 Yuzheng Lai1*†
Yuzheng Lai1*† Mohammad Mofatteh2†
Mohammad Mofatteh2† José Fidel Baizabal-Carvallo3,4
José Fidel Baizabal-Carvallo3,4 Jianfeng He1
Jianfeng He1 Wenhao Wu5Daohong Wang1Wenshan Yan1Jicai Ma6Sijie Zhou7Yu Sun8,9Yi He1Shumei Li10Hao Sun1*
Wenhao Wu5Daohong Wang1Wenshan Yan1Jicai Ma6Sijie Zhou7Yu Sun8,9Yi He1Shumei Li10Hao Sun1*- 1Department of Neurology, Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine (Nanhai District Hospital of Traditional Chinese Medicine of Foshan City), Foshan, China
- 2School of Medicine, Dentistry and Biomedical Sciences, Queen’s University Belfast, Belfast, United Kingdom
- 3Parkinson's Disease Center and Movement Disorders Clinic, Department of Neurology, Baylor College of Medicine, Houston, TX, United States
- 4Department of Sciences and Engineering, University of Guanajuato, León, Mexico
- 5The Second Clinical Medical College, Guangdong Medical University, Zhanjiang, China
- 6Department of Neurology, The Affiliated Yuebei People’s Hospital of Shantou University Medical College, Shaoguan, China
- 7Department of Surgery of Cerebrovascular Diseases, First People's Hospital of Foshan, Foshan, China
- 8Department of Neurology, Xiapu County Hospital, Ningde, China
- 9Department of Neurology and Advanced National Stroke Center, Foshan Sanshui District People's Hospital, Foshan, China
- 10Intervention Center, Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine (Nanhai District Hospital of Traditional Chinese Medicine of Foshan City), Foshan, China
Background and purpose: Using post-treatment methods to predict functional outcomes of acute ischemic stroke (AIS) patients undergoing endovascular thrombectomy (EVT) is crucial in stroke medicine. The National Institute of Health Stroke Scale (NIHSS) score at 24 h has been widely used; however, there is a paucity of data on using earlier NIHSS scores and their association with outcome. In this study, we aimed to investigate the usage of NIHSS at 1-h time window -ultra-early neurological improvement (UENI)- as a surrogate marker associated with the functional outcomes of AIS patients treated with EVT.
Methods: We included 485 adults (≥18 years old) who underwent emergency EVT at four academic comprehensive stroke centers between 2020 and 2021. Patients with pre-EVT Alberta Stroke Program Early CT Score (ASPECTS) < 6, missing follow-up data, and missing data of the first hour NIHSS were excluded (n = 20). UENI was defined as post-EVT NIHSS reduction of 4 points or more or NIHSS as 0–1 within 1-h post-EVT. An mRS score of 0–2 after three months was defined as favorable outcome, and independent walking independence was defined as mRS of 3.
Results: A total of 465 patients were included in our final analysis. We identified 122 (26.2%) patients with UENI. While 82.79% of the patients with UENI achieved favorable functional outcomes at 3-months, only 32.36% of patients without UENI had favorable functional outcome (p < 0.0001). In addition, lower hospitalization costs were associated with patients who had UENI, compared to No-UENI (p = 0.003). A multivariate logistic regression analysis revealed that younger age (p < 0.0001), shorter last know normal to puncture time (LKNPT) (p = 0.013), higher pre-treatment ASPECTS (p = 0.039), final modified thrombolysis in cerebral infarction (mTICI) ≥2b (p = 0.002), and fewer number of EVT attempts (p = 0.002) were variables independently associated with UENI. The presence of UENI was independently associated with a better outcome OR: 7.999 (95% C.I. 4.415–14.495).
Conclusion: UENI was observed in about a quarter of patients with AIS undergoing EVT. Younger age, shorter LKNPT, higher pre-treatment ASPECTS, final mTICI≥2b, and fewer number of EVT attempts, were independently associated with UENI. The presence of UENI was independently associated with better functional outcome at 3 months.
1 Introduction
Despite recent advances in providing neurological care, stroke remains one of the major causes of mortality and patient disability worldwide (1). Endovascular thrombectomy (EVT) has significantly improved the treatment of acute ischemic stroke (AIS) and has become the standard of care in many neurological and critical care centers globally (2, 3).
As it has been reported in multiple studies, early neurological improvements can be used as a surrogate marker for predicting the functional outcome of AIS patients undergoing EVT (4–10). For instance, a surrogate for long-term outcome after EVT can be a reduction in the National Institute of Health Stroke Scale (NIHSS) score of larger than 4 points or NIHSS of 0 or 1 at 24 h (11). Therefore, identification of surrogates for early neurological improvement can be crucial in predicting longer-term outcomes of AIS patients with large vessel occlusion undergoing EVT.
