
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 01 April 2025
Sec. Stroke
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1524262
 Wouter M. Sluis1*
Wouter M. Sluis1* Simone M. Uniken Venema2
Simone M. Uniken Venema2 Anouk van der Hoorn3
Anouk van der Hoorn3 Joseph C. J. Bot4
Joseph C. J. Bot4 Wim H. van Zwam5
Wim H. van Zwam5 Jeannette Hofmeijer6,7
Jeannette Hofmeijer6,7 H. Bart van der Worp1 on behalf of the MR CLEAN Registry Investigators
H. Bart van der Worp1 on behalf of the MR CLEAN Registry InvestigatorsBackground: Coma in the first hours after anterior circulation ischemic stroke is rare. We aimed to assess the causes of coma and outcomes after endovascular thrombectomy (EVT) in this relatively unexplored subgroup of patients.
Materials and methods: We used data from the MR CLEAN Registry, a prospective, multicenter, observational cohort study of patients treated with EVT in the Netherlands between March 2014, and December 2018. We included patients with anterior circulation ischemic stroke treated within 6.5 h of symptom onset and assessed frequency and causes of coma, defined as a score of 8 or lower on the Glasgow Coma Scale. Patients with a posterior circulation stroke were excluded. The primary outcome was the score on the modified Rankin Scale at 90 days. We compared outcomes of comatose and non-comatose patients with logistic regression.
Results: Fifty-two (1%) of 4,869 patients were comatose. The main causes of coma were bilateral ischemia, a post-ictal state after an epileptic seizure, and respiratory insufficiency. Comatose patients were less likely to receive intravenous thrombolysis (54% vs. 73%; p = 0.004) and onset-to-groin times were longer (226 vs. 199 min; p = 0.012). Patients with coma had poorer functional outcomes (adjusted common odds ratio (OR), 2.73; 95%CI: 1.45–5.13) and more frequently died within 90 days (adjusted OR, 2.95; 95%CI: 1.47–5.90).
Conclusion: Bilateral ischemia, a post-ictal state after an epileptic seizure and respiratory insufficiency are common causes of coma in patients with anterior circulation ischemic stroke treated with EVT. These patients have a high risk of death or dependency at 90 days.
About one fifth of patients with acute ischemic stroke caused by a proximal arterial occlusion in the anterior circulation has a reduced consciousness on admission in the first 6 h of stroke onset (1), but coma, defined as a score on the Glasgow Coma Scale (GCS) of 8 or lower (2), is rare (3). In the first hours of anterior circulation ischemic stroke, coma may be caused by simultaneous involvement of both hemispheres, or by new ischemia in the hemisphere contralateral to a large previous hemispheric lesion. In about one third of the patients no underlying cause is found (3, 4). Coma could also be caused by stroke-induced epileptic seizures or by other causes than the stroke itself, such as hypoglycaemia or severe arterial hypotension (5).
Coma is not a contraindication to endovascular thrombectomy (EVT) in patients with anterior circulation ischemic stroke due to a large vessel occlusion (LVO) (6, 7), but the frequency of this condition and the outcomes after EVT are unknown. We therefore aimed to assess the frequency of coma in patients with ischemic stroke caused by a proximal occlusion in the anterior circulation, the causes of such coma, and the outcomes after EVT.
We used data from the Multicenter Randomized Controlled Trial of Endovascular Treatment for Acute Ischemic Stroke in the Netherlands (MR CLEAN) Registry - a prospective, multicenter, observational study of patients with acute ischemic stroke treated with EVT in routine clinical practice in the Netherlands in 17 centers (8). The current study is based on data from patients included in the Registry between March 16, 2014, and December 31, 2018. Inclusion criteria for the present analysis were: age ≥ 18 years; a clinical diagnosis of acute ischemic stroke with a proximal arterial occlusion in the anterior circulation (internal carotid artery, middle cerebral artery [M1 and M2], or anterior cerebral artery [A1 and A2]), demonstrated with computed tomography angiography, magnetic resonance angiography, or digital subtraction angiography; and EVT initiated within 6.5 h of symptom onset or last seen well. We adhered to the RECORD guidelines (9). The checklist is attached as a Supplementary Table S1. The study protocol of the MR CLEAN Registry was reviewed by the Erasmus University Medical Center Ethics Committee, which served as the central review board for all participating centers. The requirement for written informed consent was waived. Patients or their representatives were provided with information on the study orally and in writing and were given the opportunity to refuse participation.
Local investigators collected clinical and demographic data from patient records and assessed the score on the modified Rankin Scale (mRS) at 90 days (+/− 14 days).
