 Sarah Chételat1,2†Eve-Yaël Gerber2,3†
Sarah Chételat1,2†Eve-Yaël Gerber2,3† Sarah El Khadlaoui4
Sarah El Khadlaoui4 Frank Behrendt2,5*Michaela Stark1,2Stefan Schädler2,6
Frank Behrendt2,5*Michaela Stark1,2Stefan Schädler2,6 Maximilian Maywald7Lena Fabritius4
Maximilian Maywald7Lena Fabritius4 Johannes Gerb4,8Denis Grabova4Wiebke Trost2
Johannes Gerb4,8Denis Grabova4Wiebke Trost2 Andreas Zwergal4,8Ralf Strobl4,9Katrin Parmar2,10Hans Ulrich Gerth2,11Leo H. Bonati2,12,13
Andreas Zwergal4,8Ralf Strobl4,9Katrin Parmar2,10Hans Ulrich Gerth2,11Leo H. Bonati2,12,13 Sandra Becker-Bense4‡Corina Schuster-Amft2,5,14*‡
Sandra Becker-Bense4‡Corina Schuster-Amft2,5,14*‡- 1School of Health Professions, Institute of Physiotherapy, Zurich University of Applied Sciences, Winterthur, Switzerland
- 2Department of Research, Reha Rheinfelden, Rheinfelden, Switzerland
- 3Department of Psychology, University of Basel, Basel, Switzerland
- 4German Center for Vertigo and Balance Disorders (DSGZ), University Hospital, LMU Munich, Munich, Germany
- 5School of Engineering and Computer Science, Bern University of Applied Sciences, Biel, Switzerland
- 6Physiotherapie Stefan Schädler, Sumiswald, Switzerland
- 7Department of Psychiatry and Psychotherapy, University Hospital, LMU Munich, Munich, Germany
- 8Department of Neurology, University Hospital, LMU Munich, Munich, Germany
- 9Institute for Medical Information Processing, Biometry, and Epidemiology (IBE), LMU Munich, Munich, Germany
- 10Departments of Head, Spine and Neuromedicine and Biomedical Engineering, Translational Imaging in Neurology (ThINk) Basel, University Hospital Basel and University of Basel, Basel, Switzerland
- 11Department of Medicine, University Hospital Münster, Münster, Germany
- 12Department of Neurology, Stroke Center, University Hospital Basel, Basel, Switzerland
- 13Department of Clinical Research, University of Basel, Basel, Switzerland
- 14Department of Sport, Exercise and Health, University of Basel, Basel, Switzerland
Background: Persistent Postural-Perceptual Dizziness (PPPD) is a frequent chronic functional disorder that manifests with dizziness, unsteadiness, or non-spinning vertigo present for at least 3 months. Characteristic provocation factors are moving or complex visual stimuli and exclusion of organic diseases. To assess the severity and impact of PPPD, Japanese researchers developed the Niigata PPPD Questionnaire (NPQ). The study's aim was to evaluate the concurrent construct validity and reliability [including test-retest reliability, internal consistency, standard error of measurement (SEM), and minimal detectable change (MDC)] of the German version of the NPQ (12 items) and its revised version, NPQ-R, which contains 19 items addressing additional symptoms and symptom behavior.
Methods: The Swiss Reha Rheinfelden and the German Center for Vertigo and Balance Disorders included 265 PPPD patients (mean age 50.2 ± 16.8 years, disease duration 46.3 ± 76.6 months). Patients completed the NPQ and the NPQ-R (twice), the DHI and potentially related constructs: anxiety (ABC-Scale, VSS), depression (HADS), and general health (SF-36) once. To assess the questionnaires' reliability and validity, several statistical measures were calculated, including Spearman's rank correlation coefficients, Intraclass Correlation Coefficients (ICC2, 1), Cronbach's alpha, SEM, and MDC.
Results: On average, patients scored 29.9 ± 13.2 for NPQ and 52.3 ± 19.6 for NPQ-R. Correlations between NPQ/NPQ-R and (1) disease-specific questionnaires were rs= 0.712 and rs= 0.752 (DHI), rs=0.426 and rs= 0.0.462 (VSS-V), rs= -0.500 and rs= -0.545 (ABC-Scale), (2) anxiety-specific subscales rs = 0.394 and rs = 0.430 (VSS-A) and rs= 0.354 and rs= 0.430 (HADS-A), (3) depression-related subscales rs=0.438 and rs= 0.487 (HADS-D), and (4) general health rs ranged between rs= -0.216 and −0.578 (all SF-36 subscales). Internal consistency, test-retest reliability, SEM and MDC calculated for NPQ/NPQ-R were α = 0.88/α = 0.91, ICC=0.83 (CI 0.77 to 0.0.87), SEM 5.55/8.37, and MDC 15/23 points.
Conclusion: The German versions of NPQ and NPQ-R are valid and reliable patient-reported outcome measures for assessing PPPD, demonstrating satisfactory psychometric measurement properties including convergent construct validity and reliability parameters: internal consistency, test-retest reliability, SEM, and MDC as an evaluative measure. The NPQ-R, with its additional subscales addressing associated symptoms and symptom behavior, represents both the patient and clinician perspective on PPPD-specific problems. Therefore, we recommend utilizing the NPQ-R for a comprehensive assessment of PPPD.
1 Background
Persistent Postural-Perceptual Dizziness (PPPD) is the current term for chronic vertigo and dizziness syndromes characterized by one or more vestibular symptoms, including vertigo, dizziness, unsteadiness, or imbalance in stance and gait, in the absence of an identifiable organic etiology (1, 2). Functional dizziness syndromes have been recognized since the latter half of the 19th century and are currently the most prevalent types of vestibular disorders in our society, particular within specialized vertigo centers (up to 20%) (1–3). However, it was not until 2017 that the committee for the International Classification of Vestibular Disorders (ICVD) of the Bárány Society, the International Society of Neurootology, developed the first consensus document defining functional vertigo and dizziness (Table 1). This document introduced the new term “Persistent Postural-Perceptual Dizziness” (PPPD) along with its classification criteria (1). PPPD can develop following an acute organic vestibular or non-vestibular disorder, resulting in secondary PPPD (sPPPD), or it can develop independently in the absence of somatic triggers, referred to as primary PPPD (pPPPD) (1, 4). Its core features are based on common findings in syndromes described earlier such as “phobic postural vertigo”, “space-motion discomfort”, “functional vertigo”, “visual vertigo”, or “chronic subjective dizziness” (1, 2).
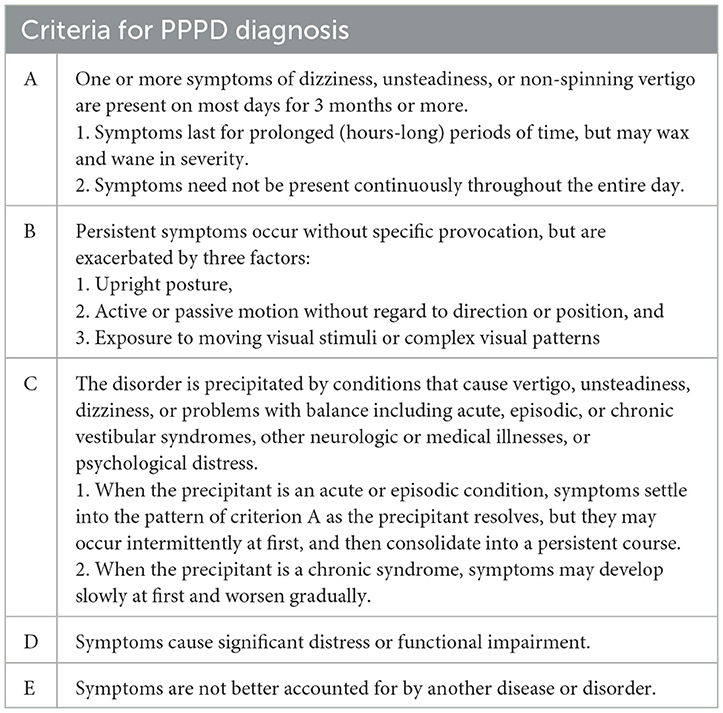
Table 1. Diagnosis criteria of persistent postural-perceptual dizziness (PPPD) from the committee for the Classification of Vestibular Disorders of the Bárány Society (according to Staab et al., (1), p. 196).
To date, there is no valid measurement instrument available in German-speaking countries for the assessment of PPPD-specific subjective patients' complaints and their severity (1, 5). The currently available patient reported outcome measurement tools, such as the Dizziness Handicap Inventory (DHI) or the Vertigo Symptom Scale (VSS), primarily address general dizziness issues. However, they do not adequately capture the specific complaints reported by patients with PPPD who do not exhibit an organic vestibular deficit. Such specific symptoms would particularly encompass the characteristic situational exacerbation factors associated with PPPD, including maintaining an upright posture, engaging in active or passive movement, and exposure to dynamic or complex stimuli (6, 7).
