) as well as OS (right).
Discussion
DLBCL is a set of highly aggressive NHLs with variable and heterogeneous prognoses. IPI and aaIPI are currently the most widely accepted prognostic indices to stratify DLBCL patients (2). Nevertheless, several drawbacks exist in the use of IPI and aaIPI. Firstly, these indices were designed prior to the introduction of rituximab. Additionally, their ability to adequately and finely identify patients at risk of treatment failure in the rituximab era, in terms of both PFS and OS, is still being debated (29, 30). Currently, 30%−35% of patients who are treated by R-CHOP in the first line will experience a poor outcome with early or late relapse or primary refractoriness. This evidence, therefore, suggests the need for a more sensitive prognostic score able to identify patients at risk for adverse outcomes and to adjust the treatment approach accordingly (23, 31).
In our present analysis, we identified four independent and routinely collected biomarkers, namely, Ki67 ≥ 70%, bulky presentation ≥7.5 cm, meningeal lymphomatosis, and ΔSUVmax PET0–PET4 <71%, which were highly predictive of PFS, the main predictor of treatment success.
The KBMP4 scoring model robustly discriminates patients' PFS into low- (0 factors), intermediate- (1 or 2), and high-risk (≥3) subgroups. In the low-risk subgroup, 100% of patients remained relapse-free, whereas in the high-risk subgroup, 100% of patients relapsed, within a median time of 6.3 months, ranging from 1.9 to 8.2. Of note, although all but 1, namely, bulky presentation, of the four key parameters of the model proved successful in predicting OS, likely due in part to the low death rate, the model clearly showed significant differences in OS across the three subgroups, with 0% of death in the low-risk subgroup and 44.4% of high-risk patients dying in a median time of 9 months, ranging from 6.9 to 13.2. Contrastingly, when applied to our cohort of patients, IPI > 2 and aaIPI > 1 failed to show statistical significance for both PFS and OS.
With respect to biological features, IHC-defined GC/non-GC subclassification based on the Hans algorithm and DE profile along with molecularly defined DH/TH status have been suggested to have prognostic significance (3, 8, 10). DH/TH status is not routinely assessed in our institutions and was, therefore, not tested for predictive ability. MYC status, limited to DE profile in our cohort, did not show statistical significance for OS. Nonetheless, it is worth mentioning that, among 11 deceased patients, there were 5 MYC+ in whom KBMP4 was low in 1, intermediate in 3, and high in 1; there were 6 MYC– in whom KBMP4 was intermediate in 3 and high in 3. Non-GC lymphomas, with a higher trend toward extranodal involvement and meningeal lymphomatosis, are reportedly more aggressive than GC lymphomas (32). However, 10% to 20% of cases are “unclassifiable” according to the Hans algorithm, whose predictive value for survival is currently being debated (33). In our study, these parameters had no significant predictive value regarding PFS or OS. In contrast, consistent with previous studies (34), our results revealed that Ki67 IHC expression ≥70% was associated with an unfavorable impact on PFS and OS.
The adverse prognostic impact of bulky presentation in DLBCL is widely reported, notably in case of failure to reach CR on interim PET, which can be reversed by involved-field radiotherapy as demonstrated by the UNFOLDER trial (35). But the defining tumor-size range varies from 5–6 to 10 cm among studies (31). According to the National Comprehensive Cancer Network, bulky disease should be defined as a tumor ≥7.5 cm in diameter (36). In our study, the cutoff was also set at 7.5 cm, and this parameter was found statistically significant for PFS, in both univariate and multivariate Cox model analyses, but not for OS.
Central nervous system (CNS) involvement, usually an exclusion criterion in most clinical trials, is responsible for high morbidity and shortened OS (37). It is, therefore, a strong indicator of early relapse and fatal outcomes. In this respect, our results confirm that meningeal lymphomatosis is associated with an unfavorable outcome and bring support to the standard approaches for CNS prophylactic or curative strategies in every newly diagnosed DLBCL (38).
