
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 02 April 2025
Sec. Neurological Biomarkers
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1548666
 Yizhou Chen1†
Yizhou Chen1† Meifang Liu2,3†Yi Zhang4Xiaolin Yang1Mengqi Yue1Xu Chen1Haiqiang Wang1Zirong Wang1Haocheng Yu1Jing Shi1,2,3*
Meifang Liu2,3†Yi Zhang4Xiaolin Yang1Mengqi Yue1Xu Chen1Haiqiang Wang1Zirong Wang1Haocheng Yu1Jing Shi1,2,3*Objective: This cross-sectional study is based on the NHANES (1999–2010) database and aims to explore the potential relationship between the CALLY index and stroke in the U.S. population.
Methods: This cross-sectional study utilized data from NHANES (1999–2010), including 17,511 American participants after data cleaning. Laboratory markers related to the CALLY index were obtained through standardized biological sample collection and analysis procedures performed by trained professionals. Stroke status was determined based on self-reported questionnaires. Various statistical methods were employed to examine the association between the CALLY index and stroke, as well as its predictive efficacy for stroke risk, including multivariable logistic regression, subgroup analysis, RCS analysis, and ROC analysis.
Results: Among the 17,511 participants analyzed, our findings revealed a nonlinear L-shaped negative association between the CALLY index and stroke risk. In Model 3, a higher CALLY index was significantly associated with a lower stroke risk (OR: 0.99, 95% CI: 0.98–0.99, p = 0.045). Additionally, participants in the highest quartile (Q4) of the CALLY index had a 25% lower likelihood of stroke compared to those in the lowest quartile (Q1) (OR: 0.75, 95% CI: 0.58–0.97, p = 0.030). Furthermore, ROC analysis demonstrated that the CALLY index had superior predictive performance for stroke risk compared to the SIRI and SII indices.
Conclusion: A reduced CALLY index may be linked to a higher risk of stroke. Furthermore, the CALLY index demonstrates superior predictive performance compared to the SIRI and SII indices. The association between the CALLY index and stroke risk provides valuable insights for future stroke prevention and management strategies.
Stroke, also referred to as a cerebrovascular accident (CVA), is a leading cause of mortality and disability worldwide. Stroke is classified into ischemic stroke (IS) and hemorrhagic stroke (HS), with ischemic stroke comprising more than 70% of cases. The incidence of ischemic stroke has been rising annually, with an increasingly younger age of onset (1). Hemorrhagic stroke is a severe condition resulting from the rupture of cerebral blood vessels, leading to localized mechanical and compressive damage (2). If left untreated, ischemic stroke and cerebral ischemia can lead to severe neurological dysfunction or even death. Numerous studies have demonstrated that both types of stroke involve blood–brain barrier disruption, inflammatory cytokine release, and immune cell infiltration, with immune cells and inflammatory responses playing critical roles in stroke pathogenesis (3–5).
Studies have demonstrated that the Systemic Inflammation Response Index (SIRI) and the Systemic Immune-Inflammation Index (SII) are strongly associated with stroke onset and prognosis (6–8). The C-reactive protein–albumin–lymphocyte (CALLY) index is a newly developed inflammation-based biomarker. It consists of the inflammatory index (C-reactive protein), nutritional index (serum albumin), and immune index (lymphocytes), which reflect inflammation levels, nutritional status, and immune function, respectively (9). Previously, it has been mainly utilized for postoperative prognosis assessment in patients with solid tumors, such as liver cancer (10), gastric cancer (11), breast cancer (12), and oral cancer (13). As a composite index, it offers a more comprehensive assessment of the patient’s immune status and systemic inflammatory balance, exhibiting significant advantages in tumor prognosis prediction. In stroke pathophysiology, inflammation, immune responses, and nutritional status play pivotal roles. The CALLY index, as a composite biomarker, reflects systemic inflammation, immune status, and nutritional condition. Therefore, it serves as a promising biomarker for predicting stroke risk and guiding early interventions and preventive strategies. However, studies investigating the CALLY index in neurological diseases remain limited. This study thus aims to explore the association between the CALLY index and stroke and further evaluate its predictive value for stroke occurrence.
The data for this study were obtained exclusively from the NHANES database,1 a nationally representative cross-sectional survey conducted by the Centers for Disease Control and Prevention (CDC) in collaboration with the National Center for Health Statistics (NCHS) (14). The NHANES database collects demographic, health status, laboratory, and nutritional data through a complex multistage probability sampling design, incorporating household interviews, mobile examination centers, and biospecimen collection. The study protocol was approved by the NCHS Research Ethics Review Board, and informed consent was obtained from all participants (15). This study included NHANES data from 1999 to 2010 for cross-sectional analysis. The objective was to investigate the association between the CALLY index and stroke. Initially, individuals aged 18 years or older from six consecutive NHANES cycles (1999–2010) were included, yielding a total sample size of 35,379. Participants were excluded if they had missing data on stroke or CALLY index-related variables (N = 6,829), lacked covariate data (N = 10,584), were lost to follow-up (N = 453), or were identified as extreme outliers (N = 2). The final analytical sample comprised 17,511 participants. Detailed information is shown in Figure 1.
