 Chensheng Pan
Chensheng Pan Wenzhe Sun
Wenzhe Sun Yan Lan
Yan Lan Zhou Zhu
Zhou Zhu
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurosci. , 06 April 2022
Sec. Brain Imaging Methods
Volume 16 - 2022 | https://doi.org/10.3389/fnins.2022.812410
This article is part of the Research Topic Multi-Dimensional Characterization of Neuropsychiatric Disorders View all 11 articles
Poststroke depression (PSD), affecting about one-third of stroke survivors, exerts significant impact on patients’ functional outcome and mortality. Great efforts have been made since the 1970s to unravel the neuroanatomical substrate and the brain-behavior mechanism of PSD. Thanks to advances in neuroimaging and computational neuroscience in the past two decades, new techniques for uncovering the neural basis of symptoms or behavioral deficits caused by focal brain damage have been emerging. From the time of lesion analysis to the era of brain networks, our knowledge and understanding of the neural substrates for PSD are increasing. Pooled evidence from traditional lesion analysis, univariate or multivariate lesion-symptom mapping, regional structural and functional analyses, direct or indirect connectome analysis, and neuromodulation clinical trials for PSD, to some extent, echoes the frontal-limbic theory of depression. The neural substrates of PSD may be used for risk stratification and personalized therapeutic target identification in the future. In this review, we provide an update on the recent advances about the neural basis of PSD with the clinical implications and trends of methodology as the main features of interest.
Poststroke depression (PSD) is a common complication of stroke, involving about 29% of patients at any time within 5 years poststroke (Ayerbe et al., 2013). PSD is associated with heavier healthcare burden, poorer functional outcome, and higher long-term mortality in stroke survivors (Robinson et al., 1986; Ghose et al., 2005; Jia et al., 2006; Ayerbe et al., 2013; Bartoli et al., 2013; Kutlubaev and Hackett, 2014). To aid in early prediction and effective intervention for PSD, its etiology and mechanisms need to be scrutinized. Based on accumulating evidence, it is generally believed that PSD has underlying neurobiological causes and is not only a psychosocial response to the new disability or stressful life event (Folstein et al., 1977; Towfighi et al., 2017; Mayman et al., 2021). The association between lesion location and PSD first reported in the 1970s (Robinson et al., 1975, 1983; Robinson and Price, 1982), although extensively investigated as a potential biological factor of PSD, is still of considerable debate (Nickel and Thomalla, 2017; Towfighi et al., 2017). Most of those studies were of traditional design with relatively low spatial accuracy for visual lesion localization (Nickel and Thomalla, 2017). Until 2003, a new technique called voxel-based lesion-symptom mapping (VLSM) was developed to test the lesion–behavior correlation at the voxel level and has been widely used to identify the neural substrates of symptoms after focal brain damage such as PSD, poststroke cognitive impairment, poststroke dysphagia, and stroke-related myocardial injury (Bates et al., 2003; Ay et al., 2006; Kim et al., 2017; Hess et al., 2021; Weaver et al., 2021a). Moreover, there is a growing consensus that the rough lesion location used in traditional lesion analysis and the spatial topography information used in VLSM only represent the “tip of the iceberg”: a surface-level depiction of the lesion largely blind to its impact on the underlying extensive brain networks (Catani et al., 2012; Fox, 2018). The brain network dysfunction caused by a given stroke lesion, instead of the lesion itself, might be the key neural substrate of poststroke symptoms especially when patients with the same symptom have lesions in various brain regions with little lesion overlap (Fox, 2018). Thanks to advances in neuroimaging techniques and statistical methodologies in the past two decades, lesion-symptom inference in high spatial resolution, with robust statistics and from the perspective of the human connectome, can be performed and new evidence for the neural substrates of PSD, beyond those findings from traditional studies, is emerging. In this review, we provide a brief summary of traditional studies and an update on the latest advances about the neural basis of PSD, which may shed light on the etiology, prediction, therapeutic target identification, and future research directions for PSD.
The Diagnostic Statistical Manual of Mental Disorders-5 (DSM-5), as gold standard for PSD diagnosis, defines PSD as “depressive disorder due to another medical condition” with depressive features, major depressive-like episode, or mixed-mood features (American Psychiatric Association, 2013). Some aspects in DSM-5 criteria, such as “disturbance is the direct pathophysiological consequence of another medical condition,” are almost impossible to prove in clinical practice (American Psychiatric Association, 2013). Therefore, the diagnosis of PSD relies on a thorough clinical interview with careful exploration of presenting symptoms and is commonly assisted by the use of screening tools (specifically the depression rating scales validated in PSD screening) (Chun et al., 2021). Although multiple depression scales have been applied and compared in previous studies, the optimal screening tool for PSD remains undetermined (Towfighi et al., 2017). One meta-analysis reported three scales as promising options with relatively high sensitivity and specificity in PSD screening: Center of Epidemiological Studies-Depression Scale (CESD), Hamilton Depression Rating Scale (HDRS), and Patient Health Questionnaire (PHQ)-9, compared with other scales including Geriatric Depression Scale (GDS), Hospital Anxiety and Depression Scale (HADS), and PHQ-2 (Meader et al., 2014). Another study found that HDRS, Beck Depression Inventory (BDI), and Clinical Global Impression (CGI) assessment by professionals showed similar performance in PSD screening (Berg et al., 2009). Of note, the optimal rating scale along with the optimal cutoff value for PSD diagnosis may vary across different stages after stroke (Berg et al., 2009), which warrants further investigation. The methods for PSD diagnosis or measurement in previous studies on the neural substrates of PSD are summarized in Table 1.
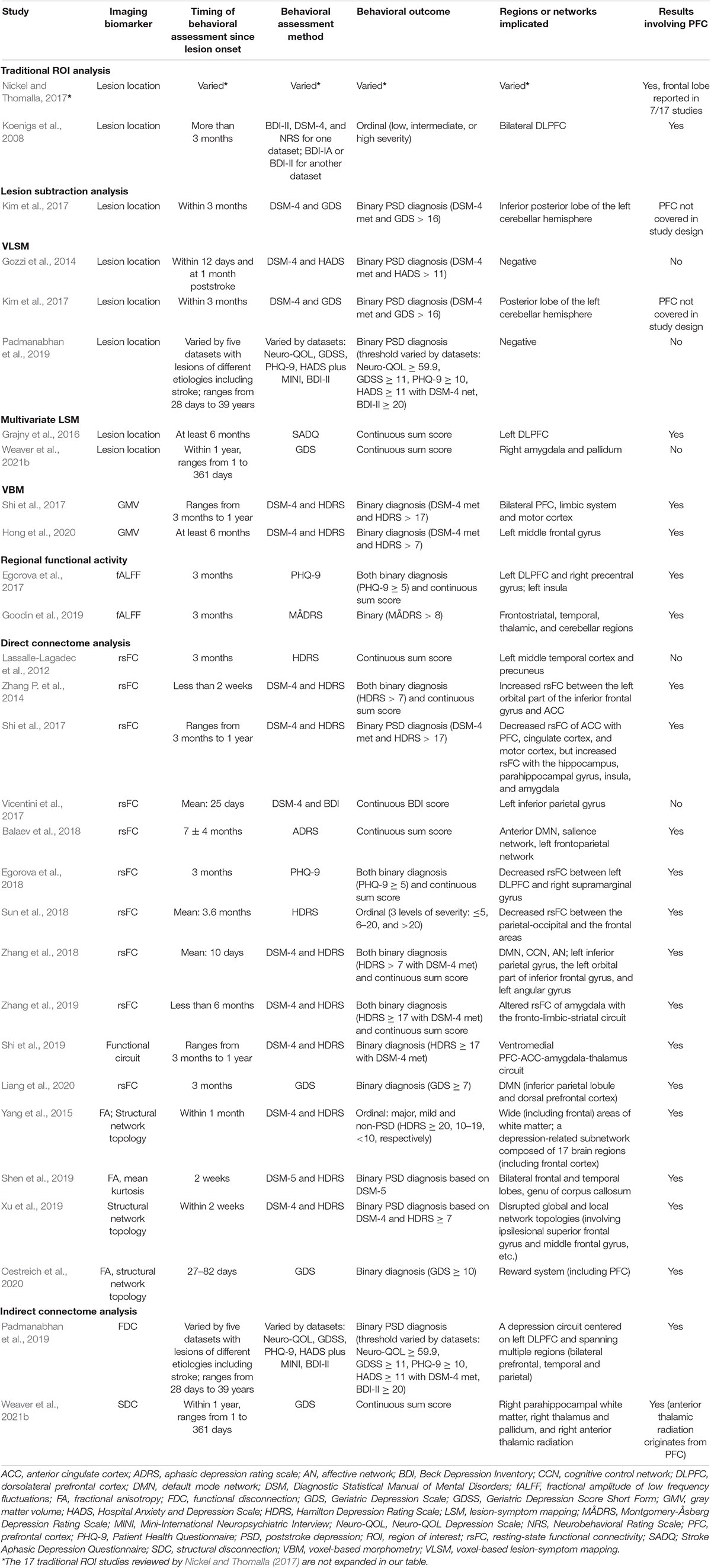
Table 1. Study design and findings for studies on neural substrates of PSD.