Imaging through PET also holds a valuable place in discriminating low- and high-risk DLBCL patients and, most importantly, in the interim assessment of chemosensitivity. TMTV and TLG are not routinely assessed in our institutions. Quantitative measurement of ΔSUVmax between baseline PET0 and interim PET2 and PET4 is a novel approach for aggressive lymphoma, not universally accepted (39), but whose results are used to guide optimal treatment strategy (40). The optimal PET0–PET2 ΔSUVmax cutoff used to identify early and late responders to the R-CHOP regimen has been set at <66%, while the optimal PET0–PET4 ΔSUVmax cutoff used to identify nonresponders who will require salvage treatment has been set at <71% (16). Patients reaching complete metabolic response have a 2-year PFS > 70%. In accordance with published data, we observed a strong predictive value of PET0–PET4 ΔSUVmax for both PFS and OS, although we observed a false positivity rate of 31.5% in patients who could have been subject to unnecessary treatment intensification without histological assessment or PET4 proofreading. In contrast to reports in the medical literature, PET0–PET2 ΔSUVmax predictive value was limited to univariate analysis for PFS (41, 42), while in accordance with other studies, it was strongly demonstrated in multivariate and Kaplan–Meier analyses for OS (43). These results suggest the need for further investigation of PET0–PET2 ΔSUVmax predictive value.
The originality of the KBMP4 prediction model resides in its convenience and reproducibility, as it is based on robust prognostic factors, which are well described in the medical literature. Indeed, each parameter of the score is systematically collected at baseline, and PET is the major imaging technique in staging and response assessment, notably for all non-elderly patients. This score demonstrated a good ability to discriminate between low-, intermediate-, and high-risk patients, allowing for accurate predictions of PFS and OS.
Our results have potentially important implications for the management of newly diagnosed DLBCL patients. Firstly, our scoring scheme appears to offer improved DLBCL patient prognostic classification, allowing for enhanced foresight for physicians, patients, and their families and caregivers (44). Furthermore, early stratification according to prognosis and predicted response to treatment may offer ground to enroll patients in clinical trials exploring alternative regimens (45–47), especially those targeting new druggable molecules, with the hope to find out innovative treatments, including cellular therapy (48), better suited to the patient's profile than R-CHOP. Specifically, our findings may play a role in the context of the expected next generation of clinical trials based on the LYSA RT3 (Real Time Molecular Characterization of DLBCL, NCT03104478) study in the area of personalized treatment for cancer.
The main weaknesses of our study rest in the limited number of centers having been involved, resulting in small sample size, as well as the retrospective nature of our work. Furthermore, although MYC status was not found to be statistically significant regarding OS, it would be interesting to know if there were differences between subgroups of MYC+ and MYC– subjects, which was challenging due to the small number of MYC+ patients in our cohort. External validation of our prognostic model should be conducted to assess its reliability in a larger number of patients, including subjects meeting all the four key KBMP4 parameters, which may allow for further discriminating the intermediate-risk patients into low- and high-intermediate additional subgroups reflecting their prognostic profiles more accurately.
Conclusion
In summary, KBMP4 is a promising prognostic scoring model that has demonstrated the ability to discriminate between low-, intermediate-, and high-risk DLBCL patients in our cohort, with respect to both PFS and OS. Ki67 ≥70%, bulky tumor ≥7.5 cm, meningeal involvement, and PET0–PET4 ΔSUVmax <71% were identified as independent predictors of relapse and, except for bulky tumor, of OS in patients who were newly diagnosed with DLBCL. The use of this score in clinical practice may allow for improved treatment guidance and tailored treatment for each patient.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by Comité d'Ethique du CHU de Brest. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
VR collected data and references and wrote the manuscript. MMaa, P-YS, RA, FS, and DB reviewed PET-CT data. LR proofread the manuscript. IQ-R and LS reviewed histological data. RL, A-SL, and MMal enrolled patients and reviewed the manuscript. AT, HS, CB, and J-CI reviewed the manuscript. J-RE designed and directed the study, collected data, and wrote the manuscript. All authors contributed to the article and approved the submitted version.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnume.2022.829138/full#supplementary-material
References
1. Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri SA, Stein H, et al. Classification of Tumours of Haematopoietic and Lymphoid Tissues. Revised 4th edition. Lyon, France: World Health Organization. (2017).
