
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurosci., 04 July 2022
Sec. Neurodevelopment
Volume 16 - 2022 | https://doi.org/10.3389/fnins.2022.893003
 Sergio Serrada-Tejeda
Sergio Serrada-Tejeda Rosa M. Martínez-Piédrola
Rosa M. Martínez-Piédrola Nuria Máximo-Bocanegra*
Nuria Máximo-Bocanegra* Patricia Sánchez-Herrera-Baeza
Patricia Sánchez-Herrera-Baeza Marta Pérez-de-Heredia-Torres
Marta Pérez-de-Heredia-Torres
Introduction: The variety in symptomatology and clinical presentation of individuals diagnosed with Phelan-McDermid Syndrome (PMS) can delay medical diagnosis, so identifying specific neurobehavioral variables and facilitating differential diagnosis with patients with idiopathic Autism Spectrum Disorder (ASD) can guide early detection.
Methods: A descriptive analysis of the level of adaptive behavior in 50 patients diagnosed with PMS was performed (SHANK3deletion: N = 44; SHANKmutation: N = 6). Subsequently, a comparative analysis was performed with 28 children aged between 4 years and 6 years and 11 months (SHANK3deletion = 14; ASD = 14). Differences between the two groups were evaluated and Bonferroni correction was applied for multiple comparisons.
Results: Differences were identified in the variables of communication (z = −2.715, p = 0.007), Self-Direction (z = −2.199, p = 0.028) and social participation (z = −3.190, p = 0.001), with better adaptive behavior skills being observed in participants with a SHANK3mutation. Better adaptive skills in the sample of participants with ASD, were found and statistically significant differences were identified in the variables of academic skills (z = −3.084, p = 0.002), use of community resources (z = −1.889, p = 0.050) and health and safety (z = −2.90, p = 0.004).
Conclusion: Participants with SHANK3mutation show better communication and social participation skills than those with a diagnosis of SHANK3deletion. The observed differences between ASD and individuals with PMS reflect deficits in practical and conceptual adaptive skills that may limit and hinder daily adaptive functioning.
Phelan-McDermid syndrome (PMS) is a genetic disorder and one of the most common single-gene forms associated with the diagnosis of autism spectrum disorder (ASD). The current classification system for PMS, differentiates between PMS-SHANK3 individuals and PMS-SHANK3 unrelated (Phelan et al., 2022). In PMS-SHANK3 individuals the neurobehavioral phenotype is due to a deletion of the terminal end of chromosome 22 in the 22q13 region, unbalanced translocations, ring chromosomes, as well as a consequence of pathogenic variants or mutations of the SHANK3 gene (Bonaglia et al., 2001; Luciani et al., 2003; Wilson et al., 2003). This genetic abnormality, responsible for most of the clinical features and signs (Bonaglia et al., 2001; Wilson et al., 2003; Delhaye et al., 2009), is of special interest due to the putative association between ASD and PMS as the SHANK3 gene is one of the many genes implicated in the etiology of ASD (Durand et al., 2006; Bill and Geschwind, 2009; Uchino and Waga, 2013), and whose deficiency is associated with 0.5–2% of cases of ASD and intellectual disability (Soorya et al., 2013; Leblond et al., 2014; Richards et al., 2017).
Despite the increase in the diagnosis of PMS as a result of advanced molecular genetic testing (Phelan and McDermid, 2012), the first study conducted in Spain (Gómez Taylor et al., 2020) describes a very low prevalence (4 × 10–4/10,000), and whose figures are far from the estimated global rate, which is in the range of 2.5–10 per million births, although this is likely to be a gross underestimate as it is based on a limited statistical analysis (National Organization for Rare Disorders. Phelan-McDermid Syndrome). In this sense, and as in other cultural contexts (Boccuto et al., 2013; Zwanenburg et al., 2016), it can be considered an underdiagnosed disease, probably due to the non-specific characteristics and symptomatology of the diagnosis.
As in other genetic diseases, early detection and establishment of an initial diagnosis is a key element. In individuals with PMS, this assessment process, can often be hampered by the presence of associated impairments in cognitive ability, communication, or interaction with the environment (Phelan et al., 2011; Soorya et al., 2017). Most reported cases of PMS are caused by deletions in 22q13. 3 (Bonaglia et al., 2011; Soorya et al., 2013; Sarasua et al., 2014a), and, although information on individuals with mutation in SHANK3 is still rare (De Rubeis et al., 2018) and a small number of cases have been described (Soorya et al., 2013; Holder and Quach, 2016; De Rubeis et al., 2018), it has been estimated that haploinsufficiency in SHANK3 could account for about 1% of ASD cases (Betancur and Buxbaum, 2013; Leblond et al., 2014; De Rubeis et al., 2018). In recent studies, genetic analysis indicates that the size of the deletion and severity of clinical manifestations are positively correlated (Luciani et al., 2003; Wilson et al., 2003; Soorya et al., 2013; Sarasua et al., 2014a), with clinical signs such as hypotonia (Luciani et al., 2003; Wilson et al., 2003; Sarasua et al., 2011), developmental delay (Luciani et al., 2003; Wilson et al., 2003; Sarasua et al., 2011), dysmorphic features (Soorya et al., 2013), and language and communication difficulties (Sarasua et al., 2014b). However, other studies report that subjects with smaller deletions are also severely affected (Misceo et al., 2011; Sarasua et al., 2014b; Oberman et al., 2015), but show more favorable development (Zwanenburg et al., 2016; Cammarata-Scalisi et al., 2022).
