 Fernando García-Gutiérrez1†
Fernando García-Gutiérrez1† Marta Marquié1,2†Nathalia Muñoz1
Marta Marquié1,2†Nathalia Muñoz1 Montserrat Alegret1,2
Montserrat Alegret1,2 Amanda Cano1,2
Amanda Cano1,2 Itziar de Rojas1,2
Itziar de Rojas1,2 Pablo García-González1Clàudia Olivé1
Pablo García-González1Clàudia Olivé1 Raquel Puerta1
Raquel Puerta1 Adelina Orellana1,2
Adelina Orellana1,2 Laura Montrreal1Vanesa Pytel1Mario Ricciardi1
Laura Montrreal1Vanesa Pytel1Mario Ricciardi1 Carla Zaldua3Peru Gabirondo3
Carla Zaldua3Peru Gabirondo3 Wolfram Hinzen4,5Núria Lleonart1
Wolfram Hinzen4,5Núria Lleonart1 Ainhoa García-Sánchez1
Ainhoa García-Sánchez1 Lluís Tárraga1,2
Lluís Tárraga1,2 Agustín Ruiz1,2
Agustín Ruiz1,2 Mercè Boada1,2
Mercè Boada1,2 Sergi Valero1,2*
Sergi Valero1,2*- 1Ace Alzheimer Center Barcelona, Universitat Internacional de Catalunya, Barcelona, Spain
- 2Networking Research Center on Neurodegenerative Diseases (CIBERNED), Instituto de Salud Carlos III, Madrid, Spain
- 3Accexible Impacto s.l., Urduliz, Bizkaia, Spain
- 4Department of Translation and Language Sciences, Universitat Pompeu Fabra, Barcelona, Spain
- 5Institut Català de Recerca i Estudis Avançats (ICREA), Barcelona, Spain
Alzheimer's disease (AD) is a neurodegenerative condition characterized by a gradual decline in cognitive functions. Currently, there are no effective treatments for AD, underscoring the importance of identifying individuals in the preclinical stages of mild cognitive impairment (MCI) to enable early interventions. Among the neuropathological events associated with the onset of the disease is the accumulation of amyloid protein in the brain, which correlates with decreased levels of Aβ42 peptide in the cerebrospinal fluid (CSF). Consequently, the development of non-invasive, low-cost, and easy-to-administer proxies for detecting Aβ42 positivity in CSF becomes particularly valuable. A promising approach to achieve this is spontaneous speech analysis, which combined with machine learning (ML) techniques, has proven highly useful in AD. In this study, we examined the relationship between amyloid status in CSF and acoustic features derived from the description of the Cookie Theft picture in MCI patients from a memory clinic. The cohort consisted of fifty-two patients with MCI (mean age 73 years, 65% female, and 57% positive amyloid status). Eighty-eight acoustic parameters were extracted from voice recordings using the extended Geneva Minimalistic Acoustic Parameter Set (eGeMAPS), and several ML models were used to classify the amyloid status. Furthermore, interpretability techniques were employed to examine the influence of input variables on the determination of amyloid-positive status. The best model, based on acoustic variables, achieved an accuracy of 75% with an area under the curve (AUC) of 0.79 in the prediction of amyloid status evaluated by bootstrapping and Leave-One-Out Cross Validation (LOOCV), outperforming conventional neuropsychological tests (AUC = 0.66). Our results showed that the automated analysis of voice recordings derived from spontaneous speech tests offers valuable insights into AD biomarkers during the preclinical stages. These findings introduce novel possibilities for the use of digital biomarkers to identify subjects at high risk of developing AD.
1. Introduction
Alzheimer's disease (AD) stands as the primary contributor to dementia cases worldwide, with no effective treatment available (Alzheimer's & Dementia, 2023). This progressive neurodegenerative disease impacts different cognitive domains, including memory, language, attention, and behavior, ultimately incapacitating the individual from performing daily tasks (Alzheimer's & Dementia, 2023). The disease's pathophysiology involves the formation of amyloid-β plaques (Aβ) and neurofibrillary tangles of phosphorylated tau protein (p-tau) in the brain. The accumulation of these two substrates eventually leads to neuroinflammation, reduced brain metabolism, and atrophy, which underlie the observed cognitive alterations (Peña-Casanova et al., 2012). However, compelling evidence suggests that the pathophysiological events related to AD begin several years, even decades, before the onset of clinical symptoms (Sperling et al., 2011). Therefore, much of the efforts in the field have been focused on identifying individuals in the early stage of mild cognitive impairment (MCI) (Alzheimer's & Dementia, 2023).
Once an individual with AD has progressed to the dementia stage and there is a loss of autonomy, i.e., cognitive impairment is already evident, the opportunities for potential disease-modifying interventions become limited. Consequently, several AD diagnostic criteria recommend the use of biomarkers tightly associated with AD pathological hallmarks (McKhann et al., 2011; Dubois et al., 2014) in the evaluation of patients with cognitive decline, including quantification of Aβ and p-tau in the cerebrospinal fluid (CSF) (Molinuevo et al., 2018) and positron emission tomography (PET) (Johnson et al., 2012). In individuals with MCI, the detection of positive AD biomarkers is relevant for future planning, identifying suitable patients for clinical trials, and establishing early interventions (Weimer and Sager, 2009). Nevertheless, currently available AD biomarkers are expensive, invasive, and not widely accessible, usually restricted to applied and research settings (Whelan et al., 2022; Thijssen et al., 2022).
As a result, the evaluation of cognitive functions through neuropsychological tests has been extensively utilized as an accessible alternative to disease biomarkers for identifying individuals at high risk of developing AD (Espinosa et al., 2013; Alegret et al., 2013). Most studies have focused on evaluating memory and executive functions (Small et al., 1999; Buckner, 2004) as those are the cognitive deficits most affected during the disease continuum (Albert et al., 2011). Nevertheless, language alterations have also been shown as a sensitive hallmark of early cognitive impairment in AD (Taler and Phillips, 2008). For example, (Eyigoz et al., 2020) identified several linguistic parameters obtained in naturalistic probes as good prognostic markers for MCI. In Wang et al. (2022), the authors observed that the percentage of silenced pauses in the speech differed significantly across the different AD stages. Similarly, Mazzeo et al. (2022) showed that a single-word comprehension impairment could be an indicator for identifying patients who may need assistance with self-care in the upcoming years. Moreover, employing neuroimaging techniques, numerous studies have revealed alterations in brain connectivity (Montembeault et al., 2019; Rafiq et al., 2022; Wang et al., 2022) and atrophy (Smits et al., 2014; Wei et al., 2018) directly associated with language functions.
These findings, coupled with the digitalization experienced over the last few years, have increased the popularity of spontaneous speech (SS) protocols administered using digital tools (Beltrami et al., 2018; de la Fuente Garcia et al., 2019; Thomas et al., 2020). Classical cognitive assessments, based on traditional settings (i.e., neuropsychological batteries) usually demand the physical presence of clinicians in specialized health centers and are not always optimal for decentralized remote clinical trials (Tröger et al., 2022). In contrast, digital cognitive assessments are better-suited protocols when automated procedures are recommended or needed (Lindsay et al., 2021).
Among the numerous parameters that can be obtained computationally when applying a SS protocol, acoustic parameters (e.g., those derived from the speech waveform) are some of the most interesting in cognitive research. Patients with AD dementia (ADD) exhibit longer and more frequent hesitations, lower speech, and articulation rates, and longer pauses in SS tasks than non-demented individuals (Mueller et al., 2018). To integrate all the information extracted from SS, several approaches based on machine learning (ML) techniques have been applied. Tóth et al. (2018) adjusted models using SS in a recall task and found significant differences in speech tempo, articulation rate, silent pause, and length of utterance between early-stage ADD patients and healthy control individuals. Fraser et al. (2016) identified several voice abnormalities in speech related to ADD. Vocal and temporal features also demonstrated good discriminant properties when differencing among MCI, mild ADD, and moderate ADD (accuracy > 80%) (König et al., 2015). In a study using data from over 8700 participants, acoustic parameters generated from a simple reading task were found to differ among cognitively healthy individuals, MCI patients, and participants with global cognitive impairment, especially those with the lowest and higher degree of impairment (Nagumo et al., 2020).
Until now, most studies involving SS have prioritized the development of diagnostic tools, with a primary focus on identifying individuals with ADD (Asgari et al., 2017; Xue et al., 2021; Mahajan and Baths, 2021; He et al., 2023). Only a limited number of investigations have examined the application of SS in subjects with MCI, and even fewer studies have explored its association with biomarkers of interest, such as amyloid accumulation in the brain or CSF (Verfaillie et al., 2019; Mueller et al., 2021; Hajjar et al., 2023). In this context, Verfaillie et al. (2019) identified an association between high amyloid burden and fewer specific words during SS in 63 individuals with subjective cognitive decline (SCD) from a memory clinic. Mueller et al. (2021) showed that a positive amyloid status was longitudinally associated with poor achievement in several SS parameters (i.e., unique/total word production) using the Cookie Theft picture in a cohort of cognitively unimpaired individuals. Recently, Hajjar et al. (2023) explored the association between variables extracted from SS and amyloid status assessed by CSF in a population of cognitively healthy individuals and MCI using ML techniques. For the first time, the authors demonstrated that the SS can predict the amyloid status outperforming neuropsychological tests typically used to evaluate language obtaining an AUC of 0.77.
The present study aims to provide further evidence to address the existing gap between SS and the amyloid status quantified by CSF in an applied setting, using a sample of patients with MCI evaluated in a memory clinic. In particular, the Cookie Theft picture from the Boston Diagnostic Aphasia Examination was used as a speech task, ensuring easier standardization and maintaining great simplicity by analyzing only acoustic parameters (i.e., excluding lexico-syntatic parameters that are slower to analyze, more expensive, and frequently conditioned by more prior validation processes).
