 Roberto Lopez-Rosado
Roberto Lopez-Rosado Andrea Kimalat
Andrea Kimalat Matthew Bednarczyk
Matthew Bednarczyk Jane E. Sullivan
Jane E. Sullivan
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurosci. , 16 April 2019
Sec. Perception Science
Volume 13 - 2019 | https://doi.org/10.3389/fnins.2019.00337
This article is part of the Research Topic The Sensing Brain: The Role of Sensation in Rehabilitation and Training View all 13 articles
Objective: To determine if sensory amplitude electrical stimulation (SES) delivered via sock electrode combined with standing and mobility activities improved gait speed, sensation, balance, and participation in chronic stroke. It was hypothesized that SES would enhance the effectiveness of exercise, resulting in reduced impairment and improved function.
Design: Case Series.
Setting: Home-based intervention.
Participants: Thirteen adults (56.5 + 7.84 years old) with chronic stroke (8.21 + 4.36 years post) and hemiparesis completed the study. Participants were community ambulators.
Intervention: Participants completed 6 weeks of self-administered SES delivered via sock electrode concurrent with standing and mobility activities for a minimum of 5 days/week for 30-min, twice daily.
Outcome Measures: Berg Balance Scale (BBS), Stroke Rehabilitation Assessment of Movement—LE subscale (STREAM), 10 Meter Walk Test (10 MWT), Activities-Specific Balance Confidence Scale (ABC), Stroke Impact Scale (SIS), Perceptual Threshold of Electrical Stimulation (PTTES), and Monofilament testing were administered at pre-test, post-test, and 3-month follow up.
Results: Baseline sensory scores and change scores on functional outcomes were analyzed using Pearson Product-Movement Correlation Coefficients, Friedman test, and Linear mixed models. There was a significant change with 10 MWT self-selected pace (Friedman's p = 0.038). Pre-post intervention changes in other outcome measures were not significant. According to the Cohen's effect size classification, there were medium effect sizes for both the STREAM-LE and Monofilaments.
Conclusion: The use of home-based SES via sock electrode combined with standing and mobility activities may contribute to improve gait speed in chronic stroke.
Stroke is a leading cause of disability and the fifth leading cause of death in adults in the United States (Mozaffarian et al., 2015). Approximately 50% of this population regains independent ambulation by the end of rehabilitation; however 73% have some degree of long-term gait disability (Woolley, 2001). The amount of community walking done by individuals post-stroke is considerably less than their healthy peers (Michael and Macko, 2007). Falls are a serious consequence of stroke (Langhorne et al., 2000), with more than half of individuals experiencing a fall (Ashburn et al., 2008; Sackley et al., 2008). Post stroke falling is associated with gait and balance dysfunction (Minet et al., 2015). Post stroke changes in sensory dysfunction (Carey, 1995; Winward et al., 2007; Connell et al., 2008; Tyson et al., 2008) have also been associated with falls following stroke (Yates et al., 2002; Tyson et al., 2006; Wutzkea et al., 2013).
Sensory amplitude stimulation (SES) is electrical stimulation utilized at a threshold to stimulate sensory neurons only without stimulating motor neurons. In healthy adults, SES has been reported to enhance cortical motor excitability (Hamdy et al., 1998; Ridding et al., 2000; Kaelin-Lang et al., 2002; Golaszewski et al., 2004; Tinazzi et al., 2005; Meesen et al., 2010) and produce short-term plastic changes in the motor and sensory cerebral cortices (Ridding et al., 2001; Tinazzi et al., 2005; Wu et al., 2005). The enhanced afferent input provided by SES has been hypothesized to contribute to motor recovery of individuals with neurological conditions (Kwong et al., 2008; Bastos Conforto et al., 2018).