In the current study, we aimed to evaluate the predictors of Ultra Early Neurological Improvement (UENI) after EVT and the relationship between UENI and outcome. We defined the Ultra Early Neurological Improvement as post-EVT NIHSS reduced by 4 points or more or NIHSS as 0–1 within 1 h after EVT (12).
2 Methods
2.1 Study design
We conducted a retrospective analysis of prospectively collected data from patients who underwent EVT at four academic comprehensive stroke centers in China from 2020 to 2021. The patients’ data was derived from the Big Data Observatory Platform for stroke in China and from the hospital data platform.
Inclusion criteria were as follows: (1) patients who underwent emergency EVT; (2) age ≥ 18 years old; (3) within 24 h from onset. Exclusion criteria were as follows: (1) pre-EVT Alberta Stroke Program Early CT Score (ASPECTS) < 6 (lower scores denotes greater parenchymal involvement), (2) missing follow-up data and, (3) missing NIHSS data within the first hour following EVT.
2.2 Data collection
We collected the baseline patient characteristics, risk factors of cerebrovascular disease, initial premorbid modified Rankin Scale (mRS), door-to-needle time (DNT), onset-to-needle time (ONT), door-to-puncture time (DPT), last know normal-to-puncture time (LKNPT), door-to-recanalization time (DRT), modified thrombolysis in cerebral infarction (mTICI) post thrombectomy. Successful reperfusion was defined as mTICI ≥2b. At least two attending neurologists collected data together. In case of discrepancies in data collection or interpretation, a consensus by the group was reached under the supervision of a senior clinician. As per the requirements by the China Stroke Center protocol, all EVT patients should have their NIHSS assessed within 1 h after EVT. The NIHSS score was assessed prospectively.
2.3 Outcome measures
The patients’ outcomes were evaluated by the mRS at 3 months after EVT. Favorable outcome was defined as mRS of 0–2. Walking independence was defined as mRS of ≤3.
2.4 Statistical analysis
The non-parametric Mann–Whitney U test was performed using the IBM SPSS 26 version (IBM-Armonk, NY) to analyze non-normally distributed continuous data, reported as medians along with the interquartile range (IQR). Normally distributed data are reported as means with corresponding standard deviations (SD) and compared using the student’s t-test. We carried out a multivariate logistic regression analysis with the backward Wald’s method and presence of “UENI” as the dependent variable to assess the effect of variables showing a statistically significant association in the bivariate analysis. The exp. (B) coefficient as odds ratios with 95% confidence interval (C.I.) were used to standardize the weight of independent variables and assess their association with the presence of UENI. The Hosmer-Lemeshow test was used to assess goodness of fit and calibration of the regression model and the Nagelkerke test to calculate the determination coefficient R2 of the model. The same procedure was used to assess the effect of UENI as independent variable in the 3-months outcome with “favorable outcome (mRS 0–2)” as the dependent variable. For the latter model, we included only variables independently associated with a favorable outcome at 3 months. Results were considered statistically significant if the p-value was less than 0.05.
2.5 Ethics approval and consent to participate
The study protocol was approved by the hospital’s institutional review board. Informed consents were waived due to the retrospective nature of the study in compliance with national laws and regulations. All procedures performed in the studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
3 Results
There were 485 patients initially, four of whom were excluded due to loss at follow-up, four patients were excluded due to pre-treatment ASPECTS score < 6, and 12 patients were excluded due to missing NIHSS data within the first hour following EVT. After the application of the inclusion and the exclusion criteria, 465 patients were enrolled in our study. Patients were divided into two groups: No-UENI (n = 343, 73.8%) and UENI (n = 122, 26.2%). There were statistically significant differences between age (p = 0.001), pre-treatment ASPECTS (p = 0.0001), vessel occlusion site (p = 0.030), DRT (p = 0.025), LKNPT (p = 0.002), mTICI of 3 (p = 0.027), number of EVT passes (p = 0.001), and symptomatic intracranial hemorrhage (sICH) (p = 0.003) between groups (Table 1). Internal carotid artery occlusion (isolated or in tandem with middle cerebral artery) were less common in patients with UENI: 35 (28.68%) vs. 135 (39.35%), (p = 0.036). In summary, patients with UENI were younger had higher pre-treatment APECTS scores, shorter DRT and LKNPT, required a lesser number of EVT passes and achieved more frequently mTICI ≥2b or 3. They also had less frequently tandem ICA + MCA-M1 occlusions and sICH. Sex and risk factors for ischemic stroke did not differ between groups.
