 Valeria Pingue1,2*‡
Valeria Pingue1,2*‡ Irene Bossert3Daniela D’Ambrosio4
Irene Bossert3Daniela D’Ambrosio4 Antonio Nardone1,2Giuseppe Trifirò3
Antonio Nardone1,2Giuseppe Trifirò3 Nicola Canessa5,6†Diego Franciotta7†
Nicola Canessa5,6†Diego Franciotta7†- 1Department of Clinical-Surgical, Diagnostic and Pediatric Sciences, University of Pavia, Pavia, Italy
- 2Neurorehabilitation and Spinal Units of Pavia Institute, Istituti Clinici Scientifici Maugeri IRCCS, Pavia, Italy
- 3Nuclear Medicine Unit, Istituti Clinici Scientifici Maugeri IRCCS, Pavia, Italy
- 4Medical Physics Unit, Istituti Clinici ScientificiMaugeri SpA SB IRCCS, Pavia, Italy
- 5IUSS Cognitive Neuroscience (ICON) Center, Scuola Universitaria Superiore IUSS, Pavia, Italy
- 6Istituti Clinici Scientifici Maugeri IRCCS, Cognitive Neuroscience Laboratory of Pavia Institute, Pavia, Italy
- 7UOM, Laboratory of Clinical Pathology, Department of Laboratories, APSS Santa Chiara Hospital, Trento, Italy
Background: Measuring 18F-FDG PET-detected brain glucose uptake provides reliable information on metabolic tissue abnormalities, cells dysfunction, and neurovascular changes after traumatic brain injury (TBI).
Objectives: We aimed to study the relationship between post-traumatic brain glucose metabolism and functional outcomes in the so far unexplored field of longitudinally 18F-FDG PET-monitored patients undergoing rehabilitation after moderate-to-severe TBI.
Methods: Fourteen patients consecutively admitted to our unit in the post-acute phase after TBI underwent 18F-FDG-PET scans performed before and 6 months after inpatient rehabilitation program. The Glasgow Coma Scale (GCS) for neurological status, and the Functional Independence Measure (FIM) plus the Glasgow Outcome Scale-Extended (GOSE) scales for the rehabilitation outcome, were applied on admission and discharge. Voxel-wise analyses were performed, with the Statistical Parametric Mapping (SPM12) software, to investigate pre- vs. post-rehabilitation changes of brain metabolism, and their relationships with clinical indices.
Results: In the whole sample, 18F-FDG uptake significantly increased in the following five regions that were hypometabolic before rehabilitation: inferior frontal gyrus bilaterally, alongside right precentral gyrus, inferior parietal lobule, and cerebellum. However, only for the right precentral gyrus the median voxel peak-value at baseline resulted a significant predictor of both cognitive (FIM cognitive subscale, p = 0.012), and functional (GOS-E, p = 0.02; post- vs. pre-treatment GOS-E difference, p = 0.009) improvements. ROC curve analysis showed that a peak voxel-value of 1.7998 was the optimal cut-off for favorable rehabilitation outcome. Unfavorable functional outcomes were predicted by increased 18F-FDG uptake in the inferior frontal gyrus (GOS-E, p = 0.032) and precentral gyrus (FIM cognitive subscale, p = 0.017; GOS-E, p = 0.015).
Conclusion: This proof-of-principle study enlightens the metabolic changes occurring in moderate-to-severe TBI course. Notably, such changes preferentially involve definite frontal brain areas regardless of TBI localization and entity. These findings pave the way for further studies with translational purposes.
Introduction
Traumatic brain injury (TBI) is defined as an alteration of the brain function leading to neurological, behavioral, and cognitive impairment as a result of biomechanical insults (1). With an estimated annual incidence rate between 134 and 618 per 100,000 persons (2), TBI is the most common cause of neurological disorders (3), and of death and disability in children and young adults worldwide (4, 5).
Brain damage after TBI can follow a combination of primary mechanical and delayed secondary injury (6). Concussive impacts immediately produce abnormal ionic fluxes that result in imbalanced ionic concentrations in the brain tissue, along with an indiscriminate release of excitatory neurotransmitters (7). These acute abnormalities are followed by hypometabolic states and abnormal neuronal functioning (due to axonal and mitochondrial damage), decreased cerebral blood flow (CBF) (7), and blood–brain barrier (BBB) dysfunction (8). CBF reduction leaves glycolysis as the main pathway to satisfy metabolic requirements during TBI acute and post-acute phases (7). Two-deoxy-2-(18F) fluoro-D-glucose (18F-FDG) is a radiotracer developed for the study of glucose metabolism and, specifically, the rate of cellular glycolysis (9). To date, widespread and consistent evidence has confirmed the reliability of 18F-FDG PET in assessing brain metabolic alterations due to both pathophysiological cerebral tissue and neurovascular changes after TBI (10–12).
Indeed, 18F-FDG PET studies on this topic have demonstrated that both the extent of metabolic decrease, and length of metabolic recovery of hypometabolism are related to TBI severity (10–14). In some cases, the hypometabolism in specific brain regions has been correlated with cognitive and behavioral dysfunction (10, 13, 15). A recent study on patients with cognitive impairment after TBI, reported decreased metabolic activity in the prefrontal cortex, and increased 18F-FDG uptake in the limbic system, which were associated with chronic symptoms of depression (15). However, due to heterogeneous clinical presentation of TBI, no well-defined metabolic patterns capable to predict TBI outcome have been identified so far (16). Moreover, in addition to characterizing hypometabolic patterns, there is the need to establish whether 18FDG PET can track changes in glucose metabolism indicative of adaptive, or maladaptive reshape of brain damage (17). This could help clinicians to predict the evolution of the disease and, in turn, middle-/long-term complications.
Based on the hypothesis that the topography and temporal evolution of metabolic changes of distinctive brain areas could help define prognosis and predict rehabilitation outcome in TBI, we performed a prospective, longitudinal study on TBI patients who underwent brain 18F-FDG PET scans and multiple functional scale evaluations before and after a standardized rehabilitation program.
Materials and methods
Study design and population
In this single-center prospective study, we included 14 patients (mean age, 44.3 ± 14.8; male/female ratio, 2.5:1.0) with moderate-to-severe TBI, consecutively admitted to the Neurorehabilitation Unit of the ICS Maugeri Institute of Pavia (IRCCS) between May 21, 2021, and April 23, 2022. The inclusion criteria were: (1) age ≥ 18 years; (2) admission for a rehabilitation-based TBI treatment program within 2 months after TBI; (3) moderate [Glasgow Coma Scale (GCS) score, 9–12] to severe (GCS score, 3–8) TBI on admission. We excluded patients with pre-existing neurological diseases, age ≥ 65 years, unstable neurological, or non-neurological clinical conditions (e.g., behavioral disorders, uncontrolled status epilepticus, or sepsis), presence of penetrating TBI, or inability to complete rehabilitation treatment (e.g., death during hospitalization) (see Figure 1).