2. The International Non-Hodgkin's Lymphoma Prognostic Factors. A predictive model for aggressive non-Hodgkin's lymphoma. N Engl J Med. (1993) 329:987–94. doi: 10.1056/NEJM199309303291402
3. Sarkozy C, Traverse-Glehen A, Coiffier B. Double-hit and double-protein-expression lymphomas: aggressive and refractory lymphomas. Lancet Oncol. (2015) 16:e555–67. doi: 10.1016/S1470-2045(15)00005-4
4. Barrans S, Crouch S, Smith A, Turner K, Owen R, Patmore R, et al. Rearrangement of MYC is associated with poor prognosis in patients with diffuse large B-cell lymphoma treated in the era of rituximab. J Clin Oncol. (2010) 28:3360–5. doi: 10.1200/JCO.2009.26.3947
5. Epperla N, Maddocks KJ, Salhab M, Chavez JC, Reddy N, Karmali R, et al. C-MYC-positive relapsed and refractory diffuse large B-cell lymphoma: impact of additional “hits” and outcomes with subsequent therapy. Cancer. (2017) 123:4411–8. doi: 10.1002/cncr.30895
6. Green TM, Young KH, Visco C, Xu-Monette ZY, Orazi A, Go RS, et al. Immunohistochemical double-hit score is a strong predictor of outcome in patients with diffuse large B-cell lymphoma treated with rituximab plus cyclophosphamide, doxorubicin, vincristine, and prednisone. J Clin Oncol. (2012) 30:3460–7. doi: 10.1200/JCO.2011.41.4342
7. Perry AM, Alvarado-Bernal Y, Laurini JA, Smith LM, Slack GW, Tan KL, et al. MYC and BCL2 protein expression predicts survival in patients with diffuse large B-cell lymphoma treated with rituximab. Br J Haematol. (2014) 165:382–91. doi: 10.1111/bjh.12763
8. Scott DW, King RL, Staiger AM, Ben-Neriah S, Jiang A, et al. High grade B-cell lymphoma with MYC and BCL2 and/or BCL6 rearrangements with diffuse large B-cell lymphoma morphology. Blood. (2018) 131:2060–4. doi: 10.1182/blood-2017-12-820605
9. Alizadeh AA, Eisen MB, Davis RE, Ma C, Lossos IS, Rosenwald A, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. (2000) 403:503–11. doi: 10.1038/35000501
10. Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. (2004) 103:275–82. doi: 10.1182/blood-2003-05-1545
11. Chapuy B, Stewart C, Dunford AJ, Kim J, Kamburov A, Redd RA, et al. Molecular subtypes of diffuse large B-cell lymphoma are associated with distinct pathogenic mechanisms and outcomes. Nat Med. (2018) 24:679–90. doi: 10.1038/s41591-018-0016-8
12. Itti E, Meignan M, Berriolo-Riedinger A, Biggi A, Cashen AF, Véra P et al. An international confirmatory study of the prognostic value of early PET/CT in diffuse large B-cell lymphoma: comparison between Deauville criteria and ΔSUVmax. Eur J Nucl Med Mol Imaging. (2013) 40:1312–20. doi: 10.1007/s00259-013-2435-6
13. Vercellino L, Cottereau AS, Casasnovas O, Tilly H, Feugier P, Chartier L et al. High total metabolic tumor volume at baseline predicts survival independent of response to therapy. Blood. (2020) 135:1396–405. doi: 10.1182/blood.2019003526
14. Guo B, Tan X, Ke Q, Cen H. Prognostic value of baseline metabolic tumor volume and total lesion glycolysis in patients with lymphoma: a meta-analysis. PLoS ONE. (2019) 14:e0210224. doi: 10.1371/journal.pone.0210224
15. Lin C, Itti E, Haioun C, Petegnief Y, Luciani A, Dupuis J, et al. Early 18F-FDG PET for prediction of prognosis in patients with diffuse large B-cell lymphoma: SUV-based assessment versus visual analysis. J Nucl Med. (2007) 48:1626–32. doi: 10.2967/jnumed.107.042093