Based on the relatively new diagnostic criteria of the Bárány Society, Yagi and colleagues developed the first PPPD-specific patient-reported outcome measure in 2019: the Niigata PPPD Questionnaire in Japanese (NPQ) (8). The NPQ consists of 12 items divided into three subscales that evaluate the patient's dizziness complaints. The subscales focus on three typical PPPD provocation and/or amplication factors in PPPD: (1) being in an upright posture or while walking, (2) during movement, and (3) during visual stimulation. Twelve questions regarding these three reinforcing factors are evaluated using a Likert scale ranging from zero (no impact) to six (indicating unbearable impact), resulting in a total possible score of 72 points. In a retrospective study involving 50 patients with PPPD and 50 individuals with various vestibular syndromes, such as Menière's disease, Yagi and colleagues investigated the questionnaire's capacity to discriminate between the two patient groups (discriminate validity). It resulted in an initial valid and reliable patient-reported outcome measurement tool. The visual stimulation scale proved to be the most suitable for discrimination (8). However, the original NPQ exhibits some methodological flaws: (1) the items address only certain aspects of the diagnostic criteria, notably omitting considerations of psychosocial functioning impairment; (2) more attention could have been placed on scale's development and validation, particularly in accordance with the COSMIN guidelines that recommend the inclusion of both patient and expert perspectives during the development process of a patient-reported outcome measure focusing on content validity; and (3) a larger sample size for validation purposes is required (9).
Due to these shortcomings and to facilitate the accessibility of this measurement instrument in German-speaking countries, an official German translation of the NPQ was created including forward and backward translation by three officially recognized translators and the study team after consultation with the authors of the NPQ, based on existing guidelines (10). Additionally, the perspective from 28 health professionals specializing the field of dizziness and vertigo, as well as 11 patients diagnosed with PPPD, were included based on a three-round Delphi procedure and semi-structured interviews, respectively (11). The modified NPQ-R resulted in the addition of seven new items (now 19 items) and two new subscales (now five subscales). These modifications included additional questions addressing symptom behavior and psychosocial impairment associated with PPPD symptoms, such as difficulties with concentration. The NPQ-R now provides a comprehensive PROM for patients with PPPD-related symptoms that can comprehensively capture their symptoms. The process of expansion and all content-related details are described in Behrendt et al. (11). The German and the English versions of the NPQ and the NPQ-R are provided as Supplementary files 1–4. The evaluation scale remained the same Likert scale as in the original Japanese NPQ from zero (none) to six (6 = unbearable). The new NPQ-R total score can range from zero to 114 points.
The aim of the present study was to examine convergent construct validity and test-retest reliability of the German version of the Niigata PPPD Questionnaire (NPQ) and its revised version (NPQ-R) to support diagnostic procedures for PPPD and the monitoring of the treatment progress. We hypothesized a strong correlation r > 0.5 between the total scores of the NPQ/NPQ-R and the total scores of the DHI and VSS, as all three instruments assess vestibular disease-specific constructs.
2 Methods
2.1 Study design
This prospective study, comprising two measurement events, was designed to evaluate the internal consistency, test-retest reliability, standard error of measurement and convergent construct validity of the German NPQ and NPQ-R. The study was conducted in accordance with the Helsinki Declaration and received approval from the Ethics Committee Northwest and Central Switzerland (reference number: 2021-00974) as well as the Institutional Review Board of the Ludwig-Maximilians-University Munich Germany (reference number: 23-0126). All patients were provided with written and oral information about the project following the initial contact and were subsequently invited to participate in the study. Written informed consent was obtained from all participants prior to the start of data collection.
2.2 Participants
Patient inclusion criteria were diagnosis of PPPD, age > 18 years, good knowledge of German, and a signed informed consent. The exclusion criteria included the presence of other forms of vertigo.
In this bi-center study, patients from Switzerland and Germany were included. In Switzerland, outpatients were recruited from PPPD-specialists from the Oto-Rhino-Laryngology Clinics of the Cantonal Hospitals of Lucerne, the University Hospitals Zurich and Basel, the Reha Rheinfelden, and private practices. In Germany, all patients were recruited through the outpatient unit of the German Center for Vertigo and Balance Disorders (DSGZ) at the LMU University Hospital in Munich. PPPD diagnosis was confirmed according to the criteria established by the Bárány Society (1). The routine clinical assessment in all patients comprised a comprehensive clinical neurological, neuro-orthoptic, and neuro-otological examination, which encompassed procedures such as bithermal caloric irrigation and video head impulse test to evaluate both low- and high-frequency ranges of the vestibulo-ocular reflex. Neuro-orthoptic examination included detailed ocular motor examination, measurements of the subjective visual vertical and fundusphotography by use of a laser scanning opthalmoscope. The latter was especially important in order to exclude acute vestibular tone imbalance, e.g., spontaneous or head shaking nystagmus, skew deviation, head tilt, tilts of the subjective visual vertical or cyclorotation of the eyes (ocular torsion) as parts of the so-called ocular tilt reaction (12, 13). If useful, additional examinations such as static posturography, gait analysis, pure tone audiometry, or vestibular-evoked myogenic potentials were performed in a standardized manner. Patients with secondary PPPD with a residual unilateral peripheral deficit in the high- and/or low frequency range of the vestibulo-ocular reflex following a preceding acute unilateral vestibulopathy were included in the study only if this deficit was completely compensated centrally. Specifically, this meant that patients demonstrated no signs of acute vestibular tone imbalance and exhibited no vestibular sway patterns during static posturography. Additionally, the German patients were classified as either primary (p) or secondary sPPPD depending on the presence or absence of a confirmed preceding somatic trigger.
2.3 Measures
The NPQ and NPQ-R are utilized to assess the patient's subjective perception of severity, impairments, and limitations due to PPPD, thereby functioning as evaluative instruments (11). To assess the construct validity of the German versions of NPQ and NPQ-R, patients were asked to complete the following five patient-reported outcome measures:
1) The Dizziness Handicap Inventory (DHI) is a disease specific questionnaire assessing the impact of dizziness including 25 items within three subscales: physical, emotional and functional (14). The DHI evaluates items on an ordinal scale, which consists of the response options “yes” (four points), “sometimes” (two points) or “no” (zero points). The total score ranges from zero to 100, with the expression from “no disability” to “strongest perceived disability”. Overall, the German version of the DHI shows moderate to good psychometric properties (α = 0.90, ICC2/1 = 0.95 (CI 0.91, 0.98), concurrent validity: r = −0.53 to −0.72 with the SF-36, r = −0.64 with Activities-specific Balance Confidence (ABC) Scale, r = 0.41 with Hospital Anxiety and Depression Scale, subscale anxiety (HADS-A), r = 0.66 with Hospital Anxiety and Depression Scale, subscale depression (HADS-D) (7, 15).
2) The SF-36 Health Survey (SF-36) is a generic assessment tool measuring the perceived health related quality of life. The questionnaire contains 36 items comprising eight subscales and two composite domains that reflect physical and mental health. The subscales indicate physical functioning (pfi), role limitations due to physical problems (rolph), physical pain (pain), general health perceptions (ghp), vitality (vital), social functioning (soc), role limitations due to emotional problems (rolem), general mental health (mhi). Scoring is conducted by a computerized evaluation program by summing up the item responses per subscale whereby special weightings are applied for some subscales. The German Version of the SF-36 showed satisfactory psychometric properties, in particular for people with dizziness: internal consistency: α = 0.72–0.89, reliability ICC: 0.79 to 0.97, concurrent validity: r = −0.53 to −0.72 with the DHI.
PPPD has often been associated with psychiatric comorbidities, in particular anxiety and depressive disorders (16–18). However, PPPD is considered a functional diagnosis rather than a psychiatric diagnosis (19). To evaluate the association between PPPD symptoms and anxiety and depressive disorders, the following patient-reported outcome measures were used:
3) The German Version of the Vertigo Symptom Scale (VSS-G) (6, 20) evaluates the frequency and severity of dizziness symptoms within the last 12 months. It is composed of 34 items categorized into two subscales: autonomic arousal and somatic anxiety (VSS-A), and vertigo and related symptoms (VSS-V). This questionnaire is scaled to ordinal level, with response options reflecting frequency: zero (never), once to three times per year (few times, one point), four to twelve times per year (several times, two points), on average > 1/month (quite often, three points), and on average > 1/week (very often, four points) resulting in a total score range between zero and 136 points, indicating a spectrum from no symptoms to severe vertigo. The psychometric properties of the VSS-G scale show moderate to good internal consistency: α = 0.90, reliability: ICC = 0.93, and convergent validity: VSS-G: r = 0.56 with DHI, VSS-A: r = 0.45 with HADS-A and for discrimination VSS-V: r = 0.19 with HADS-A (6, 20).
4) The ABC scale is used as an instrument to assess functional mobility impairment (21). Comprising 16 items, the questionnaire assesses individuals' confidence in maintaining their balance during various daily activities, such as standing on a chair. The ABC scale ranges from zero (not at all confident) to 100 percent (absolutely confident) (21). Scores below 50 percent indicate a low level of physical functioning, while scores between 50 and 80 percent indicate a moderate level of physical functioning. Healthy, physiically active adults achieve scores above 80 percent (22, 23). The German Version of the ABC Scale (ABC-D) demonstrated satisfactory to very good psychometric properties (internal consistency: α = 0.91–0.95, reliability: ICC = 0.94, criterion validity: r = 0.57 with the SF- 36 domain physical health, r = 0.59 with the SF-36 domain mental health (22, 23).
