 Ying Liang
Ying Liang Juan Chen1
Juan Chen1
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol., 24 February 2025
Sec. Neurological Biomarkers
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1488726
This article is part of the Research TopicGenetic Insights and Diagnostic Innovations in Cerebrovascular and Cerebrospinal Fluid DisordersView all 5 articles
Ischemic stroke is a leading cause of mortality and morbidity globally. Prompt intervention is essential for arresting disease progression and minimizing central nervous system damage. Although imaging studies play a significant role in diagnosing ischemic stroke, their high costs and limited sensitivity often result in diagnostic and treatment delays. Blood biomarkers have shown considerable promise in the diagnosis and prognosis of ischemic stroke. Serum markers, closely associated with stroke pathophysiology, aid in diagnosis, subtype identification, prediction of disease progression, early neurological deterioration, and recurrence. Their advantages are particularly pronounced due to their low cost and rapid results. Despite the identification of numerous candidate blood biomarkers, their clinical application requires rigorous research and thorough validation. This review focuses on various blood biomarkers related to ischemic stroke, including coagulation and fibrinolysis-related factors, endothelial dysfunction markers, inflammatory biomarkers, neuronal and axonal injury markers, exosomes with their circular RNAs and other relevant molecules. It also summarizes the latest methods and techniques for stroke biomarker detection, aiming to provide critical references for the clinical application of key stroke biomarkers.
Stroke remains one of the leading causes of disability and mortality worldwide. According to the World Health Organization (WHO), stroke is the second leading cause of death globally, accounting for approximately 5.5 million deaths annually, with about half of the survivors experiencing long-term disability (1, 2). Among these, ischemic stroke constitutes approximately 80% of all stroke cases, primarily caused by the obstruction of cerebral blood vessels, leading to ischemia and hypoxia of brain tissue, and resulting in irreversible neuronal damage (3). Early diagnosis and timely treatment are crucial for reducing the disability and mortality rates among ischemic stroke patients (4, 5). Currently, the primary clinical treatment strategy for ischemic stroke is intravenous thrombolysis within the “golden window” to restore blood perfusion. However, some patients present with subtle or atypical symptoms, and the specificity of imaging-based assessments remains limited, leading to misdiagnosis, missed diagnoses, and delays in clinical decision-making. Therefore, there is an urgent need to establish novel laboratory-based rapid auxiliary diagnostic strategies (6).
Biomarkers are defined as measurable indicators that objectively reflect normal or pathological physiological processes or predict and assess responses to therapeutic interventions. In the context of ischemic stroke, biomarkers can provide insights into the pathophysiological mechanisms triggered by cerebrovascular occlusion, including inflammation, oxidative stress, and neuronal injury. They not only facilitate early diagnosis and subtype differentiation but also serve as crucial tools for disease assessment, prognosis prediction, and individualized therapeutic decision-making (7). Compared to traditional imaging-based diagnostics, biomarker detection in blood or other bodily fluids is generally more cost-effective, technically less complex, and offers the potential for dynamic monitoring, making it an indispensable tool in clinical practice (8).
The study of stroke biomarkers has been extensively discussed in multiple reviews, yet existing literature often lacks a comprehensive evaluation of their clinical applications and associated challenges. This review aims to systematically summarize the currently identified biomarkers for ischemic stroke, evaluate their research status and detection methodologies, and explore unresolved critical issues and future research directions.
Acute ischemic stroke (AIS) primarily results from atherosclerosis, cardioembolism, small vessel disease, and other rare causes, such as hypercoagulable states, arterial dissection, and genetic disorders. Among these, atherosclerosis is the most common mechanism, characterized by lipid deposition, chronic inflammation, and endothelial dysfunction, leading to the formation of atherosclerotic plaques. Plaque rupture can trigger platelet aggregation and coagulation cascade reactions, ultimately leading to thrombosis and acute occlusion of cerebral arteries, resulting in symptoms such as cerebral ischemia, neuronal necrosis, and functional impairment (9).
The pathogenesis of ischemic stroke involves multiple pathological processes, among which thrombosis is a key mechanism (10). The rupture of atherosclerotic plaques exposes the subendothelial matrix, leading to platelet activation and coagulation factor recruitment, thereby triggering the coagulation cascade. This process results in thrombus formation and vascular occlusion. The coordinated interaction between platelet activation and fibrin formation is a critical pathological event, along with abnormal activation of the coagulation system. Glial cells also play a crucial role in cerebral ischemia (11). The activation of microglia and astrocytes exhibits spatiotemporal specificity. In the early phase, microglia predominantly exhibit a pro-inflammatory phenotype (M1), concurrently inducing astrocytes to transition into a pro-inflammatory subtype (A1). As the disease progresses, microenvironmental signals drive these cells toward an anti-inflammatory phenotype (M2 and A2), thereby facilitating tissue repair and neuronal functional recovery. During neuronal injury, astrocytes release glial fibrillary acidic protein (GFAP), which is closely associated with the severity of neuronal damage.
Within hours following a stroke, the ischemic brain tissue rapidly initiates an inflammatory response. Perivascular microglia and macrophages release various cytokines, including tumor necrosis factor-alpha (TNF-α) and interleukin-6. Neutrophil infiltration occurs within minutes of ischemic stroke onset and peaks between 24 and 72 h. Within 48 h, monocytes and lymphocytes are also recruited to the brain (12). Subsequently, activated microglia, macrophages, and infiltrating leukocytes release additional inflammatory mediators, including TNF-α and interleukins (IL-1β, IL-6), thereby initiating a sustained inflammatory response through the secretion of IL-8 and IL-6. This inflammatory cascade leads to increased levels of fibrinogen and C-reactive protein (CRP), as well as the upregulation of adhesion molecules, including members of the immunoglobulin superfamily such as intercellular adhesion molecule-1 (ICAM-1) and vascular cell adhesion molecule-1 (VCAM-1) (13). Additionally, pro-inflammatory factors enhance matrix metalloproteinase (MMP) activity, further disrupting the blood–brain barrier (BBB), exacerbating cerebral edema, and promoting neuronal damage. Notably, MMP-9 levels significantly increase following stroke, contributing to extracellular matrix degradation and leukocyte infiltration, thereby amplifying the inflammatory response (Figure 1).
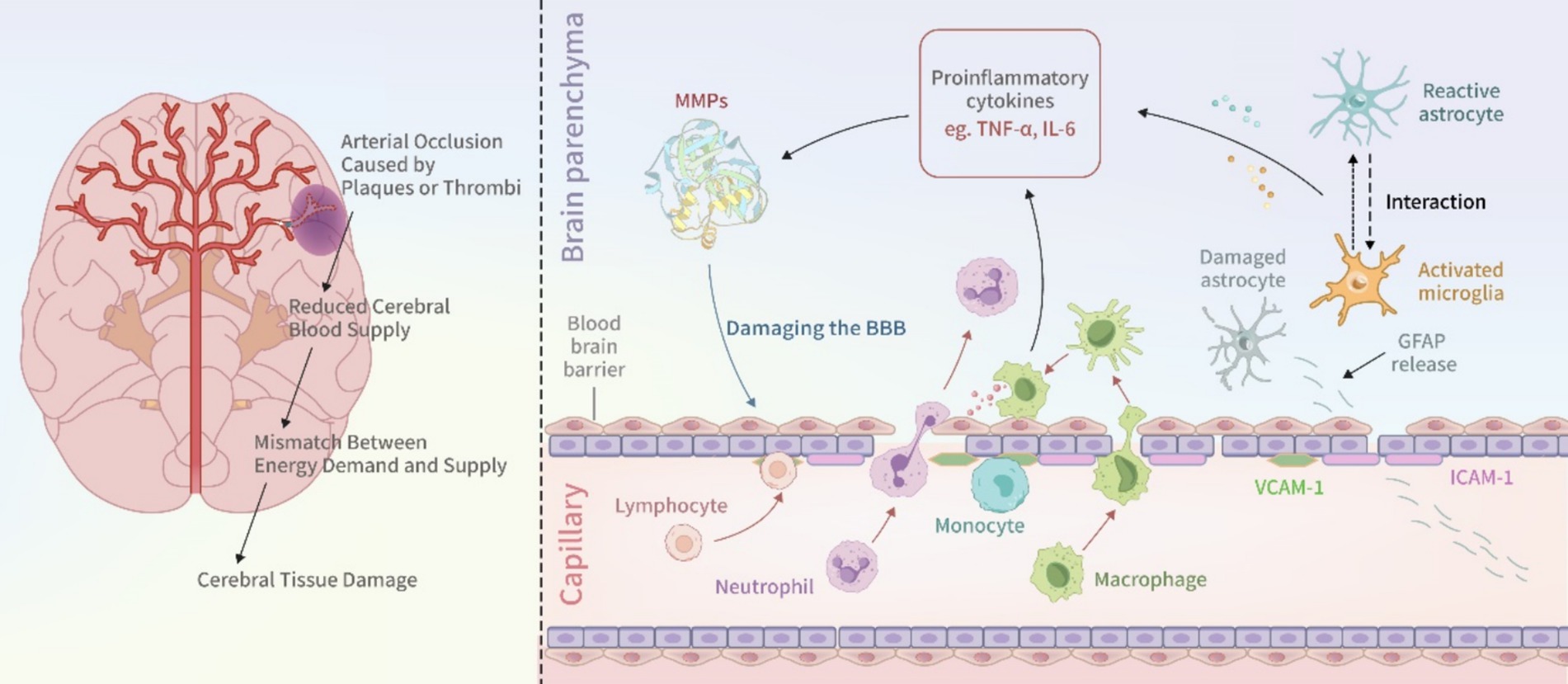
Figure 1. Pathogenesis of ischemic stroke.
Thus, the pathogenesis of ischemic stroke involves multiple pathological pathways and bioactive molecules, many of which can serve as diagnostic and prognostic biomarkers. Based on their respective pathophysiological roles, these biomarkers can be broadly categorized into coagulation and fibrinolysis-related factors, endothelial dysfunction markers, inflammatory biomarkers, neuronal and axonal injury markers, and other relevant molecules (Table 1).