16. Casasnovas RO, Ysebaert L, Thieblemont C, Bachy E, Feugier P, Delmer A, et al. FDG-PET-driven consolidation strategy in diffuse large B-cell lymphoma: final results of a randomized phase 2 study. Blood. (2017) 130:1315–26. doi: 10.1182/blood-2017-02-766691
17. Li X, Xie X, Zhang L, Li X, Li L, Wang X et al. Research on the midterm efficacy and prognosis of patients with diffuse large B-cell lymphoma by different evaluation methods in interim PET/CT. Eur J Radiol. (2020) 133:109301. doi: 10.1016/j.ejrad.2020.109301
18. Zucca E, Cascione L, Ruberto T, Facchinelli D, Schär S, Hayoz S et al. Prognostic models integrating quantitative parameters from baseline and interim positron emission computed tomography in patients with diffuse large B-cell lymphoma: post-hoc analysis from the SAKK38/07 clinical trial. Hematol Oncol. (2020) 38:715–25. doi: 10.1002/hon.2805
19. Coiffier B, Lepage E, Brière J, Herbrecht R, Tilly H, Bouabdallah R et al. CHOP chemotherapy plus rituximab compared with CHOP alone in elderly patients with diffuse large-B-cell lymphoma. N Engl J Med. (2002) 346:235–42. doi: 10.1056/NEJMoa011795
20. Coiffier B, Sarkozy C. Diffuse large B-cell lymphoma: R-CHOP failure – what to do? Hematology Am Soc Hematol Educational Program. (2016) 2016:366–78. doi: 10.1182/asheducation-2016.1.366
21. Dunleavy K, Fanale MA, Abramson JS, Noy A, Caimi PF, Pittaluga S et al. Dose-adjusted EPOCH-R (etoposide, prednisopne, vincristin, cyclophosphamide, doxorubicine and rituximab) in untreated aggressive diffuse large B-cell lymphoma with MYC rearrangement: a prospective, munticentre, single-arm phase 2 study. Lancet Haematol. (2018) 5:e609–17. doi: 10.1016/S2352-3026(18)30177-7
22. Magnusson T, Narkhede M, Mehta A, Goyal G. No difference in overall survival between R-CHOP and R-EPOCH among patients with advanced stage MYC-rearranged, double hit or triple hit diffuse large B-cell lymphoma. Presented at the EHA (2021).
23. Costa LJ, Maddocks K, Epperla N, Reddy NM, Karmali R, Umyarona E, et al. Diffuse large B-cell lymphoma with primary treatment failure: Ultra-high risk features and benchmarking for experimental therapies. Am J Hematol. (2017) 92:161–70. doi: 10.1002/ajh.24615
24. Crump M, Neelapu SS, Farooq U, Van Den Neste E, Kuruvilla J, Westin J, et al. Outcomes in refractory diffuse large B-cell lymphoma: results from the international SCHOLAR-1 study. Blood. (2017) 130:1800–8. doi: 10.1182/blood-2017-03-769620
25. Gisselbrecht C, Glass B, Mounier N, Singh Gill D, Linch DC, Trneny M et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. (2010) 28:4184–90. doi: 10.1200/JCO.2010.28.1618
26. Cheson BD, Fisher RI, Barrington SF, Cavalli F, Schwartz LH, Zucca E et al. Recommendations for initial evaluation, staging and response assessment of Hodgkin and non-Hodgkin lymphoma: the Lugano classification. J Clin Oncol. (2014) 32:3059–68. doi: 10.1200/JCO.2013.54.8800
27. Tilly H, Gomes da Silva M, Vitolo U, Jack A, Meignan M, Lopez-Guillermo A, et al. Diffuse large B-cell lymphoma (DLBCL): ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. (2015) 26 Suppl 5:v116–125. doi: 10.1093/annonc/mdv304
28. Le Gouill S, Ghesquière H, Oberic L, Morschhauser F, Tilly H, Ribrag V, et al. Obinutuzumab vs rituximab for advanced DLBCL: a PET-guided and randomized phase 3 study by LYSA. Blood. (2021) 137:2307–20. doi: 10.1182/blood.2020008750
