
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurosci. , 24 November 2023
Sec. Translational Neuroscience
Volume 17 - 2023 | https://doi.org/10.3389/fnins.2023.1272068
This article is part of the Research Topic Patient Education in the Treatment of Chronic Pain View all 4 articles
 Ferran Cuenca-Martínez1
Ferran Cuenca-Martínez1 Luis Suso-Martí1*
Luis Suso-Martí1* Joaquín Calatayud1Francisco José Ferrer-Sargues2Vicente Muñoz-Alarcos1
Joaquín Calatayud1Francisco José Ferrer-Sargues2Vicente Muñoz-Alarcos1 Patricio Alba-Quesada1
Patricio Alba-Quesada1 Gemma Biviá-Roig2
Gemma Biviá-Roig2Introduction: In recent years, pain neuroscience education (PNE) has been the focus of extensive research in the scientific literature in the field of physical therapy, but the results obtained are controversial and its clinical application remains unclear. The main aim of this umbrella review was to assess the effectiveness of PNE in patients with chronic musculoskeletal pain (CMP).
Methods: We searched systematically in PubMed (Medline), PEDro, EMBASE, CINAHL and PsycINFO. Methodological quality was analyzed using AMSTAR-2 scale and overlapping analysis using GROOVE tool.
Results: 16 systematic reviews were included. A qualitative synthesis was performed for the following sets of patients with CMP: overall CMP, chronic spinal pain, patients with fibromyalgia and patients with osteoarthritis. In general terms, it seems that the addition of the PNE-based intervention to other treatments, mostly exercise-based interventions although we might refer to it in terms of a multimodal approach, leads to greater clinical improvements than the multimodal approach alone. We have found this especially in the reduction of the influence of psychosocial variables. However, it seems that studies testing the effectiveness of PNE in isolation, systematic reviews with or without meta-analysis did not show statistically significant improvements overall in terms of pain intensity, disability levels or psychosocial variables.
Discussion: There is a great heterogeneity in the results obtained and the PNE protocols used, a critically low quality in the reviews included and a very high overlap, so there is a need to improve the studies in this field before clinical application.
Systematic review registration: PROSPERO (CRD42022355634).
Chronic Musculoskeletal Pain (CMP) is a major public health concern. Approximately 20% of the adult population suffers from CMP (Goldberg and McGee, 2011), which is one of the leading causes of disability worldwide, according to the Global Burden Disease study (Vos et al., 2012). In addition to reducing the quality of life of those who suffer from this condition (Breivik et al., 2006; Tüzün, 2007), it may also result in a serious socioeconomic burden (Espinoza et al., 2022). CMP is a complex and multifactorial phenomenon (Apkarian and Baliki, 2009). The findings of some studies indicate that these patients develop central sensitization mechanisms that contribute to the chronification of pain (Graven-Nielsen and Arendt-Nielsen, 2010; Adams and Turk, 2018). Furthermore, the perception of pain in patients is influenced by factors such as hypervigilance, catastrophizing, kinesiophobia, and anxiety and depression (Keefe et al., 2004). In this light, treating CMP presents a considerable challenge for health care professionals, who should incorporate biopsychosocial approach that address biological, psychological and social factors into their treatment plan (Turk and Okifuji, 2002; Edwards et al., 2016).
Currently, European guidelines emphasize the importance of patient education as part of the treatment of CMP. Education is a planned experience intended to influence the behavior and knowledge of patients through methods of counseling, teaching, and behavior modification (Engers et al., 2008). Patient education increases patients’ knowledge of their condition and promotes positive pain-related beliefs and behaviors (Robinson et al., 2016). Over the past few years, the field of pain neuroscience education (PNE) has attracted a great deal of attention. The aim of this educational strategy is to provide the patient with a thorough understanding of the neurobiological and neurophysiological processes involved in their pain experience (Nijs et al., 2011; Moseley, 2013). It provides patients with an opportunity to improve their understanding of pain and reconceptualize their ideas about it, thereby changing the negative beliefs they have about pain and their incorrect perceptions of it (Moseley and Butler, 2015). Previous research in PNE has suggested that tis intervention could increase knowledge about pain, produce cognitive changes and also have positive effects on pain intensity, disability, kinesiophobia and catastrophizing, as well as on pain-mediating factors such as hypervigilance, anxiety, attitudes and beliefs (Salazar-Méndez et al., 2023; Zimney et al., 2023).
In recent years, PNE has been the focus of extensive research in the scientific literature in the field of physical therapy, and several clinical trials and systematic reviews have been conducted to determine its efficacy. Overall, the results are promising, and show that PNE can be an effective intervention in combination with manual therapy or exercise, although in isolation it may have no effect in patients with CMP (Barbari et al., 2021). However, there are some controversies. A mixed-methods systematic review and meta-analysis found no evidence to indicate that PNE results in clinically important changes over control for pain or disability (Watson et al., 2019). In this regard, it has been suggested that PNE may be effective only for some patients, implying individual differences in response to treatment that may influence outcome variables (Watson et al., 2021). Furthermore, Barbari et al. (2021) highlight that, despite the potential of PNE in CMP patients, the application remains a challenge due to the fact that not all patients can understand PNE concepts in the same way, not all patients are equal despite they are labeled as suffering of chronic MSK pain, and not all clinicians have the training and resources necessaries to apply PNE.
Finally, one challenge in the current scientific literature in this area involves the existence of a large number of systematic reviews, but many of them have overlaps in the studies they include, as well as other methodological shortcomings, which can lead to potentially biased clinical recommendations (Ioannidis, 2016). For this reason, conducting an umbrella review offers a solution, synthesizing the results and conclusions of systematic reviews, and offering insight into possible biases (Lunny et al., 2021). Therefore, the main aim of this umbrella review was to assess and synthetize the previous systematic reviews in the field of PNE for patients with CMP, critically evaluate the published literature in order to elucidate the controversies and determine the effectiveness of PNE in this population.
This study was conducted in accordance with the Preferred Reporting Items for Overviews of Systematic Reviews including harm checklist (PRIO-harms), which consists of 27 items (56 sub-items), followed by a 5-stage process flow diagram (identification, screening, eligibility, inclusion, and separation of relevant studies) (Bougioukas et al., 2018). The review was previously registered in the international prospective register of systematic reviews PROSPERO (CRD42022355634).
The inclusion criteria employed in this article were based on methodological and clinical factors such as population, intervention, control, outcomes and study design (PICOS) (Stone, 2002).
The participants selected for the articles were adults with CMP (including chronic low back or neck pain, osteoarthritis, or rheumatoid arthritis, in addition to those who suffer nonspecific or widespread musculoskeletal pain conditions like fibromyalgia). The diagnosis of CMP was consistent with the British Pain Society definition (chronic pain, that lasts beyond the time that tissue healing would normally be expected to have occurred, often taken as ≥3 months) (British Pain Society, 2013).
We included all systematic reviews assessing the effects of PNE. The intervention should have been composed of planned and structured sessions where patients were educated about the basic neurophysiology of pain, trying to reconceptualize their experience so that it would be considered less threatening (Watson et al., 2019). Interventions based on psychological treatment or cognitive behavioral therapy were excluded. Comparator groups could be non-active interventions, waiting list, minimal interventions (relaxation, breathing or educational advice) or no intervention. If any other treatment (such as medication or manual therapy) was included, it had to be applied in the intervention group as well.
The measures used to assess the results and effects were variables related to clinical outcomes (pain intensity, disability, depressive symptoms, anxiety, pain catastrophizing, and fear-related movement).
We selected systematic reviews (with or without a meta-analysis) of randomized controlled clinical trials (RCCTs) or controlled clinical trials (CCTs) and excluded systematic reviews that included RCCTs or CCTs in combination with non-experimental designs. There were no restrictions for any specific language, as recommended by the international criteria (Moher et al., 1998).
We conducted the search for published scientific articles between 1950 and November 14th, 2022, in the following databases: PubMed (Medline), PEDro, EMBASE, CINAHL, and PsycINFO. The reference sections of the included studies and original studies were screened manually. Supplementary material S1 shows the search strategies, which was adapted for each database. The search was conducted by two independent reviewers (FCM and LSM) using the same methodology. Differences that emerged during this phase were resolved by consensus. The reference sections of the original studies were screened manually, and the authors were contacted for further information if necessary.
Initially, the two independent reviewers conducted a screening (FCM and LSM) assessing the relevance of the systematic reviews (with and without a meta-analysis) regarding the studies’ questions and objectives. The first screening was based on each study’s title information, abstract, and keywords. The full text was reviewed if there was no consensus or if the abstracts contained insufficient information. In the second phase of the screening, the full text was assessed if the studies met all of the inclusion criteria. Differences between the reviewers were resolved by a discussion and consensus process mediated by a third reviewer (JFFS). The data described in the results section were extracted by means of a structured protocol that ensured that the most relevant information was obtained from each study.
The two independent reviewers (FCM and LSM) assessed the methodological quality of the systematic reviews (with or without meta-analysis), assessing each of the selected studies based on the Modified Quality Assessment Scale for Systematic Reviews (AMSTAR-2) developed by Barton et al. (2008) a scale shown to be a valid and reliable tool for assessing the methodological quality of systematic reviews. With a total of 16 items (scoring “yes”; “yes in part” and “no”), with a final assessment as a critically low, low, moderate, and high quality. In addition, we calculated the kappa coefficient (κ) and percentage (%) agreement scores to assess reliability prior to any consensus and estimated the inter-rater reliability using κ: (1) κ > 0.7 indicates a high level of agreement between the reviewers; (2) κ of 0.5–0.7 indicates a moderate level of agreement; and (3) κ < 0.5 indicates a low level of agreement (McHugh, 2012). Disagreements on the final quality assessment score were resolved by consensus with a third independent reviewer (JFFS).
