 Wanyue Li
Wanyue Li Yaru Shang1†
Yaru Shang1† Weisheng Zhuang
Weisheng Zhuang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurosci., 30 May 2022
Sec. Perception Science
Volume 16 - 2022 | https://doi.org/10.3389/fnins.2022.813975
Objective: This study aims to evaluate the effectiveness and long-term effects of response inhibition training as a therapeutic approach in healthy adults.
Methods: The PubMed, Embase, Web of Science, China National Knowledge Infrastructure (CNKI), Wanfang, and China Science and Technology Journal Database (VIP) were searched for studies. Data on the improvement of Cognitive function and its long-term effect were extracted by two authors independently. The pooled data were meta-analyzed using a random-effects model, and the quality of each eligible study was assessed by The Cochrane Collaboration’s tool.
Results: Nine articles were included. 1 of the articles included 2 trials, so 10 eligible trials (response inhibition training group vs. control group) were identified. A total of 490 patients were included. Response inhibition training has beneficial effects on improving cognitive function in healthy adults compared to control treatment (SMD, −0.93; 95% CI, −1.56 to −0.30; Z = 2.88, P = 0.004), the subgroup analysis results showed that either GNG training alone (SMD, −2.27; 95% CI, −3.33 to −1.21; Z = 4.18, P < 0.0001) or the combination of both SST and GNG significantly improved cognitive function in healthy adults (SMD, −0.94; 95% CI, −1.33 to −0.56; Z = 4.80, P < 0.0001), whereas SST training alone did not have such an effect (SMD, −0.15; 95% CI, −0.76 to 0.47; Z = 0.47, P = 0.64). But its long-term effects are not significant (SMD, −0.29; 95% CI, −0.68 to 0.10; Z = 1.45, P = 0.15). The subgroup analysis results showed that neither GNG training alone (SMD, −0.25; 95% CI, −0.75 to 0.24; Z = 0.99, P = 0.32) nor SST training alone (SMD, 0.03; 95% CI, −0.42 to 0.48; Z = 0.14, P = 0.89) could improve the cognitive function of healthy adults in the long term. In contrast, the combination of both training (SMD, −0.95; 95% CI, −1.46 to −0.45; Z = 3.68, P = 0.0002) can have long-term effects on the improvement of cognitive function in healthy adults.
Conclusion: The findings of our study indicate that response inhibition training can improve the cognitive function of healthy adults and that more RCTs need to be conducted to validate their usefulness in clinical cases.
Response inhibition can be conceptualized as the ability to stop, change or delay a behavioral response (Logan et al., 1984; Miyake et al., 2000; Bickel et al., 2012; Baumeister, 2014). It is one of the core components of executive function, and the ability to actively suppress, interrupt or delay behavior (Kooijmans et al., 2000; Groman et al., 2009; Muraven, 2010; Brydges et al., 2012). Individuals inhibit dominant responses formed through inhibitory control to flexibly adapt to changing environments while excluding or reducing the impact of irrelevant information on current information processing (Aron et al., 2004, 2007; Hofmann et al., 2009; Houben and Wiers, 2010; Nederkoorn et al., 2010; Murphy and Garavan, 2011; Verbruggen et al., 2014; Turton et al., 2017).
The research paradigm of response inhibition mainly includes Go/No-go tasks (GNG) and stop-signal tasks (SST). The consistent pairing of the no-go response with the target stimulus facilitated retrieval of the no-go target stimulus association and resulted in improved response inhibition to the target stimulus (Donders, 1969; Maguire and France, 2019). For example, Houben and Jansen (2011) used a GNG task with an alcohol-related stimulant in an attempt to reduce alcohol consumption. Participants in the training condition reported reduced alcohol consumption after training compared to the control condition, suggesting that an association was formed between the alcohol stimulus and the no-go response, which transferred to a reduction in alcohol consumption (Houben and Jansen, 2011). In the SST training paradigm, participants were asked to classify target and neutral stimuli as quickly as possible, however, in a subset of trials, the stop signal would appear after the target stimulus, and participants were asked to suppress their responses (Lawrence et al., 2015). In this way, an association between the target stimulus and the stop response was established. In the control condition, the stop signal was not always paired with a particular type of stimulus or was not presented at all. Lawrence et al. (2015) demonstrated that participants who received SST training in which stop-signals were paired with unhealthy foods consumed significantly less high-calorie food immediately after training, compared to those in the control condition. This suggests that establishing an association between unhealthy food and a stop response results in a reduction in the consumption of unhealthy foods.
In a meta-analysis by Jones et al. (2016), participants learn to associate appetitive cues with inhibition of behavior. The meta-analysis demonstrated that a single session of inhibitory control training (ICT) leads to a robust reduction in food and alcohol consumption in the laboratory. The effect of ICT on behavior was dependent on the task used: the effect was robust when modified GNG tasks were used and was marginally significant when Stop Signal tasks were used. In another study by Allom et al. (2015), results suggest that go/no-go inhibitory control training paradigms can influence health behavior, but perhaps only in the short term. Neither of the interventions included in the meta-analysis of these two studies was response inhibition training, Allom et al. (2015) used interventions for modified response inhibition training, Jones et al. (2016), the study population was also not all normal, including heavy drinkers, overly obese people, and addicted smokers. In contrast, there is a lack of research on the effectiveness and long-term effects of response inhibition training in improving cognitive function in healthy adults. However, most of the subjects used in the above studies had significant cognitive deficits, and response inhibition training is likely to significantly improve cognitive impairment in such individuals (Spierer et al., 2013; van Koningsbruggen et al., 2013; Jones et al., 2016), while it is controversial whether response inhibition training has an ameliorating effect on cognitive impairment in healthy adults. There is evidence of no real training and transfer effects after inhibitory, controlled training in young healthy adults (Enge et al., 2014). It has also been shown that response inhibition training can improve cognitive function in healthy adults (Ji et al., 2016). Cognitive interventions in children during their intellectual development and older populations can help the development of intellectual and other abilities and have, therefore, necessitated this review and meta-analysis to assess the effectiveness and long-term effects of response inhibition training as a treatment in healthy adults.
Ethical approval and patient consent were not required because this was a systematic review and meta-analysis of previously published studies (Higgins and Thompson, 2002). This meta-analysis and systematic review were conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Moher et al., 2009) guidelines and a previously published protocol (PROSPERO: CRD42021277898).