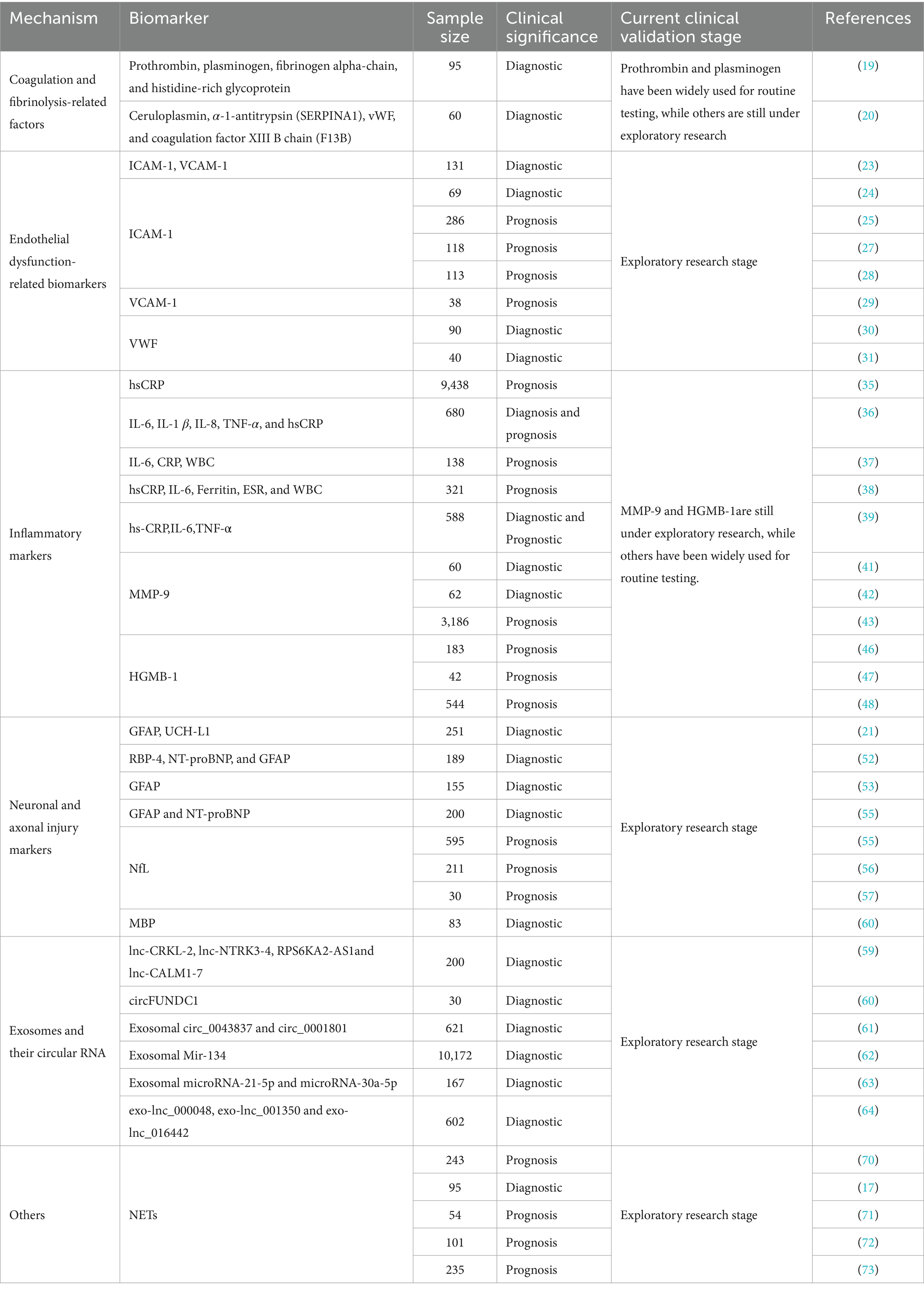
Table 1. Biomarkers for stroke detection.
It is important to note that the pathophysiological processes of ischemic stroke exhibit distinct temporal dynamics. Specifically, in the hyperacute phase (<6 h), acute phase (6–72 h), and subacute phase (>72 h), different blood biomarkers display varying sensitivities and specificities (14). Therefore, the temporal dependency of biomarker expression must be carefully considered in both research and clinical applications to achieve more precise diagnostic and prognostic evaluations. For example, IL-6 levels begin to rise within hours after stroke onset, and persistently elevated IL-6 levels in the subacute phase may indicate ongoing inflammatory injury (15, 16). Similarly, GFAP is released progressively within 12 h post-stroke, making it a valuable biomarker for predicting intracranial pathology in both the hyperacute and acute phases. Furthermore, neutrophil extracellular traps (NETs) exhibit rapid fluctuations following thrombolysis or mechanical thrombectomy, providing insights into reperfusion status and aiding in the identification of futile recanalization (17).
The coagulation and fibrinolysis systems are pivotal in the pathophysiology of stroke. Detecting related factors is vital for the early diagnosis and treatment of stroke. Biomarkers such as thrombin-antithrombin complex (TAT), tissue plasminogen activator inhibitor complex (t-PAIC), activated partial thromboplastin time (APTT), prothrombin time (PT), fibrinogen (FIB), D-dimer, and fibrin degradation products (FDP) reflect dynamic changes in thrombosis and fibrinolytic activity, aiding clinical decision-making. Elevated D-dimer levels indicate active fibrinolysis, commonly used to assess thrombus burden and prognosis in stroke patients. Ohara et al. highlighted that serum D-dimer assists in diagnosing cryptogenic stroke and secondary prevention, with continuous monitoring enhancing the efficacy of antithrombotic treatment in cryptogenic stroke (18). Lee et al., through proteomics, identified four candidate biomarkers—prothrombin, plasminogen, fibrinogen alpha chain, and histidine-rich glycoprotein—with AUC values over 0.9, confirming their diagnostic value related to coagulation mechanisms (19). Misra et al. used SWATH-MS-based proteomics to identify ceruloplasmin, α-1-antitrypsin (SERPINA1), von Willebrand factor (vWF), and coagulation factor XIII B chain (F13B) as effective biomarkers for distinguishing total stroke, ischemic stroke, and intracerebral hemorrhage (ICH) from healthy controls (20). Bioinformatics suggested common pathways in stroke cases, including complement and coagulation cascades, platelet degranulation, immune processes, and acute phase reactions (21).
Endothelial dysfunction can lead to dysregulation of vascular endothelial cell function, further exacerbating cerebral blood flow reduction and tissue damage.
ICAM-1 and VCAM-1 belong to the immunoglobulin superfamily and are primarily expressed on the surface of endothelial cells. Following ischemic injury, elevated levels of pro-inflammatory cytokines induce the expression of ICAM-1 and VCAM-1 in the endothelial cells of the blood–brain barrier (BBB), thereby mediating neuroinflammation (22). Elevated levels of ICAM-1 and VCAM-1 have been detected in the blood and infarct regions of stroke patients (23). Studies suggest that ICAM-1 may serve as a potential prognostic biomarker for AIS. Nielsen et al. evaluated ICAM-1 levels in AIS patients and found that they were significantly elevated within <8 h of stroke onset, whereas S100B and E-selectin levels showed no significant changes (24). Additionally, Wang et al. reported that the sensitivity and specificity of serum ICAM-1 in predicting AIS were 74 and 76%, respectively (25). Moreover, the rs5498 polymorphism of ICAM-1 has been associated with an increased risk of ischemic stroke in Caucasian populations (26). Furthermore, the combined detection of ICAM-1 and CRP has been shown to predict the 3-month prognosis of AIS patients (27). However, some studies have failed to establish a significant correlation between soluble ICAM-1 and stroke prognosis (28). In contrast, VCAM-1 levels have been proposed as a predictor of stroke prognosis, although they do not correlate with infarct volume or disability severity (29). Overall, the diagnostic and prognostic value of ICAM-1 and VCAM-1 in ischemic stroke remains incompletely understood, necessitating further research and clinical validation.
VWF is a multimeric glycoprotein secreted by endothelial cells and megakaryocytes, primarily involved in platelet adhesion and blood coagulation. Sabbah et al. found that serum VWF levels were significantly elevated in patients with AIS compared to control groups. Elevated plasma VWF levels were observed in patients with acute ischemic atherosclerotic stroke, suggesting that serum VWF levels could serve as a biomarker for AIS, particularly for the atherosclerotic subtype (30).
Sharma et al., through proteomic studies, also identified VWF as useful in distinguishing total stroke, ischemic stroke, and intracerebral hemorrhage (ICH) from healthy controls. Changes in its concentration may lead to endothelial dysfunction and are associated with inflammation and endothelial dysfunction in AIS patients, making it a novel candidate protein (31). Steliga et al. also summarized that VWF could serve as a diagnostic biomarker for AIS (32). Baez et al. included 12 articles involving blood combinations of stroke protein biomarkers and proposed a new biomarker combination model (NR2 + GFAP + MMP-9 + VWF + S100β) involving VWF for the early diagnosis of ischemic stroke subtypes (33). Moreover, VWF is considered an effective biomarker for predicting the risk of death in ischemic stroke patients. Kawano et al. found that elevated VWF levels are an independent predictor of mortality within 1 year after stroke onset (34). Further research on these biomarkers and their roles in the pathophysiology of ischemic stroke is crucial for improving patient prognosis and developing targeted therapeutic strategies.
C-reactive protein (CRP), as an acute-phase protein, serves not only as an indicator of systemic inflammation but also as a crucial biomarker for evaluating prognosis post-stroke. Elevated CRP levels are associated with poor outcomes in stroke patients and reflect the systemic inflammatory state (35). IL-6 plays a key role in immune regulation within the central nervous system, while TNF-α exacerbates brain tissue damage by inducing apoptosis and promoting inflammatory responses (36).
Lasek-Bal et al. reported that IL-6 levels on the first day after stroke could predict acute neurological and functional status, while increased CRP and leukocyte counts were associated with worse acute stroke prognosis (37). Reiche et al. studied two composite indices reflecting inflammation levels—INFLAM Index 1 (comprising the z-scores of hsCRP, IL-6, ferritin, ESR, and WBC) and INFLAM Index 2 (derived by subtracting the z-score of 25(OH)D from INFLAM Index 1 and adding the z-scores of iron and TSP). These indices demonstrated significant predictive value for AIS in both healthy volunteers and AIS patients, with AUC values of 0.851 and 0.870, respectively. They also identified redox imbalance related to IL-6 signaling as a potential target for preventing short-term mortality in AIS (38). Ma et al. developed diagnostic and prognostic models for ischemic stroke using inflammatory markers such as hs-CRP, IL-6, and TNF-α, which were validated in additional cohorts (39).