To assess the overlap of primary studies among systematics reviews the methodological approach GROOVE (Graphical Representation of Overlap for OVErviews) was employed. This tool is an Excel-based file which automatically calculates the overall covered areas for a whole matrix of evidence, and, at the same time, for each possible pair of SRs included in the overview. The tool summarizes the number of reviews, index publications and primary studies (including double counting) included in the matrix. With this data, it calculates the covered area and provides the interpretation of the overall overlap assessment, being slight if the covered area is <5%, moderate if it is ≥5% and < 10%, high if it is ≥10% and < 15%, and very high if is ≥15%. This tool is intended to be used mainly by authors of overviews of systematic reviews (Pérez-Bracchiglione et al., 2022).
The initial search revealed 206 records, and an additional 5 were retrieved manually from the reference list. Through the title and abstract screening and the full-text assessment, 16 systematic reviews were eligible according to our criteria. The study screening strategy is shown in the form of a flow chart (Figure 1).
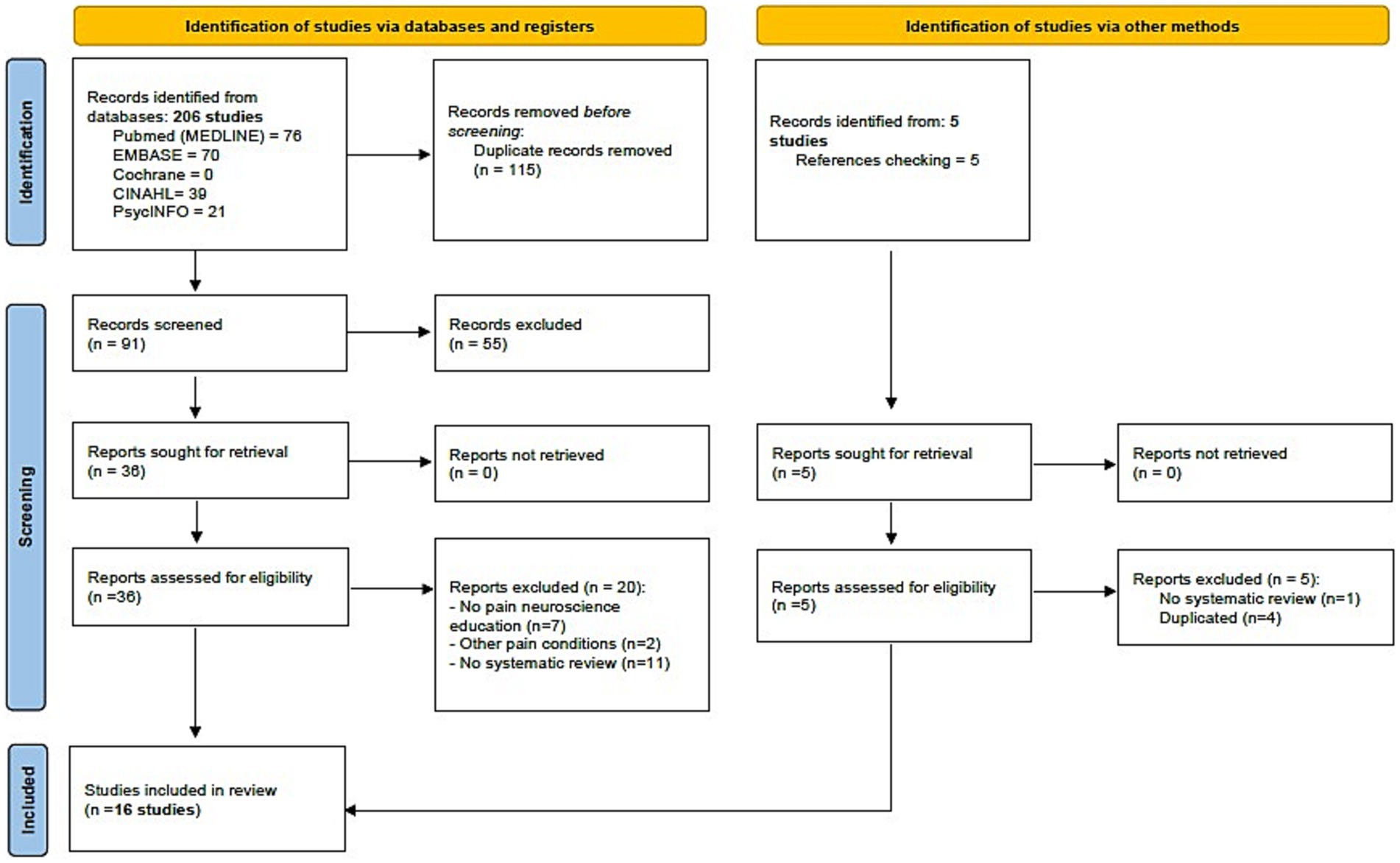
Figure 1. Study flow diagram (PRISMA 2020).
Table 1 lists the characteristics of the systematic reviews included (study design, original studies included, demographic characteristics, interventions, variables, and results). Interventions included PNE combined usually with physical therapy interventions or exercise interventions. The most analyzed tools for pain intensity were the visual analog pain scale (VAS) and numerical pain rating scale (NPRS). For functionality, the RMDQ, neck disability index (NDI), pain disability index (PDI), fibromyalgia impact questionnaire (FIQ), western Ontario and McMaster Universities Arthritis index (WOMAC) and Quebec back pain disability scale (QBPDS) were used. Finally, for the psychosocial variables were the Tampa Scale of Kinesiophobia (TSK) and the Pain Catastrophizing Scale (PCS).
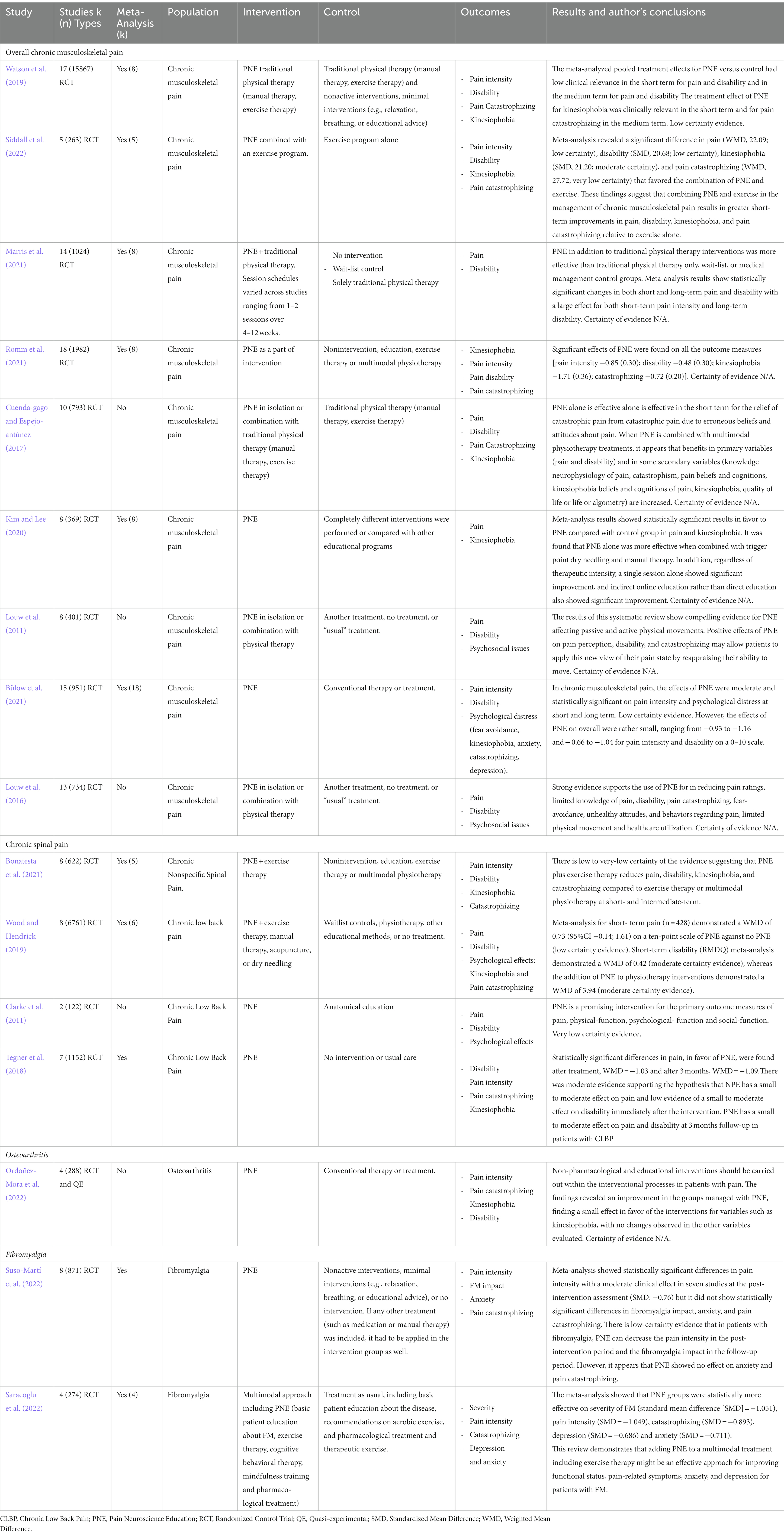
Table 1. Characteristics of the included studies.
The control groups in the studies analyzed by the meta-analyses and reviews included in this paper were: manual therapy (MT), exercise, usual treatment, biomedical/anatomical education, dry needling (DN), self-management techniques.
Table 2 showed the results of methodological quality. All reviews scored as “critically low” quality. The inter-rater reliability of the methodological quality assessment was high (κ = 0.795).