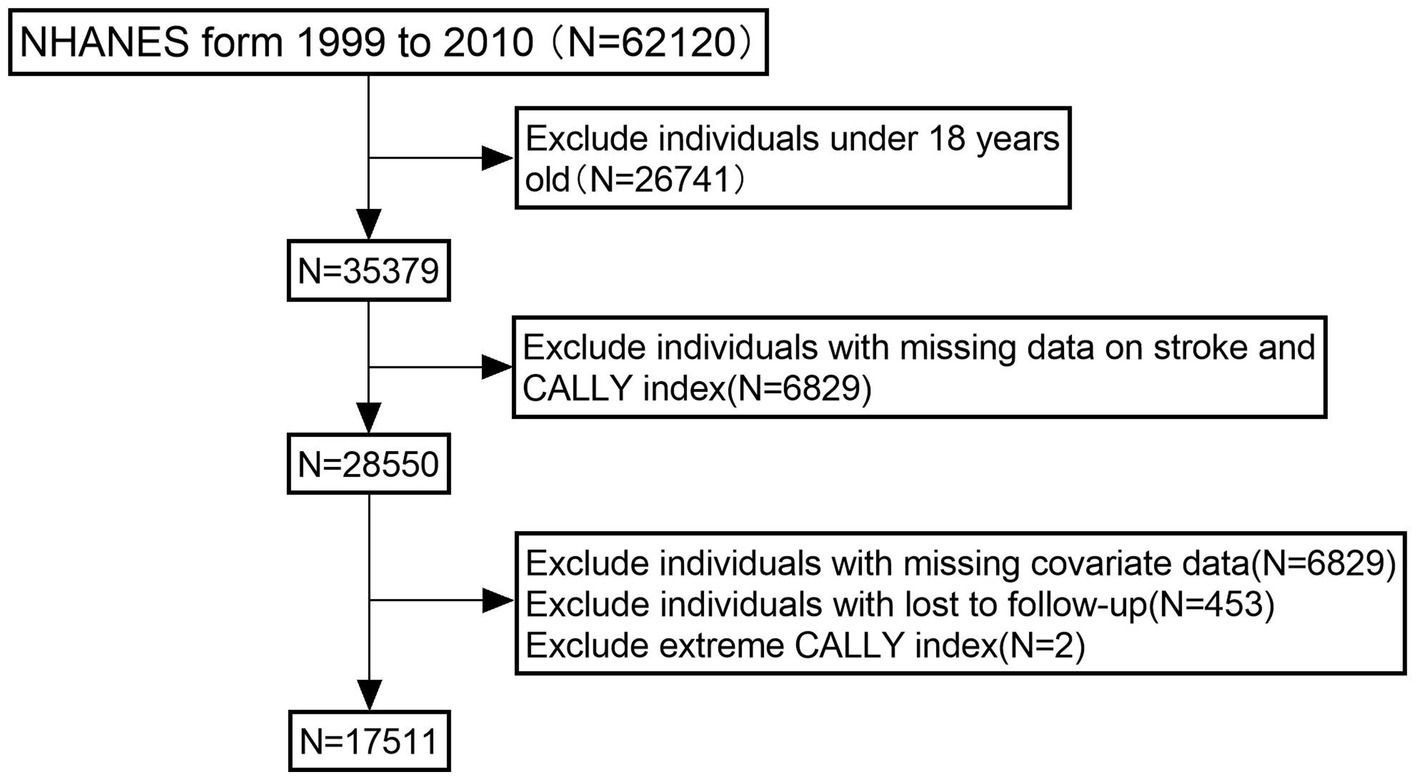
Figure 1. Flowchart of the sample selection from NHANES 1999–2010.
In this study, stroke diagnosis was primarily determined based on self-reported data from personal interviews. Participants completed a questionnaire in which they reported whether a physician or other healthcare professional had diagnosed them with a stroke (16). Laboratory parameters related to the CALLY, SIRI, and SII indices were measured by trained professionals using standardized biospecimen collection and analysis protocols. The calculation formulas for the CALLY, SIRI, and SII indices are as follows (17–19): CALLY = Serum albumin level (g/dL) × Lymphocyte count (1,000 cells/mL)/C-reactive protein (mg/dL) /10; SIRI = Neutrophil count (cells/mL) × Monocyte count (cells/mL)/Lymphocyte count (cells/mL); SII = Neutrophil count (cells/mL) × Platelet count (cells/mL)/Lymphocyte count (cells/mL).
Covariates primarily comprised demographic characteristics and established stroke risk factors. Demographic characteristics included sex, age, race/ethnicity, education level, and marital status. Age was stratified into three groups: 18–39, 40–59, and ≥60 years. Race/ethnicity was classified into Mexican American, Non-Hispanic Black, Non-Hispanic White, and Other. Education level was categorized as follows: Junior Middle School or Below (9th–11th Grade, including 12th grade with no diploma, and Less Than 9th Grade), Senior High School or General Educational Development (High School Graduate/General Educational Development or Equivalent), and College or Above (Some College or Associate Degree, and College Graduate or Above). Marital status was classified as Married/Partnered (Married, Living with Partner), Separated/Widowed (Widowed, Divorced, Separated), and Single (Never Married). Smoking status was defined as “Yes” if a participant had smoked at least 100 cigarettes in their lifetime; otherwise, it was classified as “No.” Alcohol consumption was defined as “Yes” if a participant had consumed at least 12 alcoholic drinks in any given year; otherwise, it was classified as “No.” Body mass index (BMI) (20), hypertension (21), diabetes (22), and coronary heart disease (23) all established stroke risk factors, were included as covariates. Hypertension was defined as a self-reported physician diagnosis or current use of antihypertensive medication. Diabetes and coronary heart disease were defined based on self-reported physician diagnoses.
First, we organized the data for analysis. Categorical variables were presented as counts and proportions, and the chi-square test was employed to compare intergroup differences. Quartile-based adjustments and analyses were conducted for the CALLY index. Subsequently, three weighted generalized linear regression models were applied to examine the association between the CALLY index and stroke: Model 1 (unadjusted), Model 2 (adjusted for sex, race, and age), and Model 3 (adjusted for sex, race, age, BMI, education level, marital status, smoking status, alcohol consumption, hypertension, diabetes, and coronary heart disease). Finally, restricted cubic splines (RCS) with three knots were employed to investigate the potential non-linear association between the CALLY index and stroke. Segmented regression models were utilized to evaluate the relationship and determine its linearity. Additionally, area under the curve (AUC) and receiver operating characteristic (ROC) curve analyses were performed to assess the predictive capability of the CALLY index and other inflammatory markers, including SIRI and SII. The accuracy and effectiveness of these markers in distinguishing different clinical or disease states were assessed using AUC and ROC curve analyses. All analyses were conducted using R (version 4.3.3).
This study included 17,511 individuals from the NHANES database across 6 cycles (1999–2010). The mean age was 49.53 ± 18.3 years, with males comprising 49.0% and females 51.0%. The weighted demographic and laboratory characteristics of participants, stratified by stroke status (stroke: 637; no stroke: 16,876), revealed significant differences in age (66.96 ± 13.58 vs. 48.87 ± 18.13, p < 0.001) and BMI (29.64 ± 6.36 vs. 28.83 ± 6.62, p = 0.003) between stroke and non-stroke individuals. Significant differences were also observed in race, education level, marital status, smoking status, alcohol consumption, hypertension, and coronary heart disease (all p < 0.001). Detailed information is provided in Table 1. In the box plot, the maximum CALLY index in the non-stroke group was significantly higher than that in the stroke group (p < 0.001), suggesting a potential association between a higher CALLY index and a reduced risk of stroke (Figure 2).
