 Xinyan Li
Xinyan Li Qianxi Li
Qianxi Li Chenyu Li1
Chenyu Li1 Chunjia Zhang
Chunjia Zhang Xin Zhang
Xin Zhang
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol., 17 February 2025
Sec. Neurorehabilitation
Volume 16 - 2025 | https://doi.org/10.3389/fneur.2025.1442004
Spinal cord injury (SCI) is a severe disorder of the central nervous system characterized by high prevalence and significant disability, imposing a substantial burden on patients and their families. In recent years, exercise training has gained prominence in the treatment of SCI due to its advantages, including low cost, high safety, ease of implementation, and significant efficacy. However, a consensus regarding the effects of various exercise training modalities and intensities on functional recovery in individuals with SCI remains elusive, and the efficacy and risks associated with high-intensity exercise training (HIET) are subjects of ongoing debate. Some studies have indicated that HIET offers superior therapeutic benefits, such as enhanced cardiovascular stress reflex sensitivity and increased release of neurotrophic factors, compared to moderate- or low-intensity exercise training. Nonetheless, HIET may entail risks, including secondary injuries, heightened inflammatory responses, and falls. This study reviews the positive and negative effects of HIET on various body systems in individuals with SCI, focusing on mechanisms such as neuroplasticity and immune regulation, to provide a theoretical basis and evidence for its prospective clinical application. Additionally, the limitations of existing studies are analyzed to inform recommendations and guidance for future research.
Spinal cord injury (SCI) is a prevalent, highly disabling, and progressive neurological condition (1). Currently, more than 20 million people worldwide suffer from SCI, and from 1990 to 2019, the prevalence of SCI increased by 81.5%, incidence by 52.7%, and years lived with disability (YLDs) by 65.4% (2). SCI can be categorized into primary and secondary injuries. Primary injuries typically involve axonal damage, vascular disruption, and cellular membrane destruction, while secondary injuries comprise a cascade of responses to primary trauma, including inflammation, ischemia, vascular dysfunction, free radical formation, apoptosis, and necrosis (3). Current treatment modalities for SCI are predominantly invasive and include surgical decompression, neural bridging, neurostimulation and neuromodulation, brain-computer interfaces, and stem cell therapy (4). By contrast, exercise training represents a cost-effective and non-invasive treatment option with fewer adverse effects (5–7). Exercise training is increasingly employed as a comprehensive treatment approach that integrates multiple therapeutic strategies (8).
Exercise training has been reported to achieve efficacy comparable to pharmacotherapy (9), irrespective of the level of injury (10, 11). It leverages residual muscle strength to activate the remaining musculature (12) and provides benefits such as fat reduction, muscle development, metabolic enhancement, blood pressure regulation, and increased bone density (13, 14) (see Table 1 [1, 2]). These improvements contribute to enhanced functional independence, mental health, and quality of life for patients (12, 15). Importantly, individuals with SCI must maintain a high level of exercise intensity to achieve functional improvements (16) (see Table 1 [3]). Extremely low-intensity exercise may yield limited benefits compared to high-intensity exercise training (HIET) (16–18) (see Table 1 [3, 4]). Studies have indicated that HIET with lower total training volume induces greater physiological adaptations than moderate-intensity exercise (19). However, the current clinical use of HIET remains conservative due to safety concerns, and lack of consensus on HIET’s efficacy and risks.