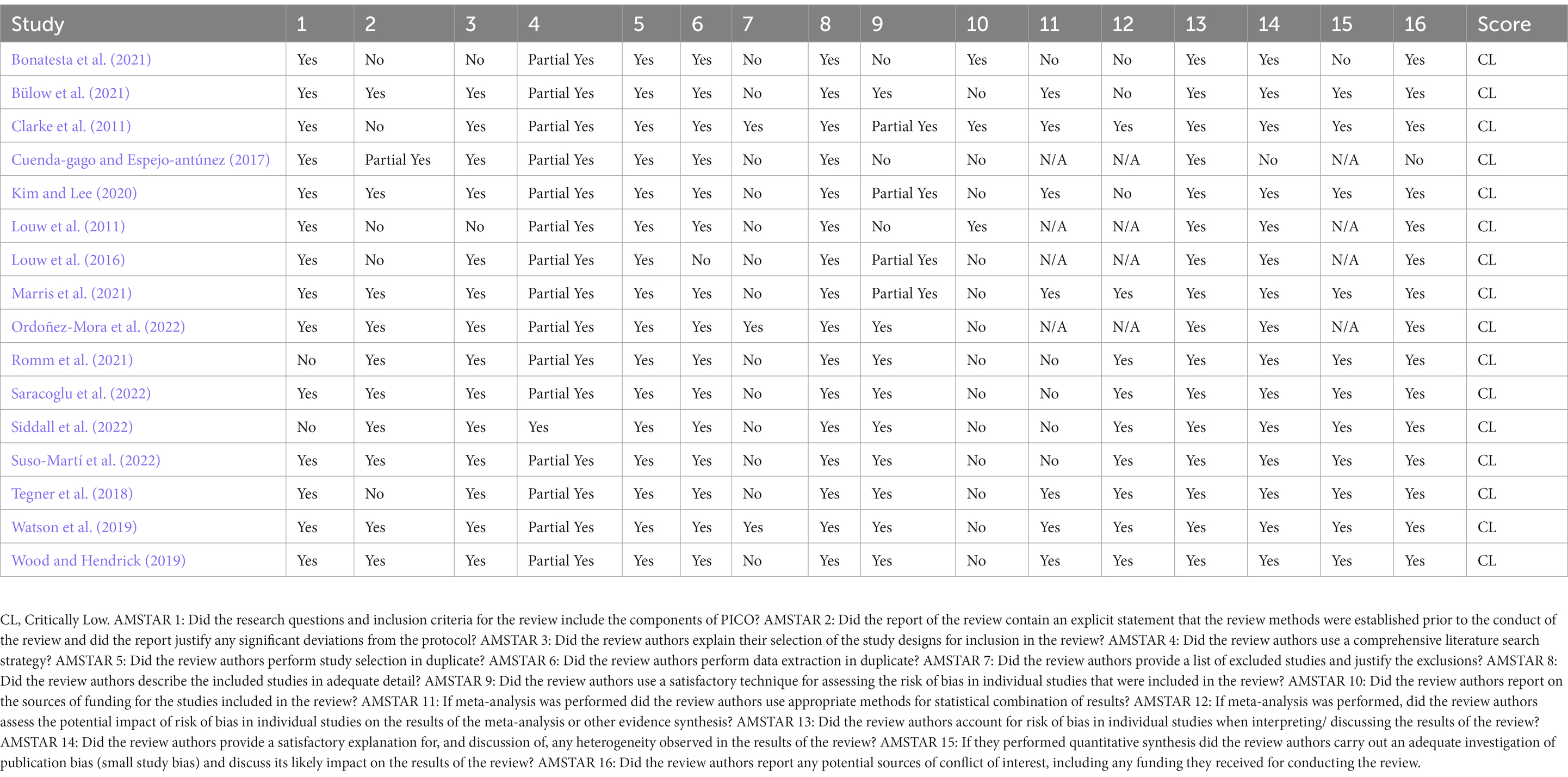
Table 2. AMSTAR results.
A subgroup analysis was performed with the aim of homogenizing the results. Therefore, a qualitative synthesis was performed for the following sets of patients with CMP: reviews that included all kind of patients with CMP (overall CMP), chronic spinal pain, patients with fibromyalgia and patients with osteoarthritis. In addition, results were presented according to the different time points: short term (< 3 months); medium-term (> 3 months but < 12 months) or long-term (≥ 12 months). A common effect size was estimated using the Cochrane recommendations and used for the qualitative synthesis in the figures (Higgins et al., 2023).
Three meta-analyses found between-group differences in pain scales showing an overall moderate effect favorable to PNE [Marris et al. (2021): Standardized Mean Difference (SMD) = −0.756; 95% Confidence Interval (CI): −0.059 to −1.571; Kim and Lee (2020): SMD = −0.53; 95% CI: −1.05 to −0.01; Romm et al. (2021): SMD = −0.85; 95% CI: −1.46 to −0.23].
In a temporal analysis, 4 meta-analyses observe a low to large effect favorable to PNE in the short term [Bülow et al. (2021): SMD = 0.32; 95% CI: 0.58 to −0.05; Watson et al. (2019): MD = 5.91; 95% CI: −13.75 to 1.93; Marris et al. (2021): SMD = 0.837; 95% CI: −0.299 to 1.972; Siddall et al. (2022): SMD = −2.09; 95% CI: 3.38 to −0.80] and low quality of evidence (Watson et al., 2019). 2 meta-analyses extrapolate the effects of PNE in the long term, showing small to large effects favorable to PNE [Bülow et al. (2021): SMD = 0.40; 95% CI: 0.78 to 0.03; Marris et al. (2021): SMD = 0.964; 95% CI: −0.032 to 1.959] (Figure 2).
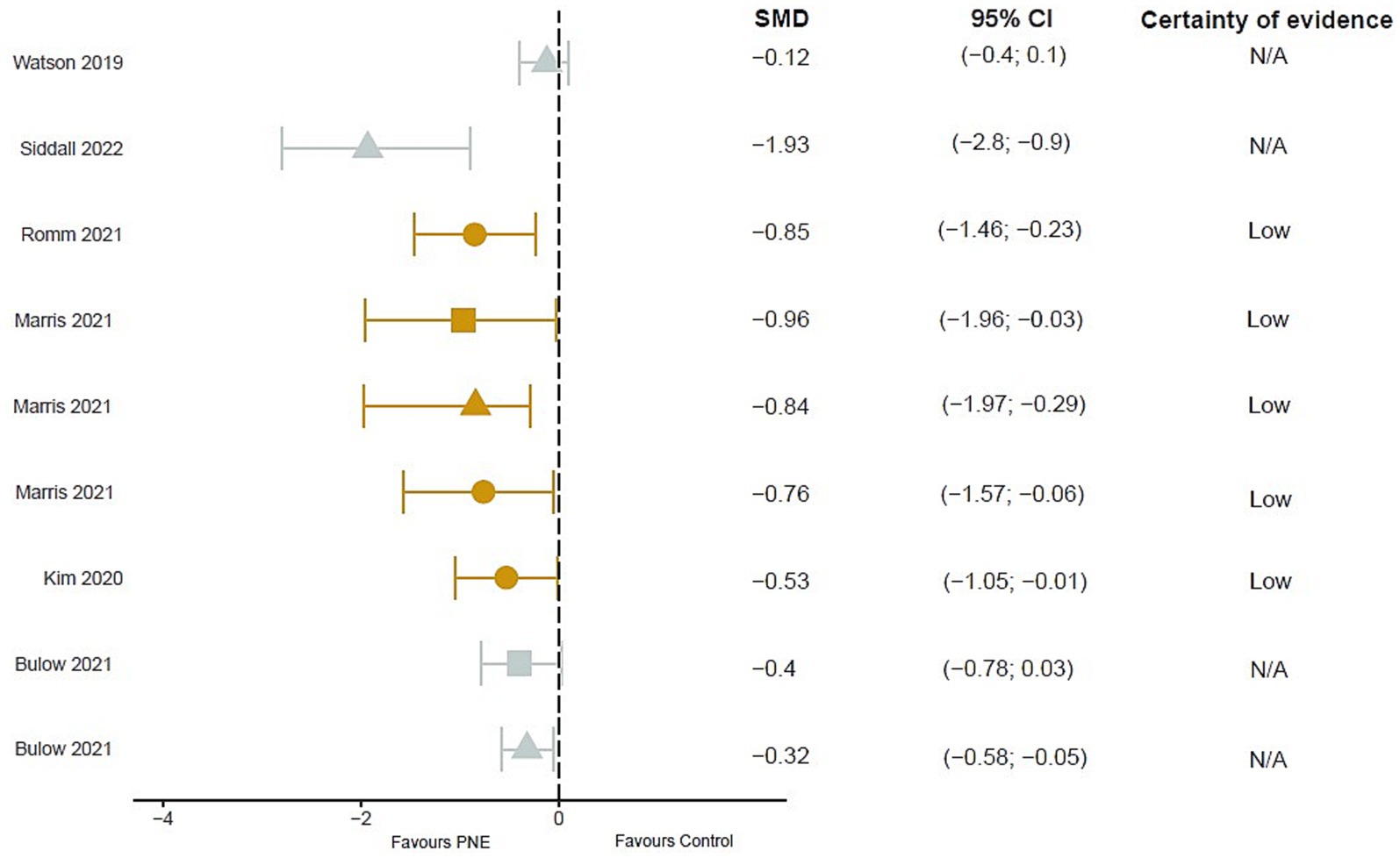
Figure 2. Results of mean differences regarding pain intensity in patients with overall chronic musculoskeletal pain. The colors show the certainty of evidence according to GRADE (red = very low certainty evidence; yellow = low certainty evidence; green = moderate certainty evidence, grey = not available). Circles = overall measurement; Triangles = short term measurement; square = long term measurement. SMD, Standardized mean difference; N/A, Not available; CI, Confidence interval.
Similarly, different reviews indicate that the combined treatment of PNE with exercise or another intervention showed better outcome compared to the conventional physiotherapy control group, a usual medical control, or an exercise-only group in the short, medium and long term (Louw et al., 2011, 2016; Cuenda-gago and Espejo-antúnez, 2017; Barbari et al., 2020).
6 meta-analyses (Watson et al., 2019; Bülow et al., 2021; Marris et al., 2021; Romm et al., 2021; Watson et al., 2021; Siddall et al., 2022) and 3 reviews (Louw et al., 2011, 2016; Cuenda-gago and Espejo-antúnez, 2017) analyzed the effect of PNE on different tools, such as the RMDQ, ODI, FIQ questionnaires and the QBPD and SF-36 scales.