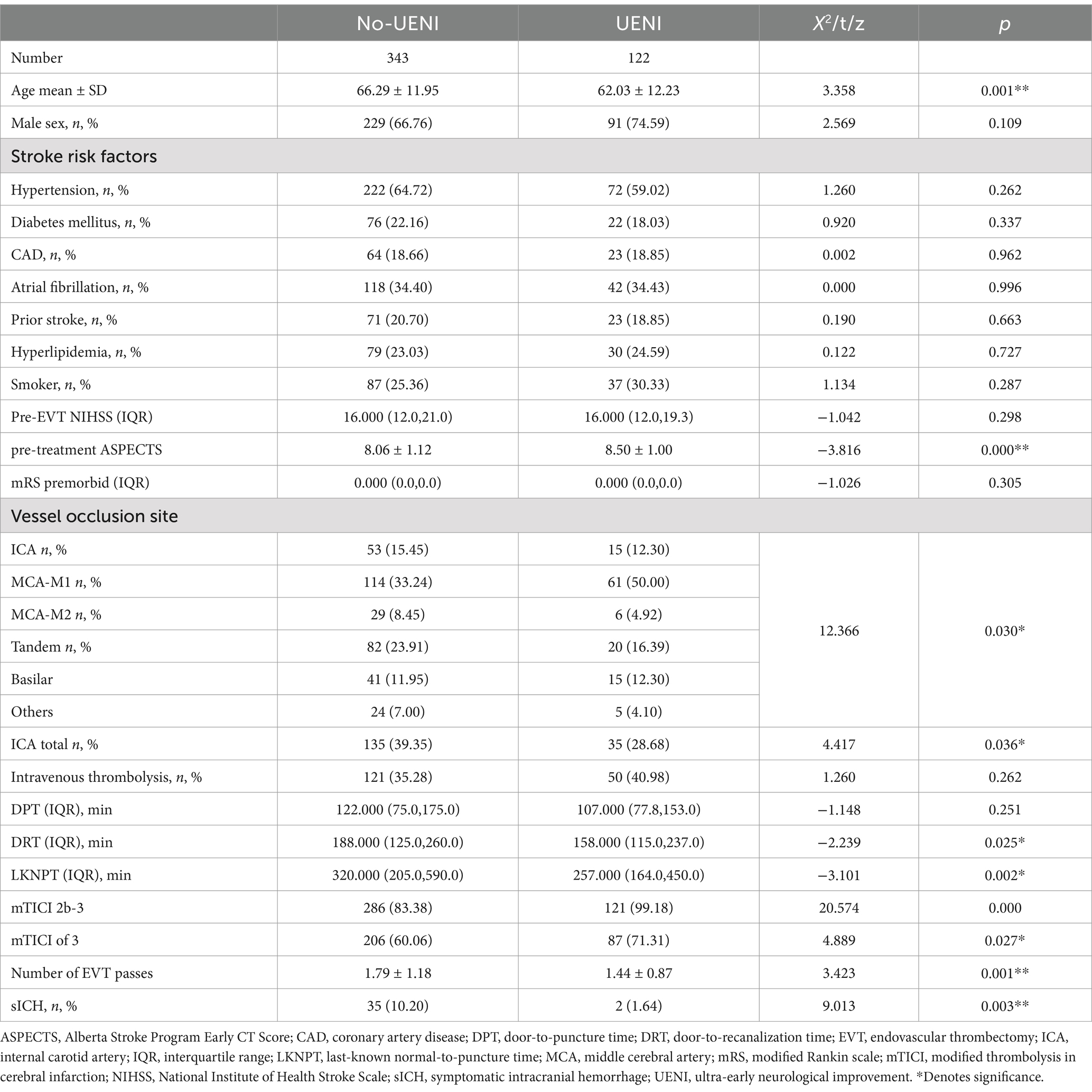
Table 1. Comparison of baseline characteristics UENI and No-UENI.
After the multivariate regression analysis, younger age, large vessel occlusion site, shorter LKNPT, higher pre-treatment ASPECTS, mTICI final≥2b, and fewer EVT attempts were independently associated with UENI (Table 2). The 90-day mRS scores distribution is shown in Supplementary Table 1.
