
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Neurol., 28 March 2025
Sec. Multiple Sclerosis and Neuroimmunology
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1571605
 Diego Centonze1,2*†
Diego Centonze1,2*† Alessia Di Sapio3†
Alessia Di Sapio3† Vincenzo Brescia Morra4
Vincenzo Brescia Morra4 Elena Colombo5
Elena Colombo5 Matilde Inglese6,7
Matilde Inglese6,7 Damiano Paolicelli8
Damiano Paolicelli8 Marco Salvetti2,9
Marco Salvetti2,9 Roberto Furlan10,11
Roberto Furlan10,11Multiple sclerosis (MS) is a chronic central nervous system disease characterized by neurodegeneration and inflammation. Neurofilament light chain (NfL), a protein released during axonal injury, has gained recognition as a potential biomarker for monitoring MS progression and treatment response. Evidence indicates that blood NfL (bNfL) offers a minimally invasive, cost-effective tool for tracking neuroaxonal damage. Regular bNfL assessments can identify subclinical disease activity, guide treatment intensification, and support individualized care. However, bNfL level evaluation is currently not optimized in Italian clinical practice. This work examines the utility of bNfL monitoring in clinical practice, focusing on optimizing its use within specific patient profiles, especially in resource-limited settings. bNfL testing, particularly in targeted MS patient profiles, including stable patients exhibiting subclinical signs of disease activity, such as fatigue, and patients off-treatment, represents a promising adjunct for personalized disease management. Its integration into clinical practice, alongside MRI and clinical assessments, can enhance decision-making and improve care efficiency, especially in settings with limited MRI resources. Further research is needed to standardize testing protocols and establish disease-specific cutoffs.
Multiple sclerosis (MS) is a chronic inflammatory disease affecting the central nervous system (CNS) (1), characterized by neuroaxonal damage that correlates with clinical events, magnetic resonance imaging (MRI) findings, and disease prognosis (2). Neurofilament light chain (NfL), a structural protein within the neuronal cytoskeleton, mainly localized in axons but also found in neuronal cell body (3), is crucial for maintaining neuronal integrity in both the central and peripheral nervous system. Neuro-axonal injury leads to the release of NfL into cerebrospinal fluid (CSF), reflecting underlying neurodegenerative and inflammatory processes (4). This release is seen in MS (5) as well as in other conditions such as Alzheimer’s disease and amyotrophic lateral sclerosis (4). Elevated NfL levels indicate neuro-axonal damage, regardless of the primary cause (6).
Although most NfL remains within the CSF, approximately 2% is released in the blood (6), allowing blood NfL (bNfL) to be used as a minimally invasive biomarker. Technological advancements, such as single-molecule array (SiMoA) assays (7, 8) and more recent immunometric assays, have enabled the detection of NfL in serum and plasma at picogram/milliliter concentrations (9), facilitating its use in clinical and research settings (4, 5).
Retrospective cohort studies (10–15) and phase 2 and 3 clinical trials in relapsing and progressive MS (16–20) have demonstrated the promise of NfL as a biomarker. High correlations between CSF and bNfL levels (10, 13, 14) suggest that blood-based measurements of NfL can reliably reflect neuroaxonal damage, making bNfL a useful tool for monitoring disease activity (10, 11).
In patients with relapsing and progressive MS, elevated bNfL concentrations have been observed compared to healthy controls (10, 11). Levels of bNfL correlate with clinical and MRI indicators of inflammatory disease activity, including baseline T2 lesion volume and number (11, 21, 22), T1-hypointense lesion and volume (23, 24), and the presence and quantity of gadolinium-enhancing (Gd+) lesions (10, 25).
Similarly, pediatric MS patients exhibit elevated bNfL levels during their first clinical demyelinating episode (26), with higher levels correlating with MRI activity, relapses, and EDSS scores, mirroring the correlations seen in adults (27). Additionally, the initiation of effective treatment leads to a reduction in bNfL levels, as demonstrated in both clinical trials and real-world studies (6).
Currently, NfL is primarily used as a secondary outcome measure in clinical trials for MS therapies (28), and further validation is needed before it can be routinely adopted in clinical practice. NfL assays are still designated for research-oriented use in most neurodegenerative diseases.
Despite its promising role in MS management and its potential for widespread clinical adoption, the practical use of bNfL testing remains limited. Consensus documents have outlined potential clinical applications for bNfL analysis in MS, providing recommendations on its role, optimal timing, and factors influencing bNfL levels, such as age and comorbidities (29–31). Several challenges, however, must be addressed before it becomes a routine practice, including the need for standardized assay protocols, consistency in the timing of sample collection, and consideration for confounding factors like age, comorbidities, and BMI (5, 29).
Given the potential of bNfL to improve MS management, and the source-limitation of territorial clinical settings in Italy, a panel of Italian experts in the management of MS discussed specific scenarios that should be prioritized for bNfL testing in clinical practice. Experts gathered in two expert meetings that were guided by a moderator. The first meeting, held in Rome in June 2024, discussed the value of bNfL measuring, investigated the characteristics of the MS patient to be prioritized for the bNfL evaluation, and the barrier to bNfL use. During the second virtual meeting, held in July 2024, the experts agreed on the patients’ characteristics emerged in the first meeting. Their goal was to provide practical recommendations to guide decision-making and optimize patient outcomes as this biomarker is widely adopted.
High bNfL levels also have a prognostic value, predicting severe clinical outcomes and MS progression during acute disease activity, including relapses (10, 11, 32), development of Gd+ T1 lesions (17), new T2-weighted lesions (11, 16, 19), increased risk of disability worsening (10, 16, 17, 25), and increased expanded disability status scale (EDSS) scores (11, 25, 32). Additionally, bNfL levels can predict future brain and spinal cord atrophy (6, 11).
bNfL levels are linked to retinal neuroaxonal loss in relapsing–remitting MS (33). Research has highlighted the prognostic value of combining bNfL levels with other metrics, such as optical coherence tomography (OCT)-derived retinal measures (34). Compared to OCT alone, this combination provides enhanced predictive power for disease activity (34). The combination of bNfL, OCT metrics, and clinical scores, such as the Bayesian Risk Estimate for MS at Onset (BREMSO), provides both a positive and negative predictive model for early EDSS progression, demonstrating high specificity and sensitivity (35).