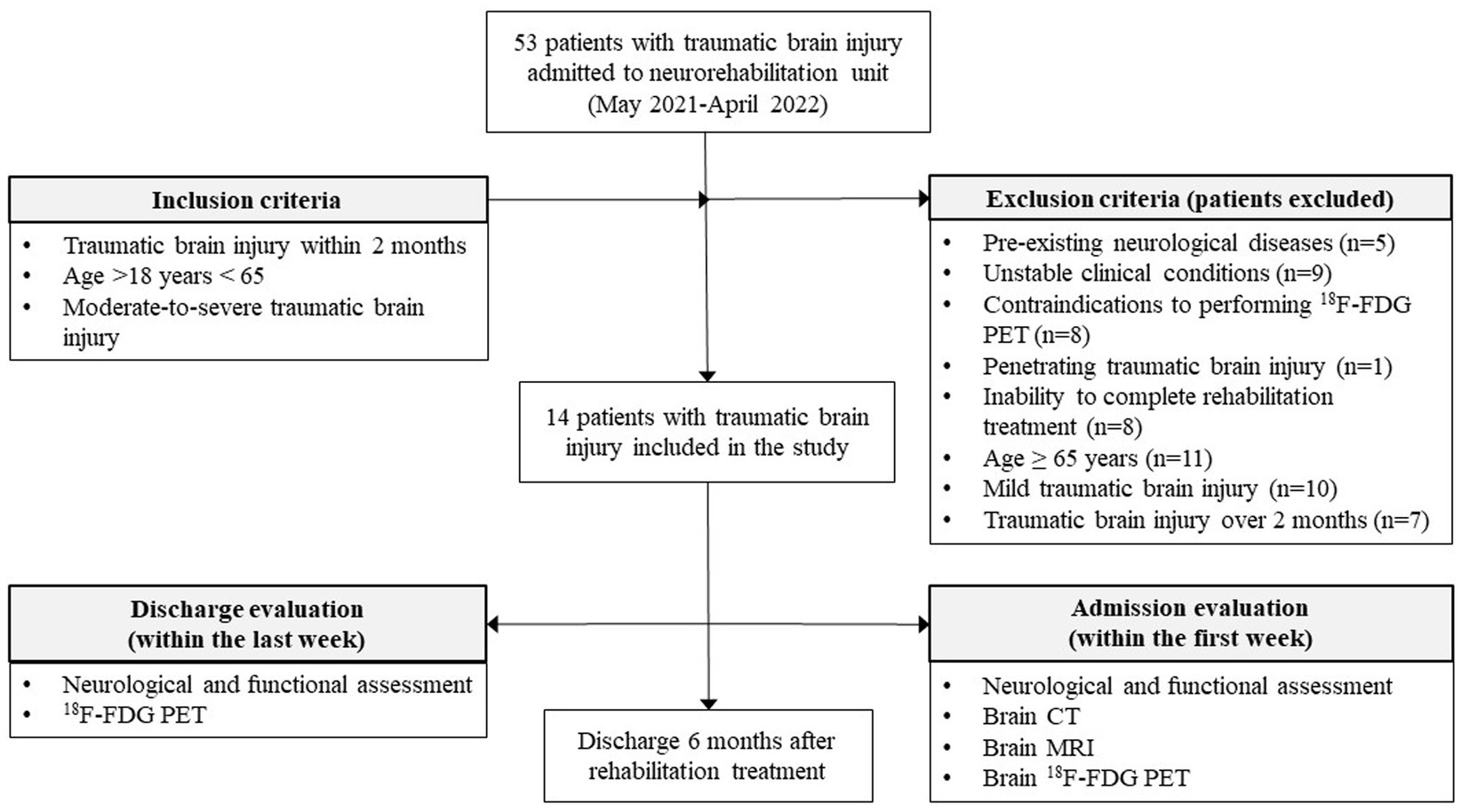
Figure 1. Algorithm of the study design.
Following the acute event and post-acute hospitalization, all patients underwent a 6-month standard neurorehabilitation program, consisting of treatment cycles performed 6 days per week. These treatments included nursing assistance, physiotherapy, occupational therapy, speech therapy, cognitive training, nutrition assistance, as well as neuropsychological and social support.
The study design complied with the ethical guidelines of the Declaration of Helsinki, and was approved by the local Ethics Committee of ICS Maugeri (#2532 CE/2021). All participants, or their authorized representatives, signed a written informed consent.
Variables and measurements
We collected the following variables: sex, age at occurrence of injury, neurological and functional evaluation, as well as injury characteristics on admission, and, particularly, the presence of focal damage (e.g., subdural hematoma, epidural hematoma, cerebral contusion) on brain CT, and/or of diffuse axonal injury on brain MRI, with the associated neurosurgical procedures (craniotomy or craniectomy). All patients underwent clinical and instrumental examinations within 1 week of admission to the Unit. 18F-FDG PET acquisitions were performed at baseline (1 week after admission), and within 1 week of discharge, respectively. GCS is a standardized system for evaluating the degree of neurological impairment and level of consciousness in all kinds of brain injury, which is classified as severe (3-to-8 scores), moderate (9-to-12), or mild (13-to-15) (18). Functional and global outcomes were evaluated, across baseline and discharge time points, by comparing pre- and post-scores of two scales, namely the Functional Independence Measure (FIM), which measures disability by tracking progress in functional status (19), and the Glasgow Outcome Scale-Extended (GOS-E), which evaluates the global outcome in TBI patients (20). FIM scores are calculated through 13 motor (FIM-m) and 5 cognitive (FIM-c) items in terms of burden of care. Each item is graded on a 1-to-7 scale, based on the level of independence (1 = total assistance required, 7 = complete independence). GOS-E scores can be dichotomized as favorable (scores, 4–8), or unfavorable (scores, 1–3) outcome in relation with patients’ dependence on others and on community reintegration (21). These scales are routinely used in clinical practice to evaluate rehabilitation outcomes.
18F-FDG PET image acquisition and reconstruction
All patients underwent pre- and post-rehabilitation 18F-FDG PET scan acquisitions (GE Discovery 690 PET), in accordance with the guidelines of the European Association of Nuclear Medicine (22). We collected static emission images 45-min after injecting 2, 5 MBq/Kg of 18F-FDG in fasting patients. This post-injection time interval enables an equal distribution of the tracer across the entire brain, with negligible blood flow-dependent differences, and an optimal signal-to-noise ratio (23). Scan acquisition lasted 15 min. Uniform reconstruction protocols were applied. In particular, we used both ordered subset-expectation maximization algorithms and CT attenuation-based correction procedures. A quality control process was performed to check for major artefacts in raw images, including defective image uniformity and orientation, or attenuation correction due to mismatches between CT and PET images.
18F-FDG PET image pre-processing and correlated statistical analysis
We used the Statistical Parametrical Mapping (SPM12) software,1 as implemented in MATLAB (Mathworks Inc., Sherborn, MA, United States), to perform a standard pre-processing of PET scans. Each image was first normalized to a standardized 18F-FDG PET template registered to the Montreal Neurological Institute standard space (24), using the default SPM12 bounding-box, resampled at an isotropic voxel size of 2 mm, and spatially smoothed with an 8 mm isotropic 3D Gaussian FWHM kernel. The 18F-FDG PET template has been reported to ensure high normalization accuracy, and to reduce noise-related random effects (24). To account for the between-subject 18F-FDG uptake variability (25), each image was proportionally scaled to its global mean (26). This approach enables higher signal-to-noise ratio, in comparison with the other available scaling methods (e.g., cerebellar reference area) (27).