5) The HADS is a concise self-report questionnaire designed for individuals with physical impairments, assessing levels of anxiety and depression in relation to the preceding week (15, 24). The 14-item questionnaire consists of two subscales: anxiety (HADS-A) and depression (HADS-D). Four ordinal response categories include zero (not at all), one (not very much/sometimes), two (quite a lot/very often), and three points (very much indeed/nearly all the time) (24). The score for each subscale ranges from zero to 21 points. A score ≥ eight defines the caseness on both subscales (25). Scores per subscale ≥eleven indicate severe to very severe symptomatology. The questionnaire has demonstrated good psychometric properties (internal consistency: α = 0.8 to 0.81), reliability: ICC = 0.81 to 0.89, construct validity HADS-A: r = 0.65 with other anxiety rating procedures, HADS-D r = 0.7 with other depression rating procedures, in different patient populations, e.g., neurologic or psychosomatic patients (25–27).
Furthermore, all patients completed a form to collect demographic information for descriptive purposes. Additionally, a subsample of the patients in Switzerland received an assessment sheet to evaluate the comprehensiveness and comprehensibility of the NPQ-R.
2.4 Procedures
At baseline, all participants received the aforementioned questionnaires either by postal mail or through personal contact. The questionnaires were accompanied by an informational letter detailing the procedure and a stamped, addressed envelope for return. The procedure is illustrated in Figure 1.
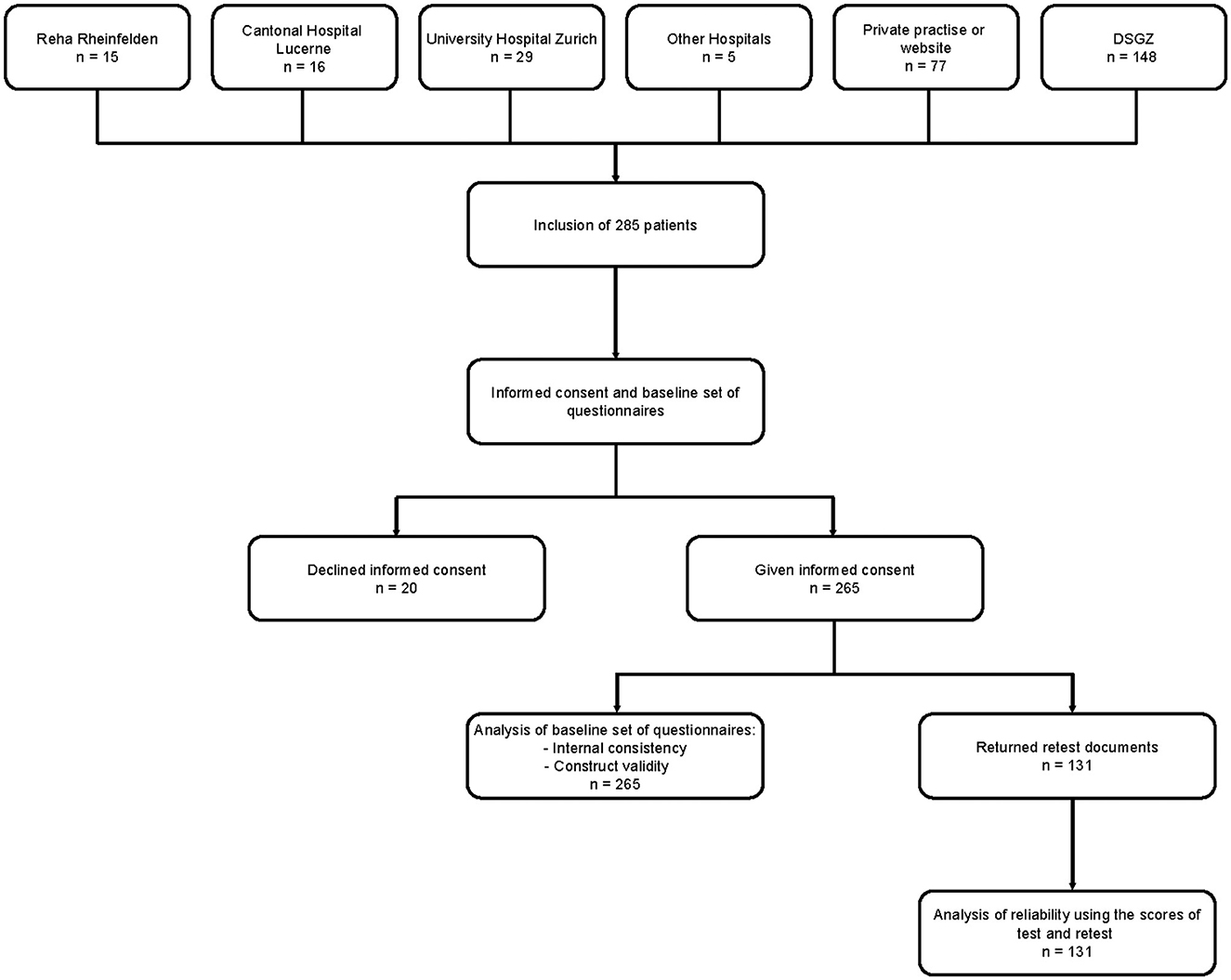
Figure 1. Flow Chart of data collection and analysis procedure. DSGZ, German Center for Vertigo and Balance Disorders; n, number of participants.
In a subset of patients, the NPQ-R which includes the NPQ, was subsequently collected a second time at least 6 days later by postal mail. Additionally, the collection and processing of the responses were monitored weekly, including reminders sent by email or phone for any unanswered questionnaires or unclear responses.
2.5 Statistical analysis
Questionnaires with missing values exceeding 15% were excluded from analysis to mitigate potential selection bias (28). Demographics and test data were analyzed using descriptive statistics while frequency distributions were described using histograms. According to Terwee et al., floor or ceiling effects are present when 15% of subjects achieve the highest or lowest possible score (29).
In order to pool the data from Germany and Switzerland, NPQ-R and NPQ-R-Retest were tested for equivalence using an Independent Sample T-Test. The Equivalence Independent Samples T-Test results indicated that there are no statistically significant differences in both the total NPQ-R and NPQ-R-Retest scores, as evidenced by p > 0.05, specifically 0.886 and 0.231, respectively. Additionally, the equivalence bounds for Cohen's d were within the range of −0.003 to 0.003 for the NPQ-R and −0.002 to 0.002 for the NPQ-R-Retest, further suggesting no significant differences. Normal distribution of NPQ-R and NPQ retest scores were evaluated by visual inspection and the Shapiro-Wilk Test. The Shapiro-Wilk test results for Reha Rheinfelden indicate that both NPQ-R and NPQ-R Retest follow a normal distribution, with p-values of 0.704 and 0.730, respectively. Similarly, for DSGZ, both NPQ-R and NPQ-R Retest showed normal distribution, with p-values of 0.763 and 0.304. In order to get an overview of the scale structure, Cronbach's α was calculated to determine internal consistency whereby values between 0.7 and 0.95 are considered acceptable (30). Additionally, the comparisons to the original NPQ serves as a reference.
To determine reproducibility of the instrument, test-retest reliability was examined using intraclass correlation coefficients (ICC; two-way mixed effect model, absolute agreement between single scores) (31, 32). ICC values ≥0.70 are considered as the minimum standard for reliability in a study population of at least 50 subjects (29).
To assess not only the variability (reliability parameter) between the participants, but also the agreement between repeated measurements (agreement parameter), the measurement error (standard error of measurement, SEM) and the limits of agreements were also calculated. The minimal detectable change (MDC) is based on the measurement error (28).
To evaluate convergent construct validity, the scores of the NPQ-R were correlated with the scores of the DHI, VSS, ABC Scale, HADS, and SF-36. The correlation of the ordinal scaled variables was calculated using the Spearman's rank correlation coefficient (33) with guidelines proposed by Cohen: rs = 0.10 to 0.29 = low correlation; rs = 0.30 to 0.49 = medium/moderate correlation; rs = 0.50 to 1.0 = large/high correlation (34). Regarding construct validity, we hypothesized that a high correlation r > 0.5 according to Cohen (34) will exist between the total score of the NPQ-R and the total score of the DHI and the VSS because all three instruments are related as disease-specific patient reported outcome measures. The NPQ and NPQ-R scores were statistically compared in primary PPPD vs. PPPD by t-test.
Level of significance was set at p ≤ 0.05. Statistical analyses were performed with R version 2021.09.2 (35), SPSS version 22.0.0.0 (IBM Corp. Armonk, US), and JASP version 0.16.2 (University of Amsterdam, The Netherlands).
3 Results
3.1 Study sample and setting
The study included 265 patients (130 males and 135 females). One hundred seventeen patients were recruited from different centers in Switzerland (between September 2021 and December 2023) and 148 patients were recruited from the DSGZ at the Ludwig-Maximilians-University Munich (GER, between April 2023 and December 2023). Descriptive data of all 265 patients for the two study centers are summarized in Table 2. After ensuring equivalence, data from both study centers were merged into a single master data file for all subsequent analyses.
