
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurosci., 16 March 2023
Sec. Perception Science
Volume 17 - 2023 | https://doi.org/10.3389/fnins.2023.1148176
This article is part of the Research TopicInterplay Between Pain and Cognitive Dysfunction Volume IIView all 5 articles
 Selma Delgado-Gallén1,2,3*
Selma Delgado-Gallén1,2,3* MD Soler1,2,3
MD Soler1,2,3 María Cabello-Toscano1,4,5
María Cabello-Toscano1,4,5 Kilian Abellaneda-Pérez1,2,3
Kilian Abellaneda-Pérez1,2,3 Javier Solana-Sánchez1,2,3
Javier Solana-Sánchez1,2,3 Goretti España-Irla1,2,3
Goretti España-Irla1,2,3 Alba Roca-Ventura1,4,5
Alba Roca-Ventura1,4,5 David Bartrés-Faz1,4,5
David Bartrés-Faz1,4,5 Josep M. Tormos1,6
Josep M. Tormos1,6 Alvaro Pascual-Leone1,7,8
Alvaro Pascual-Leone1,7,8 Gabriele Cattaneo1,2,3
Gabriele Cattaneo1,2,3Pain processing involves emotional and cognitive factors that can modify pain perception. Increasing evidence suggests that pain catastrophizing (PC) is implicated, through pain-related self-thoughts, in the maladaptive plastic changes related to the maintenance of chronic pain (CP). Functional magnetic resonance imaging (fMRI) studies have shown an association between CP and two main networks: default mode (DMN) and dorsoattentional (DAN). Brain system segregation degree (SyS), an fMRI framework used to quantify the extent to which functional networks are segregated from each other, is associated with cognitive abilities in both healthy individuals and neurological patients. We hypothesized that individuals suffering from CP would show worst health-related status compared to healthy individuals and that, within CP individuals, longitudinal changes in pain experience (pain intensity and affective interference), could be predicted by SyS and PC subdomains (rumination, magnification, and helplessness). To assess the longitudinal progression of CP, two pain surveys were taken before and after an in-person assessment (physical evaluation and fMRI). We first compared the sociodemographic, health-related, and SyS data in the whole sample (no pain and pain groups). Secondly, we ran linear regression and a moderation model only in the pain group, to see the predictive and moderator values of PC and SyS in pain progression. From our sample of 347 individuals (mean age = 53.84, 55.2% women), 133 responded to having CP, and 214 denied having CP. When comparing groups, results showed significant differences in health-related questionnaires, but no differences in SyS. Within the pain group, helplessness (β = 0.325; p = 0.003), higher DMN (β = 0.193; p = 0.037), and lower DAN segregation (β = 0.215; p = 0.014) were strongly associated with a worsening in pain experience over time. Moreover, helplessness moderated the association between DMN segregation and pain experience progression (p = 0.003). Our findings indicate that the efficient functioning of these networks and catastrophizing could be used as predictors of pain progression, bringing new light to the influence of the interplay between psychological aspects and brain networks. Consequently, approaches focusing on these factors could minimize the impact on daily life activities.
Chronic pain (CP) is an unpleasant sensory and emotional experience associated with negative cognitive and emotional aspects like the feeling of unpleasantness, pain catastrophizing (PC), and decreased physical and psychological functioning across the lifespan (Dahlhamer, 2018). This prolonged pain experience encompasses pain intensity (i.e., how much a patient is in pain) and pain affection aspects, the degree of emotional arousal caused by the sensory experience of pain (Haefeli and Elfering, 2006).
These aspects influence pain perception and modulation, and vice-versa (Wiech, 2016, 2018; Opdebeeck et al., 2018; Wiech and Shriver, 2018; Delgado-Gallén et al., 2021), resulting in large inter-individual differences in terms of pain assessment and treatment. Thus, in the past decades, PC and functional brain connectivity (FC) has been shown to play an important role in understanding pain experience, its chronification, and treatment response.
Pain catastrophizing, intended as the tendency to magnify and ruminate about pain, boasts attentional biases to threatening aspects of painful experience (Gilliam et al., 2017) and, consequently, impacts self-reported pain intensity and pain-related psychological aspects (Jensen et al., 2017; Suso-Ribera et al., 2017; Häggman-Henrikson et al., 2021). Therefore, the combination of PC and unpleasantness can lead to suffering, anger, fear, frustration, or anxiety, having an important role in adjustment to CP (Ziadni et al., 2018) and pain management (Gilliam et al., 2017).
In this line, it has been suggested that the relationship between pain and depressed mood is mediated by PC (Dong et al., 2020). In addition, studies exploring the differential relationships among individual components of PC (helplessness, magnification, and rumination) and pain outcomes (Müller, 2011; Craner et al., 2016; Stensland, 2021), indicated that catastrophic thoughts and behavior are as well linked with pain co-morbidities as sleep (Abeler et al., 2020), mental health (Dong et al., 2020) and physical activity. Furthermore, the predictive value of PC in pain evolution has been found in several studies. For instance, high levels of PC predicted a decrease in physical activity due to sedentary behavior (Zhaoyang et al., 2020), or higher levels of acute or persistent pain after surgery for knee osteoarthritis (Burns et al., 2015).
Also, the neural correlates of these phenomena have been explored in multiple studies. Altered brain connectivity in pain disorders in task-oriented and resting-state functional magnetic resonance imaging (rs-fMRI) has been shown altered in the presence of acute and CP (Baliki et al., 2014; Kucyi et al., 2014; Yu et al., 2014; Hemington et al., 2016; Pfannmöller and Lotze, 2019; Spisak et al., 2019; You et al., 2021; De Ridder et al., 2022; Solé-Padullés et al., 2022). Crucially it has been suggested that two specific main large-scale brain networks are related to altered pain processing and pain chronification: the dorsoattentional network (DAN), and the default mode network (DMN) (Spreng et al., 2013; Baliki et al., 2014; Becerra et al., 2014; Kucyi et al., 2014; Kilpatrick et al., 2015; Seidler et al., 2015; Franzmeier et al., 2017; Kim et al., 2019; van Ettinger-Veenstra et al., 2019; Jones et al., 2020; De Ridder et al., 2022).
DAN network is prominently involved in goal-directed attention and top-down selection of stimuli and responses, interacting dynamically with the salience network (SN) and control executive network. Concretely, DAN is responsible for the maintenance of spatial priority maps for covert spatial attention, saccade planning, and visual working memory (Vossel et al., 2014). In CP patients it has been found that the functional connectivity of this network, especially concerning its connectivity with other large-scale networks, is consistently altered (Coppola et al., 2019; Mao et al., 2022), and could normalize after pain therapy (Yoshino et al., 2018).
On the other hand, the DMN, which controls self-representational processing, is normally deactivated during task or stimulus exposure, but not in CP patients (Legrain et al., 2009; Seminowicz et al., 2011; Kucyi et al., 2014; De Ridder et al., 2022), exhibiting abnormal DMN resting-state functional connectivity (rs-FC). Alteration in the connectivity of this network has been coupled to several pain types (e.g., low back pain, complex regional pain syndrome (CRPS), chronic widespread pain, or osteoarthritic pain), potentially explaining why pain becomes an integral part of the self. Finally, DMN has been also consistently associated with pain anticipation, pain intensity, and PC (Napadow et al., 2010; Ter Minassian et al., 2012; Loggia et al., 2013; Kucyi et al., 2014; De Ridder et al., 2022).
In this study we aim to use a novel approach in the study of the relationship between CP, PC, and brain networks functional connectivity, using rs-fMRI combined with graph theory methods (i.e., the topological organization of brain networks) (Wang et al., 2010; Ewers et al., 2021). Concretely we will study networks system segregation (SyS) (Wig, 2017), a paradigm based on the idea that effective network functioning is supported by maintaining subnetworks’ segregation while simultaneously allowing integration between them (Wig, 2017), resulting in a brain more adaptable to task demands. Brain networks’ segregation degree has been previously associated with cognitive abilities in healthy adults and patients affected by neurologic diseases (van den Heuvel and Sporns, 2013; Malagurski et al., 2020; Ewers et al., 2021; Riedel et al., 2021).
From our knowledge, this is the first study that explores how SyS, the ratio of rs-FC within brain networks and their connection with the rest of the cortex, could be related to the presence of pain, and the potential role of SyS and pain-related psychological factors in longitudinal changes in the pain experience.
This study was performed in the framework of the Barcelona Brain Health Initiative (BBHI) (Cattaneo et al., 2018, 2020), an ongoing prospective longitudinal study that started in 2017 to identify lifestyle factors and biological mechanisms underlying good brain health in middle-aged adults (40–65 years). Between 2018 and 2021 participants underwent an online self-assessment (through the BBHI web-based platform) of sociodemographic characteristics, mental health (MH), quality of life (QoL), and self-perceived cognitive concerns (see Figure 1 for more details). Between 2019 and 2020 they answered the baseline pain questionnaire (T1), and from 2020 to 2021 the second one (T2).
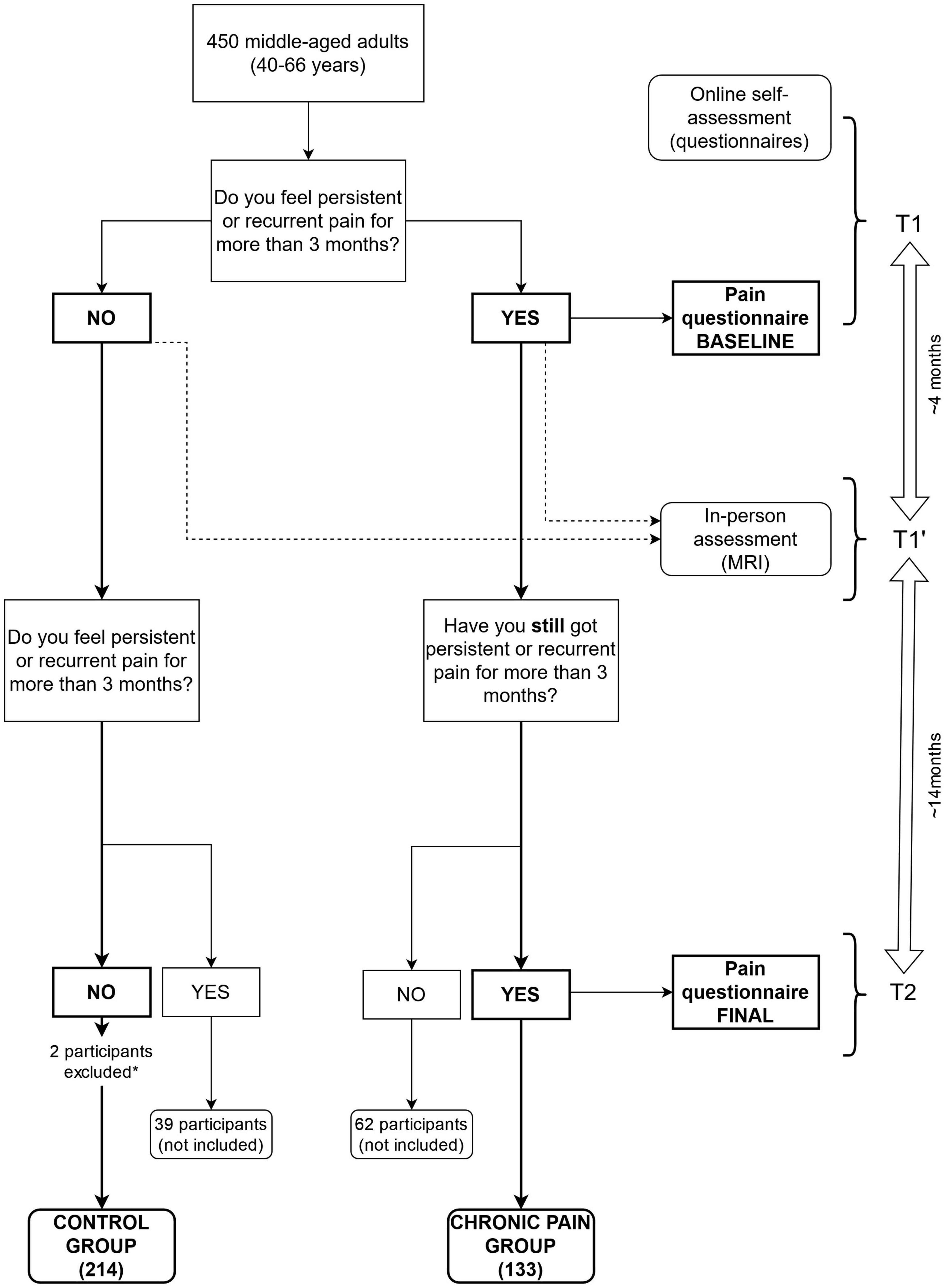
Figure 1. Flowchart of the selection and distribution of patients in this study. Chart illustrating how participants were asked to fill questionnaires (T1 and T2) and undertake an MRI (T1′), and then formed the pain group (YES-YES) and the no pain group (NO-NO). Those participants who did not maintain pain on both questionnaires were not included on this study (YES-NO, NO-YES). Mean time between first questionnaire (T1) and the MRI (T1′) was approximately 4 months, and between the MRI and the second questionnaire (T2), 14 months. *Two participants were excluded from the no pain group for having excessive motion (at least the 50% of the between scans movements were above a 0.5 mm threshold).