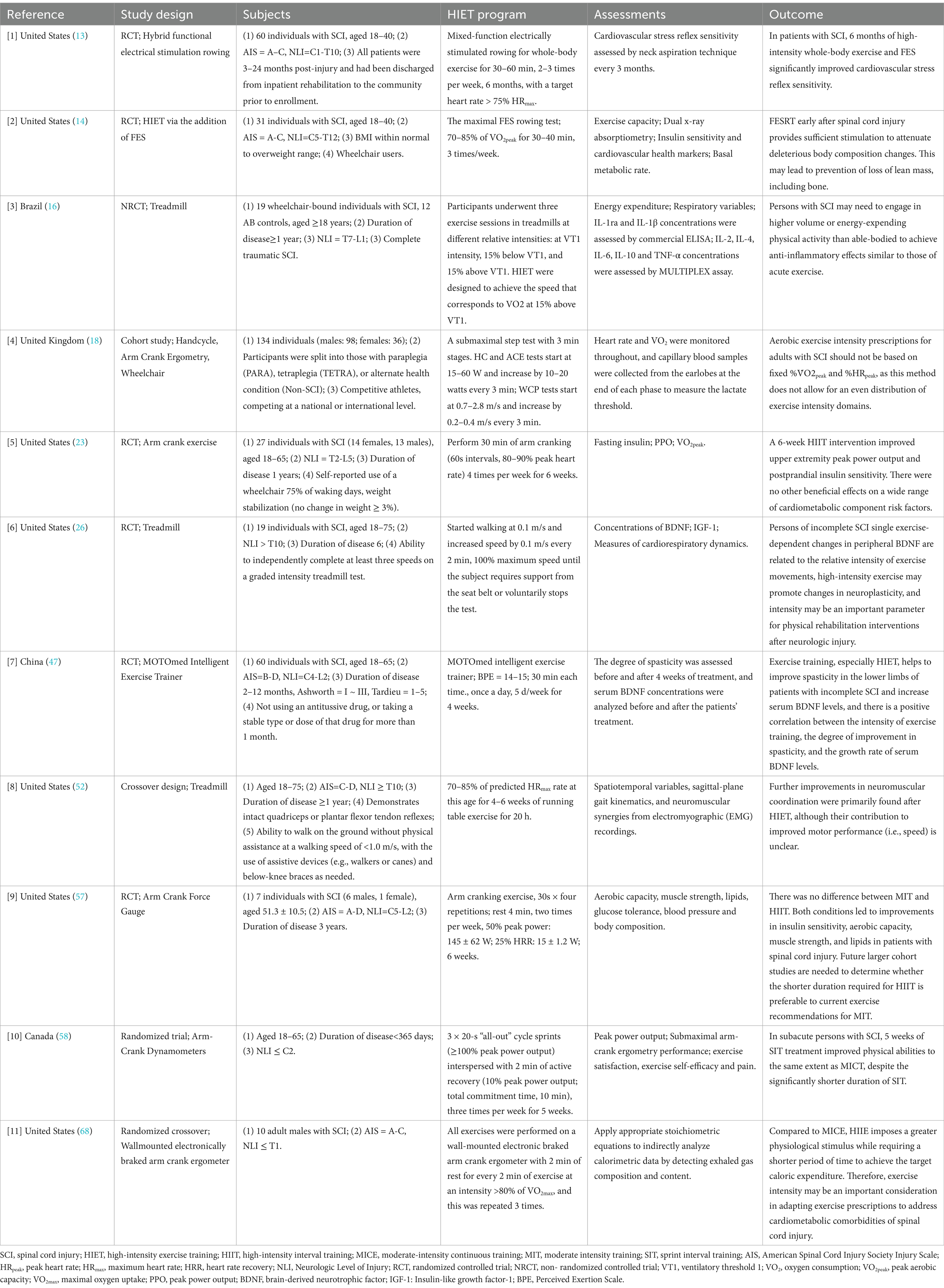
Table 1. Clinical trials of HIET after SCI.
Currently, there are no standardized criteria for exercise intensity in individuals with SCI. Most clinical studies have assessed exercise intensity based on heart rate or speed. This review included studies in which HIET was explicitly implemented for subjects with SCI, with exercise intensity defined through heart rate ranges, exercise loads, or similar parameters. Based on the literature, HIET is defined as 75–100% of the maximum heart rate or 70–90% of the maximum speed, adjusted for individual differences. In animal studies, HIET criteria often include 70–85% of maximum walking speed or self-defined greater walking speed and 80–85% of maximum heart rate. Further research is necessary to optimize these criteria and develop effective exercise training protocols to facilitate recovery in individuals with SCI.
The potential benefits and applications of high-intensity interval training (HIIT), a specific form of HIET involving repetitive high-intensity workouts with short rest intervals, have been detailed in existing literature. However, comprehensive reviews of other types of HIET, including animal experiments, remain scarce (20). This review focuses on the effects of HIET, encompassing HIIT and other high-intensity exercise modalities, on functional recovery after SCI. It examines exercise protocols in current studies, highlights relevant shortcomings, and provides recommendations while elucidating the advantages of HIET.
HIET has been shown to significantly enhance postprandial insulin sensitivity, blood pressure regulation, maximal oxygen consumption, and systemic vascular function, thereby exerting positive effects on the cardiovascular and pulmonary systems.
SCI often results in impaired respiratory muscle function, cardiorespiratory dysfunction, and diminished aerobic capacity, which collectively reduce cardiopulmonary reserve and increase the risk of cardiovascular diseases (21). Compared to low-intensity exercise, HIET improves postprandial insulin sensitivity, thereby lowering obesity rates and cardiac burden, although it does not significantly affect a wide range of cardiometabolic risk factors (22, 23) (see Table 1 [5]). Additionally, autonomic dysreflexia, a condition frequently associated with SCI, can cause abnormal blood pressure fluctuations, underscoring the importance of blood pressure regulation for cardiovascular health. One study (13) (see Table 1 [1]) demonstrated that HIET enhances cardiovascular stress sensitivity compared to low-intensity exercise training under similar conditions. However, a single HIET session may not significantly improve stress sensitivity. To achieve meaningful cardiovascular benefits, individuals with SCI may require high-intensity whole-body exercise combined with mixed-function electrical stimulation. Notably, HIET has been associated with significant improvements in maximal oxygen consumption and systemic vascular function compared to low-intensity exercise training (24).
HIET upregulates the expression of brain-derived neurotrophic factor (BDNF) and the mammalian target of rapamycin (mTOR) in the spinal cord tissues of rats with SCI. This activation of the mTOR pathway protects mitochondrial quantity and quality, inhibits neuroglial cell activation, and promotes the repair of spinal cord nerves (Figure 1).