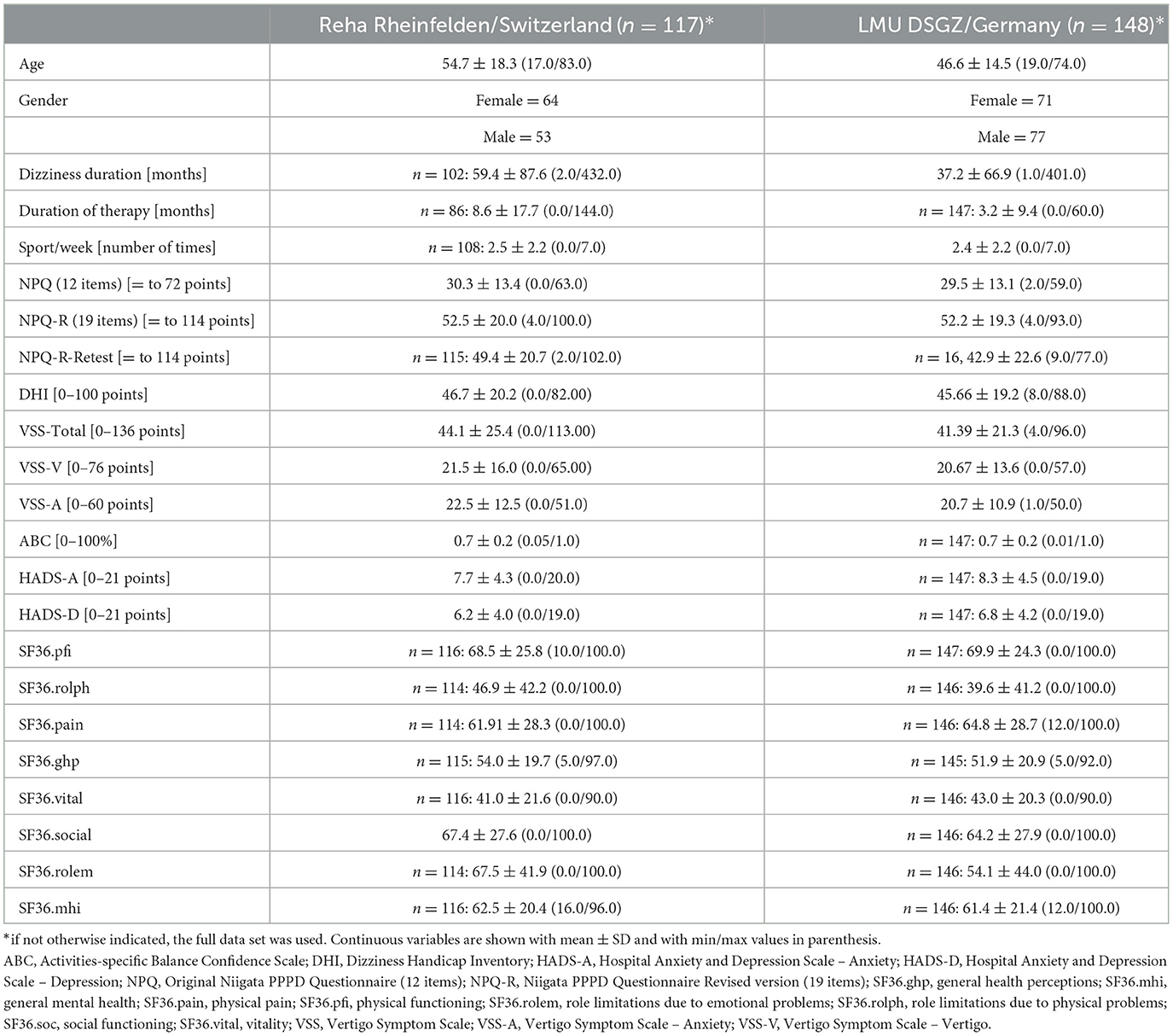
Table 2. Descriptive analysis of both recruiting centers.
To determine test-retest reliability, 131 patients completed the NPQ-R twice. Mean age for the total population was 50.2 +/- 16.8 years (Mfemale= 53.1 ± 15.8; Mmale= 47.09 ± 17.2). Disease duration was 46.3 ± 76.6 months (Mfemale= 47.7 ± 77.4; Mmale= 44.8 ± 76.1) and therapy duration varied between zero and 144 months. Descriptive data for all questionnaires of the total study population is provided in Table 2. No forms had missing data exceeding the predefined 15%-level. The scores from the NPQ-R ranged from 4 to 100 points. Accordingly, no floor or ceiling effects were present (36).
Out of 118 patients in Switzerland, 114 returned the additional evaluation sheet regarding the NPQ-R's comprehensiveness and comprehensibility. Nearly all patients rated comprehensiveness and comprehensibility positively, with scores ranging between 92% and 99% for each of the 19 items.
Among the 148 PPPD patients in Germany, 95 patients were classified as having pPPPD and 53 as having sPPPD (16benign paroxysmal vertigo, 16 vestibular migraine, 8 acute unilateral vestibulopathy, 4 circulatory dysregulations, e.g., orthostatic, syncope, 3 infectious symptoms, 2 transient ischemic attack, 1 acceleration trauma). Statistical analyses revealed no significant differences neither of NPQ nor of NPQ-R in pPPPD vs. sPPPD (NPQ: pPPPD 29.1 ± 12.9 vs. sPPPD 30.1 ± 13.6, p = 0.675; NPQ-R: pPPPD 51.8 ±18.6 vs. sPPPD 52.8 ± 20.7, p = 0.776).
Table 2 presents an overview on all descriptive parameters for both sexes, indicating slightly higher mean values for females compared to males, with the exception of the SF-36 subscale for physical functioning and SF-36 subscale for role limitations due to physical problems.
Table 3 provides an overview of the correlations between the NPQ-R, the NPQ and all other patient-reported outcome measures utilized in the study. As expected, the correlation between the NPQ and NPQ-R was high (rs = 0.969). The highest correlation for the NPQ and NPQ-R and all other patient-reported outcome measures was found between the NPQ-R and DHI (rs = 0.752). VSS exhibit moderate (VSS: rs = 0.498; VSS-V: rs = 0.462; VSS-A: rs = 0.430) correlations with NPQ-R and also moderate (VSS: rs = 0.459; VSS-V: rs = 0.426; VSS-A: rs = 0.390) correlations with NPQ. Negative moderate correlations were found between NPQ-R and SF36 subscale physical functioning (r = −0.538) as well as NPQ (r = −0.578). HADS-A and HADS-D show moderate correlations with NPQ-R (r = 0.430 and 0.487) and NPQ (r = 0.354 and 0.438). ABC has a moderate negative correlation with both NPQ- R (r = −0.545) and NPQ (r = −0.542).
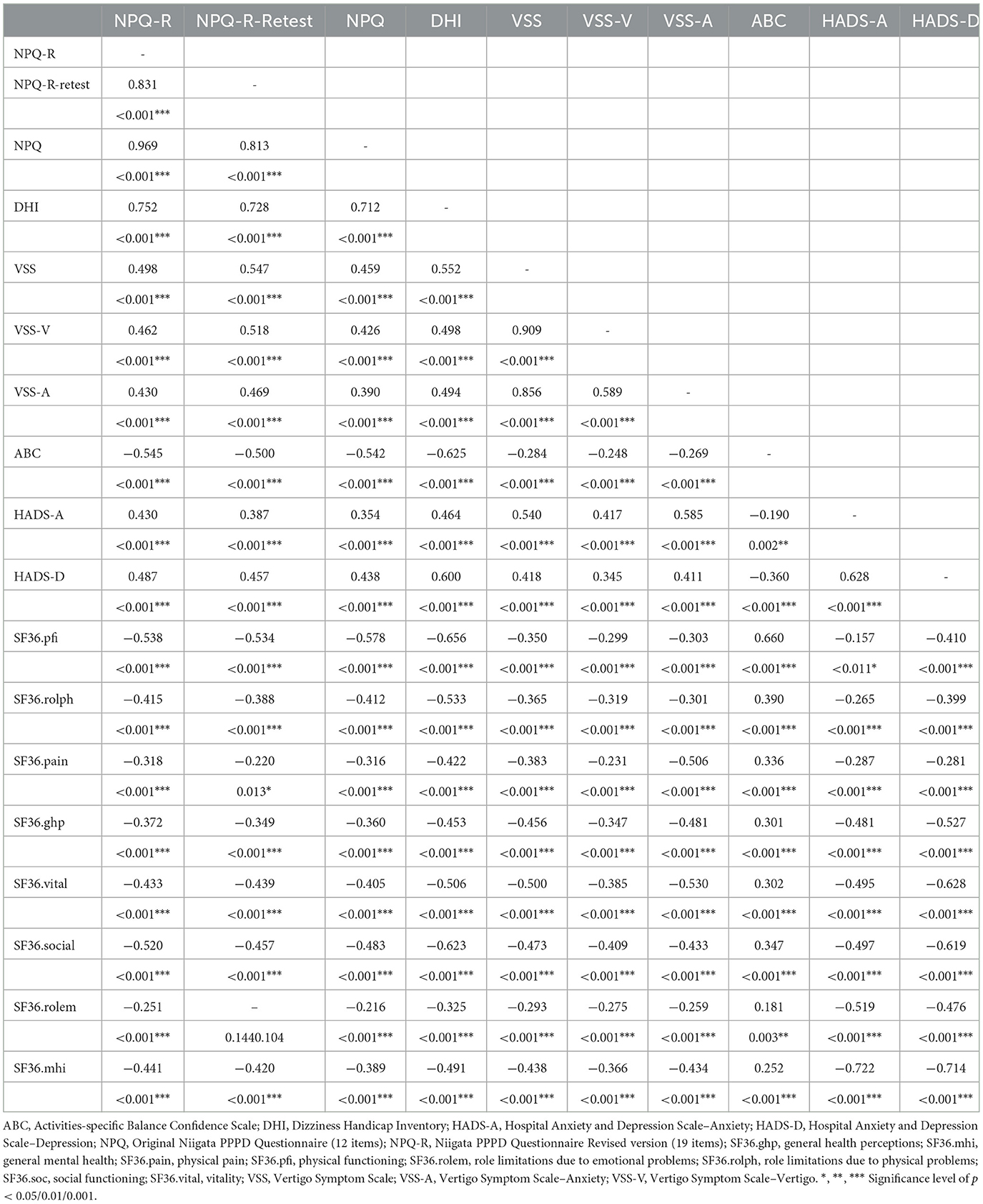
Table 3. Spearman rank correlations between NPQ-R, NPQ-R-Retest, NPQ and all other assessments (n = 131).