Parallelly, between May 2018 and February 2021 (T1′), participants performed an in-person assessment, including a medical exam and MRI. The same in-person evaluation protocol was applied to all participants.
Online questionnaires and in-person assessments were not paralleled in time and were not equal for all participants. The time gap between T1 and T1′ was approximately 4 months, and between T1′ and T2, 14 months. However, the minimum distance between questionnaires, and between the fMRI scan and T2 was fixed at 3 months to leave room for a reliable pain progression and assure that the criteria for the diagnosis of CP (3 months) were satisfied in each questionnaire independently from the other.
Participants with CP were excluded if (1) pain was due to cancer, fracture, infection, or diagnosis of neurologic or psychiatric disease, (2) made active substance abuse disorder in the past 2 years, (3) uses of prescription opioids exceeding 60 mg morphine equivalents per day, (4) were not suitable for MRI scan and (5) they had excessive head motion during the MRI (at least in the 50% of the scans movements were above a 0.5 mm threshold).
From our sample, 450 participants completed online and in-person assessments (see Figure 1): 133 consistently answered having CP (see below for a CP definition) that persisted for at least 3 months in both questionnaires, 216 without CP in any time-point (where 2 participants were excluded for excessive head motion during MRI), 39 participants that developed CP (that is, they first answered not having CP, and in the second questionnaire they did), and 62 that recovered from a CP (i.e., they started with CP and then they reported not having pain anymore). Considering our principal aim to study pain chronification and its maintenance, the present work included 347 volunteers (133 with CP and 214 without CP).
The protocol was approved by the “Comité d’Ètica i Investigació Clínica de la Unió Catalana d’Hospitals” and was carried out following the Declaration of Helsinki (World Medical Association, 2013). Written informed consent was obtained from all participants before inclusion in the study.
Participants were screened online for CP, which was considered the pain that persists or recurs for > 3 months according to the International Association for the Study of Pain (IASP) criteria (Treede et al., 2015).
Only those participants who answered to have recurring or persisting pain underwent the posterior pain assessment explained below. Thus, the pain group in this study was formed by participants who answered to have pain during at least 3 months in both questionnaires (T1 and T2), while participants who had not CP in either of the questionnaires were included in the no pain group. Non-recurrent or non-persistent pain (i.e., acute pain) was not assessed in this study, neither in healthy nor in CP subjects.
The Brief Pain Inventory-Short Form (BPI-SF) (Keller et al., 2004) was used to assess the intensity and severity of pain and pain onset. Validation studies among CP patients and the published Spanish translation demonstrated good psychometric properties (Badia et al., 2003).
Pain intensity was estimated considering the mean of pain intensity in the last week, considering that asking for a short past period (i.e., 1 week) is more reliable than asking for “current” pain (Haefeli and Elfering, 2006).
Pain interference was estimated through seven domains divided into two subdimensions (with the arithmetic mean): affective (relations with others, enjoyment of life, sleep, and mood) and activity (walking, general activity, and work), according to the BPI user guide (Cleeland and Ryan, 1991). Although sleep is seen as a third domain in some studies, we used it in the affective domain (Miettinen et al., 2019).
Questions about the number of pain sites (one, two, three, or four or more pain sites), and pain medication (non-steroidal anti-inflammatory, anti-migraines…) were added to the questionnaire.
The first and second assessments were conducted during 2019–2020 (T1) and 2020–2021 (T2), respectively, (approximately 10 months between both, see Figure 1).
To calculate the longitudinal progression of the pain experience, we calculated the mean between pain intensity and pain affective interference at each time point:
Then we subtracted the numerical value of the first assessment from the second assessment, resulting in a worsening if the final score was positive or an amelioration if it was negative.
Pain catastrophizing can be understood as an expansion of maladaptive cognitive response during actual or perceived painful stimuli, comprising negative cognitive and emotional processes. The PC scale is a multidimensional construct that encompasses elements of rumination, magnification, and helplessness. It can be computed by summing responses to all 13 items, and uses a 5-point scale, ranging from 0 (not at all) to 4 (all the time). The total scale score ranges from 0 to 52, with higher scores representing greater catastrophic thinking. Participants are asked to indicate the degree to which they experienced each of the 13 thoughts or feelings when experiencing pain. This scale has been demonstrated to have good psychometric proprieties (Sullivan et al., 1995; García Campayo et al., 2008; Olmedilla Zafra et al., 2013) and it has been validated in the Spanish language.
We employed the ultra-brief self-reported Patient Health Questionnaire-4 (PHQ-4) to assess MH. The PHQ-4 had four items asking about mood disorder symptoms (two items for depression and the other two items for anxiety) in the past 2 weeks. All items were rated on a four-point scale ranging from 0 (not at all) to 3 (nearly every day). The published Spanish translation also demonstrated good psychometric properties in a validation study (Kocalevent et al., 2014).
To assess the QoL, we used WHO-QoL-AGE, a 13-item questionnaire scored on a 5-point Likert scale. This questionnaire attempts to assess satisfaction with one’s life, living place, general health (i.e., hearing, vision…), daily activities, personal relationships, goal achievements, or economic status (The Whoqol Group, 1998). The published Spanish translation has good psychometric data in a validation study (Lucas-Carrasco, 2012).
We used PROMIS® Cognitive Abilities and Cognitive Concerns scales to assess cognitive troubles. This scale consists of 12-item, extracted from the PROMIS item bank, measuring self-reported cognitive deficits in memory, working memory, attention, processing speed, or cognitive flexibility (Fieo et al., 2016). Each item asked participants to answer “within the last 7 days” using five response options.
Magnetic resonance imaging data were acquired in a 3T Siemens scanner (MAGNETOM Prisma) (Siemens Healthcare GmbH, Erlangen, Germany) with a 32-channel head coil, at the Unitat d’Imatge per Ressonància Magnètica IDIBAPS (Institut d’Investigacions Biomèdiques August Pi i Sunyer) at Hospital Clínic de Barcelona, Barcelona. MRI session included accelerated multi-band sequences adapted from the Human Connectome Project and provided by the Center of Magnetic Resonance Research at the University of Minnesota. For all participants, a high-resolution T1-weighted structural image was obtained with a magnetization-prepared rapid acquisition gradient-echo (MPRAGE) three-dimensional protocol, and a total of 208 contiguous axial slices were obtained in ascending fashion [repetition time (TR) = 2,400 ms, echo time (TE) = 2.22 ms, inversion time = 1,000 ms, flip angle = 8°, a field of view (FOV) = 256 mm and 0.8 mm isotropic voxel]. Additionally, a high-resolution 3D SPC T2 weighted acquisition was undertaken (TR = 3,200 ms, TE = 563 ms, flip angle = 120°, 0.8 mm isotropic voxel, FOV = 256 mm). In the same session, they also underwent rs-fMRI multiband (anterior-posterior phase-encoding; acceleration factor = 8) interleaved acquisitions (T2*weighted EPI scans, TR = 800 ms, TE = 37 ms, 750 volumes, 72 slices, slice thickness = 2 mm, FOV = 208 mm). All the MRI images were examined by a senior neuroradiologist (NB) to detect any clinically significant pathology (none found). Then, all the acquisitions were visually inspected before analysis (MC-T and LM-P.) to ensure that they did not contain MRI artifacts or excessive motion.
The rs-fMRI preprocessing pipeline comprised spatial standardization and nuisance correction by making use of functions from FMRIB Software Library (FSL; version 5.0.11)1, FreeSurfer (version 6.0)2 and Statistical Parametric Mapping (SPM12).3 To start with, the first 10 scans were removed to ensure magnetization equilibrium. After that, all images were field inhomogeneity corrected (FSL topup tool), all scans realigned to a reference image (FSL MCFLIRT), and then standardized into native T1-weighted space (SPM Coregister). Finally, normalization (SPM Normalize) of all fMRI images to Montreal Neuroscience Institute (MNI152) standard space was performed to ensure among-subjects comparability. As for nuisance correction, different components were defined and manually removed from the rs-fMRI images by the “fsl_regfilt” tool implemented in FSL. These components correspond to (1) motion regressors of rotation, translation, and their derivatives, as estimated during scans’ realignment, (2) a drift estimated by a discrete cosine transform (DCT) as a low-pass frequency filter (< 0.01), and (3) signals from white matter (WM) and cerebrospinal fluid (CSF). To extract these, CSF and WM masks were obtained from automatic subcortical segmentation of brain volume, based on the existence of an atlas containing probabilistic information on the location of structures (Fischl et al., 2002). This step was part of the FreeSurfer “recon-all” processing stream, which was run with default parameters, except for the addition of the T2 flag for the improvement of pial surfaces reconstruction. Both T1-w and T2-w images were used for processing anatomical information.
As head movement may affect rs-fMRI results (Van Dijk et al., 2012; Power et al., 2013, 2014, 2015), the in-scanner head motion was considered. In this study, the framewise displacement (FWD) mean was calculated for every subject. FWD was computed as in Power et al. (2012), using the vectors of rotation and translation estimated during scans’ realignment as part of the preprocessing pipeline (Power et al., 2012).
A node-based approach was adopted to quantify subject rs-FC and SyS of seven resting-state networks (RSN) as defined in the Yeo atlas (Thomas Yeo et al., 2011). These functional connectivity measures have been previously used to study brain networks implicated in pain progression (Kastrati et al., 2022; Lee et al., 2022). To increase Yeo-atlas spatial resolution and precision at rs-FC computation, the 100 nodes, and 7 networks Schaeffer-Yeo atlas was used (Figure 2; Schaefer et al., 2018).4 Per each of the 100 regions of interest (ROIs), a BOLD signal was extracted and averaged across all voxels falling within an ROI. Then, ROI-to-ROI rs-FCs were computed as Pearson-Moment correlations, and subsequently, Fisher-z transformed. Negative values were set to zero and autocorrelations were not considered in the further computation.
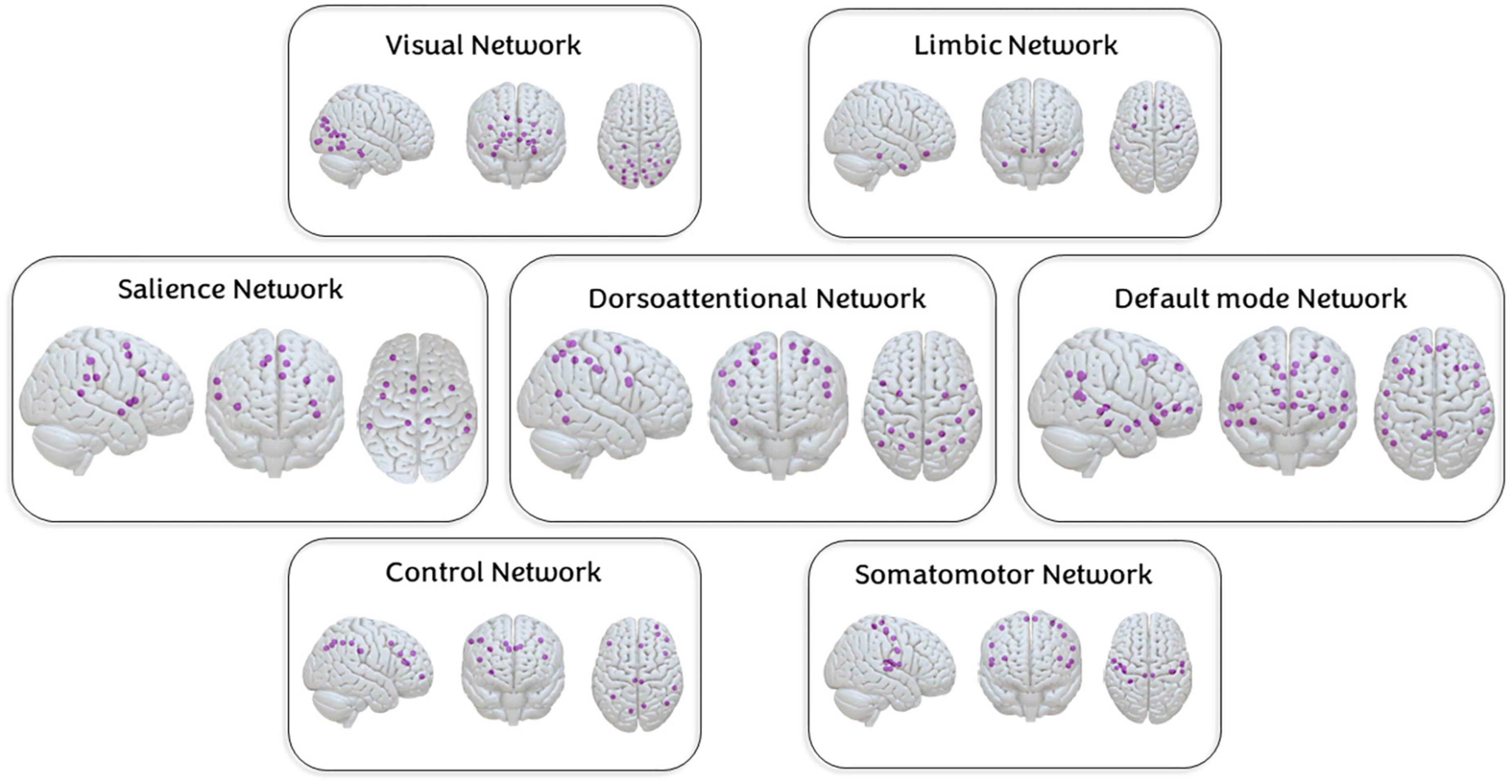
Figure 2. Nodes of the seven networks. Nodes of each of the studied networks based on the Schaffer-Yeo atlas of 100 regions of interest and 7 networks.