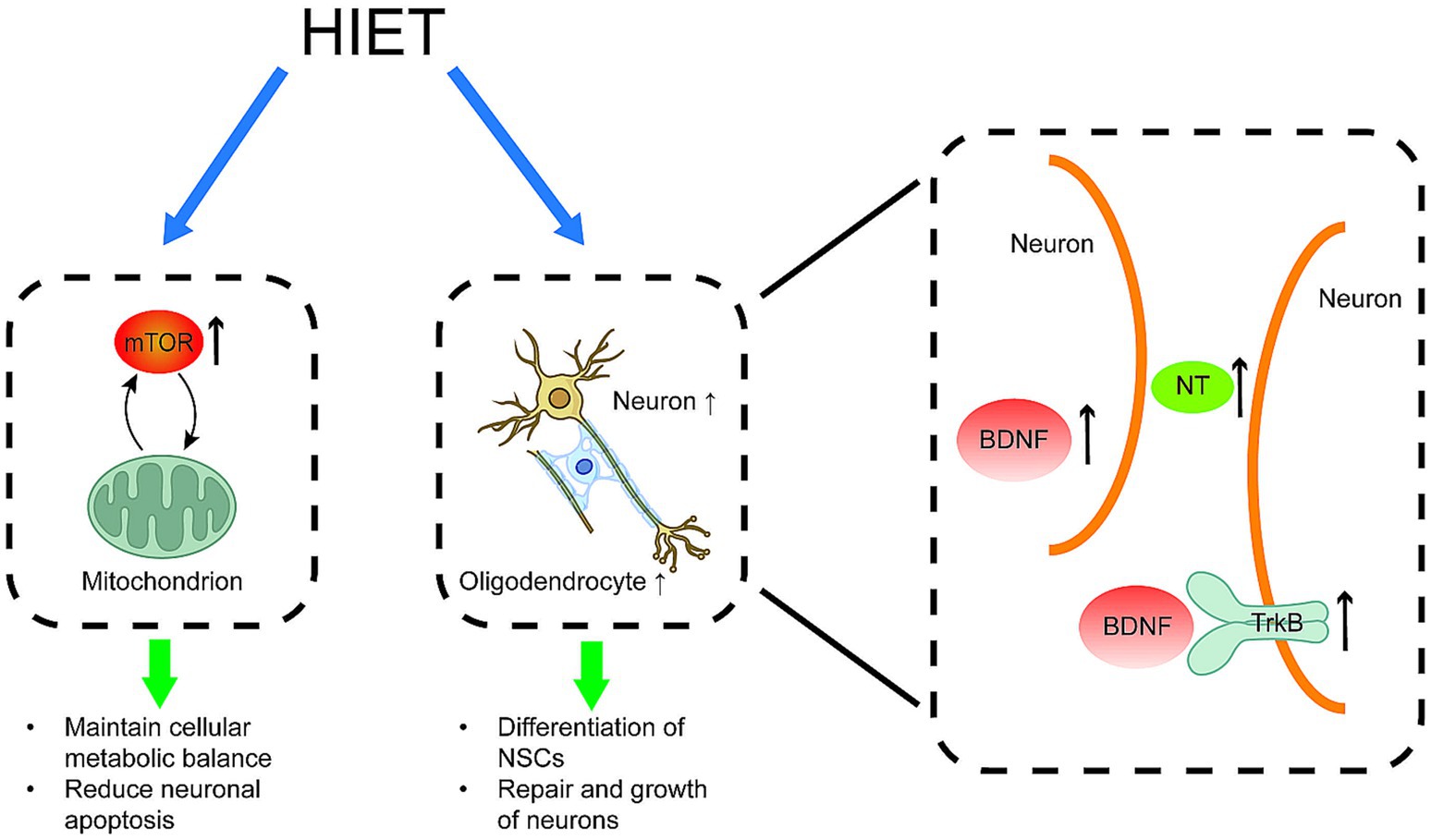
Figure 1. Positive effects of HIET on spinal cord histopathological changes HIET has been shown to elevate the levels of BDNF, mTOR, TrkB proteins, and neurotrophic factors (NT) in spinal cord tissues. These changes promote the formation of oligodendrocytes, the differentiation of neural stem cells (NSCs), protection of mitochondria and the repair and growth of normal spinal cord neurons. BDNF: brain-derived neurotrophic factor; mTOR: mammalian target of rapamycin; NT: neurotrophic factor; TrkB protein: tyrosine kinase receptor B protein; NSCs: neural stem cells.
Exercise training enhances neuroplasticity by promoting myelin structural repair, neurotrophin (NT) secretion, and the proliferation and differentiation of endogenous neural stem cells (NSCs) (25). However, these molecular mechanisms require a specific level of exercise intensity, particularly NT, which is strongly dependent on exercise intensity (26) (see Table 1 [6]). BDNF facilitates the differentiation and maturation of oligodendrocytes, enhancing spinal cord neuroplasticity and promoting neural pathway repair (27). Studies (28, 29) (see Table 2 [1, 2]) have demonstrated that high-intensity weight-loss walking training in SCI rat models significantly promotes the synthesis and transport of endogenous pro-myosin receptor B (TrkB) and BDNF and increases the number of Nysted’s vesicles in spinal cord tissues. In contrast, low-intensity training did not produce similar effects, failing to elevate TrkB and BDNF levels despite upregulating BDNF expression compared to non-exercising rats.