We used paired-sample t-testto investigate longitudinal changes by comparing brain metabolism across admission and discharge time points in the whole sample. We reported as statistically significant only the voxels surviving a statistical threshold of p < 0.05, which was corrected for multiple comparisons based on cluster extent using topological false discovery rate, with p < 0.005 at the voxel level. Toolbox rex2 was used to extract, from the resulting clusters, the mean 18F-FDG metabolism levels of each patient’s pre- and post-treatment statistical maps, for subsequent correlation analysis matched with clinical measures.
Statistical analysis
The reported values were expressed as median and interquartile range (IQR), or absolute frequency and percentage, measured before (T0) and after (T1) the rehabilitation program, and calculated as absolute variations over baseline values (Δ = T1−T0). Data were tested for normality of distribution via Shapiro–Wilk test, and log-transformed when needed to correct for skewness. Comparisons of neurological and functional measures across admission and discharge were performed through Wilcoxon signed-rank test. We used Spearman’s correlation index to identify relationships between strength of metabolism in the brain regions showing significant pre- vs. post-changes, and rehabilitation outcomes.
Analysis through receiver operating characteristic (ROC) curves, and area under the curve (AUC), was performed to assess the accuracy of 18F-FDG PET uptake values in the right precentral gyrus for distinguishing between patients with favorable (GOS-E scores 4–8) vs. unfavorable (GOSE scores 1–3) functional outcome (21).
Finally, a multiple linear regression analysis was carried out to test the potential predictive role of 18F-FDG uptake values, as measured in the brain regions showing significant pre- vs. post-changes possibly associated with functional outcome. The multiple model included a combination of independent variables, including age, sex, severity of TBI, laterality of contusion. Linearity and univariate analyses between dependent and independent variables were checked. Statistical analyses were performed using IBM SPSS Statistics version 21 (Somers, NY, United States). Threshold for statistical significance was set at p < 0.05.
Results
Table 1 summarizes the demographic and clinical features of the 14 enrolled patients.
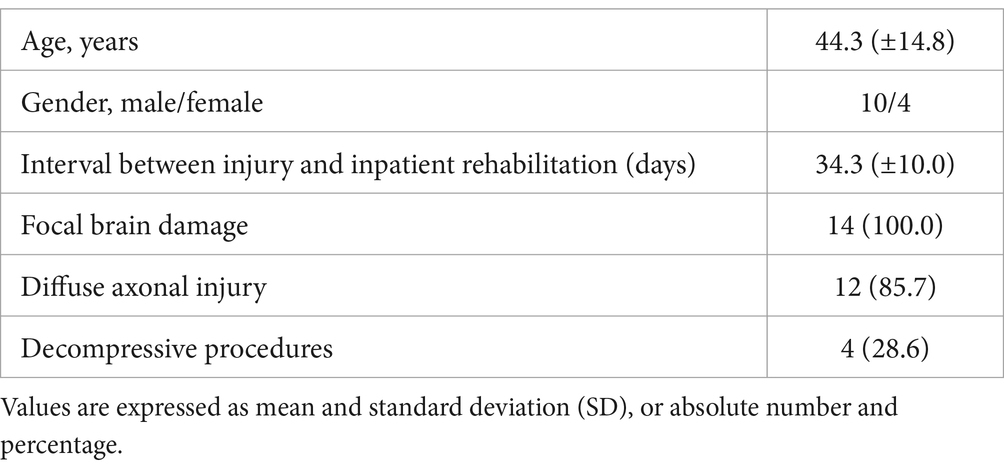
Table 1. Clinical-demographic features of the 14 patients with traumatic brain injury.
Structural focal damage, detected in all patients, mainly involved frontal (14 patients), and temporal lobes (10 patients), without a significant hemispheric prevalence (p = 0.788). Twelve patients displayed both focal and diffuse lesions on brain CT and MRI.
All the enrolled patients completed the intensive rehabilitation program, and achieved significant neurological and functional improvement (Table 2).

Table 2. Neurological and functional assessment of patients with traumatic brain injury on admission and on discharge from rehabilitation unit.
Whole-brain comparisons of pre- vs. post-rehabilitation time points highlighted five hypometabolic clusters in which 18F-FDG uptake significantly increased on discharge, namely, the inferior frontal gyrus in both the hemispheres, alongside the precentral gyrus, inferior parietal lobule and cerebellum in the right hemisphere (Table 3; Figure 2). We considered these clusters as “Regions-of-Interest” (ROI) for subsequent correlation analysis between pre- vs. post-treatment metabolic and behavioral changes.
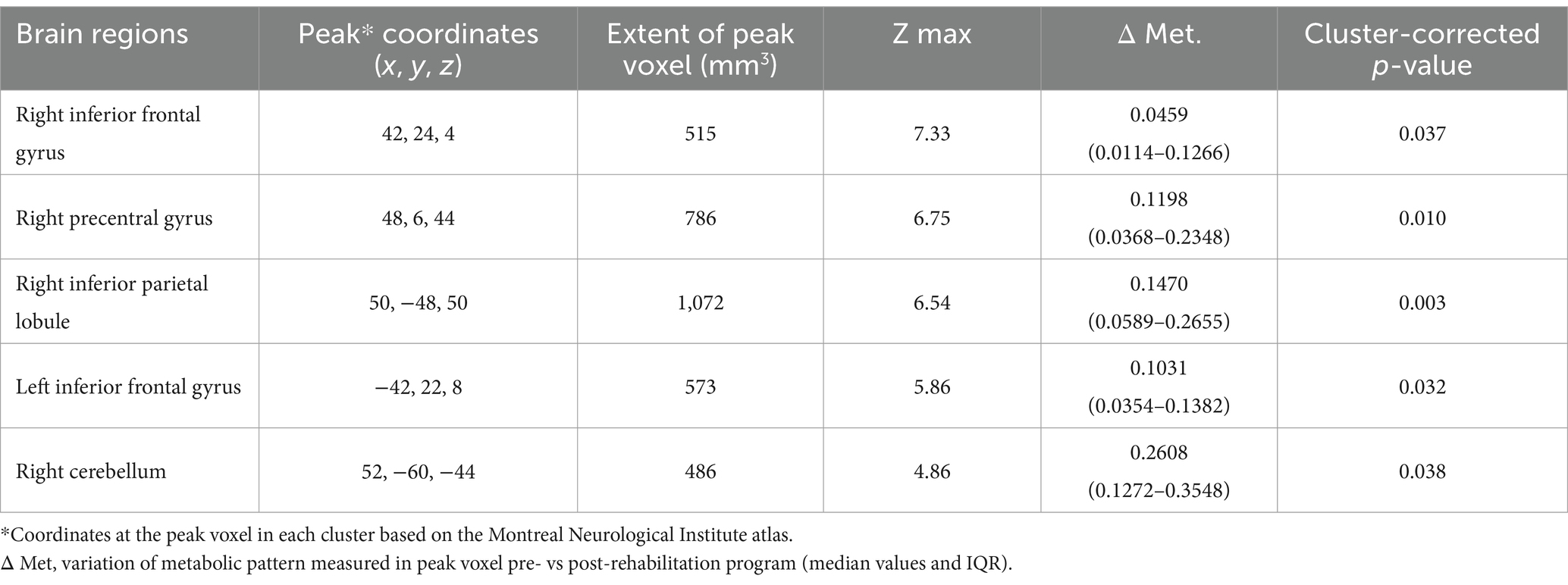
Table 3. Brain regions with 18F-FDG PET-assessed increase of glucose metabolism in patients with traumatic brain injury.