Although bNfL is a well-established and reliable marker of neuroinflammation—a key factor in disability accumulation and disease progression—it may have limitations in accurately reflecting the progression of disability when there is no acute disease activity (36). Nevertheless, some studies (25) have identified associations between plasma NfL levels and disability progression, cognitive decline, and brain volume loss, even in contexts when there is minimal evidence of disease activity. In addition, recent evidence showed that one elevated bNfL dosage in stable patients undergoing therapy for at least 12 months is strongly associated with an increased risk of losing NEDA-3 in the following year (37).
Despite some isolated findings indicating no significant changes in bNfL levels following treatment (38), most of clinical trials and real-world studies have demonstrated that bNfL reflects the efficacy of MS therapies (18–20), reinforcing its value as a biomarker for assessing prognosis and monitoring treatment response.
A growing body of evidence supports the predictive value of bNfL for long-term outcomes in MS (18, 24, 39). Elevated bNfL levels have been associated with future brain atrophy over 2 to 12 years (11, 12, 24, 40, 41), particularly when measured early in the disease course.
Furthermore, bNfL concentrations have been shown to be elevated several years before the clinical onset of MS (42), suggesting its potential for detecting subclinical disease activity and, thus, directly reflecting biological mechanisms of MS. This makes bNfL a more sensitive biomarker for the early detection of disease activity than MRI-based measurements of brain atrophy (18).
Several research groups have investigated the longitudinal role of blood NfL as a marker for ongoing disease activity and treatment response in prospective MS cohorts (43–45). For example, a study by Akgun et al. (44) found that bNfL levels begin to rise approximately 5 months before clinical relapse, peaking at onset and returning to baseline within 4–5 months after remission, underscoring the utility of serial bNfL measurements for proactive disease monitoring. However, while bNfL reliably predicts brain atrophy, its role in forecasting long-term EDSS progression remains debated, with mixed evidence across different patient populations. Elevated bNfL levels have been associated with an increased risk of EDSS worsening over the next 1–3 years (10, 11, 32, 46). Another study (41), with a 10-year follow-up, failed to demonstrate such a correlation despite a clear correlation with brain atrophy. Similarly, the predictive value of bNfL for conversion to secondary progressive MS is still under investigation (39, 47). Studies with long-term follow-ups show a stronger correlation in patients with more aggressive disease (6, 29, 48), where the role of confounders is possibly minimal.
Although bNfL testing is currently used primarily in research, evidence supports its potential clinical application in MS for disease monitoring and treatment evaluation. As an adjunct tool, bNfL could complement clinical and MRI monitoring in tracking MS activity and informing therapeutic decisions (49). Unlike MRI, which captures structural changes that may lag behind ongoing neuroaxonal damage, bNfL provides more immediate insights into active neurodegeneration, enabling frequent and cost-effective monitoring (31). Additionally, bNfL offers advantages in detecting neuroaxonal injury in regions that MRI may overlook, such as the spinal cord or subtle alterations in brain structure not captured by conventional imaging (31). Notably, elevated bNfL levels remain detectable for approximately 3 months after new lesions develop, whereas Gd+ lesions are typically visible on MRI only for 3–4 weeks. This extended presence of bNfL may provide a longer detection window for disease activity, enhancing monitoring beyond the sensitivity of MRI alone (17).
Integrating bNfL measurements with MRI and clinical assessments offers a more robust, multimodal approach to MS management. This combined strategy enhances the sensitivity and specificity of disease activity detection while supporting more individualized care through well-informed treatment adjustments. A recent study examined the impact of incorporating bNfL in routine practice at a tertiary MS clinic by analyzing clinicians’ decision-making through questionnaire responses (50). The study involved routine bNfL testing in various clinical scenarios, such as monitoring DMTs, assessing new symptoms, and aiding in differential diagnosis (50). Results showed that bNfL measurements influenced clinical decisions in nearly 20% of cases, with the highest impact seen in cases with new symptoms or differential diagnosis concerns (50). Clinicians reported greater decision confidence after reviewing bNfL results, especially when elevated levels were detected, leading to treatment modifications and reduced reliance on additional MRI scans. However, no impact was observed on the estimated efficacy of DMTs (50).
As efforts to develop reference values and disease-specific cutoffs for bNfL (51–53) continue, its role in guiding therapeutic decisions in MS is expected to expand significantly.
There are several advantages of using bNfL as a biomarker, including its stability across different conditions (54), high reproducibility in assays like the SiMoA (7, 8), and lower cost compared to MRI (31).
However, it is critical to recognize and account for factors that influence bNfL levels. For example, bNfL levels show an approximate 2.2% annual increase from age 18 to 70 in healthy individuals, and CSF NfL levels also rise with age (10, 55). Adjusting for these age-related changes using a Z-score calculation may provide a more accurate and sensitive measure of disease progression (30). Additionally, elevated bNfL levels have been associated with low BMI, diabetes, cardiovascular disease, renal impairment, and smoking (30, 56–58). Neurotoxic medications and recent physical trauma or intense physical exertion may also contribute to fluctuations in NfL levels (4). However, these confounding factors can be minimized by tracking bNfL levels longitudinally in the same patient.
Biotin supplements, commonly used by MS patients, were previously considered a potential interference risk for bNfL measurement using SiMoA technology. However, recent studies have shown that the SiMoA assay design effectively mitigates this concern by removing excess biotin during processing, ensuring accurate bNfL measurement (59). A manufacturer’s application note states that biotin concentrations up to 80 μM in serum, plasma, or sample diluent do not impact the performance of SiMoA bead-based assay. Since the highest biotin dose intake of 300 mg/day used in high-dose treatments for MS, corresponds to a maximum serum/plasma concentration of 4.92 μM no significant interference can occur in the assay (60). Moreover, manufacturers of in vitro diagnostic tests follow the recognized consensus standards Clinical and Laboratory Standard Institute (CLSI EP07) (61), that provides a structured approach to identifying and verifying interference in bioassays, ensuring that clinical chemistry tests are reliable and accurate.