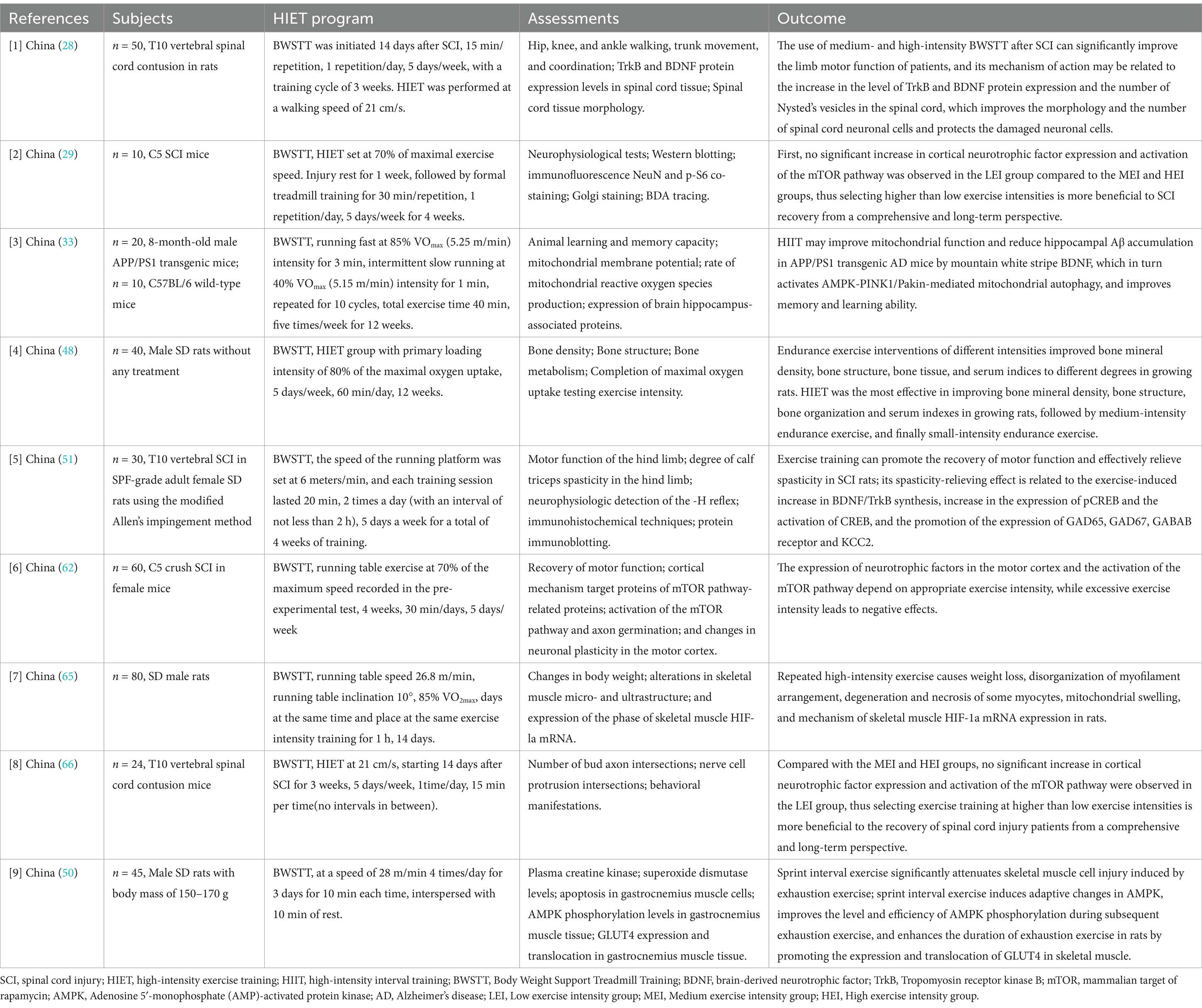
Table 2. Animal experiments of HIET after SCI.
The mTOR pathway plays a pivotal role in exercise-induced nerve growth. Zhan (29) (see Table 2 [2]) found that mTOR expression significantly increased in spinal cord tissues of SCI rats following HIET, triggering endogenous axonal regeneration. Mitochondria, vital for cellular metabolism, produce ATP molecules via phosphorylation. Neurons require adequate energy for survival; mitochondrial dysfunction leads to neuronal apoptosis (30). Post-SCI, altered mitochondrial morphology and function, including Ca2+ disorders, initiate cascade reactions leading to neuronal death (31).
Few studies have assessed the effects of HIET on mitochondria post-SCI. Research on neurodegenerative diseases (32, 33) (see Table 2 [2, 3]) indicates that HIIT preserves mitochondrial quantity and quality to meet neuronal energy demands. This preservation occurs through BDNF-mediated activation of the AMPK/PINK1/Parkin pathway in Alzheimer’s disease models. Furthermore, HIIT enhances mitochondrial membrane potential, reduces reactive oxygen species (ROS) production, and decreases amyloid-β peptide levels in the hippocampus. HIIT also exhibits anti-inflammatory effects by inhibiting glial cell activation and reducing inflammatory cytokine release, protecting neurons from damage and preventing apoptosis. Additionally, HIIT increases lactate levels, which regulate mitochondrial quality and promote BDNF expression (34). However, further studies are necessary to confirm whether HIIT affects spinal cord neuronal mitochondria after SCI.