System segregation (SyS) is a graph theory metric to quantify the extent to which major functional networks are segregated from each other (see Figure 3). As expressed in
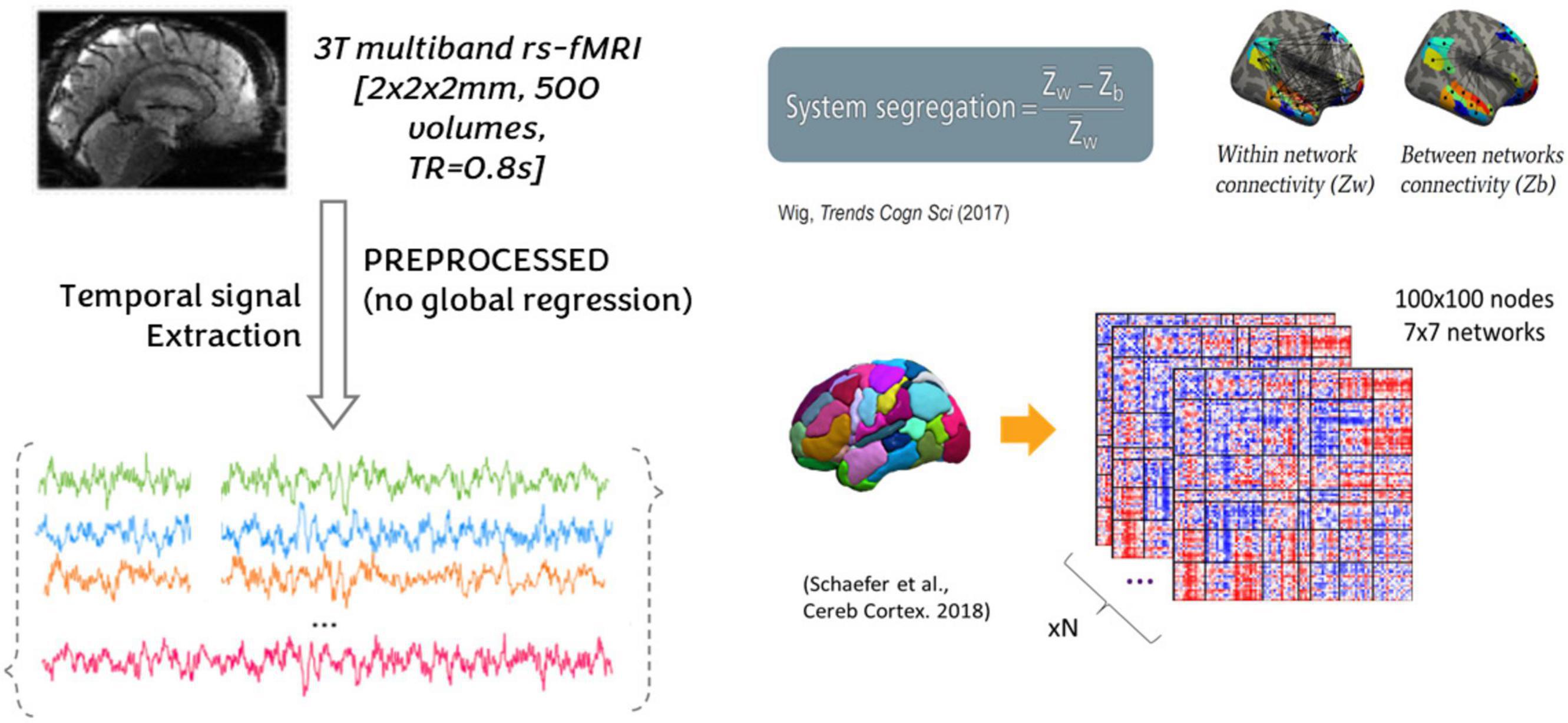
Figure 3. Nodes of the seven networks. A node-based approach was adopted to quantify subject rs-FC and SyS of seven resting-state networks (RSN) as defined in the Yeo atlas (Thomas Yeo et al., 2011). Per each of the 100 regions of interest (ROIs), a BOLD signal was extracted and averaged across all voxels falling within an ROI. Then, ROI-to-ROI rs-FCs were computed as Pearson-moment correlations, and subsequently, Fisher-z transformed. Negative values were set to zero and autocorrelations were not considered in the further computation. SyS captures the balance between within-network (Wnet) and between-networks (Bnet) rs-FC. Within-network rs-FC was computed as the average rs-FC connecting all the nodes within the same network. Between-network rs-FC was computed as the average rs-FC connecting nodes of a particular network to nodes from the rest of the cortex.
System segregation (SyS) captures the balance between within-network (Wnet) and between-networks (Bnet) rs-FC. Within-network rs-FC was computed as the average rs-FC connecting all the nodes within the same network. Between-network rs-FC was computed as the average rs-FC connecting nodes of a particular network to nodes from the rest of the cortex.
We first analyzed group differences (no pain and CP) in sociodemographic data [age, biological sex, and body mass index (BMI)], health-related questionnaire scores (MH, cognitive complaints, and QoL), and head movements during the scan using Welch t-tests and chi-square statistics. In addition, we also ran a multivariate analysis between these groups on the segregation of networks, correcting for the delay between the first questionnaire and MRI, head movement during MRI, age, and biological sex.
We ran bivariate correlations to explore the association between psychological variables (MH, QoL, cognitive concerns), PC subscales, and pain variables at baseline (intensity, interference, number of pain sites, duration, and medication intake). Besides, we ran partial correlations between SyS and pain factors (intensity, interference, and the number of pain sites), correcting for age, gender, and head motion.
We explored the differences between pain characteristics (intensity, affective and activity interference, number of pain sites, pain duration, and pain-related medication) in both time points using t-tests and chi-square statistics.
To explore which variables affected pain experience over time, we ran a first multiple regression model with pain experience as the primary outcome, and sociodemographic data (age, biological sex, and BMI), pain baseline ratings (pain-related medication, intensity, total interference, duration, and the number of pain sites), PC scale total score and health-related questionnaires (MH, QoL, and cognitive concerns) as regressors.
Then, we ran different multiple regression models using pain experience progression (Pain experience 2- Pain experience 1) as the dependent variable and sociodemographic (age and biological sex), PC subscales, pain characteristics at baseline (intensity, affective interference, and activity interference), and SyS. We also added covariable head motion during the MRI, as it has an important influence on intrinsic functional connectivity and its interpretation (Van Dijk et al., 2012), in the model and the time between the first questionnaire (T1) and MRI (T1′).
Finally, we added a multicollinearity diagnostic to ensure the interdependence of regressors using the variance inflation factor coefficient. Variables in this step were selected from previous analyses depending on if they had achieved significant effects (like pain intensity, interference, and catastrophizing) or if they could alter SyS results (age, biological sex, distance between first questionnaire and fMRI, and head motion during fMRI).
To explore the interaction between catastrophism’s helplessness and brain networks related to pain progression, we run moderation models through SPSS Process®, and we look for the Johnson-Neyman interval. Finally, to explore the possible effect of pain experience in interaction with catastrophism’s helplessness on brain connectivity we repeated the models using brain SyS as the dependent variable and pain experience as the independent variable.
Statistical analyses were performed using SPSS version 20.0 (Statistical Package for Social Sciences, Chicago, IL, USA). Regression models’ graphics were created through R v.3.6.3 (R Foundation for Statistical Computing, Vienna, Austria). Brain nodes and segregation graphic representation were created with the Surf Ice tool (version 6-October-2021; v1.0.20211006), which is an OpenGL Shading Language surface rendering source code.
When we compared the no pain and CP group for sociodemographic data and health-related questionnaires, we found significant differences in age (F = 6,271; p = 0.013), gender (x2 = 8.396; p = 0.003), BMI (F = 9,352; p = 0.002), MH (F = 24,772; p < 0.001), cognitive complaints (F = 31,945; p < 0.001), QoL (F = 40,392; p < 0.001) and head movement during the scan (F = 4,652; p = 0.032). CP group was composed predominantly of women (63.2%) and older people when compared with the no pain group (mean = 54.81; SD = 7.04) (detailed information is in Table 1).
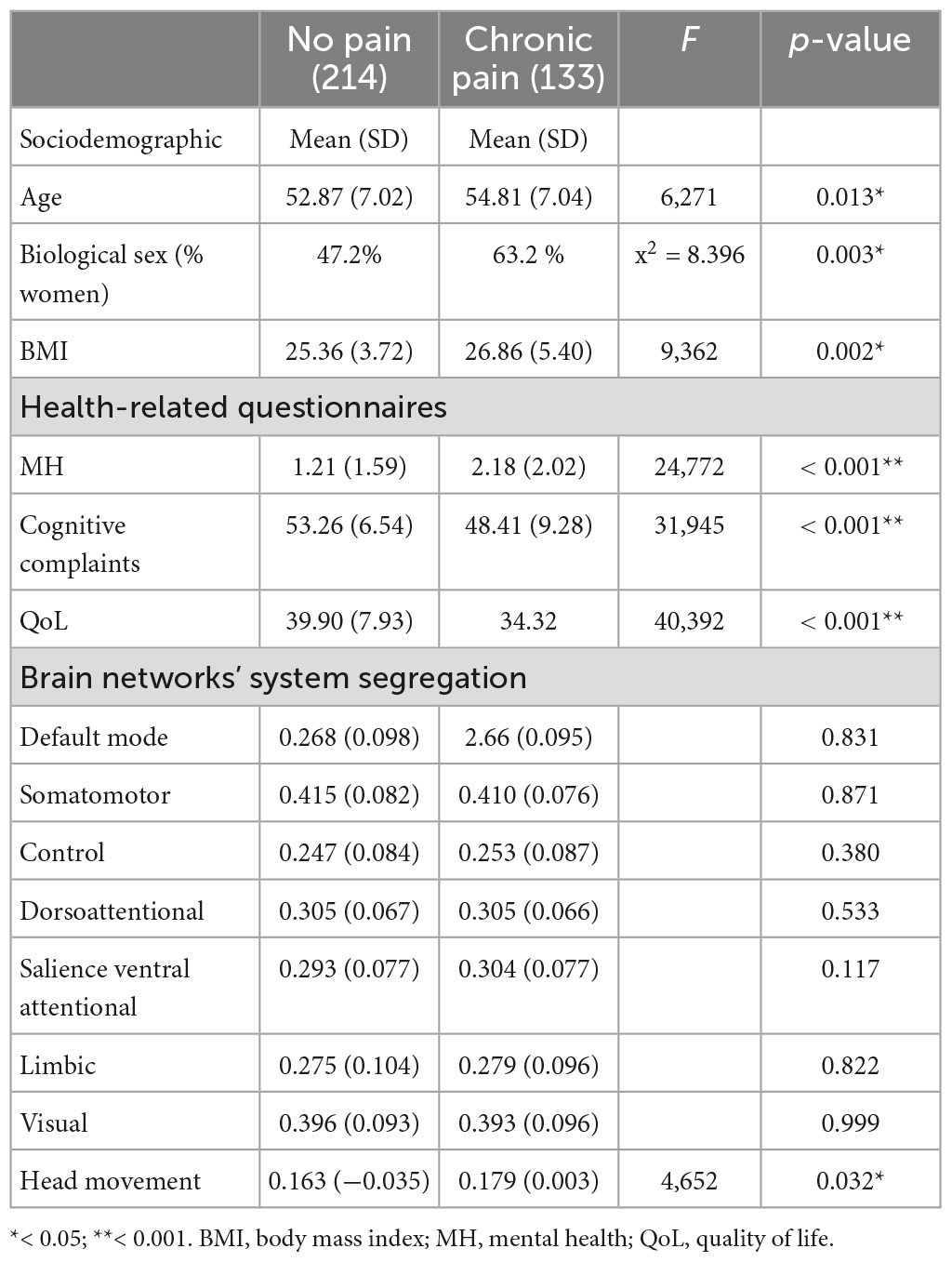
Table 1. Sociodemographic data and system network segregation differences between no pain and pain group.
Regarding SyS, the multivariate analysis (corrected by head movement, the time between the first questionnaire, biological sex, and age; see Table 1) showed no differences between groups in DMN (F = 0.046; p = 0.831), somatomotor network (F = 0.026; p = 0.871), control network (F = 0.772; p = 0.380), DAN (F = 0.390; p = 0.533), SN (F = 2.466; p = 0.117), limbic network (F = 0.050; p = 0.822) and visual network (F = 0.000; p = 0.999) (Table 1).