More recently, researchers on mental disorders tend to define depressive disorders as a complex symptom network. Both DSM-5 criteria and the sum score of a depression rating scale are based on the traditional “common cause” theory, assuming that depression as an entity causes various symptoms and these symptoms are interchangeable and diagnostically equivalent so that the number or severity of symptoms can be simply added up (Borsboom, 2008; Borsboom and Cramer, 2013; Fried and Cramer, 2017). The depressive symptoms, however, actually interact with each other in complex ways, which has long been common knowledge among clinicians (Borsboom, 2008; Borsboom and Cramer, 2013; Fried and Cramer, 2017). In the psychopathological network theory, mental disorders are conceptualized as dynamic and complex networks of symptoms influencing each other by creating causal pathways and feedback loops (e.g., depressed mood - > insomnia - > fatigue - > depressed mood, in depressive disorders) (Borsboom, 2008; Borsboom and Cramer, 2013; Fried and Cramer, 2017). Depressive symptom networks have been well established in neurologically healthy populations (van Borkulo et al., 2015; Belvederi Murri et al., 2020), and interactions among depressive symptoms may also exist in the stroke population (Ashaie et al., 2021). One recent study modeled poststroke depressive symptoms at three timepoints (discharge and 3 and 12 months after discharge) as networks in which depressed mood was consistently identified as a central symptom and might be responsible for triggering or sustaining the rest of symptoms via symptom–symptom interactions (Ashaie et al., 2021). Interestingly, the network structure and connectivity of poststroke depressive symptoms might vary across time after stroke (Ashaie et al., 2021). Accumulating evidence suggests that certain biological processes (e.g., inflammation and focal brain damage) may not be equally related to all depressive symptoms (Moriarity et al., 2022). Investigating risk factors and biomarkers for individual depressive symptoms has become a new research paradigm (Fried et al., 2014, 2020; Jokela et al., 2016; White et al., 2017; Triolo et al., 2021; Moriarity et al., 2022).
The majority of the evidence about the association between lesion location and PSD is derived from traditional region-of-interest (ROI) analysis in which the lesion is assigned to overlap with a region or not by reviewing the scan without manual segmentation, followed by comparison for the prevalence of PSD in populations defined by the presence or absence of involvement of the ROI. The results from traditional studies before 2017 have been reviewed elsewhere and will not be redundantly described here (Nickel and Thomalla, 2017). In brief, the earliest notion that depression was more likely to be associated with left than with right hemispheric strokes and with lesions in the left anterior brain than with other regions (Robinson and Price, 1982; Starkstein et al., 1987) was not supported by other studies: some concluded with the association between PSD and right hemispheric strokes (MacHale et al., 1998; Wei et al., 2015), while others ended up with no association at all between lesion location and PSD (Carson et al., 2000; Kutlubaev and Hackett, 2014). No conclusion could be drawn regarding the role of lesion location (laterality, anterior–posterior gradient, within specific brain regions, etc.) in the etiology of PSD based on traditional evidence (Nickel and Thomalla, 2017). The traditional ROI approach has its intrinsic limitations. First, the association between the ROI and PSD might be just a coincidence due to the coexisting involvement of other brain regions with common blood supply (so-called consistent error) (Ay et al., 2006; Mah et al., 2014). Second, the traditional approach dichotomizes the study sample with respect to involvement of a relatively large ROI, which precludes point localizations and may result in false negative results due to improper sampling or counterbalancing of effects among multiple small regions within a large ROI (Ay et al., 2006). Another traditional approach called lesion subtraction analysis is also used for lesion-symptom inference (Rorden and Karnath, 2004). Based on the hypothesis that the causative neural substrate is more frequently involved in patients with a specific symptom than in those without, the voxel-wise lesion incidence map of the non-PSD group is subtracted from that of the PSD group showing brain regions more frequently involved in PSD. One lesion subtraction study identified left cerebellar stroke to be correlated with PSD, which was consistent with the result of a subsequent VLSM analysis (Kim et al., 2017). However, the lesion subtraction plot alone may only provide a descriptive result of the possible neural substrate due to lack of statistical tests.
It is not surprising to get inconsistent results from traditional studies (and some other methods in the following text) given the heterogeneity in depression rating scales (Table 1), diverse timepoints of depression assessment since stroke onset (Table 1), small sample size, selection bias (e.g., exclusion for aphasia), different definitions of lesion location, inadequate imaging quality, combining lesions of various etiologies into a single analysis, and so on (Robinson and Jorge, 2016; Nickel and Thomalla, 2017; Towfighi et al., 2017). Of note, the interval between stroke onset and depression assessment might be an important factor exerting influence on the results of the traditional approach (and other methods as well). A longitudinal study focusing on depression at specific stages of stroke found that the association of PSD with left anterior lesions appeared to be a transient phenomenon restricted to the acute stage and the laterality tended to reverse to the right hemisphere in the long-term follow-up (Astrom et al., 1993). Another independent study also suggested that only in-hospital depression was associated with lesions in the left anterior hemisphere and depression at 1–2 years poststroke was associated with right-hemisphere lesion volume and lesion proximity to the occipital pole (Shimoda and Robinson, 1999). A meta-analysis with stratification by time of assessment showed that the association between right hemispheric stroke and PSD only existed at the subacute stage of stroke (Wei et al., 2015). It is conceivable that the neuroanatomic substrates of PSD might change over time or there might be distinct mechanisms for PSD at different stages of stroke (Astrom et al., 1993; Shimoda and Robinson, 1999). Therefore, studies mixing patients of various stages poststroke tend to produce inconsistent and unreliable results and performing PSD assessments at homogeneous stages after stroke might be helpful in future studies. Although inconclusive, some researchers still believe that there is an association between left frontal strokes and PSD within the first 2 months after stroke based on some converging evidence (Astrom et al., 1993; Shimoda and Robinson, 1999; Rajashekaran et al., 2013; Robinson and Jorge, 2016). The role of the left prefrontal cortex (PFC) in PSD was further supported by multiple clinical trials showing that repetitive transcranial magnetic stimulation (rTMS) targeted at the left dorsolateral PFC (DLPFC) can significantly alleviate the symptoms of PSD and vascular depression (Jorge et al., 2004; McIntyre et al., 2016; Gu and Chang, 2017; Shen et al., 2017; Frey et al., 2020).
The general procedure of VLSM analysis involves lesion segmentation on computed tomography (CT) or magnetic resonance imaging (MRI) scans, spatial normalization of lesion masks, mass-univariate statistical tests voxel by voxel for the association between lesion status at a given voxel and presence or severity of the symptom of interest, correction for multiple comparisons to control false positive rates, and interpretation of the significant clusters. Three lesion-symptom mapping (LSM) studies on PSD before 2017 did not provide consistent results, as described in the previous review (Nickel and Thomalla, 2017). The first study showed negative results, and another two identified lesions in the left cerebellum and left DLPFC, respectively, as the neural substrates of PSD (Gozzi et al., 2014; Grajny et al., 2016; Kim et al., 2017). These are considered as pilot exploratory LSM studies with small sample size (n < 100) and therefore low statistical power (Nickel and Thomalla, 2017). Another study in 2019 which performed VLSM in five datasets (total n = 461) with focal brain damage of various etiologies (including stroke) failed to find any lesion location to be correlated with depression after brain damage (but did identify a functional depression circuit via connectome analysis) (Padmanabhan et al., 2019). Generally, only voxels with lesion incidence above a certain threshold (e.g., at least 10 patients or 5% of patients, indicating sufficient lesion affection) could be included in VLSM to ensure reasonable statistical power and anatomical validity (Medina et al., 2010; Sperber and Karnath, 2017). Small sample size tends to provide insufficient lesion coverage, leaving those infrequently involved brain regions with lower statistical power or being unexplored (Kimberg et al., 2007; Gozzi et al., 2014). Indeed, a large sample size will be required if we want to perform whole-brain VLSM analysis without predefined ROIs, considering the recent evidence that about 3,000 subjects were needed to achieve a lesion coverage of 86% of total brain voxels (Weaver et al., 2021a). The original VLSM approach with mass-univariate tests still suffers the aforementioned consistent error originating from collateral vasculature (Mah et al., 2014; Karnath et al., 2018). The latest machine learning-based multivariate LSM approaches, believed to be able to overcome this limitation, seem as promising alternatives in future studies (Mah et al., 2014; Karnath et al., 2018). One multivariate LSM study mentioned above applied support vector regression-based LSM (SVR-LSM) and found the association between lesions in the left DLPFC and severity of poststroke depressive symptoms (PSDS; Zhang Y. et al., 2014; Grajny et al., 2016). Another recent SVR-LSM study found that infarcts in the right amygdala, right pallidum, and right hippocampus were associated with PSDS (Weaver et al., 2021b). External validation confirmed the association between infarcts in the right amygdala and pallidum, but not the right hippocampus, and PSDS (Weaver et al., 2021b). Another latest method named multivariate sparse canonical correlations technique (SCCAN), generally superior to the univariate approach at small sample sizes, may also be recommended in future studies (Pustina et al., 2018). Some neural substrates unlikely to be identified with the univariate approach may be unveiled with multivariate LSM which integrates lesion information from multiple voxels simultaneously in lesion-symptom inference (Karnath et al., 2018). Multivariate approaches are preferred if we have good reasons to assume that the symptom of interest is represented in an extensively distributed brain network, as in these cases the ability of the univariate approach to detect all of the network modules may be limited (Karnath et al., 2018; Xu et al., 2018). Based on current LSM studies showing non-convergent results, the role of lesion location in the etiology of PSD still warrants further investigation with large datasets and advanced methodologies.