SCI-induced denervation triggers apoptosis and atrophy of brain neurons, resulting in the loss of afferent information in somatosensory brain regions and impaired motor innervation throughout the body. Consequently, the sensory-motor cortex undergoes extensive reorganization of neuronal circuits, altering the electrical activity of neural populations in affected regions (35, 36). SCI can also cause cognitive deficits, potentially due to chronic inflammation and glial activation. Elevated pro-inflammatory factors in the brain after SCI hinder neurogenesis and lead to neurodegeneration (37–39).
HIIT ameliorates cerebral neurodegeneration by upregulating hippocampal PINK1, Parkin, and BDNF proteins, promoting AMP-dependent protein kinase expression, and reducing amyloid-β protein accumulation in Alzheimer’s disease models. These effects improve memory and learning abilities (33) (see Table 2 [3]). Studies on exercise training in SCI models show increased IL-6 levels and reduced pro-inflammatory cytokines, such as IL-1β and TNF-α, in the hippocampus. Exercise also decreases IFN-γ levels, counteracting chronic brain inflammation. Additionally, exercise promotes selective transport of the synaptic protein SNAP25, induces PGC-1α and SIRT1 upregulation, reduces p53 acetylation, and increases mitochondrial respiratory complex content, thereby regulating brain plasticity and activating neuroprotective pathways (40). Nevertheless, further research is needed to elucidate the effects of HIET on the brain microenvironment and on neuronal remodeling and repair.
SCI often extends to remote regions, inducing secondary plastic changes in the peripheral nervous system. It disrupts motor signal transmission, resulting in prolonged limb immobility, secondary complications from compression or inactivity, and potential atrophy and degeneration of motor neuron pools distal to the lesion (41). Studies suggest that intermittent exercise of any intensity can promote axonal growth in injured peripheral nerves, with HIIT showing more pronounced effects. The intensity of exercise is directly proportional to neurotrophic factor content, which enhances the proliferative activity of peripheral neuron precursor cells. This activity promotes neuronal migration to injured areas, mitigates apoptosis, and stimulates growth of movement-related axons, facilitating peripheral nerve repair (41, 42).
HIET can modulate the inflammatory response by balancing pro-inflammatory and anti-inflammatory factors. The immune system primarily drives the inflammatory response in spinal cord tissues following SCI, which induces a neuroinflammatory reaction predominantly mediated by microglia (MG) and macrophages within the tissues (43). Subsequently, platelets release cytokines, chemokines, and eicosanoids, initiating neutrophil infiltration. Activated MGs secrete significant quantities of pro-inflammatory factors, resulting in extensive infiltration of inflammatory cells and cytokines and delaying leukocyte recovery (43, 44).
Regulatory T cells (Tregs) represent a subset of T cells that regulate autoimmune reactivity in vivo and play an anti-inflammatory role following SCI. Walsh et al. (45) reported that HIET increases Treg levels more effectively than low- and moderate-intensity training, thereby suppressing the inflammatory response in spinal cord tissues and mitigating the secondary damage caused by excessive inflammation. Another study (16) (see Table 1 [3]) involved both SCI patients and able-bodied individuals undergoing three exercise sessions at varying relative intensities: at ventilatory threshold 1 (VT1), 15% below VT1, and 15% above VT1. The sessions were conducted with 48-h to 7-day intervals to ensure complete recovery. A single bout of exercise increased the circulating concentration of interleukin-6 (IL-6), which is secreted by contracting myocytes. This elevation triggered an anti-inflammatory cascade, thereby mitigating the excessive inflammatory response.
The findings demonstrated that, regardless of intensity, the levels of IL-6, IL-8, IL-10, and IL-4 increased in all participants. However, individuals with SCI exhibited higher levels of pro-inflammatory factors, including IL-1β, IL-2, and tumor necrosis factor-alpha (TNF-α), than able-bodied individuals, while displaying lower levels of anti-inflammatory factors such as IL-1ra, IL-4, and IL-10. Thus, it can be inferred that individuals with SCI require relatively intense HIET to counteract the progressive decline in the acute systemic anti-inflammatory cytokine response. Achieving a balance between pro-inflammatory and anti-inflammatory cytokine levels similar to that of the general population may alleviate excessive inflammatory responses.
HIET has been demonstrated to alleviate cramping, enhance bone density, and improve myasthenia gravis more effectively than exercises of lower intensity. Paralysis following SCI frequently leads to neurogenic disuse osteoporosis, significantly increasing the risk of fractures in the distal femur and proximal tibia (46). Alterations in the excitability of supraspinal inhibitory pathways, combined with heightened motor neuron excitability after SCI, contribute to spasticity (47). Additionally, prolonged bed rest and diminished central nervous system control of skeletal muscles in individuals with SCI may cause muscle atrophy, attributed to changes in acetylcholine receptor subtypes and reduced acetylcholinesterase activity (39).