In adults post-stroke, SES use has been associated with body structure/function-domain improvements in force (Ng and Hui-Chan, 2007; Klaiput and Kitisomprayoonkul, 2009; Yan et al., 2009; Conforto et al., 2010; Tyson et al., 2013) and sensation (Ng and Hui-Chan, 2007; Tyson et al., 2013). Positive activity-domain changes such as improved gait speed, walking distance, balance, trunk control, and foot placement have been reported. Use-dependent plastic changes in the sensorimotor cortex following SES intervention have been demonstrated post-stroke. A recent systematic review on SES use following stroke examined 15 studies and concluded that the intervention has beneficial effects on motor recovery, especially when concurrently administered with standing and mobility activities The diverse outcome measures used across studies precluded meta-analysis, but the majority of studies reported significant effects on at least one outcome.
While preliminary positive findings following SES interventions post-stroke have been reported, important gaps in the literature remain. Only a small number of studies have examined retention by conducting follow up testing. The majority of SES studies to date have utilized surface electrodes located either over muscles or nerves corresponding to the target function. This electrode placement might actually interfere with activity. Several recent studies have utilized wearable electrodes (socks, gloves), which enable peripheral stimulation over a broad receptor field concurrent with activity (Ng and Hui-Chan, 2007; Yan et al., 2009; Tyson et al., 2013). Finally, studies have been primarily conducted in a clinic or research lab. Few studies have sought to examine whether beneficial effects can occur with a home-based SES intervention.
The aim of this study was to examine the effects of a 6-week intervention of home-based SES via sock electrode delivered during standing and mobility activities in individuals with chronic stroke. This will be known as “SES plus activity.” Our primary hypothesis was that there would be significant improvements in gait speed, balance, and balance confidence, which would be retained at 3-months post-intervention. We also hypothesized that there would be improvements in quality of life and in lower extremity active movement.
Participants were recruited from a university-based stroke database. Inclusion criteria were: (1) diagnosis of chronic stroke (>6 months); (2) able to ambulate in the community; (3) at least 21 years of age; (4) English-speaking. Exclusion criteria were: (1) contraindications to electrical stimulation (such as active local infection, inflammation, or malignancy); (2) positive history of neurologic diagnosis other than stroke; (3) chemodenervation (e.g., BotoxTM) in the more involved lower extremity within the past 6 months. All participants were informed of their rights and the expectations for the study. Participants provided informed consent per the protocol as outlined by the Northwestern University Institutional Review Board Office.
This study used a case series design with a pre-test, post-test, and follow-up. All assessment sessions were completed in a university setting. Research participants completed the 6-week intervention primarily in their home and community. We used STROBE cohort reporting guides (von Elm et al., 2007).
Electrical stimulation for SES plus activity was delivered using a muscle stimulator (EMPI, Inc., St. Paul, MN, USA) through a Silver-Thera sock electrode (Prizm Medical, Inc., Duluth, GA, USA) worn on the more involved foot. A secondary 2 × 2″ pre-gelled electrode was placed over the Tibialis anterior muscle belly. Stimulator parameters were as follows: symmetrical biphasic waveform, pulse duration 250 ms, stimulus frequency 50 Hz, duty cycle 10-s ON: 10-s OFF, and amplitude above sensory threshold but below motor threshold. Participants performed standing and mobility activities while receiving SES plus activity for a minimum of 30 min twice a day, 5 days/week for 6 weeks. Participants were not provided with a standard set of upright activities. They were only instructed to be standing and active during the stimulation. Participants reported walking around their home, leaving the house to run errands to the pharmacy and supermarket, attending church services and doctor's appointments. A compliance meter on the stimulator captured stimulation time, but didn't account for movement time. Additionally, all participants completed a daily log sheet and recorded stimulation time and standing and mobility activities. Daily logs were detailed and discussed with all participants during reassessment times; this method proved to be efficacious as our participants reported feeling independent while being accountable recording their activities.
Participants returned to the university setting for a minimum two sessions during the 6-week period. The purpose of the visits was to monitor adherence, answer participant questions, to assess the stimulator, and readjust the sensory threshold if needed.
The outcome measures administered at pre-test, post-test, and 3 months follow-up included:
The reliability and responsiveness of this test has been established in chronic stroke, as well as its high correlation with self- reported outcome measures in this population. Lower scores correspond to higher gait speed and lower risk for falls. Both self-selected and fast pace were assessed (Bushnell et al., 2015).