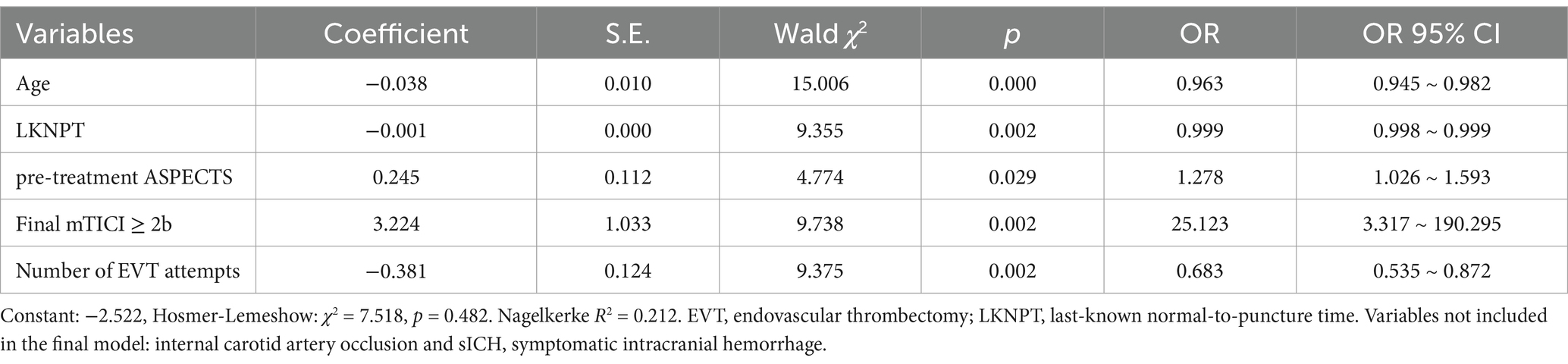
Table 2. Analysis of regression of factors associated with UENI.
Our analysis demonstrated that 82.79% of patients achieved favorable outcomes in the UENI group, while only 32.36% of patients achieved favorable outcomes in the No-UENI group. In addition, the UENI group had fewer hospitalization costs compared with the No-UENI group (median 84171.150 RMB vs. 91244.665 RMB) (Table 3). The mRS scores distribution between groups after 3 months is shown in Figure 1. In the multivariate regression analysis, age, diabetes mellitus, NIHSS score at presentation, pre-treatment APECTS, intravenous thrombolysis, final mTICI ≥2band sICH were included in the final model, along with UENI (OR: 7.999, 95% C.I. 4.415–14.495) (Table 4). Suggesting that UENI is independently associated with a better 3-month prognosis in stroke patients undergoing thrombectomy.

Table 3. Comparison of outcome of UENI and No-UENI.
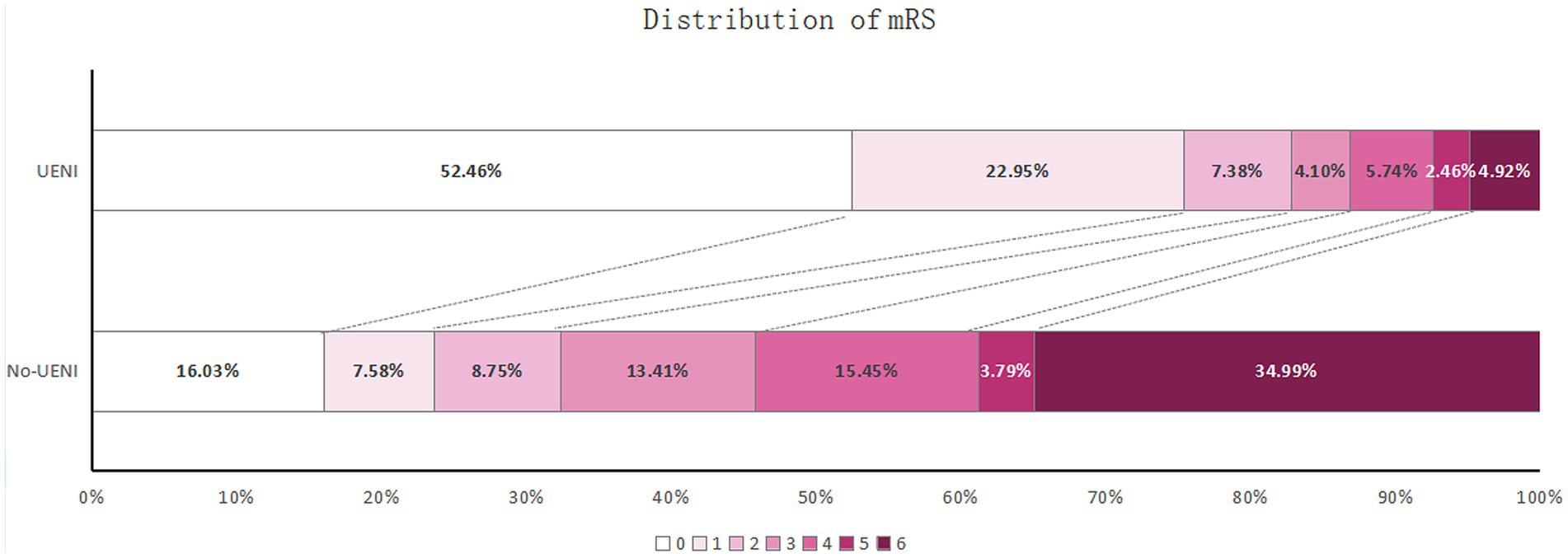
Figure 1. Distribution of 3-months mRS scores in No-UENI and UENI patients.