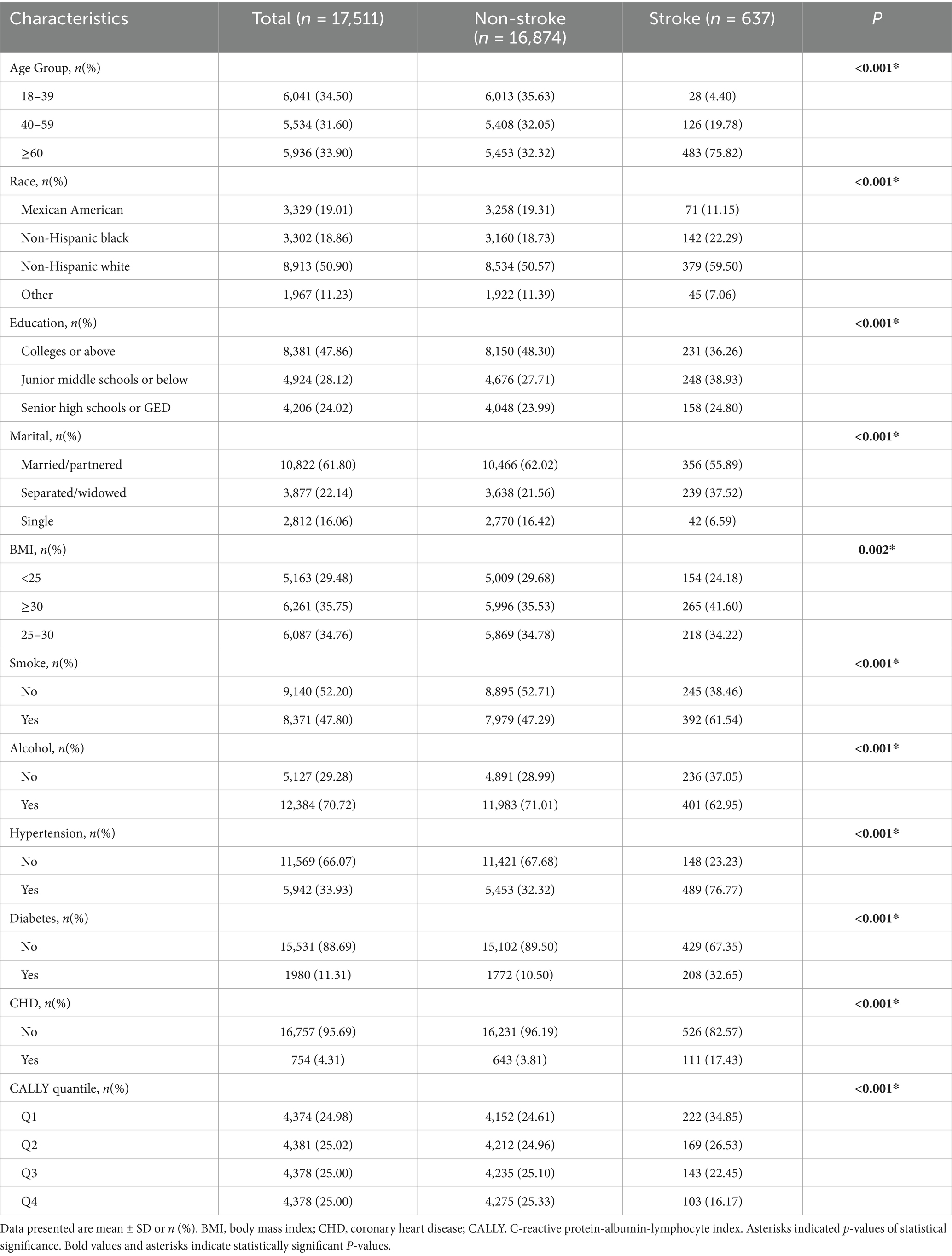
Table 1. Baseline characteristics.
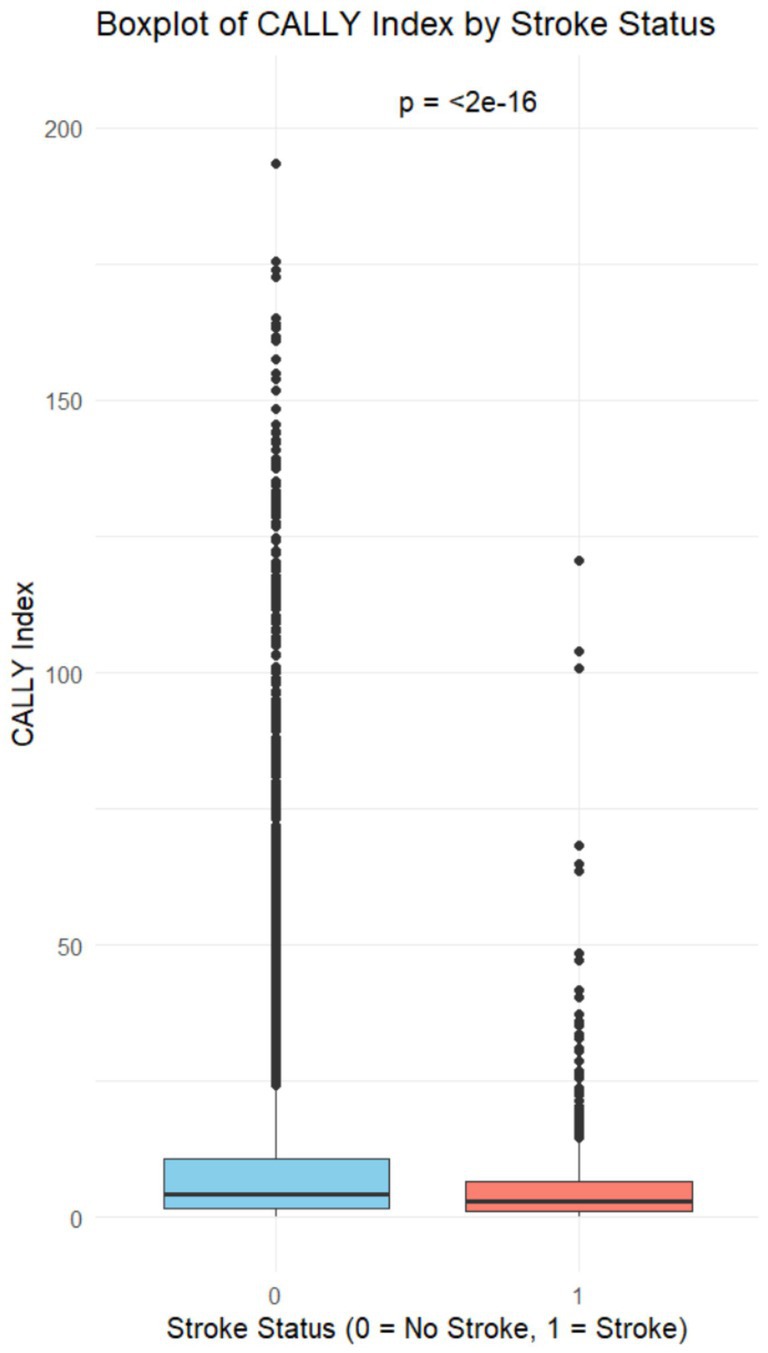
Figure 2. Boxplot of CALLY index by stroke status.