29. Sehn LH, Berry B, Chhanabhai M, Fitzgerald K, Gill K, Hoskins P, et al. The Revised International Prognostic Index (R-IPI) is a better predictor of outcome than the standard IPI for patients with diffuse large B-cell lymphoma treated with R-CHOP. Blood. (2007) 109:1857–61. doi: 10.1182/blood-2006-08-038257
30. Ziepert M, Hasenclever D, Kunht E, Glass B, Schmitz N, Pfreundschuh M et al. Standard International prognostic index remains a valid predictor of outcome for patients with aggressive CD20+ B-cell lymphoma in the rituximab era. J Clin Oncol. (2010) 28:2373–80. doi: 10.1200/JCO.2009.26.2493
31. Schmitz N, Zeynalova S, Nickelsen M, Kansara R, Villa D, Sehn LH, et al. CNS International Prognostic Index: a risk model for CNS relapse in patients with diffuse large B-cell lymphoma treated with R-CHOP. J Clin Oncol. (2016) 34:3150–6. doi: 10.1200/JCO.2015.65.6520
32. Chang KC, Huang GC, Jones D, Tsao CJ, Lee JY, Su IJ. Distribution and prognosis of WHO Lymphoma Subtypes in Taiwan Reveals a Low incidence of germinal-center derived tumors. Leuk Lymphoma. (2004) 45:1375–84. doi: 10.1080/10428194042000198849
33. Benesova K, Forsterova K, Votavova H, Campr V, Stritesky J, Velenska Z, et al. The Hans algorithm failed to predict outcome in patients with diffuse large B-cell lymphoma treated with rituximab. Neoplasma. (2013) 60:68–73. doi: 10.4149/neo_2013_010
34. Li ZM, Huang JJ, Xia Y, Zhu YJ, Zhao W, Wei WX et al. High Ki-67 expression in diffuse large B-cell lymphoma patients with non-germinal center subtype indicates limited survival benefit from R-CHOP therapy. Eur J Haematol. (2012) 88:510–7. doi: 10.1111/j.1600-0609.2012.01778.x
35. Pfreundschuh M, Murawski N, Ziepert M, Altmann N, Dreyling MH, Borchmann P et al. Radiotherapy (RT) to bulky (B) and extralymphatic (E) disease in combination with 6xR-CHOP-14 or R-CHOP-21 in young good-prognosis DLBCL patients: Results of the 2x2 randomized UNFOLDER trial of the DSHNHL/GLA. J Clin Oncol. (2018) 36(15_Suppl):7574. doi: 10.1200/JCO.2018.36.15_suppl.7574
36. Pfreundschuh M, Ho AD, Cavallin-Stahl E, Wolf M, Pettengell R, Vasova I, et al. Prognostic significance of maximum tumour (bulk) diameter in young patients with good-prognosis diffuse large-B-cell lymphoma treated with CHOP-like chemotherapy with or without rituximab: an exploratory analysis of the MabThera International Trial Group (MInT) study. Lancet Oncol. (2008) 9:435–44. doi: 10.1016/S1470-2045(08)70078-0
37. Ma J, Li Q, Shao J, Ma Y, Lin Z, Kang H, et al. Central nervous system involvement in patients with diffuse large B-cell lymphoma: analysis of the risk factors and prognosis from a single-center retrospective cohort study. Cancer Manag Res. (2019) 11:10175–85. doi: 10.2147/CMAR.S225372
38. Abramson JS, Hellmann M, Barnes JA, Hammerman P, Toomey C, Takvorian T, et al. Intravenous methotrexate as central nervous system (CNS) prophylaxis is associated with a low risk of CNS recurrence in high-risk patients with diffuse large B-cell lymphoma. Cancer. (2010) 116:4283–90. doi: 10.1002/cncr.25278
39. Adams HJ, Kwee TC. Prognostic value of interim FDG-PET in R-CHOP-treated diffuse large B-cell lymphoma: systematic review and meta-analysis. Crit Rev Oncol Hematol. (2016) 106:55–63. doi: 10.1016/j.critrevonc.2016.07.003