Chen et al. (48) (see Table 2 [4]) demonstrated that HIET accelerates systemic fluid circulation in growing rats while enhancing the metabolism and absorption of minerals and related substances, thereby promoting calcium and phosphorus ion deposition in bones, including the tibia, knee, and hip joints. Compared to low- and moderate-intensity endurance training, HIET yielded superior improvements in bone mineral density, bone structure, and bone tissue, as well as increased levels of osteocalcin, alkaline phosphatase, and anti-tartrate-resistant acid phosphatase during the growth period. These findings suggest that HIET may lower the risk of fractures in the distal femur and proximal tibia.
Gong (49) proposed that HIIT, a form of HIET, stimulates the potential of myocyte responses, promoting skeletal muscle hypertrophy more effectively than moderate-intensity continuous training. Sprint interval training, a subset of HIIT, was found to induce adaptive changes in rat adenylate-activated protein kinase (AMPK) through sprint interval exercise, enhancing the expression and translocation of glucose transporter 4 (GLUT4) in skeletal muscle and mitigating skeletal muscle cell damage caused by exhaustive exercise (50) (see Table 2 [9]).
Fang (51) (see Table 2 [5]) observed that HIET stimulated brain-derived neurotrophic factor (BDNF) and TrkB synthesis in SCI rats more effectively than low- and moderate-intensity training, ameliorating spasticity in the lower limbs of individuals with incomplete SCI. Similarly, Zhang et al. (47) (see Table 1 [7]) established a positive correlation between exercise intensity and spasticity improvement in individuals with SCI. Patients were categorized into three groups: conventional rehabilitation, low-intensity training, and high-intensity training. Both exercise groups utilized the MOTOmed intelligent exercise trainer to train lower limbs in conjunction with conventional rehabilitation. Low intensity was defined as 8–10 on Borg’s Perceived Exertion Scale (BPE), while high intensity was rated at 14–15. Spasticity in the ankle plantar flexor calf triceps was assessed using the Modified Ashworth Scale (MAS) and Modified Tardieu Scale (MTS). The results confirmed a positive correlation between training intensity and spasticity improvement.
Furthermore, high-intensity treadmill training has been shown to enhance neuromuscular synergy in individuals with SCI, thereby improving muscle coordination, increasing movement efficiency and accuracy, and facilitating motor function recovery (52) (see Table 1 [8]).
Individuals with SCI often develop neuropathic pain, including abnormal pain, spontaneous pain, and nociceptive sensitization (53). Exercise training has been shown to mitigate neuropathic pain by strengthening sensory pathways, enhancing neuroplasticity, activating anti-inflammatory mechanisms, and suppressing inflammatory mediators and neurotransmitters involved in pain pathways (54). Exercise also modulates γ-aminobutyric acid levels in the dorsal horn of the spinal cord through TrkB signaling, alleviating mechanical allodynia and thermal hyperalgesia in rats with incomplete SCI (55).
Although few studies have explored the impact of exercise intensity on neuropathic pain, HIET is hypothesized to exert a more substantial influence on sensory pathways, neuroplasticity, and anti-inflammatory responses than low- or moderate-intensity exercise. Consequently, the potential of HIET in alleviating neuropathic pain warrants further investigation.
HIET has been shown to provide patients with SCI a heightened sense of security and control over their bodies, fostering hope and enabling them to achieve their goals (56). This approach has demonstrated efficiency in achieving desirable results within a short timeframe (57, 58) (see Table 1 [9, 10]), thereby reducing hospitalization costs and expediting the resumption of normal life activities. Training conducted on surfaces resembling those encountered in daily life, such as running tracks, has been found to facilitate reintegration into real-world activities more effectively (17).
SCI results in motor and sensory deficits as well as autonomic dysfunction. Hyporeflexia or hyperactivity of the urethral and sphincter muscles and dysfunction in urethral-sphincter synergy are typical symptoms of SCI-induced abnormal voiding. Gastrointestinal dyskinesia associated with SCI includes gastric dilatation, delayed gastric emptying, and reduced propulsive transport throughout the gastrointestinal tract (59). Interestingly, the functions of the urinary and digestive systems may be improved through enhanced neural stimulation induced by HIET, although the underlying mechanisms remain unclear (60, 61).
Although HIET offers neuroprosthetic benefits for individuals with SCI, because of excessive exercise intensity, duration and frequency of practice, it also presents certain challenges (Figure 2), including the potential for excessive inflammatory responses, impaired mitochondrial function, all of which can exacerbate secondary injuries. Zhan et al. (62) (see Table 2 [6]) observed that SCI mice undergoing HIET exhibited reduced endurance during training and a higher mortality rate compared to mice subjected to low- or moderate-intensity training. Excessive HIET poses two principal risks: (1) when anti-inflammatory factors such as interleukin (IL)-10 and IL-4 predominate, the inflammatory response is suppressed excessively, leading to compromised immunity and increased susceptibility to infections such as urinary tract infections; (2) when pro-inflammatory factors such as IL-6 and IL-8 dominate, the inflammatory response intensifies, exacerbating secondary injuries (16) (see Table 1 [3]).