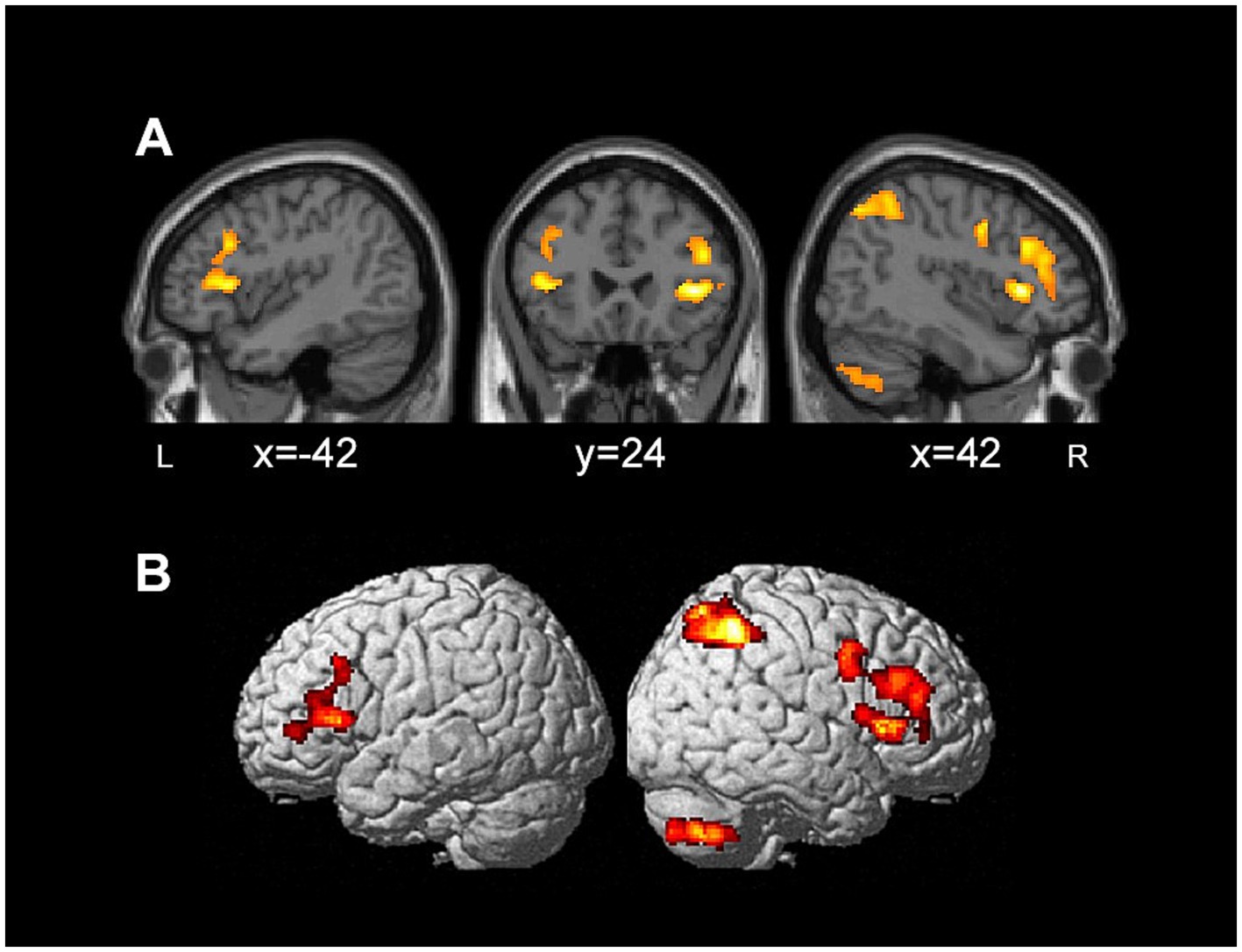
Figure 2. Brain regions with increased 18F-FDG PET glucose metabolism in patients with traumatic brain injury after rehabilitation, displayed on sagittal and coronal sections (A), as well as 3D renders (B).
We therefore hypothesized a possible relationship between the increase of glucose consumption in these areas, and the improvement in rehabilitation outcome, as measured with the functional scales. Through a cross-sectional analysis, we first correlated the pre-rehabilitation 18F-FDG uptake values of the five ROI with the functional outcome of TBI patients on discharge. Only the change in glucose uptake within the right precentral gyrus showed a significant positive correlation with better functional recovery on discharge, as measured with the FIM cognitive subscale (rho = 0.65, p = 0.012), and the GOS-E scores (rho = 0.60, p = 0.021) measured at baseline. Post- vs. pre-treatment difference was also significant for the GOS-E (rho = 0.66, p = 0.009) (Figure 3).