2. Materials and methods
The study had a cross-sectional design and included 52 patients with MCI who underwent clinical and neuropsychological evaluations, a lumbar puncture (LP) for the assessment of AD-core biomarkers in CSF, and lastly, a SS test using the acceXible platform.
2.1. Study participants
This study included 52 patients with a diagnosis of MCI (Petersen, 2004) who were evaluated at the memory clinic from Ace Alzheimer Center Barcelona (single site) between April 2022 and January 2023. Participants were either referred to the memory clinic by their general health practitioner due to cognitive problems (or subjective complaints) or they attended the open house initiative without the need for a physician's referral (Boada et al., 2014). All clinical and biomarker measures were obtained within a 6-month window from the SS protocol administration. This project is part of a study focused on the identification of risk factors of dementia through speech analysis (Tartaglia: MIA.2021.M02.0005).
2.2. Clinical assessment
Study participants completed neurological, neuropsychological, and social evaluations at the Ace Alzheimer Center Barcelona Memory Clinic and were followed up annually. A consensus diagnosis was assigned to each patient by a multidisciplinary team of professionals (Boada et al., 2014). Demographic information collected included age, sex, and years of formal education. The cognitive assessment included the Spanish version of the Mini-Mental State Examination (MMSE) (Folstein, 1992), the memory part of the Spanish version of the Seven Minute test (Del Ser et al., 2006), the Spanish version of the Neuropsychiatric Inventory Questionnaire (NPI-Q) (Boada et al., 2005), the Hachinski's ischemic score scale (Hachinski et al., 1974), the Blessed Dementia Scale (Blessed et al., 1968), and the Clinical Dementia Rating (CDR) scale (Morris, 1993), as well as the comprehensive Neuropsychological Battery of Fundació ACE (NBACE) (Alegret et al., 2012). MMSE (Folstein, 1992), and NBACE (Alegret et al., 2012) were assessed on all visits. At the baseline, all participants had a CDR of 0.5.
2.3. Neuropsychological assessment
Cognitive data were collected at the baseline using the NBACE. NBACE is a 45-min battery designed to assess cognitive domains especially affected in the elderly when cognitive impairment is suspected (Alegret et al., 2012). The NBACE was proposed as a brief, easy-to-administer and goal-directed compilation of globally-used neuropsychological tests in our target population. In this study, the following cognitive domains were explored: attention, information processing speed, verbal learning and memory, language, visuoperception, visuospatial ability, praxis, and executive functions. Normative data and cut-off scores of the NBACE subtests for individuals over 44 years old can be found elsewhere (Alegret et al., 2012, 2013).
2.4. Lumbar puncture and quantification of CSF core biomarkers for AD
Lumbar punctures (LPs) were performed at Ace Alzheimer Center Barcelona by an experienced neurologist under fasting conditions. The collection protocol follows the recommendations of the Alzheimers Biomarkers Standardization (Vanderstichele et al., 2012). The CSF was collected passively in 10 mL polypropylene tubes (Sarstedt Ref 62.610.018) and centrifuged (2000× g 10 min at 4 °C) within 2 h of acquisition. After centrifugation, the fluid was aliquoted into polypropylene tubes (Sarstedt Ref 72.694.007) and stored at -80 °C until analysis. The day of the analysis, one aliquot of 0.5 mL was thawed and used for the determination of Aβ1-42. Aβ1-42 protein was quantified by the commercially available chemiluminescense enzyme immunoassay (CLEIA) using the Lumipulse G 600 II automatic platform (Fujirebio Europe, Göteborg, Sweden) (Leit ao et al., 2019). Cutoffs from the Ace Alzheimer Center Barcelona CSF program were used to dichotomize Aβ1-42. A patient was considered amyloid positive when Aβ1-42 levels were <796 pg/mL (Orellana et al., 2022).
2.5. Recording protocol and preparation of voice data
Each participant performed the speaking task with the supervision of a neuropsychologist and using the acceXible platform app on a tablet. This app identifies vocal biomarkers for disease detection and monitoring. The image of the Cookie Theft picture was presented on the screen, and participants were asked to describe the image in detail. The voice was automatically recorded as part of an ongoing research protocol. The evaluations were conducted in Spanish and in a quiet environment. Participants audios were standardized to a frequency of 16KHz. Subsequently, the initial and final silences were automatically removed, and the deep learning model presented in Defossez et al. (2020) was applied to remove environmental noise. Acoustic features from the extended Geneva Minimalistic Acoustic Parameter Set (eGeMAPS) (v02) were extracted from every record using the open-source toolkit OpenSmile (v2.4.2) (Eyben et al., 2015). The set of features from the eGeMAPS are oriented to provide a simplified and standardized selection of relevant acoustic parameters for detecting physiological changes in voice production guided by findings of previous related studies (Scherer, 1986; Banse and Scherer, 1996). Appendix 1 includes the list of these 88 features.
2.6. Ethical considerations
This study and its informed consent were approved by the ethics committees of the Hospital Universitari de Bellvitge (Barcelona) (ref. PR007/22) under Spanish biomedical laws (Law 14/2007, 3 July, regarding biomedical research; Royal Decree 1716/2011, 18 November) and followed the recommendations of the Declaration of Helsinki. All participants signed an informed consent for the spontaneous speech protocol and for the lumbar puncture procedure.
The informed consent for the LP provides patients with information about the procedure, the most frequent side effects, and the primary objective of obtaining the AD-core biomarkers in CSF (which extends beyond clinical purposes and includes research interests). Twenty four h later after the LP, a member of the ACEs nursing team contacted the patients via phone to monitor any potential side effects and offer medical advice if needed. To ensure transparency, patients are also informed about the utilization of audio files collected during the speech test, including the primary research objectives and the security measures implemented for processing and storage on our servers or by our collaborators.
2.7. Data modeling
Statistical analyses were performed on STATA 15 (Stata Corporation, College Station, TX, USA) and ML modeling using Python (version 3.9.16).
Demographic, clinical, neuropsychological, and acoustic variables were contrasted between participants with positive and negative amyloid status using t-test or χ2 analyses. Logistic regression analyses were performed to evaluate the association of neuropsychological tests and acoustic variables with positive amyloid status. As all these bivariate and multivariate analyses were performed only for a descriptive purpose, no corrections for multiple testing were applied.
ML techniques were used for the prediction of amyloid-positive status using acoustic, neuropsychological, and demographic variables. The demographic variables considered were sex, age, and years of formal education. On the other hand, the neuropsychological variables included were total scores on similarities, digit forward, and digit backwards from the Wechsler Adult Intelligence Scale, third edition (WAIS-III) (Wechsler, 2002); long-term and recognition memory on the word list subtest from the Wechsler Memory Scale, third version (WMS-III) (Wechsler, 1997); the 15-Objects Test (Pillon et al., 1989); Poppelreuter-type overlap figures (Sala et al., 1995); the Automatic Inhibition Subtest of the Syndrom Kurtz Test (SKT) (time in s) (Erzigkeit, 1989); phonetic and semantic verbal fluencies (Artiola et al., 1999; Goodglass and Kaplan, 1972); an abbreviated 15-item naming test from the Boston Naming Test (BNT) (Kaplan et al., 2001); Verbal Comprehension (Alegret et al., 2012); and the Luria's Clock test (Golden, 1980) (variables were listed in Table 1). As input data for the models, three different sets of features were considered. The first dataset was based on the neuropsychological and demographic variables, the second included the eGeMAPS acoustic parameters (88 variables), and the third combined demographic and acoustic variables (92 variables). The aim of the first feature set, based on neuropsychological and demographic variables, was to establish a baseline model for comparing the capacity of the acoustic parameters for predicting the amyloid status.
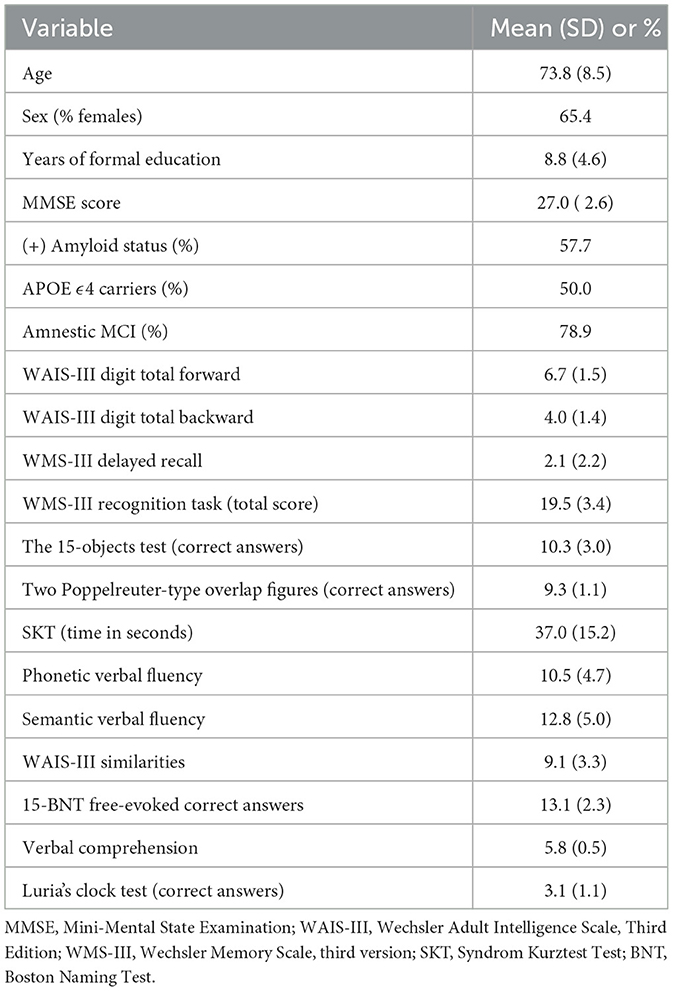
Table 1. Demographic and clinical characteristics of the study participants.