Baseline imaging characteristics, including occlusion site, the Alberta Stroke Program Early CT Score (ASPECTS), and collateral status (10, 11), the extended treatment in cerebral infarction (eTICI) score after EVT (12), and follow-up imaging were assessed by the MR CLEAN Registry imaging core laboratory, blinded to clinical findings. Complications after treatment were assessed by a central serious adverse events adjudication committee, and included recurrent ischemic stroke, pneumonia, symptomatic intracranial hemorrhage (sICH, defined according to the Heidelberg Bleeding Classification) (13), and stroke progression (defined as neurological deterioration with an increase of ≥4 points on the NIHSS and follow-up imaging compatible with ischemia in the same territory without another underlying cause of deterioration). If no follow-up imaging was performed this was defined as neurological deterioration with an unknown cause.
As the GCS was not routinely collected in the Registry, written clinical information was evaluated for the GCS for all patients with a baseline score of 2 or higher on the level of consciousness question (item 1a) of the NIHSS. Patients were classified as comatose if the score on GCS derived from the written clinical information was 8 or lower. When patients were intubated and sedated for another reason (e.g., respiratory insufficiency due to a non-neurological cause), they were not counted as comatose if the GCS before intubation was known and above 8. If a pre-intubation GCS was not available, these patients were not considered comatose. The written clinical information of comatose patients was used to determine causes of coma.
The primary outcome measure was the score on the mRS at 90 (± 14) days. Secondary outcome measures were mortality at 90 days and futile recanalization, defined as functional dependence or death (mRS score, ≥ 3) at 90 days despite successful recanalization (eTICI ≥2b) at the end of EVT.
The frequency and causes of coma are described with descriptive statistics. Comparisons between baseline characteristics of patients who were comatose and those who were not were made with χ2, Student’s t or Mann–Whitney U test, where appropriate. We used multivariable (ordinal) logistic regression to calculate adjusted (common) odds ratios (a(c)OR) for all outcomes and adjusted for age, pre-stroke score on the mRS, NIHSS at baseline, onset-to-groin time, history of diabetes, history of atrial fibrillation, and treatment with intravenous thrombolysis. For the multivariable regression analyses, multiple imputation was performed for predictor values with missing data. A sensitivity analysis was performed without using multiple imputation for missing data. Statistical significance was defined as a p value <0.05. All statistical analyses were performed with R studio version 1.3.1056. (Rstudio PBC).
A total of 4,869 patients were included in this analysis (Supplementary Figure S1). Fifty-two (1%) patients were comatose before EVT. In 20 patients (39%) the cause of coma was a radiologically apparent bilateral ischemic lesion. Twelve patients had acute ischemic stroke in the presence of a previous cortical ischemic stroke in the contralateral hemisphere and eight had acute bilateral ischemic stroke, of whom six had a bilateral large vessel occlusion (LVO). Only one patient with a bilateral LVO was treated with EVT on both sides, which was only successful for one side. Of the remaining comatose patients, nine (17%) were respiratory insufficient, five (10%) were in a post-ictal state after a seizure, two (4%) were hypotensive due to cardiogenic shock, and the other patients were either hypothermic (1 patient, 2%), intoxicated with alcohol (1 patient, 2%), post-anoxic after cardiac arrest (1 patient, 2%) or in septic shock (1 patient, 2%). In twelve patients (23%) no clear cause of coma could be determined. Six of these patients eventually died of space-occupying edema, which was not visible on non-contrast CT before EVT. None of these patients was treated with decompressive surgery.
Patients who were comatose were comparable to non-comatose patients with respect to age, sex, medication, and comorbidities but were more frequently functionally dependent before the stroke (33% vs. 13%, p < 0.001), had a higher NIHSS (25 vs. 15, p < 0.001), more often a stroke of the left hemisphere (75% vs. 53%, p = 0.002), or a carotid-T occlusion [internal carotid artery (ICA) + middle cerebral artery (MCA), 39% vs. 19% (p = 0.001)]. Fewer comatose patients were given IVT (54% vs. 73%, p = 0.003) and they had worse ASPECTS and collateral scores (Table 1). Two comatose patients (3.8%) had a very low ASPECTS score (0 through 2), which was slightly higher than the group of patients without coma (n = 51, 1.1%).