This is a self-reported survey that captures participant's perceived balance confidence in a 0–100% range (the higher the score, the better the perceived balance). Reliability and normative scores have been reported for chronic stroke (Salbach et al., 2006).
The BBS examines static and dynamic balance performance. Reliability and responsiveness data is highly correlated with the ABC for individuals post-chronic stroke. Higher scores are indicative of better balance performance (Salbach et al., 2006).
This is a multi-dimensional, self-reported health status measure post-stroke. Reliability and validity has been established specifically for individuals post-stroke. Responsiveness and normative data have been reported (Bushnell et al., 2015).
The STREAM-LE was used to assess voluntary movement in the lower extremity. It has established reliability and responsiveness and normative data in adults post-stroke, and it is recommended as one assessment for function and strength in the paretic lower extremity (Huang et al., 2015).
Assessment with monofilaments was conducted with the Semmes-Weinstein monofilaments (SWM) test on the sole of the paretic feet. Reliability of the SWM test was high on the paralyzed side (rs = 0.86, κ = 0.71–0.79), it was low on the other side without paralysis (rs = 0.33–0.50, κ = 0.33–0.50; Arakawa et al., 2012).
Friedman tests were used to assess overall change over time. Linear mixed models were used as post-tests to demonstrate between which assessment points a significant change was seen. Due to the small sample size, these models were also fit adjusting for one covariate at a time.
Baseline sensory scores and change scores on functional outcomes were analyzed using Pearson Product-Movement Correlation Coefficients. Effect sizes were calculated for each of the outcome measures, as previous similar studies (Sullivan et al., 2015).
Fifteen participants were enrolled; 13 completed the study. Table 1 summarizes participants' characteristics. Two participants dropped* from the study because of personal reasons unrelated to the study.
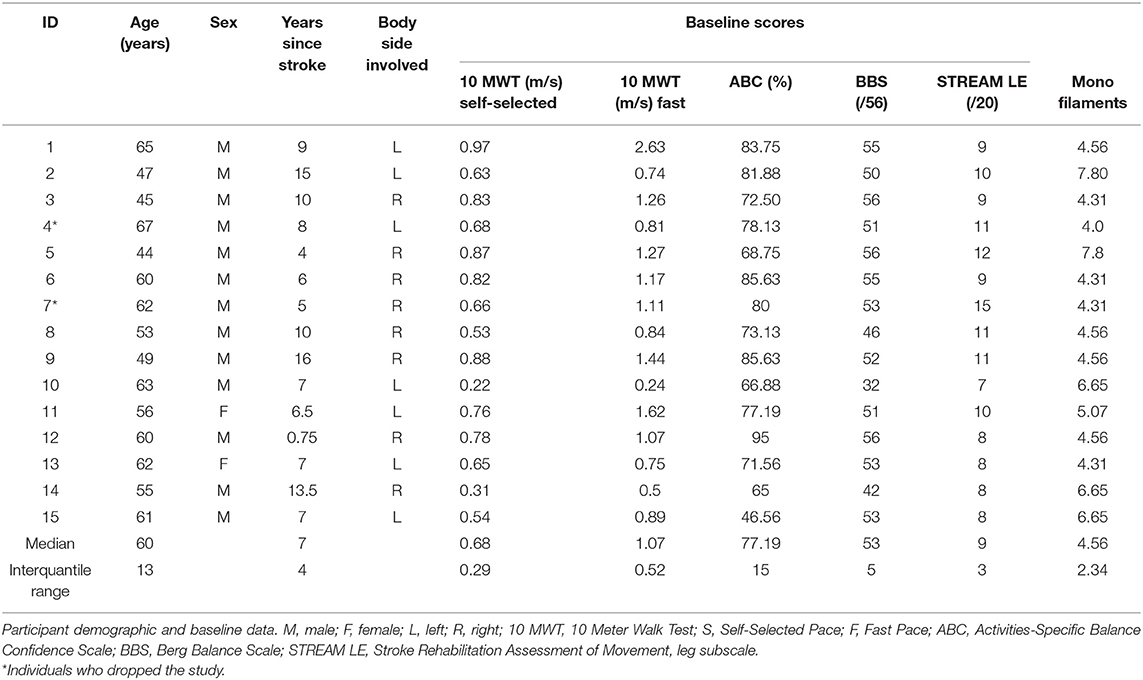
Table 1. Participant demographic and baseline data.