2 meta-analyses observe a moderate to large effect in favor of PNE when compared to control groups following self-management education or treatment as usual, but with no statistically significant result in the case of Marris et al. (2021) (SMD = 1.009; 95% CI: −0.213 to 2.232) and showing statistically significant differences in Romm et al. (2021) (SMD = −0.48; 95% CI −0.82 to −0.15). In the short term 5 meta-analyses observed a small to moderate with moderate evidence favorable to PNE [Bülow et al. (2021): SMD = 0.17; 95% CI −0.34 to −0.01; Watson et al. (2019): MD = 4.09, 95% CI = 7.72 to 0.45; Watson et al. (2021): MD = 7.36, 95% CI = 3.93 to 11.12; Marris et al. (2021): SMD = 0.791; 95% CI −0.994 to 2.575; Siddall et al. (2022): SMD = −0.68; 95%CI −1.17 to −0.2]. 3 meta-analyses analyzed the effect in the medium and long term, favorable effects were observed with moderate evidence in the medium term [Watson et al. (2019): MD = 8.14]. In the long term, no statistically significant differences were observed [Bülow et al. (2021): SMD = 0.27; 95% CI: 0.59 to 0.06; Marris et al. (2021): SMD = 1.374; 95% CI: −0.103 to 2.850] (Figure 3).
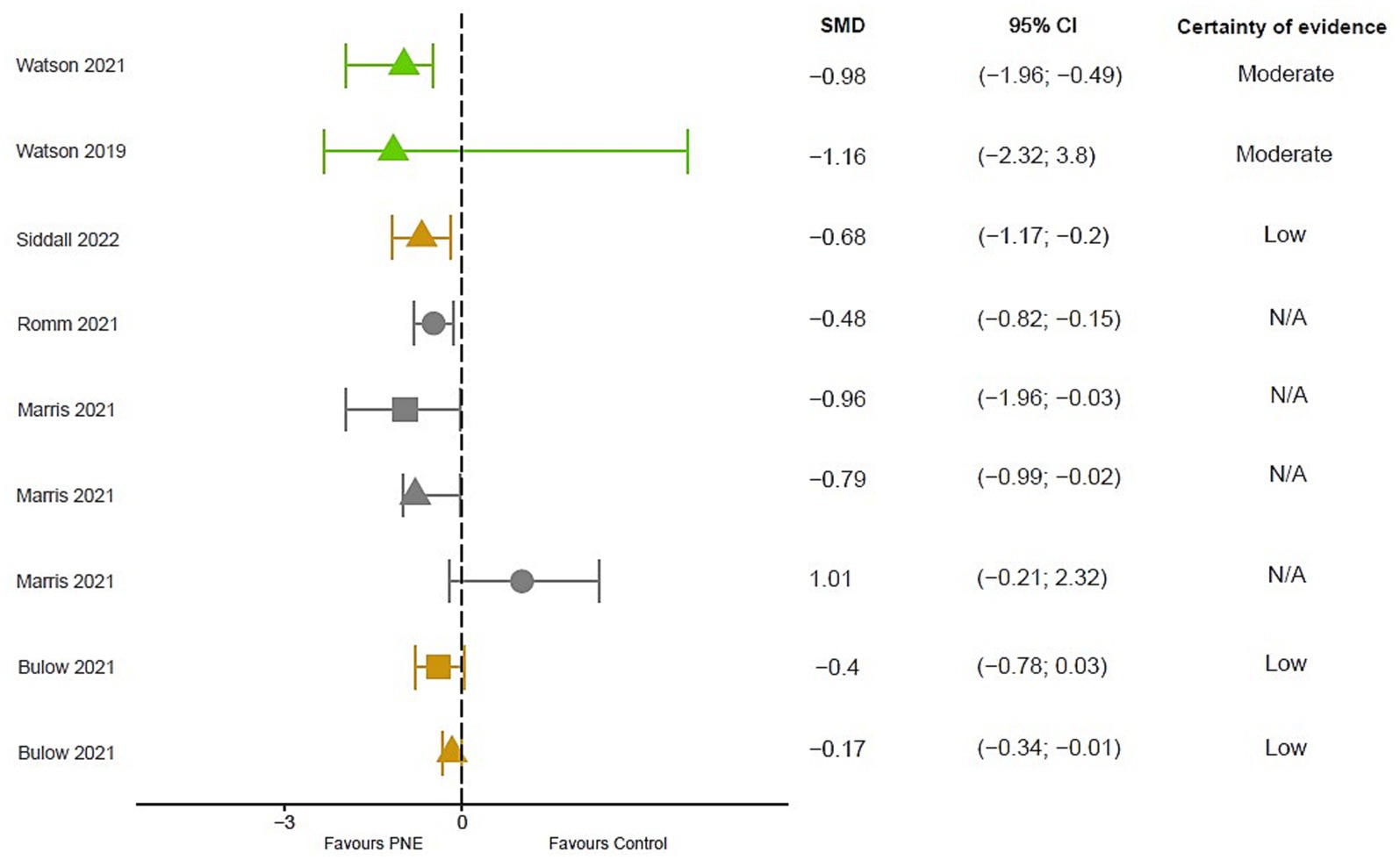
Figure 3. Results of mean differences regarding disability in patients with overall chronic musculoskeletal pain. The colors show the certainty of evidence according to GRADE (red = very low certainty evidence; yellow = low certainty evidence; green = moderate certainty evidence, grey = not available). Circles = overall measurement; Triangles = short term measurement; square = long term measurement. SMD, Standardized mean difference; N/A, Not available; CI, Confidence interval.
The included reviews observe superior effects of the use of PNE with respect to the control groups of conventional physical therapy or usual medical follow-up for the tools used RMDQ, ODI, NDI and PSFS when PNE is combined with TM and/or exercise (Louw et al., 2011, 2016; Cuenda-gago and Espejo-antúnez, 2017). However, controversies exist as no superiority could be demonstrated for the combination of PNE and DN compared to DN alone, as both groups improved on the ODI and NDI scale (Louw et al., 2016). A meta-analysis highlights a possible dependence of the control group compared to NSP on the total outcome effects (Romm et al., 2021).
5 meta-analyses (Watson et al., 2019; Kim and Lee, 2020; Bülow et al., 2021; Romm et al., 2021; Siddall et al., 2022) and 3 reviews (Louw et al., 2011, 2016; Cuenda-gago and Espejo-antúnez, 2017) conducted an analysis on the effects of PNE on variables such as kinesiophobia or catastrophizing.
4 meta-analyses found a large and statistically significant favorable effect in relation to kinesiophobia (TSK) [Romm et al. (2021): SMD = −1.71; Kim and Lee (2020): SMD = −0.86; 95% CI: −1.22 to −0.51; Watson et al. (2019): MD = 13.55; 95% CI, −25.89 to −1.21; Siddall et al. (2022); SMD = −1.20; 95% CI: 1.84 to −0.57]. In addition, 1 meta-analysis also found a benefit in catastrophizing [Watson et al. (2019): MD = 3.33; 95% CI: −6.01 to −0.65].
The included reviews follow the trend of favorable analysis of the use of PNE in the different treatments for TSK, PCS, SOPAR, and FABS scales (Louw et al., 2011, 2016; Cuenda-gago and Espejo-antúnez, 2017). They also highlight the possible influence of a group and individual treatment and the difference between only receiving one PNE session or several.
The overlap analysis performed using the GROOVE tool showed a corrected overlap area of 16.45%, showing a very high level of overlap. The detail of the overlap is shown in Figure 4.
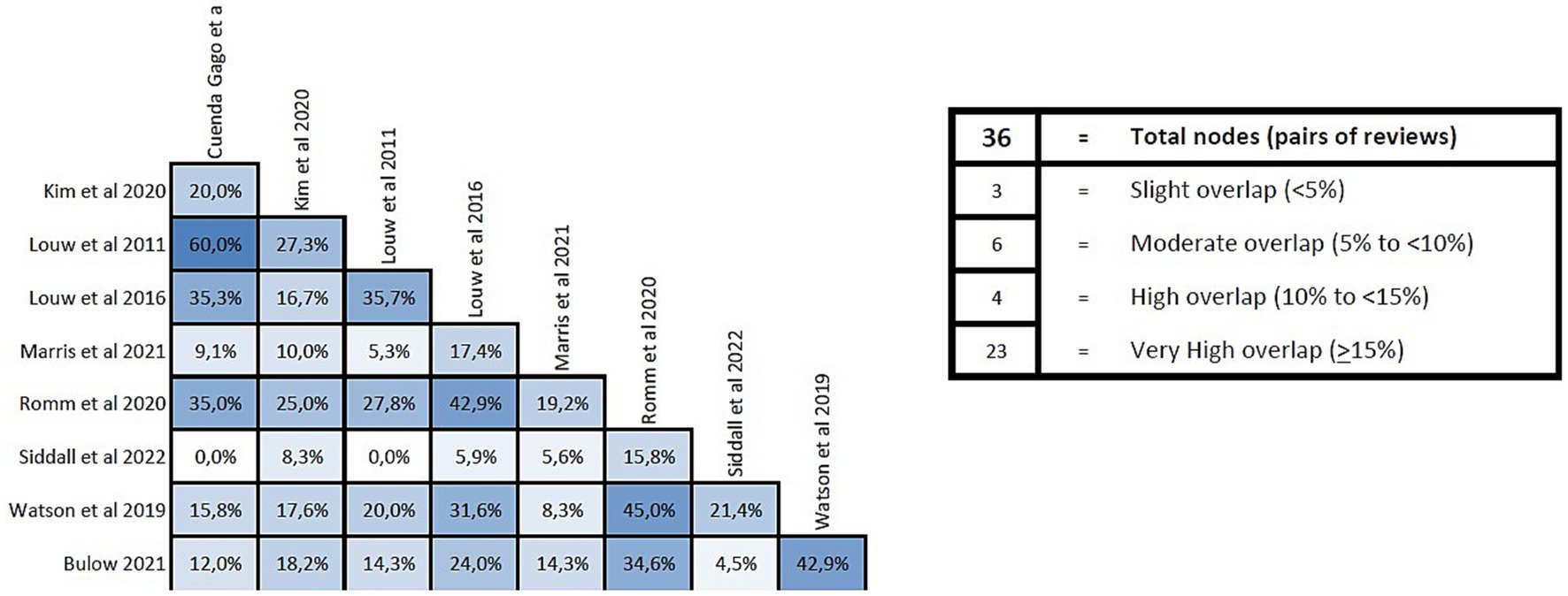
Figure 4. Overlap analysis performed using the GROOVE regarding reviews in patients with chronic musculoskeletal pain.