Matrix metalloproteinase-9 (MMP-9) plays a crucial role in degrading components of the extracellular matrix, activating pro-inflammatory cytokines, and compromising the integrity of the blood–brain barrier (BBB). The activation of M1-polarized microglia has been shown to upregulate MMP-9 expression, leading to BBB disruption and ischemic brain injury (40). Abdelnaseer et al. reported that serum MMP-9 levels within 24 h of stroke onset were significantly correlated with clinical stroke severity (41). Similarly, Weekman et al. demonstrated a positive association between MMP-9 levels and infarct volume, with the strongest correlation observed within the first 6 hours post-stroke. Notably, MMP-9 is considered the only biomarker capable of precisely predicting the final infarct volume, where higher MMP-9 expression is linked to larger infarct areas (42). Further research by Zhong et al. revealed that elevated serum MMP-9 levels in the acute phase of ischemic stroke were positively correlated with mortality and severe disability within 3 months post-stroke (43). These findings suggest that targeted inhibition of MMP-9 activity may serve as a promising therapeutic strategy to mitigate brain injury and improve stroke prognosis (44).
High mobility group box 1 (HMGB1) has been identified as a potential diagnostic and prognostic biomarker for ischemic stroke (45). A study by Tsukagawa demonstrated that serum and plasma HMGB1 levels were significantly elevated in patients with ischemic stroke (46). Moreover, Sapojnikova et al. reported a strong correlation between MMP-9 and HMGB1 levels in stroke patients, with both biomarkers closely associated with poor prognosis (47). Similarly, Shen et al. found that elevated serum HMGB1 levels served as a reliable predictor of AIS recurrence (48). However, it is important to note that HMGB1 exhibits a complex biphasic role in the pathogenesis and progression of ischemic stroke. In the hyperacute and acute phases (within 4–5 days post-stroke), HMGB1 functions as a pro-inflammatory mediator, exacerbating neuronal death and blood–brain barrier disruption. Conversely, in the late acute, subacute, and chronic phases (>3 weeks post-stroke), HMGB1 contributes to vascular remodeling and neurofunctional recovery (49).
Ischemic stroke leads to increased blood–brain barrier permeability and the release of neuronal and axonal injury biomarkers, such as GFAP, neurofilament light chain protein (NFL), and S100 proteins. These markers are rapidly released into the blood following brain tissue injury, with their levels accurately reflecting the extent of brain damage and providing crucial prognostic information. Luger et al. conducted a study to assess the diagnostic accuracy of serum GFAP and ubiquitin carboxy-terminal hydrolase L1 (UCH-L1) concentrations, measured using ELISA, in differentiating between acute cerebral hemorrhage and ischemic stroke. The results indicated that the area under the curve (AUC) for GFAP was 0.866, surpassing the 0.590 AUC for UCH-L1 (21). Bustamante et al. validated a panel of blood biomarkers, including RBP-4, NT-proBNP, and GFAP, which distinguished IS from ICH with moderate accuracy at 100% specificity (50). Kalra et al. tested the diagnostic accuracy of GFAP in a prospective cohort of stroke patients in India. Using the highly sensitive SIMOA technology, GFAP concentrations were measured within 12 h of admission in acute stroke patients. ROC analysis identified an optimal GFAP threshold of 0.57 μg/L for distinguishing intracerebral hemorrhage from ischemic stroke and stroke mimic conditions (AUC 0.871 [95% CI 0.810–0.933], p < 0.001) (51). Recently, a systematic review confirmed the high diagnostic accuracy of blood GFAP levels as a discriminative test for cerebral hemorrhage and ischemic stroke (52). Additionally, Lee et al. developed a time-resolved fluorescence lateral flow immunoassay (TRF-LFIA) utilizing europium nanoparticle (EuNP)-conjugated specific monoclonal antibodies targeting NT-proBNP and GFAP for simultaneous quantification. The combination of GFAP and NT-proBNP was determined to be the most effective biomarker pair for differentiating IS from HS based on an algorithm (53). In summary, the use of blood biomarkers, particularly GFAP, holds promise for the diagnosis and differentiation of ischemic stroke and cerebral hemorrhage. Further research is necessary to validate these findings and establish standardized protocols for measuring acute stroke biomarkers.
Neurofilament light chain (NfL) levels have been shown to be a robust biomarker in cerebrospinal fluid (CSF) for neuronal damage and neurodegeneration. Several studies have demonstrated the potential of NfL as a blood biomarker for ischemic stroke. Sanchez et al. conducted a systematic review and meta-analysis, including 19 studies that reported serum/plasma NfL values from a total of 4,237 different stroke patients, to evaluate the utility of blood NfL as a diagnostic, prognostic, and monitoring biomarker for stroke. They found that blood NfL levels varied significantly across three different time periods: acute (0–7 days), subacute (9–90 days), and chronic (>90 days) phases of stroke, with a sharp peak observed in the early subacute phase, 14 to 21 days post-stroke. Additionally, blood NfL can serve as a diagnostic biomarker for differentiating AIS from transient ischemic attacks and other cerebrovascular subtypes (54). Pedersen et al. included 595 ischemic stroke cases in their study to investigate the correlation between serum NfL concentrations at different time points post-stroke. They found that NfL could predict neurological and functional outcomes in both the acute phase (range 1–14 days, median 4 days) and the long-term (cases followed up after 3 months) (55). Uphaus et al. also highlighted NfL as a biomarker for predicting cerebrovascular function 90 days post-ischemic stroke (56). Barba et al. explored the relationship between serum NfL concentrations and clinical outcomes in patients with AIS, finding that patients with higher NfL levels showed less clinical improvement post-treatment. In patients with moderate to severe AIS, serum NfL levels were correlated with clinical and radiological scores at different time points and were predictive of short-term and intermediate-term clinical outcomes (57).
Myelin basic protein (MBP) is a membrane protein synthesized by oligodendrocytes that plays a crucial role in stabilizing myelin structure and is highly specific to neural tissue. In cases of brain injury, myelin damage leads to the release of MBP into the bloodstream, resulting in elevated serum levels. The concentration of MBP in the blood serves as an indicator of central nervous system injury. Studies have shown that serum MBP levels in patients with AIS are positively correlated with infarct volume, suggesting its potential as a biomarker for brain injury assessment (58).
Exosomes are nanoscale extracellular vesicles secreted by most cells, capable of crossing the blood–brain barrier and transferring various bioactive molecules between cells. They facilitate intercellular communication and are closely associated with the occurrence and progression of various diseases. Exosomes, particularly the functional substances they carry, play a crucial role in the pathogenesis and recovery process of ischemic stroke by affecting the neurovascular unit. Following an ischemic stroke event, various types of cells, including peripheral blood cells, endothelial cells, and brain cells, release exosomes. These exosomes can traverse the blood–brain barrier and be detected in cerebrospinal fluid and peripheral blood. Consequently, exosomes are increasingly recognized as potential biomarkers for the early diagnosis and prognosis of IS.
Xu et al. demonstrated that long non-coding RNAs (lncRNAs) such as lnc-CRKL-2, lnc-NTRK3-4, RPS6KA2-AS1, and lnc-CALM1-7, isolated from the serum of acute stroke patients, are significantly elevated (59). Bai et al. isolated exosomes from serum samples of IS patients and normal controls, finding elevated expression of circFUNDC1 in exosomes derived from IS patients’ serum. Receiver operating characteristic (ROC) analysis revealed an area under the curve (AUC) of 0.882 for circFUNDC1, indicating its high sensitivity and specificity as a diagnostic biomarker for IS (60). Xiao et al., through exosome circular RNA sequencing, large-sample validation, and diagnostic model construction, identified exosomal circ-0043837 and circ-0001801 as independent predictors of large-artery atherosclerosis (LAA) stroke. These circular RNAs showed significantly higher expression levels compared to controls, with diagnostic accuracies of AUC = 0.89 and AUC = 0.91, respectively, surpassing the diagnostic performance of plasma circular RNAs (61). Zhou et al. found that levels of miR-134 and miR-223 in exosomes from IS patients were significantly higher than those in non-ischemic stroke patients. Additionally, these levels correlated positively with NIHSS scores (r = 0.65, p < 0.01) and infarct volume (r = 0.68, p < 0.01), suggesting that miR-134 and miR-223 have potential diagnostic value for assessing the occurrence and severity of IS (62).
Exosomes are not only useful for the early diagnosis of IS but also help distinguish between different stages of the disease. Wang et al. found that, compared to controls, plasma exosomes in subacute and recovery-phase stroke patients showed significantly elevated levels of miRNA-21-5p, while exosomal miR-30a-5p was significantly higher in ultra-early stroke patients but lower than in controls during the acute phase. Furthermore, early diagnosis of large-artery atherosclerosis (LAA), which is associated with the worst prognosis, is particularly crucial (63). Zhang et al. observed significant increases in exosomal lnc_000048, lnc_001350, and lnc_016442 in LAA patients, with levels rising with stroke severity and showing better predictive capability for prognosis than NIHSS scores (64).
In recent years, multiple studies have demonstrated significant alterations in the expression of specific exosomal miRNAs in patients with AIS. Several miRNAs exhibit upregulated expression in AIS, including exosomal miR-212/132, miR-21, miR-9, miR-124, miR-134, and miR-223. In contrast, the expression level of exosomal miR-126 is downregulated in AIS patients (62, 65–68). These distinct miRNA expression patterns not only provide insights into the pathophysiological mechanisms of AIS but also hold potential clinical value as biomarkers for early diagnosis and disease assessment.
NETs are web-like structures released by neutrophils, primarily composed of free DNA, nucleosomes, and citrullinated histone H3 (citH3). NETs play a crucial role in the onset and progression of AIS. Studies have shown that NETs exacerbate early blood–brain barrier (BBB) disruption in AIS, increasing its permeability and potentially facilitating inflammatory cell infiltration, thereby aggravating neuronal damage (69). Research by Vallés et al. revealed that plasma NET levels in AIS patients were significantly higher than those in healthy individuals (70). Similarly, Lim et al. reported a marked increase in NET levels in AIS patients, and receiver operating characteristic (ROC) curve analysis demonstrated that the area under the curve (AUC) for double-stranded DNA (dsDNA) in early AIS diagnosis reached 0.859, suggesting its potential as an early diagnostic biomarker for AIS (17). Beyond its diagnostic implications, NETs are also closely associated with AIS severity and prognosis. Studies indicate that NET levels in thrombi and peripheral blood can reflect stroke severity and effectively predict short-term patient outcomes (71). Additionally, NETs may influence treatment responses in AIS. Evidence suggests that NETs could serve as prognostic biomarkers for futile recanalization following intravenous thrombolysis or mechanical thrombectomy. Arnaud et al. found that NETs were universally present in AIS thrombi, with all patients exhibiting NET-containing clots. High NET content in thrombi was correlated with failed recanalization, prolonged procedure time, and poorer stroke outcomes as assessed by the National Institutes of Health Stroke Scale (NIHSS) and modified Rankin Scale (mRS) scores (72). Moreover, analysis by Chen et al. demonstrated that the enrichment of NETs affects thrombus mechanical properties, potentially influencing the success rate of mechanical thrombectomy. Lower NET levels were significantly associated with higher rates of initial vascular recanalization (73).