Any articles published before June 2021 in PubMed, Embase, Web of Science, China National Knowledge Infrastructure (CNKI), Wanfang, and China Science and Technology Journal Database (VIP) were searched using the following keywords: “Inhibition OR Suppression OR Interference Inhibition OR Go/No-go OR stop-signal tasks OR SST AND Training.” We manually searched for further literature by tracing the references included in the articles. We searched for papers published in English and Chinese. The inclusion criteria are presented as follows: (1) study design is RCT, (2) interventional studies that focus on response inhibition training, (3) including healthy participants older than 18 years, (4) reporting pre-training and follow-up assessment on at least one outcome measure.
We extracted the following information: author, year of publication, sample size, evaluation methodology, intervention methods, intervention frequency, Intervention intensity, and intervention time. Data were extracted independently by 2 investigators, and discrepancies were resolved by consensus. We applied a Java program called Plot Digitizer1 to convert plotted values into numerical form if adequate information was not provided by a study. We also contacted the corresponding author to obtain the data when necessary. The outcome indicators of this study were the degree of improvement in cognitive ability and the long-term effect outcome, the former including the scores of the included literature assessment tasks such as Go RT (ms), Go/no-go (RT), Stroop interference score (ms), go/no-go (IES), Working memory, Go RTs (ms), and the latter including the scores of the different period time assessment tasks.
All eligible studies were assessed by two other authors independently. A third reviewer arbitrated in cases of disagreement. The Cochrane Risk of Bias Tool was used to assess the risk of bias of included RCTs (Higgins et al., 2008; Higgins and Green, 2008). We assessed seven types of bias accordingly, namely selection biases (random sequence generation and allocation concealment), blinded (performance bias and detection bias), attrition bias (incomplete outcome data), reporting bias (selective outcome reporting), and other biases. We categorized the risk of bias for each item as low, unclear, or high.
We estimated the standardized mean difference (SMD) and 95% confidence interval (CI) for the continuous outcome Cognitive function scores [Go RTs in ms, Go/no-go (RT), Stroop interference score (ms), go/no-go (IES), Working memory] using a random-effects model. Heterogeneity was reported using the I2 statistic, with an I2> 50% indicating significant heterogeneity. When significant heterogeneity emerged, we searched for potential sources of heterogeneity by sequentially omitting a study. Meta-analyses were performed or subgroup analyses were performed according to the different interventions (GNG/SST/GNG and SST). All statistical analyses were performed using Review Manager version 5.3 (Higgins and Thompson, 2002) (The Cochrane Collaboration, Software Update, Oxford, United Kingdom).
Figure 1 shows the detailed flowchart of the search and selection results. A total of 877 potentially relevant articles were identified initially. Finally, In the end, nine articles (Berkman et al., 2014; Enge et al., 2014; Allom and Mullan, 2015; Chen, 2016; Ji et al., 2016; Zhao et al., 2018; Schroder et al., 2020; Wang et al., 2020; Xu et al., 2021) were included, two articles in Chinese, seven articles in English. 1 of the articles included 2 trials, so there were 10 trials in the final meta-analysis. The baseline characteristics of the 10 eligible RCTs in the meta-analysis are summarized in Table 1. The total sample size included was 490. The 10 trials were all RCT studies (response inhibition training versus control group), two of which were blank controls, and the remaining eight studies were placebo training controls (Figure 1).
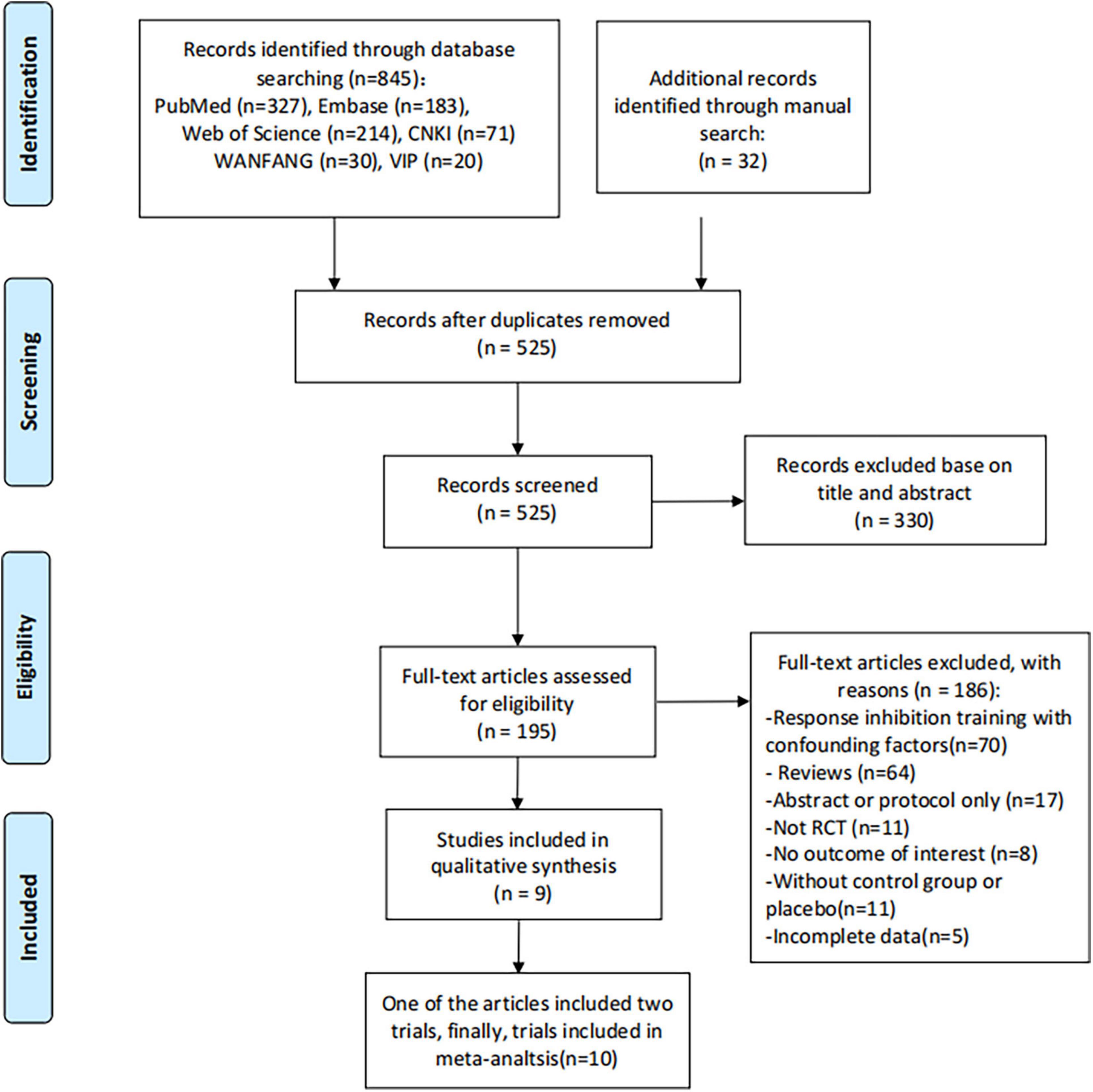
Figure 1. Flow diagram of study searching and selection process.