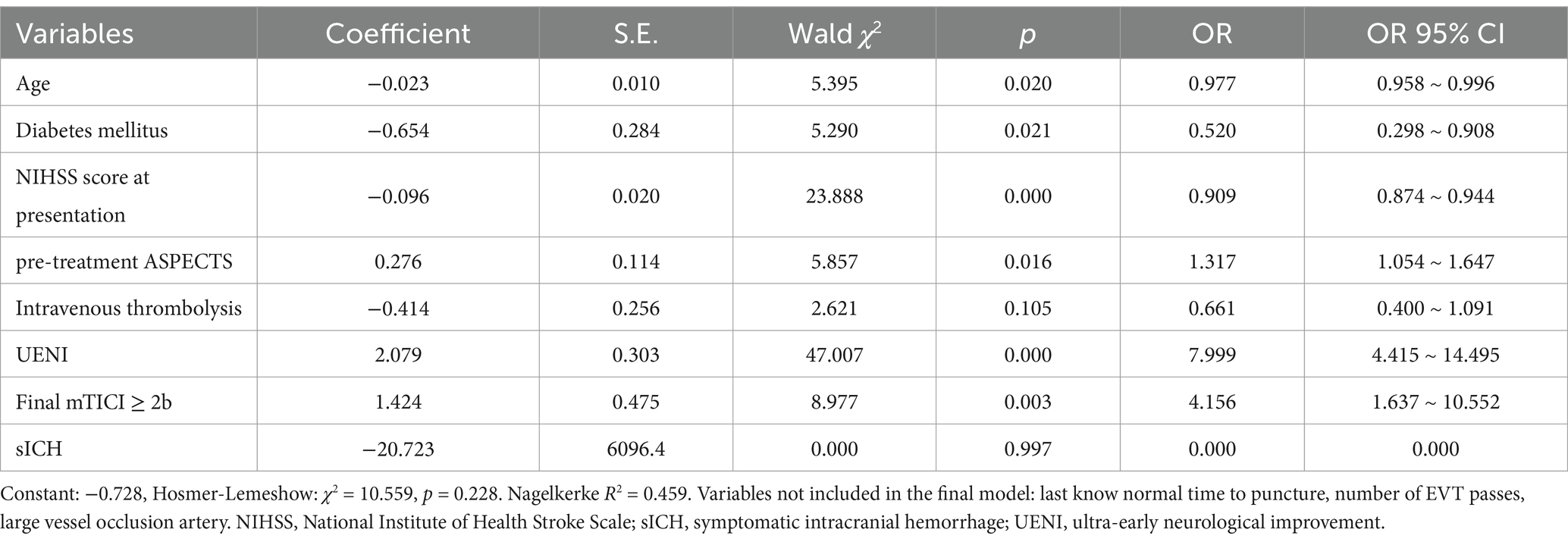
Table 4. Analysis of regression of factors associated with favorable outcome (mRS 0–2) at 3 months.
4 Discussion
In this multi-center retrospective study of 465 AIS patients, we aimed to evaluate the NIHSS score shortly following the EVT procedure in order to define a group of patients with UENI and assessed if this variable associated with a better functional outcome of AIS at follow-up. In our study, we defined UENI as a reduction of 4 or more points in post-EVT NIHSS or NIHSS as 0–1 within 1 h following EVT. We found that 26.2% of patients fulfilled the criteria. No differences in sex distribution or stroke risk factors were observed between patients with UENI and No-UENI. Moreover, no differences in the functional status (mRS at presentation) before the AIS event were observed between these groups.
Our data revealed that in the UENI group, 82.79% of patients achieved favorable outcomes, whereas favorable outcomes were only achieved in 32.36% of patients in the No-UENI group. In addition, there was less hospitalization costs associated with patients who had UENI (p = 0.003). Furthermore, UENI patients achieved favorable outcomes more frequently at 3 months, compared with the No-UENI group (p < 0.0011).
Making appropriate medical and surgical decisions in the acute phase of AIS is important, as patients’ outcomes often rely on the usage of medium and/or long-term prognosis indicators (13). Baseline factors and scores, such as NIHSS have been routinely used as outcome predictors for patients with AIS (14).
It is important to acknowledge that since the advent of EVT, post-treatment measures have gained significance and have become as important as baseline measures for predicting functional outcomes in patients with AIS (14). Therefore, it is reasonable to hypothesize that post-EVT NIHSS score can be used as an appropriate surrogate for the assessment of AIS patient prognosis (15–19).
There have been slight disagreements between different studies regarding the exact definition of early neurological improvements. However, it has been generally defined as 24-h NIHSS improvement of ≥8 or 10 points or a 24-h NIHSS score of 0–1 (2, 18, 19). In addition, other studies reported that early trajectory of the post-EVT NIHSS score within two days can be an accurate predictor of functional outcome (14). However, the significance of ultra-early post-EVT indicators, namely post-EVT NIHSS, has remained understudied (20).