To provide a more intuitive overview of these biomarkers and their roles, we present a summary table outlining their specific functions and recent research progress in ischemic stroke (Table 1).
Currently, common diagnostic methods for stroke biomarkers in clinical practice include enzyme-linked immunosorbent assay (ELISA), quantitative real-time PCR (qPCR), liquid chromatography-tandem mass spectrometry (LC-MS/MS), immunoturbidimetry, next-generation sequencing (NGS), single-molecule array (Simoa), and biosensing technologies (Figure 2). This paper summarizes the advantages, disadvantages, and clinical applications of various detection methods (Table 2).
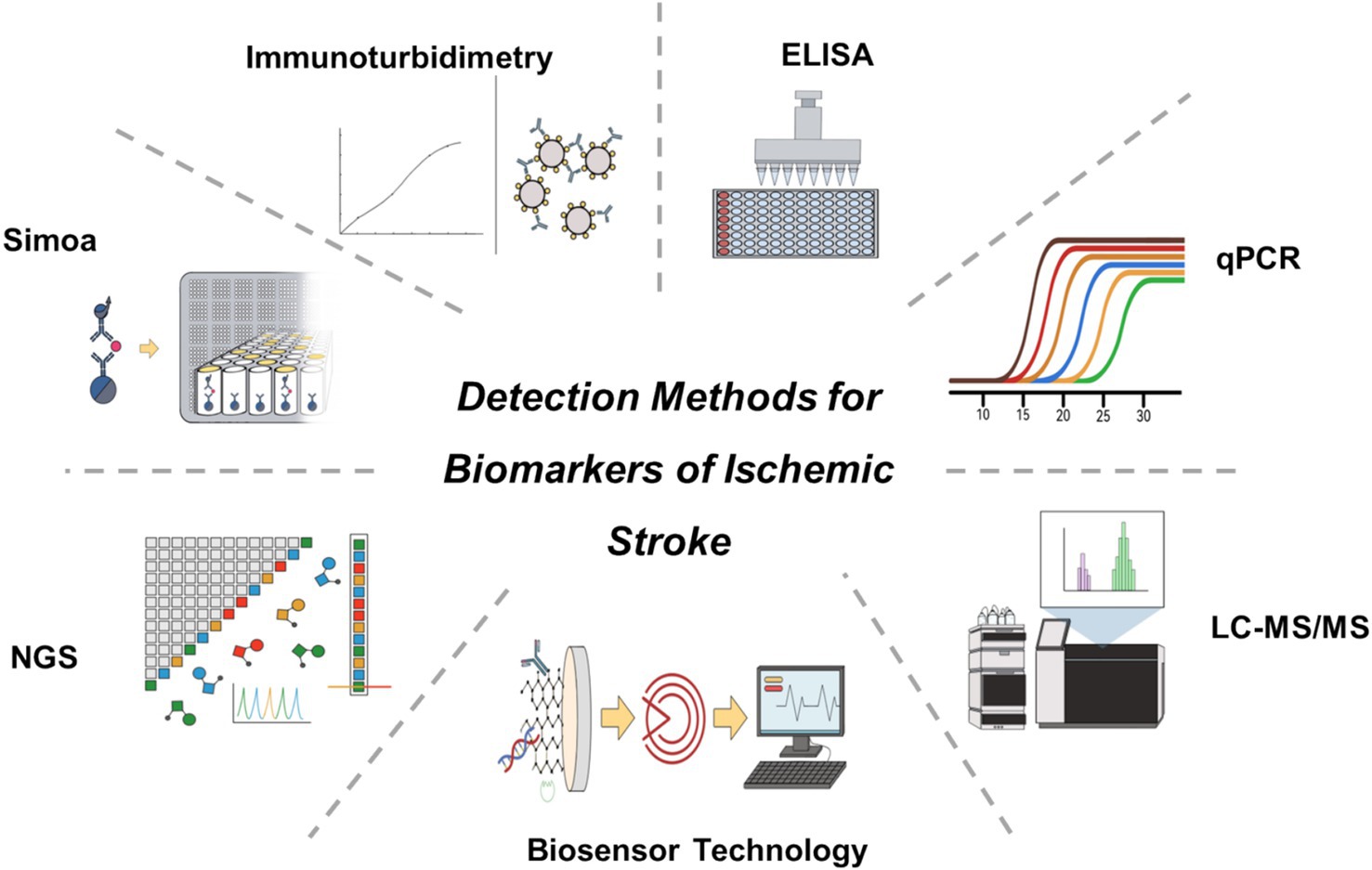
Figure 2. Common detection methods for ischemic stroke-related biomarkers.

Table 2. Comparison of detection methods for ischemic stroke-related biomarkers.
ELISA is a widely used method for detecting protein levels in body fluids, characterized by high sensitivity and specificity. It utilizes antigen–antibody reactions, with enzyme-labeled antibodies to detect target proteins. ELISA is suitable for detecting various stroke-related biomarkers, such as CRP (74–76), IL-6 (43, 74, 75), TNF-α (75, 76), ICAM-1, MMP-9 (43, 75), VCAM-1 (77, 78), GFAP53 (79, 80), and S10053 (81). The advantages of ELISA include simplicity of operation, good reproducibility, and the ability to detect multiple samples simultaneously. However, its disadvantages are longer detection time and higher costs.
qPCR is a technique used to quantify RNA levels by labeling PCR amplification products with fluorescent dyes and monitoring the fluorescence signal changes in real-time. It is suitable for detecting genetic biomarkers like miRNA and lncRNA. The advantages of qPCR include high sensitivity, strong specificity, and accurate quantification, capable of detecting low-abundance RNA molecules (82–84). However, qPCR requires high-quality RNA samples, is complex to operate, and has high costs.
LC–MS/MS combines the separation capabilities of liquid chromatography with the high sensitivity of mass spectrometry. It is used to detect metabolites such as fatty acid derivatives, amino acids, and oxidative stress markers like 3-nitrotyrosine nitrated fibrinogen (85), 8-iso-PGF2α (86), and MDA (87). The advantages of LC–MS/MS are high sensitivity, strong specificity, and the ability to detect multiple metabolites simultaneously, making it a key tool in metabolomics research. However, LC–MS/MS equipment is expensive, the operation is complex, and it requires professional technicians.
Immunoturbidimetry measures the turbidity changes in a solution due to antigen–antibody complex formation, quantifying protein biomarkers in blood. It is suitable for detecting coagulation and fibrinolysis system-related factors such as D-dimer, FIB, TAT, t-PAIC, APTT, PT, FDP, and SAA (88, 89). The advantages of immunoturbidimetry include rapid detection, ease of operation, and lower costs, but its sensitivity and specificity are relatively lower.
NGS is a high-throughput DNA sequencing technology used for comprehensive analysis of genomes, transcriptomes, and epigenomes. It can detect DNA methylation states and RNA expression profiles, suitable for studying complex genetic biomarkers (90, 91). The advantages of NGS include high throughput, strong sensitivity, and specificity, and the ability to detect thousands of genes and their regulatory elements simultaneously. However, NGS equipment and operating costs are high, data analysis is complex, and it requires professional bioinformatics support.
Simoa is a breakthrough in biomarker detection due to its extremely high sensitivity and specificity. This technology combines single-molecule immunocapture with fluorescence detection, capable of detecting extremely low concentrations of biomarkers, making it advantageous in stroke biomarker detection. Simoa’s core lies in its ability to capture and detect single target molecules in each reaction well, significantly enhancing detection sensitivity. Compared to traditional ELISA, Simoa can detect biomarkers at femtomolar levels. Simoa has been used to detect neuronal injury markers such as GFAP, NFL, and S100, which are rapidly released into the blood after brain tissue injury, providing crucial information for prognosis assessment (92–94).
Recent research has expanded the application of Simoa in stroke biomarker detection, developing multiplex detection platforms for simultaneous detection of multiple inflammatory and neuronal injury markers, improving detection efficiency and data reliability. Onatsu et al. utilized Simoa to analyze the NfL levels in 136 patients with AIS, discovering that the presence and extent of axonal injury estimated by NfL were correlated with the final infarct volume (95). Mattila et al. measured the GFAP levels and release rates in patients with acute cerebral ischemia using the Simoa method, finding that for patients with acute cerebral ischemia, prehospital sampling within 3 h combined with a specific rule (prehospital GFAP >410 pg./mL or prehospital GFAP 90–410 pg./mL combined with GFAP release >0.6 pg./mL/min) exhibited high specificity (NPV 98.4%) in 68% of acute cerebral ischemia patients (96).
Recent years have seen significant progress in the application of biosensing technologies for stroke biomarker detection, showing great potential and prospects. Biosensors combine biological recognition elements with physical sensors, converting biological molecules into detectable signals, enabling high sensitivity, rapid, and on-site detection, playing a key role in early diagnosis, condition monitoring, and personalized treatment of stroke.
Electrochemical biosensors detect biological molecules’ interactions with electrode surfaces to produce electrical signals, achieving high sensitivity detection. Rodríguez-Penedo et al. (97) developed a method for on-site GFAP detection using microcentrifuge tubes through electrochemical means, enabling rapid detection of hemorrhagic stroke biomarkers. These electrochemical biosensors provide high accuracy results in a short time, suitable for on-site acute stroke diagnosis.
Optical biosensors leverage optical signal transduction mechanisms to enhance the sensitivity and specificity of biomarker detection. These sensors employ fluorescence detection, surface plasmon resonance (SPR), or colorimetric analysis to convert biomolecular interactions into quantifiable optical signals, significantly improving detection accuracy and real-time monitoring capabilities. Due to their high sensitivity and rapid response characteristics, optical biosensors are particularly suitable for early diagnosis of ischemic stroke and continuous biomarker monitoring.