Therefore, and due to the variety in symptomatology and clinical presentation, research has focused on elaborating detailed phenotypes of development, communication (Sarasua et al., 2014a) or behavioral variables (Phelan and McDermid, 2012; Richards et al., 2017; Droogmans et al., 2019) to facilitate the diagnosis of PMS. To date, although traits similar to those observed in ASD have been identified, such as poor eye contact, the presence of stereotyped movements or self-stimulation (Soorya et al., 2013; Droogmans et al., 2019), in some instances, individuals with PMS do not meet the criteria for a diagnosis of ASD. In addition, it has been observed that the difficulties identified in younger individuals are often associated with emotional and behavioral difficulties, as well as a greater presence of ASD traits and deficits in social communication (Oberman et al., 2015), which may negatively impact adaptive skills that are necessary for daily functioning (Shaw et al., 2011; Reierson et al., 2017; Droogmans et al., 2019).
Therefore, and due to the scarce information and studies with individuals with PMS-SHANK3, the objectives of the present study were to obtain detailed information on the adaptive behavioral profile of individuals depending on the genetic alteration presented (PMSdeletion vs. PMSmutation) and to analyze whether there are significant differences compared to a matched sample of participants with ASD.
The data from this descriptive study are part of a larger longitudinal research project examining the evolution of adaptive behavior and sensory difficulties in the PMS population. The study was approved by the Clinical Research Ethics Committee of the Universidad Rey Juan Carlos. The families of the study participants completed the informed consent document and accepted the sending of supporting documentation for diagnostic confirmation.
This study was conducted in Spain and the collection, management, storage, communication, and transfer of all data was completed in accordance with the provisions of the Declaration of Helsinki World Medical Association [WMA], 2017, the data protection law in force in the General Data Protection (EU Regulation 2016-679 of the European Parliament and of the Council of 27 April 2016), and current Spanish regulations on personal data protection.
Convenience sampling was performed between July 2020 and December 2020. The participant samples of the present study are constituted by two groups: a first group of participants with a diagnosis of PMS and a second group with a diagnosis of ASD. For both participant samples the parents signed and accepted the informed consent form. Participants with PMS were recruited through an internal communication sent by the management of the Asociación Síndrome Phelan-McDermid (Spain). The participants with a diagnosis of ASD were recruited through a public early care service of the Community of Madrid that attends to children with special needs, transitory or permanent, caused by deficiencies, alterations in development or risk of suffering them, and who have been previously evaluated by the Regional Center for Coordination and Evaluation of Children (CRECOVI) of the Community of Madrid.
PMS participants met the inclusion criteria if they had a confirmed diagnosis by demonstration of a SHANK3deletion with comparative genomic hybridization (CGH) or by whole exome sequencing (WES) in case of a SHANK3mutation. Participants with ASD were included if they were within the age range and had a confirmed diagnosis of ASD identified by a physician, psychologist, neurologist, or psychiatrist, as described in the DSM-5 American Psychiatric Association [APA], 2013. ASD participants had no associated medical diagnoses, so no genetic alterations were reported in any of them. To perform the comparative analysis, an age-matched-subsample of the SHANK3deletion group was included and compared with a group of children with a diagnosis of ASD and an age of less than 6 years and 11 months.
To complete the ABAS-II questionnaire, a copy was sent to the parents and/or legal guardians of each participant for completion. Before beginning the completion of the questionnaire, families were instructed on the importance of understanding the general instructions and the specific criteria for scoring. In this way, the research team ensured that all participants’ families had the same information to assign the score for the frequency of the behaviors. However, when necessary, the research team contacted by telephone those families who requested help in completing the questionnaire due to difficulties in understanding the instructions, or if some of the questionnaire items remained unanswered. In both situations, the researchers clarified doubts in the completion of the questionnaire and made sure that the families assigned a specific value for all the items in the questionnaire.
A separate document was also sent to collect information related to the patients, including sociodemographic data, type of genetic disorder, as well as attendance to specific rehabilitation treatments.
The Adaptive Behavior Assessment Questionnaire (ABAS-II): provides a comprehensive assessment of the adaptive skills of individuals from birth to 89 years of age (Montero and Fernández-Pinto, 2013). The ABAS-II is a very valuable tool for the assessment of individuals who may have difficulties with the daily adaptive skills necessary for effective functioning in different environments. The ABAS-II assesses ten specific areas of adaptive skills that are grouped into three indexes or domains of adaptive behavior. Both the adaptive skill areas and domains are based on the American Association on Intellectual Developmental Disabilities (AAIDD) definition of adaptive behavior. The ABAS-II provides a General Adaptive Composite (GAC) that summarizes performance in all adaptive skill areas: Conceptual Domain (Communication, Functional (pre)academic skills, and Self-Direction); Social Domain (Leisure and social interaction skills); and Practical Domain (Use of community resources, Home or school life, Health and safety, Self-care, Motor skills, and Employment). Composite scores for Conceptual, Social and Practical domains, as well as the GAC, have a score of 100 and a standard deviation of 15, and in case of the adaptive skill areas, the raw scores are converted to scaled scores with a mean of 10 and a standard deviation of 3. Its psychometric properties demonstrated high test-retest reliability (r > 0.80) and adequate validity and internal consistency (GAC: r > 0.90; conceptual, social, and practical domains: r > 0.83).
Basic descriptive methods were used for the statistical analysis of the sample. For qualitative variables, the number of cases present in each category and the corresponding percentage were calculated and, for quantitative variables, the median and interquartile range were calculated as they did not follow a normal distribution.
Due to the difference in sample size between PMS subsamples, a descriptive analysis of the results obtained was performed. Moreover, for a comparative analysis the Wilcoxon rank-sum test was used for participants comparisons (PMSdeletion vs ASD) and medians and quartiles were provided for each group. Estimates for the median of the treatment differences and Hodges-Lehmann 2-tailed 95% confidence intervals were provided for each group comparison. To correct for type I error Bonferroni correction was applied to adjust for multiple comparisons at a level of significance of p < 0.0035 (0.05/14). Statistical analysis was performed with the SPSS 25.0 program for Windows (Copyright© 2013 IBM SPSS Corp.). Differences considered statistically significant are those whose p < 0.05.