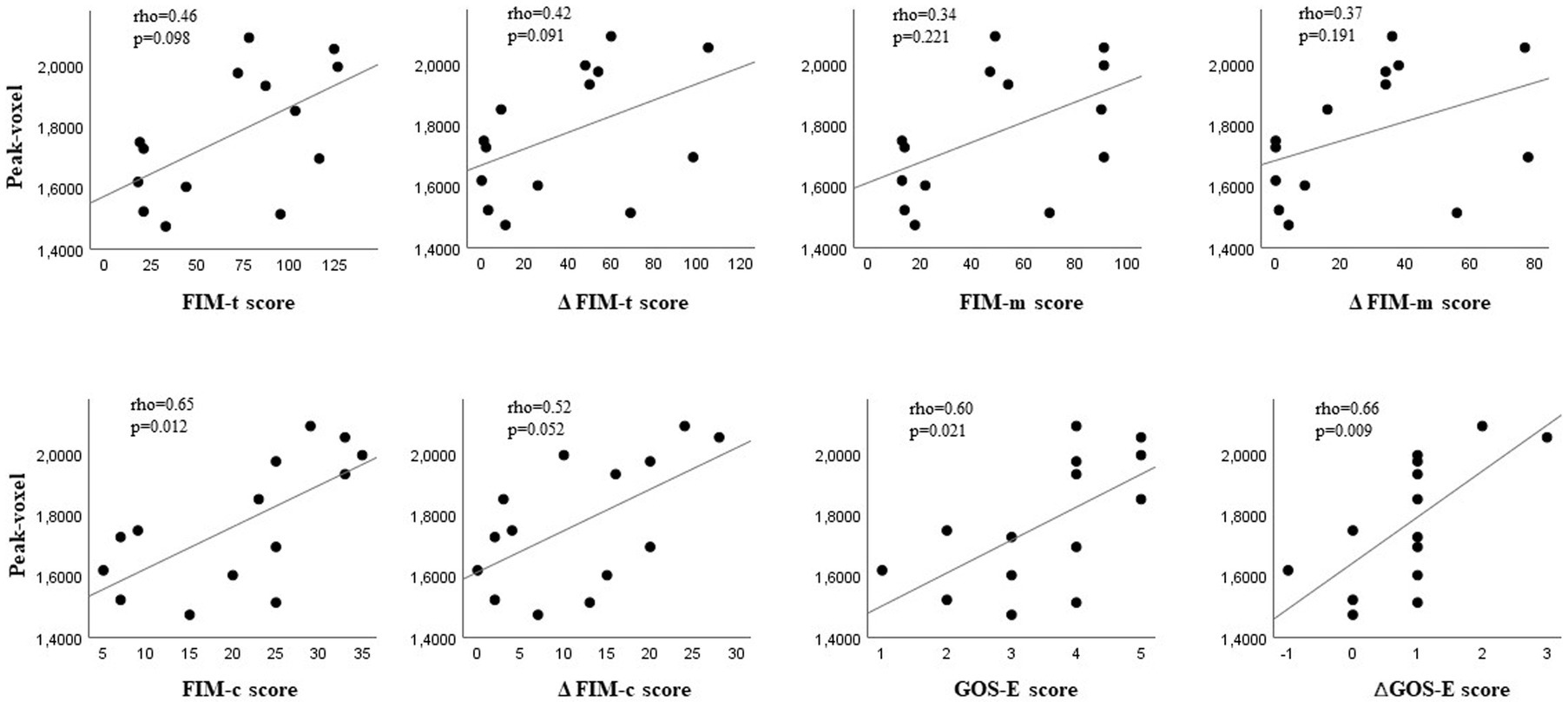
Figure 3. Basal glucose metabolism in the right precentral gyrus and functional outcome in patients with traumatic brain injury undergoing rehabilitation. Correlations between basal brain 18F-FDG PET-detected glucose uptake values in the right precentral gyrus and functional outcome on discharge, calculated as total scores and as post- vs. pre-treatment score differences on the following scales: Functional Independence Measure (FIM), FIM motor subscale (FIM-m), FIM cognitive subscale (FIM-c), and Glasgow Outcome Scale-Extended (GOS-E).
We further checked the cross-sectional analysis for potential confounding variables. The linear regression model quantified whether, and to what extent, baseline 18F-FDG uptake in the right precentral gyrus predicted functional outcome (Table 4).
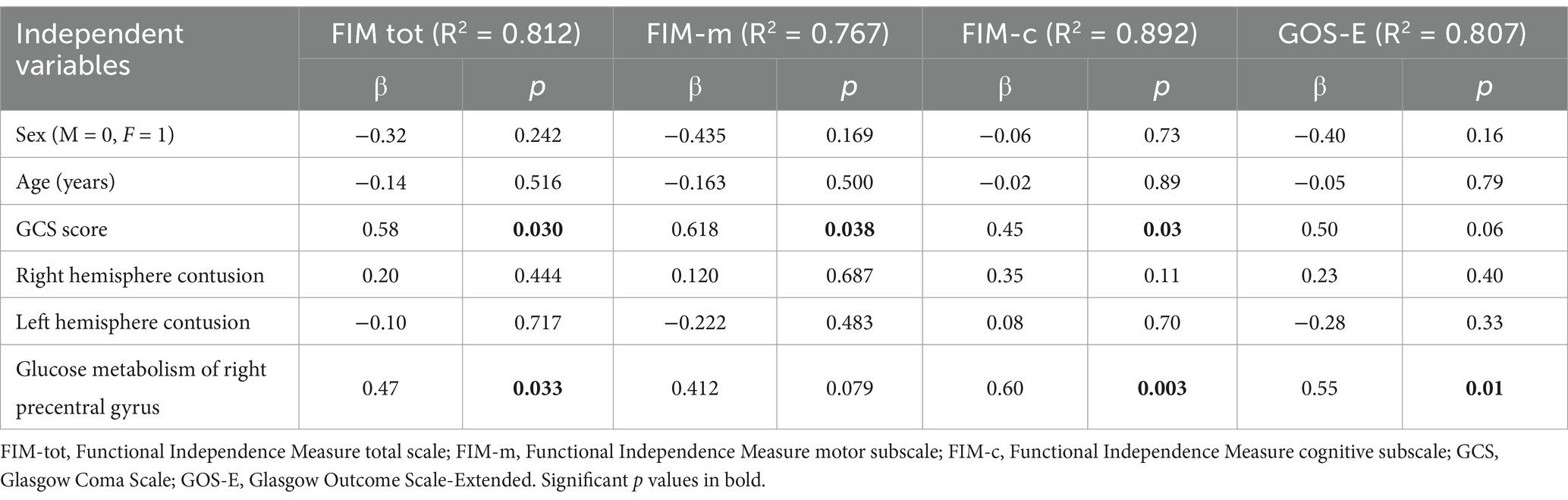
Table 4. Multiple linear regression analysis of clinical-demographic and 18F-FDG PET scan variables on admission as predictors of rehabilitation outcome.
18F-FDG uptake in the right precentral gyrus before the rehabilitation program emerged as the strongest independent predictor of the distinct facets of recovery on discharge, measured with FIM total scale (β = 0.474, p = 0.033), FIM cognitive subscale (β = 0.606, p = 0.003), and GOS-E (β = 0.556, p = 0.018). As expected, GCS measured brain damage severity at T0 emerged as the main predictor of functional outcome, independently from the other variables included in the regression model. Univariate analyses confirmed that the variables reported in Table 4 were independently related to outcome.
ROC curve analysis showed that a peak voxel value of 1.799 in the right precentral gyrus identified patients with favorable outcome assessed with GOS-E on discharge, with a sensitivity of 75%, and a specificity of 100% (AUC = 0.854, CI 95% 0.640–0.1000, p = 0.028) (Supplementary Figure S1).
Finally, we searched for a relationship between metabolic changes (post- vs. pre-treatment increase of glucose metabolism) in the five ROI, and functional outcome at discharge. The increase of 18F-FDG uptake in the right inferior frontal gyrus and right precentral gyrus was significantly associated with worse functional outcome scores on discharge (Supplementary Table S1). Namely, the post- vs. pre-treatment variations of glucose metabolism in the right precentral gyrus were significantly correlated with poor outcome, as measured with the FIM cognitive subscale (rho = −0.56, p = 0.017), and GOS-E score (rho = −0.63, p = 0.015). Post- vs. pre-treatment difference was also significant on the GOS-E (rho = −0.61, p = 0.019). Increased 18F-FDG uptake in the right inferior frontal gyrus was associated with worse scores on the GOS-E (rho = −0.57, p = 0.032), as well as its post- vs. pre-treatment difference (rho = −0.53, p = 0.04) (Figure 4).
