 Chen Chen
Chen Chen Ziwei Hou2†
Ziwei Hou2†
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Neurol. , 02 April 2025
Sec. Stroke
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1537895
This article is part of the Research Topic Reviews in Preventative Health for Stroke and Education to Stroke Prevention View all 6 articles
In 2016, doctors in China proposed the Chinese version of FAST, called Stroke 120, to improve stroke identification and response in the Chinese population. And we modified Stroke 120 by adding “3” and “6” which aimed to reduce the prehospital delays and improve the prognosis of patients with stroke.
Stroke is the leading cause of disability and death worldwide, and the incidence of stroke is higher in China than in most other countries (1). In 2007, American scholars proposed the Facial drooping, Arm weakness, Speech difficulties and Time to call emergency services (FAST) stroke educational tool (2). In 2016, doctors in China proposed the Chinese version of FAST, called Stroke 120, to improve stroke identification and response in the Chinese population (3).
The meaning of Stroke 120 is as follows: number 1 represents “check whether the face is asymmetrical;” 2 represents “examine the two arms for weakness”; and 0 represents “(absence of) clear speech.” The detection rate of stroke by family doctors has increased by 12.5% in China (4). However, some shortcomings remain in this approach. First, “FAS” in FAST emphasizes the symptoms, “T” emphasizes time, and the word FAST itself again emphasizes immediate action. Although Stroke 120 emphasizes the symptoms and emergency helpline number, it ignores the important window for timely response. Furthermore, it seems that there are still many people who do not understand the meaning of “one face” and “two arms.”