Three logistic regression models were developed to investigate the independent association between the CALLY index and stroke. In Model 1 (unadjusted), a higher CALLY index was associated with a lower risk of stroke (OR: 0.97, 95% CI: 0.96–0.98, p < 0.001). In Model 2, after adjustment for sex, race, and age, the findings remained consistent with Model 1 (OR: 0.99, 95% CI: 0.98–0.99, p = 0.003). In Model 3, after further adjustment for BMI, education level, marital status, smoking status, alcohol consumption, hypertension, diabetes, and coronary heart disease, a higher CALLY index remained associated with a lower risk of stroke (OR: 0.99, 95% CI: 0.98–0.99, p = 0.045) (Table 2). Thus, each 1 SD increase in the CALLY index was associated with a 1% reduction in stroke risk. Additionally, the CALLY index was categorized into quartiles for analysis. In Model 3, participants in Q4 had a 25% lower likelihood of stroke than those in Q1 (OR: 0.75, 95% CI: 0.58–0.97, p = 0.030). Similarly, participants in Q3 had a 22% lower likelihood of stroke than those in Q1 (OR: 0.78, 95% CI: 0.62–0.98, p = 0.036) (Table 2). Finally, weighted RCS analysis was conducted to model and visualize the association between the CALLY index and stroke risk. The analysis revealed a non-linear, L-shaped association between the CALLY index and stroke risk (p < 0.001) (Figure 3).
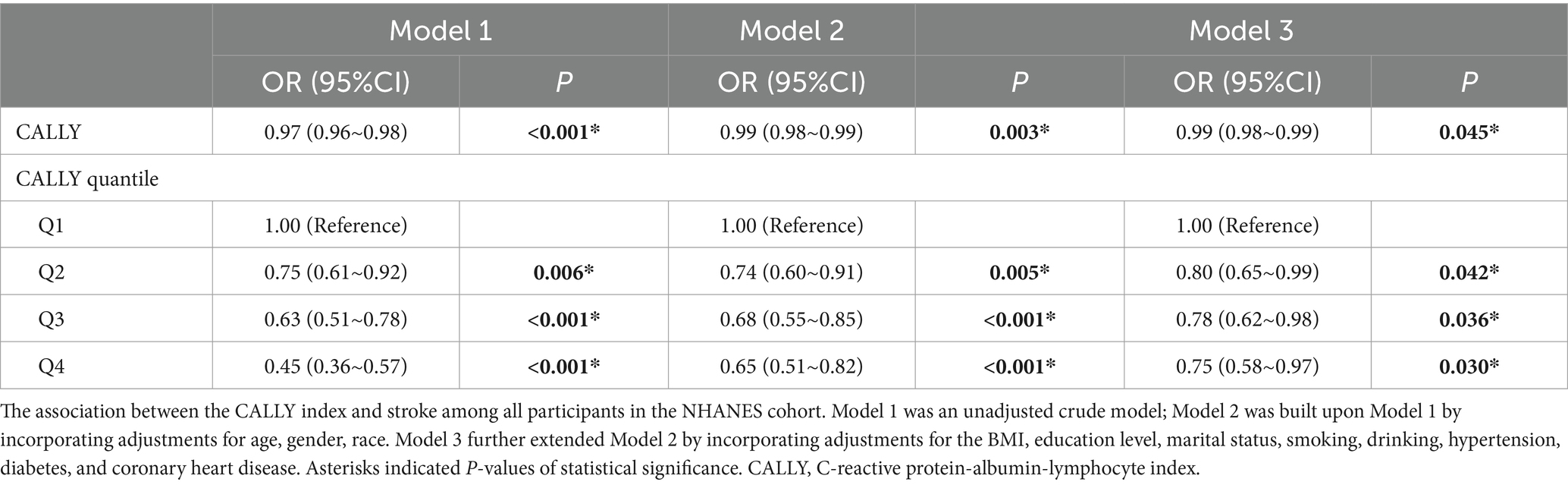
Table 2. Weighted multivariate logistic analysis CALLY and stroke.
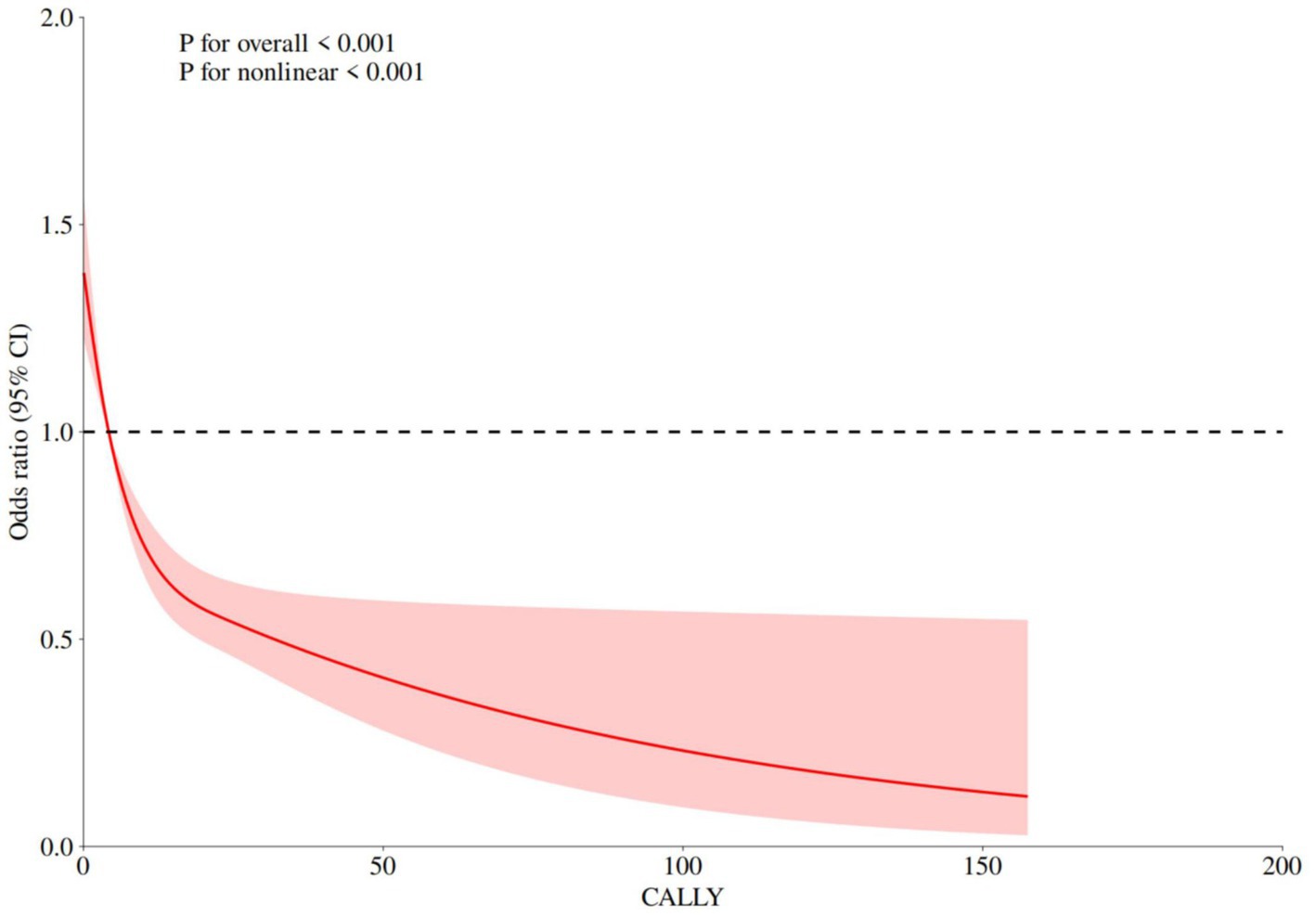
Figure 3. RCS analysis of relationship between the CALLY index and stroke.