For the datasets including acoustic variables, the following models were considered: (1) models with no previous feature engineering: Elastic Net (EN) and Random Forest (RF), (2) models combined with a prior dimensionality reduction using principal component analysis (PCA): EN, logistic regression (LR), support vector machines (SVM), and K-nearest neighbors (KNN), and (3) wrapper-based feature selection combining variable-length particle swarm optimization (VLPSO) (Tran et al., 2018) and KNN. Given the small number of input features in the dataset based on neuropsychological and demographic variables, the VLPSO feature selection strategy was not applied.
Briefly, the VLPSO is a wrapped-based feature selection algorithm (Xue et al., 2015). This population-based metaheuristic is used to remove irrelevant and redundant features in order to maximize the performance on a given task. In this study, the VLPSO algorithm was used to select variables maximizing the classification performance. A more detailed explanation of the VLPSO implementation used in this research can be found in Appendix 3. Moreover, Appendix 4 contains the hyperparameters of the algorithms used in this study.
To obtain a more reliable estimate of the goodness of fit of the models, they were evaluated by applying bootstrapping (5,000 iterations) to the training set with the leave-one-out cross validation (LOOCV) as shown in Figure 1. The Scikit-Learn (Buitinck et al., 2013) implementation was used for all the models described, except the VLPSO algorithm. The VLPSO code is available on GitHub.
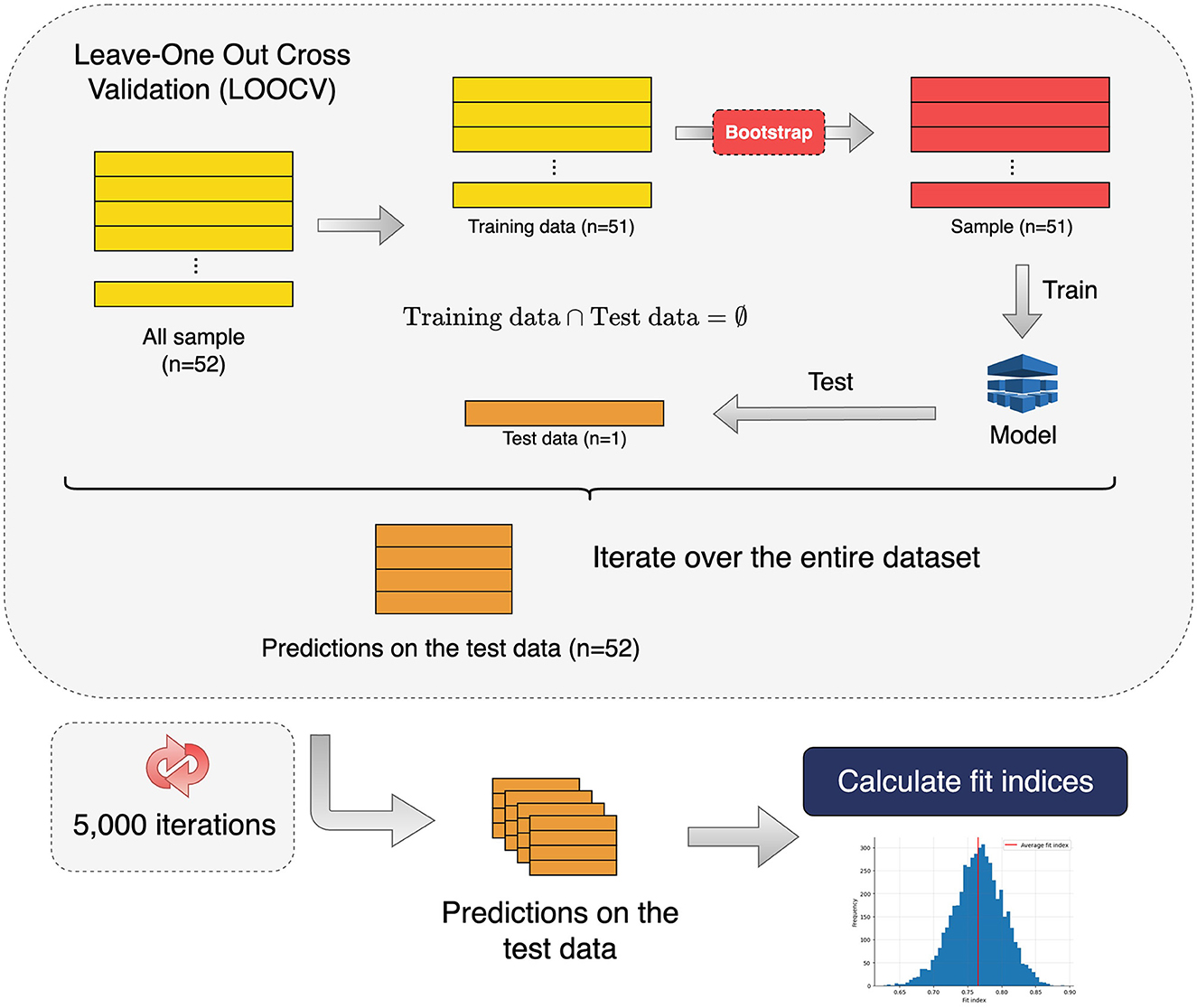
Figure 1. Pipeline used to evaluate the goodness-of-fit of all the models used to predict amyloid status. Performance metrics and confidence intervals were calculated from the metric distribution obtained after 5,000 iterations of a nested leave-one-out cross validation (LOOCV) where the training set used for adjusting the models was generated by bootstrapping.
3. Results
3.1. Statistical analysis
Demographic and clinical data of the 52 participants are described in Table 1. The cohort had a mean age of 73 years, 65% were female, and they completed a mean of 8.8 years of formal education. Thirty cases (57.7%) showed a positive amyloid status. Within those with a negative amyloid status, fifteen cases (68.2%) had a normal CSF profile and seven (31.8%) showed elevated t-tau and/or p-tau levels (suspected non-Alzheimer changes). Fifty percent of the sample were APOE ϵ4 carriers. Among subjects with a positive amyloid status, 56.6% carried an APOE ϵ4 allele, while for those with a negative status, the percentage decreased to 18.1%. The audio recording of the picture presentation had an average duration of 46 s (SD=15.6).
The bivariate contrasts for demographic and neuropsychological variables between participants with positive and negative amyloid status are shown in Table 2. Those participants with a positive amyloid status were significantly older, had fewer years of formal education, and when contrasting neuropsychological tests, they showed lower scores in the WMS-III, the 15-Objects Test, semantic verbal fluency, WAIS-III, BNT, and higher execution time of the SKT (all significant comparisons p < 0.043). To assess whether neuropsychological tests showed significant differences according to amyloid status controlling for the demographic characteristics of the sample, multivariate logistic models were applied adjusting the effect of neuropsychological tests by age, sex, and years of formal education. Amyloid status (positive/negative) was considered as the dependent variable. None of the neuropsychological variables maintained a significant effect in discriminating the amyloid status (Supplementary Table A2).
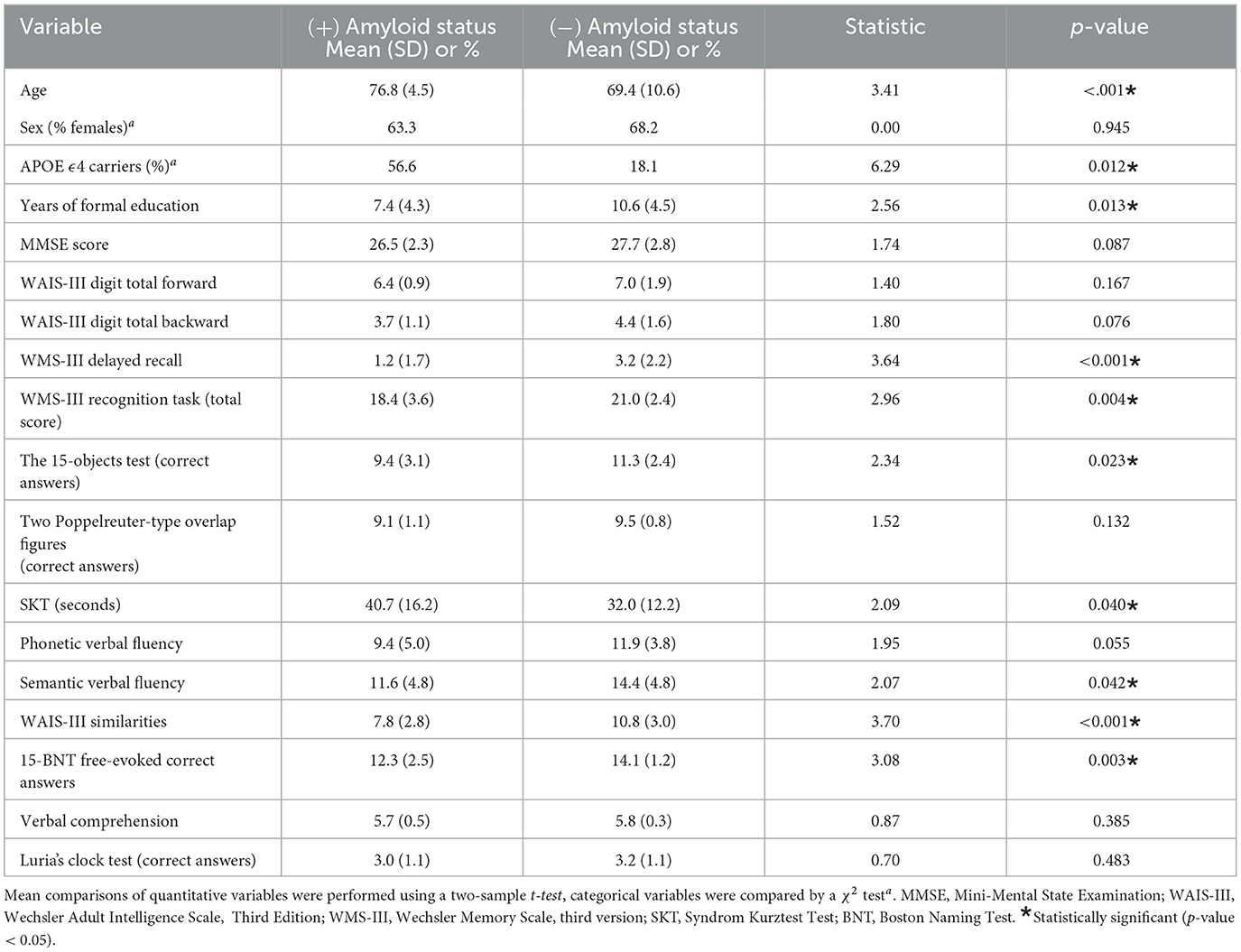
Table 2. Mean comparison of clinical and sociodemographic variables stratified by amyloid status.