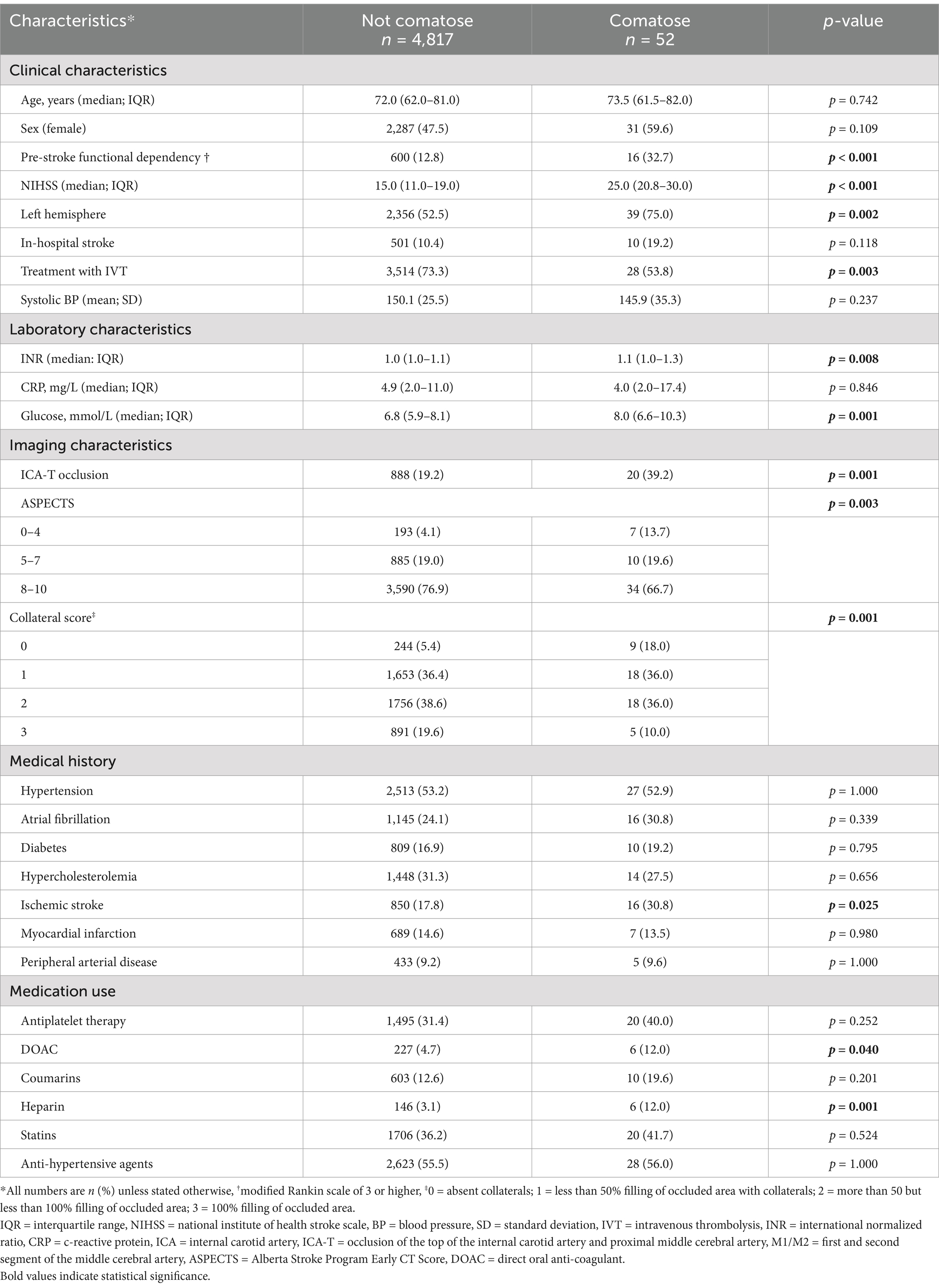
Table 1. Baseline characteristics of patients with or without coma at hospital admission.
Onset-to-groin times were longer for comatose patients (225 vs. 199 min, p = 0.012) and treatment was more often performed under general anesthesia (61% vs. 23% p < 0.001). The NIHSS at 24 to 48 h was higher in the comatose group (21 vs. 9, p < 0.001) and comatose patients were more often diagnosed with stroke progression (19% vs. 9%, p = 0.015) (Tables 2, 3).