Gray matter atrophy may serve as a transdiagnostic neural substrate for various mental illnesses (Goodkind et al., 2015). Voxel-based morphometry (VBM) is able to evaluate the intergroup difference of gray matter volume (GMV) at the voxel level using high-resolution structural MRI (sMRI; Ashburner and Friston, 2000). The procedure of VBM involves spatially normalizing and segmenting sMRI images into the same standard space (Ashburner and Friston, 2000). The gray matter segments are smoothed so that each voxel represents the average of itself and its neighbors (Ashburner and Friston, 2000). Parametric statistical tests are performed at the voxel level, followed by corrections for multiple comparisons with the theory of random fields (Ashburner and Friston, 2000). One study performed VBM analysis in 30 first-ever ischemic frontal stroke patients showing that decreased GMV in PSD was mainly observed in the prefrontal-limbic system and motor cortex compared with non-PSD patients (Shi et al., 2017). The involved limbic structures were mainly located in the right hemisphere, and the PFC showed a decreased GMV in both hemispheres (Shi et al., 2017). Recent evidence from another VBM study in 23 PSD and 33 non-PSD subcortical stroke patients suggested that the PSD group had significantly decreased GMV in the left middle frontal gyrus (MFG; Hong et al., 2020). Together with the clinical-demographic variables, the MFG’s GMV prediction model was able to distinguish PSD from non-PSD with high sensitivity and specificity (Hong et al., 2020). The results from VBM studies are in accordance with the aforementioned role of the frontal cortex in PSD, as well as the frontal-limbic model which is well-recognized in depressive disorders such as major depressive disorder (MDD) and vascular depression (Taylor et al., 2013; Lai, 2021).
Resting-state functional MRI (rs-fMRI), reflecting brain activation via blood oxygenation level-dependent (BOLD) signal, has been widely used in research of neuropsychiatric disorders including stroke and depression (Ovadia-Caro et al., 2014; Oathes et al., 2015). Several measurements, such as amplitude of low-frequency fluctuations (ALFF) and fractional ALFF (fALFF), were developed to reflect the characteristics of spontaneous brain activity within a brain region (Zang et al., 2007; Zou et al., 2008). One rs-fMRI study performed in 64 participants at 3 months poststroke found significantly higher fALFF in PSD in the left DLPFC and the right precentral gyrus compared with non-PSD patients and a significant association between higher PSD severity and higher fALFF in the left insula (Egorova et al., 2017). The aberrant regional brain activity could be a more sensitive feature than lesion location and volume to characterize PSD in small samples (Egorova et al., 2017). Another rs-fMRI study identified a significant correlation between PSD severity and fALFF in frontostriatal, temporal, thalamic, and cerebellar regions (Goodin et al., 2019). These fMRI results also provided evidence for the role of the frontal-limbic system in PSD. However, functional neuroimaging is time-consuming and vulnerable to head motions which is difficult to control in stroke patients (Ovadia-Caro et al., 2014; Fox, 2018). Another major limitation of fMRI studies is that they can hardly be used for causal inference (Fox, 2018). Unlike visual or voxel-based lesion analyses which have a clear temporal order between lesion and PSD, fMRI analysis typically has neuroimaging performed at the time of or after PSD diagnosis for a case–control comparison. Therefore, whether this functional difference between PSD and non-PSD is causative, or whether it is a reactive or adaptive alteration to depression, remains elusive (Fox, 2018). The results from fMRI analyses should be regarded as correlation rather than causation (Fox, 2018). Future studies with longitudinal design might unravel the potential causal relationship between gray matter atrophy, regional functional abnormality, and development of PSD.
Based on large amounts of lesion studies, the lesions of PSD patients fail to overlap in a single brain region. It has long been discovered that some neuropsychiatric symptoms can result from dysfunctions of anatomically intact brain regions which are distant but connected to the lesion (“diaschisis” phenomenon) (Carrera and Tononi, 2014). In the era of brain networks and human connectome, we have good reasons to assume that PSD might be a complex disconnection syndrome resulting from disruption of networks of interacting brain regions (Gong and He, 2015). There are two types of brain connectivity being explored. Functional connectivity (FC) is measured by the correlation of the fMRI BOLD time series between brain regions, and structural (or anatomical) connectivity (SC) can be derived from diffusion tensor imaging (DTI) in which water diffuses more freely along white matter fibers than across them (Fox and Raichle, 2007; Jbabdi et al., 2015). Brain networks can be analyzed at different levels: microscale (single neuron and synapses), mesoscale (neuronal groups), and macroscale (brain regions and inter-region pathways) (Sporns et al., 2005). Quantitative analysis, especially graph theory analysis, can reveal important features of complex networks such as highly connected hubs, modularity, and small-world topology (Bullmore and Sporns, 2009; He and Evans, 2010). Importantly, these quantifiable network features were found to change in normal development, aging, and various neuropsychiatric disorders (He and Evans, 2010; Menon, 2011; Ovadia-Caro et al., 2014). With both FC and SC techniques, complex symptoms like PSD that transcend localization to single brain regions may be mapped to widely distributed brain networks.
Typically, the FC is directly derived from each patient’s fMRI scans. One study in frontal stroke patients performed connectivity analysis with the anterior cingulate cortex (ACC) as the seed found decreased resting-state FC (rsFC) with the PFC, cingulate cortex, and motor cortex, but increased rsFC with the hippocampus, parahippocampal gyrus, insula, and amygdala, in the PSD group (Shi et al., 2017). Another study in temporal stroke patients found that the left amygdala had increased rsFC with the bilateral precuneus and right orbital frontal lobe but decreased rsFC with the right putamen in PSD compared with non-PSD patients (Zhang et al., 2019). The right amygdala had increased rsFC with the right temporal pole, right rectus gyrus, and left orbital frontal lobe but decreased rsFC with the right primary sensory area (S1) (Zhang et al., 2019). The amygdala’s rsFCs with the right orbital frontal cortex, right insula, and right cingulate cortex were correlated with the HDRS score (Zhang et al., 2019). A multivariate Granger causality analysis in right frontal ischemic stroke patients found an emotional circuit (composed of ventromedial PFC, ACC, amygdala, and thalamus) to explain the network alterations in PSD (Shi et al., 2019). The DLPFC could predict the activity of the ACC via the temporal pole, and the activity of the insula could be regulated negatively by the thalamus via ACC (Shi et al., 2019). Altered rsFC of the default mode network (DMN), cognitive control network (CCN), and affective network (AN) was observed in PSD compared with non-PSD patients and normal comparisons (NC; Zhang et al., 2018). The left orbital part of the inferior frontal gyrus, the left inferior parietal gyrus, and the left angular gyrus (which indicated altered rsFCs) were significantly correlated with HDRS scores in PSD patients (Zhang et al., 2018). Dysfunction of the AN in PSD was also observed in another study which found that the rsFCs of the left inferior temporal gyrus, the left orbital part of the inferior frontal gyrus, and the right triangular part of the inferior frontal gyrus were increased with the ACC in PSD compared with non-PSD stroke patients (Zhang P. et al., 2014). Moreover, the rsFC between the left orbital part of the inferior frontal gyrus and ACC was positively correlated with PSD severity (Zhang P. et al., 2014). As for the CCN, PSD was associated with decreased rsFC between left DLPFC and right supramarginal gyrus (Egorova et al., 2018). Graph theory analysis found that the DMN configuration (especially at core hubs such as dorsal PFC and inferior parietal lobule) might be more essential in the pathogenesis of PSD than stroke lesions (Liang et al., 2020). RsFC between anterior DMN and salience network positively correlated with PSD severity, and rsFC between anterior DMN and left frontoparietal network decreased after treatment of PSD (Balaev et al., 2018). Earlier evidence suggested that DMN dysfunction soon after stroke was predictive of PSD severity at 3 months poststroke (Lassalle-Lagadec et al., 2012). Both PSD and poststroke anxiety was found to be associated with DMN disruption (Vicentini et al., 2017). Depression symptoms were found to be correlated with increased rsFC in the left inferior parietal gyrus (Vicentini et al., 2017). Other than fMRI, electroencephalography (EEG) can also be used for rsFC analysis. In one study using mutual information-based graph theory analysis on EEG data, stroke patients showed a decreasing trend in the rsFC between the parietal–occipital and the frontal areas as PSD severity increased (Sun et al., 2018). These functional studies provided promising evidence for the role of emotion- and cognition-related networks in PSD, of which the clinical applicability is yet to be determined considering the complexity of brain networks. Furthermore, most rs-fMRI studies lack the ability of causal inference but reveal a correlation instead as discussed in the previous section (Rorden and Karnath, 2004; Fox, 2018). A functional alteration may be the result of compensation for PSD rather than its cause, and treatment strategies suppressing the alteration could make the symptom worse (Fox, 2018). Targeting the region where brain activity is correlated with but not causally related to PSD may have no effect at all (Fox, 2018). These ambiguities, along with the susceptibility to motion artifacts, make it difficult to translate fMRI correlates directly with therapeutic targets (Rorden and Karnath, 2004; Ovadia-Caro et al., 2014; Fox, 2018).
