
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurosci. , 14 May 2019
Sec. Autonomic Neuroscience
Volume 13 - 2019 | https://doi.org/10.3389/fnins.2019.00458
This article is part of the Research Topic Autonomic Neuroscience Editor’s Pick 2021 View all 19 articles
 Yun-Ru Lai1,2
Yun-Ru Lai1,2 Chih-Cheng Huang2Wen-Chan Chiu3Rue-Tsuan Liu3Nai-Wen Tsai2
Chih-Cheng Huang2Wen-Chan Chiu3Rue-Tsuan Liu3Nai-Wen Tsai2 Hung-Chen Wang4
Hung-Chen Wang4 Wei-Che Lin5
Wei-Che Lin5 Ben-Chung Cheng1,3Yu-Jih Su3Chih-Min Su6Sheng-Yuan Hsiao1,6Pei-Wen Wang3Jung-Fu Chen3
Ben-Chung Cheng1,3Yu-Jih Su3Chih-Min Su6Sheng-Yuan Hsiao1,6Pei-Wen Wang3Jung-Fu Chen3 Cheng-Hsien Lu1,2,7,8*
Cheng-Hsien Lu1,2,7,8*Background: Variability in the glycated hemoglobin (HbA1c) level is associated with a higher risk of microvascular complications in patients with type 2 diabetes. We tested the hypothesis that HbA1c variability is not only strongly associated with the presence but also the degree of severity of cardiovascular autonomic neuropathy (CAN) in patients with long diabetes durations (more than 10 years).
Methods: For each patient, the intrapersonal mean, standard deviation (SD), and coefficient of variation (CV) for HbA1c were calculated using all measurements obtained 3 years before the study. We constructed the composite autonomic scoring scale (CASS) as a measure of the severity of cardiovascular autonomic functions. Stepwise logistic regression and linear regression analyses were performed to evaluate the presence of CAN and the influence of independent variables on the mean CASS, respectively.
Results: Those with CAN had a higher mean age, a higher low-density lipoprotein cholesterol (LDL-C), HbA1c-SD, HbA1c-CV, mean HbA1c, and index HbA1c, higher prevalence of retinopathy as the underlying disease, and lower high-density lipoprotein (HDL) levels. Stepwise logistic regression showed that HbA1c-SD and retinopathy were risk factors that were independently associated with the presence of CAN. Mean HbA1c, HbA1c-CV, HbA1c-SD, and index HbA1c were positively correlated with mean CASS, and a multiple linear regression analysis revealed that HbA1c-SD was independently associated with the mean CASS.
Conclusion: HbA1c variability is strongly associated with not only the presence but also the degree of severity of CAN. A longitudinal study is required to confirm whether controlling blood glucose level is effective in reducing CAN progression.
Diabetic cardiovascular autonomic neuropathy (CAN) is common but is one of the most overlooked complications of diabetes (Ewing et al., 1980). Autonomic nervous systems, including parasympathetic and sympathetic nervous systems, innervate various organ systems and modulate their function. CAN indicates a length-dependent pattern of the disease (Papanas and Ziegler, 2015). The vagus nerve, responsible for approximately 75% of the parasympathetic activity in humans, can be damaged in the early phase of CAN (Ewing et al., 1985), resulting in decreased parasympathetic activity and contributing to sympathetic predominance. As the disease progresses, sympathetic denervation occurs in the late stage of CAN. Therefore, it has a wide spectrum of clinical presentation.
There is a wide variation in the prevalence of CAN, depending on the definition and criteria used for diagnosis. Estimating the severity of CAN is also a formidable challenge for clinicians. Although there are no uniform criteria for diagnosing or staging CAN (Tesfaye et al., 2010; Rolim et al., 2013), the recent Toronto Consensus recommends the use of four cardiovascular reflex tests [deep breathing, Valsalva maneuver (VM), orthostatic (30:15) and orthostatic hypotension] and frequency-domain tests as the most sensitive and specific method of assessing the presence of CAN in patients with diabetes (Spallone et al., 2011). Further, Phillip Low constructed the composite autonomic scoring scales (CASS) for laboratory quantification of generalized autonomic failure (Low, 1993) and the CASS have been proven useful for estimating the severity of CAN (Huang et al., 2016).
There are several well-known risk factors associated with CAN development, including age, diabetes duration, glycemic control, hypertension, and dyslipidemia, body mass index (BMI), and development of other microvascular complications (e.g., retinopathy, proteinuria) (Dafaalla et al., 2016). Glycemic variability (GV) is a term used to describe the impairment of glycemic control. Multiple measures of GV have been suggested as potential predictors for CAN, and long-term GV assessment using HbA1c variability is significantly associated with the presence of CAN (Fleischer, 2012; Jun et al., 2015; Yang et al., 2018).
Cardiovascular autonomic neuropathy has a strong influence on various cardiovascular diseases and leads to severe morbidity and mortality in patients with diabetes (Vinik et al., 2003; Vinik and Ziegler, 2007). To date, there is paucity of information on the estimation of the overall severity of CAN using the CASS and its relationship between chronic glycemic impairment and different cardio-metabolic parameters in patients with long-duration type 2 diabetes. Scientists have been exploring the role of chronic GV in the subsequent severity of CAN and developing therapeutic strategies that may be beneficial in patients with diabetes. Therefore, potential risk factors need to be delineated to determine patients who are most appropriate for aggressive treatment. In this study, we tested the hypothesis that chronic GV is not only a risk factor for the presence of CAN but is also associated with the severity of CAN in patients with type 2 diabetes. The successful translation of these approaches offers the promise of reducing microvascular complications and improving the quality of life of patients with type 2 diabetes.