2 meta-analyses observed a small effect favorable to PNE with low evidence in the short term for low back pain [Wood and Hendrick (2019): Weighted Mean Difference (WMD) = 0.73; 95% CI −0.14 to 1.61; Tegner et al. (2018): WMD = −1.03; 95% CI: −0.55 to −1. 52], found similar results in general spine pain [Bonatesta et al. (2021): SMD = −0.53; 95% CI: −0.86 to −0.20]. In the medium term 2 meta-analyses showed similar results [Tegner et al. (2018): WMD = −1.09; 95% CI: −2.17 to 0.00; Bonatesta et al. (2021): SMD = −0.57; 95% CI: −1.01 to −0.14] (Figure 5).
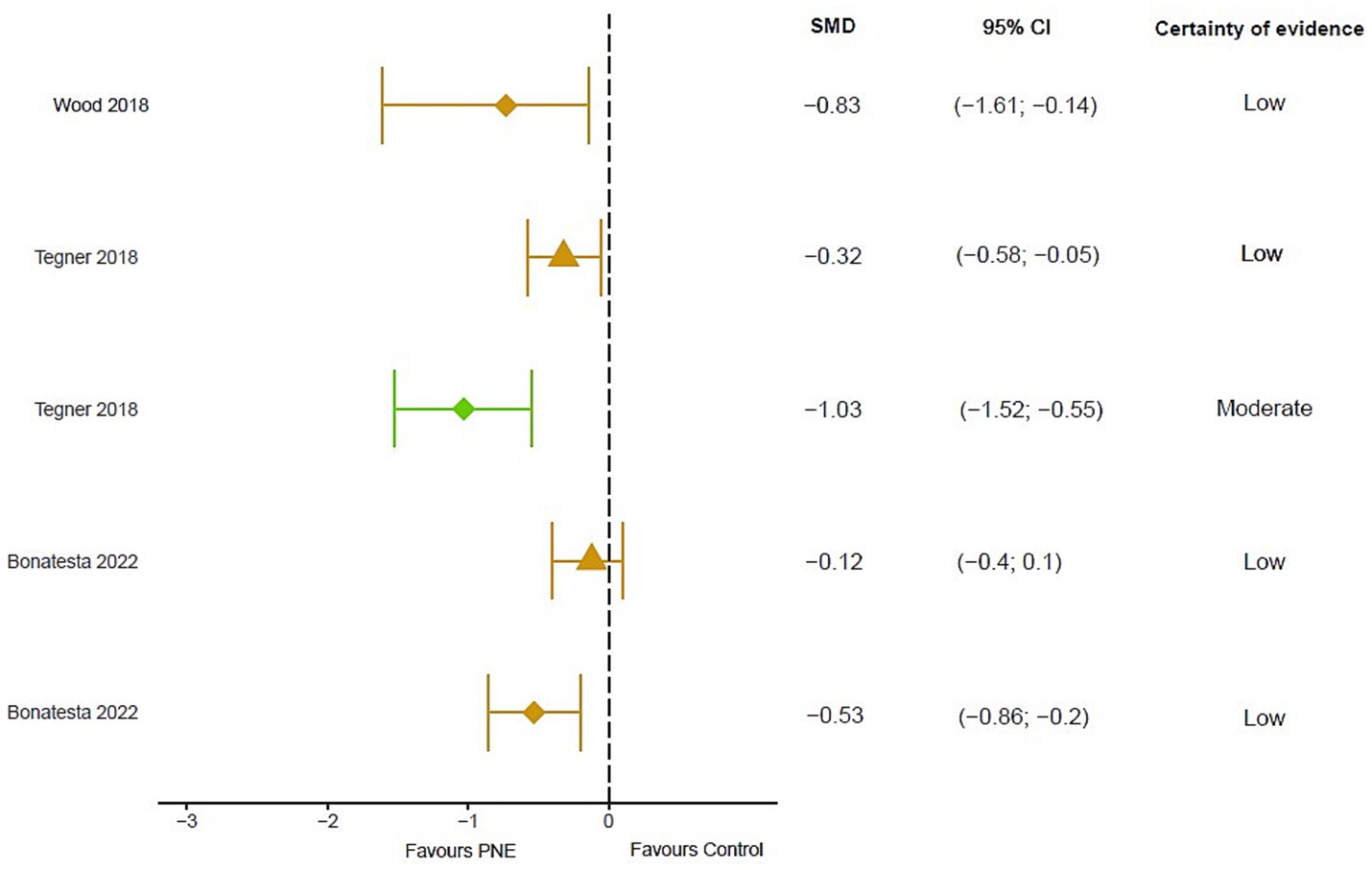
Figure 5. Results of mean differences regarding pain intensity in patients with overall chronic spinal pain. The colors show the certainty of evidence according to GRADE (red = very low certainty evidence; yellow = low certainty evidence; green = moderate certainty evidence, grey = not available). Circles = overall measurement; Triangles = short term measurement; diamond = medium term. SMD, Standardized mean difference; N/A, Not available; CI, Confidence interval.
2 meta-analyses analyzed the effects of PNE as sole treatment in low back pain, where a statistically significant result was obtained in the short term [Clarke et al. (2011): MD = 5] although these changes were not clinically significant. In contrast, in the medium term, significant clinical changes favorable to PNE were observed [Clarke et al. (2011): MD = 19]. The addition of PNE to treatment appears to improve outcomes in pain intensity, maintained in the short and long term (Barbari et al., 2020).
In the short term 2 meta-analyses observed a clinically significant effect of PNE together with multimodal treatment with moderate quality evidence [Wood and Hendrick (2019): WMD = 3.94; 95% CI 3.37 to 4.52; Tegner et al. (2018): SMD = −0.47; 95% CI: −0.80 to −0.13]. However, 1 meta-analysis observed no differences in the short-term use of PNE combined with exercise compared with the exercise-only control group with very low-quality evidence [Bonatesta et al. (2021): SMD = −0.24; 95% CI: −0.53 to 0.05]. 2 meta-analyses found favorable differences for PNE compared with exercise alone in the medium-term [Bonatesta et al. (2021): SMD = −0.93; 95% CI: −1.08 to −0.03; Tegner et al. (2018): SMD = −0.38; 95% CI, −0.74 to −0.02] with a low to moderate effect and very low-quality evidence. These results were not maintained in the long term [Wood and Hendrick (2019): WMD = 2.18; 95% CI: −0.67 to 5.02] (Figure 6).
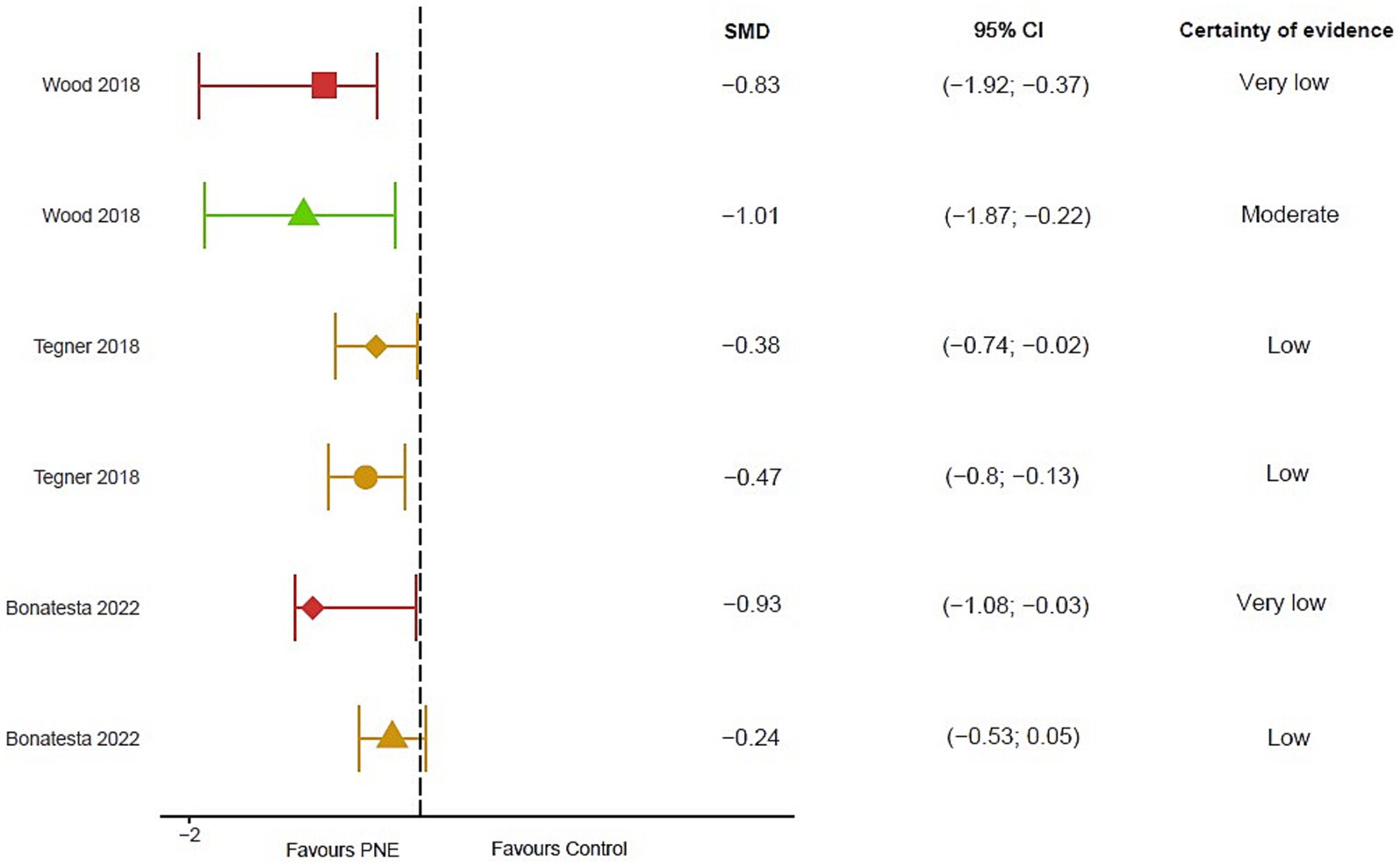
Figure 6. Results of mean differences regarding disability in patients with overall chronic spinal pain. The colors show the certainty of evidence according to GRADE (red = very low certainty evidence; yellow = low certainty evidence; green = moderate certainty evidence, grey = not available). Circles = overall measurement; Triangles = short term measurement; square = long term measurement; diamond = medium term. SMD, Standardized mean difference; N/A, Not available; CI, Confidence interval.