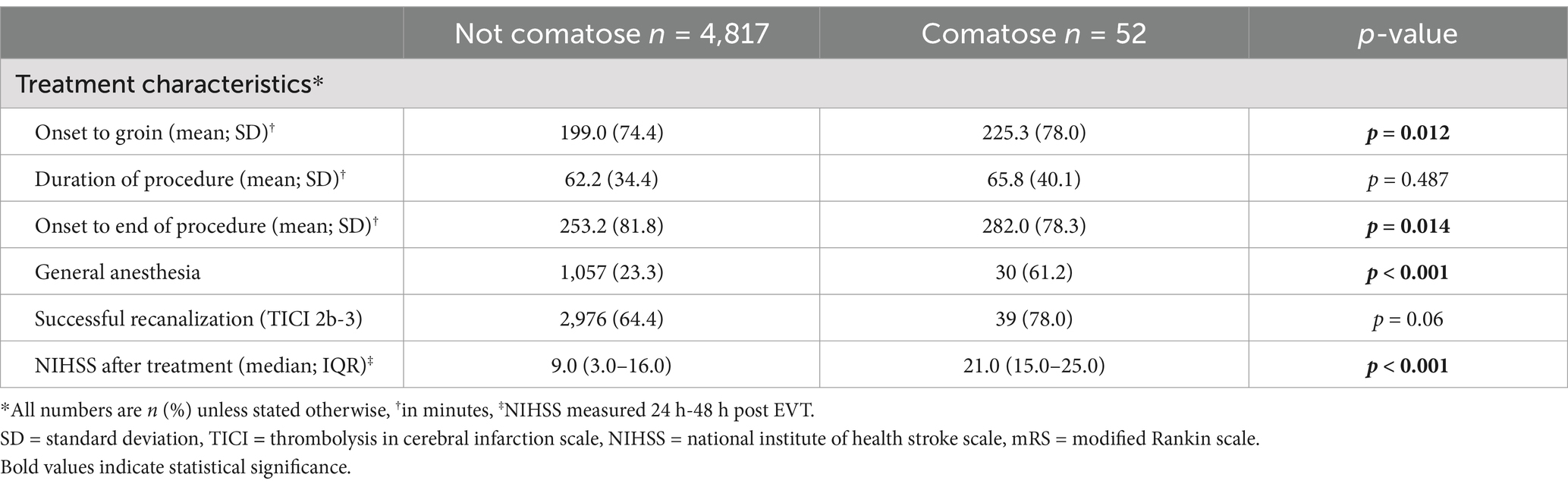
Table 2. Treatment characteristics and complications of comatose and non-comatose patients.
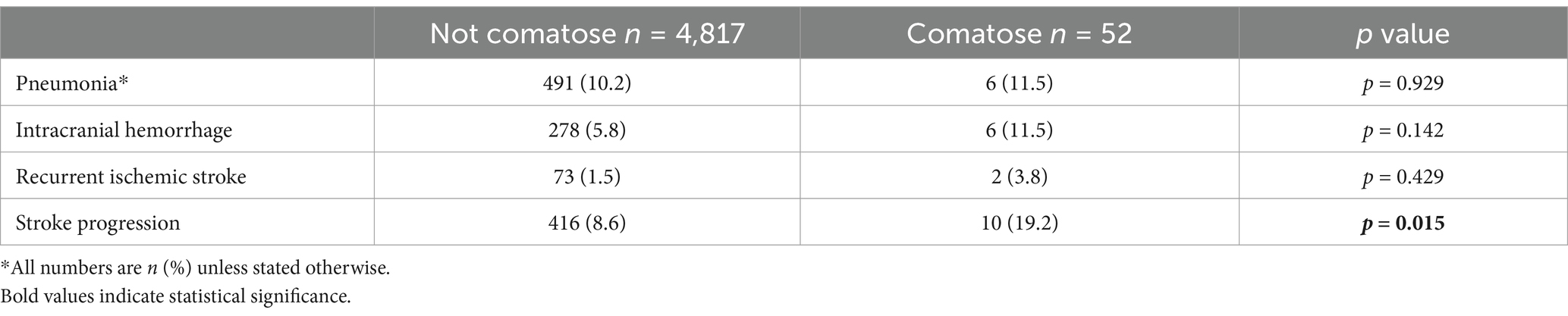
Table 3. Complications in comatose and non-comatose patients.
After adjustment for confounders, comatose patients died more often within 90 days (69% vs. 26%; aOR 2.95; 95%CI:1.47–5.90; Tables 1, 4; Figure 1), with a median time to death of 3 days (IQR 2–7).