Quality of life significantly correlated with multiple pain sites (r = −0.243 p = 0.005), pain intensity (r = −0.282, p = 0.001) and interference (r = −0.521, p < 0.001), cognitive complaints (r = 0.398, p < .001), MH (r = −0.533, p < 0.001), rumination (r = −0.250, p = 0.004), magnification (r = −0.442, p < 0.001) and helplessness (r = −0.478, p < 0.001). No correlation was present between QoL and pain duration (r = −0.011, p = 0.900) or pain medication (r = −0.087, p = 0.321).
For MH, we found significant correlations with multiple pain sites (r = 0.184, p = 0.034), pain medication (r = 0.187, p = 0.031), pain intensity (r = 0.213, p = 0.014), pain interference (r = 0.371, p < 0.001), QoL, cognitive concerns (r = −0.423, p < 0.001), rumination (r = 0.288, p = 0.001), magnification (r = 0.471, p < 0.001) and helplessness (r = 0.422, p < 0.001). No correlation was found with pain duration.
Finally, cognitive complaints were positively correlated with multiple pain sites (r = −0.182, p = 0.038), MH, QoL, magnification (r = −0.222, p = 0.011), and helplessness (r = −0.191, p = 0.029).
Concerning SyS and pain factors (intensity, interference, and the number of pain sites) associations, we only found pain interference and SyS of DMN (r = 0.186, p = 0.034) and SN (r = 0.215, p = 0.014), and a tendency of an association with DAN (r = 0.161, p = 0.068).
Pain characteristics at baseline in our sample are drawn in Figure 4. The most common location was back pain (44.4%), followed by lower (24.8%) and upper limbs (12.8%). During the in-person assessment, participants with CP were asked if they had a diagnosis: 29 suffered from migraine, 15 from cervicalgia, 8 from fibromyalgia, 1 from polymyositis traumatic, 16 from knee pathologies, 54 from low back pain, 15 from other diagnoses that were cursing with CP and 36 had no specific diagnosis. Several participants had more than one diagnosis.
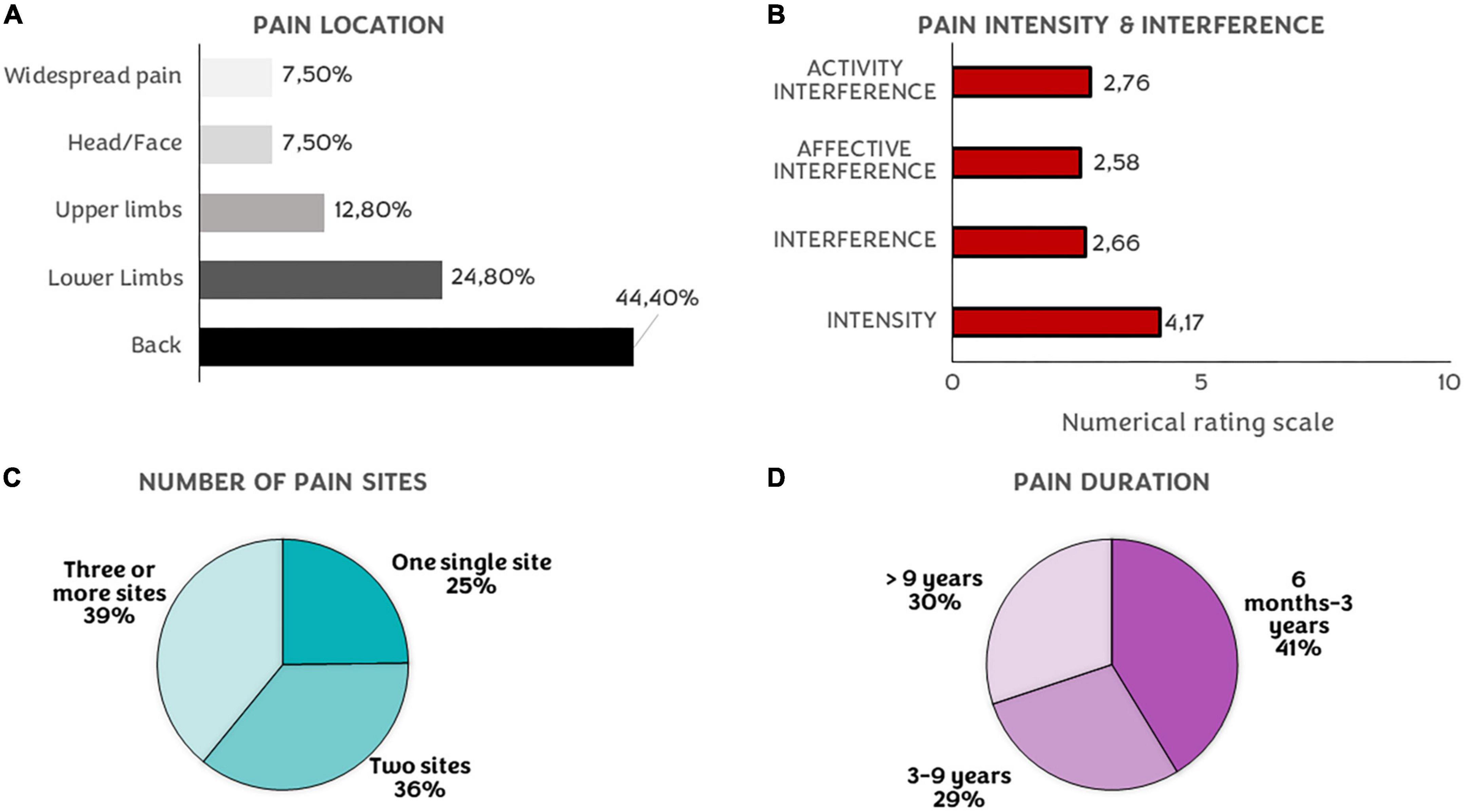
Figure 4. Pain characteristics. (A) Percentages of participants’ pain location. (B) Mean of interference (sum, activity, and affective) and intensity ratings on a numerical rating scale (0–10). (C) Percentages of the number of pain sites. (D) Pain duration of the CP in our sample.
Regarding the number of pain sites, in the first assessment, 75.2% of participants with CP had more than one single painful site and more than half of the sample had their pain for more than 3 years (58.7%). The total interference summed mean was 2.66 (SD = 2.21), 2.76 (SD = 2.36) in the activity subdomain, and 2.58 (SD = 2.39) in the affective subdomain. Finally, the mean intensity for the last week was 4.17 (SD = 1.47).
The pain-relief drugs were the most used treatment at baseline (31.6%), although 31.6% of participants were not enrolled in any kind of treatment at that moment. Finally, 32.3% of our sample treated their pain with other techniques, like physical or psychological therapies. The mean catastrophizing total score was 16.44 (SD = 8.65), helplessness 6.41 (SD = 4.19), rumination 6.44 (SD = 3.37), and magnification 3.60 (SD = 2.26).
When comparing two-time points (Table 2), we found significant differences in intensity (p = 0.004), interference (total, affective, and activity) (p = 0.021; p = 0.033; p = 0.047), and medication intake (p = 0.024). The number of pain sites and pain duration instead showed no differences (p = 0.800). Regarding the worsening or amelioration of pain intensity and affective interference, that is, what we considered as pain experience, 53.3% showed improvements during this period, and 47.7 % exhibited worsening symptoms.
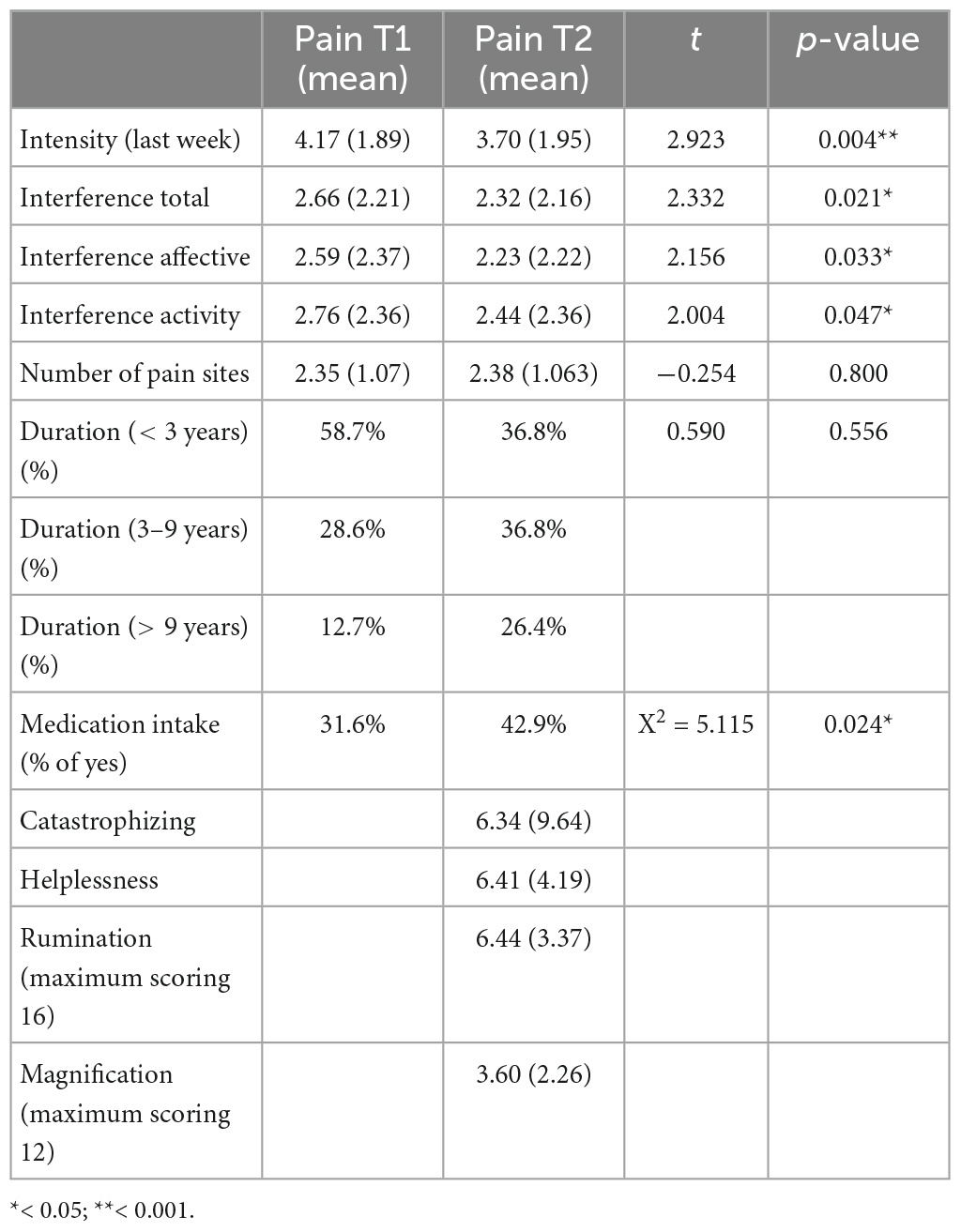
Table 2. Comparisons between pain variables in first and second questionnaires.
When we adjusted the first regression model, where all sociodemographic (BMI, age, and biological sex), health-related questionnaires (MH, QoL, and cognitive concerns), and pain characteristics (PC, pain medication, intensity, interference, duration, and the number of pain sites) were independent variables, we found that PC (β = 0.481; p < 0.001), pain intensity (β = −0.299; p = 0.002) and total interference (β = −0.562; p < 0.001) were associated with pain experience over time.
The second regression model crucially showed that more segregation of DMN (β = 0.193; p = 0.037), and less segregation in the DAN (β = −0.215; p = 0.014) were associated with worst pain experience progression. Moreover, activity and affective interference (β = 0.255; p = 0.022; β = −0.678; p < 0.001, respectively), pain intensity at baseline (β = −0.428; p < 0.001), and helplessness (β = 0.325; p < 0.003) were also related with worst pain experience progression.
Finally, when we explored the potential moderator role of helplessness on the relation between SyS and pain experience, we found that helplessness moderates the effect of DMN segregation on pain experience progression (p = 0.0313, 5,000 bootstrap samples, 95% CI 0.57–1.20), and a tendency in moderate the relation between DAN SyS (p = 0.098, 5,000 bootstrap samples, 95% CI −0.13–1.52) (see Figure 5) and pain experience progression. Johnson-Neyman plots revealed that a score of 7 in the helplessness subscale is the critical value to have a significant association between DMN segregation and pain experience progression (see Figure 6).