A total of 238 patients (≥20 years old) with type 2 diabetes who visited the outpatient diabetic clinic at Kaohsiung Chang Gung Memorial Hospital in Taiwan were identified from our previous cross-sectional prospective study (IRB 96-1361B, 99-2276C) (Huang et al., 2016). The exclusion criteria included (1) number of HbA1c measurements less than four, (2) diabetes duration less than 10 years; (3) moderate-to-severe heart failure [New York Heart Association (NYHA) class III and IV]; and (4) any type of arrhythmia that prevents the analysis of heart rate variability, or pacemaker implantation due to any cause. Thus, only 110 participants were enrolled in the study (Figure 1). The study was approved by the Ethics Committee of Chang Gung Memorial Hospital Institutional Review Board (201701243B0 and 201800388B0C501).
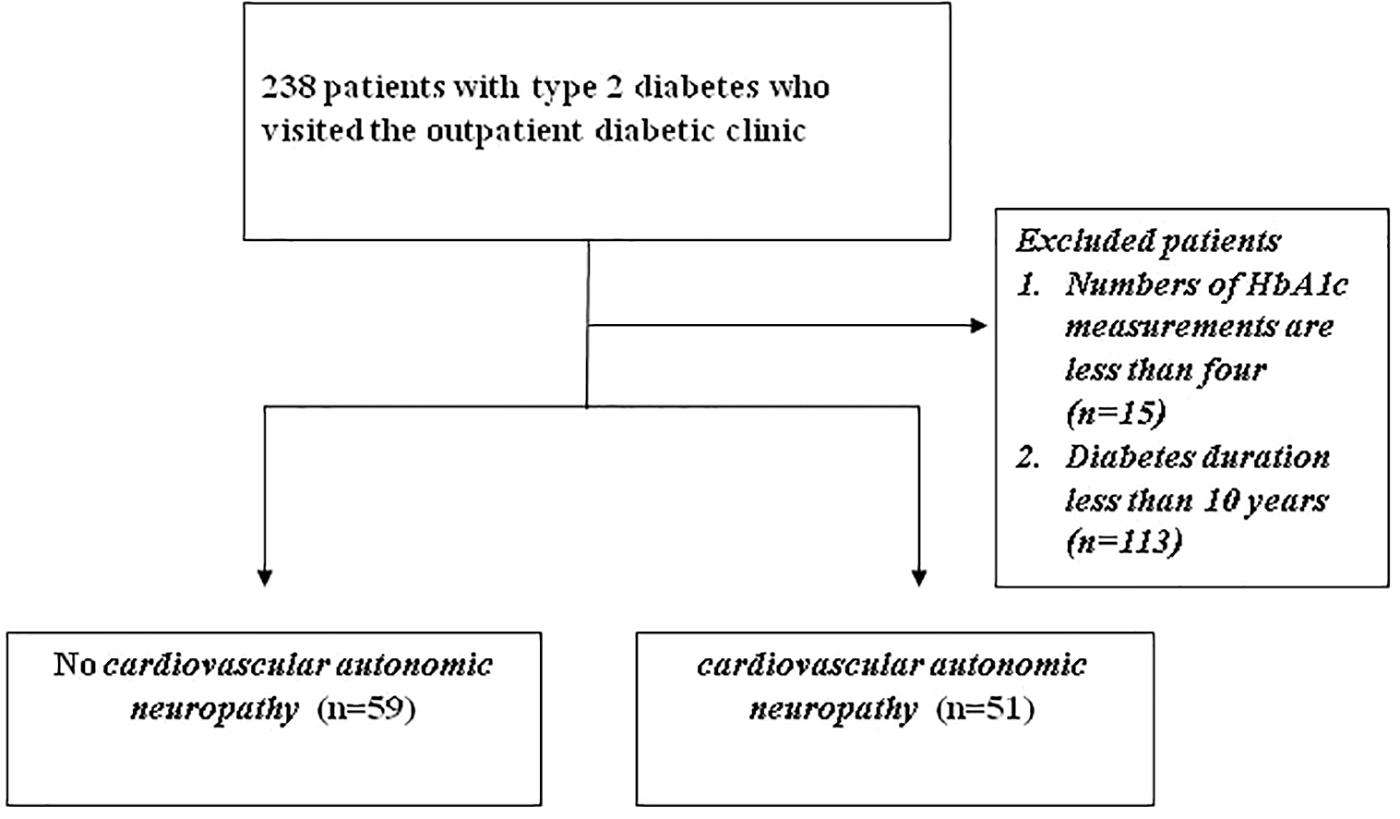
Figure 1. Enrollment of patients.
All patients underwent complete neurological and physical examinations upon enrollment and at their subsequent follow-ups at the outpatient clinic. A detailed medical history regarding prior use of medications was obtained from the patients and their families through standardized questions. Demographic data, including age, sex, duration of diabetes (years), BMI, systolic, and diastolic blood pressure (BP) during autonomic function testing, underlying diseases [hypertension, coronary artery disease (CAD), ischemic stroke, and diabetic retinopathy (DR)], and laboratory parameters were obtained at baseline.
For each patient, the intrapersonal mean, SD, and coefficient of variation [CV = HbA1c-SD/(0.1 × mean HbA1c)] of HbA1c was calculated using all measurements obtained 3 years before the study. The HbA1c-SD was considered a measure of GV and the CV, a normalized measure of GV. Because the number of individual visits could influence the HbA1c-SD (with fewer visits likely to artificially inflate SD), we defined the adjusted SD of HbA1c as the SD of HbA1c divided by [n/(n-1)]0.5 (where n is the number of HbA1c measurements), to minimize any effect of different values of HbA1c on the ones calculated (Kilpatrick et al., 2008). Our study was repeated using adjusted HbA1c-SD instead of HbA1c-SD.