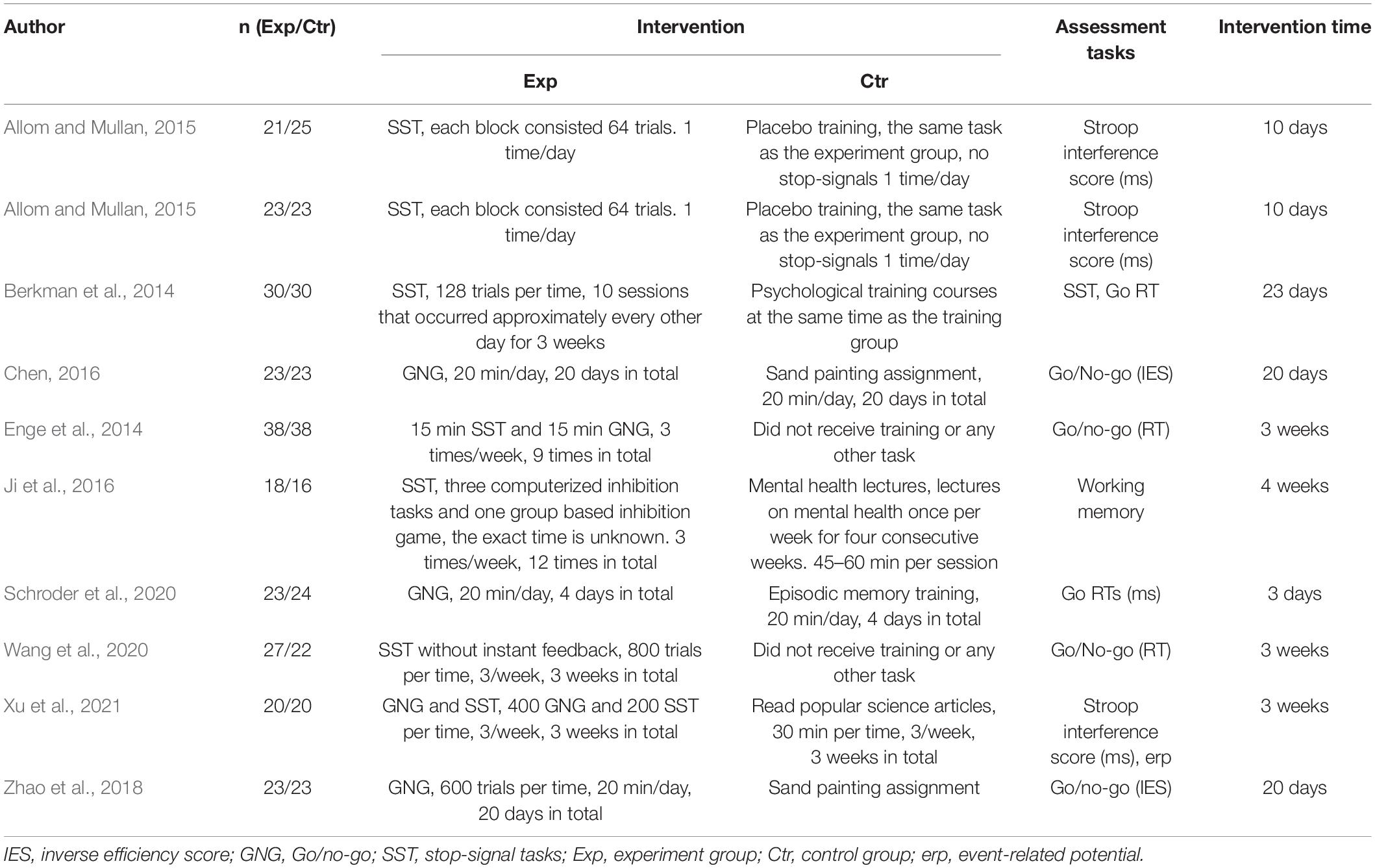
Table 1. Summary of the demographic and clinical characteristics of the included RCT studies (general response inhibition training vs. control group).
Chen (2016) and Wang et al. (2020) did not account for the allocation concealment (selection bias) and blinding of outcome assessment (detection bias). Berkman et al. (2014) did not account for the allocation concealment (selection bias). Zhao et al. (2018) did not account for random sequence generation (selection bias) and allocation concealment (selection bias). The remaining six studies were high-quality studies (Figure 2).