Table 2 illustrates the mean outcome measures over time of those who completed the study. There was a significant change over time with 10 MWT at self-selected pace (Friedman's p = 0.038). Using a linear mixed models analysis, there was a significant effect on 10 MWT at self-selected pace, p = 0.030, comparing baseline to post-test. This remained significant after adjusting for time from onset of stroke, or the use of an assistive device. The change in other outcome measures between assessment periods was not significant.
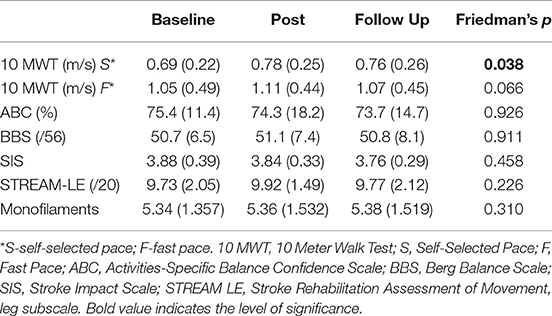
Table 2. Mean (SD) of outcomes measures over time.
To account for sample size, Cohen's effect size classifications were determined (Cohen, 1988). There were medium effect sizes for both the STREAM-LE and Monofilaments in participants from baseline to follow up. A large effect size was also observed for both 10 MWT at self-selected and fast pace (see Table 3).
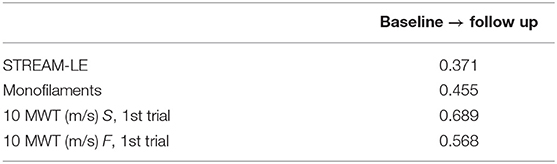
Table 3. Effect size of treatment between Baseline and Follow-Up.
Baseline sensory status of the hemiparetic plantar surface of the foot was assessed via the Perceptual Threshold of Electrical Stimulation (PTTES) and Monofilament testing on three locations. This tool has been shown to be reliable for testing sensation following stroke.
Baseline sensory status (both PTTES & Monofilaments) showed moderate to strong correlation with Baseline SIS 16 scores and change scores on the SIS 16 and ABC, suggesting sensory status may be associated with self- perception of physical performance (refer to Table 4).
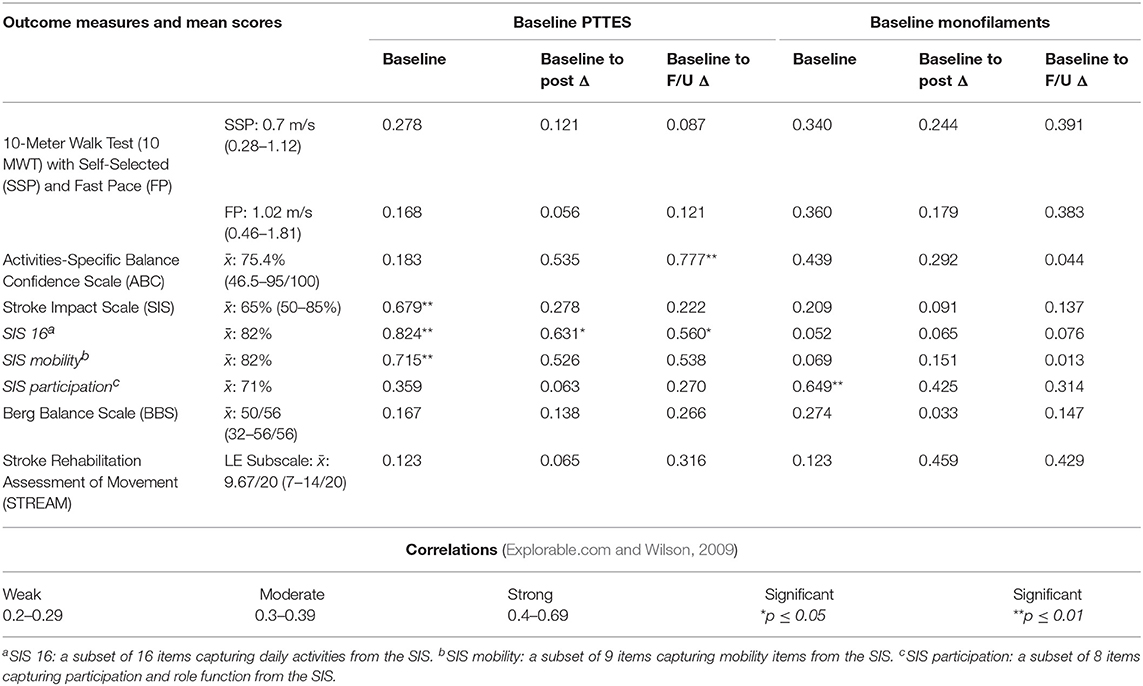
Table 4. Correlations between outcome measures and sensory data.
Participants experienced significant group effects changes in self-selected walking speed following SES plus activity in the home and community setting. These effects were maintained after the end of the intervention, but they weren't sustained at follow up.
Moderate to strong correlations with Baseline SIS 16 scores and change scores on the SIS 16 and ABC may suggest that sensory status may be associated with self- perception of physical performance. Greater sensory impairment was associated with lower self- reported baseline status. It remains unclear whether utilizing PTTES and/or Monofilaments to assess sensory status is the optimal approach.
The significant improvement in the gait speed of individuals with a more recent stroke and younger age may be related to an enhanced neural plasticity potential. The medium effect sizes in the STREAM-LE supports that possibility. Stimulating the paretic distal lower extremity at the sensory level may have an effect on the motor output level required for self-selected gait speed, suggesting a sensorimotor integration loop. This may potentially influence optimal SES dosage parameters to positively affect self-selected gait speed, which has implications on balance functional levels in individuals post-stroke at a chronic stage.