The final study sample consisted of a total of 50 participants with a diagnosis of PMS (SHANK3deletion: N = 44 and SHANK3mutation: N = 6) and a sample of 14 participants with a diagnosis of idiopathic ASD. The sociodemographic data of the samples are described in Table 1.
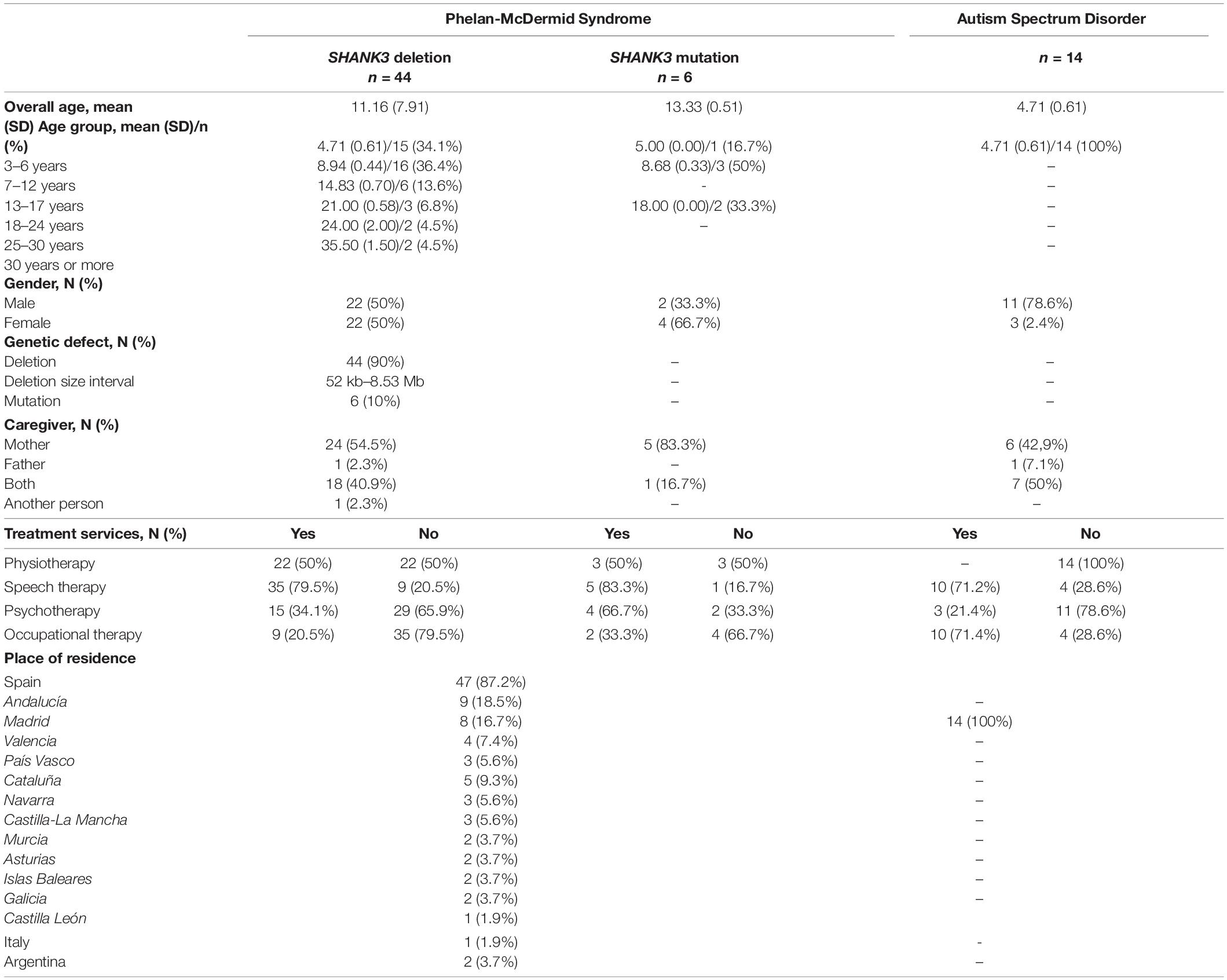
Table 1. Participants demographic data.
Table 2 shows the descriptive analysis between the subsamples of participants with PMS. The ranges of scores obtained by individuals with SHANK3mutation showed unequal score values. In the adaptive skills of self-direction, leisure, social interaction, and home or school living, individuals with mutation showed adaptive skill values comprised within the expected mean performance. In comparison to individuals with deletion, adaptive skills scores showed little variability and values associated with very low performance.