In summary, while various extrinsic and intrinsic factors may affect bNfL concentrations, careful interpretation and consideration of these factors ensure its reliable use as a biomarker. As consensus guidelines continue to evolve, they provide clearer criteria for interpretation of bNfL levels in the context of disease monitoring and treatment response in MS (29–31).
Currently, several limitations restrict bNfL’s widespread clinical use, including cost consideration, resource allocation, and logistical feasibility. For these reasons, it is essential to establish precise guidelines to determine which patient groups and timeframes are best suited for bNfL analysis (29–31). Although an emerging consensus supports its utility across all MS patients, its use in a limited resource setting should be prioritized in cases where bNfL measurement offers the most clinically actionable insights.
In clinically stable patients who exhibit subclinical signs of disease activity, such as fatigue, sudden onset of anxiety and depression (62), or early cognitive changes without corresponding MRI findings, bNfL measurements every 4–5 months after 1 year of treatment may serve as an early indicator of disease reactivation (Table 1). This approach could help detect subtle disease progression, prompting more frequent MRI evaluations or a change in therapy. Very high bNfL levels may indicate a need for treatment escalation or closer monitoring, whereas low or normal bNfL levels would support the continuation of the current therapy (30). However, elevated bNfL levels in seemingly stable MS patients should also prompt evaluation of other potential causes, such as head trauma or comorbid conditions like polyneuropathy or cerebrovascular events (4).
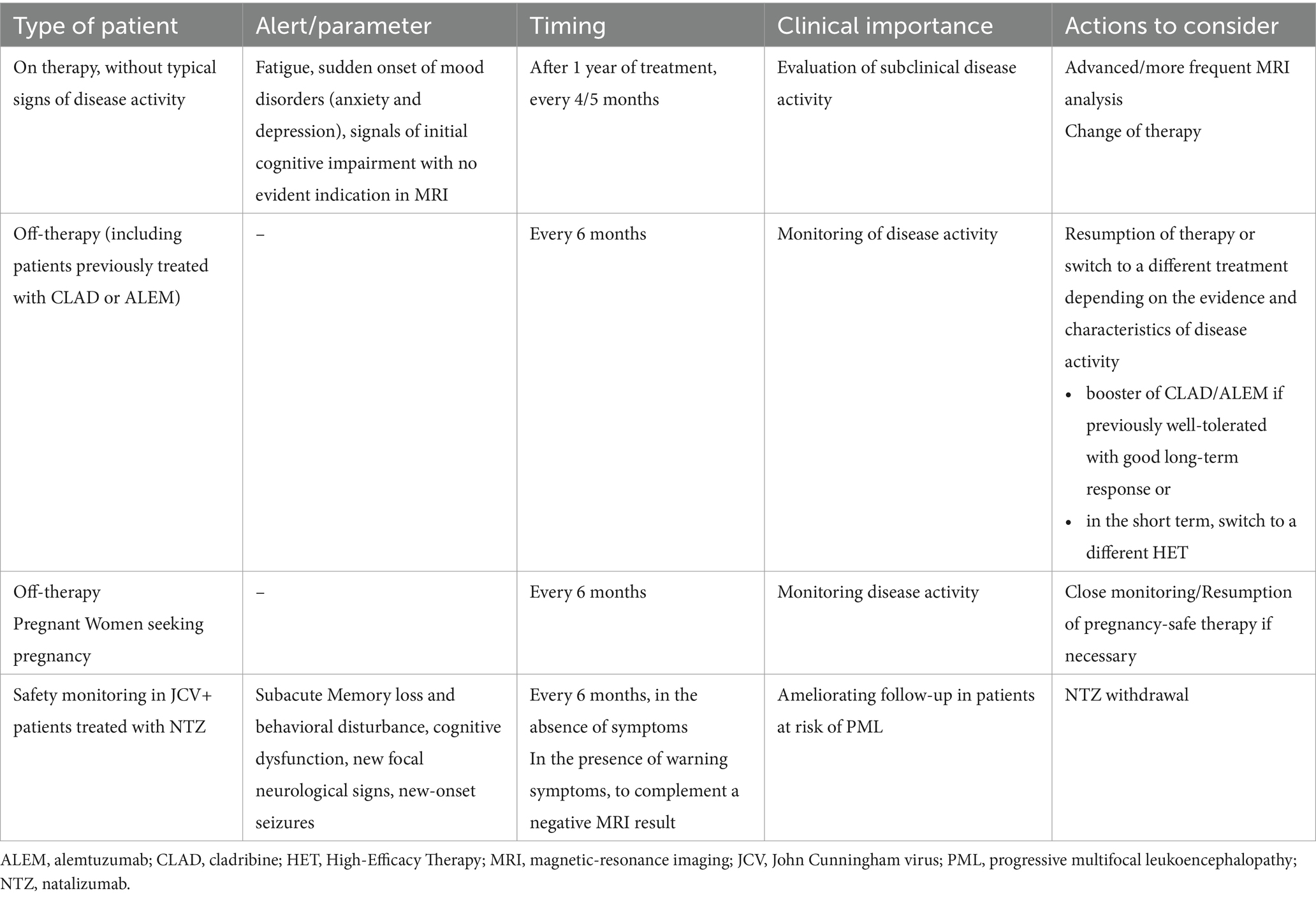
Table 1. High-priority categories of MS patients for bNfL monitoring in clinical practice settings.
The value of bNfL monitoring is especially pronounced when MRI access is limited, as bNfL levels can help optimize the timing of MRI follow-ups. In these cases, bNfL levels serve as a cost-effective adjunct, potentially minimizing unnecessary MRI scans while offering comprehensive disease surveillance.
For patients in off-treatment phases or those following immune reconstitution therapies such as cladribine or alemtuzumab, biannual bNfL monitoring is particularly relevant (Table 1). Real-world data show that cladribine sustains reduced bNfL levels, confirming its role in limiting axonal damage (20, 63, 64) and validating bNfL as a therapeutic response biomarker. Notably, a study by Manni et al. (64) found an inverse correlation between 12-month bNfL levels and the time to NEDA-3 loss, further supporting bNfL as a predictor of MS progression following cladribine treatment. Similarly, alemtuzumab significantly reduces bNfL levels post-treatment, with effects lasting up to 7 years (65). A pilot study further highlighted that bNfL level fluctuations in alemtuzumab-treated patients corresponded with relapse events or MRI lesion activity, suggesting that long-term bNfL monitoring could help assess the efficacy of immune reconstitution therapies (44). In these cases, stable bNfL levels may signal adequate disease control, whereas elevated levels could trigger MRI evaluations or the resumption of treatment. Regular bNfL monitoring in such patients could also reduce the need for frequent MRI scans, potentially lowering healthcare costs without compromising disease surveillance.