Therefore, we modified Stroke 120 by adding “3” and “6.” Numbers 1 and 2 represent 1/2, emphasizing “paralysis or numbness of half the body;” and 0 still means “(absence of) clear speech.” However, three emphasizes the window for intravenous thrombolysis for cerebral infarction, i.e., 3 h, and 6 denotes the window for arterial thrombectomy for cerebral infarction i.e., 6 h (Figure 1). Finally, Stroke 12036 represents recognizing the symptoms and dialing 120 in 3 and 6 h.
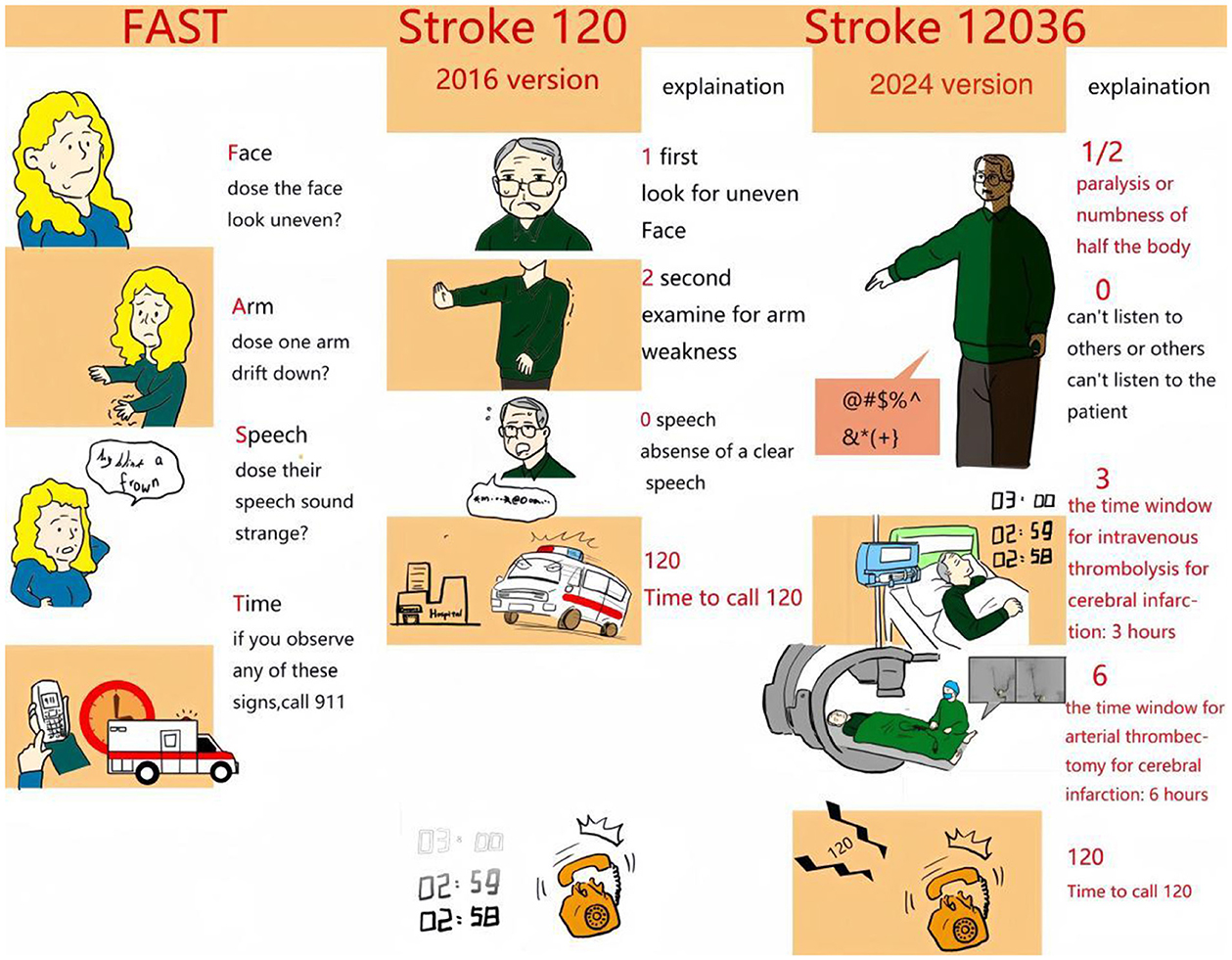
Figure 1. Stroke educational tool in USA and China. Left panel: FAST. Middle panel: Stroke 1-2-0. Right panel: Stroke 1-2-0-3-6. (In right panel, the differents from the previous version are shown in red).
Among these numbers, 120 is the emergency helpline number that Chinese people are familiar with; and 36 is a multiple of 12. Therefore, 12036 is easier to understand and remember than FAST. In addition to recognizing the symptoms by 120, there is a sense of urgency for 3 and 6 h. This tool was designed and released three times on Douyin account (the Chinese version of the video application TikTok). The video was played more than 400,000 times and shared nearly 20,000 times, indicating that the masses easily understood and accepted stroke 12036 (Figure 2).
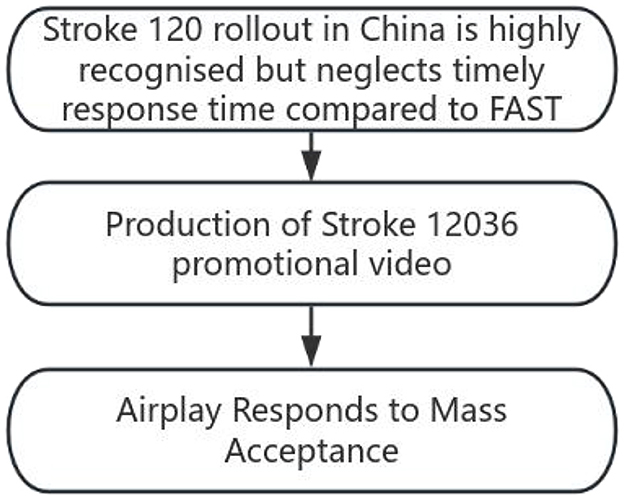
Figure 2. Study design flow chart.
We now plan to test this new strategy locally to establish a more suitable and final plan for China's family doctors and the general population. We aim to reduce the prehospital delays and improve the prognosis of patients with stroke (Figure 3).