To assess the consistency of the association between the CALLY index and stroke across different subgroups, we performed subgroup analyses stratified by age, race, marital status, hypertension, diabetes, and coronary heart disease. The results revealed no significant interactions among these variables (p: 0.064–0.523) (Table 3), suggesting that the association between the CALLY index and stroke was not substantially modified by these covariates, thereby reinforcing the robustness of the findings.
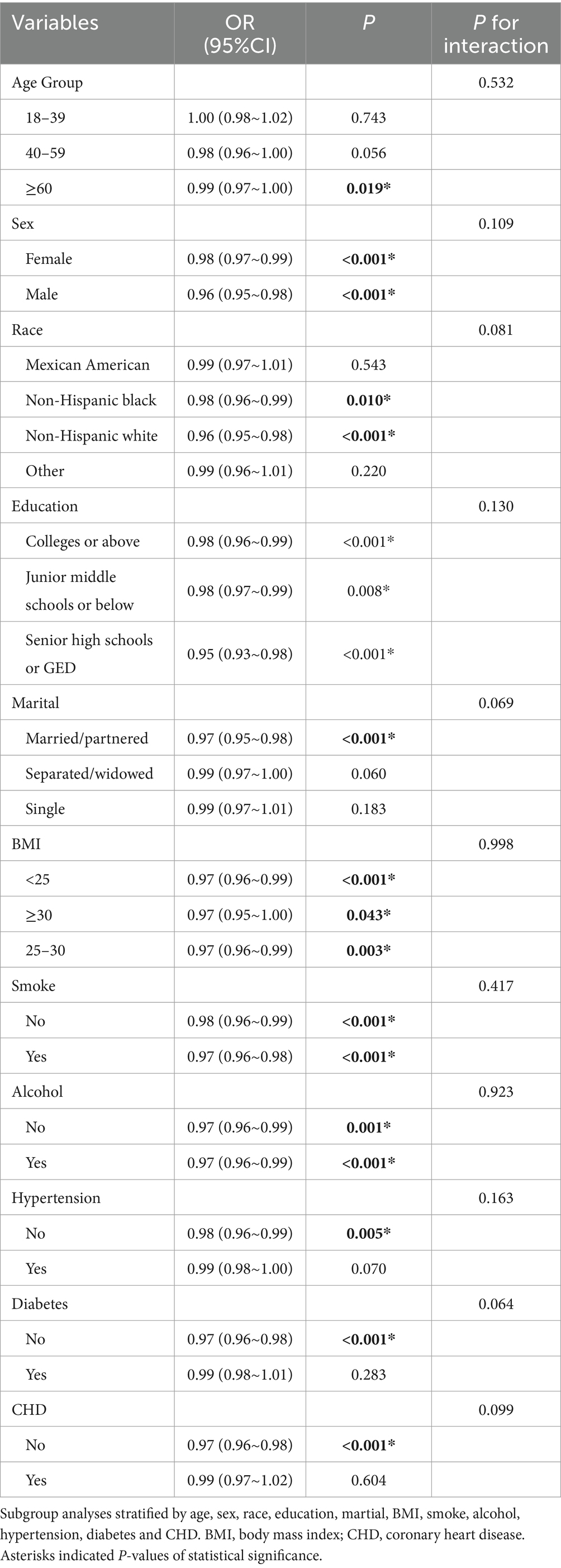
Table 3. Subgroup analysis.
Sensitivity analyses were performed to assess the predictive ability of the CALLY, SIRI, and SII indices for stroke. The ROC curve analysis showed that the AUC value of the CALLY index (0.590, 95% CI: 0.568–0.612) was higher than that of the SIRI (0.577, 95% CI: 0.554–0.600) and SII indices (0.525, 95% CI: 0.502–0.548) (Figure 4). These findings suggest that the CALLY index exhibits greater stability and accuracy in predicting stroke risk compared to the SIRI and SII indices. Additionally, ROC analysis of the CALLY index across three models revealed that the AUC for Model 2 was 0.770 (95% CI: 0.754–0.786), whereas for Model 3, it was 0.827 (95% CI: 0.813–0.840) (Figure 5).
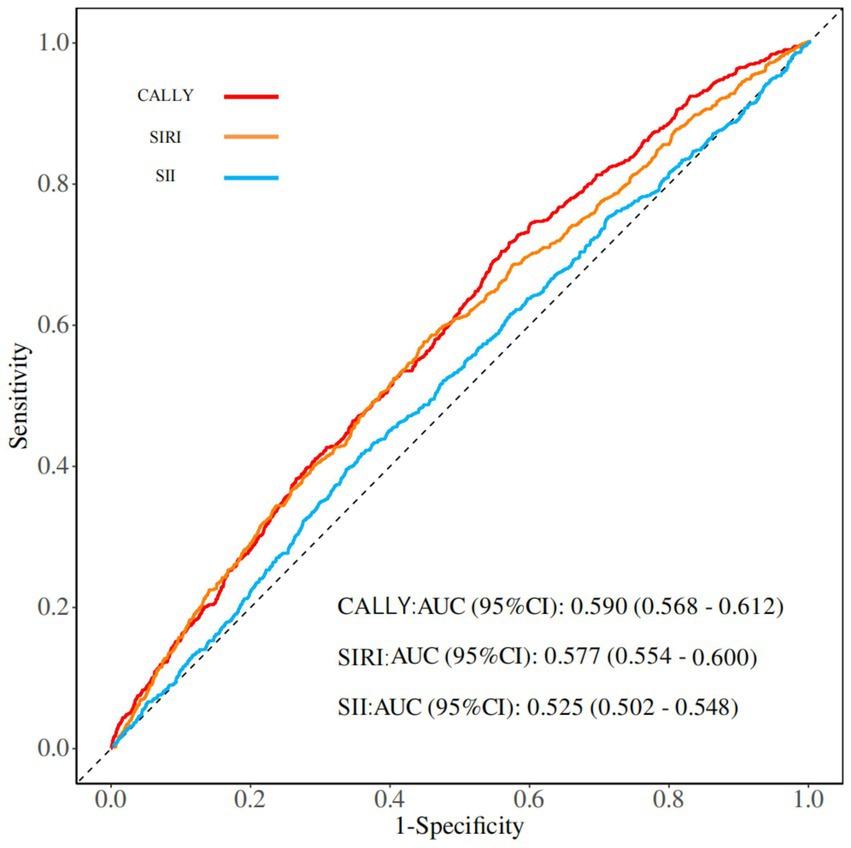
Figure 4. ROC analysis of the CALLY index, SIRl index, and Sll index.