Approximately 15–30% of MS patients may experience relapses during pregnancy, and pregnancy can influence the course of MS, as reviewed in Villaverde-Gonzalez et al. (66). Relapse risk in MS decreases during pregnancy but increases significantly postpartum, especially within the first 3 months of postpartum (66). DMT discontinuation before pregnancy and extended washout periods are factors linked to an increased risk of relapse during pregnancy (66, 67). Although evidence on bNfL dynamics in MS patients during pregnancy is limited, it is known that bNfL levels naturally increase during pregnancy in healthy women. These levels also show a positive correlation with maternal age and tend to be higher in cases of preeclampsia (68). A study showed that in stable patients, bNfL levels in the third trimester were similar to those of healthy pregnant women, however, these levels increased during relapses (69). For women planning pregnancy or currently pregnant and off treatment, bNfL monitoring could provide early warning signs, facilitating proactive disease management with pregnancy-safe DMTs, if deemed necessary (Table 1).
For MS patients treated with natalizumab who test positive for John Cunningham virus (JCV) antibodies, bNfL monitoring every 6 months between MRI scans is advisable to improve follow-up for patients at risk of progressive multifocal leukoencephalopathy (PML) (70) (Table 1). Early detection of PML is associated with improved patient outcomes (71), and bNfL has been proposed as a reliable biomarker for its early identification in MS patients (72).
By focusing on these high-priority patient groups, bNfL analysis can be strategically implemented in a targeted manner to maximize its clinical impact while working within the constraints of current healthcare resources.
In an ideal setting with ample resources, more patient groups would benefit from bNfL monitoring. For newly diagnosed or treatment-naïve MS patients, an initial bNfL assessment should be conducted before starting therapy, followed by a re-baseline measurement after therapy initiation. This approach is essential for more accurate longitudinal comparisons in the future, providing a clearer view of disease progression than single-point measurements. Determining the optimal timing for the initial bNfL assessment in treatment-naïve patients, whether during an acute phase or after stabilizing from an acute event, is paramount.
A baseline measurement during a stable phase may provide a more accurate reference for evaluating the effects of subsequent DMTs. If bNfL levels are elevated at baseline, this information could influence the therapeutic approach, potentially supporting an early decision to initiate a more aggressive treatment. Ideally, bNfL levels should be reassessed 6–12 months after starting treatment to evaluate the response, monitor disease progression and guide any necessary therapy adjustments. Due to the significant inter-individual variability in bNfL levels, longitudinal monitoring within individual patients is the most effective approach. In patients starting first-line DMTs, bNfL levels generally decrease within 3–6 months, indicating a reduction in neuroinflammation. Conversely, a sustained elevation of bNfL levels despite treatment may indicate unresolved neuroinflammation and suboptimal therapeutic effects, potentially necessitating treatment adjustments. In such cases, regular monitoring every 3–6 months may provide important insights into the effectiveness of current treatment in controlling disease activity.
In cases of potential relapse mimics, where patients present with symptoms similar to a relapse but lack definitive MRI or objective evidence, bNfL testing can help distinguish between actual inflammatory activity and mimicking conditions.
When minimal evidence of disease activity is observed, either radiological (a mildly positive MRI in a prognostically non-unfavorable location) or clinical (without disability accrual), after a period of long-term disease stability, a closer follow-up is suggested. In these instances, the persistence of elevated bNfL levels may indicate the need for a therapy switch.
Indeed, bNfL levels are reported to gradually decrease following an acute relapse. However, persistently elevated bNfL levels with no noticeable decrease 3–4 months after an acute event may predict a poorer prognosis or an underlying smoldering disease, suggesting that a switch to a higher-efficacy therapy could be advisable.
Using bNfL as a biomarker reflecting disease course can help optimize treatment decisions, minimizing the risks of overtreatment and ensuring timely responses to actual disease activity.
Looking ahead, bNfL is anticipated to play an expanding role in managing diverse neurological disorders beyond MS, offering a valuable biomarker for monitoring the neurodegeneration of different etiologies. Developing biobanks to store bNfL samples could greatly enhance large-scale longitudinal studies, improving our understanding of disease mechanisms and reinforcing the biomarker’s clinical applications. However, successfully integrating bNfL into clinical practice across multiple centers will require the standardization of testing methods and platforms to ensure uniformity and reliability in results.
While bNfL provides key insights into disease activity, it is not yet a standalone diagnostic tool and cannot replace MRI for MS diagnosis or ongoing disease monitoring. Instead, bNfL should be incorporated into a multimodal approach that combines clinical evaluations and imaging findings. Future research should aim to establish disease-specific thresholds, explore the kinetics of bNfL release, and investigate potential combinations with other biomarkers to enhance its prognostic capabilities. Additionally, as highlighted in Table 1, bNfL monitoring holds promise for the early detection of PML, representing another potential application of this biomarker.
Despite its utility, bNfL lacks specificity to MS, as its levels may also rise due to various other neurological conditions or injuries (4), complicating its application in distinguishing MS activity or treatment response. Additionally, specific comorbidities associated with progressive MS may lead to elevated bNfL levels. This lack of specificity may limit bNfL’s ability to accurately capture the neurodegenerative components of progressive MS or reflect the effects of neuroprotective therapies. Possible limitations due to bNfL sensitivity compared to MRI should be considered, as the temporal association with new gadolinium-enhancing lesions needs to be further investigated (73). Understanding the dynamics of bNfLs in MS patients in different conditions will be crucial for advancing its use in personalized MS care. While bNfL is primarily useful for monitoring disease activity in relapsing MS, its applicability in progressive MS remains limited. Emerging evidence suggests that glial fibrillary acidic protein (GFAP) may serve as a complementary biomarker, as it reflects neurodegenerative processes more characteristic of progressive MS (29).
bNfL levels serve as a powerful biomarker, offering essential insights into the neurodegenerative processes associated with MS. Their stability and capacity to reflect disease activity in real-time hold potential for enhancing personalized care in MS. However, to maximize its clinical impact in resource-limited clinical settings, it is essential to prioritize patient profiles that would benefit the most from bNfL monitoring. A targeted approach to bNfL testing can optimize its benefits, reduce unnecessary interventions, and support a more personalized, cost-effective strategy for MS care.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
DC: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing, Data curation. ADS: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing, Data curation. VBM: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, Data curation. EC: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, Data curation. MI: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, Data curation. DP: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, Data curation. MS: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing, Data curation. RF: Conceptualization, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing, Data curation.