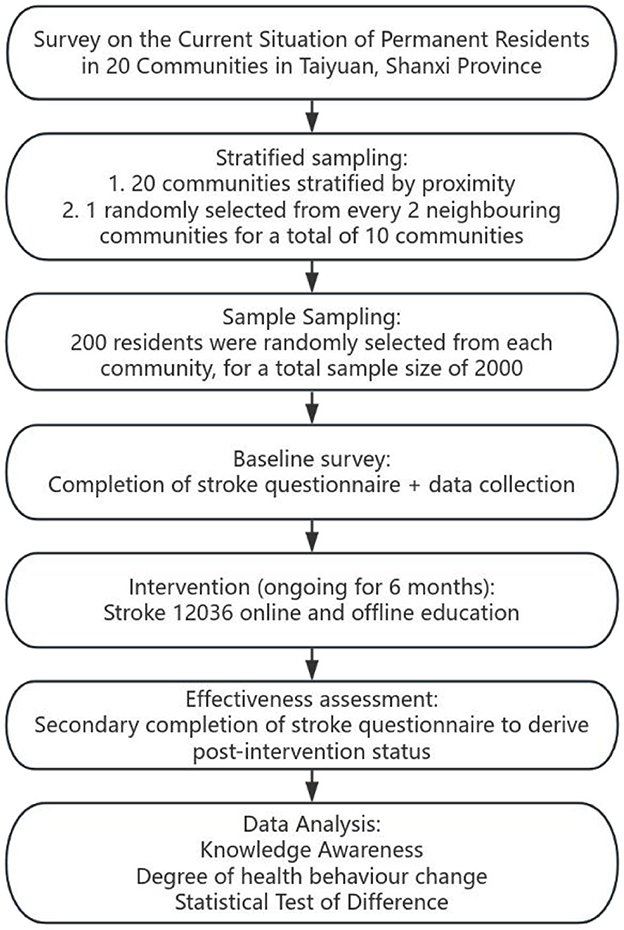
Figure 3. Flow chart of future research plans.
CC: Conceptualization, Writing – original draft. ZH: Writing – review & editing. LL: Writing – review & editing. RW: Writing – review & editing. HL: Writing – review & editing. HS: Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. This work was financially supported by Four Batches Innovation Project of Invigorating Medical through Science a Technology of Shanxi Province (2022XM07); Scientific Research Incentive Fund of Shanxi Cardiovascular Hospital (XYS20220107); Shanxi Province Chinese Medicine Science and Technology special research project (2024ZYY2A023).
We would like to thank Editage (https://www.editage.cn/) for English language editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Nguyen TN, Abdalkader M, Fischer U, Qiu Z, Nagel S, Chen HS, et al. Endovascular management of acute stroke. Lancet. (2024) 404:1265–78. doi: 10.1016/S0140-6736(24)01410-7
2. Özdemir Z, Acar E. YouTube as a source of recognizing acute stroke; progress in 2 years. BMC Public Health. (2024) 24:2208. doi: 10.1186/s12889-024-19710-4
3. Zhao J, Li X, Liu X, Xu Y, Xu J, Xu A, et al. Changing the strategy and culture of stroke awareness education in China: implementing Stroke 1-2-0. Stroke Vasc Neurol. (2020) 5:374–80:374–80. doi: 10.1136/svn-2019-000324
Keywords: stroke, 1-2-0-3-6, rapid identification, timely action, China
Citation: Chen C, Hou Z, Li L, Wang R, Liu H and Shen H (2025) Stroke 1-2-0-3-6: rapid identification and timely action for stroke in China. Front. Neurol. 16:1537895. doi: 10.3389/fneur.2025.1537895
Received: 02 December 2024; Accepted: 17 March 2025;
Published: 02 April 2025.
Edited by:
Patricia Pia Wadowski, Medical University of Vienna, AustriaReviewed by:
Vikas Bhatia, Post Graduate Institute of Medical Education and Research (PGIMER), IndiaCopyright © 2025 Chen, Hou, Li, Wang, Liu and Shen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chen Chen, MTM5MzQxNjE4NzBAMTYzLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.