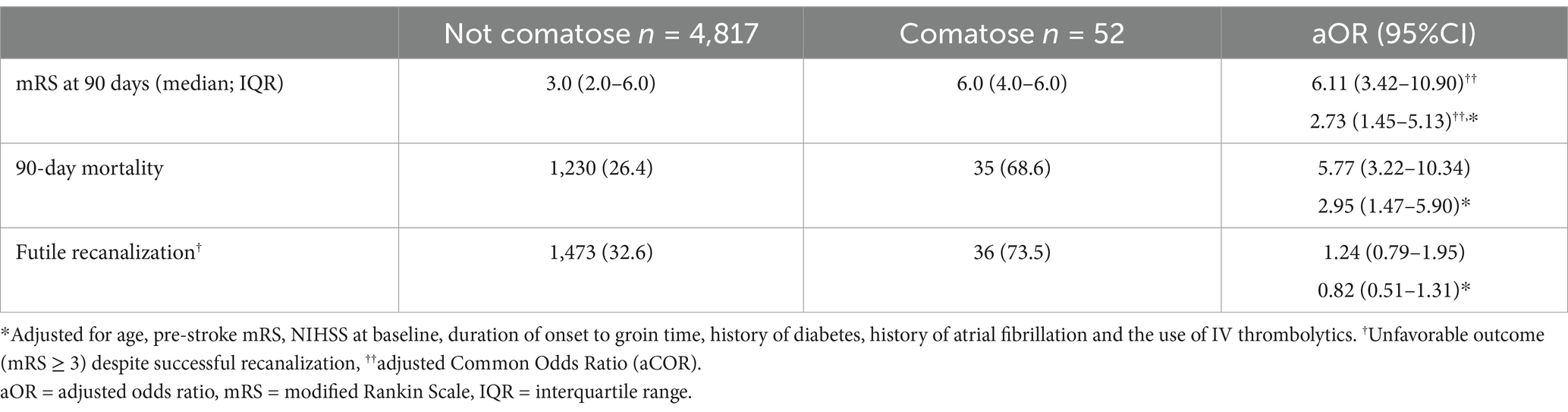
Table 4. Outcome measures in comatose and non-comatose patients.
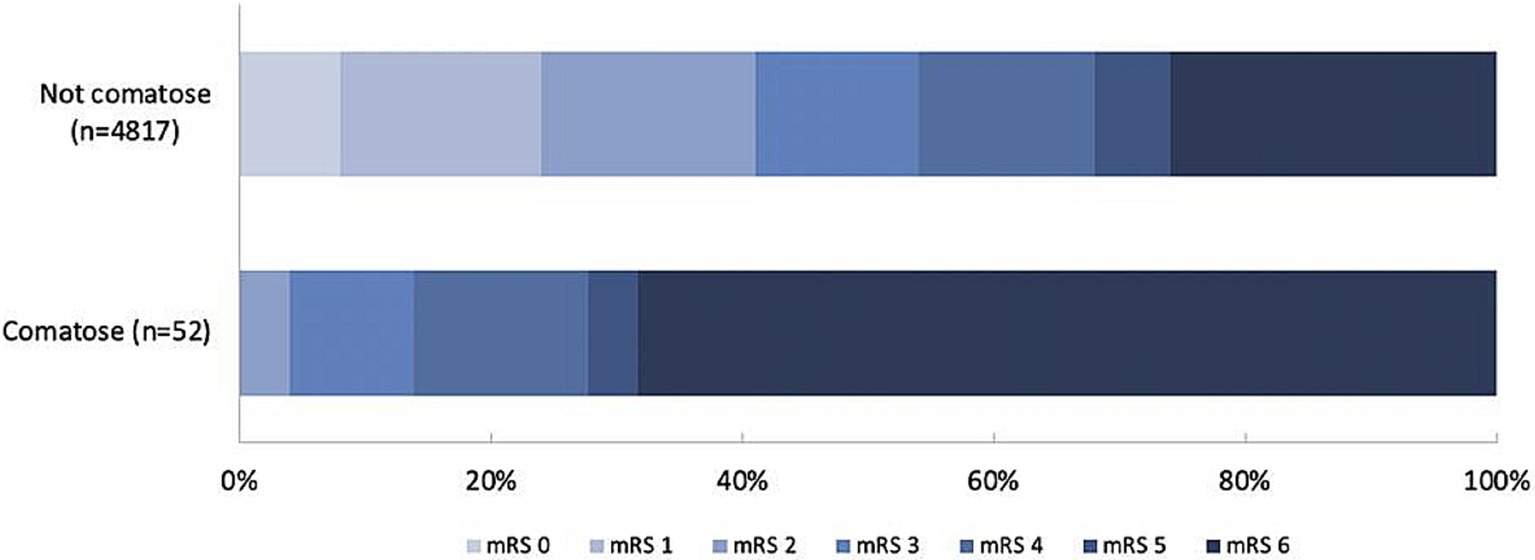
Figure 1. 90-day mRS of patients with or without coma. mRS = modified Rankin Scale.
