 Guorong Jia
Guorong Jia Dejian Bian2†‡
Dejian Bian2†‡ Chao Cheng
Chao Cheng Changjing Zuo
Changjing Zuo- 1Department of Nuclear Medicine, Shanghai Changhai Hospital, Navy Military Medical University, Shanghai, China
- 2Department of Emergency, Shanghai Changhai Hospital, Navy Military Medical University, Shanghai, China
IgG4-related disease is a fibrous-inflammatory process belonging to immunomodulation disorders. We report a case of a 57-year-old man with the IgG4-related disease (RD). 68Ga-FAPI-04 PET/CT showed more significant uptake in most lesions than in 18F-FDG PET/CT except for the cervical and mediastinal lymph nodes. Besides, uptake in the submandibular glands were only detected in 68Ga-FAPI-04 PET/CT. The biopsy result of the cervical lymph nodes confirmed the diagnosis of IgG4-related disease. After treatment, only slight FDG-avid cervical lymph nodes were observed in the 18F-FDG PET/CT, while the raised uptake of 68Ga-FAPI-04 could be observed in the pancreas and submandibular glands. 68Ga-FAPI-04 PET-CT might have promising applications in evaluating IgG4-RD, whether in initial or follow-up imaging during steroid therapy.
Introduction
IgG4-related disease (RD) is an autoimmune-mediated disorder that involves different organs. A large amount of immune cell infiltration of the IgG4-related disease induced a focal mass that mimics a malignancy tumor in imaging examination (1). Especially in the pancreas, autoimmune pancreatitis has sometimes been misdiagnosed as pancreatic cancer (2). It is of great importance to distinguish IgG4-RD from tumors. Previous studies have validated the utility of 18F-fluorodeoxyglucose (18F-FDG) PET/CT in the differential diagnosis (3). Fibroblast activation protein is not only present in tumor stroma but also in some benign lesions with prominent fibroblast proliferation. 68Ga-labeled fibroblast activation protein inhibitor (68Ga-FAPI) is a novel PET agent. Some researchers have highlighted that 68Ga-FAPI PET/CT would contribute to diagnosing IgG4-related disease (RD) (4), but few studies to date have compared the role of 18F-FDG PET/CT and 68Ga-FAPI PET/CT in the follow-up of IgG4-RD. Here, we reported a case comparing the pre- vs. post- and 18F-FDG vs. 68Ga-FAPI-04 images of an IgG4-RD patient who underwent the prednisone treatment.
Case description
A 57-year-old man with jaundice for 4 months, abdominal pain and diarrhea for 2 months was presented to the emergency department. He was diagnosed with suspected cholangiocarcinoma because of the thickening of the bile duct wall observed on contrast-enhanced CT. The 18F-FDG PET/CT and 68Ga-FAPI-04 PET/CT were executed for the differential diagnosis and possible tumor staging (Figure 1 Maximum intensity projection images of 18F-FDG and 68Ga-FAPI-04 PET/CT). The pre-treatment 18F-FDG PET/CT pictures (Figures 2A–E) showed elevated uptake of the following lesions: cervical (SUVmax 4.7) and mediastinal lymph nodes (SUVmax 2.7), intrahepatic bile ducts (SUVmax 3.3), pancreas (SUVmax 3.0), and prostate (SUVmax 2.3). 68Ga-FAPI-04 PET/CT was also performed, and higher uptake in most lesions mentioned above was observed except for the cervical and mediastinal lymph nodes, Besides that, submandibular glands were also involved (Figures 3A–E). The patient's total bilirubin was elevated to 94.7 µmol/L. The tumor marker CA19-9 was 204.63 U/ml. The amylase was 228 U/L, and the IgG4 was 26.2 g/L (reference range: 0.03–2.1 g/L). A loco-regional lymphadenectomy and biopsy were performed. According to the biopsy result of the cervical lymph nodes, the final diagnosis was classified as an IgG4-RD. Subsequently, treatment with oral prednisone was initiated. The initial dose was 40 mg/d which lasted for 2 weeks. Then reduced by 5 mg every week, until the final dose of 5 mg/d which was used for 6 months. One month after treatment with prednisolone, the value of IgG4 was decreased to 13.6 g/L, CA19-9 to 36.94 U/ml, and the total bilirubin was reduced to 29.8 µmol/L. The symptoms of jaundice were relieved remarkably. During the same period of time, a slight FDG-avid lesion was detected only in the right cervical lymph node (SUVmax 1.7) (Figures 2F–J), but the raised uptake of 68Ga-FAPI-04 could still be observed in the pancreas (SUVmax 5.6) and submandibular glands (SUVmax 2.3) (Figures 3F–J).