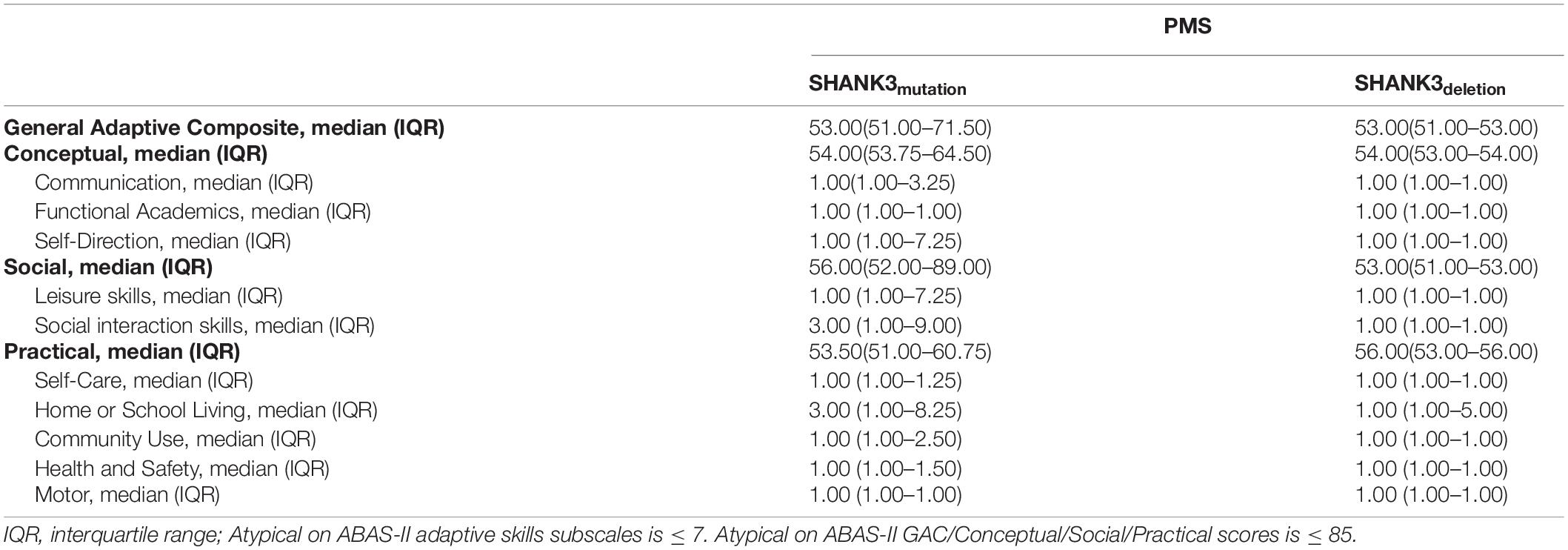
Table 2. ABAS-II descriptive results according to PMS genetic defect.
In the adaptive behavior domains, similar results were obtained in both subsamples, with scores associated with very low levels of adaptive behavior. However, participants with a SHANK3 mutation showed better adaptive behavior skills in the social domain, with scores in the middle range of performance.
The comparative analysis of participants with SHANK3deletion and ASD is shown in Table 3. In this case, the age range was adjusted to ensure greater stability in the measurements. The resulting sample consisted of a total of 28 participants (SHANK3deletion = 14 and ASD = 14) ranging in age from 4 years to 6 years and 11 months. The mean age for both samples (SHANK3deletion and ASD) was 4.71 (0.61) Gender distribution of participants was 10 males and 4 females for the SHANK3deletion group, and 11 males and 3 females for the ASD sample.
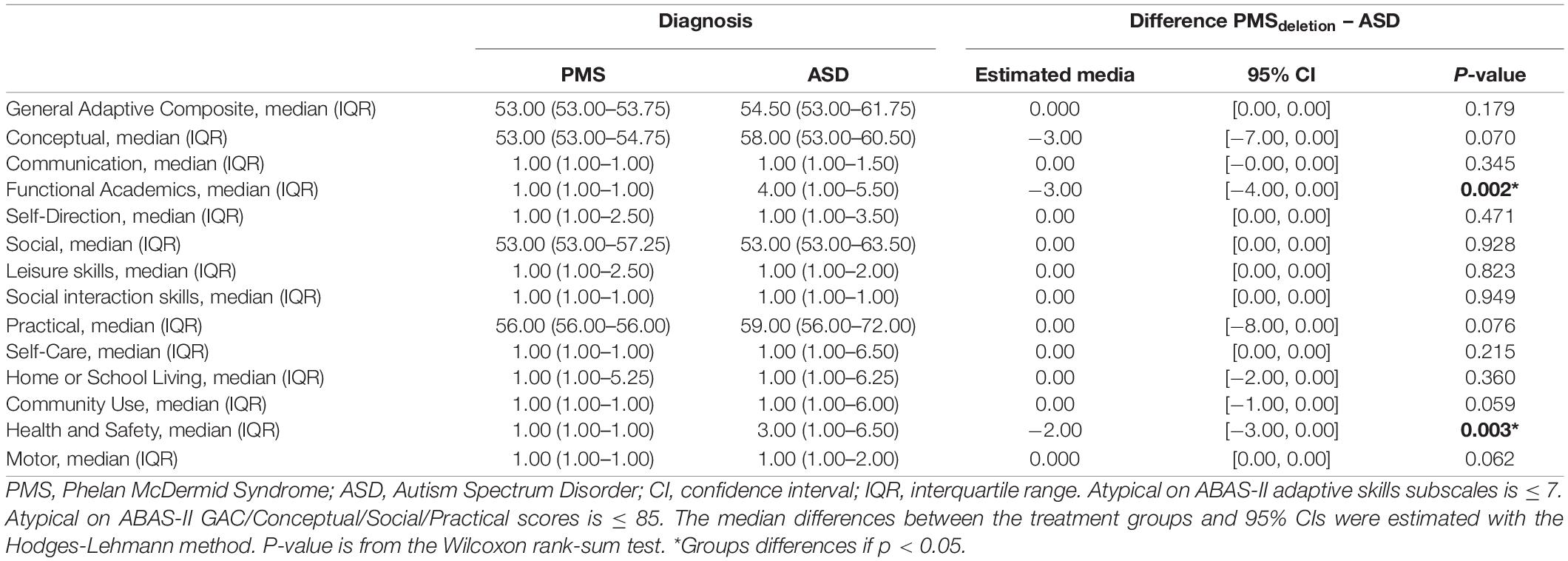
Table 3. Descriptive statistics and comparative analysis of the ABAS-II in PMS and ASD population.