3.2 Reliability and reliability-related parameters: internal consistency, test-retest reliability, SEM, and MDC
3.2.1 Internal consistency
Cronbach's α values ranged between 0.62 and 0.78 for the subscales separately and α=0.91 for the 19-item NPQ-R (Table 4). For comparison purposes, the values of the 12-item NPQ version are also shown in Table 5.
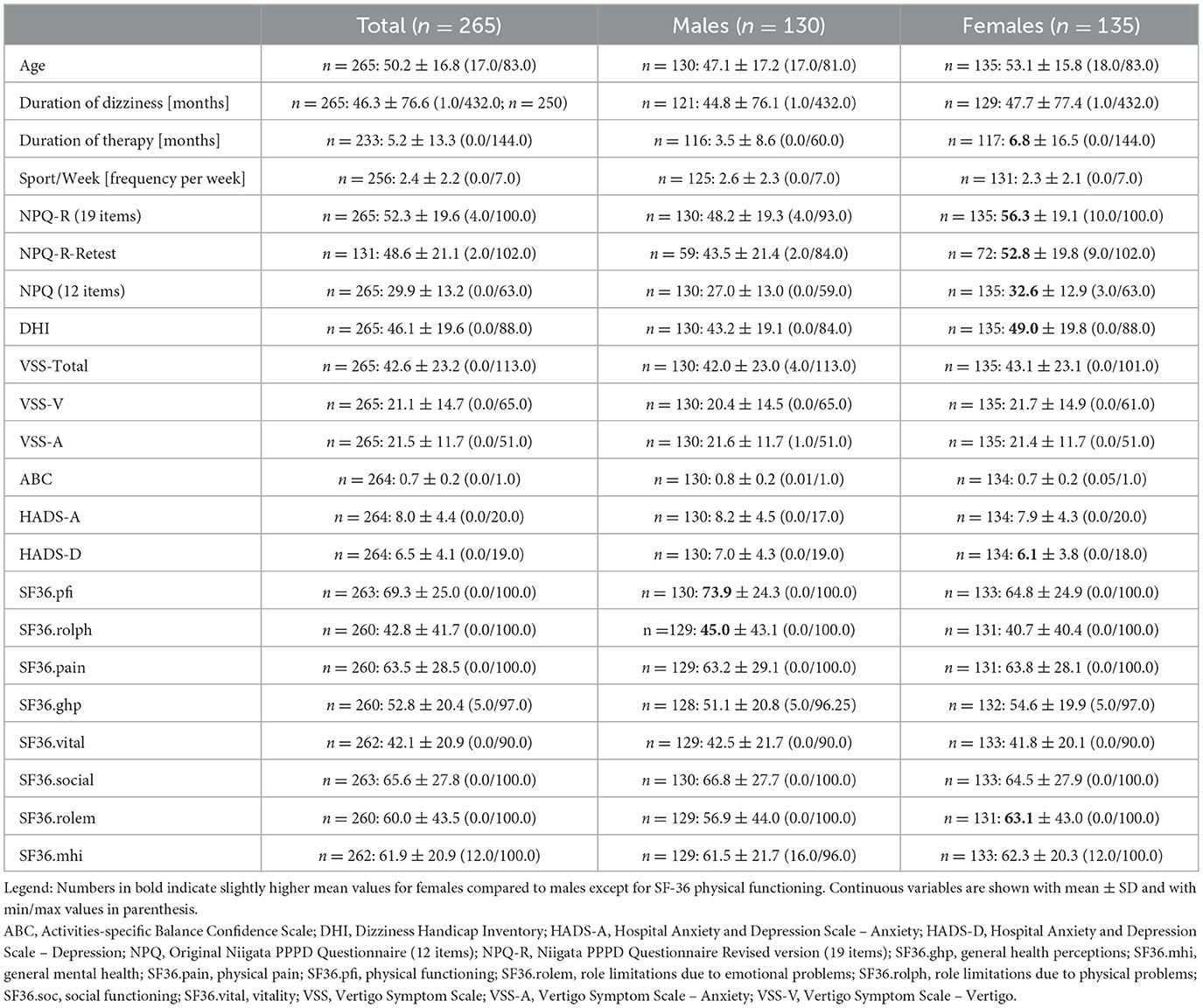
Table 4. Descriptive analysis for the total study population and for both sexes.

Table 5. Cronbach's alpha for NPQ-R and NPQ (n = 265).
Furthermore, item analyses for the subscales revealed a higher α in each subscale, if the following items within one subscale were dropped: upright postured/walking item 11 (α = 0.734), movement item 8 (α = 0.717), visual item 2 (α = 0.799), associated symptoms (NPQ-R) item 9 (α = 0.738), and symptom behavior (NPQ-R) item 7 (α = 0.560) as seen in Table 6.
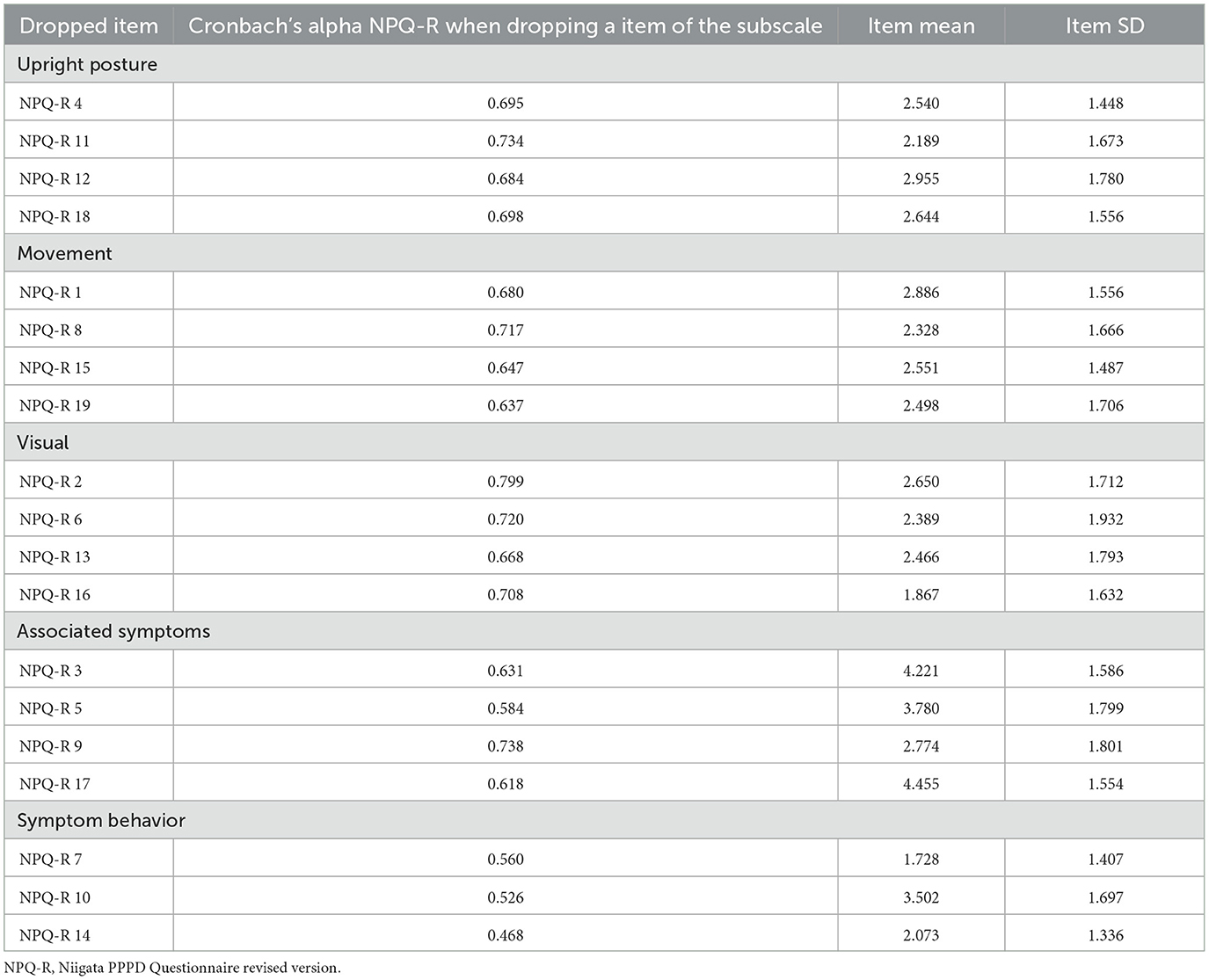
Table 6. Item analysis of the NPQ-R when dropping one item per subscale (n = 265).