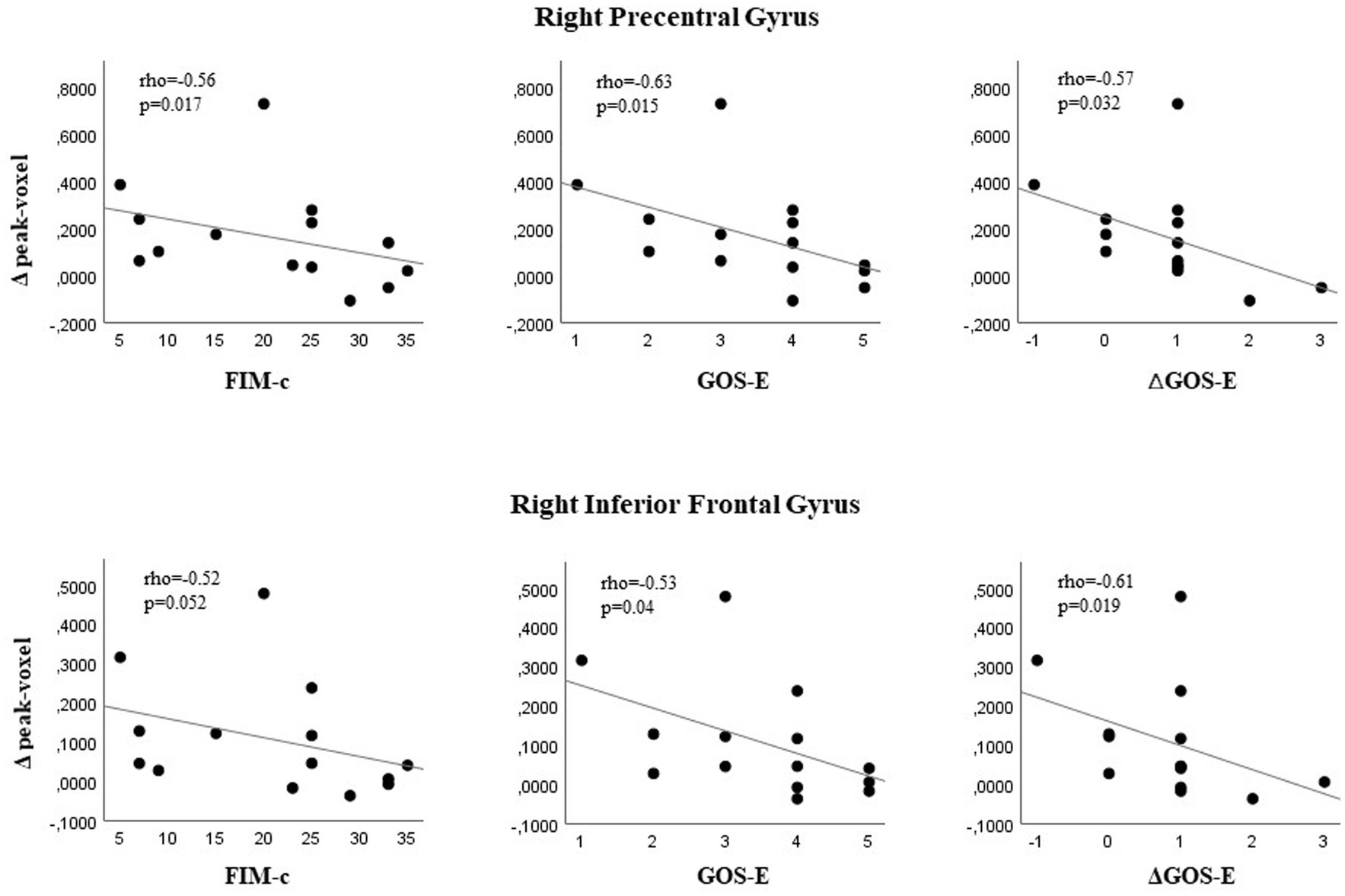
Figure 4. Glucose metabolic changes in the right precentral/inferior frontal gyrus and functional outcome in patients with traumatic brain injury undergoing rehabilitation. Correlations between pre- vs. post-treatment brain 18F-FDG PET-detected glucose uptake values in the right precentral/inferior frontal gyrus and functional outcome on discharge, calculated as scores, total scores and as post- vs. pre-treatment score differences on Functional Independence Measure cognitive subscale (FIM-c), and Glasgow Outcome Scale-Extended (GOS-E).
Discussion
In this longitudinal study we used 18F-FDG PET, before and after intensive inpatient rehabilitation in the post-acute phase of moderate-to-severe TBI, to examine the relationship between variations in brain glucose metabolism and functional outcome. Three main findings of our study are notable. First, voxel-wise analysis highlighted a significant improvement of 18-FDG uptake after the rehabilitation program in only five brain regions that were hypometabolic at the baseline. Second, among these areas, only in the right precentral gyrus the higher baseline levels of 18F-FDG uptake were associated with functional recovery in terms of disability. Third, surprisingly, glucose metabolism on discharge increased in the right inferior frontal gyrus and in precentral gyrus in patients with worse outcome scores on the FIM cognitive subscale and the GOS-E scale, among all the included patients, who showed post-rehabilitation functional improvement.
This unexpected finding suggests that an increase of glucose consumption in specific brain areas might entail different prognostic evaluations, namely, prediction of favorable outcome when detected before rehabilitation, or a less degree of functional improvement when detected 6 months later. This could be possibly explained by distinct processes equally sustained by increase in glucose consumption. Indeed, it is likely that, following a traumatic injury, the brain enters a sub-acute phase of enhanced plasticity, requiring energy supply that might ultimately foster recovery (28, 29). However, the brain circuitry can be reshaped in either adaptive, or maladaptive ways (28). In particular, persistent and low-grade neuroinflammation with relatively high tissue metabolic demands can interfere with the processes promoting recovery, thus facilitating neurodegeneration, and sustaining functional and cognitive deficits (30). Glucose hypometabolism, as measured with 18F-FDG PET, has been also correlated with chronic sequelae in TBI, typically involving cognitive and memory domains (8, 13, 15, 31). More recently, post-concussion chronic cognitive symptoms have been associated with decreased glucose consumption in the prefrontal cortex (15). The present results provide the first evidence that changes in glucose metabolism in frontal and pre-frontal gyrus could predict functional outcome in the post-acute phase of TBI.
In the attempt of quantifying the degree of hypometabolism for translational purposes, we showed that 18F-FDG PET voxel values above a given threshold (i.e., 1.799), detected on admission and before the rehabilitation program in the right precentral gyrus, might represent an early prognostic biomarker of good functional and rehabilitation outcome, independently from age, side of contusion, and severity of brain injury.
The prefrontal cortex plays a key role in processes like planning of voluntary movements, particularly in concert with selective structures of the cortical motor network, such as the rostral supplementary motor and lateral premotor areas (32, 33). Moreover, recent studies have highlighted its key role in the attention network, through the top-down cognitive control of sensory processing, and in goal-directed behavior (34). Therefore, the extent of structural and functional alterations in these prefrontal areas could possibly predict cognitive impairment after TBI (35, 36), but, in accordance with our data, may also have a role in functional recovery. This finding supports the hypothesis that the frontal lobes represent an ideal target of different types of rehabilitative strategies to maximise outcome (37). These might include, for instance, brain stimulation protocols that target the prefrontal cortex and especially the right precentral gyrus (38).