Microfluidic biosensors use microfluidic technology to achieve biomarker detection. Sayad et al. developed a magneto-impedance-based microfluidic platform for detecting GFAP in blood, classifying acute stroke subtypes (98). This platform integrates microfluidic technology and magneto-impedance biosensors, providing high sensitivity and specificity in GFAP detection, offering a new method for early stroke diagnosis and classification.
To provide a clearer comparison of biosensing technologies used for detecting biomarkers in AIS, we have summarized the detection mechanisms, readout methods, and diagnostic performance of various biosensors (Table 3).
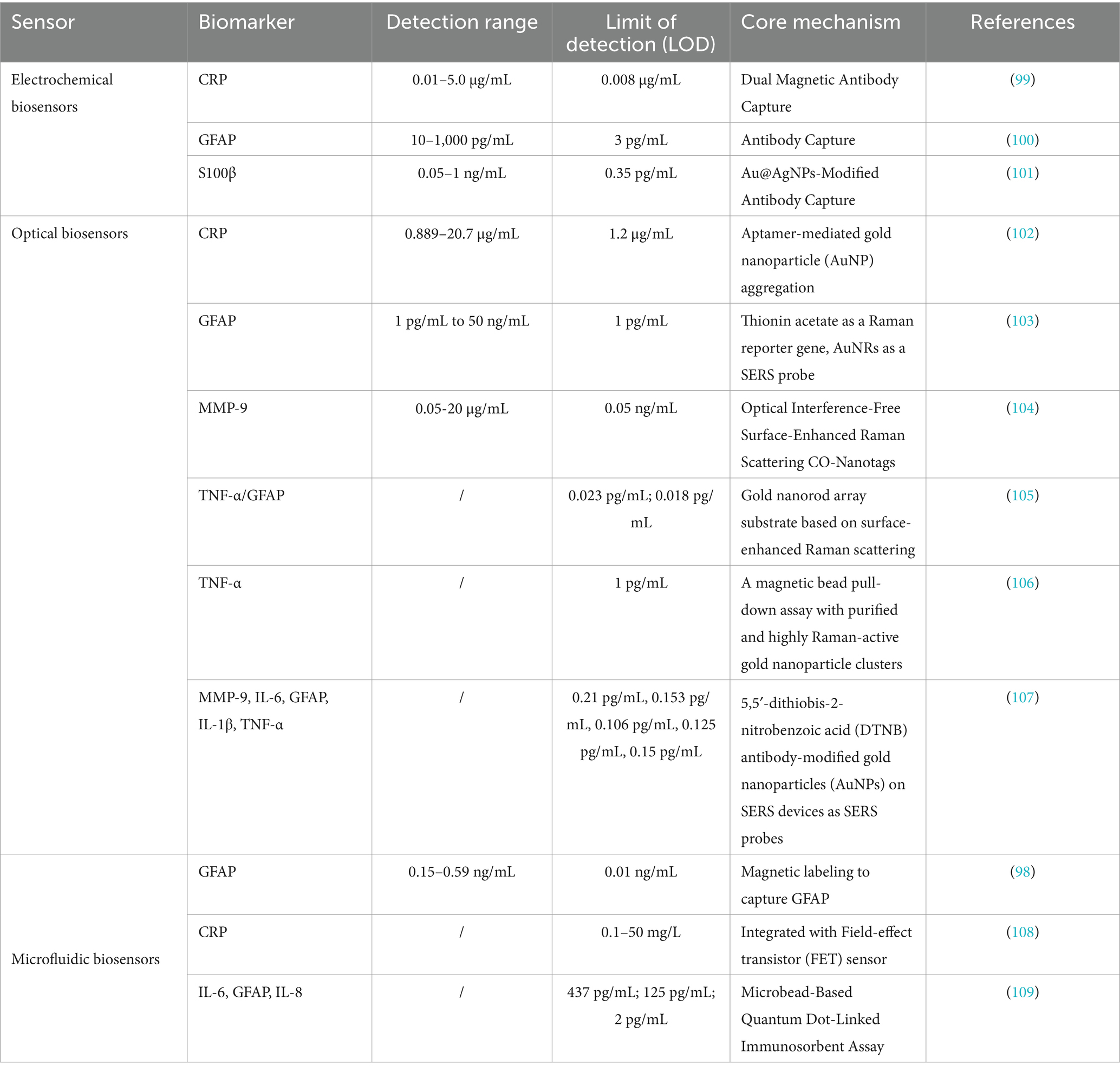
Table 3. Comparison of biosensors for AIS diagnosis.
Biomarkers play a crucial role in the diagnosis, prognostic assessment, and therapeutic monitoring of ischemic stroke. However, despite extensive research identifying numerous stroke-related biomarkers, their clinical application remains limited by several challenges, including insufficient specificity, complex dynamic variations, labor-intensive detection methods, and a lack of standardization. An ideal stroke biomarker should possess characteristics similar to cardiac troponin T (cTnT) in myocardial infarction—accurately reflecting pathophysiological changes while being detectable through rapid, efficient, and precise methods suitable for clinical use.
Currently, ischemic stroke biomarkers primarily include inflammatory factors, neuronal injury proteins, and coagulation and fibrinolysis-related factors. However, these biomarkers typically represent only specific aspects of the pathological process rather than the entire disease course. Additionally, individual variations in stroke etiology limit the clinical applicability of single biomarkers. One promising future research direction is the integration of multi-omics data to identify core biomarkers that dynamically reflect stroke progression. Furthermore, the development of multiplex biomarker panels combining inflammatory, coagulation, neuronal injury, and metabolic markers may enhance diagnostic sensitivity and specificity. Incorporating imaging modalities and clinical scoring systems, such as the National Institutes of Health Stroke Scale (NIHSS), could further improve the clinical utility of biomarkers.
Beyond biomarker discovery, advancements in detection technologies will be critical for their successful clinical implementation. Current methodologies, including ELISA, qPCR, and LC–MS/MS, are widely used in research but face challenges such as complexity, lengthy processing times, and high equipment requirements, making them less suitable for the rapid diagnosis of this time-sensitive condition. In recent years, ultra-sensitive detection technologies, such as Simoa and biosensors, have achieved significant breakthroughs, with progressively lower detection limits. If these platforms can be further optimized to meet the needs of portable and point-of-care testing (POCT), the clinical translation of stroke biomarkers could be significantly accelerated. Additionally, the integration of artificial intelligence (AI) and machine learning algorithms may enhance diagnostic accuracy.
At present, most stroke biomarkers remain in the clinical research phase and have yet to be widely implemented in routine diagnostics. Future studies should focus on large-scale, multicenter cohort investigations with rigorous study designs, including prospective cohort studies, to establish clear reference ranges, specificity, and clinically relevant cutoff values for various biomarkers.
Overall, only by simultaneously advancing our understanding of the pathogenesis of AIS and enhancing the sensitivity, specificity, stability, and resistance to interference of detection technologies can stroke biomarkers truly support early diagnosis, disease monitoring, and personalized treatment strategies.
YL: Writing – original draft. JC: Writing – review & editing. YC: Writing – review & editing. YT: Writing – review & editing. LL: Writing – review & editing. YX: Writing – review & editing. SW: Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. The present study is supported by the Funding for Scientific Research Projects from Wuhan Municipal Health Commission (WX23A57).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Krishnamurthi, RV, Ikeda, T, and Feigin, VL. Global, regional and country-specific burden of Ischaemic stroke, intracerebral Haemorrhage and subarachnoid Haemorrhage: A systematic analysis of the global burden of disease study 2017. Neuroepidemiology. (2020) 54:171–9. doi: 10.1159/000506396
2. Owolabi, MO, Thrift, AG, Martins, S, Johnson, W, Pandian, J, Abd-Allah, F, et al. The state of stroke services across the globe: report of world stroke organization–World Health Organization surveys. J Int J Stroke. (2021) 16:889–901. doi: 10.1177/17474930211019568
3. Murphy, SJ, and Werring, DJ. Stroke: causes and clinical features. Medicine. (2020) 48:561–6. doi: 10.1016/j.mpmed.2020.06.002
4. Herpich, F, and Rincon, F. Management of Acute Ischemic Stroke. Crit Care Med. (2020) 48:1654–63. doi: 10.1097/CCM.0000000000004597
5. Saini, V, Guada, L, and Yavagal, DR. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology. (2021) 97:S6–S16. doi: 10.1212/WNL.0000000000012781
6. Hasan, TF, Hasan, H, and Kelley, RE. Overview of Acute Ischemic Stroke Evaluation and Management. Biomedicines. (2021) 9:1486. doi: 10.3390/biomedicines9101486
7. Kamtchum-Tatuene, J, and Jickling, GC. Blood biomarkers for stroke diagnosis and management. NeuroMolecular Med. (2019) 21:344–68. doi: 10.1007/s12017-019-08530-0
8. Montellano, FA, Ungethüm, K, Ramiro, L, Nacu, A, Hellwig, S, Fluri, F, et al. Role of blood-based biomarkers in ischemic stroke prognosis a systematic review. Stroke. (2021) 52:543–51. doi: 10.1161/strokeaha.120.029232
9. Tuo, QZ, Zhang, ST, and Lei, P. Mechanisms of neuronal cell death in ischemic stroke and their therapeutic implications. Med Res Rev. (2022) 42:259–305. doi: 10.1002/med.21817
10. Staessens, S, and De Meyer, SF. Thrombus heterogeneity in ischemic stroke. Platelets. (2021) 32:331–9. doi: 10.1080/09537104.2020.1748586
11. Li, J, Pan, Y, Xu, J, Li, S, Wang, M, Quan, K, et al. Residual inflammatory risk predicts poor prognosis in acute ischemic stroke or transient ischemic attack patients. Stroke. (2021) 52:2827–36. doi: 10.1161/STROKEAHA.120.033152
12. Li, Z, Bi, R, Sun, S, Chen, S, Chen, J, Hu, B, et al. The role of oxidative stress in acute ischemic stroke-related thrombosis. Oxid Med Cell Longev. (2022) 2022:1–19. doi: 10.1155/2022/8418820
13. Maida, CD, Norrito, RL, Daidone, M, Tuttolomondo, A, and Pinto, A. Neuroinflammatory mechanisms in ischemic stroke: focus on Cardioembolic stroke, background, and therapeutic approaches. Int J Mol Sci. (2020) 21:6454. doi: 10.3390/ijms21186454
14. van Putten, MJ, Fahlke, C, Kafitz, KW, Hofmeijer, J, and Rose, CR. Dysregulation of astrocyte ion homeostasis and its relevance for stroke-induced brain damage. Int J Mol Sci. (2021) 22:5679. doi: 10.3390/ijms22115679
15. Zhou, X, Chen, H, Wang, L, Lenahan, C, Lian, L, Ou, Y, et al. Mitochondrial dynamics: A potential therapeutic target for ischemic stroke. Front Aging Neurosci. (2021) 13:721428. doi: 10.3389/fnagi.2021.721428
16. Mo, Y, Sun, Y-Y, and Liu, K-Y. Autophagy and inflammation in ischemic stroke. Neural Regen Res. (2020) 15:1388–96. doi: 10.4103/1673-5374.274331
17. Lim, HH, Jeong, IH, An, GD, Woo, KS, Kim, KH, Kim, JM, et al. Evaluation of neutrophil extracellular traps as the circulating marker for patients with acute coronary syndrome and acute ischemic stroke. J Clin Lab Anal. (2020) 34:e23190. doi: 10.1002/jcla.23190
18. Ohara, T, Farhoudi, M, Bang, OY, Koga, M, and Demchuk, AM. The emerging value of serum D-dimer measurement in the work-up and Management of Ischemic Stroke. Int J Stroke. (2020) 15:122–31. doi: 10.1177/1747493019876538