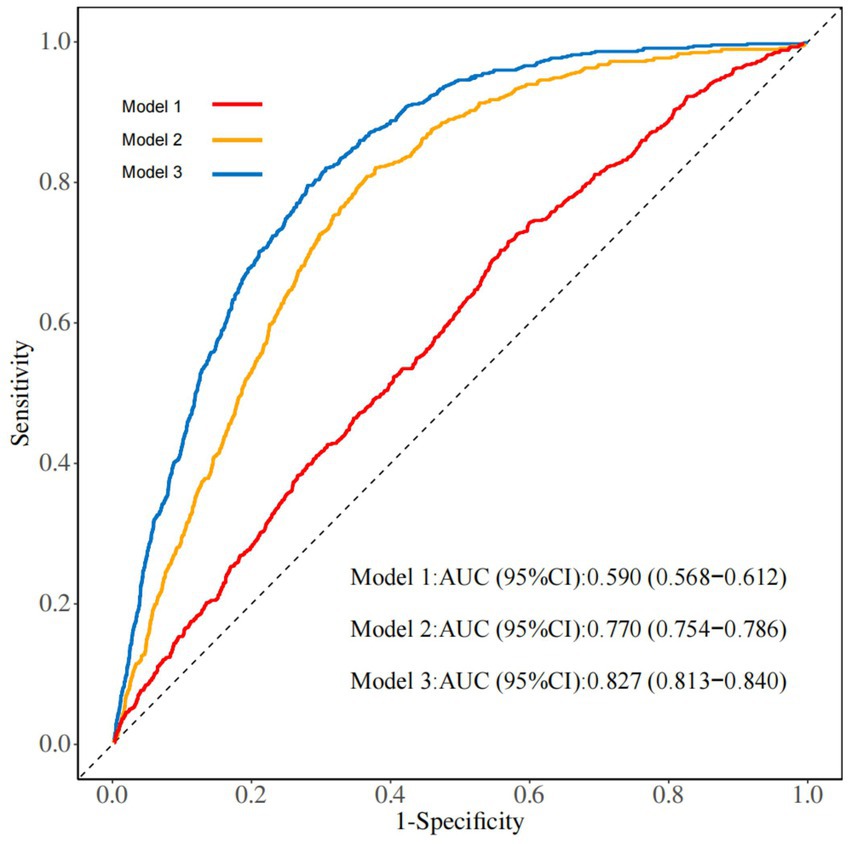
Figure 5. ROC analysis of the three models of the CALLY index.
This study aimed to assess the association between the CALLY index and stroke risk in U.S. adults (≥18 years) from 1999 to 2010. We found that the CALLY index was significantly elevated in individuals with stroke compared to those without. Furthermore, RCS analysis identified a potential nonlinear L-shaped inverse association between the CALLY index and stroke risk. This phenomenon may be attributed to the fact that elevated levels of albumin and lymphocytes could suppress inflammatory damage through mechanisms such as antioxidant activity and immune modulation. However, once these levels surpass a certain threshold, their protective effects no longer exhibit linear enhancement, leading to a plateau in risk within higher index ranges. Finally, subgroup and ROC analyses further confirmed the robustness and predictive accuracy of the results. Additionally, comparisons with other inflammatory markers suggested that the CALLY index demonstrated superior stability and predictive accuracy for stroke risk.
During the pathological processes of both IS and HS, the body undergoes a series of immune-inflammatory responses. In ischemic stroke, early ischemia and hypoxia result in brain tissue damage, energy metabolism disorders, and blood–brain barrier disruption, leading to neuronal death and the formation of an ischemic penumbra (24, 25).In hemorrhagic stroke, vascular rupture causes blood components to extravasate directly into the brain, forming hematomas that result in structural damage (26). Following stroke onset, cells affected by the initial injury trigger a rapid cascade of events, leading to an intense inflammatory response.
A cross-sectional study based on the 2005–2018 NHANES database, including 902 stroke patients, suggested that an elevated SII index may be associated with a higher risk of ischemic stroke (27). Additionally, a cross-sectional study of stroke patients within a hypertensive population, based on the 1999–2020 NHANES database, demonstrated that higher SIRI index levels were significantly associated with an increased incidence of stroke in hypertensive patients (28). Both studies suggest that lymphopenia during stroke may reflect immune dysfunction. This phenomenon may be explained by the distinct roles of T and B lymphocytes in stroke pathophysiology. Studies indicate that following IS onset, CD8+ cytotoxic T lymphocytes infiltrate the ischemic site within 3 h. These cells induce direct neuronal damage by releasing cytotoxic proteins, including granzyme and perforin. Furthermore, they secrete inflammatory mediators, including IL-16, which promote the recruitment of immune cells and exacerbate damage to the vascular endothelium and blood–brain barrier (29, 30). In contrast, B cells can inhibit the activation and recruitment of T cells, macrophages, and other immune cells, thereby reducing the extent of cerebral infarction and improving neurological deficits (31). In HS, lymphocytes are also critical mediators. Evidence suggests that lymphocytes regulate local inflammatory responses by secreting cytokines, modulating blood–brain barrier permeability, and ameliorating neurological symptoms following brain hemorrhage (32).
A prospective cohort study investigating the effects of C-reactive protein (CRP) levels and dyslipidemia on stroke reported that elevated CRP levels and dyslipidemia were associated with an increased stroke risk in men (33).Similarly, studies have indicated that serum CRP levels rise significantly 48–72 h post-admission in patients with HS, with the magnitude of elevation correlating with hematoma volume (34).As an inflammatory marker, CRP levels rise rapidly during stroke, likely in response to immune activation triggered by ischemic or hemorrhagic brain injury. This cascade activates inflammatory cells and promotes cytokine release, which in turn stimulates hepatic CRP synthesis (35, 36).
A strong association has been observed between albumin levels and IS. A study conducted in a cohort of 2,986 individuals from North Manhattan reported that low serum albumin levels were associated with an increased risk of IS, particularly in cases of cardiogenic embolism and cryptogenic subtypes (37). Similarly, a prospective study examining the association between serum albumin levels and clinical outcomes in IS patients reported that each 1 g/L decrease in serum albumin was linked to a 3% increase in the risk of poor functional prognosis and a 7% increase in mortality risk (38). In patients with HS, studies have suggested that hypoalbuminemia may be associated with an elevated risk of HS and a higher incidence of adverse events in its prognosis. These findings indicate that albumin, as a nutritional marker, reflects both an individual’s overall health status and systemic inflammation levels (39). The potential mechanisms may involve albumin’s antioxidant, anti-inflammatory, and endothelial-protective properties (40–42). Compared with the SIRI and SII indices, the CALLY index exhibits greater stability and accuracy in predicting stroke risk, potentially due to its dependence on serum albumin levels.