A major advantage of using an NIHSS score shortly after EVT for functional outcomes is that it summarizes the effect of other variables with potential prognostic weight into a single score in order to predict the functional outcome few months later, providing a potential frame to guide clinical and surgical decisions (20). In our study, younger age at AIS presentation, less parenchymal involvement assessed with ASPECTS, shorter ischemic time determined with LKNPT, greater recanalization flow by the mTICI score and less thrombotic-occlusion burden reflected by the lower number of EVT passes, related to a UENI.
Different studies have reported more discriminative power in predicting desirable functional outcomes could be achieved by incorporating immediate post-EVT NIHSS (21). In addition, constructing several multivariable regression analysis models revealed that those models which incorporated post-EVT NIHSS were more successful in predicting the patients’ outcomes (21). Similarly, another study revealed that functional outcomes can be predicted with high accuracy using early trajectory of NIHSS score within 48 h post-EVT (14). Our study is subject to some limitations. This is a retrospective study of prospectively collected data with a relatively small sample size, which can compromise the external validity of the findings. As a retrospective study, patient data collection and recording could be at risk of recall and classification bias, despite all the efforts for standardization between all 4 centers involved in the study. Patients with an ASPECTS score below 6 were excluded. This exclusion criterion removed cases with greater parenchymal involvement, which may limit the generalizability of the results to patients with more severe AIS. Future studies with more inclusive criteria are required to generalize these findings. It is also important to consider that the current study was conducted in China, which has a significant stroke burden. Findings from this study can differ from results observed in different healthcare settings using different stroke care protocols or covering patients with different demographics. Future large-scale multi-center international studies are required to address these limitations. Despite such limitations, disseminating these findings from the current study can prompt other stroke centers across the globe to use UENI to predict functional patient outcomes. In addition, findings from the current study can be used in combination with other factors to build predictive models for the prognosis of AIS patients undergoing EVT (22–29).
5 Conclusion
Appropriate medical and surgical decisions in the acute phase of AIS rely on the usage of medium and/or long-term indicators of prognosis. We showed that younger age, higher pre-treatment ASPECTS, shorter LKNPT, mTICI 2b-3 and, fewer numbers of EVT attempts were associated with UENI. In addition, UENI related to fewer hospitalization costs and more frequent favorable outcomes at 3 months. Data obtained from our study underscores that UENI can be associated to functional outcome, but further larger studies should confirm UENI as a reliable independent surrogate of favorable functional outcome in patients with AIS undergoing EVT.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Guangdong Provincial Hospital of Integrated Traditional Chinese and Western Medicine. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin because according to the national guidelines due to the retrospective nature of the study.
Author contributions
YL: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft. MM: Data curation, Project administration, Validation, Writing – original draft, Writing – review & editing. JB-C: Data curation, Formal analysis, Writing – review & editing. JH: Data curation, Formal analysis, Investigation, Writing – review & editing. WW: Data curation, Formal analysis, Investigation, Writing – review & editing. DW: Data curation, Formal analysis, Investigation, Writing – review & editing. WY: Data curation, Formal analysis, Investigation, Writing – review & editing. JM: Data curation, Formal analysis, Investigation, Writing – review & editing. SZ: Data curation, Formal analysis, Investigation, Writing – review & editing. YS: Data curation, Formal analysis, Investigation, Writing – review & editing. YH: Data curation, Formal analysis, Investigation, Writing – review & editing. SL: Data curation, Formal analysis, Investigation, Writing – review & editing. HS: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The study was supported by Foshan Science and Technology Bureau (Grant No.2220001005122), The Foshan 14th Five-Year Priority Speciality Construction Project, The Foshan Nanhai District 14th Five-Year Priority Speciality Construction Project and Foshan Traditional Chinese Medicine Immune Health Technology Innovation Base.