Direct SC analysis is typically based on each patient’s DTI scans. SC at the neuronal level is the densely distributed axonal streamlines within white matter to connect gray matter regions. Regions that are structurally connected tend to also be functionally connected; however, FC presents a different pattern than SC due to the impact of extensive polysynaptic connections (Fox and Raichle, 2007; Fornito et al., 2015). Recent evidence suggested that the functional brain network dysfunction after stroke can be explained by structural disconnection (SDC; Griffis et al., 2019, 2020). Therefore, SDC could be a more upstream neural substrate of PSD than functional network dysfunction. One study used fractional anisotropy (FA) to reflect white matter integrity and found that the mean FA of the intact areas of stroke-lesioned tracts was lower than that of completely intact fiber tracts (Yang et al., 2015). FA reductions were observed in wide areas of white matter in PSD compared with non-PSD (Yang et al., 2015). Graph theory analysis revealed that decreased local efficiency of a depression-related subnetwork was a significant risk factor for major depression poststroke (Yang et al., 2015). Another study suggested that aberrant global and local structural network topologies might contribute to the development and severity of PSD (Xu et al., 2019). Recent evidence showed that reduced FA, along with increased extracellular free water (a marker of neuroinflammation) and GMV loss, in the reward system was predictive of PSD (Oestreich et al., 2020). However, one major limitation of FA and tractography analysis lies in their susceptibility to complex brain architecture such as fiber crossing (Mori and van Zijl, 2002; Jeurissen et al., 2013). For example, FA may be actually increased after microstructural disruption in regions of fiber crossing. The diffusion tensor model can account only for the Gaussian diffusion process which is not always the case in the human brain and the fiber crossing issue should not be overlooked in future DTI studies (Jeurissen et al., 2013). Diffusion kurtosis imaging (DKI), applying a more complex model than DTI to quantify non-Gaussian water diffusion and reveal complex microstructures, was also used to investigate the role of white matter integrity in PSD (Jensen et al., 2005). DKI may be useful for unveiling abnormalities in isotropic structures, such as fiber crossing and gray matter, where DTI is less applicable (Jensen et al., 2005). One DKI study found that the FA value of the left frontal lobe and the mean kurtosis (MK) value of the bilateral frontal and temporal lobes and genu of the corpus callosum were significantly decreased in PSD compared with non-PSD patients and NC (Shen et al., 2019). Concerning the relationship between the structural and functional networks in PSD, one study identified the SC-FC coupling as a potential biomarker of PSD (Zhang et al., 2021).
Thanks to great efforts such as the Human Connectome Project, connectome atlases of averaged FC and SC patterns from hundreds or thousands of normal populations are now readily available (Glasser et al., 2016). Beyond lesion analysis, we can now combine lesion data with connectome atlases to map the network substrates for PSD without specialized neuroimaging for each individual (Boes et al., 2015; Fox, 2018).
Lesion-network mapping (LNM), a technique to combine lesion with normative functional connectome, generally involves three steps: translating the three-dimensional lesion into the standard space; estimating FC of the lesion with the rest of the brain using normative functional connectome atlas; and overlapping or statistically comparing FC maps derived from patients with the same symptom to identify regions common to the syndrome of interest (Boes et al., 2015; Fox, 2018). LNM is becoming increasingly popular in recent years to map the strategic network substrates of various conditions such as PSD, poststroke behavioral deficits, and mania after brain damage (Padmanabhan et al., 2019; Cotovio et al., 2020; Salvalaggio et al., 2020). A recent LNM study suggested that the lesion locations associated with depression after focal brain damage could be mapped to a human depression circuit centered on left DLPFC (Padmanabhan et al., 2019). Three rTMS targets reported to be effective in treating PSD fell within this circuit (Padmanabhan et al., 2019). A similar method named “dys-connectome” or disconnectome has been used to map the structural network substrates for PSD, poststroke behavioral deficits, poststroke fatigue, and so on (Salvalaggio et al., 2020; Ulrichsen et al., 2021; Weaver et al., 2021b). Powerful tools, such as BCBtoolkit and Lesion Quantification Toolkit, allow researchers to indirectly estimate SDCs with the lesions embedded in the structural connectome atlas and then perform disconnection-symptom inference at tract or voxel levels (Foulon et al., 2018; Griffis et al., 2021). Recent evidence from a multivariate disconnection-symptom mapping study found that SDCs in the right parahippocampal white matter, right thalamus and pallidum, and right anterior thalamic radiation were significantly associated with PSDS (Weaver et al., 2021b).
The atlas-based approach, without need for specialized neuroimaging, may prove a broadly applicable and versatile way for understanding the neural basis of neuropsychiatric symptoms after focal brain damage (Boes et al., 2015; Fox, 2018). However, the atlas-based approach does not necessarily reveal the actual disconnection patterns (Weaver et al., 2021b). The connectome architecture has its intrinsic individual variability (Mueller et al., 2013). It should also be noted that concomitant conditions, other than the stroke lesion, may have impact on brain networks. For example, cerebral small vessel disease (CSVD) is common in elderly stroke patients and can increase the risk of PSD (Tang et al., 2010, 2014; Bae et al., 2019; Liang et al., 2019). Moreover, structural network disruption was observed in CSVD compared with NC (Xie et al., 2017; Lawrence et al., 2018). The impact on the brain network from concomitant factors with inter-person variability may only be taken into account by direct connectome analysis. In terms of causal inference, lesion network maps span several regions at all levels of the neuro-axis and the extent to which any of them are causal to the symptoms is unknown and would require other complementary approaches. The indirect nature of the atlas-based approach requires confirmation and complementation by other methods including direct mapping of residual structural and functional connections in the patients (Salvalaggio et al., 2020; Bobes et al., 2021; Boes, 2021).
Studies reviewed in this work are summarized in Table 1 regarding study design and findings. From the time of lesion analysis to the era of brain networks, our knowledge and understanding of the neural substrates for PSD are increasing. Pooled evidence (Table 1) from traditional lesion analysis, univariate or multivariate LSM, regional structural and functional analyses, and connectome analysis, to some extent, echoes the frontal-limbic theory described in multiple depressive disorders including MDD and vascular depression (Taylor et al., 2013; Robinson and Jorge, 2016; Lai, 2021). Despite differences in etiology and symptom profile (da Rocha e Silva et al., 2013; Albert, 2018), PSD and MDD may share the common neural basis. As shown in Table 1, the PFC as replicated across studies of various methodologies may be the structure most heavily implicated in the pathogenesis of PSD. The role of PFC in depressive disorders has been confirmed by multiple clinical trials, showing that rTMS targeted at the left DLPFC can significantly alleviate the symptoms of PSD, vascular depression, and MDD (Jorge et al., 2004; O’Reardon et al., 2007; George et al., 2010; McIntyre et al., 2016; Gu and Chang, 2017; Shen et al., 2017; Frey et al., 2020; Sackeim et al., 2020). We believe that the PFC is most promising as the avenue for future research or the target for treatment of PSD and other depressive disorders. The distinct roles of subregions of the PFC in mood regulation (Koenigs et al., 2008) and the optimal stimulation target within PFC for neuromodulation therapy are yet to be scrutinized. To date, the definite neural substrates of PSD along with their clinical applications still entail further investigation. Patients with focal brain damage have long been proper study samples for understanding human brain-behavior mechanisms (Fox, 2018; Vaidya et al., 2019), and the findings from research on PSD may also be generalized to depressive disorders in neurologically healthy population.
To improve inter-study consistency and accumulate further evidence, we provide some suggestions for future studies in the field. First, in addition to DSM-5 criteria, researchers may apply a validated depression rating scale with a consistent cutoff value for PSD diagnosis (Berg et al., 2009). Scales that can be generalized to patients with aphasia may be recommended to reduce bias in patient selection (Cobley et al., 2012). Second, serial assessments of depression status (and neuroimaging if necessary) at acute, subacute, and chronic stages of stroke are performed to uncover the potentially dynamic neural substrates of PSD across various stages after stroke. Third, LSM and connectome studies in multicentric large datasets with cross or external validation are recommended to derive comprehensive maps for the strategic lesion locations and disconnection patterns for PSD. Fourth, the neural substrates of PSD at the individual symptom level are uncovered, rather than simply using a binary PSD diagnosis or a continuous sum score. Note that depressive symptoms may have different risk factors and biomarkers (Fried et al., 2014; Moriarity et al., 2022), and the neural substrates of PSD may also be symptom-specific. The symptom-specific anatomical correlates, as well as the complex and dynamic pattern of symptom-symptom interactions, may help us better understand the brain-behavior mechanisms of PSD. Fifth, preregistration of anatomical hypotheses may add rigor to this field. The anatomical hypothesis and analysis plan before observing the research outcomes are defined to prevent problematic research practices such as false positive results from p-hacking and publication bias (Nosek et al., 2018, 2019).
Understanding the neural substrates for PSD is of great predictive value. For example, the strategic lesion locations and disconnection patterns for PSD can be used to develop prediction models for risk stratification and early intervention (Munsch et al., 2016; Salvalaggio et al., 2020; Weaver et al., 2021a,b). Only a few PSD prediction models based on routine clinical-demographic data have been developed and validated (de Man-van Ginkel et al., 2013; Hirt et al., 2020). Stroke severity, physical disability, history of depression, and cognitive impairment have been the most well-recognized predictors of PSD (Towfighi et al., 2017). Sex, age, education level, social support, and personality traits (e.g., neuroticism) are also considered potential (although less clear) predictors of PSD (Towfighi et al., 2017; Chun et al., 2021). A previous study found that both functional dependence and neuroanatomical measures were correlated with more PSD symptoms (Singh et al., 2000). Although inferior frontal lesion location was a risk factor of PSD, the degree of functional dependence imparted the greatest risk (Singh et al., 2000). To date, no imaging predictor is found to outperform classic clinical-demographic variables in PSD prediction. Considering the biopsychosocial multifactorial nature of PSD, incorporating neural substrates into clinical-demographic predictors might be a good choice in PSD prediction (Munsch et al., 2016; Towfighi et al., 2017; Hong et al., 2020). Moreover, advances in methodology as detailed above may provide new promising imaging predictors for PSD in the future. The neural substrates of PSD also have significant preventive and therapeutic value. Many studies (Table 1) can provide convergent evidence for the role of PFC in PSD and therefore the effectiveness of rTMS targeted on left DLPFC. Future studies on brain networks might find personalized preventive or therapeutic targets for PSD based on human connectome (e.g., an emerging technique called connectomic neuromodulation) (Cocchi and Zalesky, 2018; Fox, 2018; Horn and Fox, 2020; Siddiqi et al., 2020). The optimal individualized stimulation site may provide enhanced response to neuromodulation therapy for depression (Cash et al., 2019, 2021). Of note, distinguishing adaptive brain alterations to PSD from causative neural substrates is of great importance in future studies because strategies to inhibit the adaptive changes may lead to exacerbation of PSD (Fox, 2018). Moreover, the techniques reviewed here for uncovering neural substrate can also be extended to clinical research for a broad range of disorders with focal brain damage.