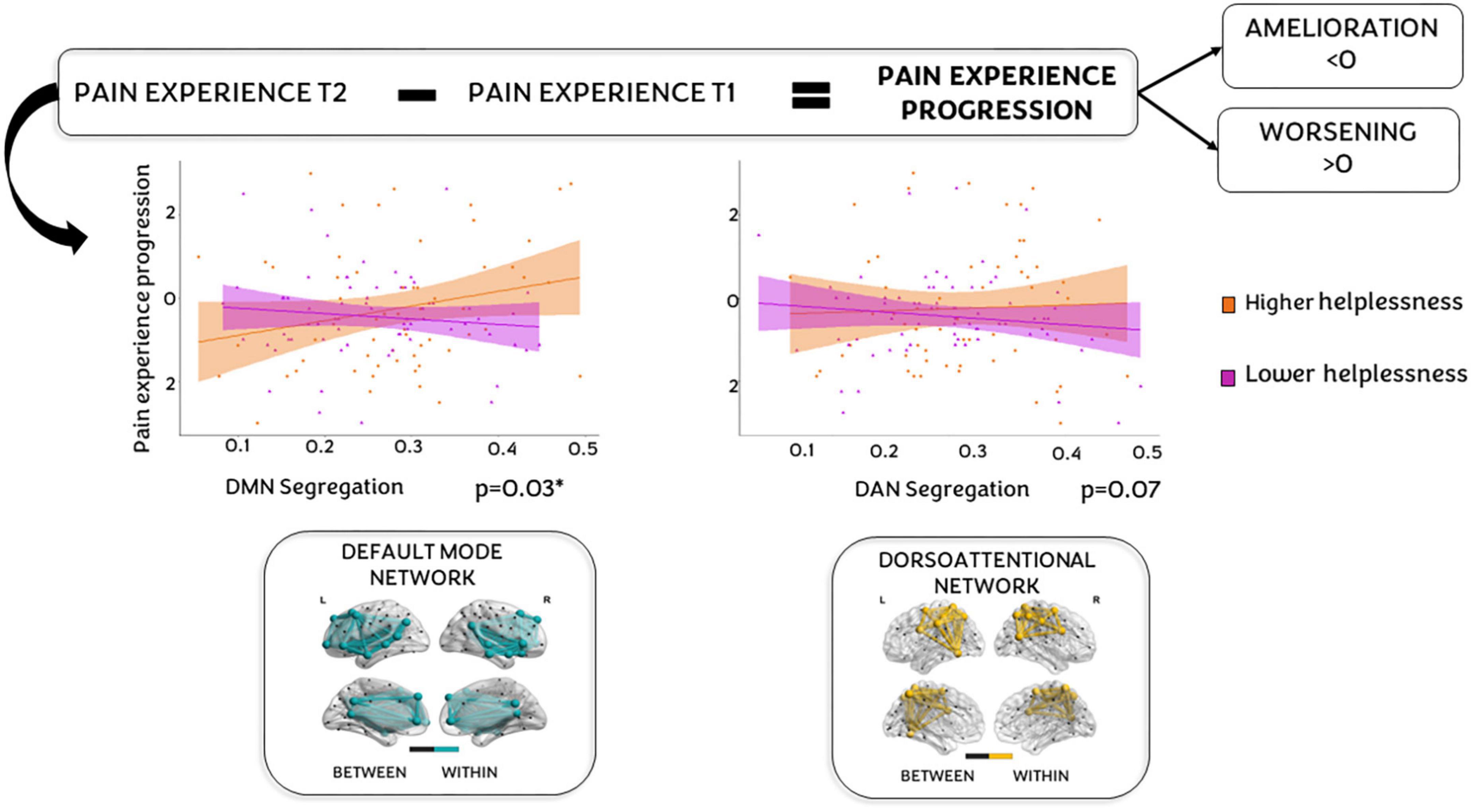
Figure 5. System segregation and helplessness predict chronic pain progression. On top, a chart explaining how pain progression has been calculated (subtracting pain experience T1 from pain experience T2). Positive values indicates a worsening while negative results an amelioration. In the middle, two scatter plots reflecting how each network [default mode network (DMN) at left and dorsoattentional network (DAN) at right] was associated with CP progression depending on low/high helplessness (violet, and orange, respectively). At the bottom of the figure, nodes in the graph represent studied regions of interest (ROIs) as defined by the Schaefer-Yeo atlas of 100 nodes and 7 networks. The nodes and edges illustrate ROIs blue for DMN (left) and yellow for DAN (right). Within network connectivity is represented in black (only representative) and refers to outside network ROIs and the connectivity between them and the DAN or DMN.
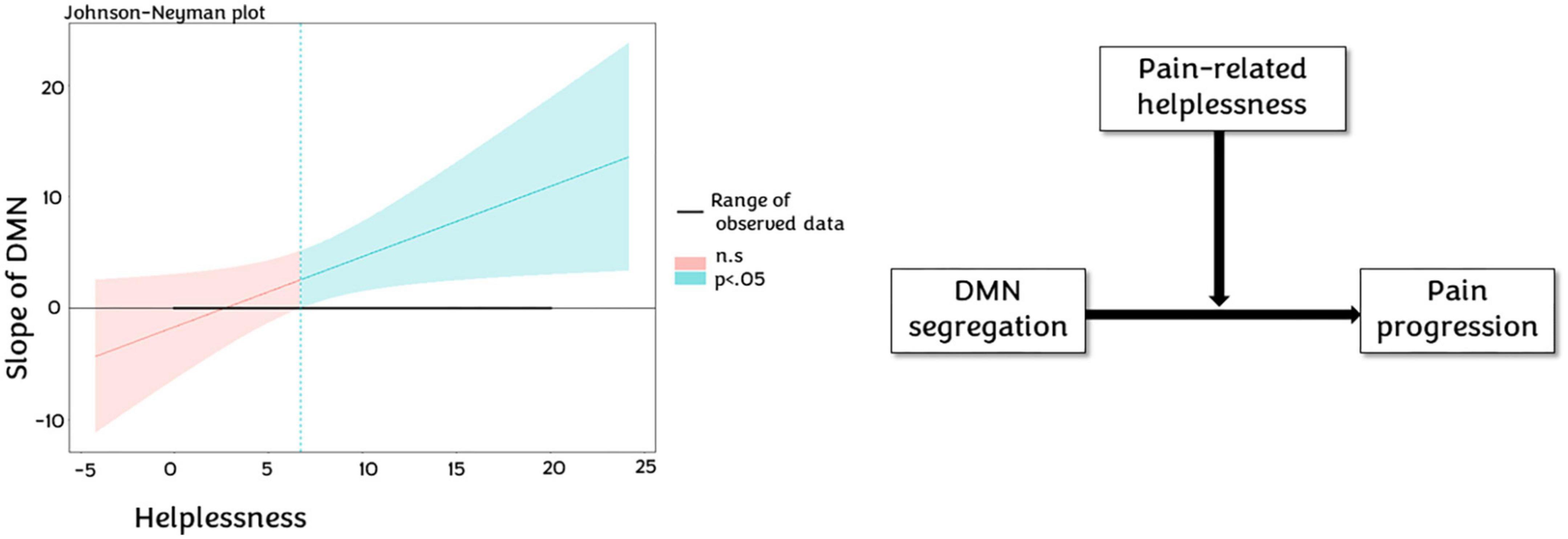
Figure 6. Helplessness moderation. At the left, Johnson-Neyman plot show how helplessness moderates the default mode network (DMN) slope since the score 6, where it accentuates the impact of DMN segregation on CP progression. At the right, representative chart of moderation of pain helplessness in the relationship between DMN segregation and pain progression.
When we swap the dependent and independent variables to explore catastrophism’s helplessness, in interaction with pain experience, and modulated brain SyS, we found no significant associations.
In this paper, we explored the role of SyS and psychological aspects in the evolution of pain experience over time. First, significant differences in self-perceived health status were found between the pain and no pain groups. Second, PC and brain network segregation of DMN and DAN were the main predictors of pain progression. Finally, moderation analyses revealed that helplessness, a PC’s subdomain, moderated the relationship between DMN and the progression of the pain experience. To our knowledge, this is the first study using the fMRI SyS model to identify biomarkers that can predict the progression of CP.
When we compared participants with and without CP, we found a high prevalence of CP (38.3%) in our sample, according to previous reports of a peak prevalence in late middle-aged adults (50–65 years), affecting up to 20–80% of people (Gibson and Lussier, 2012). The pain group was older, formed predominantly by women, and had an average BMI in the overweight range (bordering on mild obesity), also showing the worst health status (MH, cognition, QoL). This is in line with previous studies that found an association between overweight/obesity and low back pain, particularly stronger in women than men (Breivik et al., 2006; Stone and Broderick, 2012; Dahlhamer, 2018). Another difference observed was an increased head motion during the scan for the pain group, possibly related to an increased difficulty to keep still due to their condition.
We did not observe differences in SyS in any network, probably due to the non-clinical characteristics of our pain sample (i.e., low disability or low impact in their daily lives, low to mild fluctuations in pain intensity, and well-controlled pain).
We found several correlations between pain factors and psychological variables (QoL, MH, and self-perceived cognitive complaints), as has been widely described in pain literature (Edwards et al., 2016; Kawai et al., 2017). The subjective and prolonged experience of pain in our cohort was associated with significant mood consequences, such as light depressive symptoms and less capacity to enjoy life. Unquestionably, feeling pain may evolve from normal reactive emotional symptoms, related to stress (Hammen, 2005; Abdallah and Geha, 2017), to clinically relevant depression associated with CP (DeVeaugh-Geiss et al., 2010). Increasing evidence suggests that the pain-related plasticity and depression-related neural circuits are responsible for subtle changes in areas involved in the emotional and cognitive aspects of pain over time that contributes to the behavioral manifestation of altered affective processes (Doan et al., 2015). Finally, as will be discussed later, PC is an important risk factor for a wide range of pain-related effects, including increased pain intensity, increased emotional distress, depression, decreased physical function, and prolonged disability (Schütze et al., 2018).
Our results indicated that changes in pain experience over time were associated with higher levels of PC and, helplessness was the only domain that vaticinated greater pain impact.
Pain catastrophizing is defined as “an exaggerated negative mental set brought to bear during actual or anticipated painful experience” (Sullivan et al., 2001), and can be divided into three main dimensions: magnification (an exaggerated threat value of pain), rumination (excessive focus pain-related stimuli) and helplessness.
Sullivan (Sullivan, 2012) described how magnification and rumination could overlap with features from primary appraisals (i.e., evaluating the pain stimulus), while helplessness overlaps with secondary appraisal (i.e., the evaluation of oneself to effectively deal with a stressful situation, like pain stimulus). Consequently, cognitions of helplessness are related to higher perceived pain intensity, possibly due to feelings of loss of control, negative future expectations, or rumination, factors that enhance affective pain experience (Müller, 2011).
Pain catastrophizing is related not only to psychological factors but also to altered brain connectivity in pain-related areas and top-down inhibition mechanisms [e.g., a reduced engagement of the descending pain modulatory system; see Malfliet et al. (2017) for review]. Rumination in PC can be considered as a cognitive style (“mind-wandering like”) (Èeko et al., 2015), and is responsible for the occurrence of thoughts not related to a given task and not tied to the immediate environment (Häggman-Henrikson et al., 2021). In general terms, a rumination is a form of circular thinking that swallows the individual in a path without a way out, and it can be broadly defined as a perseverative self-focused thinking process, whereby an individual goes over and over the same thoughts in his or her mind. This process, which can be activated during or after a painful event, generally interferes with a person’s ability to inhibit thoughts, generate alternative ways of thinking, and switch the focus of attention. PC, which possibly appears as a kind of fear of pain, helps perpetuate the cognitive-behavioral pain cycle, collaborating in the activation of negative cognitive and meta-cognitive processes, that in turn can lead to worse coping behaviors and an exacerbation of pain (Ziadni et al., 2018).
This is consistent with previous studies focused on cognitive-affective processes of pain (Gentili et al., 2019; Gonzalez et al., 2019; You et al., 2021). You et al. (2021) demonstrated the existence of pain-specific resilience, referring to the ability to maintain relatively stable and healthy levels of psychological functioning in face of ongoing and persistent pain (You et al., 2021). Sociodemographic (Tanner et al., 2021), structural and functional MRI (Tanner et al., 2021; You et al., 2021), clinical pain symptoms, negative pain-related emotions, and PC (Sturgeon and Zautra, 2013; Gonzalez et al., 2019) have been related to resilience and better outcomes in the presence of recurrent pain, while to our knowledge, this is the first study to explore the interaction between all these variables.
We found associations between pain interference and DMN, and SN, as well as a significant tendency in DAN. One important point, that distinguishes our results from other studies, is that higher segregation of DMN and lower segregation of DAN were associated with this pain experience evolution over time, which is coherent and match with previous results. Besides, helplessness was found to moderate the relationship between DMN and pain experience progression. When we explore the role of the interaction between helplessness and pain experience on brain SyS we found no significant effects, suggesting that brain SyS in certain networks, in interaction with helplessness, affects pain experience evolution over time, and not the reverse.
In this section, we aim to address all the points by substantially revising the main findings on each network individually and collectively, as well as their relationship with helplessness.
First, concerning DAN, its alteration has already been shown to predict pain intensity progression, possibly due to a cognitive evaluation of pain as a permanent threat to the body (Pfannmöller and Lotze, 2019). In this view, our results could be interpreted as dysregulated DAN internal and external connectivity could reduce the ability to correctly process nociceptive stimuli and, consequently, increase the perception of pain intensity over time. Thus, it could be possible that an imbalance in FC between networks causes a sort of “attentional resources kidnapping,” increasing the aversive response to pain. This constant painful input and its maladaptive brain changes (i.e., malfunction of the descending pain pathways), reinforced by catastrophic thoughts, ultimately provoke an increase in self-perceived pain intensity over time.