2 meta-analyses demonstrated a positive but not statistically significant effect for kinesiophobia in the short term [Wood and Hendrick (2019): WMD = 4.72; 95% CI: 2.32 to 7.13; Tegner et al. (2018): WMD = −5.73 (95% CI: −13.06 to 2.14)] or a global spine analysis [Bonatesta et al. (2021): SMD = −0.70; 95% CI: −1.51 to 0.11].
Similarly, 2 showed a positive but not statistically significant effect for catastrophizing in the short term for low back pain [Wood and Hendrick (2019): WMD = 2.54; 95% CI: −4.23 to 9.31] or the overall spine [Bonatesta et al. (2021): MD = −3.26; 95% CI: −6.15 to −0.37].
The overlap analysis performed using the GROOVE tool showed a corrected overlap area of 15.45%, showing a very high level of overlap. The detail of the overlap is shown in Figure 7.
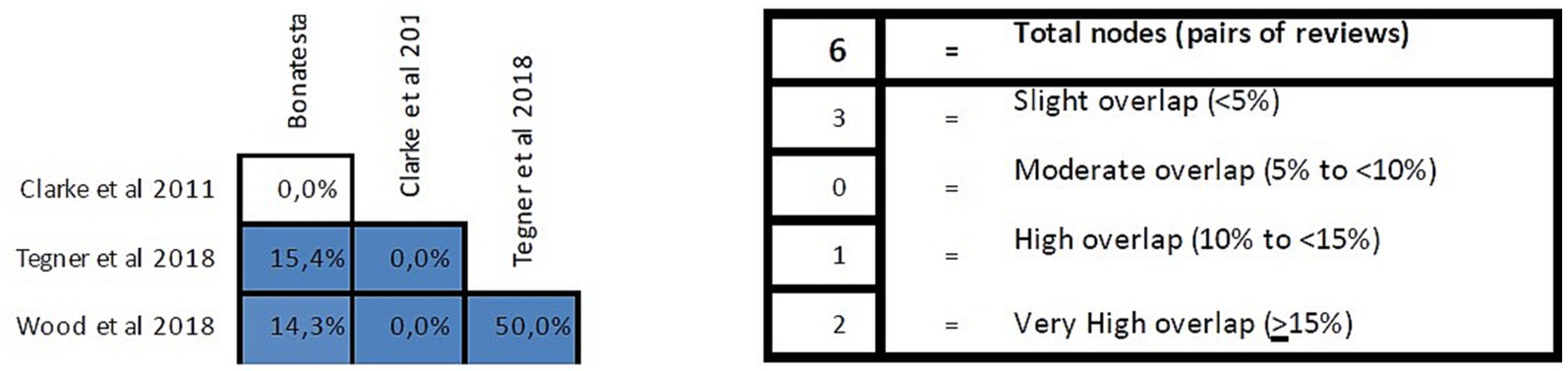
Figure 7. Overlap analysis performed using the GROOVE regarding reviews in patients with chronic spinal pain.
Two reviews with meta-analysis (Saracoglu et al., 2022; Suso-Martí et al., 2022) and two reviews analyzed the total effect of PNE in fibromyalgia. The most analyzed tools for pain intensity were the VAS scale and NPRS, and for assessing functionality the FIQ questionnaire and a subscale of the ICF. As for psychosocial variables, they were the HADS scale and the PCS questionnaire. The control groups with which the PNE was compared in the studies analyzed by the meta-analyses and reviews included in this work were: self-management techniques, TM, no intervention, exercise, other educational pathways.
Two meta-analyses evaluated the effect of PNE on pain intensity, showing significant differences between the intervention groups compared to the control group, where PNE obtained a moderate [Suso-Martí et al. (2022): SMD: −0.76; 95% CI: −1.33 to −0.19] to large [Saracoglu et al. (2022): SMD = −1.049; 95% CI = −1.400, −0.698] effect for the variables VAS and NPRS.
In the medium- and long-term analysis, it could not be affirmed (without significant differences) that PNE decreases pain intensity [Suso-Martí et al. (2022): SMD: −0.42; 95% CI: −0.93 to 0.08], although an overall favorable effect can be observed. PNE improved the efficacy of endogenous pain mechanisms and active coping to persistent pain (García-Ríos et al., 2019). In contrast, a review could not conclude that PNE in isolation treatment has a positive effect on pain intensity in the short and long term (Elizagaray-garcía et al., 2016).
The impact of fibromyalgia was measured by the FIQ questionnaire, where a meta-analysis did not observe a significant difference for PNE in post-intervention [Suso-Martí et al. (2022): SMD: −0.37; 95% CI: −0.85 to 0.11], also observing contradictory evidence on the CIF and SF-36 functionality subscale in the short-medium term where the combination of exercise and group PNE or other active coping strategies did improve pain intensity for the CIF subscale (Elizagaray-garcía et al., 2016). We did observe a favorable clinical effect on FM severity in the medium and long term in PNE [Suso-Martí et al. (2022): SMD = 0.44; 95% CI: −0.73 to −0.14] coinciding with another meta-analysis showing a large effect of PNE in the intervention groups (SMD = −1.051; 95% CI: −1.309 to −0.793) (Saracoglu et al., 2022).
Regarding psychosocial variables, the meta-analysis by Suso-Martí et al. (2022) evaluated PNE outcomes in the short term, where no significant difference was observed for anxiety (SMD = −0.06; 95% CI: −0.67 to 0.55) and catastrophizing (SMD = −0.10; 95% CI: −0.52 to 0.32). In the medium and long term, no statistical differences were also found for anxiety (SMD = −0.07; 95% CI: −0.69 to 0.82) or catastrophizing (SMD = −0.16; 95% CI: −0.52 to 0.19). However, the Saracoglu et al. (2022) meta-analysis did note statistical differences between groups favorable to PNE for the PCS scale with a large effect (SMD = −0.893; 95% CI: −1.437 to −0.348). A moderate effect was also noted for the HADS scale for anxiety (SMD = −0.711; 95% CI: −0.869 to −0.552) and depression (SMD = −0.686; 95% CI: −0.849 to −0.523).
Only one review analyzed the effects of PNE as a treatment in intervention groups (Ordoñez-Mora et al., 2022). Only 4 studies were included in the review and were performed on patients with radiologically proven knee OA (with diagnosis time of over 6 months) and candidates for total knee arthroplasty. Regarding pain intensity, measured by the NRS scale, a positive trend in the use of PNE was observed, but without significant differences when compared to a group without intervention or preoperative biomedical education with manual therapy as a common treatment. However, there were significant changes in favor of PNE combined with exercise compared to exercise alone. There were no significant differences between groups for functionality in the WOMAC scale analysis when PNE was compared to biomedical education. For psychosocial variables, an overall favorable trend was indicated for TSK and PCS without being significant.
The main aim of this umbrella review was to assess the effectiveness of PNE in patients with CMP. In general terms, it seems that the addition of the PNE-based intervention to other treatments, mostly exercise-based interventions although we might refer to it in terms of a multimodal approach, leads to greater clinical improvements than the multimodal approach alone. We have found this especially in the reduction of the influence of psychosocial variables. However, it seems that studies testing the effectiveness of PNE in isolation, systematic reviews with or without meta-analysis did not show statistically significant improvements overall in terms of pain intensity, disability levels or psychosocial variables. It seems therefore that the main strength of the PNE is the interaction with other interventions to enhance its effectiveness with respect to the outcomes assessed. All the reviews included had scored as “critically low” quality and the overlapping analysis showed a very high level of overlap. These aspects limit the clinical application of the recommendations made to date on PNE in CMP patients, and therefore its clinical efficacy is uncertain and dependent on several factors that need to be further explored.
PNE is a clinical intervention that has the communication process as a key point of its application and where the patient feels listened to, cared for and, in addition, allows patients to better understand their clinical condition process (Street et al., 2009). This increased knowledge from a patient perspective, together with an adequate context promoted by empathy, shared understanding between health professional and patient and increasing social support, seems to help improve the influence of psychological variables that are widely present in chronic musculoskeletal pain processes (Lee et al., 2016; Traeger et al., 2019). However, the mechanisms that explain the functioning and benefits of PNE are not entirely clear. It has been suggested that this intervention might be especially relevant for the affective-emotional component of pain (Moseley and Butler, 2015), which could lead to better coping strategies (Nijs et al., 2017). In addition, PNE could modify perceptual error in threat signal assessment in the neural network involved in pain perception, reducing nervous system sensitivity and brain activity (Saracoglu et al., 2022).