19. Lee, J, Mun, S, Park, A, Kim, D, Lee, YJ, Kim, HJ, et al. Proteomics reveals plasma biomarkers for ischemic stroke related to the coagulation Cascade. J Mol Neurosci. (2020) 70:1321–31. doi: 10.1007/s12031-020-01545-4
20. Misra, S, Singh, P, Nath, M, Bhalla, D, Sengupta, S, Kumar, A, et al. Blood-based protein biomarkers for the diagnosis of acute stroke: A discovery-based Swath-Ms proteomic approach. Front Neurol. (2022) 13:989856. doi: 10.3389/fneur.2022.989856
21. Luger, S, Jæger, HS, Dixon, J, Bohmann, FO, Schaefer, J, Richieri, SP, et al. Diagnostic accuracy of glial fibrillary acidic protein and ubiquitin Carboxy-terminal hydrolase-L1 serum concentrations for differentiating acute intracerebral hemorrhage from ischemic stroke. Neurocrit Care. (2020) 33:39–48. doi: 10.1007/s12028-020-00931-5
22. Haydinger, CD, Ashander, LM, Tan, ACR, and Smith, JR. Intercellular adhesion molecule 1: more than a leukocyte adhesion molecule. Biology. (2023) 12:743. doi: 10.3390/biology12050743
23. Blann, A, Kumar, P, Krupinski, J, McCollum, C, Beevers, DG, and Lip, GYH. Soluble intercellular adhesion Molecule-1, E-selectin, vascular cell adhesion Molecule-1 and Von Willebrand factor in stroke. Blood Coagul Fibrinolysis. (1999) 10:277–84. doi: 10.1097/00001721-199907000-00009
24. Nielsen, HH, Soares, CB, Hogedal, SS, Madsen, JS, Hansen, RB, Christensen, AA, et al. Acute Neurofilament light chain plasma levels correlate with stroke severity and clinical outcome in ischemic stroke patients. Front Neurol. (2020) 11:448. doi: 10.3389/fneur.2020.00448
25. Wang, L, Chen, Y, Feng, D, and Wang, X. Serum Icam-1 as a predictor of prognosis in patients with acute ischemic stroke. Biomed Res Int. (2021) 2021:5539304. doi: 10.1155/2021/5539304
26. Gao, H, and Zhang, XH. Associations of intercellular adhesion Molecule-1 Rs5498 polymorphism with ischemic stroke: A Meta-analysis. Mol Genet Genomic Med. (2019) 7:e643. doi: 10.1002/mgg3.643
27. Rakhimbaeva, GS, and kizi Abdurakhmonova, KB. Icam-1 and Crp as biomarkers of 3-month outcome in acute Ischaemic stroke. BMJ Neurol Open. (2023) 5:e000516. doi: 10.1136/bmjno-2023-000516
28. Orion, D, Schwammenthal, Y, Reshef, T, Schwartz, R, Tsabari, R, Merzeliak, O, et al. Interleukin-6 and soluble intercellular adhesion Molecule-1 in acute brain Ischaemia. Eur J Neurol. (2008) 15:323–8. doi: 10.1111/j.1468-1331.2008.02066.x
29. Bitsch, A, Klene, W, Murtada, L, Prange, H, and Rieckmann, P. A longitudinal prospective study of soluble adhesion molecules in acute stroke. Stroke. (1998) 29:2129–35. doi: 10.1161/01.Str.29.10.2129
30. Sabbah, AS, Elkattan, MM, Labib, DM, Hamdy, MSE, Wahdan, NS, and Aboulfotoh, ASM. Role of Von Willebrand factor level as a biomarker in acute ischemic stroke. Egypt J Neurol Psychiatry Neurosurg. (2024) 60:63. doi: 10.1186/s41983-024-00837-5
31. Sharma, R, Gowda, H, Chavan, S, Advani, J, Kelkar, D, Kumar, GS, et al. Proteomic signature of endothelial dysfunction identified in the serum of acute ischemic stroke patients by the Itraq-based Lc-Ms approach. J Proteome Res. (2015) 14:2466–79. doi: 10.1021/pr501324n
32. Steliga, A, Kowiański, P, Czuba, E, Waśkow, M, Moryś, J, and Lietzau, G. Neurovascular unit as a source of ischemic stroke biomarkers—limitations of experimental studies and perspectives for clinical application. Transl Stroke Res. (2020) 11:553–79. doi: 10.1007/s12975-019-00744-5
33. SdlC, B, García del Barco, D, Hardy-Sosa, A, Guillen Nieto, G, Bringas-Vega, ML, Llibre-Guerra, JJ, et al. Scalable bio marker combinations for early stroke diagnosis: A systematic review. Front Neurol. (2021) 12:638693. doi: 10.3389/fneur.2021.638693
34. Kawano, T, Gon, Y, Sakaguchi, M, Yamagami, H, Abe, S, Hashimoto, H, et al. Von Willebrand factor antigen levels predict poor outcomes in patients with stroke and Cancer: findings from the multicenter, prospective, observational Scan study. J Am Heart Assoc. (2024) 13:e032284. doi: 10.1161/JAHA.123.032284
35. Wang, Y, Li, J, Pan, Y, Wang, M, Meng, X, and Wang, Y. Association between high-sensitivity C-reactive protein and prognosis in different periods after ischemic stroke or transient ischemic attack. J Am Heart Assoc. (2022) 11:e025464. doi: 10.1161/JAHA.122.025464
36. Coveney, S, Murphy, S, Belton, O, Cassidy, T, Crowe, M, Dolan, E, et al. Inflammatory cytokines, high-sensitivity C-reactive protein, and risk of one-year vascular events, death, and poor functional outcome after stroke and transient ischemic attack. Int J Stroke. (2022) 17:163–71. doi: 10.1177/1747493021995595
37. Lasek-Bal, A, Jedrzejowska-Szypulka, H, Student, S, Warsz-Wianecka, A, Zareba, K, Puz, P, et al. The importance of selected markers of inflammation and blood-brain barrier damage for short-term ischemic stroke prognosis. J Physiol Pharmacol. (2019) 70:209–17. doi: 10.26402/jpp.2019.2.04
38. Reiche, EMV, Gelinksi, JR, Alfieri, DF, Flauzino, T, Lehmann, MF, de Araújo, MCM, et al. Immune-inflammatory, oxidative stress and biochemical biomarkers predict short-term acute ischemic stroke death. Metab Brain Dis. (2019) 34:789–804. doi: 10.1007/s11011-019-00403-6
39. Ma, Z, Yue, Y, Luo, Y, Wang, W, Cao, Y, and Fang, Q. Clinical utility of the inflammatory factors combined with lipid markers in the diagnostic and prognostic assessment of ischemic stroke: based on logistic regression models. J Stroke Cerebrovasc Dis. (2020) 29:104653. doi: 10.1016/j.jstrokecerebrovasdis.2020.104653
40. Gkantzios, A, Tsiptsios, D, Karatzetzou, S, Kitmeridou, S, Karapepera, V, Giannakou, E, et al. Stroke and emerging blood biomarkers: A clinical prospective. Neurol Int. (2022) 14:784–803. doi: 10.3390/neurolint14040065
41. Abdelnaseer, M, Elfayomi, N, Hassan, E, Kamal, M, Hamdy, A, and Elsawy, E. Serum matrix Metalloproteinase-9 in acute ischemic stroke and its relation to stroke severity. Egypt J Neurol Psychiatry Neurosurg. (2015) 52:274. doi: 10.4103/1110-1083.170661
42. Weekman, EM, and Wilcock, DM. Matrix metalloproteinase in blood-brain barrier breakdown in dementia. J Alzheimers Dis. (2016) 49:893–903. doi: 10.3233/jad-150759
43. Zhong, CK, Yang, JY, Xu, T, Xu, T, Peng, YB, Wang, AL, et al. Serum matrix Metalloproteinase-9 levels and prognosis of acute ischemic stroke. Neurology. (2017) 89:805–12. doi: 10.1212/wnl.0000000000004257
44. Mathias, K, Machado, RS, Stork, S, dos Santos, D, Joaquim, L, Generoso, J, et al. Blood-brain barrier permeability in the ischemic stroke: An update. Microvasc Res. (2024) 151:151. doi: 10.1016/j.mvr.2023.104621
45. Jayaraj, RL, Azimullah, S, Beiram, R, Jalal, FY, and Rosenberg, GA. Neuroinflammation: friend and foe for ischemic stroke. J Neuroinflammation. (2019) 16:142. doi: 10.1186/s12974-019-1516-2
46. Tsukagawa, T, Katsumata, R, Fujita, M, Yasui, K, Akhoon, C, Ono, K, et al. Elevated serum high-mobility group Box-1 protein level is associated with poor functional outcome in ischemic stroke. J Stroke Cerebrovasc Dis. (2017) 26:2404–11. doi: 10.1016/j.jstrokecerebrovasdis.2017.05.033
47. Sapojnikova, N, Kartvelishvili, T, Asatiani, N, Zinkevich, V, Kalandadze, I, Gugutsidze, D, et al. Correlation between Mmp-9 and extracellular cytokine Hmgb1 in prediction of human ischemic stroke outcome. BBA-Mol Basis Dis. (2014) 1842:1379–84. doi: 10.1016/j.bbadis.2014.04.031
48. Shen, LP, Yang, JS, Zhu, ZF, Li, WZ, Cui, JY, and Gu, LY. Elevated serum Hmgb1 levels and their association with recurrence of acute Ischaemic stroke. J Inflamm Res. (2024) 17:6887–94. doi: 10.2147/jir.S477415
49. Li, JM, Wang, ZX, Li, JM, Zhao, HP, and Ma, QF. Hmgb1: A new target for ischemic stroke and hemorrhagic transformation. Transl Stroke Res. (2024). 514:05. doi: 10.1007/s12975-024-01258-5
50. Bustamante, A, Penalba, A, Orset, C, Azurmendi, L, Llombart, V, Simats, A, et al. Blood biomarkers to differentiate ischemic and hemorrhagic strokes. Neurology. (2021) 96:e1928–39. doi: 10.1212/WNL.0000000000011742