40. Dührsen U, Müller S, Hertenstein B, Thomssen H, Kotzerke J, Mesters R, et al. Positron emission tomography-guided therapy of aggressive non-Hodgkin lymphomas (PETAL): a multicenter, randomized phase III trial. J Clin Oncol. (2018) 36:2024–34. doi: 10.1200/JCO.2017.76.8093
41. Islam P, Goldstein J, Flowers CR. PET-derived tumor metrics predict DLBCL response and progression free survival. Leukemia Lymphoma. (2018) 60:1965–71. doi: 10.1080/10428194.2018.1562181
42. Kitajima K, Okada M, Yoshihara K, Tokugawa T, Sawada A, Yoshihara S et al. Predictive value of interim FDG-PET/CT findings in patients with diffuse large B-cell lymphoma treated with R-CHOP. Oncotarget. (2019) 10:5403–11. doi: 10.18632/oncotarget.27103
43. Kong Y, Qu L, Li Y, Liu D, Lv X, Han J. Predictive significance of a new prognostic score for patients with diffuse large B-cell lymphoma in the interim-positron emission tomography findings. Medicine (Baltimore). (2016) 95:e2808. doi: 10.1097/MD.0000000000002808
44. Goy A. Succeeding in breaking the R-CHOP ceiling in DLBCL: learning from negative trials. J Clin Oncol. (2017) 35:3519–22. doi: 10.1200/JCO.2017.74.7360
45. Leonard JP, Kolibaba KS, Reeves JA, Tulpule A, Flinn IW, Kolevska T, et al. Randomized phase II study of R-CHOP with or without bortezomib in previously untreated patients with non-germinal center B-cell-like diffuse large B-cell lymphoma. J Clin Oncol. (2017) 35:3538–46. doi: 10.1200/JCO.2017.73.2784
46. Younes A, Thieblemont C, Morschhauser F, Flinn I, Friedberg JW, Amorim S, et al. Combination of ibrutinib with rituximab, cyclophosphamide, doxorubicin, vincristine, and prednisone (R-CHOP) for treatment-naive patients with CD20-positive B-cell non-Hodgkin lymphoma: A non-randomised, phase 1b study. Lancet Oncol. (2014) 15:1019–26. doi: 10.1016/S1470-2045(14)70311-0
47. Nowakowski GS, LaPlant B, Macon WR, Reeder CB, Foran JM, Nelson GD, et al. Lenalidomide combined with R-CHOP overcomes negative prognostic impact of non-germinal center B-cell phenotype in newly diagnosed diffuse large B-cell lymphoma: a phase II study. J Clin Oncol. (2015) 33:251–7. doi: 10.1200/JCO.2014.55.5714
Keywords: DLBCL, survival, Ki67, bulky, meningeal lymphoma, PET-CT, scoring system
Citation: Rebière V, Maajem M, Le Calloch R, Raj L, Le Bris A-S, Malou M, Salmon F, Quintin-Roué I, Tempescul A, Bourhis D, Samaison L, Saad H, Salaun P-Y, Berthou C, Ianotto J-C, Abgral R and Eveillard J-R (2022) Ki67 Immunohistochemical Expression Level ≥70%, Bulky Presentation ≥7.5 cm, Meningeal Lymphomatosis, and Interim PET ΔSUVmax After 4 Treatment Cycles <71% as Parts of a Practical Scoring System to Predict Progression-Free Survival and Overall Survival in Diffuse Large B-Cell Lymphoma. Front. Nucl. Med. 2:829138. doi: 10.3389/fnume.2022.829138
Received: 05 December 2021; Accepted: 14 February 2022;
Published: 07 April 2022.
Edited by:
Antonia Dimitrakopoulou-Strauss, German Cancer Research Center (DKFZ), GermanyReviewed by:
Pavel Koranda, Palacky University, CzechiaChristos Sachpekidis, German Cancer Research Center (DKFZ), Germany
Copyright © 2022 Rebière, Maajem, Le Calloch, Raj, Le Bris, Malou, Salmon, Quintin-Roué, Tempescul, Bourhis, Samaison, Saad, Salaun, Berthou, Ianotto, Abgral and Eveillard. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jean-Richard Eveillard, amVhbi1yaWNoYXJkLmV2ZWlsbGFyZEBjaHUtYnJlc3QuZnI=