Based on the results of the present review, a clinical approach based solely on PNE alone may be insufficient to provide clinically relevant and meaningful results, and it seems that the current state of the art tells us that we should combine it with an active and/or passive intervention (such as exercise-based interventions, manual neuro-orthopedic physical therapy, etc.) in order to improve its effectiveness. Positive effects on decreasing pain intensity, disability levels or catastrophic thoughts have been reported when researchers combined PNE together with an exercise-based intervention compared with the exercise-based intervention in isolation in patients with chronic musculoskeletal pain (Siddall et al., 2022) or in patients with chronic non-specific spinal pain (Bonatesta et al., 2021). Given that exercise has already shown positive results in patients with musculoskeletal disorders with pain such as fibromyalgia syndrome (Sosa-Reina et al., 2017; Estévez-López et al., 2021) or chronic non-specific low back pain (Hayden et al., 2005; Searle et al., 2015) in the scientific literature, future studies seem to address whether PNE could improve the efficacy of exercise-based interventions, as is the case for chronic musculoskeletal pain. It seems that our work sheds some light on this issue, although future studies should address some of the limitations and weaknesses found in the present manuscript. Finally, there is great variability in the results found depending on the different variables (content of the sessions, the format, the interventions added to the session, the characteristics of the population or the duration of the intervention). In this regard, recently, a meta-analysis found a linear association between the duration of PNE and the reduction of anxiety symptoms, catastrophizing and kinesiophobia (Salazar-Méndez et al., 2023). Future studies should determine not only whether PNE is effective, but also in which patients it is effective and in what way it is best to apply it.
This study presents several limitations. First, part of the included studies presented low methodological quality and a great heterogeneity. Second, there was inconsistency between the systematic reviews in terms of the interventions and control groups, and this limits the strength of the conclusions. Finally, as no statistical aggregation could be performed due to the low number of included studies, the conclusions are somewhat ambiguous as they satisfy a qualitative analysis, and not a quantitative one (which would be more robust).
The addition PNE-based intervention to other treatments leads to greater clinical improvements than alone interventions based on physical therapy or exercise modalities, especially in the reduction of the influence of psychosocial variables. However, the effectiveness of PNE in isolation did not show statistically significant improvements overall in terms of pain intensity, disability levels or psychosocial variables. There is a great heterogeneity in the results obtained and the PNE protocols used, a critically low quality in the reviews included and a very high overlap, so there is a need to improve the studies in this field before clinical application.
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
FC-M: Investigation, Methodology, Writing – original draft, Writing – review & editing. LS-M: Conceptualization, Data curation, Methodology, Resources, Supervision, Validation, Writing – original draft, Writing – review & editing. JC: Data curation, Formal Analysis, Project administration, Writing – original draft, Writing – review & editing. FF-S: Investigation, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. VM-A: Methodology, Writing – original draft, Writing – review & editing. PA-Q: Methodology, Writing – original draft, Writing – review & editing. GB-R: Conceptualization, Data curation, Formal Analysis, Investigation, Project administration, Resources, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by Generalitat Valenciana (Subvenciones para grupos de investigación emergentes: CIGE/2022/178).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2023.1272068/full#supplementary-material
Adams, L. M., and Turk, D. C. (2018). Central sensitization and the biopsychosocial approach to understanding pain. J. Appl. Biobehav. Res. 23:e12125. doi: 10.1111/JABR.12125
Apkarian, A., and Baliki, M. (2009). Neurobiology PG-P in, 2009 Undefined. Towards a theory of chronic pain. Elsevier. Available at: https://www.sciencedirect.com/science/article/pii/S0301008208001135. (Accessed December 15, 2020)
Barbari, V., Storari, L., Ciuro, A., and Testa, M. (2020). Effectiveness of communicative and educative strategies in chronic low back pain patients: a systematic review. Patient Educ. Couns. 103, 908–929. doi: 10.1016/j.pec.2019.11.031
Barbari, V., Storari, L., Maselli, F., and Testa, M. (2021). Applicability of pain neuroscience education: where are we now? J. Back Musculoskelet. Rehabil. 34, 511–520. doi: 10.3233/BMR-200091
Barton, C. J., Webster, K. E., and Menz, H. B. (2008). Evaluation of the scope and quality of systematic reviews on nonpharmacological conservative treatment for patellofemoral pain syndrome. J. Orthop. Sports Phys. Ther. 38, 529–541. doi: 10.2519/jospt.2008.2861
Bonatesta, L., Ruiz-Cárdenas, J. D., Fernández-Azorín, L., and Rodríguez-Juan, J. J. (2021). Pain science education plus exercise therapy in chronic nonspecific spinal pain: a systematic review and Meta-analyses of randomized clinical trials. J. Pain 23, 535–546. doi: 10.1016/J.JPAIN.2021.09.006
Bougioukas, K. I., Liakos, A., Tsapas, A., Ntzani, E., and Haidich, A. B. (2018). Preferred reporting items for overviews of systematic reviews including harms checklist: a pilot tool to be used for balanced reporting of benefits and harms. J. Clin. Epidemiol. 93, 9–24. doi: 10.1016/j.jclinepi.2017.10.002
Breivik, H., Collett, B., Ventafridda, V., Cohen, R., and Gallacher, D. (2006). Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur. J. Pain 10:287. doi: 10.1016/J.EJPAIN.2005.06.009
British Pain Society. The British pain society participant information for pain management Programmes. (2013).
Bülow, K., Lindberg, K., Vaegter, H. B., and Juhl, C. B. (2021). Effectiveness of pain neurophysiology education on musculoskeletal pain: a systematic review and meta-analysis. Pain Med. 22, 891–904. doi: 10.1093/pm/pnaa484
Clarke, C. L., Ryan, C. G., and Martin, D. J. (2011). Pain neurophysiology education for the management of individuals with chronic low back pain: a systematic review and meta-analysis. Man. Ther. 16, 544–549. doi: 10.1016/j.math.2011.05.003
Cuenda-gago, J. D., and Espejo-antúnez, L. (2017). Efectividad de la educación basada en neurociencia en el abordaje del dolor crónico musculoesquelético. Crónico 65, 1–12. doi: 10.33588/rn.6501.2016561
Edwards, R. R., Dworkin, R. H., Sullivan, M. D., Turk, D. C., and Wasan, A. D. (2016). The role of psychosocial processes in the development and maintenance of chronic pain. J. Pain 17, T70–T92. doi: 10.1016/J.JPAIN.2016.01.001
Elizagaray-garcía, I., Muriente-gonzález, J., and Gil-martínez, A. (2016). Educación al paciente con fibromialgia. Rev. Neurol. 62, 49–60. doi: 10.33588/rn.6202.2015446
Engers, A., Jellema, P., Wensing, M., Van Der Windt, D. A. W. M., Grol, R., and Van Tulder, M. W. (2008). Individual patient education for low back pain. Cochrane Database Syst. Rev. 2008:CD004057. doi: 10.1002/14651858.CD004057.PUB3
Espinoza, M. A., Bilbeny, N., Abbott, T., Carcamo, C., Zitko, P., Zamorano, P., et al. (2022). Cost analysis of chronic pain due to musculoskeletal disorders in Chile. PLoS One 17:e0273667. doi: 10.1371/JOURNAL.PONE.0273667
Estévez-López, F., Maestre-Cascales, C., Russell, D., Álvarez-Gallardo, I. C., Rodriguez-Ayllon, M., Hughes, C. M., et al. (2021). Effectiveness of exercise on fatigue and sleep quality in fibromyalgia: a systematic review and Meta-analysis of randomized trials. Arch. Phys. Med. Rehabil. 102, 752–761. doi: 10.1016/J.APMR.2020.06.019
García-Ríos, M. C., Navarro-Ledesma, S., Tapia-Haro, R. M., Toledano-Moreno, S., Casas-Barragán, A., Correa-Rodríguez, M., et al. (2019). Effectiveness of health education in patients with fibromyalgia: a systematic review. Eur. J. Phys. Rehabil. Med. 55, 301–313. doi: 10.23736/S1973-9087.19.05524-2
Goldberg, D. S., and McGee, S. J. (2011). Pain as a global public health priority. BMC Public Health 11:11. doi: 10.1186/1471-2458-11-770
Graven-Nielsen, T., and Arendt-Nielsen, L. (2010). Assessment of mechanisms in localized and widespread musculoskeletal pain. Nat. Rev. Rheumatol. 6, 599–606. doi: 10.1038/NRRHEUM.2010.107
Hayden, J. A., Van Tulder, M. W., Antti Malmivaara, V., and Koes, B. W. (2005). Meta-analysis: exercise therapy for nonspecific low Back pain. Ann. Intern. Med. 142, 765–775. doi: 10.7326/0003-4819-142-9-200505030-00013
Higgins, J. P. T., Thomas, J., Chandler, J., Cumpston, M., Li, T., Page, M. J. (eds.), et al. (2023). Cochrane Handbook for Systematic Reviews of Interventions version 6.4. Cochrane, 2023. Available at: www.training.cochrane.org/handbook
Ioannidis, J. P. A. (2016). The mass production of redundant, misleading, and conflicted systematic reviews and meta-analyses. Milbank Q. 94, 485–514. doi: 10.1111/1468-0009.12210
Keefe, F. J., Rumble, M. E., Scipio, C. D., Giordano, L. A., and Perri, L. M. (2004). Psychological aspects of persistent pain: current state of the science. J. Pain 5, 195–211. doi: 10.1016/j.jpain.2004.02.576