SZ and ZZ led the study and reviewed and edited the final manuscript. GL, WS, JM, XQ, YL, YW, and HW searched and collected the literature. CP prepared the original draft. All authors contributed to the article and approved the submitted version.
This work was funded by the National Key R&D Program of China (grant number 2017YFC1310000), Hubei Technological Innovation Special Fund (grant number 2019ACA132), and National Natural Science Foundation of China (grant numbers 82101605 and 82171465).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Albert, P. R. (2018). Is poststroke depression the same as major depression? J. Psychiatry Neurosci. 43, 76–78. doi: 10.1503/jpn.180015
American Psychiatric Association (2013). Diagnostic and Statistical Manual of Mental Disorders, 5th Edn. Washington, DC: American Psychiatric Association. doi: 10.1176/appi.books.9780890425596
Ashaie, S. A., Hung, J., Funkhouser, C. J., Shankman, S. A., and Cherney, L. R. (2021). Depression over time in persons with stroke: a network analysis approach. J. Affect. Disord. Rep. 4:100131. doi: 10.1016/j.jadr.2021.100131
Ashburner, J., and Friston, K. J. (2000). Voxel-based morphometry–the methods. Neuroimage 11(6 Pt. 1), 805–821. doi: 10.1006/nimg.2000.0582
Astrom, M., Adolfsson, R., and Asplund, K. (1993). Major depression in stroke patients. A 3-year longitudinal study. Stroke 24, 976–982. doi: 10.1161/01.str.24.7.976
Ay, H., Koroshetz, W. J., Benner, T., Vangel, M. G., Melinosky, C., Arsava, E. M., et al. (2006). Neuroanatomic correlates of stroke-related myocardial injury. Neurology 66, 1325–1329. doi: 10.1212/01.wnl.0000206077.13705.6d
Ayerbe, L., Ayis, S., Wolfe, C. D., and Rudd, A. G. (2013). Natural history, predictors and outcomes of depression after stroke: systematic review and meta-analysis. Br. J. Psychiatry 202, 14–21. doi: 10.1192/bjp.bp.111.107664
Bae, K. Y., Kang, H. J., Kim, J. W., Kim, S. W., Kim, J. T., Park, M. S., et al. (2019). Associations of white matter hyperintensities with poststroke depression: a 1-year longitudinal study. Int. J. Geriatr. Psychiatry 34, 162–168. doi: 10.1002/gps.5005
Balaev, V., Orlov, I., Petrushevsky, A., and Martynova, O. (2018). Functional connectivity between salience, default mode and frontoparietal networks in post-stroke depression. J. Affect. Disord. 227, 554–562. doi: 10.1016/j.jad.2017.11.044
Bartoli, F., Lillia, N., Lax, A., Crocamo, C., Mantero, V., Carra, G., et al. (2013). Depression after stroke and risk of mortality: a systematic review and meta-analysis. Stroke Res. Treat. 2013:862978. doi: 10.1155/2013/862978
Bates, E., Wilson, S. M., Saygin, A. P., Dick, F., Sereno, M. I., Knight, R. T., et al. (2003). Voxel-based lesion-symptom mapping. Nat. Neurosci. 6, 448–450. doi: 10.1038/nn1050
Belvederi Murri, M., Amore, M., Respino, M., and Alexopoulos, G. S. (2020). The symptom network structure of depressive symptoms in late-life: results from a European population study. Mol. Psychiatry 25, 1447–1456. doi: 10.1038/s41380-018-0232-0
Berg, A., Lonnqvist, J., Palomaki, H., and Kaste, M. (2009). Assessment of depression after stroke: a comparison of different screening instruments. Stroke 40, 523–529. doi: 10.1161/STROKEAHA.108.527705
Bobes, M. A., Van den Stock, J., Zhan, M., Valdes-Sosa, M., and de Gelder, B. (2021). Looking beyond indirect lesion network mapping of prosopagnosia: direct measures required. Brain 144:e75. doi: 10.1093/brain/awab276
Boes, A. D. (2021). Lesion network mapping: where do we go from here? Brain 144:e5. doi: 10.1093/brain/awaa350
Boes, A. D., Prasad, S., Liu, H., Liu, Q., Pascual-Leone, A., and Caviness, V. S. Jr., et al. (2015). Network localization of neurological symptoms from focal brain lesions. Brain 138(Pt. 10), 3061–3075. doi: 10.1093/brain/awv228
Borsboom, D. (2008). Psychometric perspectives on diagnostic systems. J. Clin. Psychol. 64, 1089–1108. doi: 10.1002/jclp.20503
Borsboom, D., and Cramer, A. O. (2013). Network analysis: an integrative approach to the structure of psychopathology. Annu. Rev. Clin. Psychol. 9, 91–121. doi: 10.1146/annurev-clinpsy-050212-185608
Bullmore, E., and Sporns, O. (2009). Complex brain networks: graph theoretical analysis of structural and functional systems. Nat. Rev. Neurosci. 10, 186–198. doi: 10.1038/nrn2575
Carrera, E., and Tononi, G. (2014). Diaschisis: past, present, future. Brain 137(Pt. 9), 2408–2422. doi: 10.1093/brain/awu101
Carson, A. J., MacHale, S., Allen, K., Lawrie, S. M., Dennis, M., House, A., et al. (2000). Depression after stroke and lesion location: a systematic review. Lancet 356, 122–126. doi: 10.1016/S0140-6736(00)02448-X
Cash, R. F. H., Cocchi, L., Lv, J., Fitzgerald, P. B., and Zalesky, A. (2021). Functional magnetic resonance imaging-guided personalization of transcranial magnetic stimulation treatment for depression. JAMA Psychiatry 78, 337–339. doi: 10.1001/jamapsychiatry.2020.3794
Cash, R. F. H., Zalesky, A., Thomson, R. H., Tian, Y., Cocchi, L., and Fitzgerald, P. B. (2019). Subgenual functional connectivity predicts antidepressant treatment response to transcranial magnetic stimulation: independent validation and evaluation of personalization. Biol. Psychiatry 86, e5–e7. doi: 10.1016/j.biopsych.2018.12.002
Catani, M., Dell’acqua, F., Bizzi, A., Forkel, S. J., Williams, S. C., Simmons, A., et al. (2012). Beyond cortical localization in clinico-anatomical correlation. Cortex 48, 1262–1287. doi: 10.1016/j.cortex.2012.07.001
Chun, H. Y., Ford, A., Kutlubaev, M. A., Almeida, O. P., and Mead, G. E. (2021). Depression, anxiety, and suicide after stroke: a narrative review of the best available evidence. Stroke doi: 10.1161/STROKEAHA.121.035499 [Epub ahead of print].