All subjects underwent a standardized evaluation of the cardiovascular autonomic function, as described by Low (2003). The test battery consisted of the heart rate response to deep breathing (HR_DB), Valsalva ratio (VR), and baroreflex sensitivity (BRS). The heart rate was derived using a continuously recorded standard three-lead electrocardiography (Model 3000; Ivy Biomedical, Branford, CT, United States). Arterial BP was continuously measured at the finger, using beat-to-beat photoplethysmographic recordings (Finameter Pro; Ohmeda, Englewood, OH, United States). The tests were done between 9:00 am to noon for all patients. No coffee, food, alcohol, or nicotine was permitted 4 h before the tests. Patients on medications known to cause orthostatic hypotension or otherwise affecting autonomic testing were asked to stop taking the drug for five half-lives, provided that it was not harmful to the patient’s well-being. For patients on β-blockers for BP control, the drug was omitted on the day of the study and resumed after the test. The detailed computing of HR_DB and VR were as described by Low (2003). To quantify BRS, a linear regression analysis was performed between systolic BP and RR interval (RRI) changes during the early phase II of VM. In this phase, there was a progressive decrease in systolic BP due to reduced preload (venous return) and stroke volume with associated tachycardia (gradual shortening of RRI).
To improve the assessment of laboratory grading of CAN, we constructed a CASS for laboratory quantification of CAN according to our previous diabetic study (Huang et al., 2016). The severity of CAN was assessed using the cardiovagal and adrenergic sub-scores of the CASS. In this study, the scale was modified in the adrenergic sub-score since the 5-min head-up tilt test (HUTT) was not done in the current study. Thus, the CASS version used here allotted 3 points instead of 4 for the adrenergic domain. Further, patients with a CASS score ≥2 were defined as having CAN (Huang et al., 2016).
Data are expressed as means ± standard derivations (SDs) or medians (interquartile ranges). Categorical variables were compared using Chi-square or Fisher’s exact tests. Continuous variables that were not normally distributed in the Kolmogorov–Smirnov test were logarithmically transformed to improve normality and compared. Four separate statistical analyses were performed. Firstly, patients were stratified into two groups according to the presence or absence of CAN. One-way analysis of covariance (ANCOVA) was used to compare parameters of cardiovascular autonomic study with age as the added covariate. Secondly, the risk factors for the presence of CAN including sex and baseline characteristics, underlying diseases, and parameters of laboratory testing were analyzed using stepwise logistic regression. Thirdly, correlation analysis was used to evaluate the relationship between the CASS and variables that included age, diabetes duration, BMI, waist circumference, systolic and diastolic BP, and peripheral blood studies for vascular risks. Fourthly, stepwise models of multiple linear regression analysis were used to evaluate the influence of independent variables on the mean CASS. All statistical analyses were conducted using the SAS software package, version 9.1 (2002, SAS Statistical Institute, Cary, North Carolina).
The 110 patients with diabetes included 45 women and 65 men. Patient characteristics, baseline underlying diseases and laboratory data at assessment are presented in Table 1, stratified into two groups according to the presence or absence of CAN. Those with CAN had higher mean age (P = 0.002), higher low-density lipoprotein cholesterol (LDL-C), HbA1c-SD, HbA1c-CV, mean HbA1c and index HbA1c (P = 0.04, P = 0.003, P = 0.009, P = 0.009, and P = 0.01, respectively), higher prevalence of retinopathy as the underlying disease (P < 0.0001) and lower high-density lipoprotein (HDL) levels (P = 0.02). Significant variables used in the stepwise logistic regression model included mean age, baseline LDL-C, HbA1c-SD, CV HbA1c, mean HbA1c, index HbA1c, and HDL level and the presence of retinopathy as the underlying disease. After analysis of all the aforementioned variables, only HbA1c-SD (P = 0.007, OR = 10.1, 95% CI = 1.90–54.4) and presence of retinopathy (P < 0.0001, OR = 731.1, 95% CI = 67.9–7869.3) were independently associated with the presence of CAN.
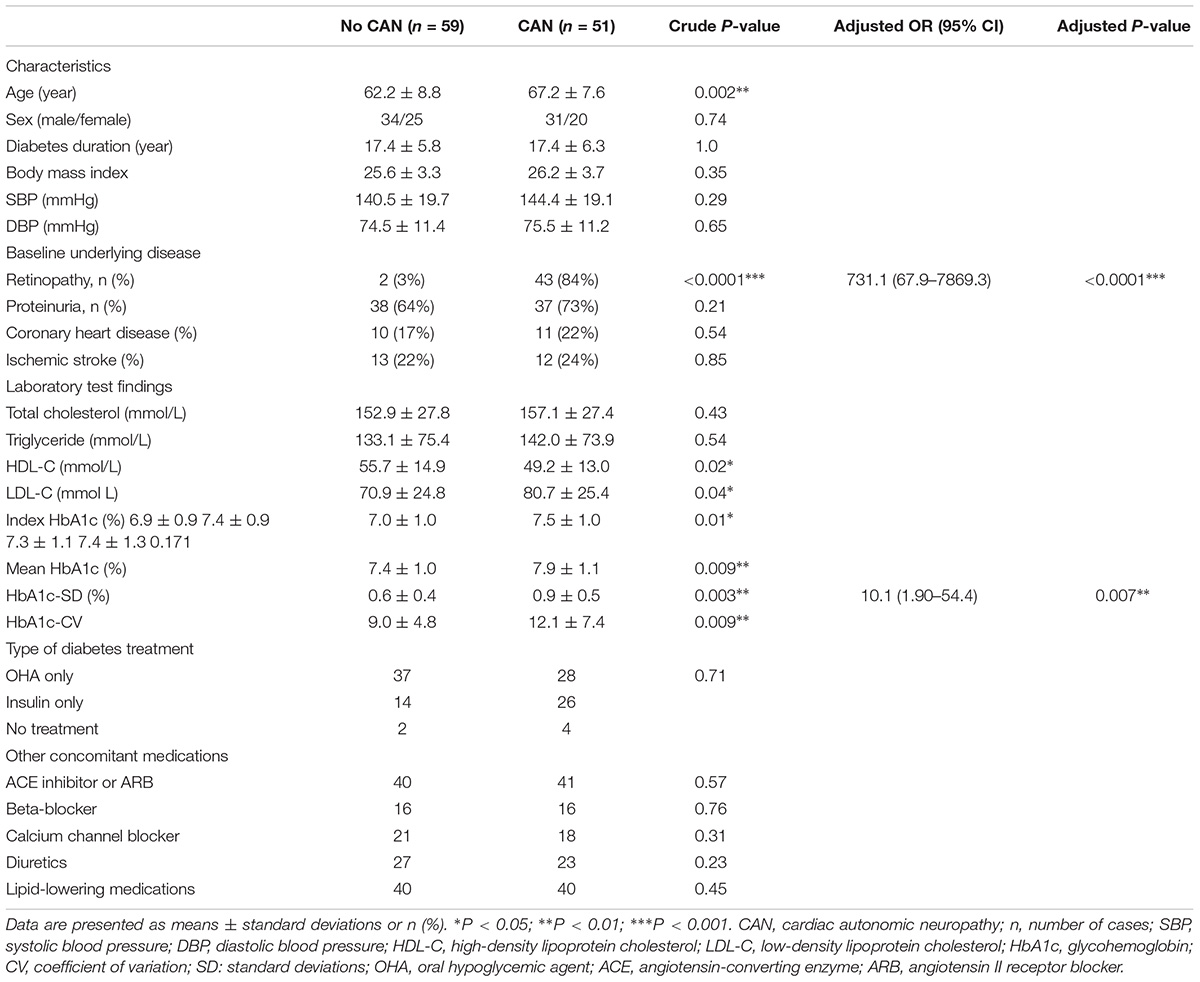
Table 1. Baseline characteristics of patients with Type 2 diabetes.