Similarly, we found a correlation between pain interference and SN segregation, suggesting that, as DAN, altered response in this network could be a contributing factor to the maintenance and chronicity of pain. SN also exhibits task- and resting-state abnormalities in some CP populations (Otti et al., 2013; Becerra et al., 2014; Cauda et al., 2014; Qiu et al., 2021), and may be dysregulated due to constant pain (Borsook et al., 2013), giving rise to a “salient state,” mostly divided into two processes: bottom-up saliency and top-down control (Melloni et al., 2012). Nonetheless, it is well justified that there is an association between a dysregulated SN and the interplay between pain symptoms and psychological aspects, as several studies have also seen before (Legrain et al., 2011; Coppieters et al., 2016; van Ettinger-Veenstra et al., 2019). Indeed, the function of the SN is essential in the processing of sensory stimuli, as the SN plays a key role in the assessment of the inherent danger of such stimuli (and how one should respond to them), and plays a central role in the memory of painful events (Kim et al., 2019).
In the same line DMN alteration in CP patients (Malfliet et al., 2017) has been associated with the “pain state” (Èeko et al., 2020), which facilitates stimulus-independent thoughts, or internally directed, spontaneous or autobiographical thoughts, also resumed in the term “self-generated thought” (Andrews-Hanna et al., 2014). Repetitive negative thinking is considered a form of avoidant coping strategy (Flink et al., 2013). Occupying one’s thoughts with repetitive negative thinking prevents the confrontation with the threat (e.g., What I could have done to prevent this situation?). Additionally, repetitive negative thinking can be negatively reinforced by abstract cognitive activity (e.g., Why do I suffer from pain?). This form of abstract thinking impedes the activation and processing of emotional and somatic responses. The process of suppression/avoidance could magnify the negative emotions and consequently fuel the catastrophic worry cycle. Usually, some of these thoughts are related to personal significance, temporal or social orientation, or somatosensory awareness. Ergo, DMN seems to play an important active role in the self-generation of cognition, thinking about one-self and future thinking, but also with rumination and PC (Èeko et al., 2020).
The predictive value of DMN rs-FC on pain management was already shown by Baliki et al. (2014), where CP disrupted the dynamics of DMN and frontoparietal network (related to attention and working memory), and other regions related to pain modulation (insula; anterior cingulate cortex, ACC) (Baliki et al., 2014). Specific nodes of DMN, like the hippocampus and medial prefrontal cortex (mPFC), are importantly implicated in pain processing. Similarly, Kucyi et al. (2014) demonstrated an enhanced mPFC connectivity in DMN, suggesting its role in the descending modulatory system underlying the degree to which patients ruminate about their CP (Kucyi et al., 2014). Hashmi et al. (2013) also found that strengthening mPFC-nucleus accumbens FC predicts the extension in which brain activity shifts from pain-related to emotion-related regions in patients with persistent subacute back pain, compared to those that get total recovery (Hashmi et al., 2013). In sum, the mPFC can be seen as a hub for the development of mental comorbidities associated with CP. The impaired cholinergic activity contributes to the deactivation of mPFC, possibly leading to cognitive and emotional deficits in CP patients (Kummer et al., 2020).
Overall, our results are consistent with findings reported by Ter Minassian et al. (2012) in their study about brain activity during pain anticipation and pain perception (Ter Minassian et al., 2012). They found that during pain anticipation, DAN was activated while DMN was deactivated, possibly due to the search for strategies to avoid pain. In contrast, during pain perception, DMN was reactivated, whereas DAN remained activated, supporting the fact that DMN and attentional networks cooperate to integrate pain-related stimuli and thoughts, as DMN is at the top of the networks that perform hierarchical integration. The authors concluded that the ACC could be the structure most involved in the coordination between these two networks, given that it can be anatomically and functionally divided during pain anticipation (cognitive; caudal ACC) and pain perception (emotional; rostral ACC).
Our results indicate that brain network functioning and cognitive-emotional strategies can interact in modulating pain experience, and both can be understood as possible protectors/risk factors.
Once CP is established, catastrophizing and segregation are not independent factors acting in the pain progression. Segregation of DMN and DAN, indeed, may represent some aspects of brain resilience that could help to maintain or get better from pain, allowing the brain to effectively process pain, or at least avoid areas not involved in pain processing. On the other hand, modifiable psychologic aspects like catastrophizing, related to cognitive reserve, may have a crucial role in pain evolution and the impact of MH. Both kinds of processes can be treated separately but in a coordinated way, as seen in studies of combined behavioral therapies (e.g., pain neuroscience education) with brain stimulation (Meeker et al., 2020; Alcon and Wang-Price, 2022), and could reduce the negative impact of emotions in the evolution of pain over time, collaborating in the selection of effective coping strategies or avoiding negative thinking. Thereby, descending modulation might be more effective, decreasing levels of pain intensity and affective interference. Finally, resilience-focused cognitive-affective approaches, including this holistic view, are important to be applied not only in highly affected CP patients, but also in individuals with a low rating in pain parameters, as they can already show lower QoL, cognition, and MH, or FC alterations.
Our main limitation was that we investigated a non-homogeneous (e.g., different kinds of pain) and non-clinical sample (low ratings in pain intensity, interference, and PC). Thus, in future work, investigating how higher catastrophizing scores, as well as intensity or interference ratings, interact with networks’ segregation in the progression of pain might shed light on how pain alters different networks and how it’s linked to emotional and cognitive aspects.
Another limitation of our study was the lack of information about pain during MRI or the presence of acute pain in the no-pain sample. Further work is certainly required to disentangle these complexities in acute (non-experimentally provoked) and CP. For example, the possibility of prognostic biomarkers of the transition from acute pain to CP, within the framework of pain-related resilience (SyS and psychological factors) is described in this manuscript.
An additional potential limitation was related to time gaps between questionnaires and MRI. Even though we used this gap as a covariable in our analysis, we cannot exclude that this aspect can introduce some bias in the results.
Although we excluded subjects with excess motion and added the mean head motion of each participant as a covariate in all the analyses related to fMRI, we cannot fully dismiss that subject motion to some degree has influenced the present results.
Finally, due to the exploratory nature of our analyses, we did not correct functional connectivity analysis for multiple comparisons.
Future studies need to confirm these results with better controlling for all these aspects and overcome present limitations.
In summary, present results indicate that non-clinical CP conditions are associated with the segregation of brain networks during rs-fMRI, more concretely SN, DAN, and DMN. Moreover, the latter effect is moderated by helplessness, a catastrophizing domain, that can be seen as a protective factor against pain impact over time.
Our result casts a new light on the interplay among the influence of the interaction between psychological aspects and brain networks in pain management. The extent of the reorganization of these networks and their functioning is critical for the evolution of pain.
Besides, the reorganization of spatial properties of the DMN, DAN, and SN may reflect different emotional, attentional, and cognitive abnormalities observed in CP conditions. Under certain assumptions, this can be construed as the common reorganization among pain patients is the extent of association of the component of the DAN, and its dissociation from the posterior components of the DMN, which seems to disrupt the competitive inhibition between the DMN and the brain networks underlying attention.
Finally, our results highlight the predictive value of fMRI that can orient researchers and clinicians about what form of treatable pathophysiology an individual patient with CP may have. Given that other fMRI techniques are not suitable to measure certain characteristics, such as the effect of attentional fluctuation or the degree of self-generated thoughts, we conclude that SyS networks are an effective metric to understand brain connectivity and neural correlates of the pain state. SyS could be used as biomarkers indicating a predisposition of pain maintenance and allowing disease progression monitoring, as well as the reversion or compensation of these alterations in different kinds of interventions, that should, in the future, be considered for more deep research. We have demonstrated that these variables should be assessed without considering the etiology of pain, giving more importance to the pain state than the pain condition per se.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The protocol was approved by the “Comité d’Ètica i Investigació Clínica de la Unió Catalana d’Hospitals” and was carried out following the Declaration of Helsinki (World Medical Association, 2013). Written informed consent was obtained from all participants before inclusion in the study.
MDS, GC, GE-I, AR-V, MC-T, KA-P, JS-S, AP-L, DB-F, JMT, and SD-G have made substantial contributions to conception, design, and interpretation of data. GC, MDS, and SD-G have made substantial contributions to analysis and interpretation of data. GE-I, AR-V, MC-T, KA-P, JS-S, and SD-G have made substantial contribution to acquisition of data. MDS, GC, and SD-G participated in drafting the manuscript. AP-L, DB-F, JMT, GE-I, AR-V, MC-T, KA-P, and JS-S contributed to revising it critically for important intellectual content. All authors have given final approval of the version to be submitted.
This research has received funding from La Caixa Foundation (grant number LCF/PR/PR16/11110004), Institut Guttmann, and Fundació Abertis. AP-L was partially supported by Fundació La Marató De TV3 (202129-30-31). DB-F was supported in part by the Spanish Ministry of Science, Innovation and Universities (MICIU/FEDER; grant number RTI2018-095181-B-C21) and the Catalan Institute for Advanced Research and Studies Academia 2019 grant award and Fundació La Marató De TV3 (202129-30-31). JMT was partly supported by the Fundació Joan Ribas Araquistain_Fjra (PREHABILITA-IUN91752), Agency for Management of University and Research Grants, Agència de Gestió d’Ajuts Universitaris i de Recerca (2018 PROD 00172), and the European Commission (call H2020-SC1-2016-2017_RIA_777107). GC was partly supported by the Fundació La Marató De TV3 (202211-30-31). KA-P was financially supported by a Juan de la Cierva-Formación research grant (FJC2021-047380-I) of the Spanish Ministry of Science and Innovation.