Kim, H., and Lee, S. (2020). Effects of pain neuroscience education on kinesiophobia in patients with chronic pain: a systematic review and meta-analysis. Phys. Ther. Rehabil. Sci. 9, 309–317. doi: 10.14474/ptrs.2020.9.4.309
Lee, H., McAuley, J. H., Hübscher, M., Kamper, S. J., Traeger, A. C., and Moseley, G. L. (2016). Does changing pain-related knowledge reduce pain and improve function through changes in catastrophizing? Pain 157, 922–930. doi: 10.1097/J.PAIN.0000000000000472
Louw, A., Diener, I., Butler, D. S., and Puentedura, E. J. (2011). The effect of neuroscience education on pain, disability, anxiety, and stress in chronic musculoskeletal pain. Arch. Phys. Med. Rehabil. 92, 2041–2056. doi: 10.1016/j.apmr.2011.07.198
Louw, A., Zimney, K., Puentedura, E. J., and Diener, I. (2016). The efficacy of pain neuroscience education on musculoskeletal pain: a systematic review of the literature. Physiother. Theory Pract. 32, 332–355. doi: 10.1080/09593985.2016.1194646
Lunny, C., Pieper, D., Thabet, P., and Kanji, S. (2021). Managing overlap of primary study results across systematic reviews: practical considerations for authors of overviews of reviews. BMC Med. Res. Methodol. 21, 1–14. doi: 10.1186/S12874-021-01269-Y/FIGURES/4
Marris, D., Theophanous, K., Cabezon, P., Dunlap, Z., and Donaldson, M. (2021). The impact of combining pain education strategies with physical therapy interventions for patients with chronic pain: a systematic review and meta-analysis of randomized controlled trials. Physiother. Theory Pract. 37, 461–472. doi: 10.1080/09593985.2019.1633714
McHugh, M. L. (2012). Interrater reliability: the kappa statistic. Biochem. Med. 22, 276–282. doi: 10.11613/bm.2012.031
Moher, D., Pham, B., Jones, A., Cook, D. J., Jadad, A. R., Moher, M., et al. (1998). Does quality of reports of randomised trials affect estimates of intervention efficacy reported in meta-analyses? Lancet 352, 609–613. doi: 10.1016/S0140-6736(98)01085-X
Moseley, G. L. (2013). Reconceptualising pain according to modern pain science. Physical Therapy Reviews 12, 169–178. doi: 10.1179/108331907X223010
Moseley, G. L., and Butler, D. S. (2015). Fifteen years of explaining pain: the past, present, and future. J. Pain 16, 807–813. doi: 10.1016/J.JPAIN.2015.05.005
Nijs, J., Clark, J., Malfliet, A., and Ickmans, K. (2017). LV-CE, 2017 undefined. In the spine or in the brain? Recent advances in pain neuroscience applied in the intervention for low back pain. Res Nijs, J Clark, a Malfliet, K Ickmans, L Voogt, S Don, H den Bandt, D Goubert, J KregelClin Exp Rheumatol, 2017•researchgate.net. https://www.researchgate.net/profile/Hester-Bandt/publication/320414985_In_the_spine_or_in_the_brain_Recent_advances_in_pain_neuroscience_applied_in_the_intervention_for_low_back_pain/links/59eee45a4585154350e83445/In-the-spine-or-in-the-brain-Recent-advances-in-pain-neuroscience-applied-in-the-intervention-for-low-back-pain.pdf (Accessed October 27, 2023)
Nijs, J., Paul van Wilgen, C., Van Oosterwijck, J., van Ittersum, M., and Meeus, M. (2011). How to explain central sensitization to patients with “unexplained” chronic musculoskeletal pain: practice guidelines. Man. Ther. 16, 413–418. doi: 10.1016/J.MATH.2011.04.005
Ordoñez-Mora, L. T., Morales-Osorio, M. A., and Rosero, I. D. (2022). Effectiveness of interventions based on pain neuroscience education on pain and psychosocial variables for osteoarthritis: a systematic review. Int. J. Environ. Res. Public Health 19:2559. doi: 10.3390/ijerph19052559
Pérez-Bracchiglione, J., Meza, N., Bangdiwala, S. I., Niño de Guzmán, E., Urrútia, G., Bonfill, X., et al. (2022). Graphical representation of overlap for OVErviews: GROOVE tool. Res. Synth. Methods 13, 381–388. doi: 10.1002/JRSM.1557
Robinson, V., King, R., Ryan, C. G., and Martin, D. J. (2016). A qualitative exploration of people’s experiences of pain neurophysiological education for chronic pain: the importance of relevance for the individual. Man. Ther. 22, 56–61. doi: 10.1016/J.MATH.2015.10.001
Romm, M. J., Ahn, S., Fiebert, I., and Cahalin, L. P. (2021). A meta-analysis of therapeutic pain neuroscience education, using dosage and treatment format as moderator variables. Pain Pract. 21, 366–380. doi: 10.1111/PAPR.12962
Salazar-Méndez, J., Leão Ribeiro, I., Garrido-Castillo, M., and Gacitúa, J. (2023). Effects of pain neuroscience education on psycho-emotional and cognitive variables in individuals with chronic musculoskeletal pain: a systematic review of randomised clinical trials. Eur. J. Phys., 1–9. doi: 10.1080/21679169.2022.2162962
Salazar-Méndez, J., Núñez-Cortés, R., Suso-Martí, L., Ribeiro, I. L., Garrido-Castillo, M., Gacitúa, J., et al. (2023). Dosage matters: uncovering the optimal duration of pain neuroscience education to improve psychosocial variables in chronic musculoskeletal pain. A systematic review and meta-analysis with moderator analysis. Neurosci. Biobehav. Rev. 153:105328. doi: 10.1016/J.NEUBIOREV.2023.105328
Saracoglu, I., Akin, E., and Aydin Dincer, G. B. (2022). Efficacy of adding pain neuroscience education to a multimodal treatment in fibromyalgia: a systematic review and meta-analysis. Int. J. Rheum. Dis. 25, 394–404. doi: 10.1111/1756-185X.14293
Searle, A., Spink, M., Ho, A., and Chuter, V. (2015). Exercise interventions for the treatment of chronic low back pain: a systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 29, 1155–1167. doi: 10.1177/0269215515570379
Siddall, B., Ram, A., Jones, M. D., Booth, J., Perriman, D., and Summers, S. J. (2022). Short-term impact of combining pain neuroscience education with exercise for chronic musculoskeletal pain: a systematic review and meta-analysis. Pain 163, E20–E30. doi: 10.1097/j.pain.0000000000002308
Sosa-Reina, M. D., Nunez-Nagy, S., Gallego-Izquierdo, T., Pecos-Martín, D., Monserrat, J., and Álvarez-Mon, M. (2017). Effectiveness of therapeutic exercise in fibromyalgia syndrome: a systematic review and meta-analysis of randomized clinical trials. Biomed. Res. Int. 2017, 1–14. doi: 10.1155/2017/2356346
Stone, P. W. (2002). Popping the (PICO) question in research and evidence-based practice. Appl. Nurs. Res. 15, 197–198. doi: 10.1053/apnr.2002.34181
Street, R. L., Makoul, G., Arora, N. K., and Epstein, R. M. (2009). How does communication heal? Pathways linking clinician-patient communication to health outcomes. Patient Educ. Couns. 74, 295–301. doi: 10.1016/j.pec.2008.11.015
Suso-Martí, L., Cuenca-Martínez, F., Alba-Quesada, P., Muñoz-Alarcos, V., Herranz-Gómez, A., Varangot-Reille, C., et al. (2022). Effectiveness of pain neuroscience education in patients with fibromyalgia: a systematic review and meta-analysis. Pain Med. 23, 1837–1850. doi: 10.1093/PM/PNAC077
Tegner, H., Frederiksen, P., Esbensen, B. A., and Juhl, C. (2018). Neurophysiological pain education for patients with chronic low Back pain. Clin. J. Pain 34, 778–786. doi: 10.1097/AJP.0000000000000594
Traeger, A. C., Lee, H., Hübscher, M., Skinner, I. W., Moseley, G. L., Nicholas, M. K., et al. (2019). Effect of intensive patient education vs placebo patient education on outcomes in patients with acute low Back pain: a randomized clinical trial. JAMA Neurol. 76, 161–169. doi: 10.1001/JAMANEUROL.2018.3376
Turk, D. C., and Okifuji, A. (2002). Psychological factors in chronic pain: evolution and revolution. J. Consult. Clin. Psychol. 70, 678–690. doi: 10.1037//0022-006x.70.3.678
Tüzün, E. H. (2007). Quality of life in chronic musculoskeletal pain. Best Pract. Res. Clin. Rheumatol. 21, 567–579. doi: 10.1016/J.BERH.2007.03.001
Vos, T., Flaxman, A. D., Naghavi, M., Lozano, R., Michaud, C., Ezzati, M., et al. (2012). Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet (London, England). 380, 2163–2196. doi: 10.1016/S0140-6736(12)61729-2
Watson, J. A., Ryan, C. G., Atkinson, G., Williamson, P., Ellington, D., Whittle, R., et al. (2021). Inter-individual differences in the responses to pain neuroscience education in adults with chronic musculoskeletal pain: a systematic review and Meta-analysis of randomized controlled trials. J. Pain 22, 9–20. doi: 10.1016/J.JPAIN.2020.03.006
Watson, J. A., Ryan, C. G., Cooper, L., Ellington, D., Whittle, R., Lavender, M., et al. (2019). Pain neuroscience education for adults with chronic musculoskeletal pain: a mixed-methods systematic review and Meta-analysis. J. Pain 20, 1140.e1–1140.e22. doi: 10.1016/J.JPAIN.2019.02.011/ATTACHMENT/BD966D05-98F1-4017-9CDD-901E82307708/MMC1.DOCX
Wood, L., and Hendrick, P. A. (2019). A systematic review and meta-analysis of pain neuroscience education for chronic low back pain: short-and long-term outcomes of pain and disability. Eur. J. Pain 23, 234–249. doi: 10.1002/EJP.1314
Keywords: chronic musculoskeletal pain, pain education, pain neuroscience education, musculoskeletal pain, umbrella review
Citation: Cuenca-Martínez F, Suso-Martí L, Calatayud J, Ferrer-Sargues FJ, Muñoz-Alarcos V, Alba-Quesada P and Biviá-Roig G (2023) Pain neuroscience education in patients with chronic musculoskeletal pain: an umbrella review. Front. Neurosci. 17:1272068. doi: 10.3389/fnins.2023.1272068
Edited by:
Jaqueline Martins Priuli, University of São Paulo, BrazilReviewed by:
Cory Alcon, High Point University, United StatesCopyright © 2023 Cuenca-Martínez, Suso-Martí, Calatayud, Ferrer-Sargues, Muñoz-Alarcos, Alba-Quesada and Biviá-Roig. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Luis Suso-Martí, bHVpcy5zdXNvQHV2LmVz
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.