Cardiovascular autonomic study in patients with type 2 diabetes stratified into two groups according to the presence or absence of CAN is presented in Table 2. The parameters of cardiovascular autonomic study were compared by ANCOVA after controlling for age. Those with CAN had higher CASS (P < 0.0001) and lower HR_DB (P < 0.0001), VR P < 0.0001, and BRS P < 0.0001.
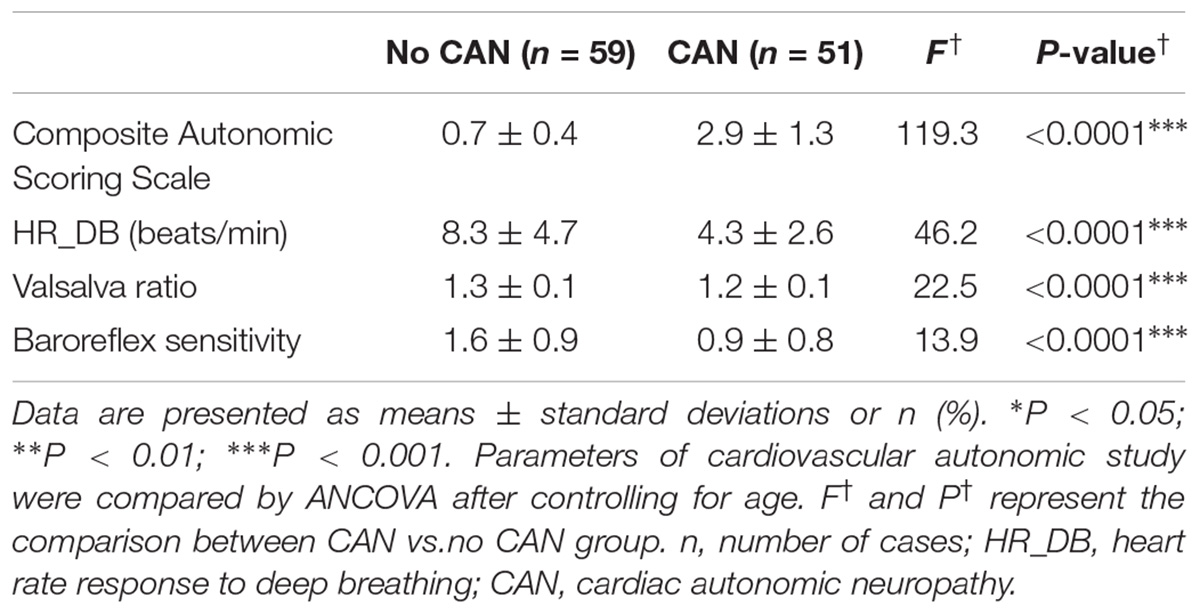
Table 2. Baseline cardiovascular autonomic study with Type 2 diabetes.
Correlation analysis parameters used to test the influence of GV and other vascular risk factors on CASS are listed in Table 3. The significant statistical results (correlation coefficient, P-value) were as follows: mean HbA1c (%) (r = 0.220, P = 0.028), HbA1c-CV (r = 0.197, P = 0.05), HbA1c-SD (r = 0.232, P = 0.02), index HbA1c (%) (r = 0.207, P = 0.039). All the correlation coefficients in mean HbA1c (%), HbA1c-CV, HbA1c-SD, and index HbA1c (%) indicate a weak positive linear relationship (r < 0.4).