The author(s) declare that financial support was received for the research and/or publication of this article. This work reports the outcome of two round tables among a panel of 8 Italian experts in multiple sclerosis management. The round tables were supported by Novartis. The funder supported the organization of the round tables for discussion, and was not involved in the design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
Editorial assistance, which was funded by Novartis Farma SpA, was provided by Valeria Benedusi and Ahana Maitra on behalf of Health Publishing and Services Srl.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Papiri, G, D'Andreamatteo, G, Cacchio, G, Alia, S, Silvestrini, M, Paci, C, et al. Multiple sclerosis: inflammatory and Neuroglial aspects. Curr Issues Mol Biol. (2023) 45:1443–70. doi: 10.3390/cimb45020094
2. Reich, DS, Lucchinetti, CF, and Calabresi, PA. Multiple Sclerosis. N Engl J Med. (2018) 378:169–80. doi: 10.1056/NEJMra1401483
3. Yuan, A, Rao, MV, and Veeranna, NRA. Neurofilaments at a glance. J Cell Sci. (2012) 125:3257–63. doi: 10.1242/jcs.104729
4. Delaby, C, Bousiges, O, Bouvier, D, Fillee, C, Fourier, A, Mondesert, E, et al. Neurofilaments contribution in clinic: state of the art. Front Aging Neurosci. (2022) 14:1034684. doi: 10.3389/fnagi.2022.1034684
5. Khalil, M, Teunissen, CE, Lehmann, S, Otto, M, Piehl, F, Ziemssen, T, et al. Neurofilaments as biomarkers in neurological disorders - towards clinical application. Nat Rev Neurol. (2024) 20:269–87. doi: 10.1038/s41582-024-00955-x
6. Bittner, S, Oh, J, Havrdova, EK, Tintore, M, and Zipp, F. The potential of serum Neurofilament as biomarker for multiple sclerosis. Brain. (2021) 144:2954–63. doi: 10.1093/brain/awab241
7. Rissin, DM, Kan, CW, Campbell, TG, Howes, SC, Fournier, DR, Song, L, et al. Single-molecule enzyme-linked immunosorbent assay detects serum proteins at Subfemtomolar concentrations. Nat Biotechnol. (2010) 28:595–9. doi: 10.1038/nbt.1641
8. Kuhle, J, Barro, C, Hrusovsky, K, Chang, L, Jeromin, A, Bridel, C, et al. International multi-site analytical validation of the Simoa Nf-light assay in human serum samples from multiple sclerosis patients (2018). Available online at: https://www.quanterix.com/publications-posters/international-multi-site-analytical-validation-simoa-nf-light-0/ (Accessed October 26, 2024).
9. Kuhle, J, Barro, C, Andreasson, U, Derfuss, T, Lindberg, R, Sandelius, A, et al. Comparison of three analytical platforms for quantification of the Neurofilament light chain in blood samples: Elisa, Electrochemiluminescence immunoassay and Simoa. Clin Chem Lab Med. (2016) 54:1655–61. doi: 10.1515/cclm-2015-1195
10. Disanto, G, Barro, C, Benkert, P, Naegelin, Y, Schadelin, S, Giardiello, A, et al. Serum Neurofilament light: a biomarker of neuronal damage in multiple sclerosis. Ann Neurol. (2017) 81:857–70. doi: 10.1002/ana.24954
11. Barro, C, Benkert, P, Disanto, G, Tsagkas, C, Amann, M, Naegelin, Y, et al. Serum Neurofilament as a predictor of disease worsening and brain and spinal cord atrophy in multiple sclerosis. Brain. (2018) 141:2382–91. doi: 10.1093/brain/awy154
12. Canto, E, Barro, C, Zhao, C, Caillier, SJ, Michalak, Z, Bove, R, et al. Association between serum Neurofilament light chain levels and long-term disease course among patients with multiple sclerosis followed up for 12 years. JAMA Neurol. (2019) 76:1359–66. doi: 10.1001/jamaneurol.2019.2137
13. Novakova, L, Zetterberg, H, Sundstrom, P, Axelsson, M, Khademi, M, Gunnarsson, M, et al. Monitoring disease activity in multiple sclerosis using serum Neurofilament light protein. Neurology. (2017) 89:2230–7. doi: 10.1212/WNL.0000000000004683
14. Piehl, F, Kockum, I, Khademi, M, Blennow, K, Lycke, J, Zetterberg, H, et al. Plasma Neurofilament light chain levels in patients with Ms switching from injectable therapies to Fingolimod. Mult Scler. (2018) 24:1046–54. doi: 10.1177/1352458517715132
15. Bava, CI, Valentino, P, Malucchi, S, Bottero, R, Martire, S, Sapio, AD, et al. Prevalence of elevated Snfl in a real-world setting: results on 908 patients with different multiple sclerosis types and treatment conditions. Mult Scler Relat Disord. (2024) 88:105748. doi: 10.1016/j.msard.2024.105748