Acknowledgments
The authors would like to thank all colleagues for data collection and patients for their contributions.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2025.1492013/full#supplementary-material
References
1. Campbell, BCV, and Khatri, P. Stroke. Stroke Lancet. (2020) 396:129–42. doi: 10.1016/S0140-6736(20)31179-X
2. Goyal, M, Menon, BK, van Zwam, WH, Dippel, DW, Mitchell, PJ, Demchuk, AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
3. Palaniswami, M, and Yan, B. Mechanical Thrombectomy is now the gold standard for acute ischemic stroke: implications for routine clinical practice. Interv Neurol. (2015) 4:18–29. doi: 10.1159/000438774
4. Soize, S, Fabre, G, Gawlitza, M, Serre, I, Bakchine, S, Manceau, PF, et al. Can early neurological improvement after mechanical thrombectomy be used as a surrogate for final stroke outcome? J Neurointerv Surg. (2019) 11:450–4. doi: 10.1136/neurintsurg-2018-014332
5. Katano, T, Suzuki, K, Takeuchi, M, Morimoto, M, Kanazawa, R, Takayama, Y, et al. National Institutes of Health stroke scale score less than 10 at 24 hours after stroke onset is a strong predictor of a favorable outcome after mechanical Thrombectomy. Neurosurgery. (2022) 91:936–42. doi: 10.1227/neu.0000000000002139
6. Kurmann, CC, Beyeler, M, Grunder, L, Lang, MF, Piechowiak, EI, Meinel, TR, et al. Association of the 24-hour National Institutes of Health stroke scale after mechanical Thrombectomy with early and long-term survival. Stroke: vascular and interventional. Neurology. (2022) 2:e000244. doi: 10.1161/SVIN.121.000244
7. Wang, M, Farouki, Y, Hulscher, F, Mine, B, Bonnet, T, Elens, S, et al. Early neurological improvement predicts clinical outcome after Thrombectomy for distal medium vessel occlusions. Front Neurol. (2022) 13:809066. doi: 10.3389/fneur.2022.809066
8. Kobeissi, H, Ghozy, S, Seymour, TJ, Bilgin, C, Liu, M, Kadirvel, R, et al. Patient characteristics associated with delayed neurological improvement following acute ischemic stroke: a systematic review and meta-analysis. Interv Neuroradiol. (2023) 15910199221149787. doi: 10.1177/15910199221149787
9. Wirtz, MM, Hendrix, P, Goren, O, Beckett, LA, Dicristina, HR, Schirmer, CM, et al. Predictor of 90-day functional outcome after mechanical thrombectomy for large vessel occlusion stroke: NIHSS score of 10 or less at 24 hours. J Neurosurgery JNS. (2021) 134:115–21. doi: 10.3171/2019.10.JNS191991
10. Lai, Y, Jou, E, Mofatteh, M, Nguyen, TN, Ho, JSY, Diana, F, et al. 7-day National Institutes of Health stroke scale as a surrogate marker predicting ischemic stroke patient” outcome following endovascular therapy. Transl Neurosci. (2023) 14:20220307. doi: 10.1515/tnsci-2022-0307
11. Saver, JL, Goyal, M, Bonafe, A, Diener, HC, Levy, EI, Pereira, VM, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N Engl J Med. (2015) 372:2285–95. doi: 10.1056/NEJMoa1415061
12. Heitsch, L, Ibanez, L, Carrera, C, Binkley, MM, Strbian, D, Tatlisumak, T, et al. Early neurological change after ischemic stroke is associated with 90-day outcome. Stroke. (2021) 52:132–41. doi: 10.1161/STROKEAHA.119.028687
13. Rangaraju, S, Frankel, M, and Jovin, TG. Prognostic value of the 24-hour neurological examination in anterior circulation ischemic stroke: a post hoc analysis of two randomized controlled stroke trials. Interv Neurol. (2016) 4:120–9. doi: 10.1159/000443801
14. Sajobi, TT, Menon, BK, Wang, M, Lawal, O, Shuaib, A, Williams, D, et al. Early trajectory of stroke severity predicts long-term functional outcomes in ischemic stroke subjects: results from the ESCAPE trial (endovascular treatment for small Core and anterior circulation proximal occlusion with emphasis on minimizing CT to recanalization times). Stroke. (2017) 48:105–10. doi: 10.1161/STROKEAHA.116.014456
15. Chen, Y, Diana, F, Mofatteh, M, Zhou, S, Chen, J, Huang, Z, et al. Functional and technical outcomes in acute ischemic stroke patients with hyperdense middle cerebral artery sign treated with endovascular thrombectomy. Front Neurol. (2023) 14:1150058. doi: 10.3389/fneur.2023.1150058
16. Sun, Y, Jou, E, Nguyen, TN, Mofatteh, M, Liang, Q, Abdalkader, M, et al. Predictors of futile recanalization after endovascular treatment in acute ischemic stroke: a multi-center study. Front Neurosci. (2023) 17:1279366. doi: 10.3389/fnins.2023.1279366