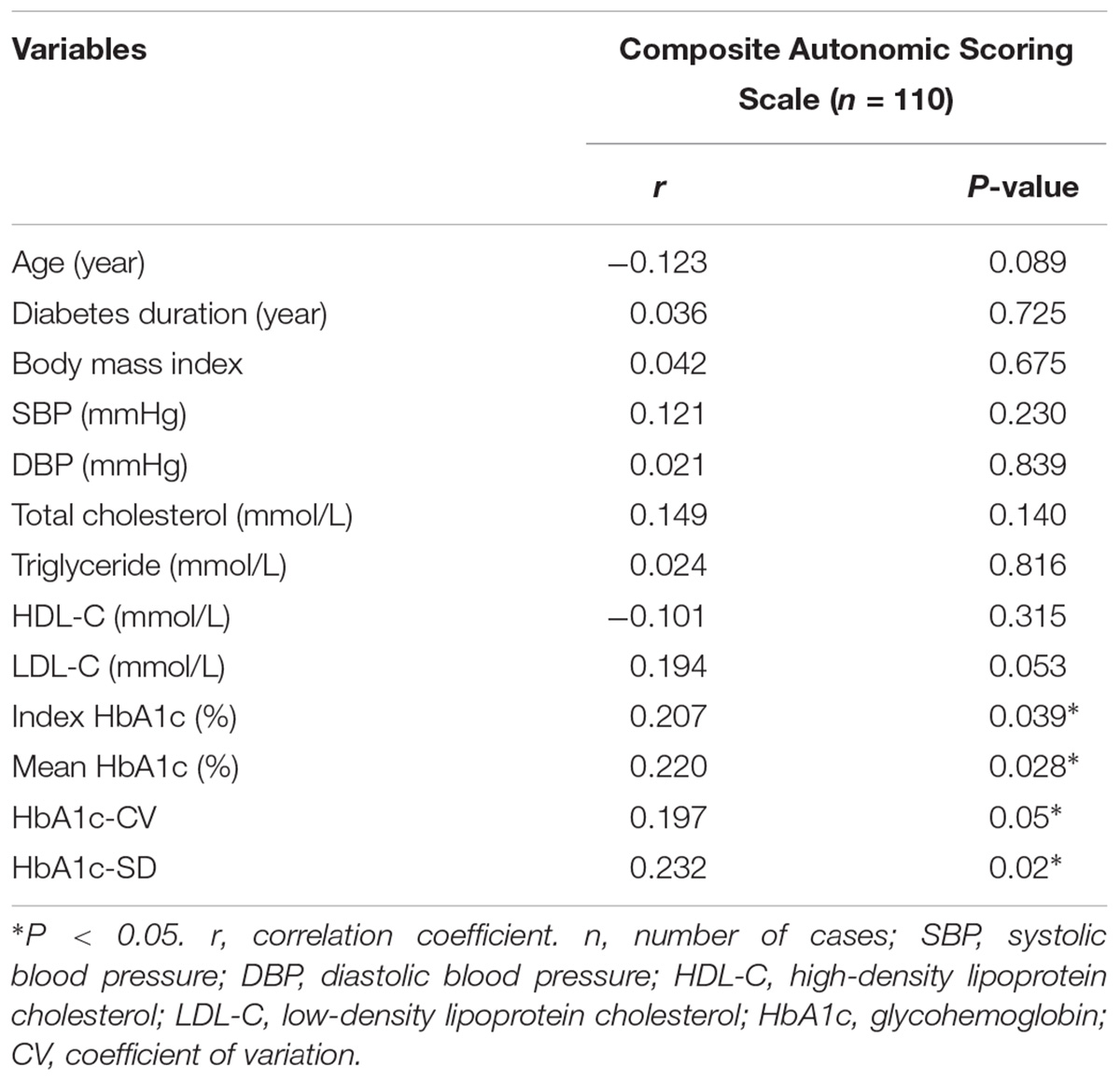
Table 3. Correlation analysis of composite autonomic scoring scale in patients with type 2 diabetes.
Effects of the variables on the CASS in patients with type 2 diabetes according to correlation analysis are listed in Table 4. Statistical analysis was subsequently carried out to decipher the relationship between the augmented CASS in patients with diabetes and GV. Based on correlation analysis, our results revealed that mean HbA1c, HbA1c-SD, and index HbA1c were significantly correlated with CASS (Table 3). We further employed multiple linear regression analysis on the aforementioned variables to identify the crucial determinant that underlies the augmented CASS in patients with diabetes. Results from the model analysis (Table 4) revealed that only HbA1c-SD were significantly associated with the CASS.
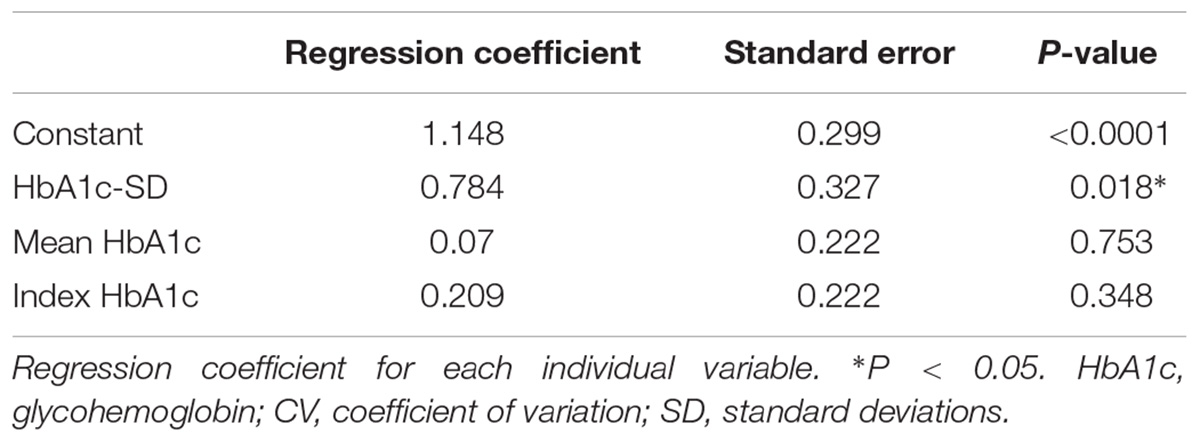
Table 4. Effects of the variables on composite autonomic scoring scale in patients with type 2 diabetes according to correlation analysis.
To our knowledge, this is the first study to confirm the hypothesis that HbA1c variability is not only strongly associated with the presence but also the degree of severity of CAN, in patients with long-duration type 2 diabetes. We examined the role of HbA1c variability on the presence and severity of CAN to obtain three major findings.
First, those with CAN had higher mean age, higher LDL-C, HbA1c-SD, HbA1c-CV, mean HbA1c, and index HbA1c, higher prevalence of retinopathy as the underlying disease, and lower HDL levels. Second, HbA1c-SD and the presence of retinopathy were independently associated with the presence of CAN. Finally, although mean HbA1c (%), HbA1c-CV, HbA1c-SD, and index HbA1c were positively correlated with the CASS score in correlation analysis, the correlation coefficient indicates a weak positive linear relationship (r < 0.4). Multiple linear regression analysis revealed that HbA1c-SD was independently associated with the mean CASS.