There were no other changes in other administered outcome measures. Participants scored highly at baseline on the BBS and ABC, so there might have been a ceiling effect. Alternatively, these outcome measures may have been less sensitive to changes with this intervention.
The sock electrode delivered electrical stimulation over the entire surface of the foot and distal leg instead of targeting specific distal lower extremity musculature. Different target areas or affected nerves may have had an impact on performance and outcomes in this study. A control trial would allow a more rigorous comparison of the elements of the intervention.
Participants self-monitored dosage and performed the prescribed intervention independently; therefore, compliance and adherence to the intervention protocol may have had an impact on outcomes. In addition, the variability of activities performed within SES plus activity is a limitation as it was not uniform across all subjects. Other limitations of this study include the small sample size, lack of a control group, and lack of formal measures of adherence to the SES plus activity program. While the results are preliminary, SES plus activity has the potential for clinical benefit and should be further studied in a large, randomized controlled study that includes a feasibility assessment.
We believe that this is the first study that combines SES with standing and mobility activities in a community setting. In an era with limited sources for formal physical therapy, a home base program that produces beneficial functional outcomes is an attractive therapeutic alternative.
Sensory data is related to both physical performance and perceived physical performance. Future studies may consider stratifying research participants based on baseline functional and chronicity level (how long ago they had the stroke). This may inform patient characteristics most associated with change. Establishing evidence based practice guidelines to determine the appropriate dosing of SES parameters to improve LE motor function had remained a challenge.
This study was approved by the Northwestern University Institutional Review Board Office, Northwestern University, Chicago IL (#STU00097364).
In our study, adults post-stroke wore a sock electrode, which allowed for concurrent delivery of Sensory Electrical Stimulation (SES) during standing and mobility activities. Our findings suggest that this intervention resulted in a significant improvement in the gait speed of younger individuals with a more recent stroke. We believe that this is the first study that combines SES with standing and mobility activities in a community setting.