The same bivariate contrasts for acoustic features between participants with positive and negative amyloid status are depicted in Supplementary Table A1. Five of the 88 acoustic features analyzed showed a significant difference between the two groups. These variables included the F3-bandwidth (voiced - coefficient of variation), the Hammarberg index (unvoiced - mean), the Alpharatio (unvoiced - mean), and the Voiced-Segment-Length/second (mean and std) (Eyben et al., 2015). When adjusting these variables for age, sex, and years of education, only F3-bandwidth (voiced - coefficient of variation) became non-significant (p > 0.05) (Supplementary Table A3).
3.2. Machine learning analysis
The fit indices of the two best models obtained for differentiating the amyloid status across the three different datasets (neuropsychological and demographic / acoustic / acoustic and demographic) by applying the evaluation strategy depicted in Figure 1 are reported in Table 3. The area under the curve (AUC) was used as the reference metric. The best AUC value was observed for the model that included only acoustic variables, followed by the model based on acoustic and demographic parameters. The models with the best performance were those incorporating the wrapper-based feature selection strategy (VLPSO+KNN) reaching AUCs of 0.79 (95CI: [0.71-0.86]) (acoustic) and 0.74 (95CI: [0.66-0.82]) (acoustic and demographic). These two models evaluated by simply performing a LOOCV without bootstrapping achieved AUCs of 0.83 and 0.79, respectively. In contrast, models based on demographic and neuropsychological variables performed poorly, with AUCs below 0.7 and accuracies close to 60%.
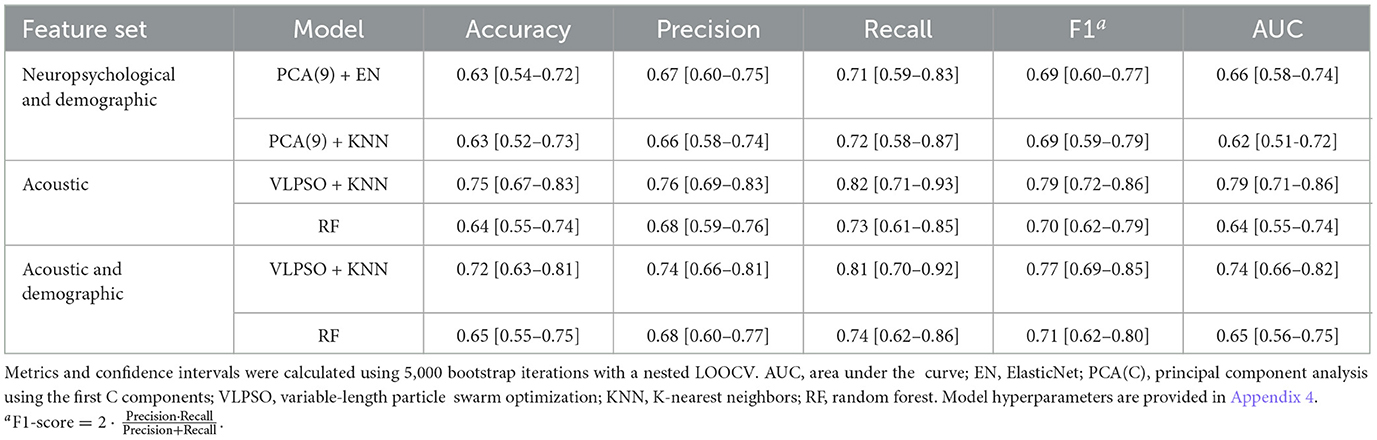
Table 3. Fit indices of the two best models obtained for each of the explored feature sets.
The dimensionality reduction achieved by the VLPSO-based models went from 88 features to 7 and 10 for the datasets based on acoustic features and combining acoustic and demographic information, respectively. Figure 2 shows the receiver operating characteristic (ROC) curves of the best models obtained for each dataset (see Table 3). The two-dimensional projection of the features associated with the best model from Table 3 (VLPSO+KNN using acoustic variables) and their decision boundary is illustrated in Figure 3.

Figure 2. Receiver operating characteristic (ROC) curve for predicting amyloid status based on demographic and neuropsychological, acoustic, and a combination of demographic and acoustic variables. The results correspond to the best models presented in Table 3. For each model, the mean AUC calculated by 5,000 bootstrap iterations as described in Figure 1 is shown. AUC: area under the curve.
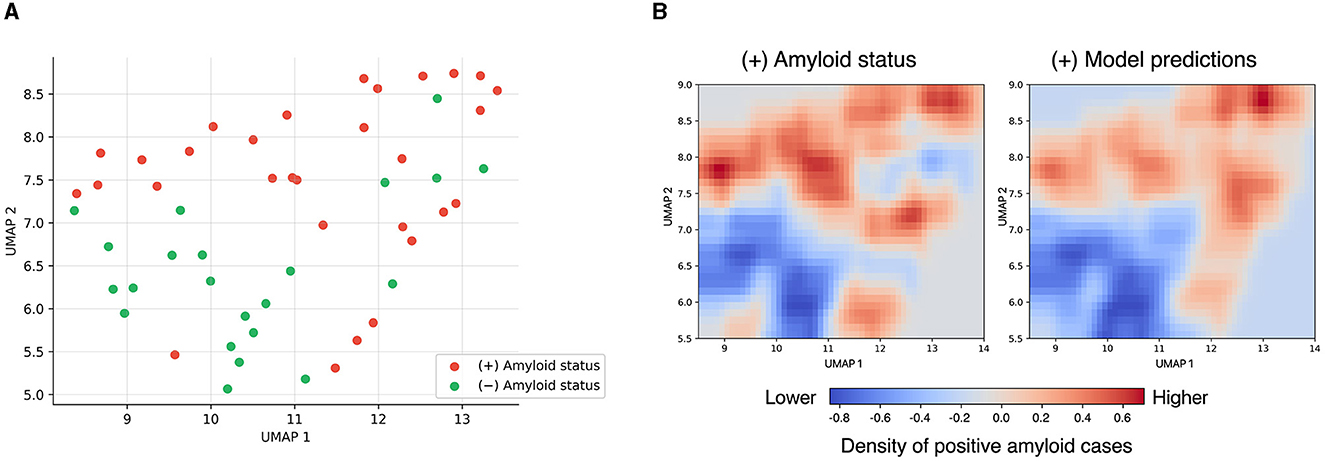
Figure 3. Uniform manifold approximation and projection (UMAP) (Sainburg et al., 2020) dimensionality reduction of the most discriminative feature set obtained by the VLPSO feature selection algorithm. (A) Projection highlighting positive and negative amyloid status. (B) Projection of the K-nearest neighbor decision boundary. On the left is the density plot representing the higher presence (red) or absence (blue) of amyloid-positive cases in the data. On the right are shown the KNN predictions of amyloid-positivity, where red indicates that the model assigns a higher probability of amyloid-positivity and blue a lower probability. UMAP hyperparameters: number of neighbors = 8 and minimum distance = 0.1; the rest of the hyperparameters were left as default.
The most discriminant features for differentiating the amyloid status were further analyzed using SHapley Additive exPlanations (SHAP) (Lundberg and Lee, 2017). Figure 4 shows the impact of each variable on the amyloid status probability. Variables were ordered based on the average absolute SHAP value in a descending order. Positive SHAP values are associated with a higher probability of a positive amyloid status, while negative values with a lower probability. The most relevant features for predicting a positive status were the frequency based: F3-bandwidth (voiced–coefficient of variation) and F2 bandwidth (voiced–mean); the spectral-based: Hammarberg index (unvoiced–mean), harmonic difference H1-A3 (voiced–mean), and spectral flux (voiced–coefficient of variation); and the temporal-based: voiced-segment-length/second (mean and std).