Cobley, C. S., Thomas, S. A., Lincoln, N. B., and Walker, M. F. (2012). The assessment of low mood in stroke patients with aphasia: reliability and validity of the 10-item Hospital version of the Stroke Aphasic Depression Questionnaire (SADQH-10). Clin. Rehabil. 26, 372–381. doi: 10.1177/0269215511422388
Cocchi, L., and Zalesky, A. (2018). Personalized transcranial magnetic stimulation in psychiatry. Biol. Psychiatry Cogn. Neurosci. Neuroimaging 3, 731–741. doi: 10.1016/j.bpsc.2018.01.008
Cotovio, G., Talmasov, D., Barahona-Correa, J. B., Hsu, J., Senova, S., Ribeiro, R., et al. (2020). Mapping mania symptoms based on focal brain damage. J. Clin. Invest. 130, 5209–5222. doi: 10.1172/JCI136096
da Rocha e Silva, C. E., Alves Brasil, M. A., Matos do Nascimento, E., de Braganca Pereira, B., and Andre, C. (2013). Is poststroke depression a major depression? Cerebrovasc. Dis. 35, 385–391. doi: 10.1159/000348852
de Man-van Ginkel, J. M., Hafsteinsdottir, T. B., Lindeman, E., Ettema, R. G., Grobbee, D. E., and Schuurmans, M. J. (2013). In-hospital risk prediction for post-stroke depression: development and validation of the Post-stroke Depression Prediction Scale. Stroke 44, 2441–2445. doi: 10.1161/STROKEAHA.111.000304
Egorova, N., Cumming, T., Shirbin, C., Veldsman, M., Werden, E., and Brodtmann, A. (2018). Lower cognitive control network connectivity in stroke participants with depressive features. Transl. Psychiatry 7:4. doi: 10.1038/s41398-017-0038-x
Egorova, N., Veldsman, M., Cumming, T., and Brodtmann, A. (2017). Fractional amplitude of low-frequency fluctuations (fALFF) in post-stroke depression. Neuroimage Clin. 16, 116–124. doi: 10.1016/j.nicl.2017.07.014
Folstein, M. F., Maiberger, R., and McHugh, P. R. (1977). Mood disorder as a specific complication of stroke. J. Neurol. Neurosurg. Psychiatry 40, 1018–1020. doi: 10.1136/jnnp.40.10.1018
Fornito, A., Zalesky, A., and Breakspear, M. (2015). The connectomics of brain disorders. Nat. Rev. Neurosci. 16, 159–172. doi: 10.1038/nrn3901
Foulon, C., Cerliani, L., Kinkingnehun, S., Levy, R., Rosso, C., Urbanski, M., et al. (2018). Advanced lesion symptom mapping analyses and implementation as BCBtoolkit. Gigascience 7, 1–17. doi: 10.1093/gigascience/giy004
Fox, M. D. (2018). Mapping symptoms to brain networks with the human connectome. N. Engl. J. Med. 379, 2237–2245. doi: 10.1056/NEJMra1706158
Fox, M. D., and Raichle, M. E. (2007). Spontaneous fluctuations in brain activity observed with functional magnetic resonance imaging. Nat. Rev. Neurosci. 8, 700–711. doi: 10.1038/nrn2201
Frey, J., Najib, U., Lilly, C., and Adcock, A. (2020). Novel TMS for stroke and depression (NoTSAD): accelerated repetitive transcranial magnetic stimulation as a safe and effective treatment for post-stroke depression. Front. Neurol. 11:788. doi: 10.3389/fneur.2020.00788
Fried, E. I., and Cramer, A. O. J. (2017). Moving forward: challenges and directions for psychopathological network theory and methodology. Perspect. Psychol. Sci. 12, 999–1020. doi: 10.1177/1745691617705892
Fried, E. I., Nesse, R. M., Zivin, K., Guille, C., and Sen, S. (2014). Depression is more than the sum score of its parts: individual DSM symptoms have different risk factors. Psychol. Med. 44, 2067–2076. doi: 10.1017/S0033291713002900
Fried, E. I., von Stockert, S., Haslbeck, J. M. B., Lamers, F., Schoevers, R. A., and Penninx, B. (2020). Using network analysis to examine links between individual depressive symptoms, inflammatory markers, and covariates. Psychol. Med. 50, 2682–2690. doi: 10.1017/S0033291719002770
George, M. S., Lisanby, S. H., Avery, D., McDonald, W. M., Durkalski, V., Pavlicova, M., et al. (2010). Daily left prefrontal transcranial magnetic stimulation therapy for major depressive disorder: a sham-controlled randomized trial. Arch. Gen. Psychiatry 67, 507–516. doi: 10.1001/archgenpsychiatry.2010.46
Ghose, S. S., Williams, L. S., and Swindle, R. W. (2005). Depression and other mental health diagnoses after stroke increase inpatient and outpatient medical utilization three years poststroke. Med. Care 43, 1259–1264. doi: 10.1097/01.mlr.0000185711.50480.13
Glasser, M. F., Smith, S. M., Marcus, D. S., Andersson, J. L., Auerbach, E. J., Behrens, T. E., et al. (2016). The human connectome Project’s neuroimaging approach. Nat. Neurosci. 19, 1175–1187. doi: 10.1038/nn.4361
Gong, Q., and He, Y. (2015). Depression, neuroimaging and connectomics: a selective overview. Biol. Psychiatry 77, 223–235. doi: 10.1016/j.biopsych.2014.08.009
Goodin, P., Lamp, G., Vidyasagar, R., Connelly, A., Rose, S., Campbell, B. C. V., et al. (2019). Correlated resting-state functional MRI activity of frontostriatal, thalamic, temporal, and cerebellar brain regions differentiates stroke survivors with high compared to low depressive symptom scores. Neural Plast. 2019:2357107. doi: 10.1155/2019/2357107
Goodkind, M., Eickhoff, S. B., Oathes, D. J., Jiang, Y., Chang, A., Jones-Hagata, L. B., et al. (2015). Identification of a common neurobiological substrate for mental illness. JAMA Psychiatry 72, 305–315. doi: 10.1001/jamapsychiatry.2014.2206
Gozzi, S. A., Wood, A. G., Chen, J., Vaddadi, K., and Phan, T. G. (2014). Imaging predictors of poststroke depression: methodological factors in voxel-based analysis. BMJ Open 4:e004948. doi: 10.1136/bmjopen-2014-004948
Grajny, K., Pyata, H., Spiegel, K., Lacey, E. H., Xing, S., Brophy, C., et al. (2016). Depression symptoms in chronic left hemisphere stroke are related to dorsolateral prefrontal cortex damage. J Neuropsychiatry Clin. Neurosci. 28, 292–298. doi: 10.1176/appi.neuropsych.16010004
Griffis, J. C., Metcalf, N. V., Corbetta, M., and Shulman, G. L. (2019). Structural disconnections explain brain network dysfunction after stroke. Cell Rep. 28, 2527–2540.e2529. doi: 10.1016/j.celrep.2019.07.100
Griffis, J. C., Metcalf, N. V., Corbetta, M., and Shulman, G. L. (2020). Damage to the shortest structural paths between brain regions is associated with disruptions of resting-state functional connectivity after stroke. Neuroimage 210:116589. doi: 10.1016/j.neuroimage.2020.116589
Griffis, J. C., Metcalf, N. V., Corbetta, M., and Shulman, G. L. (2021). Lesion quantification toolkit: a MATLAB software tool for estimating grey matter damage and white matter disconnections in patients with focal brain lesions. Neuroimage Clin. 30:102639. doi: 10.1016/j.nicl.2021.102639
Gu, S. Y., and Chang, M. C. (2017). The effects of 10-Hz repetitive transcranial magnetic stimulation on depression in chronic stroke patients. Brain Stimul. 10, 270–274. doi: 10.1016/j.brs.2016.10.010
He, Y., and Evans, A. (2010). Graph theoretical modeling of brain connectivity. Curr. Opin. Neurol. 23, 341–350. doi: 10.1097/WCO.0b013e32833aa567
Hess, F., Foerch, C., Keil, F., Seiler, A., and Lapa, S. (2021). Association of lesion pattern and dysphagia in acute intracerebral hemorrhage. Stroke 52, 2921–2929. doi: 10.1161/STROKEAHA.120.032615
Hirt, J., van Meijeren, L. C. J., Saal, S., Hafsteinsdottir, T. B., Hofmeijer, J., Kraft, A., et al. (2020). Predictive accuracy of the post-stroke depression prediction scale: a prospective binational observational study(). J. Affect. Disord. 265, 39–44. doi: 10.1016/j.jad.2020.01.019
Hong, W., Zhao, Z., Wang, D., Li, M., Tang, C., Li, Z., et al. (2020). Altered gray matter volumes in post-stroke depressive patients after subcortical stroke. Neuroimage Clin. 26:102224. doi: 10.1016/j.nicl.2020.102224
Horn, A., and Fox, M. D. (2020). Opportunities of connectomic neuromodulation. Neuroimage 221:117180. doi: 10.1016/j.neuroimage.2020.117180
Jbabdi, S., Sotiropoulos, S. N., Haber, S. N., Van Essen, D. C., and Behrens, T. E. (2015). Measuring macroscopic brain connections in vivo. Nat. Neurosci. 18, 1546–1555. doi: 10.1038/nn.4134
Jensen, J. H., Helpern, J. A., Ramani, A., Lu, H., and Kaczynski, K. (2005). Diffusional kurtosis imaging: the quantification of non-gaussian water diffusion by means of magnetic resonance imaging. Magn. Reson. Med. 53, 1432–1440. doi: 10.1002/mrm.20508
Jeurissen, B., Leemans, A., Tournier, J. D., Jones, D. K., and Sijbers, J. (2013). Investigating the prevalence of complex fiber configurations in white matter tissue with diffusion magnetic resonance imaging. Hum. Brain Mapp. 34, 2747–2766. doi: 10.1002/hbm.22099
Jia, H., Damush, T. M., Qin, H., Ried, L. D., Wang, X., Young, L. J., et al. (2006). The impact of poststroke depression on healthcare use by veterans with acute stroke. Stroke 37, 2796–2801. doi: 10.1161/01.STR.0000244783.53274.a4
Jokela, M., Virtanen, M., Batty, G. D., and Kivimaki, M. (2016). Inflammation and specific symptoms of depression. JAMA Psychiatry 73, 87–88. doi: 10.1001/jamapsychiatry.2015.1977
Jorge, R. E., Robinson, R. G., Tateno, A., Narushima, K., Acion, L., Moser, D., et al. (2004). Repetitive transcranial magnetic stimulation as treatment of poststroke depression: a preliminary study. Biol. Psychiatry 55, 398–405. doi: 10.1016/j.biopsych.2003.08.017