Special thanks are extended to all participants, the project team and research assistants, and other partners (Ad-Salutem Institute, Sodexo, I.C.A. Informàtica y Comunicaciones Avanzadas, Neuroelectrics, Corporació Catalana de Mitjans Audiovisuals, Club Metropolitan, Casa Ametller, and Agència de Qualitat i Avaluació Sanitàries de Catalunya-AQuAS) for their invaluable collaboration.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
AP-L received funding from MagStim Inc. The funder was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit It for publication.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abdallah, C. G., and Geha, P. (2017). Chronic pain and chronic stress: two sides of the same coin? Chronic Stress 1:2470547017704763. doi: 10.1177/2470547017704763
Abeler, K., Friborg, O., Engstrøm, M., Sand, T., and Bergvik, S. (2020). Sleep characteristics in adults with and without chronic musculoskeletal pain: the role of mental distress and pain catastrophizing. Clin. J. Pain 36, 707–715. doi: 10.1097/AJP.0000000000000854
Alcon, C. A., and Wang-Price, S. (2022). Non-invasive brain stimulation and pain neuroscience education in the cognitive-affective treatment of chronic low back pain: evidence and future directions. Front. Pain Res. 3:959609. doi: 10.3389/fpain.2022.959609
Andrews-Hanna, J. R., Smallwood, J., and Spreng, R. N. (2014). The default network and self-generated thought: component processes, dynamic control, and clinical relevance. Ann. N. Y. Acad. Sci. 1316, 29–52. doi: 10.1111/nyas.12360
Badia, X., Muriel, C., Gracia, A., Manuel Núñez-Olarte, J., Perulero, N., Gálvez, R., et al. (2003). Validación española del cuestionario brief pain inventory en pacientes con dolor de causa neoplásica. Med. Clín. 120, 52–59. doi: 10.1016/S0025-7753(03)73601-X
Baliki, M. N., Mansour, A. R., Baria, A. T., and Apkarian, A. V. (2014). Functional reorganization of the default mode network across chronic pain conditions. PLoS One 9:e106133. doi: 10.1371/journal.pone.0106133
Becerra, L., Sava, S., Simons, L. E., Drosos, A. M., Sethna, N., Berde, C., et al. (2014). Intrinsic brain networks normalize with treatment in pediatric complex regional pain syndrome. Neuroimage Clin. 6, 347–369. doi: 10.1016/j.nicl.2014.07.012
Borsook, D., Edwards, R., Elman, I., Becerra, L., and Levine, J. (2013). Pain and analgesia: the value of salience circuits. Prog. Neurobiol. 104, 93–105. doi: 10.1016/j.pneurobio.2013.02.003
Breivik, H., Collett, B., Ventafridda, V., Cohen, R., and Gallacher, D. (2006). Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur. J. Pain 10, 287–333. doi: 10.1016/j.ejpain.2005.06.009
Burns, L. C., Ritvo, S. E., Ferguson, M. K., Clarke, H., Seltzer, Z., and Katz, J. (2015). Pain catastrophizing as a risk factor for chronic pain after total knee arthroplasty: a systematic review. J. Pain Res. 8, 21–32. doi: 10.2147/JPR.S64730
Cattaneo, G., Bartrés-Faz, D., Morris, T. P., Sánchez, J. S., Macià, D., Tarrero, C., et al. (2018). The barcelona brain health initiative: a cohort study to define and promote determinants of brain health. Front. Aging Neurosci. 10:321. doi: 10.3389/fnagi.2018.00321
Cattaneo, G., Bartrés-Faz, D., Morris, T. P., Sánchez, J. S., Macià, D., Tormos, J. M., et al. (2020). The barcelona brain health initiative: cohort description and first follow-up. PLoS one 15:e0228754. doi: 10.1371/journal.pone.0228754
Cauda, F., Palermo, S., Costa, T., Torta, R., Duca, S., Vercelli, U., et al. (2014). Gray matter alterations in chronic pain: a network-oriented meta-analytic approach. Neuroimage Clin. 4, 676–686. doi: 10.1016/j.nicl.2014.04.007
Èeko, M., Frangos, E., Gracely, J., Richards, E., Wang, B., Schweinhardt, P., et al. (2020). Default mode network changes in fibromyalgia patients are largely dependent on current clinical pain. NeuroImage 216:116877. doi: 10.1016/j.neuroimage.2020.116877
Èeko, M., Gracely, J. L., Fitzcharles, M.-A., Seminowicz, D. A., Schweinhardt, P., and Bushnell, M. C. (2015). Is a responsive default mode network required for successful working memory task performance? J. Neurosci. 35, 11595–11605. doi: 10.1523/JNEUROSCI.0264-15.2015
Cleeland, C. S. (2009). The M. D. Anderson symptom inventory. User guide-version 1. Available online at: https://www.mdanderson.org/documents/Departments-and-Divisions/Symptom-Research/MDASI_userguide.pdf
Coppieters, I., Meeus, M., Kregel, J., Caeyenberghs, K., De Pauw, R., Goubert, D., et al. (2016). Relations between brain alterations and clinical pain measures in chronic musculoskeletal pain: a systematic review. J. Pain 17, 949–962. doi: 10.1016/j.jpain.2016.04.005
Coppola, G., Di Renzo, A., Petolicchio, B., Tinelli, E., Di Lorenzo, C., Parisi, V., et al. (2019). Aberrant interactions of cortical networks in chronic migraine: a resting-state fMRI study. Neurology 92, e2550–e2558. doi: 10.1212/WNL.0000000000007577
Craner, J. R., Gilliam, W. P., and Sperry, J. A. (2016). Rumination, magnification, and helplessness: how do different aspects of pain catastrophizing relate to pain severity and functioning? Clin. J. Pain 32, 1028–1035. doi: 10.1097/AJP.0000000000000355
Dahlhamer, J. (2018). Prevalence of chronic pain and high-impact chronic pain among adults — United States, 2016. MMWR Morb Mortal Wkly Rep. 67, 1001–1006. doi: 10.15585/mmwr.mm6736a2
De Ridder, D., Vanneste, S., Smith, M., and Adhia, D. (2022). Pain and the triple network model. Front. Neurol. 13:757241. doi: 10.3389/fneur.2022.757241
Delgado-Gallén, S., Soler, M. D., Albu, S., Pachón-García, C., Alviárez-Schulze, V., Solana-Sánchez, J., et al. (2021). Cognitive reserve as a protective factor of mental health in middle-aged adults affected by chronic pain. Front. Psychol. 12:4557. doi: 10.3389/fpsyg.2021.752623
DeVeaugh-Geiss, A. M., West, S. L., Miller, W. C., Sleath, B., Gaynes, B. N., and Kroenke, K. (2010). The adverse effects of comorbid pain on depression outcomes in primary care patients: results from the ARTIST trial. Pain Med. 11, 732–741. doi: 10.1111/j.1526-4637.2010.00830.x
Doan, L., Manders, T., and Wang, J. (2015). Neuroplasticity underlying the comorbidity of pain and depression. Neural Plast. 2015:504691. doi: 10.1155/2015/504691
Dong, H.-J., Gerdle, B., Bernfort, L., Levin, L. -Å, and Dragioti, E. (2020). Pain catastrophizing in older adults with chronic pain: the mediator effect of mood using a path analysis approach. J. Clin. Med. 9:2073 doi: 10.3390/jcm9072073
Edwards, R. R., Dworkin, R. H., Sullivan, M. D., Turk, D. C., and Wasan, A. D. (2016). The role of psychosocial processes in the development and maintenance of chronic pain. J. Pain 17, T70–T92. doi: 10.1016/j.jpain.2016.01.001
Ewers, M., Luan, Y., Frontzkowski, L., Neitzel, J., Rubinski, A., Dichgans, M., et al. (2021). Segregation of functional networks is associated with cognitive resilience in Alzheimer’s disease. Brain 144, 2176–2185. doi: 10.1093/brain/awab112
Fieo, R., Ocepek-Welikson, K., Kleinman, M., Eimicke, J. P., Crane, P. K., Cella, D., et al. (2016). Measurement equivalence of the patient reported outcomes measurement information system® (PROMIS®) applied cognition – general concerns, short forms in ethnically diverse groups. Psychol. Test Assess Model. 58, 255–307.
Fischl, B., Salat, D. H., Busa, E., Albert, M., Dieterich, M., Haselgrove, C., et al. (2002). Whole brain segmentation: automated labeling of neuroanatomical structures in the human brain. Neuron 33, 341–355. doi: 10.1016/S0896-6273(02)00569-X
Flink, I. L., Boersma, K., and Linton, S. J. (2013). Pain catastrophizing as repetitive negative thinking: a development of the conceptualization. Cogn. Behav. Ther. 42, 215–223. doi: 10.1080/16506073.2013.769621
Franzmeier, N., Göttler, J., Grimmer, T., Drzezga, A., Áraque-Caballero, M. A., Simon-Vermot, L., et al. (2017). Resting-state connectivity of the left frontal cortex to the default mode and dorsal attention network supports reserve in mild cognitive impairment. Front. Aging Neurosci. 9:264. doi: 10.3389/fnagi.2017.00264
García Campayo, J., Rodero, B., Alda, M., Sobradiel, N., Montero, J., and Moreno, S. (2008). [Validation of the Spanish version of the pain catastrophizing scale in fibromyalgia]. Med. Clin. 131, 487–492. doi: 10.1157/13127277
Gentili, C., Rickardsson, J., Zetterqvist, V., Simons, L. E., Lekander, M., and Wicksell, R. K. (2019). Psychological flexibility as a resilience factor in individuals with chronic pain. Front. Psychol. 10:2016. doi: 10.3389/fpsyg.2019.02016
Gibson, S. J., and Lussier, D. (2012). Prevalence and relevance of pain in older persons. Pain Med. 13, S23–S26. doi: 10.1111/j.1526-4637.2012.01349.x
Gilliam, W. P., Craner, J. R., Morrison, E. J., and Sperry, J. A. (2017). The mediating effects of the different dimensions of pain catastrophizing on outcomes in an interdisciplinary pain rehabilitation program. Clin. J. Pain 33, 443–451. doi: 10.1097/AJP.0000000000000419
Gonzalez, C. E., Okunbor, J. I., Parker, R., Owens, M. A., White, D. M., Merlin, J. S., et al. (2019). Pain-specific resilience in people living with HIV and chronic pain: beneficial associations with coping strategies and catastrophizing. Front. Psychol. 10:2046. doi: 10.3389/fpsyg.2019.02046
Haefeli, M., and Elfering, A. (2006). Pain assessment. Eur. Spine J. 15, S17–S24. doi: 10.1007/s00586-005-1044-x
Häggman-Henrikson, B., Visscher, C. M., Wänman, A., Ljótsson, B., Peck, C. C., and Lövgren, A. (2021). Even mild catastrophic thinking is related to pain intensity in individuals with painful temporomandibular disorders. J. Oral Rehabil. 48, 1193–1200. doi: 10.1111/joor.13251
Hammen, C. (2005). Stress and depression. Annu. Rev. Clin. Psychol. 1, 293–319. doi: 10.1146/annurev.clinpsy.1.102803.143938
Hashmi, J. A., Baliki, M. N., Huang, L., Baria, A. T., Torbey, S., Hermann, K. M., et al. (2013). Shape shifting pain: chronification of back pain shifts brain representation from nociceptive to emotional circuits. Brain 136, 2751–2768. doi: 10.1093/brain/awt211
Hemington, K. S., Wu, Q., Kucyi, A., Inman, R. D., and Davis, K. D. (2016). Abnormal cross-network functional connectivity in chronic pain and its association with clinical symptoms. Brain Struct. Funct. 221, 4203–4219. doi: 10.1007/s00429-015-1161-1
Jensen, M. P., Tomé-Pires, C., de la Vega, R., Galán, S., Solé, E., and Miró, J. (2017). What determines whether a pain is rated as mild, moderate, or severe? the importance of pain beliefs and pain interference. Clin. J. Pain 33, 414–421. doi: 10.1097/AJP.0000000000000429
Jones, S. A., Morales, A. M., Holley, A. L., Wilson, A. C., and Nagel, B. J. (2020). Default mode network connectivity is related to pain frequency and intensity in adolescents. Neuroimage Clin. 27:102326. doi: 10.1016/j.nicl.2020.102326
Kastrati, G., Thompson, W. H., Schiffler, B., Fransson, P., and Jensen, K. B. (2022). Brain network segregation and integration during painful thermal stimulation. Cereb. Cortex 32, 4039–4049. doi: 10.1093/cercor/bhab464
Kawai, K., Kawai, A. T., Wollan, P., and Yawn, B. P. (2017). Adverse impacts of chronic pain on health-related quality of life, work productivity, depression and anxiety in a community-based study. Fam. Pract. 34, 656–661. doi: 10.1093/fampra/cmx034
Keller, S., Bann, C. M., Dodd, S. L., Schein, J., Mendoza, T. R., and Cleeland, C. S. (2004). Validity of the brief pain inventory for use in documenting the outcomes of patients with noncancer pain. Clin. J. Pain 20, 309–318. doi: 10.1097/00002508-200409000-00005
Kilpatrick, L. A., Istrin, J. J., Gupta, A., Naliboff, B., Tillisch, K., Labus, J. S., et al. (2015). Sex commonalities and differences in the relationship between resilient personality and the intrinsic connectivity of the salience and default mode networks. Biol. Psychol. 112, 107–115. doi: 10.1016/j.biopsycho.2015.09.010
Kim, J., Mawla, I., Kong, J., Lee, J., Gerber, J., Ortiz, A., et al. (2019). Somatotopically specific primary somatosensory connectivity to salience and default mode networks encodes clinical pain. Pain 160, 1594–1605. doi: 10.1097/j.pain.0000000000001541
Kocalevent, R.-D., Finck, C., Jimenez-Leal, W., Sautier, L., and Hinz, A. (2014). Standardization of the Colombian version of the PHQ-4 in the general population. BMC Psychiatry 14:205. doi: 10.1186/1471-244X-14-205
Kucyi, A., Moayedi, M., Weissman-Fogel, I., Goldberg, M. B., Freeman, B. V., Tenenbaum, H. C., et al. (2014). Enhanced medial prefrontal-default mode network functional connectivity in chronic pain and its association with pain rumination. J. Neurosci. 34, 3969–3975. doi: 10.1523/JNEUROSCI.5055-13.2014
Kummer, K. K., Mitriæ, M., Kalpachidou, T., and Kress, M. (2020). The medial prefrontal cortex as a central hub for mental comorbidities associated with chronic pain. Int. J. Mol. Sci. 21, E3440. doi: 10.3390/ijms21103440
Lee, J.-J., Lee, S., Lee, D. H., and Woo, C.-W. (2022). Functional brain reconfiguration during sustained pain. eLife 11:e74463. doi: 10.7554/eLife.74463