Figure 1. The MIP images of 18F-FDG PET/CT and 68Ga-FAPI PET/CT. The pre-treatment 18F-FDG PET/CT (A) showed elevated uptake of the following lesions: cervical and mediastinal lymph nodes, intrahepatic bile ducts, pancreas, and prostate. The pre-treatment 68Ga-FAPI PET/CT (C) indicated more obvious uptake in most lesions mentioned above except for the cervical and mediastinal lymph nodes; besides that, submandibular glands were also involved. After prednisone treatment, FDG-avid lesion was detected only in the right cervical lymph node (B), but the raised uptake of 68Ga-FAPI could still be observed in the pancreas and submandibular glands (D).
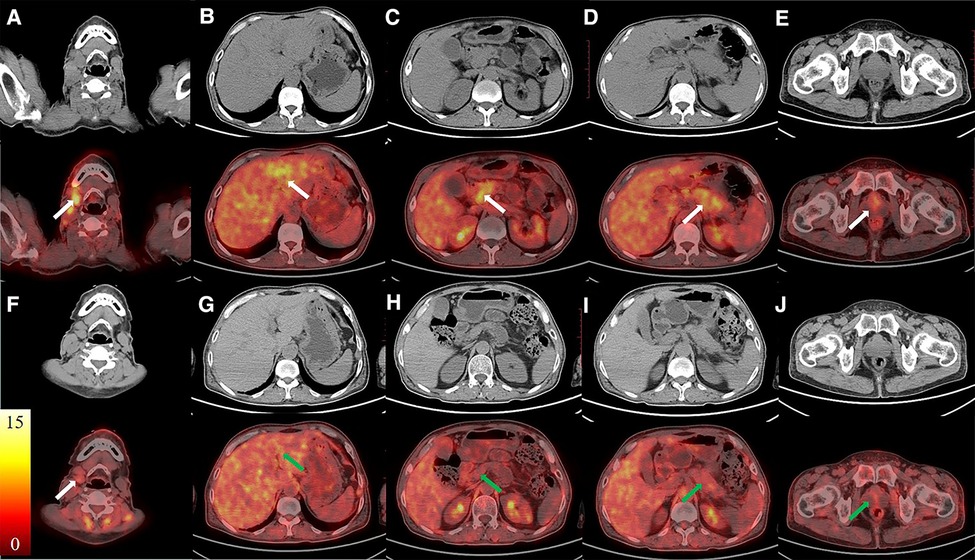
Figure 2. The images of 18F-FDG PET/CT. The CT images were in the first/third rows, and the fused PET/CT images were in the second/fourth rows. The pre-treatment images (A–E, white arrows) showed elevated uptake of the following lesions: cervical lymph nodes, intrahepatic bile ducts, pancreas, and prostate. FDG-avid lesion was detected only in the right cervical lymph node after the treatment (F–J).
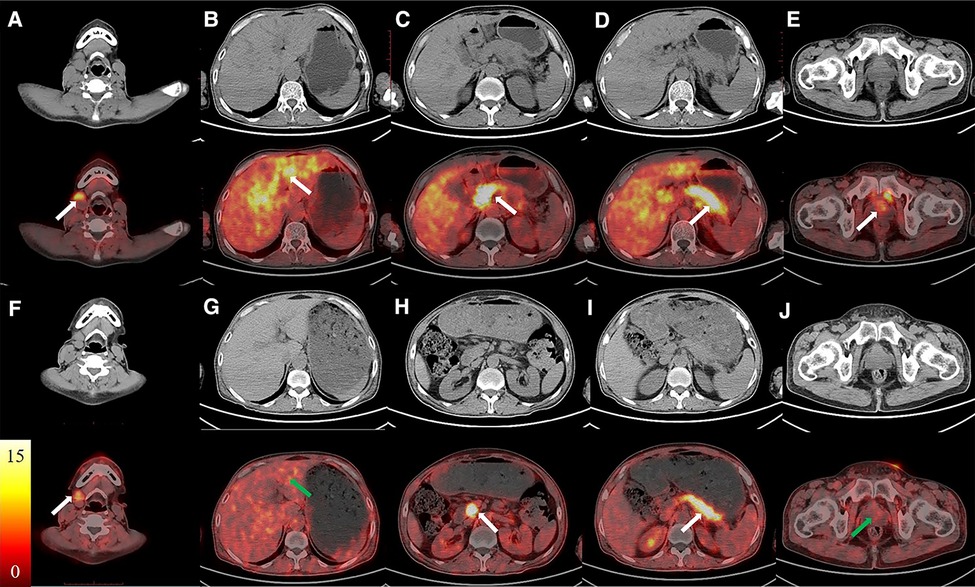
Figure 3. The images of 68Ga-FAPI PET/CT. The CT images were in the first/third rows, the fused PET/CT images were in second/fourth rows. The pre-treatment images (A–E, white arrows) showed elevated uptake of submandibular glands, intrahepatic bile ducts, pancreas, and prostate. The raised uptake of 68Ga-FAPI could still be observed in the submandibular glands and pancreas after treatment (F–J, white arrows).