RL-R was designated as first author, wrote, edited, and prepared the manuscript for publication. JS conceived the study and participated in its design and coordination and helped to draft the manuscript. RL-R, JS, MB, and AK participated in data collection and analysis. The authors of this study declared no potential conflicts of interest regarding the research conducted, authorship, or publication of this manuscript.
This work was funded by internal funds, Department of Physical Therapy and Human Movement Sciences, Northwestern University, Chicago IL.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling editor is currently editing a Research Topic with one of the authors JS, and confirms the absence of any other collaboration.
Arakawa, T., Otao, H., Okamura, M., Nakao, H., Hachiya, M., Mizokami, A., et al. (2012). Reliability of the Semmes-Weinstein monofilaments test in stroke patients. Jap. J. Health Promot. Phys. Ther. 2, 65–68. doi: 10.9759/hppt.2.65
Ashburn, A., Hyndman, D., Pickering, R., Yardley, L., and Harris, S. (2008). Predicting people with stroke at risk of falls. Age Ageing 37, 270–276. doi: 10.1093/ageing/afn066
Bastos Conforto, A., Monteiro dos Anjos, S., Marques Bernardo, W., Alves da Silva, A., Conti, J., Machado, A. G., et al. (2018). Repetitive peripheral sensory stimulation and upper limb performance in stroke: a systematic review and meta analysis. Neurorehabil. Neural Repair. 10:1177. doi: 10.1177/1545968318798943
Bushnell, C., Bettger, J. P., Cockroft, K. M., Cramer, S. C., Edelen, M. O., Hanley, D., et al. (2015). Chronic stroke outcome measures for motor function intervention trials: expert panel recommendations. Circulation 8, S163–S169. doi: 10.1161/CIRCOUTCOMES.115.002098
Carey, L. M. (1995). Somatosensory loss after stroke. Critic. Rev. Phys. Rehabil. Med. 7, 51–91. doi: 10.1615/CritRevPhysRehabilMed.v7.i1.40
Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences, 2nd Edn. South Wellfleet: Routledge.
Conforto, A. B., Ferreiro, K. N., Tomasi, C., Laurenti dos Santos, R., Moreira, V. L., Marie, S. K. N., et al. (2010). Effects of somato-sensory stimulation on motor function after subacute stroke. Neurorehabil. Neural Repair. 24, 263–272. doi: 10.1177/1545968309349946
Connell, L. A., Lincoln, N. B., and Radford, K. A. (2008). Somatosensory impairment after stroke: frequency of different deficits and their recovery. Clin. Rehabil. 22, 758–767. doi: 10.1177/0269215508090674
Explorable.com Wilson, L. T. (2009). Statistical Correlation is a Statistical Technique Which Tells us if Two Variables are Related. Available online at: https://explorable.com/statistical-correlation (accessed March 14, 2019).