51. Kalra, LP, Khatter, H, Ramanathan, S, Sapehia, S, Devi, K, Kaliyaperumal, A, et al. Serum Gfap for stroke diagnosis in regions with limited access to brain imaging (be fast India). Eur Stroke J. (2021) 6:176–84. doi: 10.1177/23969873211010069
52. Perry, LA, Lucarelli, T, Penny-Dimri, JC, McInnes, MD, Mondello, S, Bustamante, A, et al. Glial fibrillary acidic protein for the early diagnosis of intracerebral hemorrhage: systematic review and Meta-analysis of diagnostic test accuracy. Int J Stroke. (2019) 14:390–9. doi: 10.1177/1747493018806167
53. Lee, M, Rafiq Sayyed, D, Kim, H, Sanchez, JC, Sik Hong, S, Choi, S, et al. A comprehensive Exdia Trf-Lfia for simultaneous quantification of Gfap and Nt-Probnp in distinguishing ischemic and hemorrhagic stroke. Clin Chim Acta. (2024) 557:117872. doi: 10.1016/j.cca.2024.117872
54. Sanchez, JD, Martirosian, RA, Mun, KT, Chong, DS, Llorente, IL, Uphaus, T, et al. Temporal patterning of Neurofilament light as a blood-based biomarker for stroke: A systematic review and Meta-analysis. Front Neurol. (2022) 13:841898. doi: 10.3389/fneur.2022.841898
55. Pedersen, A, Stanne, TM, Nilsson, S, Klasson, S, Rosengren, L, Holmegaard, L, et al. Circulating Neurofilament light in ischemic stroke: temporal profile and outcome prediction. J Neurol. (2019) 266:2796–806. doi: 10.1007/s00415-019-09477-9
56. Uphaus, T, Bittner, S, Gröschel, S, Steffen, F, Muthuraman, M, Wasser, K, et al. Nfl (Neurofilament light chain) levels as a predictive marker for Long-term outcome after ischemic stroke. Stroke. (2019) 50:3077–84. doi: 10.1161/STROKEAHA.119.026410
57. Barba, L, Vollmuth, C, Abu-Rumeileh, S, Halbgebauer, S, Oeckl, P, Steinacker, P, et al. Serum Β-Synuclein, Neurofilament light chain and glial fibrillary acidic protein as prognostic biomarkers in moderate-to-severe acute ischemic stroke. Sci Rep. (2023) 13:20941. doi: 10.1038/s41598-023-47765-7
58. O'Connell, GC, Smothers, CG, and Gandhi, SA. Newly-identified blood biomarkers of neurological damage are correlated with infarct volume in patients with acute ischemic stroke. J Clin Neurosci. (2021) 94:107–13. doi: 10.1016/j.jocn.2021.10.015
59. Xu, X, Zhuang, C, and Chen, L. Exosomal Long non-coding Rna expression from serum of patients with acute minor stroke. Neuropsychiatr Dis Treat. (2020) 16:153–60. doi: 10.2147/NDT.S230332
60. Bai, X, Liu, X, Wu, H, Feng, J, Chen, H, and Zhou, D. Circfundc1 knockdown alleviates oxygen-glucose deprivation-induced human brain microvascular endothelial cell injuries by inhibiting Pten via Mir-375. Neurosci Lett. (2022) 770:136381. doi: 10.1016/j.neulet.2021.136381
61. Xiao, Q, Hou, R, Li, H, Zhang, S, Zhang, F, Zhu, X, et al. Circulating Exosomal circRNAs contribute to potential diagnostic value of large artery atherosclerotic stroke. Front Immunol. (2022) 12:830018. doi: 10.3389/fimmu.2021.830018
62. Zhou, J, Chen, L, Chen, B, Huang, S, Zeng, C, Wu, H, et al. Increased serum Exosomal Mir-134 expression in the acute ischemic stroke patients. BMC Neurol. (2018) 18:198. doi: 10.1186/s12883-018-1196-z
63. Wang, W, Li, D-B, Li, R-Y, Zhou, X, Yu, D-J, Lan, X-Y, et al. Diagnosis of Hyperacute and acute Ischaemic stroke: the potential utility of Exosomal Microrna-21-5p and Microrna-30a-5p. Cerebrovasc Dis. (2018) 45:204–12. doi: 10.1159/000488365
64. Zhang, S, Wang, X, Yin, R, Xiao, Q, Ding, Y, Zhu, X, et al. Circulating Exosomal Lncrnas as predictors of risk and unfavorable prognosis for large artery atherosclerotic stroke. Clin Transl Med. (2021) 11:e555. doi: 10.1002/ctm2.555
65. Chen, F, Du, Y, Esposito, E, Liu, Y, Guo, SZ, Wang, XY, et al. Effects of focal cerebral ischemia on Exosomal versus serum Mir126. Transl Stroke Res. (2015) 6:478–84. doi: 10.1007/s12975-015-0429-3
66. Burek, M, König, A, Lang, M, Fiedler, J, Oerter, S, Roewer, N, et al. Hypoxia-induced Microrna-212/132 Alter blood-brain barrier integrity through inhibition of tight junction-associated proteins in human and mouse brain microvascular endothelial cells. Transl Stroke Res. (2019) 10:672–83. doi: 10.1007/s12975-018-0683-2
67. Tan, KS, Armugam, A, Sepramaniam, S, Lim, KY, Setyowati, KD, Wang, CW, et al. Expression profile of Micrornas in young stroke patients. PLoS One. (2009) 4:e7689. doi: 10.1371/journal.pone.0007689
68. Chen, YJ, Song, YY, Huang, J, Qu, MJ, Zhang, Y, Geng, JL, et al. Increased circulating Exosomal Mirna-223 is associated with acute ischemic stroke. Front Neurol. (2017) 8:8. doi: 10.3389/fneur.2017.00057
69. Kang, LJ, Yu, HL, Yang, X, Zhu, YB, Bai, XF, Wang, RR, et al. Neutrophil extracellular traps released by neutrophils impair revascularization and vascular remodeling after stroke. Nature. Communications. (2020) 11:2488. doi: 10.1038/s41467-020-16191-y
70. Vallés, J, Lago, A, Santos, MT, Latorre, AM, Tembl, JI, Salom, JB, et al. Neutrophil extracellular traps are increased in patients with acute ischemic stroke: prognostic significance. Thromb Haemost. (2017) 117:1919–29. doi: 10.1160/th17-02-0130
71. Denorme, F, Portier, I, Rustad, JL, Cody, MJ, de Araujo, CV, Hoki, C, et al. Neutrophil extracellular traps regulate ischemic stroke brain injury. J Clin Invest. (2022) 132:e154225. doi: 10.1172/jci154225
72. Lapostolle, A, Loyer, C, Elhorany, M, Chaigneau, T, Bielle, F, Alamowitch, S, et al. Neutrophil extracellular traps in ischemic stroke thrombi are associated Wth poor clinical outcome. Stroke. (2023) 3:e000639. doi: 10.1161/SVIN.122.000639
73. Chen, X, Wang, L, Jiang, ML, Lin, L, Ba, ZJ, Tian, H, et al. Leukocytes in cerebral Thrombus respond to large-vessel occlusion in a time-dependent manner and the Association of Nets with collateral flow. Front Immunol. (2022) 13:13. doi: 10.3389/fimmu.2022.834562
74. Pawluk, H, Grzesk, G, Kolodziejska, R, Kozakiewicz, M, Wozniak, A, Grzechowiak, E, et al. Effect of Il-6 and Hscrp serum levels on functional prognosis in stroke patients undergoing iv-thrombolysis: retrospective analysis. Clin Interv Aging. (2020) 15:1295–303. doi: 10.2147/CIA.S258381
75. Fang, C, Lou, B, Zhou, J, Zhong, R, Wang, R, Zang, X, et al. Blood biomarkers in ischemic stroke: role of biomarkers in differentiation of clinical phenotype. Eur J Inflamm. (2018) 16:2058739218780058. doi: 10.1177/2058739218780058
76. Sun, C, Ma, C, Sun, Y, and Ma, L. Effect of Edaravone combined with anticoagulant therapy on the serum Hs-Crp, Il-6, and Tnf-alpha levels and activity of daily living in patients with acute cerebral infarction. J Healthc Eng. (2022) 2022:8603146. doi: 10.1155/2022/8603146
77. Zhang, X, Wang, L, Han, Z, Dong, J, Pang, D, Fu, Y, et al. Klf4 alleviates cerebral vascular injury by ameliorating vascular endothelial inflammation and regulating tight junction protein expression following ischemic stroke. J Neuroinflammation. (2020) 17:1–16. doi: 10.1186/s12974-020-01780-x
78. Zhang, J, Yang, J, Hu, J, and Zhao, W. Clinical value of serum Jkap in acute ischemic stroke patients. J Clin Lab Anal. (2022) 36:e24270. doi: 10.1002/jcla.24270
79. Amalia, L. Glial fibrillary acidic protein (Gfap): Neuroinflammation biomarker in acute ischemic stroke. J Inflamm Res. (2021) 14:7501–6. doi: 10.2147/JIR.S342097
80. Puspitasari, V, Gunawan, PY, Wiradarma, HD, and Hartoyo, V. Glial fibrillary acidic protein serum level as a predictor of clinical outcome in ischemic stroke. Open Access Maced J Med Sci. (2019) 7:1471–4. doi: 10.3889/oamjms.2019.326
81. Bhatia, R, Warrier, AR, Sreenivas, V, Bali, P, Sisodia, P, Gupta, A, et al. Role of blood biomarkers in differentiating ischemic stroke and intracerebral hemorrhage. Neurol India. (2020) 68:824–9. doi: 10.4103/0028-3886.293467
82. Sun, Y, Wang, J, Han, B, Meng, K, Han, Y, and Ding, Y. Elucidating the molecular mechanism of ischemic stroke using integrated analysis of Mirna, Mrna, and Lncrna expression profiles. Front Integr Neurosci. (2021) 15:638114. doi: 10.3389/fnint.2021.638114