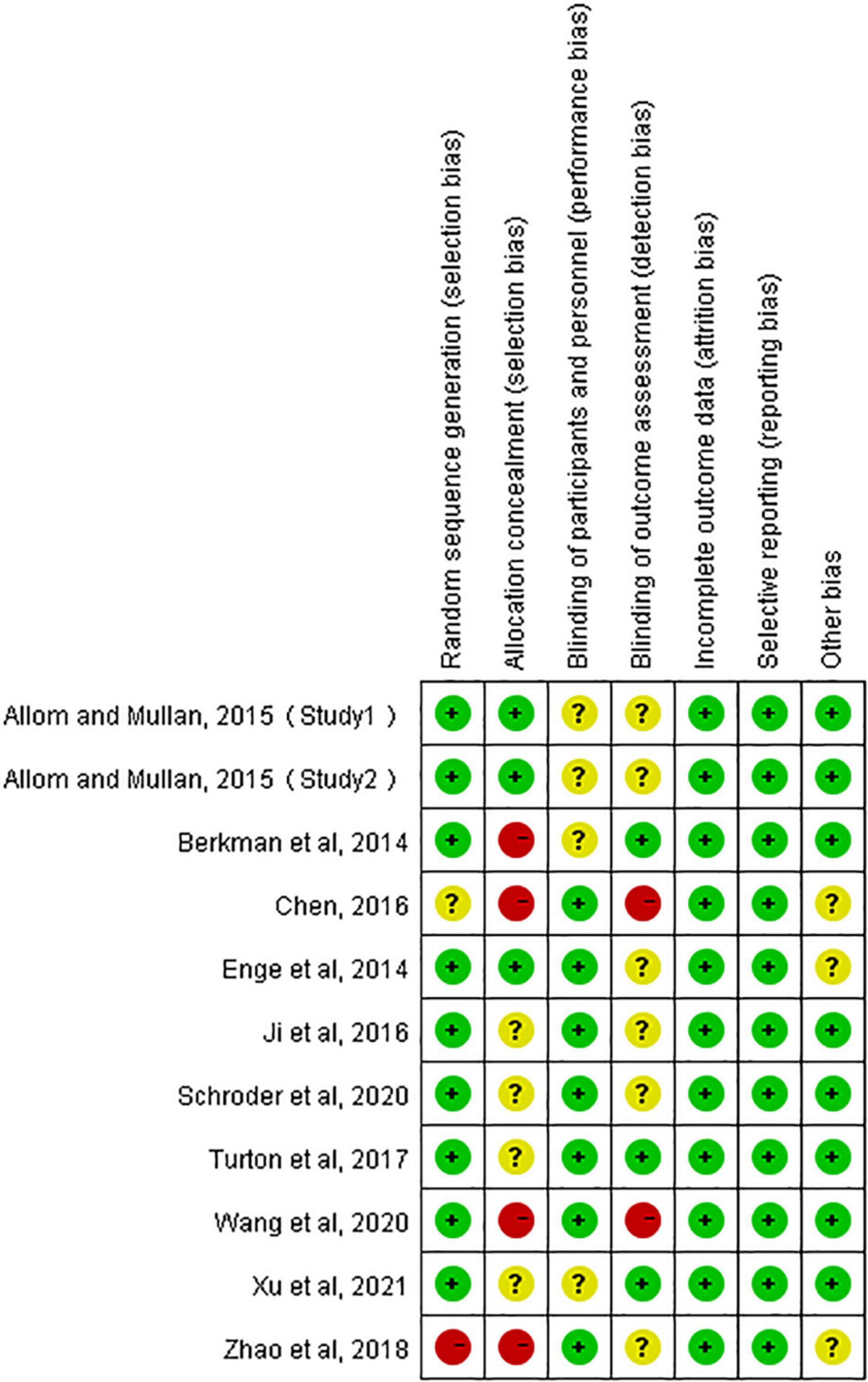
Figure 2. Risk of bias summary of RCTs. +, low risk; −, high risk; ?, unclear risk.
These outcome data were analyzed with the random-effects model, Compared to controls, response inhibition training significantly improved cognitive function in healthy people (SMD, −0.93; 95% CI, −1.56 to −0.30; Z = 2.88, P = 0.004) with high heterogeneity (I2 = 90%), so we conducted subgroup analyses based on different response inhibition training (GNG, Go/no-go tasks; SST, stop-signal tasks; GNG and SST, Go/no-go tasks and stop-signal tasks). The results showed that either GNG training alone (SMD, −2.27; 95% CI, −3.33 to −1.21; Z = 4.18, P < 0.0001) or the combination of both SST and GNG significantly improved cognitive function in healthy adults (SMD, −0.94; 95% CI, −1.33 to −0.56; Z = 4.80, P < 0.0001), whereas SST training alone did not have such an effect (SMD, −0.15; 95% CI, −0.76 to 0.47; Z = 0.47, P = 0.64) (Figure 3).
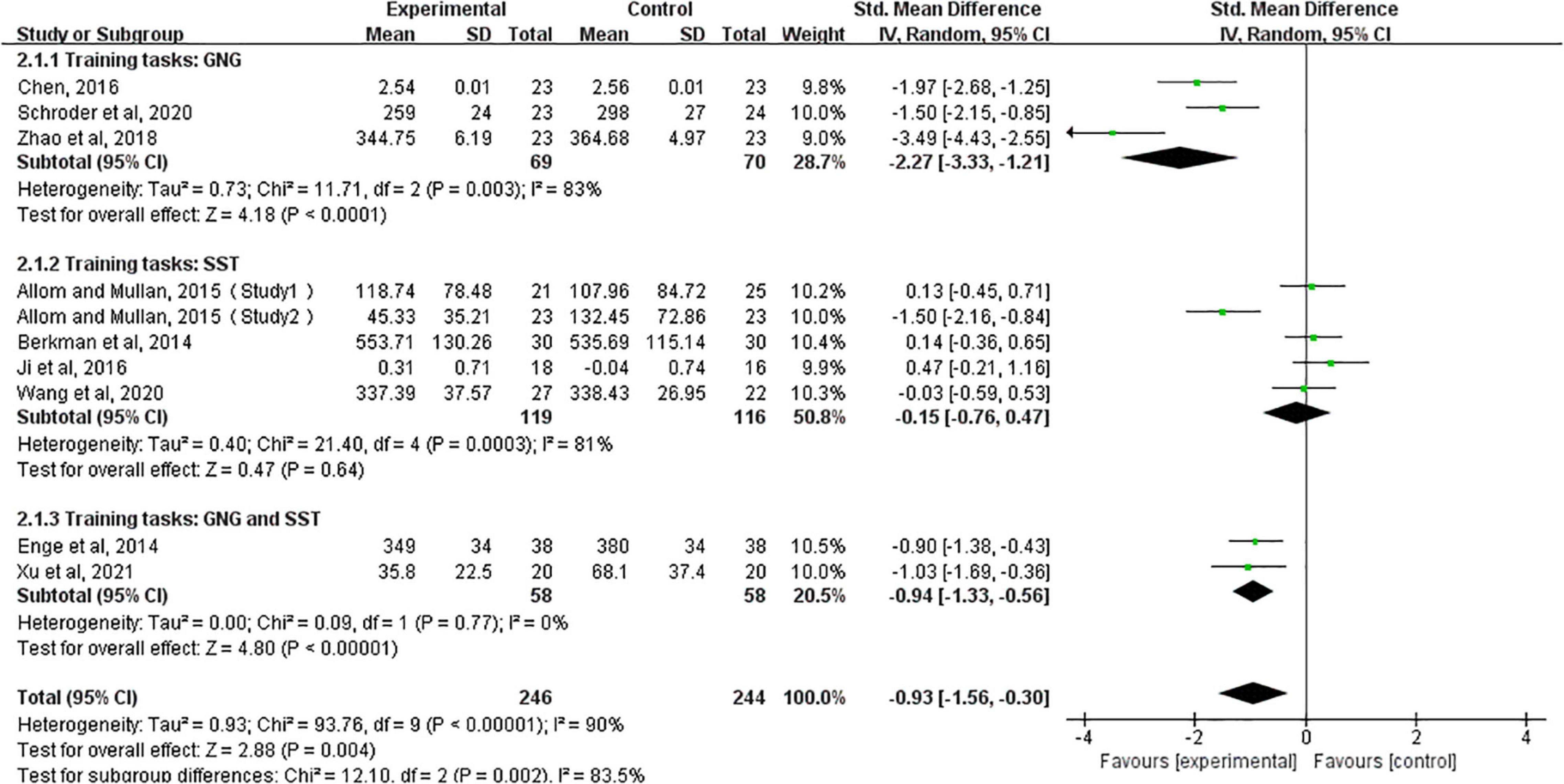
Figure 3. Immediate effects after training, based on subgroup forest plots for different training tasks (GNG, Go/no-go tasks; SST, stop-signal tasks; GNG and SST, Go/no-go tasks and stop-signal tasks).