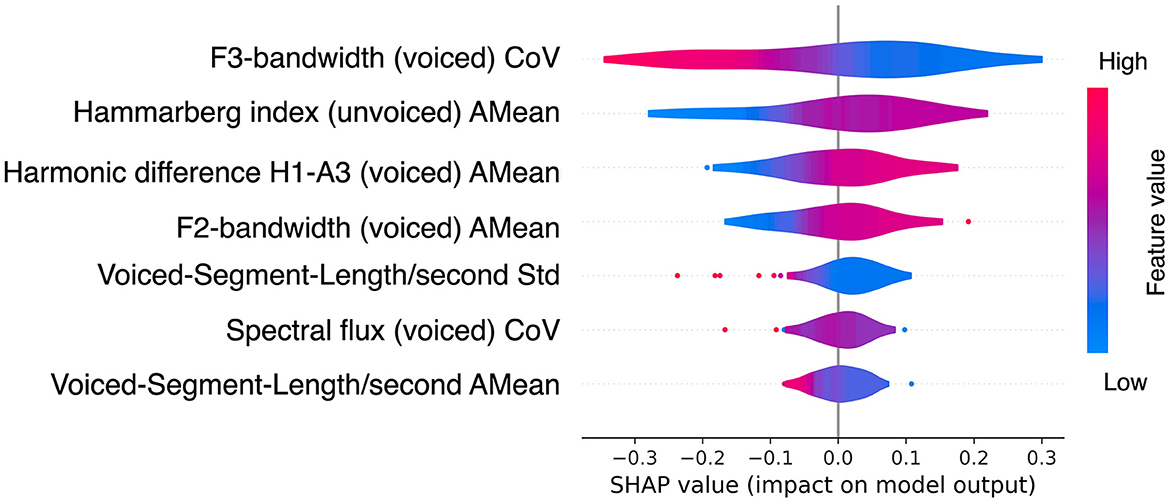
Figure 4. SHapley Additive exPlanations (SHAP) values Lundberg and Lee (2017) of the best model for predicting amyloid status. The SHAP values were calculated on the test set using LOOCV. The best model corresponds to the combination of VLPSO with KNN using acoustic variables (see Table 3). The feature color indicates how it relates to the probability of being amyloid positive or negative. The red color is associated with higher feature values, while blue is associated with lower values. Thus, lower values in the F3-bandwidth (voiced) CoV (blue area) are associated with an increased likelihood of being amyloid positive; and having a lower mean of the spectral Hammarberg index (voiced) (red area) is associated with a lower probability of being amyloid positive. CoV: coefficient of variation; AMean: arithmetic mean; Std: standard deviation.
4. Discussion
This study investigated the association between the amyloid status assessed by CSF and voice features derived from the use of the Cookie Theft picture description in a cohort of 52 MCI patients evaluated in a memory clinic. We found noticeable differences in physicoacoustic characteristics between patients with positive and negative amyloid status using a widely extended SS test. The analysis unveiled statistical variations in multiple acoustic parameters, and the applied ML models showed a good discriminatory capacity for predicting amyloid positivity (Table 3). Furthermore, by incorporating XAI techniques, we gained valuable insights into how different input variables influenced the decisions made by the models (Figure 4).
As shown in the UMAP projection (Figure 3), the features identified by our ML-based feature selection algorithm provided a clear distinction of amyloid status, leading to a good classification performance using a simple distance-based algorithm such as KNN. Interestingly, including sociodemographic variables did not improve the discriminatory capacity of the models, supporting that SS-derived information alone can act as a good predictor of amyloid status (AUC of 0.74 [0.66–0.82] vs. AUC 0.79 [0.71–0.86]). Moreover, we showed that SS features outperformed the conventional neuropsychological tests typically used to evaluate cognitive functions (Figure 2). These results provide evidence that the differences between positive and negative amyloid status in MCI subjects can be captured by aspects related to voice production.
Our results align with recent studies conducted by Hajjar et al. (2023) in a longitudinal cohort of cognitive unimpaired and MCI subjects, Mueller et al. (2018) in a longitudinal study involving healthy and early-stage MCI patients, and Verfaillie et al. (2019) in a cross-sectional study of individuals with cognitive decline. These studies demonstrated that amyloid burden is associated with several speech parameters. We also extended the relationship between the presence of brain amyloidosis, one of the main neuropathological hallmarks of AD, and speech parameters in MCI patients, providing a new landmark for the use of spontaneous speech in neurodegenerative disorders. Notably, the studies of Mueller et al. (2018) and Verfaillie et al. (2019) were based on the lexico-syntactic content of the speech, while our study focuses on the properties of the sound generated when describing a picture. The main idea here is that the analysis of speech and language could provide relevant information about the underlying pathophysiological process of AD (Voleti et al., 2019).
During the preclinical stage of AD, before symptom onset, the pathophysiological course of the disease is characterized by first the formation of amyloid plaques and later p-tau protein aggregates, which accumulate in the brain and disrupt normal neuronal function (Sperling et al., 2011). Subsequently, at the MCI stage, the accumulation of these proteins in the brain reaches a critical threshold, leading to neuronal injury and pathological changes in the volumes of different brain regions (Sperling et al., 2011). The most prominent cognitive deficits in MCI are typically in the domains of memory and executive function, which include abilities such as planning, decision-making, and problem-solving. However, it is reasonable to assume that more diverse and silent changes are taking place (Wilson and Petkov, 2011). In Mazzeo et al. (2022), researchers observed associations between disease progression, language lesions, and brain hypometabolism. In addition, evidence shows that MCI patients show longer speech and phonation time (Tóth et al., 2018; Gosztolya et al., 2019), an incremented length of silent pauses (voiceless) (Wang et al., 2022), lower speech rate (Tóth et al., 2018), presence of stammers and articulatory disfluencies that interrupt speech with longer hesitations (López-de Ipiña et al., 2013; Tóth et al., 2018), and impairments in formant features in phonological planning formants (Themistocleous et al., 2018). For a more detailed description of these alterations, (see Martínez-Nicolás et al., 2021). In our study, several voice parameters were identified as the most discriminatory using ML approaches for differentiating MCI with positive and negative amyloid status. Among the most important voice parameters identified (Figure 4), there were spectral features (relative energy in different frequency bands), associated with vocal emotional expre ssions Sauter et al. (2010), voiced segments (the portion of speech with relatively constant phonetic features) useful to differentiate AD from healthy individuals (López-de Ipiña et al., 2013; Wang et al., 2022), and measures of the Hammarberg index, a spectral measure of voice quality, which has been identified as a discriminant feature for MCI (Themistocleous et al., 2020).
The present study was unable to detect an association between amyloid status and conventional language tests included in the NBACE, such as BNT-15 or semantic verbal fluency. This result is concordant with those observed in MCI (Hajjar et al., 2023), cognitively healthy individuals (Baker et al., 2017) and those with subjective cognitive decline (Verfaillie et al., 2019). In fact, in our study, no neuropsychological test from NBACE showed a multivariate association with the amyloid status in MCI, and predictive models based on neuropsychological tests exhibited a lower discriminative capacity. These findings suggest that SS assessments may offer a more ecological and closely connected real-world representation of cognitive status for predicting Aβ42 status than traditional language evaluations, being of particular interest in the preclinical stages of AD. It is worth noting that our study exclusively focused on parameters that capture the structure and dynamics of the speech, without relying on syntactic and lexical information derived from voice recordings. This aspect is particularly significant as it enables the automated evaluation of information obtained from SS assessments, eliminating the requirement for manual language analysis.
As exposed before, the assessment of SS can be approached in different ways from narrower and more specific questions (i.e., “describe the presented image") to more open-ended elicitations (i.e., “describe the happiest moment of your life”). However, these open-ended approaches are subjected to more individual and contextual factors, resulting in more variability and limiting their generalizability when contrasting results between studies (Mueller et al., 2018). More efforts should be devoted to providing standards and protocols to improve the accuracy of procedures and algorithms and to stimulate the integration of innovative solutions in SS processing to clinical practice or trials (Haider et al., 2019; Tröger et al., 2022). In this sense, it should be noted that one of the strengths of the present study was to provide precise discriminant results by distinguishing the amyloid status (positive vs negative) in a relevant clinical population (patients with MCI) in an applied setting (a memory unit), using a simple speech strategy (description of a picture), through a very well-known and accessible tool (the Cookie Theft picture), administered during less than 1 min, and focusing attention only on acoustic features, obtained using a set of standardized variables (eGeMAPS) (Eyben et al., 2015).
We acknowledge that our study has certain limitations. First, the small sample size restricts the generalization of these results and should be treated with caution. Although the models were evaluated following an exhaustive bootstrap and cross-validation approach to obtain a more realistic approximation of their performance, larger sample sizes are required to confirm our results. Additionally, our findings were based on cross-sectional data, while the relationship between CSF biomarkers and SS is probably complex and multifactorial. Further research is required to understand the longitudinal association between amyloid burden and voice (and other speech) features, investigating the evolution of language parameters using follow-up information. Moreover, our study solely focused on predicting amyloid status in CSF, the primary pathological hallmark of AD and a key target for drug development (Alzheimer's & Dementia, 2023). However, extending the presented analytical framework to include other CSF (e.g., p-tau 181 or total tau) or neuroimaging biomarkers (e.g., hypometabolism, tau accumulation, or atrophy) is of great interest for future investigations (Scheltens et al., 2021). For example, it has been demonstrated that tau levels exhibit a stronger correlation with cognitive alterations compared to amyloid levels (Aschenbrenner et al., 2018). In addition, prior studies have shown that reductions in brain metabolism (Vanhoutte et al., 2017) or changes in activation patterns measured by fMRI (Vanhoutte et al., 2017) occur in the early stages of the disease and are associated with language production. Therefore, while the primary aim of this study was to provide an initial approximation of the predictive capacity of amyloid status from SS in MCI patients, the development of future predictive models should consider a broader panel of disease biomarkers. Finally, using the Cookie Theft picture description facilitated standardized results. Nevertheless, relying on a unique test imposes limitations when characterizing language impairment. Consequently, incorporating additional SS tests within the models should improve their predictive performance.