The estimate of the median of the Functional Academics skills differences between SHANK3deletion and ASD was −3.00%. This adaptive behavior skill difference was statistically significant (p = 0.002). The estimate of the median of the Health and Safety skills differences between SHANK3deletion and ASD was −2.00%. This adaptive behavior skills difference was statistically significant (p = 0.003). After Bonferroni correction, Functional Academics and Health and Safety were the only variables that showed significant differences between participants.
The rest of the comparative analysis of the participants with SHANK3 deletion and ASD showed that no statistically significant differences were found in the remaining adaptive skills. Similarly, neither in the general index (GAC) nor in the indexes of conceptual, social and practical adaptive skills showed differences between the two groups.
Identifying the developmental profile of adaptive behavior in a relatively large sample of people diagnosed with PMS in the Spanish population provides more detailed information on the characteristics of adaptive behavior, which may facilitate the identification of differential aspects during the evaluation and diagnosis process.
The results obtained in this study show as in previous studies (Havens et al., 2004; Dhar et al., 2010; Phelan et al., 2011; Shaw et al., 2011; Denayer et al., 2012; Phelan and McDermid, 2012; Zwanenburg et al., 2016; Brignell et al., 2021), that people with PMS present a low level of adaptive behavior, which limits effective participation in the environment and daily context. These results are similar to those obtained by Droogmans et al. (2019), in which they determine that people with PMS require a high need for assistance to perform daily activities.
The comparative analysis of the sample of participants with PMS, identified significant differences in the variables of communication, social participation, and self-direction among participants with PMS, with better skills observed in participants presenting a SHANK3 gene mutation. As in the previous study, communication skills are severely affected with greater difficulties predominating in the ability to express language (De Rubeis et al., 2018). However, although communication delay is evident, individuals with a diagnosis of PMS and SHANK3 mutation, appear to preserve better language skills, vs. those individuals affected by a SHANK3 deletion (Soorya et al., 2013).
Although in our study, the size variability of genetic alterations was not determined, in the study by Soorya et al. (2013), it was observed that larger deletions were associated with greater difficulties in communication, whereas individuals with smaller deletions or point mutations showed characteristics similar to those of children with ASD. Similar results (Xu et al., 2020) support the effect that 22q13 gene deletions and SHANK3 point mutations have on various clinical manifestations, such as developmental delay and language impairment.
Due to the similarities in the symptomatology of PMS and ASD, and similar to our study, current research has not identified significant differences in communicative or social areas. In the study developed by Richards et al. (2017), it was identified that the PMS sample showed greater difficulties in social reciprocity in showing and directing attention, observing, in addition, better skills in showing interest and responding to other people, and a lower tendency to show ritualistic and repetitive behaviors than in subjects with ASD. Similarly, Burdeus-Olavarrieta et al. (2021) identified that there were no differences between receptive and expressive communication skills, although the results showed a wide variability both within and between subjects.
Interestingly, previous studies indicate that the contributing factor to the clinical diagnosis of ASD was the social adaptive subdomain (Oberman et al., 2015) and that specific genetic deficits, but not total loss of genetic material, may explain ASD symptomatology in PMS. In other genetic syndromes with similar social adaptive profiles, such as fragile X syndrome, although an aberrant and maladaptive social behavior profile has been identified (Kaufmann et al., 2004), communication difficulties do not appear to be a differentiating feature vs. PMS (Richards et al., 2017). Likewise, in Down syndrome it has been identified that those with ASD symptomatology show more disruptive adaptive behavior and a greater presence of stereotypies and social withdrawal (Carter et al., 2007). Furthermore, although on the communicative aspects, language regression is a trait that has not been fully defined in PMS, it has been identified in previous studies (Macedoni-Lukšič et al., 2013; Figura et al., 2014; Cochoy et al., 2015). Unlike Rett syndrome, where regression occurs between the first and third year of life, in PMS the age of onset appears to be undefined (Bonaglia et al., 2011; Soorya et al., 2013).
In our study, two areas of adaptive skills were identified that differentiated the PMS sample from the ASD sample. In the case of the sample with PMSdeletion, the scores associated with Functional Academics and Health and Safety skills showed no variability, and the values remained constant, showing limitations in the ability to participate actively and unsupervised in most of the skills expected for their age. Parents report that for all items assessed, their children are not able to engage in the behaviors described. In contrast, in the sample of participants with ASD, greater variability in scores was observed. Although the level of adaptive skills remains atypical (ABASsubscales ≤ 7), they showed better scores in items related to prewriting skills, pre-reading and pre-mathematical concepts such as counting or sorting. In the case of safety and health skills, participants with ASD show needs for adult supervision in open spaces, and better behaviors in situations where adults give orders to avoid a dangerous situation.
In similar studies, such as the one developed by Shaw et al. (2011), most of the sample with PMS identified maladaptive behaviors related to difficulties in generating non-disruptive internalizing and externalizing behaviors. These behaviors can impact daily functioning and the skills needed to identify risk situations, requiring a higher level of assistance from the adult in order to perform daily activities effectively. However, although differences in score ranges were observed between the PMS subsamples and individuals with ASD, the differences were not statistically significant.
As a consequence of the difficulties shown in daily functioning and adaptive behavior, the needs generated by people with PMS in daily activities and routines must be addressed (Durand et al., 2006; Shaw et al., 2011; Denayer et al., 2012; Brignell et al., 2021). Although the scientific evidence on the speech, physical, occupational, and behavioral treatment of PMS is limited, having descriptive information on the developmental difficulties of individuals with PMS can facilitate and assist the intervention process of professionals, allowing them to improve the quality of their care, and address observable developmental difficulties more precisely.