Mortality was highest in comatose patients with a bilateral ischemic lesion (70%) or a non-neurological cause of coma (71%) and lowest in the post-ictal patients (40%). Comatose patients had a worse functional outcome at 90 days (acOR for a shift on the mRS towards a worse functional outcome: 2.73; 95%CI: 1.45–5.13; Table 4; Figure 1) and just two patients (4%) were functionally independent at 90 days: one patient in a post-ictal state after a seizure and one with an unknown cause of coma. Recanalization was futile in 74% of comatose patients. The sensitivity analysis without imputed data yielded similar results (Supplementary Table S2).
In this study, patients with ischemic stroke caused by a proximal occlusion in the anterior circulation who were comatose within 6.5 h of stroke onset had a very high risk of death or dependency at 90 days after EVT, even with angiographic recanalization. The most frequent cause of coma was an ischemic lesion in the hemisphere contralateral to the occlusion.
Acute bilateral large vessel occlusion occurs in less than 1% of patients with ischemic stroke. The prognosis is generally poor, as was the case in our six patients (4). For unknown reasons, only one of them was treated on both sides and recanalization only occurred on one side. We therefore do not know whether outcomes would have been better if patients with bilateral occlusions had bilateral recanalization. Contralateral recurrent stroke occurred in 7% of patients in The Copenhagen Stroke Study and was also associated with a worse functional outcome compared to ipsilateral recurrence (14).
Most patients with a systemic non-neurological cause of coma had signs of severe metabolic, respiratory or hemodynamic dysregulation. Hypotension, hypoxia, and infections after stroke have been associated with a worse prognosis (15–17). In about one quarter of comatose patients, no cause of reduced consciousness was identified, which is comparable to a previous study in which no cause of coma was found (3). Remarkably, in our study more than half of the patients with coma of unidentified cause died of space-occupying edema in the next days, without signs of mass effect on non-contrast CT before EVT, none of the patients in our study were treated with decompressive surgery, as opposed to around 40% in a previous MR CLEAN study (18). With the exception of one patient, all these patients primarily presented to the intervention center, so most imaging was directly prior to EVT. Space-occupying edema is a well-known cause of coma in patients with unilateral anterior circulation stroke, but clear clinical signs of mass effect generally occur after the first few hours, and only in one third of the cases within 24 h (19, 20). In a study of patients with middle cerebral artery infarction caused by an M1 occlusion, 15 of the 24 patients (63%) who eventually developed ‘malignant’ space-occupying edema had a reduced level of consciousness in the first 6 hours of stroke onset, but the proportion of patients with coma in this study is not known (21).
The finding that comatose patients were less frequently treated with IVT and had longer door-to-groin times could suggest that treating physicians are hesitant to treat comatose patients, possibly due to a lack of evidence on the efficacy of reperfusion therapy in this subgroup of patients. Another explanation could be a greater diagnostic delay, and therefore missing the time window for treatment with IVT, or suspected comorbidity with a suspected increased risk hemorrhage. In a study on IVT in patients with ischemic stroke and a decreased consciousness, IVT seemed beneficial, but this study was just as the present study not randomized and retrospective in design, possibly causing selection bias (22).
The current study is the first to report causes of coma and outcomes of EVT in patients with anterior circulation ischemic stroke, but there are limitations to consider. First, this is a retrospective analysis in a prospective registry of patients who were treated with EVT. We therefore cannot provide information on comatose patients with anterior circulation ischemic stroke who were not treated with EVT, for example because they were considered by the clinician as too severe for curative treatment. Second, causes of coma were determined retrospectively based on written clinical information, which may be insufficient to accurately reflect the actual causes of coma. EEG was not routinely performed and the presence or absence of a fetal posterior communicating artery was not assessed. Third, the group of patients with coma was very small compared to the non-comatose group and therefore the uncertainty of our estimates is considerable. Fourth, patients included in the MR CLEAN Registry were treated early in the era of EVT. Since then, devices and skills have improved which could positively influence outcomes of comatose patients. Nevertheless, our data strongly suggest that the risk of a poor outcome after EVT is high in patients who are comatose on admission is, especially in patients with bilateral ischemic stroke. Further research is needed to assess the benefit of EVT in patients without a known cause of coma.
Patients with anterior circulation ischemic stroke who are comatose before endovascular thrombectomy in the first 6.5 h often have ischemic lesions in both hemispheres or an underlying metabolic or hemodynamic dysregulation as the cause of their decreased consciousness. These patients have a very poor prognosis despite successful EVT.