17. Lai, Y, Diana, F, Mofatteh, M, Nguyen, TN, Jou, E, Zhou, S, et al. Predictors of failure of early neurological improvement in early time window following endovascular thrombectomy: a multi-center study. Front Neurol. (2023) 14:1227825. doi: 10.3389/fneur.2023.1227825
18. Felberg, RA, Okon, NJ, El-Mitwalli, A, Burgin, WS, Grotta, JC, and Alexandrov, AV. Early dramatic recovery during intravenous tissue plasminogen activator infusion: clinical pattern and outcome in acute middle cerebral artery stroke. Stroke. (2002) 33:1301–7. doi: 10.1161/01.STR.0000015556.48283.74
19. Brown, DL, Johnston, KC, Wagner, DP, and Haley, EC Jr. Predicting major neurological improvement with intravenous recombinant tissue plasminogen activator treatment of stroke. Stroke. (2004) 35:147–50. doi: 10.1161/01.STR.0000105396.93273.72
20. de Campos, AM, Carvalho, A, Rodrigues, M, Figueiredo, S, Gregório, T, Costa, H, et al. Ultra-early improvement after endovascular thrombectomy and long-term outcome in anterior circulation acute ischemic stroke. J Neurol Sci. (2020) 412:116665. doi: 10.1016/j.jns.2020.116665
21. Jeong, HG, Kim, BJ, Choi, JC, Hong, KS, Yang, MH, Jung, C, et al. Posttreatment National Institutes of Health stroke scale is superior to the initial score or thrombolysis in cerebral ischemia for 3-month outcome. Stroke. (2018) 49:938–44. doi: 10.1161/STROKEAHA.117.020587
22. Ma, J, Chervak, LM, Siegler, JE, Li, Z, Mofatteh, M, Galecio-Castillo, M, et al. Postinterventional petechial hemorrhage associated with poor functional outcome after successful recanalization following endovascular therapy. Neurosurgery. (2025) 96:438–446. doi: 10.1227/neu.0000000000003098
23. Chen, Y, Zeng, X, Kwan, ATH, Mofatteh, M, Nguyen, TN, Zhou, S, et al. Sex differences in outcomes after endovascular Thrombectomy for patients with acute ischemic stroke. Eur Neurol. (2024) 87:113–21. doi: 10.1159/000539269
24. Chen, Y, Nguyen, TN, Mofatteh, M, Abdalkader, M, Wellington, J, Yan, Z, et al. Association of Early Increase in body temperature with symptomatic intracranial hemorrhage and unfavorable outcome following endovascular therapy in patients with large vessel occlusion stroke. J Integr Neurosci. (2022) 21:156. doi: 10.31083/j.jin2106156
25. Wang, Y, Yuan, X, Kang, Y, Yu, L, Chen, W, and Fan, G. Clinical predictors of prognosis in stroke patients after endovascular therapy. Sci Rep. (2024) 14:667. doi: 10.1038/s41598-024-51356-5
26. Zhang, Z, Song, C, Zhang, L, and Yang, W. Predictive modeling of short-term poor prognosis of successful reperfusion after endovascular treatment in patients with anterior circulation acute ischemic stroke. J Healthc Eng. (2022) 2022:1–9. doi: 10.1155/2022/3185211
27. Cao, R, Ye, G, Lu, Y, Wang, Y, Jiang, Y, Sun, C, et al. The predictive value of cerebral veins on hemorrhagic transformation after endovascular treatment in acute ischemic stroke patients: enhanced insights from venous collateral circulation analysis using four-dimensional CTA. Acad Radiol. (2024) 31:1024–35. doi: 10.1016/j.acra.2023.06.034
28. Haranhalli, N, Javed, K, Boyke, A, Dardick, J, Naidu, I, Ryvlin, J, et al. A predictive model for functional outcome in patients with acute ischemic stroke undergoing endovascular Thrombectomy. J Stroke Cerebrovasc Dis. (2021) 30:106054. doi: 10.1016/j.jstrokecerebrovasdis.2021.106054
Keywords: endovascular therapy, thrombectomy, acute ischemic stroke, anterior circulation, patient outcome, neurological improvement, NIHSS
Citation: Lai Y, Mofatteh M, Baizabal-Carvallo JF, He J, Wu W, Wang D, Yan W, Ma J, Zhou S, Sun Y, He Y, Li S and Sun H (2025) Identifying the predictors of ultra early neurological improvement and its role in functional outcome after endovascular thrombectomy in acute ischemic stroke. Front. Neurol. 16:1492013. doi: 10.3389/fneur.2025.1492013
Edited by:
Anna Bersano, IRCCS Carlo Besta Neurological Institute Foundation, ItalyReviewed by:
Sharon Yeatts, Medical University of South Carolina, United StatesMohammed Ahmed Akkaif, QingPu Branch of Zhongshan Hospital Affiliated to Fudan University, China
Bowen Sun, First Affiliated Hospital of Harbin Medical University, China
Copyright © 2025 Lai, Mofatteh, Baizabal-Carvallo, He, Wu, Wang, Yan, Ma, Zhou, Sun, He, Li and Sun. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuzheng Lai, bGlua2llOTM2QGZveG1haWwuY29t; Hao Sun, MTM5MjU5OTQ5NTFAMTM5LmNvbQ==
†These authors have contributed equally to this work