16. Williams, TE, Holdsworth, KP, Nicholas, JM, Eshaghi, A, Katsanouli, T, Wellington, H, et al. Assessing Neurofilaments as biomarkers of neuroprotection in progressive multiple sclerosis: from the Ms-stat randomized controlled trial. Neurol Neuroimmunol Neuroinflamm. (2022) 9:e1130. doi: 10.1212/NXI.0000000000001130
17. Bar-Or, A, Montalban, X, Hu, X, Kropshofer, H, Kukkaro, P, Coello, N, et al. Serum Neurofilament light trajectories and their relation to subclinical radiological disease activity in relapsing multiple sclerosis patients in the Aplios trial. Neurol Ther. (2023) 12:303–17. doi: 10.1007/s40120-022-00427-8
18. Ziemssen, T, Arnold, DL, Alvarez, E, Cross, AH, Willi, R, Li, B, et al. Prognostic value of serum Neurofilament light chain for disease activity and worsening in patients with relapsing multiple sclerosis: results from the phase 3 Asclepios I and II trials. Front Immunol. (2022) 13:852563. doi: 10.3389/fimmu.2022.852563
19. Bar-Or, A, Thanei, GA, Harp, C, Bernasconi, C, Bonati, U, Cross, AH, et al. Blood Neurofilament light levels predict non-relapsing progression following anti-Cd20 therapy in relapsing and primary progressive multiple sclerosis: findings from the Ocrelizumab randomised, double-blind phase 3 clinical trials. EBioMedicine. (2023) 93:104662. doi: 10.1016/j.ebiom.2023.104662
20. Seiberl, M, Feige, J, Hilpold, P, Hitzl, W, Machegger, L, Buchmann, A, et al. Serum Neurofilament light chain as biomarker for Cladribine-treated multiple sclerosis patients in a real-world setting. Int J Mol Sci. (2023) 24:4067. doi: 10.3390/ijms24044067
21. Kapoor, R, Smith, KE, Allegretta, M, Arnold, DL, Carroll, W, Comabella, M, et al. Serum Neurofilament light as a biomarker in progressive multiple sclerosis. Neurology. (2020) 95:436–44. doi: 10.1212/WNL.0000000000010346
22. Uher, T, McComb, M, Galkin, S, Srpova, B, Oechtering, J, Barro, C, et al. Neurofilament levels are associated with blood-brain barrier integrity, lymphocyte extravasation, and risk factors following the first demyelinating event in multiple sclerosis. Mult Scler. (2021) 27:220–31. doi: 10.1177/1352458520912379
23. Van Der Vuurst De Vries, RM, YYM, W, Mescheriakova, JY, van Pelt, ED, Runia, TF, Jafari, N, et al. High Neurofilament levels are associated with clinically definite multiple sclerosis in children and adults with clinically isolated syndrome. Mult Scler. (2019) 25:958–67. doi: 10.1177/1352458518775303
24. Srpova, B, Uher, T, Hrnciarova, T, Barro, C, Andelova, M, Michalak, Z, et al. Serum Neurofilament light chain reflects inflammation-driven neurodegeneration and predicts delayed brain volume loss in early stage of multiple sclerosis. Mult Scler. (2021) 27:52–60. doi: 10.1177/1352458519901272
25. Leppert, D, Kropshofer, H, Haring, DA, Dahlke, F, Patil, A, Meinert, R, et al. Blood Neurofilament light in progressive multiple sclerosis: post hoc analysis of 2 randomized controlled trials. Neurology. (2022) 98:e2120–31. doi: 10.1212/WNL.0000000000200258
26. Niculae, AS, Niculae, LE, Vacaras, C, and Vacaras, V. Serum levels of Neurofilament light chains in pediatric multiple sclerosis: a systematic review and Meta-analysis. J Neurol. (2023) 270:4753–62. doi: 10.1007/s00415-023-11841-9
27. Kuhle, J, Chitnis, T, Banwell, B, Tardieu, M, Arnold, DL, Rawlings, AM, et al. Plasma Neurofilament light chain in children with relapsing Ms receiving Teriflunomide or placebo: a post hoc analysis of the randomized Terikids trial. Mult Scler. (2023) 29:385–94. doi: 10.1177/13524585221144742
28. Schilke, ED, Remoli, G, Funelli, E, Galimberti, M, Fusco, ML, Cereda, D, et al. Current use of fluid biomarkers as outcome measures in multiple sclerosis (Ms): a review of ongoing pharmacological clinical trials. Neurol Sci. (2024) 45:1931–44. doi: 10.1007/s10072-023-07228-3
29. Freedman, MS, Gnanapavan, S, Booth, RA, Calabresi, PA, Khalil, M, Kuhle, J, et al. Guidance for use of Neurofilament light chain as a cerebrospinal fluid and blood biomarker in multiple sclerosis management. EBioMedicine. (2024) 101:104970. doi: 10.1016/j.ebiom.2024.104970
30. Consortium of Multiple Sclerosis Centers CMSC Consensus Statement on Neurofilament Biomarkers in Multiple Sclerosis. International Journal of MScare, (2021). 23:1–32.
31. Consortium of Multiple Sclerosis Centers Best Practices Guideline on the Use of Neurofilament. (2024) Available at: https://www.mscare.org/best-practices-guideline-on-the-use-of-neurofilament/ (Accessed March 14, 2025).