3.2.2 Test-retest reliability
Test-retest reliability scores of the NPQ and the NPQ-R including the SEM and the MDC values are provided in Table 7 and in the Bland Altman Plot in Figure 3. The second NPQ-R was only sent after the first one had been received. In the meantime, patients were reminded to complete the first questionnaire as soon as possible to minimize the time gap between the two assessments. Thus, the NPQ-R was then sent for the retest between 7 and 99 days afterwards (median = 9 days; IQR = 14 days). The central line in the Bland Altman plot shows the mean difference (MD = 2.5) in NPQ-R total score between the first and second measurement and its limits of agreement (95% of the differences between measurement time point one and two are between −20.1 and 25.1) (37).

Table 7. ICC, SEM, MDC, mean difference and range of agreement for the NPQ (n = 131) and NPQ-R (n = 131).
4 Discussion
Persistent postural-perceptual Dizziness (PPPD) is defined as a chronic vestibular disorder of non-spinning vertigo that is exacerbated by three factors: upright posture, active or passive movements, and exposure to moving or complex visual patterns. It causes significant distress as well as functional impairment (1). The diagnosis of this functional neurological disorder is based on the presence of clinical key symptoms as positive characteristics as well as the exclusion of another disease. Due to the lack of a specific biomarker, the diagnosis of PPPD requires a precise assessment of vestibular symptoms, exacerbating factors, and the medical history. The Niigata PPPD Questionnaire (NPQ), designed for the standardized diagnosis and assessment of the severity of PPPD, was first developed in Japan in 2019 (8). The original NPQ was recently translated into a German version and revised through an expert Delphi consensus survey, incorporating additional items that address symptoms and symptom behavior to provide a comprehensive assessment of PPPD intensity (NPQ-R) (11). The present study assessed the convergent construct validity, internal consistency, test-retest reliability, SEM and MDC of both the translated German 12-item original NPQ and the 19-item revised NPQ-R version. Our results indicate that both versions are valid and reliable patient-reported outcome measures for assessing and monitoring symptomatology in patients with persistent postural perceptual dizziness. However, we recommend the 19-item NPQ-R due to its incorporation of both patient and expert perspectives, as well as its higher internal consistency of the total score compared to the 12-item NPQ.
4.1 Convergent construct validity
Overall, our hypothesis concerning construct validity was confirmed. Convergent construct validity of the NPQ and NPQ-R was established through the strong association between the NPQ and NPQ-R with the DHI (rs = 0.712; rs = 0.752). The high correlations suggest that the DHI captures similar triggers and functional limitations, indicating that it includes items related to the construct under investigation and is comparable to the Spanish version with rP=0.751 (36) and the French version with 0.73 (38).
The weak to moderate correlations of the NPQ and NPQ-R with the anxiety subscales VSS-A (rs = 0.390; rs = 0.430) and HADS-A (rs = 0.354; rs = 0.430) as well as with the depression subscale of the HADS (rs = 0.438 and rs = 0.487) suggest that the association between PPPD and psychiatric illness might be low, which corresponds to the French cohort with 50 patients with rs = 0.27 for HADS-D, 0.08 for HADS-A, and 0.07 for anxiety. These values are line with earlier studies in precursor functional vertigo syndromes, e.g., chronic subjective dizziness or somatoform vertigo (20, 39) as well as with the smaller French and Spanish evaluation (HADS-D 8.5, HADS-A 11.5). However, PPPD is considered a specific functional diagnosis rather than a psychiatric diagnosis (16, 18).
The ABC-score reflects the patients' confidence in performing certain activities. In our study, the ABC-score indicated only moderately impaired level of functioning (mean 0.7, Table 4), and the negative correlation between the NPQ/NPQ-R and the ABC-Scale (rs = −0.545) was even moderate. This fits to the current pathophysiological concept of PPPD that postulates an increased self-observation with a shift to high-demand postural control strategies (stiffening due to higher anti-gravity muscle activity and co-contraction). These changes can be identified by posturography and gait analyses (18, 40–43): In functional dizziness the postural sway is typically increased during simple balance tasks, but becomes normal with distraction (dual tasks) and more difficult balance tasks, i.e., the more difficult the demand of balance, the more “healthy” is the balance performance. In this context, and consistent with typical patients' reports indicating an improvement in symptoms with physical activities, it seems logical that the overall confidence of patients in performing activities is only slightly diminished. The finding of a less strong calculated association between ABC and NPQ in our study compared to the Spanish study (rp= −0.739) is due to their inhomogeneous patient cohort including not only PPPD, but two third of patients with organic vestibular syndromes and probable persisting vestibular impairment (36, 40–43).
Only low to moderate negative correlations were observed between the NPQ and NPQ-R and the SF-36 subscales, supporting our hypothesis that the SF-36, as a generic measure of overall quality of life, and the NPQ, as a disease-specific construct measure, assess different parameters. However, the negative correlations indicate that PPPD adversely affects health-related quality of life, impacting both physical and social functioning, thereby underscoring its symptomatic impact and relevance in daily life. No statistically significant differences were found between the 12-item NPQ and the 19-item NPQ-R regarding the associations between the disease-, depression-, anxiety- or general health-related questionnaires.
4.2 Reliability and reliability-related parameters: internal consistency, test-retest reliability, SEM, and MDC
The Internal consistency of the NPQ and NPQ-R can be considered highly acceptable (alpha = 0.88; alpha = 0.91). Subscale analyses also revealed acceptable values ranging between 0.71 and 0.78. Our alpha values are lower compared to the French (38) and the Spanish (36) NPQ versions with alpha values ranging between 0.81 and 0.92 and between 0.803 and 0.869, respectively. However, authors of both studies included distinct smaller patient cohorts of only 50 and 47 PPPD patients. The new subscale for symptom behavior of the NPQ-R demonstrated a moderate internal consistency with α=0.62, which falls below the recommended threshold of Tavakol and Dennick (30). These authors suggested that a lower level of internal consistency may be attributed to a small number of items within the subscale, which is the case with three items compared to four items in all other subscales. However, the symptom behavior subscale still provides information regarding the change in PPPD symptoms over time or the patient's ability to adapt to the limiting condition. Therefore, we recommend using the NPQ-R with all subscales rather than individual subscales only.
Test-retest reliability for the NPQ (Figure 2) and the NPQ-R (Figure 3) appears to be satisfactory and is comparable to the ICC scores reported for the Spanish NPQ version (36).
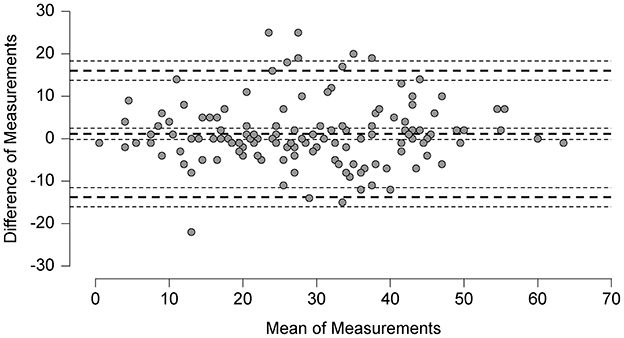
Figure 2. Bland altman plot: analysis of differences between the NPQ scores at test and retest.
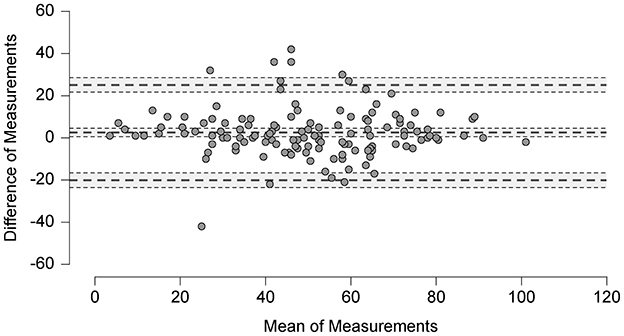
Figure 3. Bland altman plot: analysis of differences between the NPQ-R scores at test and retest.
Due to our large sample size with n = 265, the SEM (5.53) of the NPQ (12 items) is lower than the SEM the Spanish version (6.63) (36), based on 47 patients with PPPD only. Their smaller sample size might be the reason for their lower MDC with 12.99 compared to our MDC with 15.5 points for the NPQ and with 23 points for the NPQ-R.
Both Yagi et al. (8) for the original Japanese and Meletaki et al. (38) for the French version did not provide information regarding test-retest reliability, SEM and MDC.
4.3 Outlook
Our inter-item analysis indicated promising values for the differentiation ability of the NPQ-R from a descriptive perspective. All items except items 2 (“When I look through shelves in the supermarket or hardware store”) and 9 (“When I walk, I feel insecure”) demonstrated good internal consistency. Obviously, item 2 and 9 are not very specific for PPPD, since walking or standing can be influenced by several other stance and gait relevant limitations, e.g., polyneuropathy, musculoskeletal disorders, vision problems etc.