Due to the social and health crisis caused by COVID-19 and the geographic distribution of the participants, it was not possible to assess aspects of development for which the patient’s presence is required, such as IQ. However, although social restrictions were imposed for the duration of the study, the self-administered assessment instruments were conducted and completed by the primary caregivers. Nevertheless, although the ABAS-II has been previously validated in Spain and has reliable psychometric properties, as it is a self-questionnaire, the possibility of some measurement bias should be considered. However, for future lines of research we have proposed to evaluate these areas, which are relevant in this population.
The sample size of the PMS subsamples is not matched. However, the subdivision has been performed in order to follow a similar methodology to studies conducted in the PMS population. Although the difference in sample sizes of the study is high, it was considered appropriate to include the information obtained in the SHANK3mutation subsample, due to the limited number of studies reporting on its phenotype (Soorya et al., 2013; Holder and Quach, 2016; De Rubeis et al., 2018). However, although the comparative sample of individuals with SHANK3 deletion and ASD is age-matched, it was not possible to perform this same matching by gender, which could introduce additional confounding bias. However, the final ratio of males to females was close between the two groups. In addition, although it is specified that the participants with ASD have a diagnosis confirmed by a physician, none of them underwent a specific genetic analysis during the study.
The described profiles indicate that genetic alterations in the diagnosis of PMS have a negative impact on the development and acquisition of adaptive skills, hindering effective participation in the context. This study expands information on an underdiagnosed pathology and determines quantifiable differences between PMS-SHANK3 individuals, associating better communication and social participation skills in subjects with a genetic mutation. Due to average variability in sample sizes, the results should be analyzed carefully, as they may not be extrapolated to the general PMS-SHANK3 population. However, due to the limited descriptions of adaptive profiles in both SHANK3deletion and SHANK3mutation individuals, these results may help to delineate their phenotypic profiles. The differences observed between children with ASD and with SHANK3deletion identified greater deficits in practical and conceptual adaptive skills, which may negatively impact daily management by primary caregivers. However, these results cannot be extrapolated to the remaining PMS-SHANK3 individuals. Future lines of research should address these difficulties and implementing therapeutic interventions aimed at facilitating and promoting their development should be essential to support the development of this population.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comité de ética de la investigación de la Universidad Rey Juan Carlos. Written informed consent to participate in this study was provided by the participants’ legal guardian/next of kin.
SS-T and MP-H-T conceived the idea. SS-T, RM-P, and PS-H-B drafted the first version of the manuscript. SS-T was responsible for data storage and statistical analysis. MP-H-T and NM-B supervised the manuscript and reviewed the manuscript for intellectual content. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We would like to acknowledge the collaboration and participation of the families and children involved in the study.
American Psychiatric Association [APA] (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Washington, DC: American Psychiatric Association.
Betancur, C., and Buxbaum, J. D. (2013). SHANK3 haploinsufficiency: a “common” but underdiagnosed highly penetrant monogenic cause of autism spectrum disorders. Mol. Autism 4:17. doi: 10.1186/2040-2392-4-17
Bill, B. R., and Geschwind, D. H. (2009). Genetic advances in autism: heterogeneity and convergence on shared pathways. Curr. Opin. Genet. Dev. 19, 271–278. doi: 10.1016/j.gde.2009.04.004
Boccuto, L., Lauri, M., Sarasua, S. M., Skinner, C. D., Buccella, D., Dwivedi, A., et al. (2013). Prevalence of SHANK3 variants in patients with different subtypes of autism spectrum disorders. Eur. J. Hum. Genet. 21, 310–316. doi: 10.1038/ejhg.2012.175
Bonaglia, M. C., Giorda, R., Borgatti, R., Felisari, G., Gagliardi, C., Selicorni, A., et al. (2001). Disruption of the ProSAP2 gene in a t(12;22)(q24.1;q13.3) is associated with the 22q13.3 deletion syndrome. Am. J. Hum. Genet. 69, 261–268. doi: 10.1086/321293
Bonaglia, M. C., Giorda, R., Beri, S., De Agostini, C., Novara, F., Fichera, M., et al. (2011). Molecular mechanisms generating and stabilizing terminal 22q13 deletions in 44 subjects with Phelan/McDermid syndrome. PLoS Genet. 7:e1002173. doi: 10.1371/journal.pgen.1002173
Brignell, A., Gu, C., Holm, A., Carrigg, B., Sheppard, D. A., Amor, D. J., et al. (2021). Correction: Speech and language phenotype in Phelan-McDermid (22q13.3) syndrome. Eur. J. Hum. Genet. 29:719. doi: 10.1038/s41431-021-00855-4