Since the forest plot showed a large heterogeneity of studies, we used the literature-by-exclusion method for sensitivity analysis and found no literature with significant sources of heterogeneity. The funnel plot showed that the study by Zhao et al. (2018) was far from the mid-line, and the sensitivity analysis did not significantly reduce after removing this article. Therefore, we did not exclude this article (Figure 4).
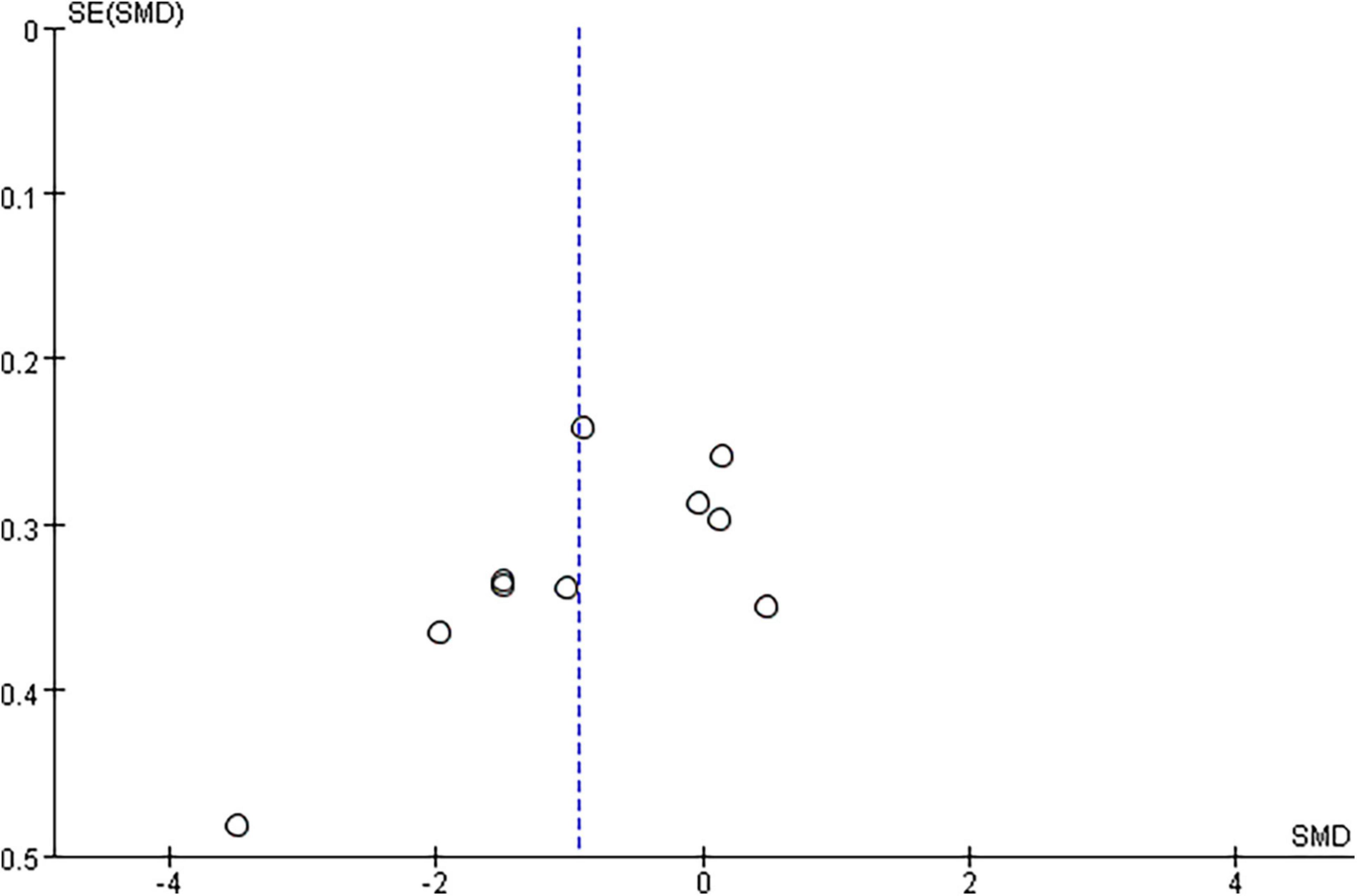
Figure 4. Funnel plots for the effect of Cognitive function. Blue color dotted line, the combined standardized mean difference (SMD) value.
A meta-analysis of long-term follow-up results showed that response inhibition training did not improve cognitive function in healthy adults in the long term (SMD, −0.29; 95% CI, −0.68 to 0.10; Z = 1.45, P = 0.15), but meta-analysis results were highly heterogeneous (I2 = 62%), so we conducted subgroup analyses based on different response inhibition training (GNG, SST, GNG, and SST). The results showed that neither GNG training alone (SMD, −0.25; 95% CI, −0.75 to 0.24; Z = 0.99, P = 0.32) nor SST training alone (SMD, 0.03; 95% CI, −0.42 to 0.48; Z = 0.14, P = 0.89) could improve the cognitive function of healthy adults in the long term. In contrast, the combination of both trainings (SMD, −0.95; 95% CI, −1.46 to −0.45; Z = 3.68, P = 0.0002) can have long-term effects on the improvement of cognitive function in healthy adults (Figure 5).