Discussion
The FDG accumulation is the reflection of glucose metabolism in the tumor or inflammation lesion. Considerable evidence has demonstrated the ability of 18F-FDG PET to assess IgG4-RD both at initial evaluation and after therapy (2, 3). 68Ga-FAPI is thought to be the potential broad-spectrum tumor PET agent targeting FAP (5). Fibroblasts were activated in some benign diseases (6), such as IgG4-RD, and it can also be FAPI-positive.
In IgG4-RD, large quantities of fibroblasts lead to fibrosis in the extracellular matrix (7, 8). Some case reports and articles have also explored the utility of 68Ga-FAPI PET/CT to assess IgG4-RD (8, 9). One study of 26 IgG4-RD patients revealed that 68Ga-FAPI PET/CT detected more involved organs in 13 (50.0%) patients and significantly higher SUV than that of 18F-FDG PET/CT (4). However, FDG-avid lymph node did not accumulate 68Ga-FAPI (4, 10). The two results were both validated in this case report. The mismatch of 68Ga-FAPI and 18F-FDG revealed that the lesion was probably in different stages; the FDG-avid lesion was inflammatory-proliferative, while the 68Ga-FAPI positive lesion was likely in a fibrotic phase. Another possible pathological reason is that fibrosis is rare in most lymphadenopathy patterns of IgG4-RD (11). Our previous study about pancreatic cancer found that 68Ga-FAPI-04 PET/CT detected more positive lymph nodes whose activity was over background than 18F-FDG PET/CT (12). The critical parameters of 18F-FDG PET/CT for diagnosing malignant metastatic lymph nodes have been highly explored such as the SUVmax cut-off point, groups of lymph nodes, and the SUV value of tumor (13). But the utility of 68Ga-FAPI in detecting malignant metastatic lymph nodes is still in the stage of development and in comparison with 18F-FDG (14).
After the prednisone treatment, slight uptake in cervical lymph node was only observed in 18F-FDG PET/CT, whereas uptake in pancreas and submandibular glands were more noticeable in the 68Ga-FAPI-04 PET/CT. The laboratory test result of IgG4 of 13.6 g/L, which was also above the reference range, partly confirmed the involvement of IgG4-RD. In another cross-sectional clinical study with inflammatory, fibrotic and overlapping manifestations of IgG4-related disease, the responsiveness to immunosuppressive therapy was more sensitive in inflammatory lesions than in fibrotic lesions (15). This reason might explain the difference in 68Ga-FAPI-04 and 18F-FDG imaging after treatment with prednisone.
Notwithstanding its limitation, our case report found that 68Ga-FAPI-04 could provide additional insights into IgG4-RD beyond the inflammation process that demonstrated by 18F-FDG. The combination of 18F-FDG and 68Ga-FAPI-04 may demonstrate even greater potency in the efficacy assessment of IgG4-RD in the future.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Ethics statement
The studies involving human participants were reviewed and approved by China Clinical Trial Registry (ChiCTR2100052378). The patients/participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
GJ collected the images and wrote the article. DB helped explore the significance of this case. CC and MW were checked and organized the content of the article. CZ supervised all the above works. All authors contributed to the article and approved the submitted version.