Aggressive control of blood glucose is pivotal for patients with type 2 diabetes, and can prevent microvascular and macrovascular complications (Brownlee and Hirsch, 2006; Siegelaar et al., 2010). Short-term GV indicated that patients with similar mean glucose or HbA1c values can show markedly different daily glucose profiles (Brownlee and Hirsch, 2006; Siegelaar et al., 2010). Either fluctuating or persisting high glucose levels can induce oxidative stress, contribute to endothelial dysfunction, and finally result in diabetic complications (Brownlee and Hirsch, 2006; Siegelaar et al., 2010). Recently, clinical evidence also demonstrated that long term GV might be related to microvascular complications in type 2 diabetes (Fleischer, 2012; Jun et al., 2015; Wei et al., 2016; Yang et al., 2018).
The pathophysiological mechanism of CAN development is multifactorial, and several studies reported the important role of cardiovascular risk factors, such as systolic BP, triglyceride levels, BMI, and smoking, in the development of CAN (Rolim et al., 2008; Dafaalla et al., 2016). Even more important, however, were the results of one clinical study that concluded that intensified multifactorial intervention (hyperglycemia, hypertension, dyslipidemia, and microalbuminuria) in patients with type 2 diabetes reduced the risk of CAN progression by 68% (Gæde et al., 1999). Another study also enhanced the role of intensive control in preventing and slowing the progression of CAN in patients with type 1 diabetes (The Diabetes Control and Complications Trial Research Group, 1998).
The risk factors for CAN that were identified may provide important clues to etiologies, or merely reflect chance associations. Only when the same risk factor is found to be associated with the severity of CAN consistently, can it be concluded that there is a plausible mechanistic link between the risk factor and the disease progression or prevention. To the best of our knowledge, only limited studies have investigated the impact of GV on the severity of CAN in type 2 diabetes (Jun et al., 2015; Yang et al., 2018). One study of 110 patients with type 2 diabetes who underwent both short term and long term GV (HbA1c variability) demonstrated that only long term GV (HbA1c variability) was significantly associated with the presence of CAN by logistic regression analysis, and higher long term GV (HbA1c variability) had an increased risk of advanced CAN (Jun et al., 2015). In this study, the authors only investigate the role of both short term and long term GV without other vascular risk factors in the severity of CAN which was graded using ordinal logistic regression analysis. Another study enrolled 681 subjects (294 normal, 318 early, and 69 severe CAN) and the severity of CAN was categorized as normal, early, or severe according to the cardiac autonomic reflex tests (CARTs) score. The study was repeated using HbA1c-CV or adj-HbA1c-SD instead of HbA1c-SD as a measure of HbA1c variability and performed to test the association between the CAN and HbA1c variability indices by multivariable logistic regression analysis (Yang et al., 2018). In comparison to the patients described in the previous two studies, our patients were older and had longer diabetes durations and HbA1c variability was not only strongly associated with the presence but also the degree of severity of CAN. The discrepancy between these studies and our study may be attributed to different enrollment criteria (e.g., age and diabetes duration of patients, the time period before the study for measurement of HbA1c variability was obtained, the minimum number of HbA1c measurements), diagnostic criteria for CAN, and statistical methods used for assessing the severity of CAN (ordinal logistic regression, multiple logistic regression and linear regression).
This study has several limitations. Firstly, although the measurement of HbA1c variability was obtained 3 years before the study and there was a relationship between HbA1c variability and the degree of severity of CAN in patients with diabetes in this observational study, our study does not allow inferring causality or whether controlling blood glucose can improve CAN, even though it can be a starting point for future studies. A prospective longitudinal study is necessary to evaluate the efficiency of CASS as a scale of severity in clinical follow-up. Secondly, we excluded patients whose disease duration for diabetes was less than 10 years and the number of HbA1c measurements were less than four. Thus, there is uncertainty in assessing the role of chronic glycemic impairment and other cardio-metabolic parameters in the patients with type 2 diabetes who were omitted. Thirdly, the severity of CAN was assessed using the modified CASS rather than the original version because the 5-min HUTT was not done in this study. We aimed to set up a highly effective autonomic screening service at the out-patient clinic. The tests of deep breathing and VM can be conducted only by one technician within 10–15 min. One may argue about the validity of the modified CASS. Table 5 lists the comparison between the modified and the original versions of CASS. The only difference is in the three points versus four points in the adrenergic sub-score. If the 5-min HUTT is done, the adrenergic sub-score may reach to four points in a patient with extremely severe autonomic failure. In other words, the limitation of modified CASS is mainly in its resolution in differentiating severe from extremely severe patients. However, it is uncommon for patients with diabetes to have severe autonomic failure. It was reported as occurring in about 1–5% of the diabetic population (Low, 1996). In the current study, only four patients had severe adrenergic failure (three points in adrenergic sub-score). The four patients are those who may have different scores between the two versions of CASS. In other words, it is certain that the other 106 patients (96%) would have the same scores even if the original version of CASS was used. Therefore, we suppose that the impact of alteration in CASS is trivial to this study. The final limitation is that only cardiovagal and adrenergic domains were assessed, and the sympathetic sudomotor function was not included in this study. Thus, all the variability in severity found in CAN may not have been accounted for and this may produce statistical bias. Other quantitative approaches to assess the sudomotor function, such as quantitative sudomotor axon reflex test or sudoscan, should be taken into account for future studies.