Golaszewski, S. M., Siedentopf, C. M., Koppelstaetter, F., Rhomberg, P., Guendisch, G. M., Schlager, A., et al. (2004). Modulatory effects on human sensorimotor cortex by whole-hand afferent electrical stimulation. Neurology 62, 2262–2269. doi: 10.1212/WNL.62.12.2262
Hamdy, S., Rothwell, J. C., Aziz, Q., Singh, K. D., and Thompson, D. G. (1998). Long-term reorganization of human motor cortex driven by short-term sensory stimulation. Nat Neurosci. 1, 64–68. doi: 10.1038/264
Huang, Y. J., Chen, K. L., Chou, Y. T., Hsueu, I. P., Hou, C. Y., and Hsieh, C. L. (2015). Comparison of the responsiveness of the long-form and simplified stroke Rehabilitation Assessment of Movement: group- and individual-level; analysis. Phys. Ther. 95, 1172–1183. doi: 10.2522/ptj.20140331
Kaelin-Lang, A., Luft, A. R., Sawaki, L., Burstein, A. H., Sohn, Y. H., and Cohen, L. G. (2002). Modulation of human corticomotor excitability by somatosensory input. J. Physiol. 540(Pt 2), 623–33. doi: 10.1113/jphysiol.2001.012801
Klaiput, A., and Kitisomprayoonkul, W. (2009). Increased pinch strength in acute and subacute stroke patients after simultaneous median and ulnar sensory stimulation. Neurorehabil. Neural Repair. 23, 351–356. doi: 10.1177/1545968308324227
Kwong, P. W., Ng, G. Y., Chung, R. C., and Ng, S. S. (2008). Trasncutaneous electrical nerve stimulation improves walking capacity and reduces spasticity in stroke survivors: a systematic review and meta analysis. Clin. Rehabil. 32, 1203–1219. doi: 10.1177/0269215517745349
Langhorne, P., Stott, D. J., Robertson, L., MacDonald, J., Jones, L., McAlpine, C., et al. (2000). Medical complications after stroke: a multicenter study. Stroke 31, 1223–1229. doi: 10.1161/01.STR.31.6.1223
Meesen, R. L., Cuypers, K., Rothwell, J. C., Swinnen, S. P., and Levin, O. (2010). The effect of long-term TENS on persistent neuroplastic changes in thehuman cerebral cortex. Hum. Brain Mapping 32, 872–882. doi: 10.1002/hbm.21075
Michael, K., and Macko, R. F. (2007). Ambulatory activity intensity profiles, fitness, and fatigue in chronic stroke. Topics Stroke Rehabil. 14, 5–12. doi: 10.1310/tsr1402-5
Minet, L. R., Peterson, E., von Koch, L., and Ytterberg, C. (2015). Occurance and predictors of falls in people with stroke. Stroke 46, 2688–2690. doi: 10.1161/STROKEAHA.115.010496
Mozaffarian, D., Benjamin, E. J., Go, A. S., Arnett, D. K., Blaha, M. J., Cushman, M., et al. (2015). Heart disease and stroke statistics-−2015 update a report from the american heart association. Circulation 131:e29-322. doi: 10.1161/CIR.0000000000000152
Ng, S. S. M., and Hui-Chan, C. W. Y. (2007). Transcutaneous electrical nerve stimulation combined with task-related training improves lower limb functions in subjects with chronic stroke. Stroke 38, 2953–2959. doi: 10.1161/STROKEAHA.107.490318
Ridding, M. C., Brouwer, B., Miles, T. S., Pitcher, J. B., and Thompson, P. D. (2000). Changes in muscle responses to stimulation of the motor cortex induced by peripheral nerve stimulation in humans. Exp. Brain Res. 2000, 135–143. doi: 10.1007/s002219900269
Ridding, M. C., McKay, D. R., Thompson, P. D., and Miles, T. S. (2001). Changes in corticomotor representations induced by prolonged peripheral nerve stimulation in humans. Clin. Neurophysiol. 112, 1461–1469. doi: 10.1016/S1388-2457(01)00592-2
Sackley, C., Brittle, N., Patel, S., Ellins, J., Scott, M., Wright, C., et al. (2008). The prevalence of joint contractures, pressure sores, painful shoulder, other pain, falls, and depression in the year after a severely disabling stroke. Stroke 39, 3329–3334. doi: 10.1161/STROKEAHA.108.518563
Salbach, N. M., Mayo, N. E., Hanley, J. A., Richards, C. L., and Wood-Dauphinee, S. (2006). Psychometric evaluation of the original and Canadian French version of the activities-specific balance confidence scale among people with stroke. Arch. Phys. Med. Rehabil. 87, 1597–1604. doi: 10.1016/j.apmr.2006.08.336