Burdeus-Olavarrieta, M., San José-Cáceres, A., García-Alcón, A., González-Peñas, J., Hernández-Jusdado, P., and Parellada-Redondo, M. (2021). Characterisation of the clinical phenotype in Phelan-McDermid syndrome. J. Neurodev. Disord. 13:26. doi: 10.1186/s11689-021-09370-5
Cammarata-Scalisi, F., Callea, M., Martinelli, D., Willoughby, C. E., Tadich, A. C., Araya Castillo, M., et al. (2022). Clinical and Genetic Aspects of Phelan-McDermid Syndrome: An Interdisciplinary Approach to Management. Genes 13:504. doi: 10.3390/genes13030504
Carter, J. C., Capone, G. T., Gray, R. M., Cox, C. S., and Kaufmann, W. E. (2007). Autistic-spectrum disorders in Down syndrome: further delineation and distinction from other behavioral abnormalities. Am. J. Med. Genet. Part B Neuropsychiat. Genet. 144B, 87–94. doi: 10.1002/ajmg.b.30407
Cochoy, D. M., Kolevzon, A., Kajiwara, Y., Schoen, M., Pascual-Lucas, M., Lurie, S., et al. (2015). Phenotypic and functional analysis of SHANK3 stop mutations identified in individuals with ASD and/or ID. Mol. Autism 6:23. doi: 10.1186/s13229-015-0020-5
De Rubeis, S., Siper, P. M., Durkin, A., Weissman, J., Muratet, F., Halpern, D., et al. (2018). Delineation of the genetic and clinical spectrum of Phelan-McDermid syndrome caused by SHANK3 point mutations. Mol. Autism 9:31. doi: 10.1186/s13229-018-0205-9
Delhaye, A., Toutain, A., Aboura, A., Dupont, C., Tabet, A. C., and Drunat, S. (2009). Chromosome 22q13.3 deletion syndrome with a de novo interstitial 22q13.3 cryptic deletion disrupting SHANK3. Eur. J. Med. Genet. 52, 328–332. doi: 10.1016/j.ejmg.2009.05.004
Denayer, A., Van Esch, H., de Ravel, T., Frijns, J. P., Van Buggenhout, G., Vogels, A., et al. (2012). Neuropsychopathology in 7 Patients with the 22q13 Deletion Syndrome: Presence of Bipolar Disorder and Progressive Loss of Skills. Mol. Syndromol. 3, 14–20. doi: 10.1159/000339119
Dhar, S. U., del Gaudio, D., German, J. R., Peters, S. U., Ou, Z., Bader, P. I., et al. (2010). 22q13.3 deletion syndrome: clinical and molecular analysis using array CGH. Am. J. Med. Genet. A. 152A, 573–581. doi: 10.1002/ajmg.a.33253
Droogmans, G., Swillen, A., and Van Buggenhout, G. (2019). Deep Phenotyping of Development, Communication and Behaviour in Phelan-McDermid Syndrome. Mol. Syndromol. 10, 294–305. doi: 10.1159/000503840
Durand, C. M., Betancur, C., Boeckers, T. M., Bockmann, J., Chaste, P., Fauchereau, F., et al. (2006). Mutations in the gene encoding the synaptic scaffolding protein SHANK3 are associated with autism spectrum disorders. Nat. Genet. 39, 25–27. doi: 10.1038/ng1933
Figura, M. G., Coppola, A., Bottitta, M., Calabrese, G., Grillo, L., Luciano, D., et al. (2014). Seizures and EEG pattern in the 22q13.3 deletion syndrome: clinical report of six Italian cases. Seizure 23, 774–779. doi: 10.1016/j.seizure.2014.06.008
Gómez Taylor, B., Moreno Sancho, M. L., Drehmer Rieger, E., Carrera Juliá, S., Nevado, J., and Sempere Ferre, F. (2020). Prevalencia del síndrome de Phelan-McDermid en España [Prevalence of the Phelan-McDermid Syndrome in Spain.]. Rev. Esp Salud. Publica. 94:e202012121.
Havens, J. M., Visootsak, J., Phelan, M. C., and Graham, J. M. Jr. (2004). 22q13 deletion syndrome: an update and review for the primary pediatrician. Clin. Pediatr. 43, 43–53. doi: 10.1177/000992280404300106
Holder, J. L., and Quach, M. M. (2016). The spectrum of epilepsy and electroencephalographic abnormalities due to SHANK3 loss-of-function mutations. Epilepsia 57, 1651–1659. doi: 10.1111/epi.13506
Kaufmann, W. E., Cortell, R., Kau, A. S., Bukelis, I., Tierney, E., Gray, R. M., et al. (2004). Autism spectrum disorder in fragile X syndrome: communication, social interaction, and specific behaviors. Am. J. Med. Genet. Part A 129A, 225–234. doi: 10.1002/ajmg.a.30229
Leblond, C. S., Nava, C., Polge, A., Gauthier, J., Huguet, G., Lumbroso, S., et al. (2014). Meta-analysis of SHANK mutations in autism spectrum disorders: a gradient of severity in cognitive impairments. PLoS Genet. 10:e1004580. doi: 10.1371/journal.pgen.1004580
Luciani, J. J., de Mas, P., Depetris, D., Mignon-Ravix, C., Bottani, A., Prieur, M., et al. (2003). Telomeric 22q13 deletions resulting from rings, simple deletions, and translocations: cytogenetic, molecular, and clinical analyses of 32 new observations. J. Med. Genet. 40, 690–696. doi: 10.1136/jmg.40.9.690
Macedoni-Lukšič, M., Krgovič, D., Zagradišnik, B., and Kokalj-Vokač, N. (2013). Deletion of the last exon of SHANK3 gene produces the full Phelan-McDermid phenotype: a case report. Gene 524, 386–389. doi: 10.1016/j.gene.2013.03.141
Misceo, D., Rødningen, O. K., Barøy, T., Sorte, H., Mellembakken, J. R., Strømme, P., et al. (2011). A translocation between Xq21.33 and 22q13.33 causes an intragenic SHANK3 deletion in a woman with Phelan-McDermid syndrome and hypergonadotropic hypogonadism. Am. J. Med. Genet. A 155A, 403–408. doi: 10.1002/ajmg.a.33798
Montero, D. Y., and Fernández-Pinto, I. (2013). ABAS-II. Sistema de Evaluación de la Conducta Adaptativa. (Adaptación española). Madrid: TEA Ediciones.