Limitations
This study has limitations. In particular, the small sample size constraints both the generalizability of results and strength of the conclusions. Additionally, while assessing outcome within 6 months post-injury allows to capture the highest degree of recovery in patients with other acquired non-traumatic brain lesions (28), it may be poorly informative in those with TBI, who could continue to improve up to 1-year post-injury (39). Finally, the study protocol did not include in-depth cognitive evaluations through more appropriate neuropsychology battery tests, which could have enabled more accurate associations between glucose metabolism changes and neurocognitive improvements. The setting was also unfit for the impact evaluation of rehabilitation protocols on outcome.
Conclusion
In conclusion, the present study provides preliminary data on the potential role of 18F-FDG PET as a useful prognostic tool for TBI patients undergoing rehabilitation courses. Voxel-wise analysis unveiled brain regions with high potential in terms of functional plasticity and neuronal network reorganization. In particular, these findings highlight a prefrontal 18F-FDG uptake, and its temporal evolution within the first months after injury, as a promising candidate of prognostic biomarker in TBI. Further studies with larger sample sizes and longer follow-up periods could help validate and expand upon these findings.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of ICS Maugeri (#2532 CE/2021). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
VP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft, Writing – review & editing. IB: Conceptualization, Data curation, Writing – review & editing. DD’A: Conceptualization, Data curation, Writing – review & editing. AN: Conceptualization, Writing – review & editing. GT: Conceptualization, Writing – review & editing. NC: Conceptualization, Data curation, Formal analysis, Supervision, Writing – review & editing, Writing – original draft. DF: Conceptualization, Data curation, Supervision, Writing – original draft, Writing – review & editing, Methodology.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was partially supported by the Italian Ministry of Health under the grant “Ricerca Corrente” funding schemes to the IRCCS.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The authors declare that no Generative AI was used in the creation of this manuscript.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1556427/full#supplementary-material
Footnotes
References
1. Kamins, J, and Giza, CC. Concussion-mild traumatic brain injury: recoverable injury with potential for serious sequelae. Neurosurg Clin N Am. (2016) 27:441–52. doi: 10.1016/j.nec.2016.05.005
2. Nguyen, R, Fiest, K.M, McChesney, J, and Kwon, C.S, Jette, N, Frolkis, A.D, et al. The international incidence of traumatic brain injury: a systematic review and Meta-analysis. Can J Neurol Sci (2016) 43:774–785. doi: 10.1017/cjn.2016.290
3. van der Horn, HJ, Out, ML, de Koning, ME, Mayer, AR, Spikman, JM, Sommer, IE, et al. An integrated perspective linking physiological and psychological consequences of mild traumatic brain injury. J Neurol. (2020) 267:2497–506. doi: 10.1007/s00415-019-09335-8
4. Maas, AI, Murray, GD, Roozenbeek, B, Lingsma, HF, Butcher, I, McHugh, GS, et al. Advancing care for traumatic brain injury: findings from the IMPACT studies and perspectives on future research. Lancet Neurol. (2013) 12:1200–10. doi: 10.1016/S1474-4422(13)70234-5
5. Graham, NS, and Sharp, DJ. Understanding neurodegeneration after traumatic brain injury: from mechanisms to clinical trials in dementia. J Neurol Neurosurg Psychiatry. (2019) 90:1221–33. doi: 10.1136/jnnp-2017-317557
6. Mele, C, Pingue, V, Caputo, M, Zavattaro, M, Pagano, L, Prodam, F, et al. Neuroinflammation and hypothalamo-pituitary dysfunction: focus of traumatic brain injury. Int J Mol Sci. (2021) 22:2686. doi: 10.3390/ijms22052686
7. Giza, CC, and Hovda, DA. The new neurometabolic cascade of concussion. Neurosurgery. (2014) 75:S24–33. doi: 10.1227/NEU.0000000000000505
8. Shetty, AK, Mishra, V, Kodali, M, and Hattiangady, B. Blood brain barrier dysfunction and delayed neurological deficits in mild traumatic brain injury induced by blast shock waves. Front Cell Neurosci. (2014) 8:232. doi: 10.3389/fncel.2014.00232
9. Portnow, LH, Vaillancourt, DE, and Okun, MS. The history of cerebral PET scanning: from physiology to cutting-edge technology. Neurology. (2013) 80:952–6. doi: 10.1212/WNL.0b013e318285c135
10. Huang, YL, Kuo, YS, Tseng, YC, Chen, DY, Chiu, WT, and Chen, CJ. Susceptibility-weighted MRI in mild traumatic brain injury. Neurology. (2015) 84:580–5. doi: 10.1212/WNL.0000000000001237
11. Ayubcha, C, Revheim, ME, Newberg, A, Moghbel, M, Rojulpote, C, Werner, TJ, et al. A critical review of radiotracers in the positron emission tomography imaging of traumatic brain injury: FDG, tau, and amyloid imaging in mild traumatic brain injury and chronic traumatic encephalopathy. Eur J Nucl Med Mol Imaging. (2021) 48:623–41. doi: 10.1007/s00259-020-04926-4
12. Wilde, EA, Wanner, IB, Kenney, K, Gill, J, Stone, JR, Disner, S, et al. A framework to advance biomarker development in the diagnosis, outcome prediction, and treatment of traumatic brain injury. J Neurotrauma. (2022) 39:436–57. doi: 10.1089/neu.2021.0099
13. Stout, DM, Buchsbaum, MS, Spadoni, AD, Risbrough, VB, Strigo, IA, Matthews, SC, et al. Multimodal canonical correlation reveals converging neural circuitry across trauma-related disorders of affect and cognition. Neurobiol Stress. (2018) 9:241–50. doi: 10.1016/j.ynstr.2018.09.006
14. Zhang, J, Mitsis, EM, Chu, K, Newmark, RE, Hazlett, EA, and Buchsbaum, MS. Statistical parametric mapping and cluster counting analysis of [18F] FDG-PET imaging in traumatic brain injury. J Neurotrauma. (2010) 27:35–49. doi: 10.1089/neu.2009.1049
15. Komura, A, Kawasaki, T, Yamada, Y, Uzuyama, S, Asano, Y, and Shinoda, J. Cerebral glucose metabolism in patients with chronic mental and cognitive sequelae after a single blunt mild traumatic brain injury without visible brain lesions. J Neurotrauma. (2019) 36:641–9. doi: 10.1089/neu.2018.5641