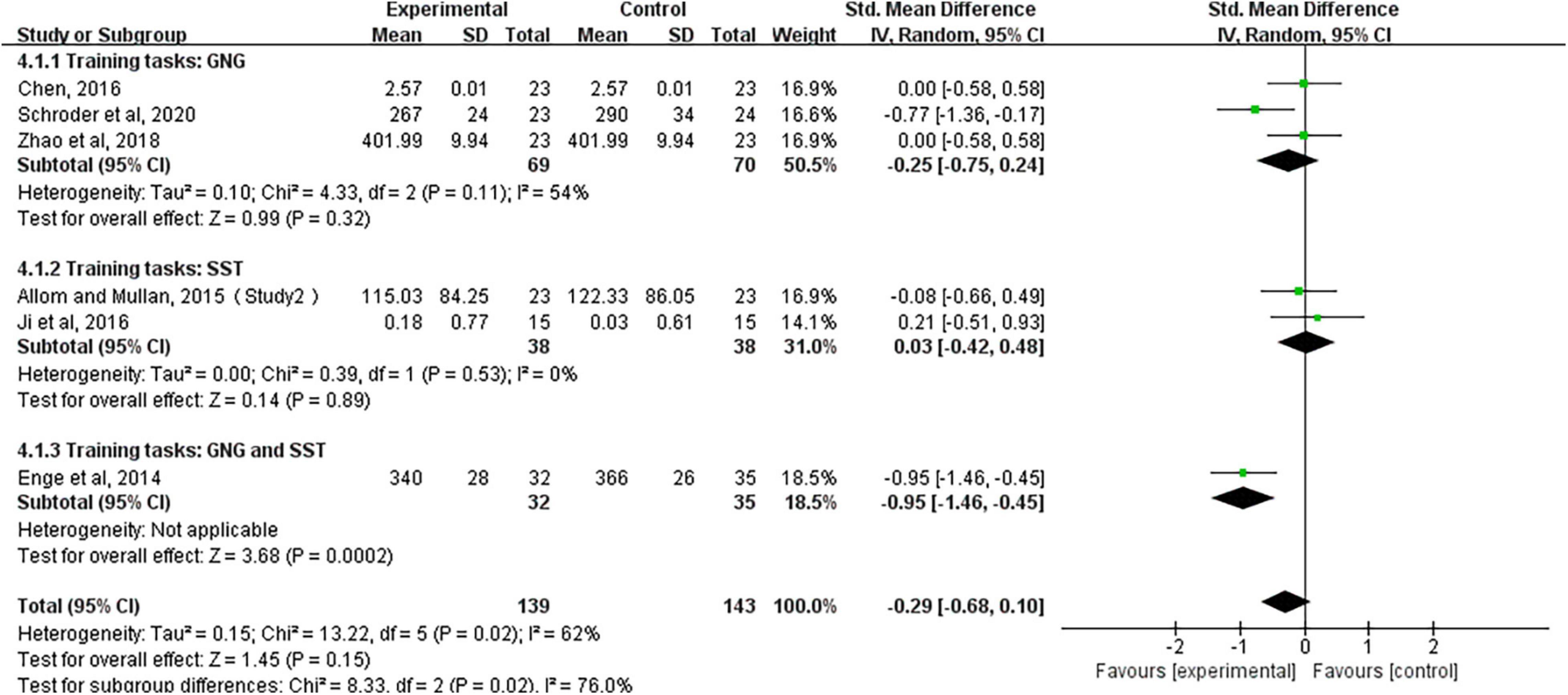
Figure 5. Long-term follow-up effects after training, based on subgroup analysis forest plots for different training tasks (e.g., GNG, Go/no-go tasks; SST, stop-signal tasks; GNG and SST, Go/no-go tasks and stop-signal tasks).
In this analysis, there was no publication bias on the Egger test for cognitive function (P = 0.052) and long-term effects (P = 0.148).
The main results of this systematic review and meta-analysis are as follows: (1) Compared with the control treatments, response inhibition training benefits improving cognitive function in healthy adults but its long-term effects are not significant. (2) Immediate results after treatment showed that either GNG training alone or the combination of both SST and GNG significantly improved cognitive function in healthy adults, whereas SST training alone did not have such an effect. (3) Long-term follow-up efficacy after treatment showed that neither GNG training alone nor SST training alone could improve the cognitive function of healthy adults in the long term. In contrast, the combination of these two training can have a long-term impact on the improvement of healthy adult cognitive functions.
The effectiveness of response inhibition training has been widely debated for a long time. The results of a meta-analysis by Jones et al. (2016) showed that food-specific inhibition training can improve the eating behavior of obese, binge eaters in the short term, and another study by Allom et al. (2015), showed that the Go/No-Go inhibitory control training paradigm can influence the health behavior of excessive smokers and drinkers, but perhaps only in the short term. Neither of the interventions included in the meta-analysis of these two studies was response inhibition training, the intervention used by Allom et al. (2015) was modified response inhibition training, and Jones et al. (2016), nor was the study population entirely normal, including heavy drinkers, overly obese individuals, and addicted smokers. In contrast, there is a lack of research on the effectiveness and long-term effects of response inhibition training in general in improving cognitive function in healthy adults. There is evidence that there is no real training and transfer effect after response inhibition training in healthy adults (Enge et al., 2014). There is also evidence that response inhibition training, in general, improves cognitive function in healthy adults (Ji et al., 2016). Therefore, to resolve this contradiction our search included only unmodified response inhibition training and the inclusion population was selected only from healthy adults to exclude the interference of conditions such as modified response inhibition training, alcohol abuse, excessive smoking, excessive obesity, and to assess the effectiveness and long-term effects of response inhibition training alone on cognitive function improvement in healthy adults.
Overall, training using GNG seems to produce larger effects than training using SST, suggesting that the two tasks may have different mechanisms that lead to different effects on behavior. Indeed, previous studies have confirmed this hypothesis, and the GNG and SST involve different functional bases and neural mechanisms. The Go/No go task and the stop-signal task training involve a functional basis of auto-activated inhibition and top-down control inhibition, respectively, and both have the same neural pathway of the sensory cortex-sub frontal gyrus-basal ganglia-thalamus-primary motor cortex, but the speed of action is different due to the different functional basis involved. Go/No go task training has a stable stimulus-response (S-R) mapping that establishes automatic activation pathways and faster inhibition; stop-signal van task training has a continuously changing S-R mapping that requires top-down cognitive control involvement and slower inhibition (Spierer et al., 2013). Therefore, preliminary evidence found that GNG training influences behavior through bottom-up response inhibition (Verbruggen and Logan, 2008). On the other hand, SST training may contribute to improved reactive control. Allom and Mullan (2015) sought to identify the underlying mechanisms of SST training, arguing that training improves Stroop performance, which is arguably a measure needed to control for response inhibition (Friedman and Miyake, 2004). However, although Stroop scores improved in those who received SST training, this did not translate into improvements in cognitive behavior. It may be the case that GNG and SST affect behavior through automatic and controlled response inhibition, respectively, but training automatic response inhibition may be more effective for behavior change.