Despite these limitations and in the context of accumulated data, such as that provided in the present study, it is possible to foresee promising horizons for the application of voice processing technology. Based on SS and IA techniques, the identification of individuals at high risk of developing AD dementia could be accessible to clinicians by the longitudinal analysis of conversations. For example, specific speech tasks could be periodically administered remotely when other cognitive assessments are not feasible or when biomarker-based evaluations are either too expensive, non-accessible, or unsuitable for a particular patient. These advancements have the potential to make the identification of high-risk individuals more accessible to clinicians and significantly contribute to public health.
5. Conclusion
In conclusion, acoustic features derived from the Cookie Theft picture description are consistently associated with amyloid status assessed by CSF in MCI patients in the setting of a memory clinic. These results offer a new window of opportunities, focused on identifying, in a widely accessible, rapid, and non-invasive manner, the underlying biochemical status in patients with MCI providing information about their future cognitive progression and risk of conversion to dementia. Such advancements in early detection and monitoring of MCI can significantly impact clinical practice, enabling timely interventions and personalized treatment strategies. Further research is needed to validate and refine the SS protocols and explore their utility in larger and more diverse populations. Ultimately, this technology has the potential to bring us closer to improved diagnostic and prognostic tools for individuals with MCI.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The study involving humans was approved by Hospital Universitari de Bellvitge (PR007/22). The study was conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SV, FG-G, MM, LT, AR, and MB: conceptualization. SV and FG-G: methodology and formal analysis. SV, FG-G, AC, IR, PG-G, CO, RP, AO, LM, and AG-S: data curation. SV, FG-G, MM, NM, MA, CZ, PG, WH, and AR: writing—review and editing. MM, NM, MA, VP, MR, CZ, PG, and NL: project administration. SV: supervision. All authors contributed to interpretation of the findings, the critical review of the manuscript, and have read and agreed to the published version of the manuscript.
Funding
This project has received funding from R&D Missions in the Artificial Intelligence program, which is part of the Spain Digital 2025 Agenda and the National Artificial Intelligence Strategy and financed by the European Union through Next Generation EU funds (project TARTAGLIA, exp. MIA.2021.M02.0005). This project has also received funding from the Instituto de Salud Carlos III (ISCIII) Acción Estratégica en Salud, integrated in the Spanish National RCDCI Plan and financed by ISCIII Subdirección General de Evaluación and the Fondo Europeo de Desarrollo Regional (FEDER–Una manera de hacer Europa) grant PI19/00335 awarded to MM, grant PI17/01474 awarded to MB, grants AC17/00100, PI19/01301, and PI22/01403 awarded to AR and by the European Union Joint Programme–Neurodegenerative Disease Research (JPND) Multinational research projects on Personalized Medicine for Neurodegenerative Diseases/Instituto de Salud Carlos III grant AC19/00097 awarded to AR and grant FI20/00215 from the Instituto de Salud Carlos III (ISCIII) awarded to IR. For CSF biomarker research, AR and MB received support from the European Union/EFPIA Innovative Medicines Initiative Joint undertaking ADAPTED and MOPEAD projects (grant numbers 115975 and 115985, respectively). AC received support from the Instituto de Salud Carlos III (ISCIII) under the grant Sara Borrell (CD22/00125) and the Spanish Ministry of Science and Innovation, Proyectos de Generación de Conocimiento grant PID2021-122473OA-I00.
Acknowledgments
The authors are grateful to all patients who consented to participate for their significant contribution to making this project possible.
Conflict of interest
MB has consulted for Araclon, Avid, Grifols, Lilly, Nutricia, Roche, Eisai, and Servier, received fees from lectures and funds for research from Araclon, Biogen, Grifols, Nutricia, Roche, and Servier. She reports grants/research funding from Abbvie, Araclon, Biogen Research Limited, Bioiberica, Grifols, Lilly, S.A., Merck Sharp & Dohme, Kyowa Hakko Kirin, Laboratorios Servier, Nutricia S.R.L., OryzonGenomics, Piramal Imaging Limited, Roche Pharma S.A., and Schwabe Farma Iberica S.L.U., all outside the submitted work, and has not received personal compensation from these organizations. AR is a member of the scientific advisory board of Landsteiner Genmed and Grifols S.A. and has stocks of Landsteiner Genmed. MM has consulted for F. Hoffmann-La Roche Ltd., and has participated in the Spanish Scientific Advisory Board of Biomarkers of Araclon.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fnins.2023.1221401/full#supplementary-material
References
Albert, M. S., DeKosky, S. T., Dickson, D., Dubois, B., Feldman, H. H., Fox, N. C., et al. (2011). The diagnosis of mild cognitive impairment due to alzheimer's disease: recommendations from the national institute on aging-alzheimer's association workgroups on diagnostic guidelines for alzheimer's disease. Alzheimer's Dement. 7, 270–279. doi: 10.1016/j.jalz.2011.03.008
Alegret, M., Espinosa, A., Valero, S., Vinyes-Junque, G., Ruiz, A., Hernandez, I., et al. (2013). Cut-off scores of a brief neuropsychological battery (nbace) for spanish individual adults older than 44 years old. PLoS ONE 8, e76436. doi: 10.1371/journal.pone.0076436
Alegret, M., Espinosa, A., Vinyes-Junqué, G., Valero, S., Hernández, I., Tárraga, L., et al. (2012). Normative data of a brief neuropsychological battery for spanish individuals older than 49. J. Clin. Exp. Neuropsychol. 34, 209–219. doi: 10.1080/13803395.2011.630652
Alzheimer's & Dementia (2023). 2023 Alzheimer's disease facts and figures. Alzheimer's Dement. 19, 1598–1695. doi: 10.1002/alz.13016
Artiola, L., Hermosillo, D., Heaton, R., and Pardee, R. (1999). Manual de normas y procedimientos para la baterìa neuropsicológica en español. Tucson: mPress.
Aschenbrenner, A. J., Gordon, B. A., Benzinger, T. L., Morris, J. C., and Hassenstab, J. J. (2018). Influence of tau pet, amyloid pet, and hippocampal volume on cognition in Alzheimer disease. Neurology 91, e859-e866. doi: 10.1212/WNL.0000000000006075
Asgari, M., Kaye, J., and Dodge, H. (2017). Predicting mild cognitive impairment from spontaneous spoken utterances. Alzheimer's & Dement. 3, 219–228. doi: 10.1016/j.trci.2017.01.006
Baker, J. E., Lim, Y. Y., Pietrzak, R. H., Hassenstab, J., Snyder, P. J., Masters, C. L., et al. (2017). Cognitive impairment and decline in cognitively normal older adults with high amyloid-β: a meta-analysis. Alzheimer's Dement. 6, 108–121. doi: 10.1016/j.dadm.2016.09.002
Banse, R., and Scherer, K. R. (1996). Acoustic profiles in vocal emotion expression. J. Pers. Soc. Psychol. 70, 614. doi: 10.1037/0022-3514.70.3.614
Beltrami, D., Gagliardi, G., Rossini Favretti, R., Ghidoni, E., Tamburini, F., and Calzà, L. (2018). Speech analysis by natural language processing techniques: a possible tool for very early detection of cognitive decline? Front. Aging Neurosci. 10, 369. doi: 10.3389/fnagi.2018.00369
Blessed, G., Tomlinson, B. E., and Roth, M. (1968). The association between quantitative measures of dementia and of senile change in the cerebral grey matter of elderly subjects. Br. J. Psychiat. 114, 797–811. doi: 10.1192/bjp.114.512.797
Boada, M., Tárraga, L., Hernández, I., Valero, S., Alegret, M., Ruiz, A., et al. (2014). Design of a comprehensive alzheimers disease clinic and research center in spain to meet critical patient and family needs. Alzheimer's Dement. 10, 409–415. doi: 10.1016/j.jalz.2013.03.006
Boada, M., Tárraga, L., Modinos, G., López, O., and Cummings, J. (2005). Neuropsychiatric inventory-nursing home version (npi-nh): Spanish validation. Neurologia (Barcelona, Spain) 20, 665–673.