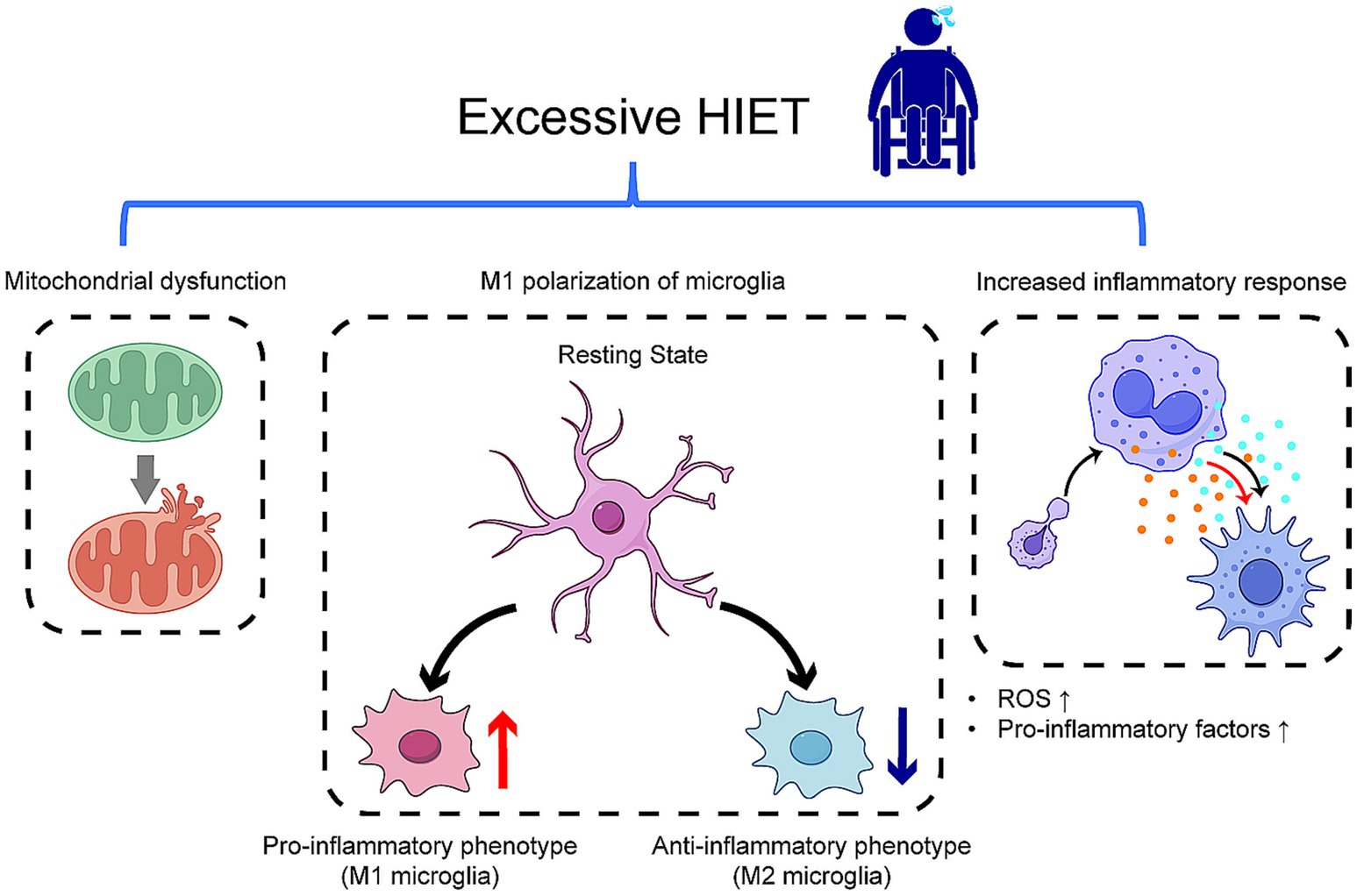
Figure 2. Effects of excessive HIET on spinal cord histopathological changes excessive exercise intensity can lead to heightened inflammation due to increased levels of pro-inflammatory or anti-inflammatory factors, resulting in diminished immunity, elevated ROS, mitochondrial swelling, and M1 polarization of microglia. These adverse effects hinder neuronal repair and contribute to secondary damage. ROS, reactive oxygen species.
Furthermore, while HIET enhances mitochondrial function, it may also elevate ROS levels, aggravating local tissue inflammation and accelerating tissue damage (34, 63). Although HIET promotes brain-derived neurotrophic factor (BDNF) production, excessive BDNF levels may result in adverse neuronal plasticity due to insufficient neuromodulation mechanisms, potentially triggering M1 polarization of spinal microglia (64). This process can heighten nociceptive sensitivities, promote hyperexcitability, and strengthen neuronal circuits through activation of the TrkB signaling pathway, leading to persistent chronic pain. Elevated BDNF levels may also cause mitochondrial swelling and myocyte damage (42, 55, 64, 65) (see Table 2 [7]).
Remarkably, SCI may also impair reproductive function. A previous study reported that HIET decreases sperm quality in SCI rats (66) (see Table 2 [8]). However, the effects and mechanisms underlying SCI-related reproductive dysfunction require further investigation.