16. van der Horn, HJ, de Haan, S, Spikman, JM, de Groot, JC, and van der Naalt, J. Clinical relevance of microhemorrhagic lesions in subacute mild traumatic brain injury. Brain Imaging Behav. (2018) 12:912–6. doi: 10.1007/s11682-017-9743-6
17. Bischof, GN, and Cross, DJ. Brain trauma imaging. J Nucl Med. (2023) 64:20–9. doi: 10.2967/jnumed.121.263293
18. Bodien, YG, Barra, A, Temkin, NR, Barber, J, Foreman, B, Vassar, M, et al. Diagnosing level of consciousness: the limits of the Glasgow coma scale Total score. J Neurotrauma. (2021) 38:3295–305. doi: 10.1089/neu.2021.0199
19. Gurka, JA, Felmingham, KL, Baguley, IJ, Schotte, DE, Crooks, J, and Marosszeky, JE. Utility of the functional assessment measure after discharge from inpatient rehabilitation. J Head Trauma Rehabil. (1999) 14:247–56. doi: 10.1097/00001199-199906000-00005
20. Wilde, EA, Whiteneck, GG, Bogner, J, Bushnik, T, Cifu, DX, Dikmen, S, et al. Recommendations for the use of common outcome measures in traumatic brain injury research. Arch Phys Med Rehabil. (2010) 91:1650–1660.e17. doi: 10.1016/j.apmr.2010.06.033
21. McCrea, MA, Giacino, JT, Barber, J, Temkin, NR, Nelson, LD, Levin, HS, et al. Functional outcomes over the first year after moderate to severe traumatic brain injury in the prospective, longitudinal TRACK-TBI study. JAMA Neurol. (2021) 78:982–92. doi: 10.1001/jamaneurol.2021.2043
22. Varrone, A, Asenbaum, S, Vander Borght, T, Booij, J, Nobili, F, Någren, K, et al. EANM procedure guidelines for PET brain imaging using [18F]FDG, version 2. Eur J Nucl Med Mol Imaging. (2009) 36:2103–10. doi: 10.1007/s00259-009-1264-0
23. Riedl, V, Bienkowska, K, Strobel, C, Tahmasian, M, Grimmer, T, Förster, S, et al. Local activity determines functional connectivity in the resting human brain: a simultaneous FDG-PET/fMRI study. J Neurosci. (2014) 34:6260–6. doi: 10.1523/JNEUROSCI.0492-14.2014
24. Della Rosa, PA, Cerami, C, Gallivanone, F, Prestia, A, Caroli, A, Castiglioni, I, et al. A standardized [18F]-FDG-PET template for spatial normalization in statistical parametric mapping of dementia. Neuroinformatics. (2014) 12:575–93. doi: 10.1007/s12021-014-9235-4
25. Gallivanone, F, Della Rosa, PA, Perani, D, Gilardi, MC, and Castiglioni, IEADC-PET Consortium. The impact of different 18FDG PET healthy subject scans for comparison with single patient in SPM analysis. Q J Nucl Med Mol Imaging. (2017) 61:115–32. doi: 10.23736/S1824-4785.16.02749-7
26. Buchert, R, Wilke, F, Chakrabarti, B, Martin, B, Brenner, W, Mester, J, et al. Adjusted scaling of FDG positron emission tomography images for statistical evaluation in patients with suspected Alzheimer’s disease. J Neuroimaging. (2005) 15:348–55. doi: 10.1111/j.1552-6569.2005.tb00335.x
27. Dukart, J, Mueller, K, Horstmann, A, Vogt, B, Frisch, S, Barthel, H, et al. Differential effects of global and cerebellar normalization on detection and differentiation of dementia in FDG-PET studies. NeuroImage. (2010) 49:1490–5. doi: 10.1016/j.neuroimage.2009.09.017
28. Nudo, RJ. Recovery after brain injury: mechanisms and principles. Front Hum Neurosci. (2013) 7:887. doi: 10.3389/fnhum.2013.00887
29. Wieloch, T, and Nikolich, K. Mechanisms of neural plasticity following brain injury. Curr Opin Neurobiol. (2006) 16:258–64. doi: 10.1016/j.conb.2006.05.011
30. Norden, DM, Muccigrosso, MM, and Godbout, JP. Microglial priming and enhanced reactivity to secondary insult in aging, and traumatic CNS injury, and neurodegenerative disease. Neuropharmacology. (2015) 96:29–41. doi: 10.1016/j.neuropharm.2014.10.028
31. Kato, T, Nakayama, N, Yasokawa, Y, Okumura, A, Shinoda, J, and Iwama, T. Statistical image analysis of cerebral glucose metabolism in patients with cognitive impairment following diffuse traumatic brain injury. J Neurotrauma. (2007) 24:919–26. doi: 10.1089/neu.2006.0203
32. Rizzolatti, G, and Luppino, G. The cortical motor system. Neuron. (2001) 31:889–901. doi: 10.1016/s0896-6273(01)00423-8
33. Wiese, H, Tönnes, C, de Greiff, A, Nebel, K, Diener, HC, and Stude, P. Self-initiated movements in chronic prefrontal traumatic brain injury: an event-related functional MRI study. NeuroImage. (2006) 30:1292–301. doi: 10.1016/j.neuroimage.2005.11.012
34. Radtke-Schuller, S, Town, SM, Yin, P, Elgueda, D, Schuller, G, Bizley, JK, et al. Dorsal prefrontal and premotor cortex of the ferret as defined by distinctive patterns of thalamo-cortical projections. Brain Struct Funct. (2020) 225:1643–67. doi: 10.1007/s00429-020-02086-7
35. Hillary, FG, Rajtmajer, SM, Roman, CA, Medaglia, JD, Slocomb-Dluzen, JE, Calhoun, VD, et al. The rich get richer: brain injury elicits hyperconnectivity in core subnetworks. PLoS One. (2014) 14;9:e104021. doi: 10.1371/journal.pone.0104021. Erratum in: PLoS One. 2014;9(11):e113545
36. Zhang, D, Zhu, P, Yin, B, Zhao, P, Wang, S, Ye, L, et al. Frontal white matter Hyperintensities effect on default mode network connectivity in acute mild traumatic brain injury. Front Aging Neurosci. (2022) 13:793491. doi: 10.3389/fnagi.2021.793491
37. Stuss, DT. Traumatic brain injury: relation to executive dysfunction and the frontal lobes. Curr Opin Neurol. (2011) 24:584–9. doi: 10.1097/WCO.0b013e32834c7eb9
38. Surendrakumar, S, Rabelo, TK, Campos, ACP, Mollica, A, Abrahao, A, Lipsman, N, et al. Neuromodulation therapies in pre-clinical models of traumatic brain injury: systematic review and translational applications. J Neurotrauma. (2023) 40:435–48. doi: 10.1089/neu.2022.0286
Keywords: traumatic brain injury, rehabilitation, PET scanning, neuroplasticity, voxel-wise analyses
Citation: Pingue V, Bossert I, D’Ambrosio D, Nardone A, Trifirò G, Canessa N and Franciotta D (2025) Brain glucose metabolism in patients with traumatic brain injury undergoing rehabilitation: a longitudinal 18F-FDG PET study. Front. Neurol. 16:1556427. doi: 10.3389/fneur.2025.1556427
Edited by:
Giuseppe Lazzarino, University of Catania, ItalyReviewed by:
Kryshawna Beard, Traumatic Brain Injury Center of Excellence, United StatesNatascha Ekdahl, Karolinska Institutet (KI), Sweden
Copyright © 2025 Pingue, Bossert, D’Ambrosio, Nardone, Trifirò, Canessa and Franciotta. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Valeria Pingue, dmFsZXJpYS5waW5ndWVAaWNzbWF1Z2VyaS5pdA==
†These authors have contributed equally to this work and share last authorship
‡ORCID: Valeria Pingue, orcid.org/0000-0001-9376-4699