Karnath, H. O., Sperber, C., and Rorden, C. (2018). Mapping human brain lesions and their functional consequences. Neuroimage 165, 180–189. doi: 10.1016/j.neuroimage.2017.10.028
Kim, N. Y., Lee, S. C., Shin, J. C., Park, J. E., and Kim, Y. W. (2017). Voxel-based lesion symptom mapping analysis of depressive mood in patients with isolated cerebellar stroke: a pilot study. Neuroimage Clin. 13, 39–45. doi: 10.1016/j.nicl.2016.11.011
Kimberg, D. Y., Coslett, H. B., and Schwartz, M. F. (2007). Power in Voxel-based lesion-symptom mapping. J. Cogn. Neurosci. 19, 1067–1080. doi: 10.1162/jocn.2007.19.7.1067
Koenigs, M., Huey, E. D., Calamia, M., Raymont, V., Tranel, D., and Grafman, J. (2008). Distinct regions of prefrontal cortex mediate resistance and vulnerability to depression. J. Neurosci. 28, 12341–12348. doi: 10.1523/JNEUROSCI.2324-08.2008
Kutlubaev, M. A., and Hackett, M. L. (2014). Part II: predictors of depression after stroke and impact of depression on stroke outcome: an updated systematic review of observational studies. Int. J. Stroke 9, 1026–1036. doi: 10.1111/ijs.12356
Lai, C. H. (2021). Fronto-limbic neuroimaging biomarkers for diagnosis and prediction of treatment responses in major depressive disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 107:110234. doi: 10.1016/j.pnpbp.2020.110234
Lassalle-Lagadec, S., Sibon, I., Dilharreguy, B., Renou, P., Fleury, O., and Allard, M. (2012). Subacute default mode network dysfunction in the prediction of post-stroke depression severity. Radiology 264, 218–224. doi: 10.1148/radiol.12111718
Lawrence, A. J., Tozer, D. J., Stamatakis, E. A., and Markus, H. S. (2018). A comparison of functional and tractography based networks in cerebral small vessel disease. Neuroimage Clin. 18, 425–432. doi: 10.1016/j.nicl.2018.02.013
Liang, Y., Chen, Y. K., Liu, Y. L., Mok, V. C. T., Ungvari, G. S., Chu, W. C. W., et al. (2019). Exploring causal pathways linking cerebral small vessel diseases burden to poststroke depressive symptoms with structural equation model analysis. J. Affect. Disord. 253, 218–223. doi: 10.1016/j.jad.2019.04.092
Liang, Y., Yao, Y. C., Zhao, L., Shi, L., Chen, Y. K., Mok, V. C., et al. (2020). Topological reorganization of the default mode network in patients with poststroke depressive symptoms: a resting-state fMRI study. J. Affect. Disord. 260, 557–568. doi: 10.1016/j.jad.2019.09.051
MacHale, S. M., O’Rourke, S. J., Wardlaw, J. M., and Dennis, M. S. (1998). Depression and its relation to lesion location after stroke. J. Neurol. Neurosurg. Psychiatry 64, 371–374. doi: 10.1136/jnnp.64.3.371
Mah, Y. H., Husain, M., Rees, G., and Nachev, P. (2014). Human brain lesion-deficit inference remapped. Brain 137(Pt. 9), 2522–2531. doi: 10.1093/brain/awu164
Mayman, N., Stein, L. K., Erdman, J., Kornspun, A., Tuhrim, S., Jette, N., et al. (2021). Risk and predictors of depression following acute ischemic stroke in the elderly. Neurology 96, e2184–e2191. doi: 10.1212/WNL.0000000000011828
McIntyre, A., Thompson, S., Burhan, A., Mehta, S., and Teasell, R. (2016). Repetitive transcranial magnetic stimulation for depression due to cerebrovascular disease: a systematic review. J. Stroke Cerebrovasc. Dis. 25, 2792–2800. doi: 10.1016/j.jstrokecerebrovasdis.2016.08.043
Meader, N., Moe-Byrne, T., Llewellyn, A., and Mitchell, A. J. (2014). Screening for poststroke major depression: a meta-analysis of diagnostic validity studies. J. Neurol. Neurosurg. Psychiatry 85, 198–206. doi: 10.1136/jnnp-2012-304194
Medina, J., Kimberg, D. Y., Chatterjee, A., and Coslett, H. B. (2010). Inappropriate usage of the Brunner-Munzel test in recent voxel-based lesion-symptom mapping studies. Neuropsychologia 48, 341–343. doi: 10.1016/j.neuropsychologia.2009.09.016
Menon, V. (2011). Large-scale brain networks and psychopathology: a unifying triple network model. Trends Cogn. Sci. 15, 483–506. doi: 10.1016/j.tics.2011.08.003
Mori, S., and van Zijl, P. C. (2002). Fiber tracking: principles and strategies – a technical review. NMR Biomed. 15, 468–480. doi: 10.1002/nbm.781
Moriarity, D. P., Joyner, K. J., Slavich, G. M., and Alloy, L. B. (2022). Unconsidered issues of measurement noninvariance in biological psychiatry: a focus on biological phenotypes of psychopathology. Mol. Psychiatry doi: 10.1038/s41380-021-01414-5 [Epub ahead of print].
Mueller, S., Wang, D., Fox, M. D., Yeo, B. T., Sepulcre, J., Sabuncu, M. R., et al. (2013). Individual variability in functional connectivity architecture of the human brain. Neuron 77, 586–595. doi: 10.1016/j.neuron.2012.12.028
Munsch, F., Sagnier, S., Asselineau, J., Bigourdan, A., Guttmann, C. R., Debruxelles, S., et al. (2016). Stroke location is an independent predictor of cognitive outcome. Stroke 47, 66–73. doi: 10.1161/STROKEAHA.115.011242
Nickel, A., and Thomalla, G. (2017). Post-stroke depression: impact of lesion location and methodological limitations-a topical review. Front. Neurol. 8:498. doi: 10.3389/fneur.2017.00498
Nosek, B. A., Beck, E. D., Campbell, L., Flake, J. K., Hardwicke, T. E., Mellor, D. T., et al. (2019). Preregistration is hard, and worthwhile. Trends Cogn. Sci. 23, 815–818. doi: 10.1016/j.tics.2019.07.009
Nosek, B. A., Ebersole, C. R., DeHaven, A. C., and Mellor, D. T. (2018). The preregistration revolution. Proc. Natl. Acad. Sci. U.S.A. 115, 2600–2606. doi: 10.1073/pnas.1708274114
Oathes, D. J., Patenaude, B., Schatzberg, A. F., and Etkin, A. (2015). Neurobiological signatures of anxiety and depression in resting-state functional magnetic resonance imaging. Biol. Psychiatry 77, 385–393. doi: 10.1016/j.biopsych.2014.08.006
Oestreich, L. K. L., Wright, P., and O’Sullivan, M. J. (2020). Microstructural changes in the reward system are associated with post-stroke depression. Neuroimage Clin. 28:102360. doi: 10.1016/j.nicl.2020.102360
O’Reardon, J. P., Solvason, H. B., Janicak, P. G., Sampson, S., Isenberg, K. E., Nahas, Z., et al. (2007). Efficacy and safety of transcranial magnetic stimulation in the acute treatment of major depression: a multisite randomized controlled trial. Biol. Psychiatry 62, 1208–1216. doi: 10.1016/j.biopsych.2007.01.018
Ovadia-Caro, S., Margulies, D. S., and Villringer, A. (2014). The value of resting-state functional magnetic resonance imaging in stroke. Stroke 45, 2818–2824. doi: 10.1161/STROKEAHA.114.003689
Padmanabhan, J. L., Cooke, D., Joutsa, J., Siddiqi, S. H., Ferguson, M., Darby, R. R., et al. (2019). A human depression circuit derived from focal brain lesions. Biol. Psychiatry 86, 749–758. doi: 10.1016/j.biopsych.2019.07.023
Pustina, D., Avants, B., Faseyitan, O. K., Medaglia, J. D., and Coslett, H. B. (2018). Improved accuracy of lesion to symptom mapping with multivariate sparse canonical correlations. Neuropsychologia 115, 154–166. doi: 10.1016/j.neuropsychologia.2017.08.027
Rajashekaran, P., Pai, K., Thunga, R., and Unnikrishnan, B. (2013). Post-stroke depression and lesion location: a hospital based cross-sectional study. Indian J. Psychiatry 55, 343–348. doi: 10.4103/0019-5545.120546
Robinson, R. G., and Jorge, R. E. (2016). Post-stroke depression: a review. Am. J. Psychiatry 173, 221–231. doi: 10.1176/appi.ajp.2015.15030363
Robinson, R. G., and Price, T. R. (1982). Post-stroke depressive disorders: a follow-up study of 103 patients. Stroke 13, 635–641. doi: 10.1161/01.str.13.5.635
Robinson, R. G., Bolla-Wilson, K., Kaplan, E., Lipsey, J. R., and Price, T. R. (1986). Depression influences intellectual impairment in stroke patients. Br. J. Psychiatry 148, 541–547. doi: 10.1192/bjp.148.5.541
Robinson, R. G., Kubos, K. L., Starr, L. B., Rao, K., and Price, T. R. (1983). Mood changes in stroke patients: relationship to lesion location. Compr. Psychiatry 24, 555–566. doi: 10.1016/0010-440x(83)90024-x
Robinson, R. G., Shoemaker, W. J., Schlumpf, M., Valk, T., and Bloom, F. E. (1975). Effect of experimental cerebral infarction in rat brain on catecholamines and behaviour. Nature 255, 332–334. doi: 10.1038/255332a0
Rorden, C., and Karnath, H. O. (2004). Using human brain lesions to infer function: a relic from a past era in the fMRI age? Nat. Rev. Neurosci. 5, 813–819. doi: 10.1038/nrn1521
Sackeim, H. A., Aaronson, S. T., Carpenter, L. L., Hutton, T. M., Mina, M., Pages, K., et al. (2020). Clinical outcomes in a large registry of patients with major depressive disorder treated with Transcranial Magnetic Stimulation. J. Affect. Disord. 277, 65–74. doi: 10.1016/j.jad.2020.08.005
Salvalaggio, A., De Filippo De Grazia, M., Zorzi, M., Thiebaut de Schotten, M., and Corbetta, M. (2020). Post-stroke deficit prediction from lesion and indirect structural and functional disconnection. Brain 143, 2173–2188. doi: 10.1093/brain/awaa156