Sullivan, J. E., Girardi, M., Hensley, M., Rohaus, J., Schewe, C., Whittey, C., et al. (2015). Improving arm function in chronic stroke: a pilot study of sensory amplitude electrical stimulation via glove electrode during task-specific training. Topics Stroke Rehabil. 22, 169–175. doi: 10.1179/1074935714Z.0000000007
Tinazzi, M., Zarattini, S., Valeriani, M., Romito, S., Farina, S., Moretto, G., et al. (2005). Long-lasting modulation of human motor cortex following prolonged transcutaneous electrical nerve stimulation (TENS) of forearm muscles: evidence of reciprocal inhibition and facilitation. Exp. Brain Res. 161, 457–464. doi: 10.1007/s00221-004-2091-y
Tyson, S. F., Hanley, M., Chillala, J., Selley, A., and Tallis, R. C. (2006). Balance disability after stroke. Phys. Ther. 86, 30–38. doi: 10.1093/ptj/86.1.30
Tyson, S. F., Hanley, M., Chillala, J., Selley, A. B., and Tallis, R. C. (2008). Sensory loss in hospital-admitted people with stroke: characteristics, associated factors, and relationship with function. Neurorehabil. Neural Repair. 22, 166–172. doi: 10.1177/1545968307305523
Tyson, S. F., Sadeghi-Demneh, E., and Nester, C. J (2013). The effects of transcutaneous electrical nerve stimulation on strength, proprioception, balance and mobility in people with stroke: a randomized controlled cross-over trial. Clin. Rehabil. 27, 785–791. doi: 10.1177/0269215513478227
von Elm, E., Altman, D. G., Egger, M., Pocock, S. J., Gotzsche, P. C., and Vandenbroucke, J. P. (2007). The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) Statement: guidelines for reporting observational studies. BMJ 335, 806–808. doi: 10.1136/bmj.39335.541782.AD
Winward, C. E., Halligan, P. W., and Wade, D. T. (2007). Somatosensory recovery: a longitudinal study of the first 6 months after unilateral stroke. Disabil. Rehabil. 29, 293–299. doi: 10.1080/09638280600756489
Woolley, S. M. (2001). Characteristics of gait in hemiplegia. Topics Stroke Rehabil. 7, 1–18. doi: 10.1310/JB16-V04F-JAL5-H1UV
Wu, C. W. H., van Gelderen, P., Hanakawa, T., Yaseen, Z., and Cohen, L. G. (2005). Enduring representational plasticity after somatosensory stimulation. NeuroImage 27, 872–884. doi: 10.1016/j.neuroimage.2005.05.055
Wutzkea, C. J., Mercerab, V. S., and Lewek, M. D. (2013). Influence of lower extremity sensory function on locomotor adaptation following stroke: a review. Topics Stroke Rehabil. 20, 233–240. doi: 10.1310/tsr2003-233
Yan, T., Hui-Chan, C. W., Yan, T., and Hui-Chan, C. W. Y. (2009). Transcutaneous electrical stimulation on acupuncture points improves muscle function in subjects after acute stroke: a randomized controlled trial. J. Rehabil. Med. 41, 312–316. doi: 10.2340/16501977-0325
Yates, J. S., Lai, S. M., Duncan, P. W., and Studenski, S. (2002). Falls in community-dwelling stroke survivors: an accumulated impairments model. J. Rehabil. Res. Dev. 39, 385–394. Available online at: https://pdfs.semanticscholar.org/ee95/98153ee1807571ba5cd534c338465922e00c.pdf
Keywords: stroke, rehabilitation, lower limb, electrical stimulation, gait, function
Citation: Lopez-Rosado R, Kimalat A, Bednarczyk M and Sullivan JE (2019) Sensory Amplitude Electrical Stimulation via Sock Combined With Standing and Mobility Activities Improves Walking Speed in Individuals With Chronic Stroke: A Pilot Study. Front. Neurosci. 13:337. doi: 10.3389/fnins.2019.00337
Received: 27 September 2018; Accepted: 22 March 2019;
Published: 16 April 2019.
Edited by:
Susan Hillier, University of South Australia, AustraliaReviewed by:
Sarah Meyer, Jessa Hospital, BelgiumCopyright © 2019 Lopez-Rosado, Kimalat, Bednarczyk and Sullivan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Roberto Lopez-Rosado, cm9iZXJ0by5sb3Blei1yb3NhZG9Abm9ydGh3ZXN0ZXJuLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.