32. Bittner, S, Steffen, F, Uphaus, T, Muthuraman, M, Fleischer, V, Salmen, A, et al. Clinical implications of serum Neurofilament in newly diagnosed Ms patients: a longitudinal multicentre cohort study. EBioMedicine. (2020) 56:102807. doi: 10.1016/j.ebiom.2020.102807
33. Bsteh, G, Berek, K, Hegen, H, Teuchner, B, Buchmann, A, Voortman, MM, et al. Serum Neurofilament levels correlate with retinal nerve Fiber layer thinning in multiple sclerosis. Mult Scler. (2020) 26:1682–90. doi: 10.1177/1352458519882279
34. Lin, TY, Vitkova, V, Asseyer, S, Martorell Serra, I, Motamedi, S, Chien, C, et al. Increased serum Neurofilament light and thin ganglion cell-inner plexiform layer are additive risk factors for disease activity in early multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. (2021) 8:e1051. doi: 10.1212/NXI.0000000000001051
35. Tiu, VE, Popescu, BO, Enache, TC II, Cherecheanu, AP, and Panea, CA. Serum Neurofilaments and Oct metrics predict Edss-plus score progression in early relapse-remitting multiple sclerosis. Biomedicines. (2023) 11:606. doi: 10.3390/biomedicines11020606
36. Gafson, AR, Jiang, X, Shen, C, Kapoor, R, Zetterberg, H, Fox, RJ, et al. Serum Neurofilament light and multiple sclerosis progression independent of acute inflammation. JAMA Netw Open. (2022) 5:e2147588. doi: 10.1001/jamanetworkopen.2021.47588
37. Malucchi, S, Bava, CI, Valentino, P, Martire, S, Lo Re, M, Bertolotto, A, et al. In multiple sclerosis patients a single serum Neurofilament light chain (Snfl) dosage is strongly associated with 12 months outcome: data from a real-life clinical setting. J Neurol. (2024) 271:7494–501. doi: 10.1007/s00415-024-12701-w
38. Barrero Hernandez, FJ, Romero Villarrubia, A, Munoz Fernandez, C, Guillen Martinez, V, Aguilera Del Moral, A, Barrios-Lopez, JM, et al. Real-world study of serum Neurofilament light chain levels in Ocrelizumab-treated people with relapsing multiple sclerosis. J Pers Med. (2024) 14:692. doi: 10.3390/jpm14070692
39. Jakimovski, D, Zivadinov, R, Ramanthan, M, Hagemeier, J, Weinstock-Guttman, B, Tomic, D, et al. Serum Neurofilament light chain level associations with clinical and cognitive performance in multiple sclerosis: a longitudinal retrospective 5-year study. Mult Scler. (2020) 26:1670–81. doi: 10.1177/1352458519881428
40. Lie, IA, Kacar, S, Wesnes, K, Brouwer, I, Kvistad, SS, Wergeland, S, et al. Serum Neurofilament as a predictor of 10-year Grey matter atrophy and clinical disability in multiple sclerosis: a longitudinal study. J Neurol Neurosurg Psychiatry. (2022) 93:849–57. doi: 10.1136/jnnp-2021-328568
41. Chitnis, T, Gonzalez, C, Healy, BC, Saxena, S, Rosso, M, Barro, C, et al. Neurofilament light chain serum levels correlate with 10-year Mri outcomes in multiple sclerosis. Ann Clin Transl Neurol. (2018) 5:1478–91. doi: 10.1002/acn3.638
42. Bjornevik, K, Munger, KL, Cortese, M, Barro, C, Healy, BC, Niebuhr, DW, et al. Serum Neurofilament light chain levels in patients with Presymptomatic multiple sclerosis. JAMA Neurol. (2020) 77:58–64. doi: 10.1001/jamaneurol.2019.3238
43. Huss, A, Senel, M, Abdelhak, A, Mayer, B, Kassubek, J, Ludolph, AC, et al. Longitudinal serum Neurofilament levels of multiple sclerosis patients before and after treatment with first-line immunomodulatory therapies. Biomedicines. (2020) 8:312. doi: 10.3390/biomedicines8090312
44. Akgun, K, Kretschmann, N, Haase, R, Proschmann, U, Kitzler, HH, Reichmann, H, et al. Profiling individual clinical responses by high-frequency serum Neurofilament assessment in Ms. Neurol Neuroimmunol Neuroinflamm. (2019) 6:e555. doi: 10.1212/NXI.0000000000000555
45. Hyun, JW, Kim, Y, Kim, G, Kim, SH, and Kim, HJ. Longitudinal analysis of serum Neurofilament light chain: a potential therapeutic monitoring biomarker for multiple sclerosis. Mult Scler. (2020) 26:659–67. doi: 10.1177/1352458519840757
46. Sellebjerg, F, Royen, L, Soelberg Sorensen, P, Oturai, AB, and Jensen, PEH. Prognostic value of cerebrospinal fluid Neurofilament light chain and Chitinase-3-Like-1 in newly diagnosed patients with multiple sclerosis. Mult Scler. (2019) 25:1444–51. doi: 10.1177/1352458518794308
47. Manouchehrinia, A, Stridh, P, Khademi, M, Leppert, D, Barro, C, Michalak, Z, et al. Plasma Neurofilament light levels are associated with risk of disability in multiple sclerosis. Neurology. (2020) 94:e2457–67. doi: 10.1212/WNL.0000000000009571
48. Thebault, S, Abdoli, M, Fereshtehnejad, SM, Tessier, D, Tabard-Cossa, V, and Freedman, MS. Serum Neurofilament light chain predicts long term clinical outcomes in multiple sclerosis. Sci Rep. (2020) 10:10381. doi: 10.1038/s41598-020-67504-6
49. Johnsson, M, Stenberg, YT, Farman, HH, Blennow, K, Zetterberg, H, Malmestrom, C, et al. Serum Neurofilament light for detecting disease activity in individual patients in multiple sclerosis: a 48-week prospective single-center study. Mult Scler. (2024) 30:664–73. doi: 10.1177/13524585241237388
50. van Lierop, ZY, Wessels, MH, Lekranty, WM, Moraal, B, Hof, SN, Hogenboom, L, et al. Impact of serum Neurofilament light on clinical decisions in a tertiary multiple sclerosis clinic. Mult Scler. (2024) 30:1620–9. doi: 10.1177/13524585241277044
51. Solis-Tarazona, L, Raket, LL, Cabello-Murgui, J, Reddam, S, Navarro-Quevedo, S, and Gil-Perotin, S. Predictive value of individual serum Neurofilament light chain levels in short-term disease activity in relapsing multiple sclerosis. Front Neurol. (2024) 15:1354431. doi: 10.3389/fneur.2024.1354431
52. Valentino, P, Marnetto, F, Martire, S, Malucchi, S, Bava, CI, Popovic, M, et al. Serum Neurofilament light chain levels in healthy individuals: a proposal of cut-off values for use in multiple sclerosis clinical practice. Mult Scler Relat Disord. (2021) 54:103090. doi: 10.1016/j.msard.2021.103090