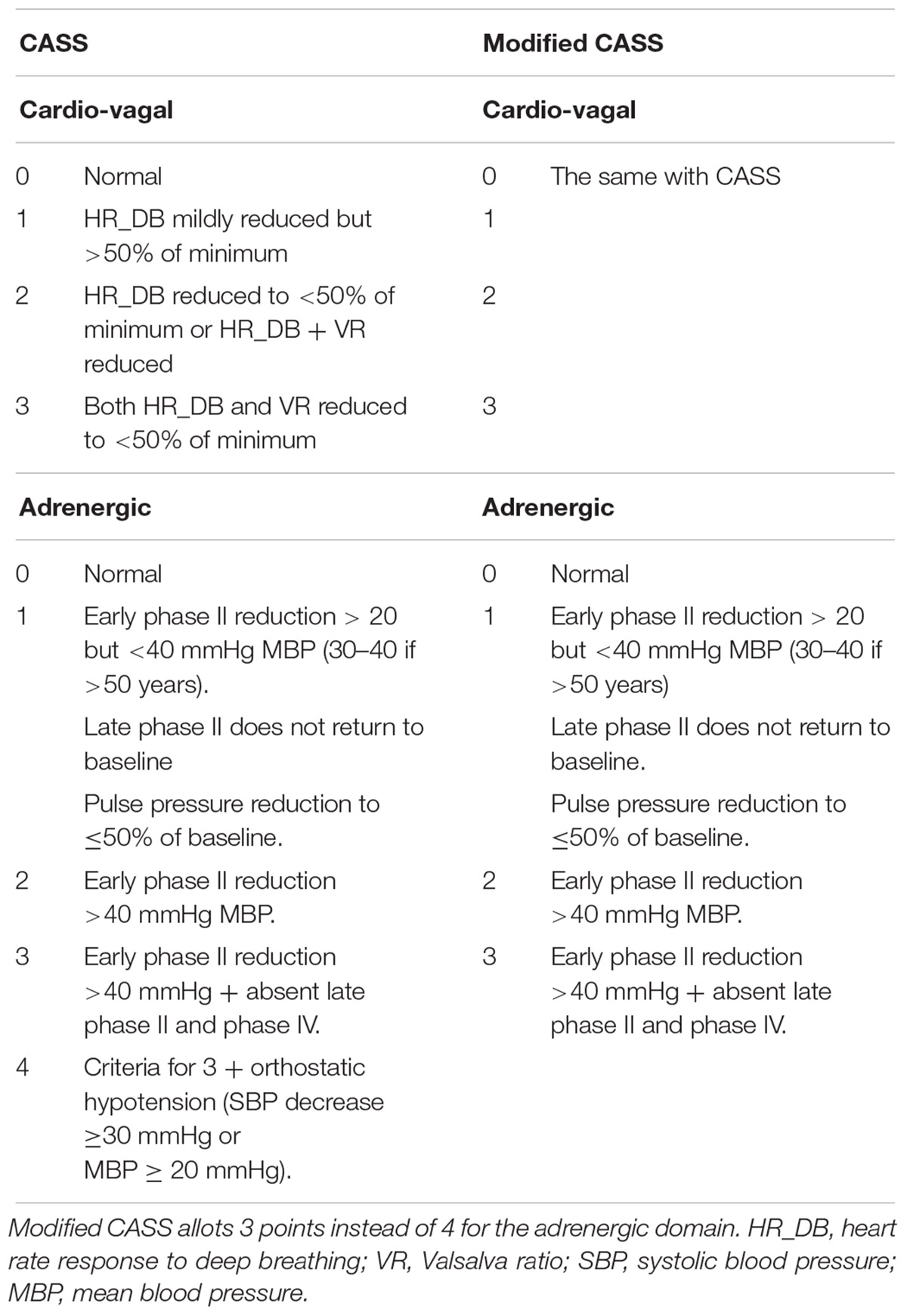
Table 5. Comparison of composite autonomic scoring Scale (CASS) and Modified CASS (sub-scores in cardiovagal and adrenergic domains).
Based on our results, HbA1c variability is not only strongly associated with the presence but also the degree of severity of CAN. As HbA1c variability is considered a prognostic factor, a longitudinal study is required in order to state that controlling blood glucose is effective in reduce CAN progression.
The data from this study can be acquired from the corresponding author upon reasonable request.
This study conformed to the guidelines of the Declaration of Helsinki, and the study has been approved by the Institutional Review Board of Chang Gung Memorial Hospital (201701243B0 and 201800388B0C501).
Y-RL participated in the design of the study and drafted the manuscript. W-CC, C-CH, R-TL, N-WT, H-CW, W-CL, B-CC, Y-JS, C-MS, S-YH, P-WW, and J-FC participated in the sequence alignment and clinical evaluation of patients. C-CH performed the statistical analysis. C-HL conceived the idea for the study, and participated in its design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.
This work was supported by grants from Chang Gung Memorial Hospital (Chang Gung Medical Research Project CMRPG8H0501).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank all the subjects who participated in this study.
BMI, body mass index; BRS, Baroreflex sensitivity; CAN, cardiac autonomic neuropathy; DBP, diastolic blood pressure; HbA1c, glycohemoglobin; HDL-C, high-density lipoprotein cholesterol; HR_DB, heart rate response to deep breathing; LDL-C, low-density lipoprotein cholesterol; SBP, systolic blood pressure; SD, standard deviation; VR, Valsalva ratio.