Legrain, V., Damme, S. V., Eccleston, C., Davis, K. D., Seminowicz, D. A., and Crombez, G. (2009). A neurocognitive model of attention to pain: behavioral and neuroimaging evidence. Pain 144, 230–232. doi: 10.1016/j.pain.2009.03.020
Legrain, V., Iannetti, G. D., Plaghki, L., and Mouraux, A. (2011). The pain matrix reloaded: a salience detection system for the body. Prog. Neurobiol. 93, 111–124. doi: 10.1016/j.pneurobio.2010.10.005
Loggia, M. L., Kim, J., Gollub, R. L., Vangel, M. G., Kirsch, I., Kong, J., et al. (2013). Default mode network connectivity encodes clinical pain: an arterial spin labeling study. Pain 154, 24–33. doi: 10.1016/j.pain.2012.07.029
Lucas-Carrasco, R. (2012). The WHO quality of life (WHOQOL) questionnaire: Spanish development and validation studies. Qual. Life Res. 21, 161–165. doi: 10.1007/s11136-011-9926-3
Malagurski, B., Liem, F., Oschwald, J., Mérillat, S., and Jäncke, L. (2020). Functional dedifferentiation of associative resting state networks in older adults – A longitudinal study. NeuroImage 214:116680. doi: 10.1016/j.neuroimage.2020.116680
Malfliet, A., Coppieters, I., Van Wilgen, P., Kregel, J., De Pauw, R., Dolphens, M., et al. (2017). Brain changes associated with cognitive and emotional factors in chronic pain: a systematic review. Eur. J. Pain 21, 769–786. doi: 10.1002/ejp.1003
Mao, C. P., Yang, H. J., Zhang, Q. J., Yang, Q. X., and Li, X. H. (2022). Altered effective connectivity within the cingulo-frontal-parietal cognitive attention networks in chronic low back pain: a dynamic causal modeling study. Brain Imaging Behav. 16, 1516–1527. doi: 10.1007/s11682-021-00623-4
Meeker, T. J., Jupudi, R., Lenz, F. A., and Greenspan, J. D. (2020). New developments in non-invasive brain stimulation in chronic pain. Curr. Phys. Med. Rehabil. Rep. 8, 280–292. doi: 10.1007/s40141-020-00260-w
Melloni, L., van Leeuwen, S., Alink, A., and Müller, N. G. (2012). Interaction between bottom-up saliency and top-down control: how saliency maps are created in the human brain. Cereb. Cortex 22, 2943–2952. doi: 10.1093/cercor/bhr384
Miettinen, T., Kautiainen, H., Mäntyselkä, P., Linton, S. J., and Kalso, E. (2019). Pain interference type and level guide the assessment process in chronic pain: categorizing pain patients entering tertiary pain treatment with the brief pain inventory. PLoS One 14:e0221437. doi: 10.1371/journal.pone.0221437
Müller, M. J. (2011). Helplessness and perceived pain intensity: relations to cortisol concentrations after electrocutaneous stimulation in healthy young men. Biopsychosoc. Med. 5:8. doi: 10.1186/1751-0759-5-8
Napadow, V., LaCount, L., Park, K., As-Sanie, S., Clauw, D. J., and Harris, R. E. (2010). Intrinsic brain connectivity in fibromyalgia is associated with chronic pain intensity. Arthritis Rheum. 62, 2545–2555. doi: 10.1002/art.27497
Olmedilla Zafra, A., Ortega Toro, E., and Abenza Cano, L. (2013). Validación de la escala de catastrofismo ante el dolor (pain catastrophizing scale) en deportistas españoles. Cuadernos de Psicología del Deporte 13, 83–94. doi: 10.4321/S1578-84232013000100009
Opdebeeck, C., Matthews, F. E., Wu, Y.-T., Woods, R. T., Brayne, C., and Clare, L. (2018). Cognitive reserve as a moderator of the negative association between mood and cognition: evidence from a population-representative cohort. Psychol. Med. 48, 61–71. doi: 10.1017/S003329171700126X
Otti, A., Guendel, H., Wohlschläger, A., Zimmer, C., and Noll-Hussong, M. (2013). Frequency shifts in the anterior default mode network and the salience network in chronic pain disorder. BMC Psychiatry 13:84. doi: 10.1186/1471-244X-13-84
Pfannmöller, J., and Lotze, M. (2019). Review on biomarkers in the resting-state networks of chronic pain patients. Brain Cogn. 131, 4–9. doi: 10.1016/j.bandc.2018.06.005
Power, J. D., Barnes, K. A., Snyder, A. Z., Schlaggar, B. L., and Petersen, S. E. (2012). Spurious but systematic correlations in functional connectivity MRI networks arise from subject motion. Neuroimage 59, 2142–2154. doi: 10.1016/j.neuroimage.2011.10.018
Power, J. D., Barnes, K. A., Snyder, A. Z., Schlaggar, B. L., and Petersen, S. E. (2013). Steps toward optimizing motion artifact removal in functional connectivity MRI; a reply to carp. Neuroimage 76, 439–441. doi: 10.1016/j.neuroimage.2012.03.017
Power, J. D., Mitra, A., Laumann, T. O., Snyder, A. Z., Schlaggar, B. L., and Petersen, S. E. (2014). Methods to detect, characterize, and remove motion artifact in resting state fMRI. Neuroimage 84, 320–341. doi: 10.1016/j.neuroimage.2013.08.048
Power, J. D., Schlaggar, B. L., and Petersen, S. E. (2015). Recent progress and outstanding issues in motion correction in resting state fMRI. Neuroimage 105, 536–551. doi: 10.1016/j.neuroimage.2014.10.044
Qiu, J., Du, M., Yang, J., Lin, Z., Qin, N., Sun, X., et al. (2021). The brain’s structural differences between postherpetic neuralgia and lower back pain. Sci. Rep. 11:22455. doi: 10.1038/s41598-021-01915-x
Riedel, L., van den Heuvel, M. P., and Markett, S. (2021). Trajectory of rich club properties in structural brain networks. Hum. Brain Mapp. 43, 4239–4253. doi: 10.1002/hbm.25950
Schaefer, A., Kong, R., Gordon, E. M., Laumann, T. O., Zuo, X.-N., Holmes, A. J., et al. (2018). Local-global parcellation of the human cerebral cortex from intrinsic functional connectivity MRI. Cereb. Cortex 28, 3095–3114. doi: 10.1093/cercor/bhx179
Schütze, R., Rees, C., Smith, A., Slater, H., Campbell, J. M., and O’Sullivan, P. (2018). How can we best reduce pain catastrophizing in adults with chronic noncancer pain? a systematic review and meta-analysis. J. Pain 19, 233–256. doi: 10.1016/j.jpain.2017.09.010
Seidler, R., Erdeniz, B., Koppelmans, V., Hirsiger, S., Mérillat, S., and Jäncke, L. (2015). Associations between age, motor function, and resting state sensorimotor network connectivity in healthy older adults. NeuroImage 108, 47–59. doi: 10.1016/j.neuroimage.2014.12.023
Seminowicz, D. A., Wideman, T. H., Naso, L., Hatami-Khoroushahi, Z., Fallatah, S., Ware, M. A., et al. (2011). Effective treatment of chronic low back pain in humans reverses abnormal brain anatomy and function. J. Neurosci. 31, 7540–7550. doi: 10.1523/JNEUROSCI.5280-10.2011
Solé-Padullés, C., Cattaneo, G., Marchant, N. L., Cabello-Toscano, M., Mulet-Pons, L., Solana, J., et al. (2022). Associations between repetitive negative thinking and resting-state network segregation among healthy middle-aged adults. Front. Aging Neurosci. 14:1062887. doi: 10.3389/fnagi.2022.1062887
Spisak, T., Kincses, B., Schlitt, F., Zunhammer, M., Schmidt-Wilcke, T., Kincses, Z. T., et al. (2019). Pain-free resting-state functional brain connectivity predicts individual pain sensitivity. bioRxiv [Preprint] doi: 10.1101/790709
Spreng, R. N., Sepulcre, J., Turner, G. R., Stevens, W. D., and Schacter, D. L. (2013). Intrinsic architecture underlying the relations among the default, dorsal attention, and frontoparietal control networks of the human brain. J. Cogn. Neurosci. 25, 74–86. doi: 10.1162/jocn_a_00281
Stensland, M. (2021). “If you don’t keep going, you’re gonna die”: helplessness and perseverance among older adults living with chronic low back pain. Gerontologist 61, 907–916. doi: 10.1093/geront/gnaa150
Stone, A. A., and Broderick, J. E. (2012). Obesity and pain are associated in the United States. Obesity 20, 1491–1495. doi: 10.1038/oby.2011.397
Sturgeon, J. A., and Zautra, A. J. (2013). Psychological resilience, pain catastrophizing, and positive emotions: perspectives on comprehensive modeling of individual pain adaptation. Curr. Pain Headache Rep. 17:317. doi: 10.1007/s11916-012-0317-4
Sullivan, M. J., Thorn, B., Haythornthwaite, J. A., Keefe, F., Martin, M., Bradley, L. A., et al. (2001). Theoretical perspectives on the relation between catastrophizing and pain. Clin. J. Pain 17, 52–64. doi: 10.1097/00002508-200103000-00008
Sullivan, M. J. L. (2012). The communal coping model of pain catastrophising: clinical and research implications. Can. Psychol. 53, 32–41. doi: 10.1037/a0026726
Sullivan, M. J. L., Bishop, S. R., and Pivik, J. (1995). The pain catastrophizing scale: development and validation. Psychol. Assess. 7, 524–532. doi: 10.1037/1040-3590.7.4.524
Suso-Ribera, C., García-Palacios, A., Botella, C., and Ribera-Canudas, M. V. (2017). Pain catastrophizing and its relationship with health outcomes: does pain intensity matter? Pain Res. Manag. 2017:9762864. doi: 10.1155/2017/9762864
Tanner, J. J., Johnson, A. J., Terry, E. L., Cardoso, J., Garvan, C., Staud, R., et al. (2021). Resilience, pain, and the brain: relationships differ by sociodemographics. J. Neurosci. Res. 99, 1207–1235. doi: 10.1002/jnr.24790
Ter Minassian, A., Ricalens, E., Humbert, S., Duc, F., Aubé, C., and Beydon, L. (2012). Dissociating anticipation from perception: Acute pain activates default mode network. Hum. Brain Mapp. 34, 2228–2243. doi: 10.1002/hbm.22062
The Whoqol Group (1998). The world health organization quality of life assessment (WHOQOL): development and general psychometric properties. Soc. Sci. Med. 46, 1569–1585. doi: 10.1016/S0277-9536(98)00009-4
Thomas Yeo, B. T., Krienen, F. M., Sepulcre, J., Sabuncu, M. R., Lashkari, D., Hollinshead, M., et al. (2011). The organization of the human cerebral cortex estimated by intrinsic functional connectivity. J. Neurophysiol. 106, 1125–1165. doi: 10.1152/jn.00338.2011
Treede, R.-D., Rief, W., Barke, A., Aziz, Q., Bennett, M. I., Benoliel, R., et al. (2015). A classification of chronic pain for ICD-11. Pain 156, 1003–1007. doi: 10.1097/j.pain.0000000000000160
van den Heuvel, M. P., and Sporns, O. (2013). An anatomical substrate for integration among functional networks in human cortex. J. Neurosci. 33, 14489–14500. doi: 10.1523/JNEUROSCI.2128-13.2013
Van Dijk, K. R. A., Sabuncu, M. R., and Buckner, R. L. (2012). The influence of head motion on intrinsic functional connectivity MRI. Neuroimage 59, 431–438. doi: 10.1016/j.neuroimage.2011.07.044
van Ettinger-Veenstra, H., Lundberg, P., Alföldi, P., Södermark, M., Graven-Nielsen, T., Sjörs, A., et al. (2019). Chronic widespread pain patients show disrupted cortical connectivity in default mode and salience networks, modulated by pain sensitivity. J. Pain Res. 12, 1743–1755. doi: 10.2147/JPR.S189443
Vossel, S., Geng, J. J., and Fink, G. R. (2014). Dorsal and ventral attention systems. Neuroscientist 20, 150–159. doi: 10.1177/1073858413494269
Wang, J., Zuo, X., and He, Y. (2010). Graph-based network analysis of resting-state functional MRI. Front. Syst. Neurosci. 4:16. doi: 10.3389/fnsys.2010.00016
Wiech, K. (2016). Deconstructing the sensation of pain: the influence of cognitive processes on pain perception. Science 354, 584–587. doi: 10.1126/science.aaf8934
Wiech, K. (2018). Biased perception and learning in pain. Nat. Hum. Behav. 2, 804–805. doi: 10.1038/s41562-018-0468-3
Wiech, K., and Shriver, A. (2018). Cognition doesn’t only modulate pain perception; it’s a central component of it. AJOB Neurosci. 9, 196–198.
Wig, G. S. (2017). Segregated systems of human brain networks. Trends Cogn. Sci. 21, 981–996. doi: 10.1016/j.tics.2017.09.006
World Medical Association (2013). World medical association declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 310, 2191–2194. doi: 10.1001/jama.2013.281053
Yoshino, A., Okamoto, Y., Okada, G., Takamura, M., Ichikawa, N., Shibasaki, C., et al. (2018). Changes in resting-state brain networks after cognitive-behavioral therapy for chronic pain. Psychol. Med. 48, 1148–1156.
You, B., Wen, H., and Jackson, T. (2021). Identifying resting state differences salient for resilience to chronic pain based on machine learning multivariate pattern analysis. Psychophysiology 58:e13921. doi: 10.1111/psyp.13921
Yu, R., Gollub, R. L., Spaeth, R., Napadow, V., Wasan, A., and Kong, J. (2014). Disrupted functional connectivity of the periaqueductal gray in chronic low back pain. Neuroimage Clin. 6, 100–108. doi: 10.1016/j.nicl.2014.08.019
Zhaoyang, R., Martire, L. M., and Darnall, B. D. (2020). Daily pain catastrophizing predicts less physical activity and more sedentary behavior in older adults with osteoarthritis. Pain 161, 2603–2610. doi: 10.1097/j.pain.0000000000001959
Keywords: chronic pain, functional magnetic resonance imaging, resilience, system segregation, pain catastrophizing, psychological distress
Citation: Delgado-Gallén S, Soler MD, Cabello-Toscano M, Abellaneda-Pérez K, Solana-Sánchez J, España-Irla G, Roca-Ventura A, Bartrés-Faz D, Tormos JM, Pascual-Leone A and Cattaneo G (2023) Brain system segregation and pain catastrophizing in chronic pain progression. Front. Neurosci. 17:1148176. doi: 10.3389/fnins.2023.1148176
Received: 19 January 2023; Accepted: 28 February 2023;
Published: 16 March 2023.
Edited by:
Hongxing Zhang, Xuzhou Medical University, ChinaReviewed by:
Junqin Ma, Southern Medical University, ChinaCopyright © 2023 Delgado-Gallén, Soler, Cabello-Toscano, Abellaneda-Pérez, Solana-Sánchez, España-Irla, Roca-Ventura, Bartrés-Faz, Tormos, Pascual-Leone and Cattaneo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Selma Delgado-Gallén, c2VsbWFkZWxnYWRvQGd1dHRtYW5uLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.