Our study has several strengths. First, we not only analyzed the predictive performance of the CALLY index for stroke but also compared its predictive ability with that of the SII and SIRI indices. Second, we adjusted for covariates in this study, constructed multiple predictive models, and performed sensitivity analyses to ensure the robustness of the final results. However, this study has several limitations. First, as a cross-sectional study, this research identifies an association between the CALLY index and stroke, but the causal relationship remains unclear. Second, as the NHANES database collects data from a representative U.S. population, the findings may not be generalizable to the global population. Furthermore, the reliance on self-reported diagnoses for case inclusion could introduce selection bias, while unmeasured covariates (e.g., genetic susceptibility, socioeconomic status) might act as residual confounders, potentially influencing the observed associations. Finally, although the CALLY index demonstrates better predictive performance than other inflammatory markers, its overall clinical utility remains limited, necessitating further investigation in future studies.
A reduced CALLY index may be linked to a higher risk of stroke. Furthermore, the CALLY index demonstrates superior predictive performance compared to the SIRI and SII indices. The association between the CALLY index and stroke risk provides valuable insights for future stroke prevention and management strategies.
Publicly available datasets were analyzed in this study. This data can be found at: https://www.cdc.gov/nchs/nhanes.
The studies involving humans were approved by the National Center for Health Statistics. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
YC: Conceptualization, Data curation, Formal analysis, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. ML: Formal analysis, Methodology, Writing – review & editing. YZ: Data curation, Methodology, Writing – review & editing. XY: Formal analysis, Methodology, Writing – review & editing. MY: Software, Visualization, Writing – review & editing. XC: Formal analysis, Methodology, Writing – review & editing. HW: Writing – review & editing. ZW: Writing – review & editing. HY: Writing – review & editing. JS: Funding acquisition, Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. The study was supported by the Fundamental Research Key Project of Yunnan Science and Technology Department (202101AZ070001-165), the Special Project for Famous Doctors of “Xingdian Talent Support Program” in Yunnan Province, and the National Natural Science Foundation of China (No. 82060901).
We thank all of the investigators for sharing summary level data on NHANES for related data, and also express our gratitude to the participants of this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
CVA, Cerebrovascular accident; IS, Ischemic stroke; HS, Hemorrhagic stroke; SIRI, Inflammation Response Index; SII, Systemic Immune-Inflammation Index; CALLY, C-reactive protein-albumin-lymphocyte; CDC, The Centers for Disease Control and Prevention; NCHS, The National Center for Health Statistics; BMI, Body mass index; RCS, Restricted cubic splines; AUC, The area under the curve; ROC, Receiver operating characteristic; CRP, CReactive protein.
1. Wu, S, Wu, B, and Liu, M. Stroke in China: advances and challenges in epidemiology, prevention, and management. Lancet Neurol. (2019) 18:394–405. doi: 10.1016/S1474-4422(18)30500-3
2. GBD 2016 Stroke collaborators. Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:439–58. doi: 10.1016/S1474-4422(19)30034-1
3. Yan, T, Chopp, M, and Chen, J. Experimental animal models and inflammatory cellular changes in cerebral ischemic and hemorrhagic stroke. Neurosci Bull. (2015) 31:717–34. doi: 10.1007/s12264-015-1567-z
4. Pluta, R, Januszewski, S, and Czuczwar, SJ. Neuroinflammation in post-ischemic neurodegeneration of the brain: friend, foe, or both? Int J Mol Sci. (2021) 22:4405. doi: 10.3390/ijms22094405
5. Wang, J. Preclinical and clinical research on inflammation after intracerebral hemorrhage. Prog Neurobiol. (2010) 92:463–77. doi: 10.1016/j.pneurobio.2010.08.001
6. Huang, S, Xie, W, and Gao, Y. A role for systemic inflammation in stroke-associated infection and the long-term prognosis of acute ischemic stroke: a mediation analysis. J Inflamm Res. (2024) 17:6533–45. doi: 10.2147/JIR.S474344
7. Li, J, Zhang, P, and Chen, H. Elevated systemic inflammation response index is associated with poor outcomes in minor ischemic stroke. Front Neurol. (2024) 15:1492224. doi: 10.3389/fneur.2024.1492224
8. Yang, Y, He, P, and Zhang, Y. Systemic immune-inflammation index predicts short-term mortality in acute ischemic stroke with severe stenosis of internal carotid artery associated pneumonia. Brain Behav. (2024) 14:e70047. doi: 10.1002/brb3.70047
9. Jiang, T, Sun, H, and Xu, T. Significance of pre-treatment CALLY score combined with EBV-DNA levels for prognostication in non-metastatic nasopharyngeal Cancer patients: a clinical perspective. J Inflamm Res. (2024) 17:3353–69. doi: 10.2147/JIR.S460109
10. Iida, H, Tani, M, and Komeda, K. Superiority of CRP-albumin-lymphocyte index (CALLY index) as a non-invasive prognostic biomarker after hepatectomy for hepatocellular carcinoma. HPB. (2022) 24:101–15. doi: 10.1016/j.hpb.2021.06.414
11. Aoyama, T, Hashimoto, I, and Maezawa, Y. CRP-albumin-lymphocyte (CALLY) index is an independent prognostic factor for the esophageal Cancer patients who received curative treatment. Anticancer Res. (2024) 44:815–22. doi: 10.21873/anticanres.16873
12. Feng, J, Wang, L, and Yang, X. Clinical significance of preoperative CALLY index for prognostication in patients with esophageal squamous cell carcinoma undergoing surgery. Sci Rep. (2024) 14:713. doi: 10.1038/s41598-023-51109-w
13. Tsai, YT, Ko, CA, and Chen, HC. Prognostic value of CRP-albumin-lymphocyte (CALLY) index in patients undergoing surgery for Oral cavity Cancer. J Cancer. (2022) 13:3000–12. doi: 10.7150/jca.74930
14. Ahluwalia, N, Dwyer, J, and Terry, A. Update on NHANES dietary data: focus on collection, release, analytical considerations, and uses to inform public policy. Adv Nutr. (2016) 7:121–34. doi: 10.3945/an.115.009258
15. Zipf, G, Chiappa, M, and Porter, KS. National health and nutrition examination survey: plan and operations, 1999-2010. Vital Health Stat. (2013) 1:1–37.