The data analyzed in this study is subject to the following licenses/restrictions: the dataset can be obtained upon reasonable request via the MR CLEAN writing committee. Requests to access these datasets should be directed to https://www.mrclean-trial.org/.
The studies involving humans were approved by Erasmus University Medical Center Ethics Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because The study was an observational registry of a non-experimental treatment. Patients or their representatives were provided with information on the study orally and in writing and were given the opportunity to refuse participation.
A list of all MR CLEAN Registry Investigators is provided in the Supplementary material.
WS: Conceptualization, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. SU: Formal analysis, Writing – review & editing. AH: Writing – review & editing. JB: Writing – review & editing. WZ: Writing – review & editing. JH: Writing – review & editing. HW: Supervision, Writing – review & editing.
The author(s) declare that financial support was received for the research and/or publication of this article. The MR CLEAN Registry was partly funded by the Toegepast Wetenschappelijk Instituut voor Neuromodulatie Foundation, Erasmus MC Medical Center, Maastricht University Medical Center, and Academic Medical Center Amsterdam.
We would like to thank all the MR CLEAN Registry investigators.
WMS is supported by the European Union’s Horizon 2020 research and innovation program (634809). HBvdW reports having received grants from the European Union, the Dutch Heart Foundation, and Stryker for research, and funding for consultancy from Bayer and TargED, all paid to his institution.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1524262/full#supplementary-material
GCS, Glasgow coma scale; EVT, Endovascular treatment; LVO, Large vessel occlusion; MR CLEAN, Multicenter randomized controlled trial of endovascular treatment for acute ischemic stroke in the Netherlands; ASPECTS, Alberta stroke program early CT score; eTICI, Extended treatment in cerebral infarction; ICH, Intracerebral hemorrhage; sICH, Symptomatic ICH; NIHSS, National institute of health stroke scale; mRS, Modified Rankin scale; IVT, intravenous thrombolysis.
1. Janssen, PM, Chalos, V, van den Berg, SA, Kompanje, EJO, Nederkoorn, PJ, van der Worp, BH, et al. Neurological deficits in stroke patients that may impede the capacity to provide informed consent for endovascular treatment trials. J Stroke Cerebrovasc Dis. (2019) 28:104447. doi: 10.1016/j.jstrokecerebrovasdis.2019.104447
2. Jennett, B, and Teasdale, G. Aspects of coma after severe head injury. Lancet. (1977) 1:878–81. doi: 10.1016/S0140-6736(77)91201-6
3. Young, MJ, Awad, A, Andreev, A, Bonkhoff, AK, Schirmer, MD, Dmytriw, AA, et al. Characterizing coma in large vessel occlusion stroke. J Neurol. (2024) 271:2658–61. doi: 10.1007/s00415-024-12199-2
4. Kwon, SU, Lee, SH, and Kim, JS. Sudden coma from acute bilateral internal carotid artery territory infarction. Neurology. (2002) 58:1846–9. doi: 10.1212/WNL.58.12.1846
5. Horsting, MW, Franken, MD, Meulenbelt, J, van Klei, WA, and de Lange, DW. The etiology and outcome of non-traumatic coma in critical care: a systematic review. BMC Anesthesiol. (2015) 15:65. doi: 10.1186/s12871-015-0041-9
6. Turc, G, Bhogal, P, Fischer, U, Khatri, P, Lobotesis, K, Mazighi, M, et al. European stroke organisation (ESO) - European Society for Minimally Invasive Neurological Therapy (ESMINT) guidelines on mechanical Thrombectomy in acute Ischaemic StrokeEndorsed by stroke Alliance for Europe (SAFE). Eur Stroke J. (2019) 4:6–12. doi: 10.1177/2396987319832140
7. Powers, WJ, Rabinstein, AA, Ackerson, T, Adeoye, OM, Bambakidis, NC, Becker, K, et al. Guidelines for the early Management of Patients with Acute Ischemic Stroke: 2019 update to the 2018 guidelines for the early Management of Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2019) 50:e344–418. doi: 10.1161/STR.0000000000000211