Funding
This study was supported by the following funds: "234 Discipline Climbing Plan” of the First Affiliated Hospital of Naval Military Medical University (2019YPT002, 2020YPT002) and Advanced and Appropriate Technology Popularization Project of Shanghai Municipal Health Commission (2019SY029).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Sánchez-Oro R, Alonso-Muñoz EM, Martí Romero L. Review of IgG4-related disease. Gastroenterol Hepatol. (2019) 42:638–47. doi: 10.1016/j.gastrohep.2019.08.009
2. Zhang J, Jia G, Zuo C, Jia N, Wang H. (18)F- FDG PET/CT helps differentiate autoimmune pancreatitis from pancreatic cancer. BMC Cancer. (2017) 17:695. doi: 10.1186/s12885-017-3665-y
3. Dondi F, Albano D, Bellini P, Volpi G, Giubbini R, Bertagna F. 18F-fluorodeoxyglucose PET and PET/computed tomography for the evaluation of immunoglobulin G4-related disease: a systematic review. Nucl Med Commun. (2022) 43:638–45. doi: 10.1097/MNM.0000000000001566
4. Luo Y, Pan Q, Yang H, Peng L, Zhang W, Li F. Fibroblast activation protein-targeted PET/CT with (68)Ga-FAPI for imaging IgG4-related disease: comparison to (18)F-FDG PET/CT. J Nucl Med. (2021) 62:266–71. doi: 10.2967/jnumed.120.244723
5. Kratochwil C, Flechsig P, Lindner T, Abderrahim L, Altmann A, Mier W, et al. (68)Ga-FAPI PET/CT: tracer uptake in 28 different kinds of cancer. J Nucl Med. (2019) 60:801–5. doi: 10.2967/jnumed.119.227967
6. Hotta M, Rieger AC, Jafarvand MG, Menon N, Farolfi A, Benz MR, et al. Non-Oncologic incidental uptake on FAPI PET/CT imaging. Br J Radiol. (2022) 20220463. doi: 10.1259/bjr.20220463. [Epub ahead of print]35776566
7. Kamisawa T, Zen Y, Pillai S, Stone JH. IgG4-related disease. Lancet (London, England). (2015) 385:1460–71. doi: 10.1016/S0140-6736(14)60720-0
8. Perugino CA, Stone JH. IgG4-related disease: an update on pathophysiology and implications for clinical care. Nat Rev Rheumatol. (2020) 16:702–14. doi: 10.1038/s41584-020-0500-7
9. Qin C, Yang L, Ruan W, Shao F, Lan X. Immunoglobulin G4-related sclerosing cholangitis revealed by 68Ga-FAPI PET/MR. Clin Nucl Med. (2021) 46:419–21. doi: 10.1097/RLU.0000000000003552
10. Pan Q, Luo Y, Zhang W. Recurrent immunoglobulin G4-related disease shown on 18F-FDG and 68Ga-FAPI PET/CT. Clin Nucl Med. (2020) 45:312–3. doi: 10.1097/RLU.0000000000002919
11. Deshpande V, Zen Y, Chan JK, Yi EE, Sato Y, Yoshino T, et al. Consensus statement on the pathology of IgG4-related disease. Mod Pathol. (2012) 25:1181–92. doi: 10.1038/modpathol.2012.72
12. Zhang Z, Jia G, Pan G, Cao K, Yang Q, Meng H, et al. Comparison of the diagnostic efficacy of 68Ga-FAPI-04 PET/MR and (18)F-FDG PET/CT in patients with pancreatic cancer. Eur J Nucl Med Mol Imaging. (2022) 49:2877–88. doi: 10.1007/s00259-022-05729-5
13. Guberina M, Herrmann K, Pöttgen C, Guberina N, Hautzel H, Gauler T, et al. Prediction of malignant lymph nodes in NSCLC by machine-learning classifiers using EBUS-TBNA and PET/CT. Sci Rep. (2022) 12:17511. doi: 10.1038/s41598-022-21637-y
14. Serfling S, Zhi Y, Schirbel A, Lindner T, Meyer T, Gerhard-Hartmann E, et al. Improved cancer detection in Waldeyer's Tonsillar ring by 68Ga-FAPI PET/CT imaging. Eur J Nucl Med Mol Imaging. (2021) 48:1178–87. doi: 10.1007/s00259-020-05055-8
Keywords: 18F-FDG, 68Ga-FAPI-04, IgG4-related disease, PET/CT, therapy
Citation: Jia G, Bian D, Cheng C, Wang M and Zuo C (2023) The different manifestations of 18F-FDG PET/CT and 68Ga-FAPI-04 PET/CT in evaluation of the steroid therapy response for IgG4-related disease: A case report. Front. Nucl. Med. 2:1038797. doi: 10.3389/fnume.2022.1038797
Received: 8 September 2022; Accepted: 6 December 2022;
Published: 4 January 2023.
Edited by:
Ismaheel Lawal, Emory University, United States© 2023 Jia, Bian, Cheng, Wang and Zuo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Changjing Zuo Y2hhbmdqaW5nLnp1b0BxcS5jb20=
†These authors have contributed equally to this work
‡ORCID Guorong Jia orcid.org/0000-0002-1293-9387 Dejian Bian orcid.org/0000-0002-2051-766X Chao Cheng orcid.org/0000-0002-2981-5890
Specialty Section: This article was submitted to PET and SPECT, a section of the journal Frontiers in Nuclear Medicine