In the follow-up efficacy analysis, neither SST nor GNG training alone was found to improve cognitive function in healthy adults, whereas the combination of the two had significant long-term effects. This gives us a new insight that SST combined with GNG training may have a more long-term, robust effect on improving the cognitive function in healthy adults. However, the mechanism needs to be confirmed by further studies. Response inhibition, the ability to regulate and inhibit human behavior so that it immediately responds to the most motivating stimuli in the environment, is a very important human ability. Individuals with strong response inhibition are better able to resist undesirable behaviors, including dietary fat intake and sleep hygiene, as well as addictive behaviors including alcohol consumption and excessive smoking (Friedman and Miyake, 2004; Hofmann et al., 2009; Houben and Wiers, 2010; Nederkoorn et al., 2010; Murphy and Garavan, 2011). Therefore, combined with the results of our study, we believe that SST combined with GNG training has social benefits and economic benefits and is worthy of clinical promotion and application. Moreover, inhibition training is one of the intervention methods to improve cognitive function, it works by reinforcing a certain cognitive process. Therefore, the duration of training certainly affects the long-term effects of inhibition training. Whereas due to the fatigue effect or ceiling effect, we claimed that the effect caused by training time is not increased indefinitely at any time but remains stable after reaching a certain level, and more research is needed to confirm this issue.
Since the forest plot showed a large heterogeneity of studies, we used the literature-by-exclusion method for sensitivity analysis and found no literature with significant sources of heterogeneity. We performed a subgroup analysis based on different intervention methods, and the heterogeneity could be explained by the small number of included literature, the small sample size, national, and geographical differences. Several limitations exist in this meta-analysis. First, the sample sizes of the 10 studies we included were relatively small (n < 100), and more RCTs with large patient samples should be conducted to explore this issue. Although this study collected and analyzed literature through various academic databases, it only evaluated publications written in English and Chinese. Finally, some unpublished and missing data may lead to some bias for the pooled effect.
In conclusion, response inhibition training is a benefit for improving cognitive function in healthy adults but its long-term effects are not significant, whereas the combination of both trainings can have long-term effects on the improvement of cognitive function.
ZC and WC took responsibility for the integrity of data and the accuracy of their analysis. WL and YS contributed to the conception and design of the study and writing of the manuscript. WZ prepared the figures and tables. WL, WM, YS, ZC, WZ, and WC contributed substantially to the literature search, data extraction and analysis, data interpretation, and quality assessment. All authors contributed to the article and approved the submitted version.
This work was supported by the National Key Research and Development Project (2020YFC2005700), Guangzhou Key Research and Development Project (202103000027), Maoming People’s Hospital Doctor Research Launch Project (BS2021010), and High-Level Hospital Construction Research Project of Maoming People’s Hospital.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Allom, V., and Mullan, B. J. (2015). Two inhibitory control training interventions designed to improve eating behaviour and determine mechanisms of change. Appetite 89, 282–290. doi: 10.1016/j.appet.2015.02.022
Allom, V., Mullan, B., and Hagger, M. J. (2015). Does inhibitory control training improve health behaviour? A meta-analysis. Health Psychol. Rev. 10, 1–38. doi: 10.1080/17437199.2015.1051078
Aron, A. R., Durston, S., Eagle, D. M., Logan, G. D., and Stuphorn, V. J. (2007). Converging evidence for a fronto-basal-ganglia network for inhibitory control of action and cognition. J. Neurosci. 27, 11860–11864. doi: 10.1523/JNEUROSCI.3644-07.2007
Aron, A. R., Robbins, T. W., and Poldrack, R. A. J. (2004). Inhibition and the right inferior frontal cortex: one decade on. Trends Cogn. Sci. 8, 170–177. doi: 10.1016/j.tics.2004.02.010
Baumeister, R. F. (2014). Self-regulation, ego depletion, and inhibition. Neuropsychologia 65, 313–319. doi: 10.1016/j.neuropsychologia.2014.08.012
Berkman, E. T., Kahn, L. E., and Merchant, J. S. (2014). Training-induced changes in inhibitory control network activity. J. Neurosci 34, 149–157. doi: 10.1523/JNEUROSCI.3564-13.2014
Bickel, W. K., Jarmolowicz, D. P., Mueller, E. T., Gatchalian, K. M., and Mcclure, S. M. (2012). Are executive function and impulsivity antipodes? A conceptual reconstruction with special reference to addiction. Psychopharmacology (Berl) 221, 361–387. doi: 10.1007/s00213-012-2689-x
Brydges, C. R., Clunies-Ross, K., Clohessy, M., Lo, Z. L., Nguyen, A., Rousset, C., et al. (2012). Dissociable components of cognitive control: an event-related potential (erp) study of response inhibition and interference suppression. PLoS One 7:e34482. doi: 10.1371/journal.pone.0034482
Chen, L. (2016). Effectiveness Of Response Inhibition Training And Its Transfer Effect In Children And Adults. Lanzhou: Northwest Normal University.