For the German NPQ and NPQ-R, we did not assess one-dimensionality and equivalence, which would extent the construct validity of the NPQ and NPQ-R. Therefore, an exploratory and confirmatory factor analyses are warranted.
4.4 Strengths and limitations
Following the COSMIN recommendations, we present the largest sample size (n = 265) compared to the original Japanese (n = 50), the French (n = 50), and the Spanish (n = 47) versions. This substantial sample size provides a robust foundation for the investigation of the psychometric properties of the NPQ and NPQ-R, thereby supporting their application in clinical practice. Furthermore, we provide data on the duration of the PPPD symptoms, the patients' therapy, and their weekly physical activity levels. Additionally, a comprehensive investigation of the 12-item NPQ and 19-item NPQ-R was conducted, examining their correlations with questionnaires related to anxiety, depression, and general health.
Strength of the study, in addition to the large number of patients included, was the recruitment of participants from different outpatient and inpatient sectors across different health care systems in two German-speaking countries. This included private practices, local, regional and university hospitals, which underscores the good applicability of the NPQ and NPQ-R. We would like to emphasize, that there were no statistical differences in the validation of the NPQ and NPQ-R between the German and Swiss cohorts, making a selection bias unlikely. For a more detailed interpretation of the associations between NPQ/NPQ- R and HADS-A and HADS-D, a more comprehensive psychiatric assessment of psychiatric comorbidities would have been beneficial. However, conducting such structured clinical interviews by a psychologist or psychiatrist would have been resource-intensive and fell outside the primary scope of this study. Nonetheless, the prevalence of depressive and anxiety symptoms in our patient cohort is in line with earlier reports (20, 39).
In our study, we focused extensively on the convergent construct validity and reliability parameters of the translated NPQ and the revised NPQ-R. Compared to Yagi et al. (8), Meletaki et al. (38), and Castillejos-Carrasco-Muñoz et al. (36), we were not interested in the discriminant validity of the NPQ, and NPQ- R. To assess the discriminative property for the German versions, a comparative investigation involving patients with PPPD alongside a sufficiently large sample of patients with various vestibular disorders and concurrent diverse symptomatology will be necessary in the future.
A minor limitation of this study could be the inclusion of patients who had already been informed of their diagnosis and received treatment, alongside treatment-naive patients. Combining these two groups may skew results, as both awareness of the diagnosis and prior therapy could significantly influence subjective PPPD symptoms.
The variable duration of the test-retest reliability period may also be regarded as an undesirable influencing factor. Some participants required more days to return the second NPQ-R questionnaire. However, we verified that the average scores for the NPQ and NPQ-R did not differ from those obtained during the first measurement event and are also comparable to the scores from the Japanese, French, and Spanish versions. Furthermore, the mean symptom duration at first measurement was 46 months (Table 4), and a relevant change of the symptomatology of such a chronic disease within a few days appears unlikely. Additionally, we performed a subgroup analysis to gain insights into a potential correlation between interval length and test-retest reliability score. For the NPQ-R data, we divided the whole study population in to a group with a 7 days test-retest duration (n = 40; ICC2, 1 = 0.913), a group with a 8 to 30 days test-retest duration (n = 66; ICC2,1 = 0.832), and a 31+ days test-retest duration (n = 9; ICC2,1 = 0.853). The results did not indicate a relevant impact on the overall test-retest scores for the study participants.
5 Conclusions
The total scale of the German version of the Niigata PPPD Questionnaire and its revised version both demonstrated satisfactory measurement properties for convergent construct validity and reliability parameters (internal consistency, test-retest, SEM and MDC) as an evaluative measure. They represent valid and reliable patient-reported outcome measures suitable for routine clinical use across various health care settings. Compared to the NPQ (12 items), the NPQ-R with its 19 items appears to capture the clinical course of PPPD equally well. However, we recommend the NPQ-R version for the evaluation of PPPD treatment, as it further considers symptom behavior and associated symptoms from the patient's and clinician's perspectives, contributing significantly to the standardized assessment of health status. The German NPQ and NPQ-R should be further evaluated for their multidimensionality through factor analytic analyses (structure-seeking and structure-confirming) and for their ability to discriminate other organic vestibular syndromes.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee Northwest and Central Switzerland and Institutional Review Board of the Ludwig-Maximilians-University Munich Germany. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
SC: Data curation, Formal analysis, Investigation, Writing – original draft. E-YG: Data curation, Formal analysis, Investigation, Writing – original draft, Visualization. SE: Investigation, Writing – review & editing. FB: Conceptualization, Formal analysis, Writing – review & editing, Visualization. MS: Conceptualization, Writing – review & editing. SS: Conceptualization, Writing – review & editing. MM: Writing – review & editing, Methodology. LF: Formal analysis, Investigation, Writing – review & editing. JG: Formal analysis, Investigation, Writing – review & editing. DG: Formal analysis, Investigation, Writing – review & editing. WT: Writing – review & editing, Methodology. AZ: Supervision, Writing – review & editing. RS: Data curation, Formal analysis, Writing – review & editing. KP: Methodology, Writing – review & editing. HG: Methodology, Writing – review & editing. LB: Writing – review & editing. SB-B: Methodology, Supervision, Writing – review & editing. CS-A: Conceptualization, Methodology, Supervision, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
A special thanks to Prof. D. Straumann, Dr. C. Candreia, and K. Weickhardt for their valuable contribution to the patient recruitment in Switzerland, Dr. Wiebke Trost and Prof. Jasmin Wandel for the advice regarding questionnaire development and statistical data analyses, and Mara Augstburger for supporting data collection. We are very grateful to all our patients, who invested their time to participate in our study. Furthermore, we are thankful to the personnel of German Center for Vertigo and Balance Disorders.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1517566/full#supplementary-material
Abbreviations
ABC-Scale, Activities-specific Balance Confidence Scale; CI, Confidence Interval; DHI, Dizziness Handicap Inventory; HADS, Hospital Anxiety and Depression Scale; HADS-A, Hospital Anxiety and Depression Scale; Anxiety Subscale; HADS-D, Hospital Anxiety and Depression Scale; Depression Subscale; ICC, Intraclass correlation coefficient; NPQ, Niigata PPPD Questionnaire; NPQ-R, revised Niigata PPPD Questionnaire; PPPD, Persistent Postural-Perceptual Dizziness; PROM, patient-reported outcome measure; MDC, minimal detectable change; SEM, Standard error of measurement; SF36. pain, physical pain; SF36.pfi, physical functioning; SF36.rolph, role limitations due to physical problems; SF36.ghp, general health perceptions; SF36.mhi, general mental health; SF36.rolem, role limitations due to emotional problems; SF36.soc, social functioning; SF36.vital, vitality; VSS, Vertigo Symptom Scale; VSS-A, VSS Anxiety Subscale; VSS-V, VSS Vertigo Subscale.
References
1. Staab JP, Eckhardt-Henn A, Horii A, Jacob R, Strupp M, Brandt T, et al. Diagnostic criteria for persistent postural-perceptual dizziness (PPPD): Consensus document of the committee for the classification of vestibular disorders of the barany society. J Vestib Res Equilib Orientat. (2017) 27:191–208. doi: 10.3233/VES-170622
2. Strupp M, Brandt T, Dieterich M. Vertigo and Dizziness: Common Complaints, 3rd ed. Cham: Springer. (2023).
3. Adamec I, Juren Measki S, Krbot Skoric M, Jazic K, Crnosija L, Milivojevic I, et al. Persistent postural-perceptual dizziness: clinical and neurophysiological study. J Clin Neurosci. (2020) 72:26–30. doi: 10.1016/j.jocn.2020.01.043
4. Eckhardt-Henn A, Tschan R, Best C, Dieterich M. Somatoforme schwindelsyndrome. Nervenarzt. (2009) 80:909–17. doi: 10.1007/s00115-009-2736-y
5. Popkirov S, Staab JP, Stone J. Persistent postural-perceptual dizziness (PPPD): a common, characteristic and treatable cause of chronic dizziness. Pract Neurol. (2018). doi: 10.1007/s11940-018-0535-0
6. Gloor-Juzi T, Kurre A, Straumann D, De Bruin ED. Translation and validation of the vertigo symptom scale into German: A cultural adaption to a wider German-speaking population. BMC Ear, Nose Throat Disord. (2012) 12:1. doi: 10.1186/1472-6815-12-7
7. Kurre A, Van Gool CJAW, Bastiaenen CHG, Gloor-Juzi T, Straumann D, De Bruin ED. Translation, cross-cultural adaptation and reliability of the German version of the dizziness handicap inventory. Otol Neurotol. (2009) 30:3. doi: 10.1097/MAO.0b013e3181977e09
8. Yagi C, Morita Y, Kitazawa M, Nonomura Y, Yamagishi T, Ohshima S, et al. A validated questionnaire to assess the severity of persistent postural-perceptual dizziness (PPPD): the Niigata PPPD Questionnaire (NPQ). Otol Neurotol. (2019) 40:e747–e752. doi: 10.1097/MAO.0000000000002325
9. Terwee CB, Prinsen CA, Chiarotto A, Cw De Vet H, Bouter LM, Marjan JA, et al. COSMIN methodology for assessing the content validity of PROMs: user manual. In: Circulation. Amsterdam: Vrije Universiteit Amsterdam (2018).