16. Zheng, Y, Huang, C, and Jin, J. Association between stroke and relative fat mass: a cross-sectional study based on NHANES. Lipids Health Dis. (2024) 23:354. doi: 10.1186/s12944-024-02351-2
17. Zhu, D, Lin, YD, and Yao, YZ. Negative association of C-reactive protein-albumin-lymphocyte index (CALLY index) with all-cause and cause-specific mortality in patients with cancer: results from NHANES 1999-2018. BMC Cancer. (2024) 24:1499. doi: 10.1186/s12885-024-13261-y
18. Lu, Y, Lu, C, and Luo, Z. Association between the systemic inflammatory response index and mortality in patients with sarcopenia. PLoS One. (2024) 19:e0312383. doi: 10.1371/journal.pone.0312383
19. Dong, K, Zheng, Y, and Wang, Y. Predictive role of neutrophil percentage-to-albumin ratio, neutrophil-to-lymphocyte ratio, and systemic immune-inflammation index for mortality in patients with MASLD. Sci Rep. (2024) 14:30403. doi: 10.1038/s41598-024-80801-8
20. Einarsson, G, Thorleifsson, G, and Steinthorsdottir, V. Sequence variants associated with BMI affect disease risk through BMI itself. Nat Commun. (2024) 15:9335. doi: 10.1038/s41467-024-53568-9
21. Qiu, W, Cai, A, and Wu, S. Hypertension awareness, treatment, control, and prognosis: insights from the sub-cohort of China PEACE million persons project. Hypertens Res. (2024) 48:1012–23. doi: 10.1038/s41440-024-02037-3
22. Yu, S, Zhao, W, and Qian, B. Uncover visit-to-visit blood pressure variability as the hidden risk factor/predictor for coronary artery disease, stroke and malignant tumor in patients with type 2 diabetes. Heliyon. (2024) 10:e40406. doi: 10.1016/j.heliyon.2024.e40406
23. Wang, R, Wang, H, and Liu, S. Coronary heart disease increases the risk of perioperative ischemic stroke after noncardiac surgery: a retrospective cohort study. CNS Neurosci Ther. (2024) 30:e14912. doi: 10.1111/cns.14912
24. Liang, Z, Lou, Y, and Hao, Y. The relationship of astrocytes and microglia with different stages of ischemic stroke. Curr Neuropharmacol. (2023) 21:2465–80. doi: 10.2174/1570159X21666230718104634
25. Gong, Z, Guo, J, and Liu, B. Mechanisms of immune response and cell death in ischemic stroke and their regulation by natural compounds. Front Immunol. (2023) 14:1287857. doi: 10.3389/fimmu.2023.1287857
26. Alsbrook, DL, Di Napoli, M, and Bhatia, K. Neuroinflammation in acute ischemic and hemorrhagic stroke. Curr Neurol Neurosci Rep. (2023) 23:407–31. doi: 10.1007/s11910-023-01282-2
27. Xue, H, Zeng, Y, and Zou, X. Systemic immune inflammation index and risk of stroke: a cross-sectional study of the National Health and nutrition examination survey 2005-2018. Front Neurol. (2024) 15:1431727. doi: 10.3389/fneur.2024.1431727
28. Chen, J, Luo, C, and Tan, D. J-shaped associations of pan-immune-inflammation value and systemic inflammation response index with stroke among American adults with hypertension: evidence from NHANES 1999-2020. Front Neurol. (2024) 15:1417863. doi: 10.3389/fneur.2024.1417863
29. Fan, L, Zhang, CJ, and Zhu, L. FasL-PDPK1 pathway promotes the cytotoxicity of CD8+ T cells during ischemic stroke. Transl Stroke Res. (2020) 11:747–61. doi: 10.1007/s12975-019-00749-0
30. Cai, W, Shi, L, and Zhao, J. Neuroprotection against ischemic stroke requires a specific class of early responder T cells in mice. J Clin Invest. (2022) 132:e157678. doi: 10.1172/JCI157678
31. Ren, X, Akiyoshi, K, and Dziennis, S. Regulatory B cells limit CNS inflammation and neurologic deficits in murine experimental stroke. J Neurosci Off J Soc Neurosci. (2011) 31:8556–63. doi: 10.1523/JNEUROSCI.1623-11.2011
32. Ma, L, Shen, X, and Gao, Y. Blocking B7-1/CD28 pathway diminished long-range brain damage by regulating the immune and inflammatory responses in a mouse model of intracerebral hemorrhage. Neurochem Res. (2016) 41:1673–83. doi: 10.1007/s11064-016-1883-3
33. Lv, M, Su, C, and Huang, F. Combined impact of elevated C-reactive protein levels and dyslipidemia on stroke: a CHNS prospective cohort study. Front Public Health. (2024) 12:1435004. doi: 10.3389/fpubh.2024.1435004
34. Di Napoli, M, Godoy, DA, and Campi, V. C-reactive protein in intracerebral hemorrhage: time course, tissue localization, and prognosis. Neurology. (2012) 79:690–9. doi: 10.1212/WNL.0b013e318264e3be
35. Jiang, S, Zhang, X, and Song, C. Joint association of METS-IR and uric acid with stoke, mediated by C-reactive protein. Front Endocrinol. (2024) 15:1448021. doi: 10.3389/fendo.2024.1448021
36. McCabe, JJ, Walsh, C, and Gorey, S. Interleukin-6, C-reactive protein, and recurrence after stroke: a time-course analysis of individual-participant data. Stroke. (2024) 55:2825–34. doi: 10.1161/STROKEAHA.124.047820
37. Xu, WH, Dong, C, and Rundek, T. Serum albumin levels are associated with cardioembolic and cryptogenic ischemic strokes: northern Manhattan study. Stroke. (2014) 45:973–8. doi: 10.1161/STROKEAHA.113.003835
38. Zhou, H, Wang, A, and Meng, X. Low serum albumin levels predict poor outcome in patients with acute ischaemic stroke or transient ischaemic attack. Stroke Vascul Neurol. (2021) 6:458–66. doi: 10.1136/svn-2020-000676
39. Morotti, A, Marini, S, and Lena, UK. Significance of admission hypoalbuminemia in acute intracerebral hemorrhage. J Neurol. (2017) 264:905–11. doi: 10.1007/s00415-017-8451-x
40. Nam, KW, Han, JH, and Kim, CK. High glycated albumin is associated with early neurological deterioration in patients with acute ischemic stroke. BMC Neurol. (2024) 24:278. doi: 10.1186/s12883-024-03747-4
41. Pan, S, Du, K, and Liu, S. Albumin adjuvant therapy for acute ischemic stroke with large vessel occlusion (AMASS-LVO): rationale, design, and protocol for a phase 1, open-label, clinical trial. Front Neurol. (2024) 15:1455388. doi: 10.3389/fneur.2024.1455388
Keywords: stroke, C-reactive protein-albumin-lymphocyte index, NHANES, inflammation, CALLY index
Citation: Chen Y, Liu M, Zhang Y, Yang X, Yue M, Chen X, Wang H, Wang Z, Yu H and Shi J (2025) Association between C-reactive protein-albumin-lymphocyte index and stroke: an NHANES analysis (1999–2010). Front. Neurol. 16:1548666. doi: 10.3389/fneur.2025.1548666
Edited by:
Guanghua Zhai, Nanjing Medical University, ChinaReviewed by:
Aditya Yashwant Sarode, Columbia University, United StatesCopyright © 2025 Chen, Liu, Zhang, Yang, Yue, Chen, Wang, Wang, Yu and Shi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jing Shi, MjY2MjgzMTI5MUBxcS5jb20=
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.