Buckner, R. L. (2004). Memory and executive function in aging and ad: multiple factors that cause decline and reserve factors that compensate. Neuron 44, 195–208. doi: 10.1016/j.neuron.2004.09.006
Buitinck, L., Louppe, G., Blondel, M., Pedregosa, F., Mueller, A., Grisel, O., et al. (2013). Api design for machine learning software: experiences from the scikit-learn project. arXiv.
de la Fuente Garcia, S., Ritchie, C. W., and Luz, S. (2019). Protocol for a conversation-based analysis study: Prevent-ed investigates dialogue features that may help predict dementia onset in later life. BMJ Open 9, e026254. doi: 10.1136/bmjopen-2018-026254
Defossez, A., Synnaeve, G., and Adi, Y. (2020). Real time speech enhancement in the waveform domain. arXiv. doi: 10.21437/Interspeech.2020-2409
Del Ser, T., Sánchez-Sánchez, F., de Yébenes, M. J. G., Otero, A., and Munoz, D. G. (2006). Validation of the seven-minute screen neurocognitive battery for the diagnosis of dementia in a spanish population-based sample. Dement. Geriatr. Cogn. Disord. 22, 454–464. doi: 10.1159/000095858
Dubois, B., Feldman, H. H., Jacova, C., Hampel, H., Molinuevo, J. L., Blennow, K., et al. (2014). Advancing research diagnostic criteria for Alzheimer's disease: the iwg-2 criteria. Lancet Neurol. 13:614–629. doi: 10.1016/S1474-4422(14)70090-0
Erzigkeit, H. (1989). “The skt–a short cognitive performance test as an instrument for the assessment of clinical efficacy of cognition enhancers,” in Diagnosis and Treatment of Senile Dementia, Cham: Springer, 164–174. doi: 10.1007/978-3-642-46658-8_14
Espinosa, A., Alegret, M., Valero, S., Vinyes-Junqué, G., Hernández, I., Mauleón, A., et al. (2013). A longitudinal follow-up of 550 mild cognitive impairment patients: evidence for large conversion to dementia rates and detection of major risk factors involved. J. Alzheimers. Dis. 34, 769–780. doi: 10.3233/JAD-122002
Eyben, F., Scherer, K. R., Schuller, B. W., Sundberg, J., André, E., Busso, C., et al. (2015). The geneva minimalistic acoustic parameter set (gemaps) for voice research and affective computing. IEEE Trans. Affect. Comput. 7, 190–202. doi: 10.1109/TAFFC.2015.2457417
Eyigoz, E., Mathur, S., Santamaria, M., Cecchi, G., and Naylor, M. (2020). Linguistic markers predict onset of alzheimer's disease. EClinicalMed. 28, 100583. doi: 10.1016/j.eclinm.2020.100583
Folstein, M. F. (1992). A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 12, 189–198.
Fraser, K. C., Meltzer, J. A., and Rudzicz, F. (2016). Linguistic features identify alzheimers disease in narrative speech. J. Alzheimer's Dis. 49, 407–422. doi: 10.3233/JAD-150520
Golden, C. J. (1980). In reply to adams's" in search of luria's battery: a false start. J. Consult. Clin. Psychol. 48, 511–516. doi: 10.1037/0022-006X.48.4.517
Goodglass, H., and Kaplan, E. (1972). The Assessment of Aphasia and Related Disorders. Philadelphia: Lea & Febiger.
Gosztolya, G., Vincze, V., Tóth, L., Pákáski, M., Kálmán, J., and Hoffmann, I. (2019). Identifying mild cognitive impairment and mild alzheimers disease based on spontaneous speech using asr and linguistic features. Comp. Speech & Lang. 53, 181–197. doi: 10.1016/j.csl.2018.07.007
Hachinski, V. C., Lassen, N. A., and Marshall, J. (1974). Multi-infarct dementia: a cause of mental deterioration in the elderly. Lancet 304, 207–209. doi: 10.1016/S0140-6736(74)91496-2
Haider, F., De La Fuente, S., and Luz, S. (2019). An assessment of paralinguistic acoustic features for detection of alzheimer's dementia in spontaneous speech. IEEE J. Sel. Top. Signal Process. 14, 272–281. doi: 10.1109/JSTSP.2019.2955022
Hajjar, I., Okafor, M., Choi, J. D., Moore, E., Abrol, A., Calhoun, V. D., et al. (2023). Development of digital voice biomarkers and associations with cognition, cerebrospinal biomarkers, and neural representation in early alzheimer's disease. Alzheimer's Dement. 15, e12393. doi: 10.1002/dad2.12393
He, R., Chapin, K., Al-Tamimi, J., Bel, N., Marquié, M., Rosende-Roca, M., et al. (2023). Automated classification of cognitive decline and probable alzheimer's dementia across multiple speech and language domains. Am. J. Speech-Lang. Pathol. 1–12. doi: 10.1044/2023_AJSLP-22-00403
Johnson, K. A., Fox, N. C., Sperling, R. A., and Klunk, W. E. (2012). Brain imaging in alzheimer disease. Cold Spring Harb. Perspect. Med. 2, a006213. doi: 10.1101/cshperspect.a006213
Kaplan, E., Goodglass, H., and Weintraub, S. (2001). Boston Naming Test, 2nd Edn. Philadelphia, PA: Lippincott Williams & Wilkins.
König, A., Satt, A., Sorin, A., Hoory, R., Toledo-Ronen, O., Derreumaux, A., et al. (2015). Automatic speech analysis for the assessment of patients with predementia and Alzheimer's disease. Alzheimer's Dement. 1, 112–124. doi: 10.1016/j.dadm.2014.11.012
Leit ao, M. J., Silva-Sp'ınola, A., Santana, I., Olmedo, V., Nadal, A., Le Bastard, N., et al. (2019). Clinical validation of the lumipulse g cerebrospinal fluid assays for routine diagnosis of alzheimers disease. Alzheimer's Res. Therap. 11, 1–12. doi: 10.1186/s13195-019-0550-8
Lindsay, H., Tröger, J., and König, A. (2021). Language impairment in alzheimers disease–robust and explainable evidence for ad-related deterioration of spontaneous speech through multilingual machine learning. Front. Aging Neurosci. 228, 642033. doi: 10.3389/fnagi.2021.642033
López-de Ipi na, K., Alonso, J.-B., Travieso, C. M., Solé-Casals, J., Egiraun, H., Faundez-Zanuy, M., et al. (2013). On the selection of non-invasive methods based on speech analysis oriented to automatic alzheimer disease diagnosis. Sensors 13, 6730–6745. doi: 10.3390/s130506730
Lundberg, S. M., and Lee, S.-I. (2017). “A unified approach to interpreting model predictions,” in Advances in Neural Information Processing Systems 30, Guyon, I., Luxburg, U. V., Bengio, S., Wallach, H., Fergus, R., Vishwanathan, S., et al. (eds.). Red Hook, NY: Curran Associates, Inc., 4765–4774.
Mahajan, P., and Baths, V. (2021). Acoustic and language based deep learning approaches for alzheimer's dementia detection from spontaneous speech. Front. Aging Neurosci. 13, 623607. doi: 10.3389/fnagi.2021.623607
Martínez-Nicolás, I., Llorente, T. E., Martínez-Sánchez, F., and Meilán, J. J. G. (2021). Ten years of research on automatic voice and speech analysis of people with alzheimer's disease and mild cognitive impairment: a systematic review article. Front. Psychol. 12, 620251. doi: 10.3389/fpsyg.2021.620251
Mazzeo, S., Polito, C., Lassi, M., Bagnoli, S., Mattei, M., Padiglioni, S., et al. (2022). Loss of speech and functional impairment in alzheimer's disease-related primary progressive aphasia: predictive factors of decline. Neurobiol. Aging 117, 59–70. doi: 10.1016/j.neurobiolaging.2022.05.002
McKhann, G. M., Knopman, D. S., Chertkow, H., Hyman, B. T., Jack Jr, C. R., Kawas, C. H., et al. (2011). The diagnosis of dementia due to alzheimers disease: Recommendations from the national institute on aging-Alzheimers association workgroups on diagnostic guidelines for alzheimer's disease. Alzheimer's Dement. 7, 263–269. doi: 10.1016/j.jalz.2011.03.005
Molinuevo, J. L., Ayton, S., Batrla, R., Bednar, M. M., Bittner, T., Cummings, J., et al. (2018). Current state of alzheimers fluid biomarkers. Acta Neuropathol. 136, 821–853. doi: 10.1007/s00401-018-1932-x
Montembeault, M., Chapleau, M., Jarret, J., Boukadi, M., Laforce Jr, R., Wilson, M. A., et al. (2019). Differential language network functional connectivity alterations in Alzheimer's disease and the semantic variant of primary progressive aphasia. Cortex 117, 284–298. doi: 10.1016/j.cortex.2019.03.018
Morris, J. C. (1993). The clinical dementia rating (cdr): current version and scoring rules. Neurology 43, 2412–4. doi: 10.1212/WNL.43.11.2412-a
Mueller, K. D., Hermann, B., Mecollari, J., and Turkstra, L. S. (2018). Connected speech and language in mild cognitive impairment and Alzheimers disease: a review of picture description tasks. J. Clin. Exp. Neuropsychol. 40, 917–939. doi: 10.1080/13803395.2018.1446513
Mueller, K. D., Van Hulle, C. A., Koscik, R. L., Jonaitis, E., Peters, C. C., Betthauser, T. J., et al. (2021). Amyloid beta associations with connected speech in cognitively unimpaired adults. Alzheimer's & Dement. 13, e12203. doi: 10.1002/dad2.12203
Nagumo, R., Zhang, Y., Ogawa, Y., Hosokawa, M., Abe, K., Ukeda, T., et al. (2020). Automatic detection of cognitive impairments through acoustic analysis of speech. Curr. Alzheimer Res. 17, 60. doi: 10.2174/1567205017666200213094513
Orellana, A., García-González, P., Valero, S., Montrreal, L., de Rojas, I., Hernández, I., et al. (2022). Establishing in-house cutoffs of csf alzheimers disease biomarkers for the at (n) stratification of the Alzheimer center barcelona cohort. Int. J. Mol. Sci. 23, 6891. doi: 10.3390/ijms23136891
Pena-Casanova, J., Sánchez-Benavides, G., de Sola, S., Manero-Borrás, R. M., and Casals-Coll, M. (2012). Neuropsychology of Alzheimer's disease. Arch. Med. Res. 43, 686–693. doi: 10.1016/j.arcmed.2012.08.015
Petersen, R. C. (2004). Mild cognitive impairment as a diagnostic entity. J. Intern. Med. 256, 183–194. doi: 10.1111/j.1365-2796.2004.01388.x
Pillon, B., Dubois, B., Bonnet, A., Esteguy, M., Guimaraes, J., Vigouret, J., et al. (1989). Cognitive slowing in parkinson's disease fails to respond to levodopa treatment: the 15-objects test. Neurology 39, 762–762. doi: 10.1212/WNL.39.6.762
Rafiq, M., Jucla, M., Guerrier, L., Péran, P., Pariente, J., and Pistono, A. (2022). The functional connectivity of language network across the life span: disentangling the effects of typical aging from alzheimers disease. Front. Aging Neurosci. 14, 959405. doi: 10.3389/fnagi.2022.959405
Sainburg, T., McInnes, L., and Gentner, T. Q. (2020). Parametric umap: learning embeddings with deep neural networks for representation and semi-supervised learning. ArXiv e. doi: 10.1162/neco_a_01434
Sala, S. D., Laiacona, M., Trivelli, C., and Spinnler, H. (1995). Poppelreuter-ghent's overlapping figures test: its sensitivity to age, and its clinical use. Arch. Clini. Neuropsychol. 10, 511–534. doi: 10.1093/arclin/10.6.511
Sauter, D. A., Eisner, F., Calder, A. J., and Scott, S. K. (2010). Perceptual cues in nonverbal vocal expressions of emotion. Quart. J. Exp. Psychol. 63, 2251–2272. doi: 10.1080/17470211003721642
Scheltens, P., De Strooper, B., Kivipelto, M., Holstege, H., Chételat, G., Teunissen, C. E., et al. (2021). Alzheimer's disease. Lancet 397, 1577–1590. doi: 10.1016/S0140-6736(20)32205-4
Scherer, K. R. (1986). Vocal affect expression: a review and a model for future research. Psychol. Bull. 99, 143. doi: 10.1037/0033-2909.99.2.143
Small, S. A., Perera, G. M., DeLaPaz, R., Mayeux, R., and Stern, Y. (1999). Differential regional dysfunction of the hippocampal formation among elderly with memory decline and alzheimer's disease. Ann. Neurol. 45, 466–472.