83. Xiang, Y, Zhang, Y, Xia, Y, Zhao, H, Liu, A, and Chen, Y. Lncrna Meg3 targeting Mir-424-5p via Mapk signaling pathway mediates neuronal apoptosis in ischemic stroke. Aging (Albany NY). (2020) 12:3156–74. doi: 10.18632/aging.102790
84. Tian, J, Liu, Y, Wang, Z, Zhang, S, Yang, Y, Zhu, Y, et al. Lncrna Snhg8 attenuates microglial inflammation response and blood-brain barrier damage in ischemic stroke through regulating Mir-425-5p mediated Sirt1/Nf-Kappab signaling. J Biochem Mol Toxicol. (2021) 35:e22724. doi: 10.1002/jbt.22724
85. Medeiros, R, Sousa, B, Rossi, S, Afonso, C, Bonino, L, Pitt, A, et al. Identification and relative quantification of 3-Nitrotyrosine residues in fibrinogen nitrated in vitro and fibrinogen from ischemic stroke patient plasma using Lc-Ms/Ms. Free Radic Biol Med. (2021) 165:334–47. doi: 10.1016/j.freeradbiomed.2021.01.049
86. Kamal, FZ, Lefter, R, Jaber, H, Balmus, IM, Ciobica, A, and Iordache, AC. The role of potential oxidative biomarkers in the prognosis of acute ischemic stroke and the exploration of antioxidants as possible preventive and treatment options. Int J Mol Sci. (2023) 24:6389. doi: 10.3390/ijms24076389
87. Rattanawong, W, Ongphichetmetha, T, Hemachudha, T, and Thanapornsangsuth, P. Neurofilament light is associated with clinical outcome and hemorrhagic transformation in moderate to severe ischemic stroke. J Cent Nerv Syst Dis. (2023) 15:11795735221147212. doi: 10.1177/11795735221147212
88. Jiang, W, Niu, J, Gao, H, Dang, Y, Qi, M, and Liu, Y. A retrospective study of immunoglobulin E as a biomarker for the diagnosis of acute ischemic stroke with carotid atherosclerotic plaques. PeerJ. (2022) 10:e14235. doi: 10.7717/peerj.14235
89. Donkel, SJ, Benaddi, B, Dippel, DW, Ten Cate, H, and de Maat, MP. Prognostic hemostasis biomarkers in acute ischemic stroke: A systematic review. Arterioscler Thromb Vasc Biol. (2019) 39:360–72. doi: 10.1161/ATVBAHA.118.312102
90. Cuadrat, RR, Kratzer, A, Arnal, HG, Rathgeber, AC, Wreczycka, K, Blume, A, et al. Cardiovascular disease biomarkers derived from circulating cell-free DNA methylation. NAR genomics. Bioinformatics. (2023) 5:lqad061. doi: 10.1093/nargab/lqad061
91. Shu, Y, Guo, Y, Zheng, Y, He, S, and Shi, Z. Rna methylation in vascular disease: A systematic review. J Cardiothorac Surg. (2022) 17:323. doi: 10.1186/s13019-022-02077-1
92. Pujol-Calderon, F, Zetterberg, H, Portelius, E, Lowhagen Henden, P, Rentzos, A, Karlsson, JE, et al. Prediction of outcome after endovascular embolectomy in anterior circulation stroke using biomarkers. Transl Stroke Res. (2022) 13:65–76. doi: 10.1007/s12975-021-00905-5
93. Ferrari, F, Rossi, D, Ricciardi, A, Morasso, C, Brambilla, L, Albasini, S, et al. Quantification and prospective evaluation of serum Nfl and Gfap as blood-derived biomarkers of outcome in acute ischemic stroke patients. J Cereb Blood Flow Metab. (2023) 43:1601–11. doi: 10.1177/0271678X231172520
94. Traub, J, Grondey, K, Gassenmaier, T, Schmitt, D, Fette, G, Frantz, S, et al. Sustained increase in serum glial fibrillary acidic protein after first St-elevation myocardial infarction. Int J Mol Sci. (2022) 23:10304. doi: 10.3390/ijms231810304
95. Onatsu, J, Vanninen, R, Jäkälä, P, Mustonen, P, Pulkki, K, Korhonen, M, et al. Serum Neurofilament light chain concentration correlates with infarct volume but not prognosis in acute ischemic stroke. J Stroke Cerebrovasc Dis. (2019) 28:2242–9. doi: 10.1016/j.jstrokecerebrovasdis.2019.05.008
96. Mattila, OS, Ashton, NJ, Blennow, K, Zetterberg, H, Harve-Rytsälä, H, Pihlasviita, S, et al. Ultra-early differential diagnosis of acute cerebral ischemia and hemorrhagic stroke by measuring the prehospital release rate of Gfap. Clin Chem. (2021) 67:1361–72. doi: 10.1093/clinchem/hvab128
97. Rodríguez-Penedo, A, Costa-Rama, E, Fernández, B, García-Cabo, C, Benavente, L, Calleja, S, et al. Palladium nanoclusters as a label to determine Gfap in human serum from donors with stroke by bimodal detection: inductively coupled plasma-mass spectrometry and linear sweep voltammetry. Microchim Acta. (2023) 190:493. doi: 10.1007/s00604-023-06059-5
98. Sayad, A, Uddin, SM, Yao, S, Wilson, H, Chan, J, Zhao, H, et al. A Magnetoimpedance biosensor microfluidic platform for detection of glial fibrillary acidic protein in blood for acute stroke classification. Biosens Bioelectron. (2022) 211:114410. doi: 10.1016/j.bios.2022.114410
99. Molinero-Fernández, A, Moreno-Guzmán, M, Arruza, L, López, MA, and Escarpa, A. Toward early diagnosis of late-onset Sepsis in preterm neonates: dual Magnetoimmunosensor for simultaneous Procalcitonin and C-reactive protein determination in diagnosed clinical samples. ACS Sens. (2019) 4:2117–23. doi: 10.1021/acssensors.9b00890
100. Salahandish, R, Hassani, M, Zare, A, Haghayegh, F, and Sanati-Nezhad, A. Autonomous electrochemical biosensing of glial fibrillary acidic protein for point-of-care detection of central nervous system injuries. Lab Chip. (2022) 22:1542–55. doi: 10.1039/d2lc00025c
101. Sun, JY, Zhao, Y, Hou, YJ, Li, HX, Yang, MF, Wang, Y, et al. Multiplexed electrochemical and Sers dual-mode detection of stroke biomarkers: rapid screening with high sensitivity. New J Chem. (2019) 43:13381–7. doi: 10.1039/c9nj01598a
102. António, M, Ferreira, R, Vitorino, R, and Daniel-da-Silva, AL. A simple aptamer-based colorimetric assay for rapid detection of C-reactive protein using gold nanoparticles. Talanta. (2020) 214:120868. doi: 10.1016/j.talanta.2020.120868
103. Sun, JY, Gao, F, Song, YA, Wang, MY, Wang, C, Ni, QB, et al. Paper lateral flow strips based on gold Nanorods for ultrasensitive detection of traumatic brain injury biomarkers. ACS Appl Nano Mater. (2023) 6:18729–38. doi: 10.1021/acsanm.3c00178
104. Gong, TX, Hong, ZY, Chen, CH, Tsai, CY, Liao, LD, and Kong, KV. Optical interference-free surface-enhanced Raman scattering co-Nanotags for logical multiplex detection of vascular disease related biomarkers. ACS Nano. (2017) 11:3365–75. doi: 10.1021/acsnano.7b00733
105. Li, JQ, Wu, JG, Chen, JX, Huang, S, Liu, J, Gao, F, et al. Dual detection of spinal cord injury biomarkers in rat model using gold Nanorod Array substrate based on surface-enhanced Raman scattering. Surf Interfaces. (2022) 34:102400. doi: 10.1016/j.surfin.2022.102400
106. Lai, YM, Schlücker, S, and Wang, YL. Rapid and sensitive Sers detection of the cytokine tumor necrosis factor alpha (Tnf-Α) in a magnetic bead pull-down assay with purified and highly Raman-active gold nanoparticle clusters. Anal Bioanal Chem. (2018) 410:5993–6000. doi: 10.1007/s00216-018-1218-0
107. Wang, MY, Wan, HY, Wang, YJ, Yuan, H, Ni, QB, Sun, BL, et al. A microfluidics-based multiplex Sers immunoassay device for analysis of acute ischemic stroke biomarkers. Transl Stroke Res. (2023). 1124:10. doi: 10.1007/s12975-023-01204-x
108. Sinha, A, Tai, TY, Li, KH, Gopinathan, P, Chung, YD, Sarangadharan, I, et al. An integrated microfluidic system with field-effect-transistor sensor arrays for detecting multiple cardiovascular biomarkers from clinical samples. Biosens Bioelectron. (2019) 129:155–63. doi: 10.1016/j.bios.2019.01.001
Keywords: stroke, biomarkers, inflammatory factors, axonal injury markers, clinical testing
Citation: Liang Y, Chen J, Chen Y, Tong Y, Li L, Xu Y and Wu S (2025) Advances in the detection of biomarkers for ischemic stroke. Front. Neurol. 16:1488726. doi: 10.3389/fneur.2025.1488726
Edited by:
Haipeng Liu, Coventry University, United KingdomReviewed by:
Xiaoyan Lan, Affiliated Central Hospital of Dalian University of Technology, ChinaCopyright © 2025 Liang, Chen, Chen, Tong, Li, Xu and Wu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yuan Xu, eXVhbnh3aDIwMjRAMTI2LmNvbQ==; Shimin Wu, bWludHlyYWluQDEyNi5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.