Shen, X. Y., Fan, Z. X., Wang, L., Cui, S., and Niu, J. L. (2019). Altered white matter microstructure in patients with post-stroke depression detected by diffusion kurtosis imaging. Neurol. Sci. 40, 2097–2103. doi: 10.1007/s10072-019-03947-8
Shen, X., Liu, M., Cheng, Y., Jia, C., Pan, X., Gou, Q., et al. (2017). Repetitive transcranial magnetic stimulation for the treatment of post-stroke depression: a systematic review and meta-analysis of randomized controlled clinical trials. J. Affect. Disord. 211, 65–74. doi: 10.1016/j.jad.2016.12.058
Shi, Y., Liu, W., Liu, R., Zeng, Y., Wu, L., Huang, S., et al. (2019). Investigation of the emotional network in depression after stroke: a study of multivariate Granger causality analysis of fMRI data. J. Affect. Disord. 249, 35–44. doi: 10.1016/j.jad.2019.02.020
Shi, Y., Zeng, Y., Wu, L., Liu, W., Liu, Z., Zhang, S., et al. (2017). A study of the brain abnormalities of post-stroke depression in frontal lobe lesion. Sci. Rep. 7:13203. doi: 10.1038/s41598-017-13681-w
Shimoda, K., and Robinson, R. G. (1999). The relationship between poststroke depression and lesion location in long-term follow-up. Biol. Psychiatry 45, 187–192. doi: 10.1016/s0006-3223(98)00178-4
Siddiqi, S. H., Taylor, S. F., Cooke, D., Pascual-Leone, A., George, M. S., and Fox, M. D. (2020). Distinct symptom-specific treatment targets for circuit-based neuromodulation. Am. J. Psychiatry 177, 435–446. doi: 10.1176/appi.ajp.2019.19090915
Singh, A., Black, S. E., Herrmann, N., Leibovitch, F. S., Ebert, P. L., Lawrence, J., et al. (2000). Functional and neuroanatomic correlations in poststroke depression: the Sunnybrook Stroke Study. Stroke 31, 637–644. doi: 10.1161/01.str.31.3.637
Sperber, C., and Karnath, H. O. (2017). Impact of correction factors in human brain lesion-behavior inference. Hum. Brain Mapp. 38, 1692–1701. doi: 10.1002/hbm.23490
Sporns, O., Tononi, G., and Kotter, R. (2005). The human connectome: a structural description of the human brain. PLoS Comput. Biol. 1:e42. doi: 10.1371/journal.pcbi.0010042
Starkstein, S. E., Robinson, R. G., and Price, T. R. (1987). Comparison of cortical and subcortical lesions in the production of poststroke mood disorders. Brain 110(Pt. 4), 1045–1059. doi: 10.1093/brain/110.4.1045
Sun, C., Yang, F., Wang, C., Wang, Z., Zhang, Y., Ming, D., et al. (2018). Mutual information-based brain network analysis in post-stroke patients with different levels of depression. Front. Hum. Neurosci. 12:285. doi: 10.3389/fnhum.2018.00285
Tang, W. K., Chen, Y. K., Lu, J. Y., Chu, W. C., Mok, V. C., Ungvari, G. S., et al. (2010). White matter hyperintensities in post-stroke depression: a case control study. J. Neurol. Neurosurg. Psychiatry 81, 1312–1315. doi: 10.1136/jnnp.2009.203141
Tang, W. K., Chen, Y., Liang, H., Chu, W. C., Mok, V. C., Ungvari, G. S., et al. (2014). Cerebral microbleeds as a predictor of 1-year outcome of poststroke depression. Stroke 45, 77–81. doi: 10.1161/STROKEAHA.113.002686
Taylor, W. D., Aizenstein, H. J., and Alexopoulos, G. S. (2013). The vascular depression hypothesis: mechanisms linking vascular disease with depression. Mol. Psychiatry 18, 963–974. doi: 10.1038/mp.2013.20
Towfighi, A., Ovbiagele, B., El Husseini, N., Hackett, M. L., Jorge, R. E., Kissela, B. M., et al. (2017). Poststroke depression: a scientific statement for healthcare professionals from the American heart association/American stroke association. Stroke 48, e30–e43. doi: 10.1161/STR.0000000000000113
Triolo, F., Belvederi Murri, M., Calderon-Larranaga, A., Vetrano, D. L., Sjoberg, L., Fratiglioni, L., et al. (2021). Bridging late-life depression and chronic somatic diseases: a network analysis. Transl. Psychiatry 11:557. doi: 10.1038/s41398-021-01686-z
Ulrichsen, K. M., Kolskar, K. K., Richard, G., Alnaes, D., Dorum, E. S., Sanders, A. M., et al. (2021). Structural brain disconnectivity mapping of post-stroke fatigue. Neuroimage Clin. 30:102635. doi: 10.1016/j.nicl.2021.102635
Vaidya, A. R., Pujara, M. S., Petrides, M., Murray, E. A., and Fellows, L. K. (2019). Lesion studies in contemporary neuroscience. Trends Cogn. Sci. 23, 653–671. doi: 10.1016/j.tics.2019.05.009
van Borkulo, C., Boschloo, L., Borsboom, D., Penninx, B. W., Waldorp, L. J., and Schoevers, R. A. (2015). Association of symptom network structure with the course of depression. JAMA Psychiatry 72, 1219–1226. doi: 10.1001/jamapsychiatry.2015.2079
Vicentini, J. E., Weiler, M., Almeida, S. R. M., de Campos, B. M., Valler, L., and Li, L. M. (2017). Depression and anxiety symptoms are associated to disruption of default mode network in subacute ischemic stroke. Brain Imaging Behav. 11, 1571–1580. doi: 10.1007/s11682-016-9605-7
Weaver, N. A., Kuijf, H. J., Aben, H. P., Abrigo, J., Bae, H. J., Barbay, M., et al. (2021a). Strategic infarct locations for post-stroke cognitive impairment: a pooled analysis of individual patient data from 12 acute ischaemic stroke cohorts. Lancet Neurol. 20, 448–459. doi: 10.1016/S1474-4422(21)00060-0
Weaver, N. A., Lim, J. S., Schilderinck, J., Biessels, G. J., Kang, Y., Kim, B. J., et al. (2021b). Strategic infarct locations for post-stroke depressive symptoms: a lesion- and disconnection-symptom mapping study. Biol. Psychiatry Cogn. Neurosci. Neuroimaging doi: 10.1016/j.bpsc.2021.09.002 [Epub ahead of print].
Wei, N., Yong, W., Li, X., Zhou, Y., Deng, M., Zhu, H., et al. (2015). Post-stroke depression and lesion location: a systematic review. J. Neurol. 262, 81–90. doi: 10.1007/s00415-014-7534-1
White, J., Kivimaki, M., Jokela, M., and Batty, G. D. (2017). Association of inflammation with specific symptoms of depression in a general population of older people: the English Longitudinal Study of Ageing. Brain Behav. Immun. 61, 27–30. doi: 10.1016/j.bbi.2016.08.012
Xie, X., Shi, Y., and Zhang, J. (2017). Structural network connectivity impairment and depressive symptoms in cerebral small vessel disease. J. Affect. Disord. 220, 8–14. doi: 10.1016/j.jad.2017.05.039
Xu, T., Jha, A., and Nachev, P. (2018). The dimensionalities of lesion-deficit mapping. Neuropsychologia 115, 134–141. doi: 10.1016/j.neuropsychologia.2017.09.007
Xu, X., Tang, R., Zhang, L., and Cao, Z. (2019). Altered topology of the structural brain network in patients with post-stroke depression. Front. Neurosci. 13:776. doi: 10.3389/fnins.2019.00776
Yang, S., Hua, P., Shang, X., Cui, Z., Zhong, S., Gong, G., et al. (2015). A significant risk factor for poststroke depression: the depression-related subnetwork. J. Psychiatry Neurosci. 40, 259–268. doi: 10.1503/jpn.140086
Zang, Y. F., He, Y., Zhu, C. Z., Cao, Q. J., Sui, M. Q., Liang, M., et al. (2007). Altered baseline brain activity in children with ADHD revealed by resting-state functional MRI. Brain Dev. 29, 83–91. doi: 10.1016/j.braindev.2006.07.002
Zhang, P., Wang, J., Xu, Q., Song, Z., Dai, J., and Wang, J. (2018). Altered functional connectivity in post-ischemic stroke depression: a resting-state functional magnetic resonance imaging study. Eur. J. Radiol. 100, 156–165. doi: 10.1016/j.ejrad.2018.01.003
Zhang, P., Xu, Q., Dai, J., Wang, J., Zhang, N., and Luo, Y. (2014). Dysfunction of affective network in post ischemic stroke depression: a resting-state functional magnetic resonance imaging study. Biomed Res. Int. 2014:846830. doi: 10.1155/2014/846830
Zhang, X. F., He, X., Wu, L., Liu, C. J., and Wu, W. (2019). Altered functional connectivity of amygdala with the fronto-limbic-striatal circuit in temporal lobe lesion as a proposed mechanism for poststroke depression. Am. J. Phys. Med. Rehabil. 98, 303–310. doi: 10.1097/PHM.0000000000001081
Zhang, X., Shi, Y., Fan, T., Wang, K., Zhan, H., and Wu, W. (2021). Analysis of correlation between white matter changes and functional responses in post-stroke depression. Front. Aging Neurosci. 13:728622. doi: 10.3389/fnagi.2021.728622
Zhang, Y., Kimberg, D. Y., Coslett, H. B., Schwartz, M. F., and Wang, Z. (2014). Multivariate lesion-symptom mapping using support vector regression. Hum. Brain Mapp. 35, 5861–5876. doi: 10.1002/hbm.22590
Keywords: poststroke depression, neural substrate, lesion analysis, gray matter atrophy, regional brain activity, brain network, lesion-network mapping, disconnectome
Citation: Pan C, Li G, Sun W, Miao J, Qiu X, Lan Y, Wang Y, Wang H, Zhu Z and Zhu S (2022) Neural Substrates of Poststroke Depression: Current Opinions and Methodology Trends. Front. Neurosci. 16:812410. doi: 10.3389/fnins.2022.812410
Received: 10 November 2021; Accepted: 04 February 2022;
Published: 06 April 2022.
Edited by:
Peng Wang, Chinese Academy of Medical Sciences and Peking Union Medical College, ChinaReviewed by:
Aaron Boes, The University of Iowa, United StatesCopyright © 2022 Pan, Li, Sun, Miao, Qiu, Lan, Wang, Wang, Zhu and Zhu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suiqiang Zhu, emh1c3VpcWlhbmdAMTYzLmNvbQ==; Zhou Zhu, emhvdXpodUBodXN0LmVkdS5jbg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.