Brownlee, M., and Hirsch, I. B. (2006). Glycemic variability: a hemoglobin A1c–independent risk factor for diabetic complications. JAMA 295, 1707–1708. doi: 10.1001/jama.295.14.1707
Dafaalla, M. D., Nimir, M. N., Mohammed, M. I., Ali, O. A., and Hussein, A. (2016). Risk factors of diabetic cardiac autonomic neuropathy in patients with type 1 diabetes mellitus: a meta-analysis. Open Heart 3:e000336. doi: 10.1136/openhrt-2015-000336
Ewing, D., Campbell, I., and Clarke, B. (1980). Assessment of cardiovascular effects in diabetic autonomic neuropathy and prognostic implications. Ann. Intern. Med. 92, 308–311. doi: 10.7326/0003-4819-92-2-308
Ewing, D. J., Martyn, C. N., Young, R. J., and Clarke, B. F. (1985). The value of cardiovascular autonomic function tests: 10 years experience in diabetes. Diabetes Care 8, 491–498. doi: 10.2337/diacare.8.5.491
Fleischer, J. (2012). Diabetic autonomic imbalance and glycemic variability. J. Diabetes Sci. Technol. 6, 1207–1215. doi: 10.1177/193229681200600526
Gæde, P., Vedel, P., Parving, H.-H., and Pedersen, O. (1999). Intensified multifactorial intervention in patients with type 2 diabetes mellitus and microalbuminuria: the Steno type 2 randomised study. Lancet 353, 617–622. doi: 10.1016/S0140-6736(98)07368-1
Huang, C.-C., Lee, J.-J., Lin, T.-K., Tsai, N.-W., Huang, C.-R., Chen, S.-F., et al. (2016). Diabetic retinopathy is strongly predictive of cardiovascular autonomic neuropathy in type 2 diabetes. J. Diabetes Res. 2016:6090749. doi: 10.1155/2016/6090749
Jun, J. E., Jin, S.-M., Baek, J., Oh, S., Hur, K. Y., Lee, M.-S., et al. (2015). The association between glycemic variability and diabetic cardiovascular autonomic neuropathy in patients with type 2 diabetes. Cardiovasc. Diabetol. 14:70. doi: 10.1186/s12933-015-0233-0
Kilpatrick, E. S., Rigby, A. S., and Atkin, S. L. (2008). HbA1c variability and the risk of microvascular complications in type 1 diabetes: data from the DCCT. Diabetes Care 31, 2198–2202. doi: 10.2337/dc08-0864
Low, P. A. (1993). Composite autonomic scoring scale for laboratory quantification of generalized autonomic failure. Mayo. Clin. Proc. 68, 748–752. doi: 10.1016/S0025-6196(12)60631-4
Low, P. A. (1996). Diabetic autonomic neuropathy. Semin. Neurol. 16, 143–151. doi: 10.1055/s-2008-1040970
Low, P. A. (2003). Testing the autonomic nervous system. Semin. Neurol. 23, 407–421. doi: 10.1055/s-2004-817725
Papanas, N., and Ziegler, D. (2015). Risk factors and comorbidities in diabetic neuropathy: an update 2015. Rev. Diabet. Stud. 12, 48–62. doi: 10.1900/RDS.2015.12.48
Rolim, L. C., Sá, J. R., Chacra, A. R., and Dib, S. A. (2008). Diabetic cardiovascular autonomic neuropathy: risk factors, clinical impact and early diagnosis. Arq. Bras. Cardiol. 90, e24–e31. doi: 10.1590/S0066-782X2008000400014
Rolim, L. C., Souza, J. S. T., and Dib, S. (2013). Tests for early diagnosis of cardiovascular autonomic neuropathy: critical analysis and relevance. Front. Endocrinol. 4:173. doi: 10.3389/fendo.2013.00173
Siegelaar, S. E., Holleman, F., Hoekstra, J. B., and Devries, J. H. (2010). Glucose variability; does it matter? Endocr. Rev. 31, 171–182. doi: 10.1210/er.2009-0021
Spallone, V., Bellavere, F., Scionti, L., Maule, S., Quadri, R., Bax, G., et al. (2011). Recommendations for the use of cardiovascular tests in diagnosing diabetic autonomic neuropathy. Nutr. Metab. Cardiovasc. Dis. 21, 69–78. doi: 10.1016/j.numecd.2010.07.005
Tesfaye, S., Boulton, A. J., Dyck, P. J., Freeman, R., Horowitz, M., Kempler, P., et al. (2010). Diabetic neuropathies: update on definitions, diagnostic criteria, estimation of severity, and treatments. Diabetes Care 33, 2285–2293. doi: 10.2337/dc10-1303
The Diabetes Control and Complications Trial Research Group. (1998). The effect of intensive diabetes therapy on measures of autonomic nervous system function in the Diabetes Control and Complications Trial (DCCT). Diabetologia 41, 416–423. doi: 10.1007/s001250050924
Vinik, A. I., Maser, R. E., Mitchell, B. D., and Freeman, R. (2003). Diabetic autonomic neuropathy. Diabetes Care 26, 1553–1579. doi: 10.2337/dc10-1303
Vinik, A. I., and Ziegler, D. (2007). Diabetic cardiovascular autonomic neuropathy. Circulation 115, 387–397. doi: 10.1161/CIRCULATIONAHA.106.634949
Wei, F., Sun, X., Zhao, Y., Zhang, H., Diao, Y., and Liu, Z. (2016). Excessive visit-to-visit glycemic variability independently deteriorates the progression of endothelial and renal dysfunction in patients with type 2 diabetes mellitus. BMC Nephrol. 17:67. doi: 10.1186/s12882-016-0300-0
Keywords: cardiovascular autonomic neuropathy, composite autonomic scoring scale, HbA1c variability, long diabetes duration, type 2 diabetes
Citation: Lai Y-R, Huang C-C, Chiu W-C, Liu R-T, Tsai N-W, Wang H-C, Lin W-C, Cheng B-C, Su Y-J, Su C-M, Hsiao S-Y, Wang P-W, Chen J-F and Lu C-H (2019) HbA1C Variability Is Strongly Associated With the Severity of Cardiovascular Autonomic Neuropathy in Patients With Type 2 Diabetes After Longer Diabetes Duration. Front. Neurosci. 13:458. doi: 10.3389/fnins.2019.00458
Received: 14 February 2019; Accepted: 24 April 2019;
Published: 14 May 2019.
Edited by:
Maurizio Acampa, Azienda Ospedaliera Universitaria Senese, ItalyReviewed by:
Antonio Roberto Zamunér, Catholic University of Maule, ChileCopyright © 2019 Lai, Huang, Chiu, Liu, Tsai, Wang, Lin, Cheng, Su, Su, Hsiao, Wang, Chen and Lu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Cheng-Hsien Lu, Y2hsdTk5QG1zNDQudXJsLmNvbS50dw==; Y2hsdTk5QGFkbS5jZ21oLm9yZy50dw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.