Donders, F. C. (1969). On the speed of mental processes. Acta Psychol. (Amst) 30, 412–431. doi: 10.1016/0001-6918(69)90065-1
Enge, S., Behnke, A., Fleischhauer, M., Küttler, L., Kliegel, M., and Strobel, A. J. (2014). No evidence for true training and transfer effects after inhibitory control training in young healthy adults. J. Exp. Psychol. Learn. Mem. Cogn. 40:987. doi: 10.1037/a0036165
Friedman, N. P., and Miyake, A. (2004). The relations among inhibition and interference control functions: a latent-variable analysis. J. Exp. Psychol. Gen. 133, 101–135. doi: 10.1037/0096-3445.133.1.101
Groman, S. M., James, A. S., and Jentsch, J. D. (2009). Poor response inhibition: At the nexus between substance abuse and attention deficit/hyperactivity disorder. Neurosci. Biobehav. Rev. 33, 690–698. doi: 10.1016/j.neubiorev.2008.08.008
Higgins, J. P. T., and Green, S. (2008). Cochrane Handbook for Systematic Reviews of Interventions: Cochrane Book Series. Hoboken, NJ: John Wiley & Sons, doi: 10.1002/9780470712184.ch1
Higgins, J. P., and Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Stat. Med. 21, 1539–1558. doi: 10.1002/sim.1186
Higgins, J., Thompson, S. G., Deeks, J. J., and Altman, D. G. (2008). Cochrane handbook for systematic reviews of interventions version 5.1.0. Cochrane Collaboration 5:S38. doi: 10.1016/j.jhsa
Hofmann, W., Friese, M., and Roefs, A. (2009). Three ways to resist temptation: the independent contributions of executive attention, inhibitory control, and affect regulation to the impulse control of eating behavior ✩. J. Exp. Soc. Psychol. 45, 431–435. doi: 10.1016/j.jesp.2008.09.013
Houben, K., and Jansen, A. (2011). Training inhibitory control. A recipe for resisting sweet temptations. Appetite 56, 345–349. doi: 10.1016/j.appet.2010.12.017
Houben, K., and Wiers, R. W. (2010). Response inhibition moderates the relationship between implicit associations and drinking behavior. Alcohol. Clin. Exp. Res. 33, 626–633. doi: 10.1111/j.1530-0277.2008.00877.x
Ji, Y., Wang, J., Chen, T., Du, X., and Zhan, Y. (2016). Plasticity of inhibitory processes and associated far-transfer effects in older adults. Psychol. Aging 31, 415–429. doi: 10.1037/pag0000102
Jones, A., Di Lemma, L. C., Robinson, E., Christiansen, P., Nolan, S., Tudur-Smith, C., et al. (2016). Inhibitory control training for appetitive behaviour change: a meta-analytic investigation of mechanisms of action and moderators of effectiveness. Appetite 97, 16–28. doi: 10.1016/j.appet.2015.11.013
Kooijmans, R., Scheres, A., and Oosterlaan, J. (2000). Response inhibition and measures of psychopathology: a dimensional analysis. Child Neuropsychol. 6, 175–184. doi: 10.1076/chin.6.3.175.3154
Lawrence, N. S., Verbruggen, F., Morrison, S., Adams, R. C., and Chambers, C. D. (2015). Stopping to food can reduce intake. Effects of stimulus-specificity and individual differences in dietary restraint. Appetite 85, 91–103. doi: 10.1016/j.appet.2014.11.006
Logan, G. D., Cowan, W. B., and Davis, K. A. (1984). On the ability to inhibit simple and choice reaction time responses: a model and a method. J. Exp. Psychol. Hum. Percept. Perform. 10:276. doi: 10.1037//0096-1523.10.2.276
Maguire, D. R., and France, C. P. (2019). Effects of amphetamine, methylphenidate, atomoxetine, and morphine in rats responding under an adjusting stop signal reaction time task. Psychopharmacology (Berl) 236, 1959–1972. doi: 10.1007/s00213-019-5183-x
Miyake, A., Friedman, N. P., Emerson, M. J., Witzki, A. H., Howerter, A., and Wager, T. D. (2000). The unity and diversity of executive functions and their contributions to complex “Frontal Lobe” tasks: a latent variable analysis. Cogn. Psychol. 41, 49–100. doi: 10.1006/cogp.1999.0734
Moher, D., Liberati, A., Tetzlaff, J., and Altman, D. G. (2009). Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement (reprinted from annals of internal medicine). PLoS Med. 6:e1000097. doi: 10.1371/journal.pmed.1000097
Muraven, M. (2010). Building self-control strength: practicing self-control leads to improved self-control performance. J. Exp. Soc. Psychol. 46, 465–468. doi: 10.1016/j.jesp.2009.12.011
Murphy, P., and Garavan, H. (2011). Cognitive predictors of problem drinking and AUDIT scores among college students. Drug Alcohol. Depend. 115, 94–100. doi: 10.1016/j.drugalcdep.2010.10.011
Nederkoorn, C., Houben, K., Hofmann, W., Roefs, A., and Jansen, A. (2010). Control yourself or just eat what you like? Weight gain over a year is predicted by an interactive effect of response inhibition and implicit preference for snack foods. Health Psychol. 29, 389–393. doi: 10.1037/a0019921
Schroder, E., Dubuson, M., Dousset, C., Mortier, E., Kornreich, C., and Campanella, S. (2020). Training inhibitory control induced robust neural changes when behavior is affected: a follow-up study using cognitive event-related potentials. Clin. EEG Neurosci. 51, 303–316. doi: 10.1177/1550059419895146
Spierer, L., Chavan, C. F., and Manuel, A. L. (2013). Training-induced behavioral and brain plasticity in inhibitory control. Front. Hum. Neurosci. 7:427. doi: 10.3389/fnhum.2013.00427
Turton, R., Nazar, B. P., Burgess, E. E., Lawrence, N. S., and Hirsch, C. R. (2017). To go or not to go: a proof of concept study testing food-specific inhibition training for women with eating and weight disorders: food-specific inhibition training and eating disorders. Eur. Eat. Disord. Rev. 26, 11–21. doi: 10.1002/erv.2566
van Koningsbruggen, G. M., Veling, H., Stroebe, W., and Aarts, H. (2013). Comparing two psychological interventions in reducing impulsive processes of eating behaviour: effects on self-selected portion size. Br. J. Health Psychol. 19, 767–782. doi: 10.1111/bjhp.12075
Verbruggen, F., and Logan, G. D. (2008). Automatic and controlled response inhibition: associative learning in the go/no-go and stop-signal paradigms. J. Exp. Psychol. Gen. 137, 649–672. doi: 10.1037/a0013170
Verbruggen, F., Best, M., Bowditch, W. A., Stevens, T., and Mclaren, I. (2014). The inhibitory control reflex. Neuropsychologia 65, 263–278. doi: 10.1016/j.neuropsychologia.2014.08.014
Wang, Y., Li, K., Xiaosong, G., and Yifei, C. (2020). Training effects and transfer effects of immediate feedback-based response inhibition training on executive function in adolescents and adults. Psychol. News 52, 1212–1223. doi: 10.3724/SP.J.1041.2020.01212
Xu, P., Wu, D., Zhou, Y., Wu, J., and Xiao, W. (2021). An event-related potential (ERP) study of the transfer of response inhibition training to interference control. Exp. Brain Res. 239, 1327–1335. doi: 10.1007/s00221-021-06055-2
Keywords: response inhibition training, meta-analysis, randomized controlled trial, long-term effects, healthy adults
Citation: Li W, Shang Y, Zhuang W, Mai W, Cheng W and Chen Z (2022) Effectiveness of Response Inhibition Training and Its Long-Term Effects in Healthy Adults: A Systematic Review and Meta-Analysis. Front. Neurosci. 16:813975. doi: 10.3389/fnins.2022.813975
Received: 12 November 2021; Accepted: 02 May 2022;
Published: 30 May 2022.
Edited by:
Notger G. Müller, University of Potsdam, GermanyReviewed by:
Qilin Yang, The Second Affiliated Hospital of Guangzhou Medical University, ChinaCopyright © 2022 Li, Shang, Zhuang, Mai, Cheng and Chen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wenwen Cheng, Y2hlbmd3d2N5QDE2My5jb20=; Zhuoming Chen, dGNoem1AMjFjbi5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.