Smits, L. L., Tijms, B. M., Benedictus, M. R., Koedam, E. L., Koene, T., Reuling, I. E., et al. (2014). Regional atrophy is associated with impairment in distinct cognitive domains in alzheimer's disease. Alzheimer's Dement. 10, S299-S305. doi: 10.1016/j.jalz.2013.06.007
Sperling, R. A., Aisen, P. S., Beckett, L. A., Bennett, D. A., Craft, S., Fagan, A. M., et al. (2011). Toward defining the preclinical stages of alzheimers disease: Recommendations from the national institute on aging-alzheimer's association workgroups on diagnostic guidelines for alzheimer's disease. Alzheimer's Dement. 7, 280–292. doi: 10.1016/j.jalz.2011.03.003
Taler, V., and Phillips, N. A. (2008). Language performance in alzheimer's disease and mild cognitive impairment: a comparative review. J. Clin. Exp. Neuropsychol. 30, 501–556. doi: 10.1080/13803390701550128
Themistocleous, C., Eckerström, M., and Kokkinakis, D. (2018). Identification of mild cognitive impairment from speech in swedish using deep sequential neural networks. Front. Neurol. 9, 975. doi: 10.3389/fneur.2018.00975
Themistocleous, C., Eckerström, M., and Kokkinakis, D. (2020). Voice quality and speech fluency distinguish individuals with mild cognitive impairment from healthy controls. PLoS ONE 15, e0236009. doi: 10.1371/journal.pone.0236009
Thijssen, E. H., Verberk, I. M., Kindermans, J., Abramian, A., Vanbrabant, J., Ball, A. J., et al. (2022). Differential diagnostic performance of a panel of plasma biomarkers for different types of dementia. Alzheimer's Dement. 14, e12285. doi: 10.1002/dad2.12285
Thomas, J. A., Burkhardt, H. A., Chaudhry, S., Ngo, A. D., Sharma, S., Zhang, L., et al. (2020). Assessing the utility of language and voice biomarkers to predict cognitive impairment in the framingham heart study cognitive aging cohort data. J. Alzheimer's Dis. 76, 905–922. doi: 10.3233/JAD-190783
Tóth, L., Hoffmann, I., Gosztolya, G., Vincze, V., Szatlóczki, G., Bánréti, Z., et al. (2018). A speech recognition-based solution for the automatic detection of mild cognitive impairment from spontaneous speech. Curr. Alzheimer Res. 15, 130–138. doi: 10.2174/1567205014666171121114930
Tran, B., Xue, B., and Zhang, M. (2018). Variable-length particle swarm optimization for feature selection on high-dimensional classification. IEEE Trans. Evol. Comput. 23, 473–487. doi: 10.1109/TEVC.2018.2869405
Tröger, J., Baykara, E., Zhao, J., Ter Huurne, D., Possemis, N., Mallick, E., et al. (2022). Validation of the remote automated ki: e speech biomarker for cognition in mild cognitive impairment: Verification and validation following dime v3 framework. Digital Biomark. 6, 107–116. doi: 10.1159/000526471
Vanderstichele, H., Bibl, M., Engelborghs, S., Le Bastard, N., Lewczuk, P., Molinuevo, J. L., et al. (2012). Standardization of preanalytical aspects of cerebrospinal fluid biomarker testing for alzheimer's disease diagnosis: a consensus paper from the alzheimer's biomarkers standardization initiative. Alzheimer's Dement. 8, 65–73. doi: 10.1016/j.jalz.2011.07.004
Vanhoutte, M., Semah, F., Sillaire, A. R., Jaillard, A., Petyt, G., Kuchcinski, G., et al. (2017). 18f-fdg pet hypometabolism patterns reflect clinical heterogeneity in sporadic forms of early-onset alzheimer's disease. Neurobiol. Aging 59, 184–196. doi: 10.1016/j.neurobiolaging.2017.08.009
Verfaillie, S. C., Witteman, J., Slot, R. E., Pruis, I. J., Vermaat, L. E., Prins, N. D., et al. (2019). High amyloid burden is associated with fewer specific words during spontaneous speech in individuals with subjective cognitive decline. Neuropsychologia 131, 184–192. doi: 10.1016/j.neuropsychologia.2019.05.006
Voleti, R., Liss, J. M., and Berisha, V. (2019). A review of automated speech and language features for assessment of cognitive and thought disorders. IEEE J. Sel. Top. Signal Process. 14, 282–298. doi: 10.1109/JSTSP.2019.2952087
Wang, H.-L., Tang, R., Ren, R.-J., Dammer, E. B., Guo, Q.-H., Peng, G.-P., et al. (2022). Speech silence character as a diagnostic biomarker of early cognitive decline and its functional mechanism: a multicenter cross-sectional cohort study. BMC Med. 20, 1–10. doi: 10.1186/s12916-022-02584-x
Wechsler, D. (1997). WMS-III: Wechsler Memory Scale Administration and Scoring Manual. San Antonio, TX: Psychological Corporation.
Wei, H., Kong, M., Zhang, C., Guan, L., Ba, M., Initiative, A. D. N., et al. (2018). The structural mri markers and cognitive decline in prodromal alzheimers disease: a 2-year longitudinal study. Quant. Imaging Med. Surg. 8, 1004. doi: 10.21037/qims.2018.10.08
Weimer, D. L., and Sager, M. A. (2009). Early identification and treatment of alzheimer's disease: social and fiscal outcomes. Alzheimer's Dement. 5, 215–226. doi: 10.1016/j.jalz.2009.01.028
Whelan, R., Barbey, F. M., Cominetti, M. R., Gillan, C. M., and Rosická, A. M. (2022). Developments in scalable strategies for detecting early markers of cognitive decline. Transl. Psychiatry 12, 473. doi: 10.1038/s41398-022-02237-w
Wilson, B., and Petkov, C. I. (2011). Communication and the primate brain: insights from neuroimaging studies in humans, chimpanzees and macaques. Hum. Biol. 83, 175–189. doi: 10.1353/hub.2011.a438019
Xue, B., Zhang, M., Browne, W. N., and Yao, X. (2015). A survey on evolutionary computation approaches to feature selection. IEEE Trans. Evol. Comput. 20, 606–626. doi: 10.1109/TEVC.2015.2504420
Keywords: Alzheimer's disease, mild cognitive impairment, early diagnosis, cerebrospinal fluid, biomarkers, machine learning, speech acoustics, automated pattern recognition
Citation: García-Gutiérrez F, Marquié M, Muñoz N, Alegret M, Cano A, de Rojas I, García-González P, Olivé C, Puerta R, Orellana A, Montrreal L, Pytel V, Ricciardi M, Zaldua C, Gabirondo P, Hinzen W, Lleonart N, García-Sánchez A, Tárraga L, Ruiz A, Boada M and Valero S (2023) Harnessing acoustic speech parameters to decipher amyloid status in individuals with mild cognitive impairment. Front. Neurosci. 17:1221401. doi: 10.3389/fnins.2023.1221401
Received: 12 May 2023; Accepted: 08 August 2023;
Published: 07 September 2023.
Edited by:
I-Shiang Tzeng, National Taipei University, TaiwanReviewed by:
Masaru Tanaka, University of Szeged (ELKH-SZTE), HungaryGang Wang, Shanghai Jiao Tong University, China
Copyright © 2023 García-Gutiérrez, Marquié, Muñoz, Alegret, Cano, de Rojas, García-González, Olivé, Puerta, Orellana, Montrreal, Pytel, Ricciardi, Zaldua, Gabirondo, Hinzen, Lleonart, García-Sánchez, Tárraga, Ruiz, Boada and Valero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sergi Valero, c3ZhbGVyb0BmdW5kYWNpb2FjZS5vcmc=
†These authors have contributed equally to this work