10. Beaton DE, Bombardier C, Guillemin F, Ferraz MB. Guidelines for the process of cross-cultural adaptation of self-report measures. Spine. (2000) 25:3186–91. doi: 10.1097/00007632-200012150-00014
11. Behrendt F, Stark M, Chételat S, Schädler S, Trost W, Parmar K, et al. The German revised version of the Niigata PPPD Questionnaire (NPQ-R): development with patient interviews and an expert Delphi consensus. PLoS ONE. (2023) 18:9. doi: 10.1371/journal.pone.0291002
12. Halmagyi GM, Curthoys IS, Brandt T, Dieterich M. Ocular tilt reaction: clinical sign of vestibular lesion. Acta Otolaryngol. (1991) 111:S481. doi: 10.3109/00016489109131342
13. Brandt T, Dieterich M. Vestibular syndromes in the roll plane: topographic diagnosis from brainstem to cortex. Ann Neurol. (1994) 36:410360304. doi: 10.1002/ana.410360304
14. Jacobson GP, Newman CW. The development of the dizziness handicap inventory. Arch Otolaryngol Neck Surg. (1990) 116:424–7. doi: 10.1037/t35080-000
15. Schädler S, Kool J, Lüthi H, Marks D, Oesch P, Pfeffer A, et al. Assessments in der Rehabilitation - Band 1: Neurologie. Göttingen: Hans Huber. (2012). 608 p.
16. Eckhardt-Henn A, Breuer P, Thomalske C, Hoffmann SO, Hopf HC. Anxiety disorders and other psychiatric subgroups in patients complaining of dizziness. J Anxiety Disord. (2003) 17:4. doi: 10.1016/S0887-6185(02)00226-8
17. Decker J, Limburg K, Henningsen P, Lahmann C, Brandt T, Dieterich M. Intact vestibular function is relevant for anxiety related to vertigo. J Neurol. (2019) 266:89–92. doi: 10.1007/s00415-019-09351-8
18. Dieterich M, Staab JP. Functional dizziness: from phobic postural vertigo and chronic subjective dizziness to persistent postural-perceptual dizziness. Curr Opin Neurol. (2017) 30:107–113. doi: 10.1097/WCO.0000000000000417
19. Holmberg JM. Pathophysiology, differential diagnosis, and management of persistent postural-perceptual dizziness: a review. Perspect ASHA Spec Interes Groups. (2020) 5:181–91. doi: 10.1044/2019_PERSP-19-00105
20. Tschan R, Wiltink J, Best C, Bense S, Dieterich M, Beutel ME, et al. Validation of the German version of the vertigo symptom scale (VSS) in patients with organic or somatoform dizziness and healthy controls. J Neurol. (2008) 255:1. doi: 10.1007/s00415-008-0863-1
21. Powell LE, Myers AM. The activities-specific balance confidence (ABC) scale. J Gerontol - Ser A Biol Sci Med Sci. (1995). 50A:28–34. doi: 10.1037/t13026-000
22. Schott N. German adaptation of the “Activities-specific Balance Confidence (ABC) scale” for the assessment of falls-related self-efficacy. Z Gerontol Geriatr. (2008) 41:475–85. doi: 10.1007/s00391-007-0504-9
23. N. S. Reliability and validity of the German short version of the Activities specific Balance Confidence (ABC-D6) scale in older adults. Arch Gerontol Geriatr. (2014) 59:272–9. doi: 10.1016/j.archger.2014.05.003
24. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
25. Bjelland I, Dahl AA, Haug TT, Neckelmann D. The validity of the Hospital Anxiety and Depression Scale: An updated literature review. J Psychosom Res. (2002) 52:69–77. doi: 10.1016/S0022-3999(01)00296-3
26. Herrmann C. International experiences with the hospital anxiety and depression scale - a review of validation data and clinical results. J Psychosom Res. (1997) 42:17–41. doi: 10.1016/S0022-3999(96)00216-4
27. Hinz A, Schwarz R. Anxiety and depression in the general population: normal values in the Hospital Anxiety and Depression Scale. Psychother Psychosom Med Psychol. (2001). 51:193–200. doi: 10.1055/s-2001-13279
28. de Vet HCW, Terwee CB, Knol DL, Bouter LM. When to use agreement versus reliability measures. J Clin Epidemiol. (2006) 59:1033–9. doi: 10.1016/j.jclinepi.2005.10.015
29. Terwee CB, Bot SDM, de Boer MR, van der Windt DAWM, Knol DL, Dekker J, et al. Quality criteria were proposed for measurement properties of health status questionnaires. J Clin Epidemiol. (2007) 60:34–42. doi: 10.1016/j.jclinepi.2006.03.012
30. Tavakol M, Dennick R. Making sense of Cronbach's alpha. Int J Med Educ. (2011) 2:53–55. doi: 10.5116/ijme.4dfb.8dfd
31. McGraw KO, Wong SP. Forming inferences about some intraclass correlation coefficients. Psychol Methods. (1996) 1:30–46. doi: 10.1037//1082-989X.1.1.30
32. Qin S, Nelson L, McLeod L, Eremenco S, Coons SJ. Assessing test–retest reliability of patient-reported outcome measures using intraclass correlation coefficients: recommendations for selecting and documenting the analytical formula. Qual Life Res. (2019) 28:1029–1033. doi: 10.1007/s11136-018-2076-0
33. Terwee CB, Knol DL, de Vet HCW, Mokkink LB. Development of a measurement instrument. In: Measurement in Medicine: A Practical Guide. Cambridge: Cambridge University Press (2011). p. 30–64.
34. Cohen J. Statistical power analysis for the behavioral sciences, Vol. 2nd. In: Statistical Power Analysis for the Behavioral Sciences. New York, NY: Routledge (1988). p. 567.
35. Core R Team. A Language and Environment for Statistical Computing. Vienna: R Foundation for Statistical Computing (2022). p. 2.
36. Castillejos-Carrasco-Muñoz R, Peinado-Rubia AB, Lérida-Ortega MÁ, Ibáñez-Vera AJ, Tapia-Toca MC, Lomas-Vega R. Validity and reliability of the Niigata PPPD Questionnaire in a Western population. Eur Arch Oto-Rhino-Laryngol. (2023) 280:12. doi: 10.1007/s00405-023-08038-1
37. Giavarina D. Understanding bland Altman analysis. Biochem Medica. (2015) 25:2. doi: 10.11613/BM.2015.015
38. Meletaki V, Gobinet M, Léonard J, Elzière M, Lopez C. French adaptation and validation of the Niigata PPPD Questionnaire: measure of severity of Persistent Postural-Perceptual Dizziness and its association with psychiatric comorbidities and perceived handicap. Front Neurol. (2024) 15:1388805. doi: 10.3389/fneur.2024.1388805
39. Staab JP. Chronic subjective dizziness. Continuum. (2012) 18:1118–41. doi: 10.1212/01.CON.0000421622.56525.58
40. Querner V, Krafczyk S, Dieterich M, Brandt T. Patients with somatoform phobic postural vertigo: the more difficult the balance task, the better the balance performance. Neurosci Lett. (2000) 285:9. doi: 10.1016/S0304-3940(00)01008-9
41. Krafczyk S, Tietze S, Swoboda W, Valkovič P, Brandt T. Artificial neural network: a new diagnostic posturographic tool for disorders of stance. Clin Neurophysiol. (2006) 117:22. doi: 10.1016/j.clinph.2006.04.022
42. Wuehr M, Brandt T, Schniepp R. Distracting attention in phobic postural vertigo normalizes leg muscle activity and balance. Neurology. (2017) 88:284–88. doi: 10.1212/WNL.0000000000003516
Keywords: Persistent Postural-Perceptual Dizziness, functional dizziness, patient-reported outcome measure, concurrent construct validity, test-retest reliability, internal consistency, standard error of measurement, minimal detectable change
Citation: Chételat S, Gerber E-Y, El Khadlaoui S, Behrendt F, Stark M, Schädler S, Maywald M, Fabritius L, Gerb J, Grabova D, Trost W, Zwergal A, Strobl R, Parmar K, Gerth HU, Bonati LH, Becker-Bense S and Schuster-Amft C (2025) Convergent construct validity and test-retest reliability of both German versions of the original and the revised Niigata PPPD Questionnaire: NPQ and NPQ-R. Front. Neurol. 16:1517566. doi: 10.3389/fneur.2025.1517566
Received: 26 October 2024; Accepted: 02 January 2025;
Published: 27 January 2025.
Edited by:
Hubertus Axer, Jena University Hospital, GermanyReviewed by:
Evangelos Anagnostou, National and Kapodistrian University of Athens, GreeceFatih Özden, Mugla University, Türkiye
Desi Phillip Schoo, The Ohio State University Wexner Medical Center, United States
Copyright © 2025 Chételat, Gerber, El Khadlaoui, Behrendt, Stark, Schädler, Maywald, Fabritius, Gerb, Grabova, Trost, Zwergal, Strobl, Parmar, Gerth, Bonati, Becker-Bense and Schuster-Amft. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Corina Schuster-Amft, Y29yaW5hLnNjaHVzdGVyYW1mdEB1bmliYXMuY2g=; Frank Behrendt, ZnJhbmsuYmVocmVuZHRAdW5pYmFzLmNo
†These authors have contributed equally to this work and share first authorship
‡These authors have contributed equally to this work and share last authorship