53. Benkert, P, Meier, S, Schaedelin, S, Manouchehrinia, A, Yaldizli, O, Maceski, A, et al. Serum Neurofilament light chain for individual prognostication of disease activity in people with multiple sclerosis: a retrospective modelling and validation study. Lancet Neurol. (2022) 21:246–57. doi: 10.1016/S1474-4422(22)00009-6
54. Altmann, P, Leutmezer, F, Zach, H, Wurm, R, Stattmann, M, Ponleitner, M, et al. Serum Neurofilament light chain withstands delayed freezing and repeated thawing. Sci Rep. (2020) 10:19982. doi: 10.1038/s41598-020-77098-8
55. Bridel, C, Van Wieringen, WN, Zetterberg, H, Tijms, BM, Teunissen, CE, Alvarez-Cermeño, JC, et al. Diagnostic value of cerebrospinal fluid Neurofilament light protein in neurology: a systematic review and Meta-analysis. JAMA Neurol. (2019) 76:1035–48. doi: 10.1001/jamaneurol.2019.1534
56. Amrein, M, Meier, S, Schafer, I, Schaedelin, S, Willemse, E, Benkert, P, et al. Serum Neurofilament light chain in functionally relevant coronary artery disease and adverse cardiovascular outcomes. Biomarkers. (2023) 28:341–51. doi: 10.1080/1354750X.2023.2172211
57. Akamine, S, Marutani, N, Kanayama, D, Gotoh, S, Maruyama, R, Yanagida, K, et al. Renal function is associated with blood Neurofilament light chain level in older adults. Sci Rep. (2020) 10:20350. doi: 10.1038/s41598-020-76990-7
58. Zhu, N, Zhu, J, Lin, S, Yu, H, and Cao, C. Correlation analysis between smoke exposure and serum Neurofilament light chain in adults: a Cross-sectional study. BMC Public Health. (2024) 24:353. doi: 10.1186/s12889-024-17811-8
59. Pape, K, Steffen, F, Zipp, F, and Bittner, S. Supplementary medication in multiple sclerosis: real-world experience and potential interference with Neurofilament light chain measurement. Mult Scler J Exp Transl Clin. (2020) 6:2055217320936318. doi: 10.1177/2055217320936318
61. McEnroe, RJ. CLSI EP07. Interference testing in clinical chemistry. 3rd ed. Wayne, PA: Clinical and Laboratory Standards Institute (2021).
62. Rossi, S, Studer, V, Motta, C, Polidoro, S, Perugini, J, Macchiarulo, G, et al. Neuroinflammation drives anxiety and depression in relapsing-remitting multiple sclerosis. Neurology. (2017) 89:1338–47. doi: 10.1212/WNL.0000000000004411
63. Paolicelli, D, Ruggieri, M, Manni, A, Gargano, CD, Carleo, G, Palazzo, C, et al. Real-life experience of the effects of Cladribine tablets on lymphocyte subsets and serum Neurofilament light chain levels in relapsing multiple sclerosis patients. Brain Sci. (2022) 12:1595. doi: 10.3390/brainsci12121595
64. Manni, A, Oggiano, F, Palazzo, C, Panetta, V, Gargano, CD, Mangialardi, V, et al. Clinical and biological predictors of Cladribine effectiveness in multiple sclerosis: a real-world, single Centre study considering a two-year interval from Year-2 dosing. J Neurol Sci. (2024) 462:123070. doi: 10.1016/j.jns.2024.123070
65. Kuhle, J, Daizadeh, N, Benkert, P, Maceski, A, Barro, C, Michalak, Z, et al. Sustained reduction of serum Neurofilament light chain over 7 years by Alemtuzumab in early relapsing-remitting Ms. Mult Scler. (2022) 28:573–82. doi: 10.1177/13524585211032348
66. Villaverde-Gonzalez, R. Updated perspectives on the challenges of managing multiple sclerosis during pregnancy. Degener Neurol Neuromuscul Dis. (2022) 12:1–21. doi: 10.2147/DNND.S203406
67. Alroughani, R, Alowayesh, MS, Ahmed, SF, Behbehani, R, and Al-Hashel, J. Relapse occurrence in women with multiple sclerosis during pregnancy in the new treatment era. Neurology. (2018) 90:e840–6. doi: 10.1212/WNL.0000000000005065
68. Evers, KS, Atkinson, A, Barro, C, Fisch, U, Pfister, M, Huhn, EA, et al. Neurofilament as neuronal injury blood marker in preeclampsia. Hypertension. (2018) 71:1178–84. doi: 10.1161/HYPERTENSIONAHA.117.10314
69. Cuello, JP, Martinez Gines, ML, Kuhle, J, Garcia Dominguez, JM, Lozano Ros, A, Romero Delgado, F, et al. Neurofilament light chain levels in pregnant multiple sclerosis patients: a prospective cohort study. Eur J Neurol. (2019) 26:1200–4. doi: 10.1111/ene.13965
70. Williamson, EML, and Berger, JR. Diagnosis and treatment of progressive multifocal leukoencephalopathy associated with multiple sclerosis therapies. Neurotherapeutics. (2017) 14:961–73. doi: 10.1007/s13311-017-0570-7
71. Vermersch, P, Kappos, L, Gold, R, Foley, JF, Olsson, T, Cadavid, D, et al. Clinical outcomes of Natalizumab-associated progressive multifocal leukoencephalopathy. Neurology. (2011) 76:1697–704. doi: 10.1212/WNL.0b013e31821a446b
72. Valentino, P, Malucchi, S, Bava, CI, Martire, S, Capobianco, M, Malentacchi, M, et al. Serum Neurofilaments are a reliable biomarker to early detect Pml in multiple sclerosis patients. Mult Scler Relat Disord. (2023) 77:104893. doi: 10.1016/j.msard.2023.104893
Keywords: neurofilament light chain, blood NfL, multiple sclerosis, MS biomarker, clinical practice
Citation: Centonze D, Di Sapio A, Brescia Morra V, Colombo E, Inglese M, Paolicelli D, Salvetti M and Furlan R (2025) Steps toward the implementation of neurofilaments in multiple sclerosis: patient profiles to be prioritized in clinical practice. Front. Neurol. 16:1571605. doi: 10.3389/fneur.2025.1571605
Edited by:
Moussa Antoine Chalah, GHU Paris Psychiatrie et Neurosciences, FranceReviewed by:
Arejas Uzgiris, Siemens Healthcare Laboratory, LLC, United StatesCopyright © 2025 Centonze, Di Sapio, Brescia Morra, Colombo, Inglese, Paolicelli, Salvetti and Furlan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diego Centonze, Y2VudG9uemVAdW5pcm9tYTIuaXQ=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.