Oberman, L., Boccuto, L., Cascio, L., Sarasua, S., and Kaufmann, W. (2015). Autism spectrum disorder in Phelan-McDermid syndrome: initial characterization and genotype-phenotype correlations. Orphanet. J. Rare Dis. 10:105. doi: 10.1186/s13023-015-0323-9
Phelan, K., Boccuto, L., Powell, C. M., Boeckers, T. M., van Ravenswaaij-Arts, C., Rogers, R. C., et al. (2022). Phelan-McDermid syndrome: a classification system after 30 years of experience. Orphanet. J. Rare Dis. 17:27. doi: 10.1186/s13023-022-02180-5
Phelan, K., and McDermid, H. (2012). The 22q13.3 delection syndrome (Phelan-McDermid Syndrome). Mol. Syndromol. 2, 186–201. doi: 10.1159/000334260
Phelan, M. C., Rogers, R. C., Saul, R. A., Stapleton, G. A., Sweet, K., McDermid, H., et al. (2011). 22q13 deletion syndrome. Am. J. Med. Genet. 101, 91–99. doi: 10.1002/1096-8628(20010615)101:2<91::aid-ajmg1340<3.0.co;2-c
Reierson, G., Bernstein, J., Froehlich-Santino, W., Urban, A., Purmann, C., Berquist, S., et al. (2017). Characterizing regression in Phelan 430 McDermid syndrome (22q13 deletion syndrome). J. Psychiatr. Res. 91, 139–144. doi: 10.1016/j.jpsychires.2017.03.010
Richards, C., Powis, L., Moss, J., Stinton, C., Nelson, L., and Oliver, C. (2017). Prospective study of autism phenomenology and the behavioural phenotype of Phelan-McDermid syndrome: comparison to fragile X syndrome, Down syndrome and idiopathic autism spectrum disorder. J. Neurodev. Disord. 9:37. doi: 10.1186/s11689-017-9217-6
Sarasua, S. M., Boccuto, L., Sharp, J. L., Dwivedi, A., Chen, C. F., Rollins, J. D., et al. (2014a). Clinical and genomic evaluation of 201 patients with Phelan-McDermid syndrome. Hum. Genet. 133, 847–859. doi: 10.1007/s00439-014-1423-7
Sarasua, S. M., Dwivedi, A., Boccuto, L., Chen, C. F., Sharp, J. L., Rollins, J. D., et al. (2014b). 22q13.2q13.32 genomic regions associated with severity of speech delay, developmental delay, and physical features in Phelan-McDermid syndrome. Genet. Med. 16, 318–328. doi: 10.1038/gim.2013.144
Sarasua, S. M., Dwivedi, A., Boccuto, L., Rollins, J. D., Chen, C. F., Rogers, R. C., et al. (2011). Association between deletion size and important phenotypes expands the genomic region of interest in Phelan-McDermid syndrome (22q13 deletion syndrome). J. Med. Genet. 48, 761–766. doi: 10.1136/jmedgenet-2011-100225
Shaw, S. R., Rahman, A., and Sharma, A. (2011). Behavioral Profiles in Phelan-McDermid Syndrome: Focus on Mental Health. J. Mental Health Res. Intell. Disabil. 4, 1–18. doi: 10.1080/19315864.2011.554615
Soorya, L., Kolevzon, A., Zweifach, J., Lim, T., Dobry, Y., Schwartz, L., et al. (2013). Prospective investigation of autism and genotype-phenotype correlations in 22q13 deletion syndrome and SHANK3 deficiency. Mol. Autism 4:18. doi: 10.1186/2040-2392-4-18
Soorya, L., Leon, J., Trelles, M. P., and Thurm, A. (2017). Framework for assessing individuals with rare genetic disorders associated with profound intellectual and multiple disabilities (PIMD): the example of Phelan McDermid Syndrome. Clin. Nuropsychol. 32, 1226–1255. doi: 10.1080/13854046.2017.1413211
Uchino, S., and Waga, C. (2013). SHANK3 as an autism spectrum disorder-associated gene. Brain Dev. 35, 106–110. doi: 10.1016/j.braindev.2012.05.013
Wilson, H., Wong, A., Shaw, S., Tse, W. Y., Stapleton, G., and McDermid, H. E. (2003). Molecular characterization of the 22q13 deletion syndrome supports the role of haploinsufficiency of SHANK3/PROSAP2 in the major neurological symptoms. J. Med. Genet. 40, 575–584. doi: 10.1136/jmg.40.8.575
World Medical Association [WMA] (2017). WMA Declaration of Helsinki—Ethical Principles for Medical Research Involving Human Subjects. Ferney-Voltaire: World Medical Association.
Xu, N., Lv, H., Yang, T., Du, X., Sun, Y., Xiao, B., et al. (2020). A 29 Mainland Chinese cohort of patients with Phelan-McDermid syndrome: genotype-phenotype correlations and the role of SHANK3 haploinsufficiency in the important phenotypes. Orphanet J. Rare Dis. 15:335. doi: 10.1186/s13023-020-01592-5
Zwanenburg, R. J., Ruiter, S. A. J., van den Heuvel, E. R., Flapper, B. C. T., and Van Ravenswaaij-Arts, C. M. A. (2016). Developmental phenotype in Phelan-McDermid (22q13.3 deletion) syndrome: a systematic and prospective study in 34 children. J. Neurodev. Disord. 8:16. doi: 10.1186/s11689-016-9150-0
Keywords: Phelan-McDermid syndrome, SHANK3, adaptive behavior, autism spectrum disorder, participation
Citation: Serrada-Tejeda S, Martínez-Piédrola RM, Máximo-Bocanegra N, Sánchez-Herrera-Baeza P and Pérez-de-Heredia-Torres M (2022) Descriptive Analysis of Adaptive Behavior in Phelan–McDermid Syndrome and Autism Spectrum Disorder. Front. Neurosci. 16:893003. doi: 10.3389/fnins.2022.893003
Received: 09 March 2022; Accepted: 07 June 2022;
Published: 04 July 2022.
Edited by:
Andreas Martin Grabrucker, University of Limerick, IrelandReviewed by:
Lauren Ethridge, University of Oklahoma, United StatesCopyright © 2022 Serrada-Tejeda, Martínez-Piédrola, Máximo-Bocanegra, Sánchez-Herrera-Baeza and Pérez-de-Heredia-Torres. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Nuria Máximo-Bocanegra, bnVyaWEubWF4aW1vQHVyamMuZXM=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.