8. Jansen, IGH, Mulder, MJHL, and Goldhoorn, RB. MR CLEAN registry investigators. Endovascular treatment for acute ischaemic stroke in routine clinical practice: prospective, observational cohort study (MR CLEAN registry). BMJ. (2018) 360:k949. doi: 10.1136/bmj.k949
9. Benchimol, EI, Smeeth, L, Guttmann, A, Harron, K, Moher, D, Petersen, I, et al. The REporting of studies conducted using observational routinely-collected health data (RECORD) statement. PLoS Med. (2015) 12:e1001885. doi: 10.1371/journal.pmed.1001885
10. Barber, PA, Demchuk, AM, Zhang, J, and Buchan, AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS study group. Alberta stroke Programme early CT score. Lancet. (2000) 355:1670–4. doi: 10.1016/S0140-6736(00)02237-6
11. Tan, JC, Dillon, WP, Liu, S, Adler, F, Smith, WS, and Wintermark, M. Systematic comparison of perfusion-CT and CT-angiography in acute stroke patients. Ann Neurol. (2007) 61:533–43. doi: 10.1002/ana.21130
12. Liebeskind, DS, Bracard, S, Guillemin, F, Jahan, R, Jovin, TG, Majoie, CBLM, et al. eTICI reperfusion: defining success in endovascular stroke therapy. J Neurointerv Surg. (2019) 11:433–8. doi: 10.1136/neurintsurg-2018-014127
13. von Kummer, R, Broderick, JP, Campbell, BC, Demchuk, A, Goyal, M, Hill, MD, et al. The Heidelberg bleeding classification: classification of bleeding events after ischemic stroke and reperfusion therapy. Stroke. (2015) 46:2981–6. doi: 10.1161/STROKEAHA.115.010049
14. Jerrgensen, HS, Nakayama, H, Reith, J, Raaschou, O, and Olsen, TS. Stroke recurrence: predictors, severity and prognosis. The Copenhagen Stroke Study. Neurology. (1997) 48:891–5. doi: 10.1212/WNL.48.4.891
15. Verschoof, MA, Groot, AE, Vermeij, JD, Westendorp, WF, van den Berg, SA, Nederkoorn, PJ, et al. Association between low blood pressure and clinical outcomes in patients with acute ischemic stroke. Stroke. (2020) 51:338–41. doi: 10.1161/STROKEAHA.119.027336
16. Rowat, AM, Dennis, MS, and Wardlaw, JM. Hypoxemia in acute stroke is frequent and worsens outcome. Cerebrovasc Dis. (2006) 21:166–72. doi: 10.1159/000090528
17. Westendorp, WF, Nederkoorn, PJ, Vermeij, JD, Dijkgraaf, MG, and van de Beek, D. Post-stroke infection: a systematic review and meta-analysis. BMC Neurol. (2011) 11:110. doi: 10.1186/1471-2377-11-110
18. Bernsen, MLE, Kauw, F, Martens, JM, van der Lugt, A, Yo, LS, van Walderveen, MA, et al. Malignant infarction after endovascular treatment: incidence and prediction. Int J Stroke. (2022) 17:198–206. doi: 10.1177/17474930211006290
19. Qureshi, AI, Suarez, JI, Yahia, AM, Mohammad, Y, Uzun, G, Suri, M, et al. Timing of neurologic deterioration in massive middle cerebral artery infarction: a multicenter review. Crit Care Med. (2003) 31:272–7. doi: 10.1097/00003246-200301000-00043
20. Hacke, W, Schwab, S, Horn, M, Spranger, M, De Georgia, M, and von Kummer, R. “Malignant” middle cerebral artery territory infarction: clinical course and prognostic signs. Arch Neurol. (1996) 53:309–15. doi: 10.1001/archneur.1996.00550040037012
21. Thomalla, G, Hartmann, F, Juettler, E, Singer, OC, Lehnhardt, F, Köhrmann, M, et al. Prediction of malignant middle cerebral artery infarction by magnetic resonance imaging within 6 hours of symptom onset: a prospective multicenter observational study. Ann Neurol. (2010) 68:435–45. doi: 10.1002/ana.22125
Keywords: stroke, MR CLEAN, coma, endovascular treatment (EVT), ischemic
Citation: Sluis WM, Uniken Venema SM, van der Hoorn A, Bot JCJ, van Zwam WH, Hofmeijer J and van der Worp HB (2025) Endovascular treatment in comatose patients with anterior circulation ischemic stroke. Front. Neurol. 16:1524262. doi: 10.3389/fneur.2025.1524262
Edited by:
João Pinho, University Hospital RWTH Aachen, GermanyReviewed by:
João Pedro Marto, Centro Hospitalar de Lisboa Ocidental, PortugalCopyright © 2025 Sluis, Uniken Venema, van der Hoorn, Bot, van Zwam, Hofmeijer and van der Worp. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Wouter M. Sluis, dy5tLnNsdWlzLTJAdW1jdXRyZWNodC5ubA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.