To date, few studies have evaluated the effects of HIET on functional recovery following SCI, and a standardized definition of HIET remains absent. Many studies have not adequately accounted for gender differences or the influence of other treatment modalities as part of a comprehensive SCI management regimen. Clinical studies often adopt conservative definitions of HIET for safety considerations, limiting the reliability and generalizability of the results. Although evidence suggests that HIET enhances functional recovery efficiency and effectiveness after SCI, it is not widely implemented to prevent secondary injuries due to the lack of precise evaluation criteria. Additionally, the absence of standardized intensity thresholds in animal models highlights the need for improved understanding and definition of “high intensity.”
Debates regarding the definition and safety of exercise intensity have hindered the adoption of HIET in the physical rehabilitation of patients with neurological injuries (17). Many patients with SCI have an incomplete and inadequate understanding of exercise intensity, often failing to distinguish between moderate and high intensity. Furthermore, miscommunication and cognitive discrepancies between healthcare professionals and patients can result in insufficient exercise intensity or the conflation of intensity with frequency and duration, thereby diminishing rehabilitation effectiveness (58) (see Table 1 [10]).
HIET is typically categorized into aerobic and resistance exercise. According to the American College of Sports Medicine Guidelines for Exercise Testing and Exercise Prescription (9th Edition) (67), exercise intensity is classified as follows: low intensity (<57% of maximum heart rate), lower intensity (57–<64%), moderate intensity (64–<76%), higher intensity (76–<96%), and HIET (96–100%). While this classification is broadly applicable, specific testing protocols and guidelines tailored to individuals with SCI are required to develop personalized treatment plans for optimal outcomes. Moreover, healthcare professionals must prioritize patient education, emphasizing the significance of exercise intensity and clearly explaining training methodologies, indicators, and metrics to enhance comprehension and adherence to rehabilitation protocols.
The commonly employed method for monitoring exercise intensity is heart rate measurement, which is practical for real-time monitoring during exercise (18, 68, 69) (see Table 1 [4, 11]). However, Fahey et al. (17) highlighted that individuals with SCI may exhibit reduced neuromuscular force due to lower extremity weakness, which limits their cardiovascular response. Consequently, the measured maximum heart rate may underestimate the actual value, leading to overestimation of exercise intensity responses. Additionally, the use of medications such as beta-blockers to manage comorbidities in individuals with SCI can further compromise the accuracy of heart rate measurements (70). Therefore, further research is essential to elucidate the effects of SCI and related medications on heart rate responses to facilitate the development of improved treatment regimens.
SCI-induced physical dysfunction significantly impairs the ability to complete exercises and movements, leading to frustration, depression, and psychological fear among patients. Studies have demonstrated that HIET may decrease the willingness to train in SCI-affected rats due to the challenges in execution, thereby reducing training efficiency (71). Sterling et al. (56) reported that physical impairments resulting from SCI heighten patients’ fear of falling during exercise. Consequently, individuals must exert greater focus on seemingly simple movements, leading to elevated levels of fatigue.
Additionally, patients have indicated that exercise equipment often cannot adapt to the real-time changes in their physical condition. The absence of proprioception makes it difficult to maintain stability on dynamic platforms, causing discomfort and strain during treadmill use. In such conditions, patients are also required to monitor their heart rate to maintain exercise intensity, and the constant shift in attention negatively impacts the continuity of their exercise routines. Therefore, conducting exercise training in outdoor environments, when feasible, could facilitate patient adaptation to daily life and positively influence their mood (72, 73).
To enhance exercise intensity monitoring, patients should not rely solely on visual prompts displayed on screens. Sports headphones can be utilized to provide auditory cues for exercise intensity through voice prompts, allowing for dynamic adjustments. In cases where training must be conducted indoors, virtual reality (VR) technology may create a visually secure and stimulating environment, alleviating the monotony of training sessions (74). Furthermore, real-time pressure detection could be integrated to adjust the treadmill’s speed automatically, ensuring both exercise intensity and patient safety, thus alleviating psychological barriers.
The proportion of female subjects in clinical trials related to SCI remains disproportionately low, and there is an absence of heart rate parameters tailored specifically to SCI individuals, resulting in imprecise outcomes. Additionally, animal studies related to HIET are limited in scope.
Although the incidence of SCI is slightly higher in males than females (75), many clinical trials on exercise training intensity in SCI populations exhibit an imbalanced sex ratio, with female participants being underrepresented (76). This disparity has significant implications, as female SCI patients may not receive appropriately tailored treatments and could face unnecessary risks.
Most studies on exercise prescription for SCI adopt a conservative approach to intensity. The criteria in many trials are derived from maximal heart rate data of able-bodied individuals, failing to account for variations in cardiovascular dynamics post-SCI (17). Such oversights introduce errors in clinical trials and undermine the efficacy of exercise interventions in the SCI population. Future clinical trials must ensure gender balance to generate specialized, accurate exercise intensity data.
Moreover, studies investigating the progression of exercise intensity in SCI animal models remain sparse. A summary of HIET research in animal models is provided in Table 2. Current animal protocols lack a standardized framework for exercise intensity progression, often relying on platform training with intensity achieved by controlling platform speed. Some experiments determine the maximal speed of mice and set training speed proportionately, while others directly set fixed speeds. However, general criteria for high intensity in laboratory or clinical settings overlook the physiological differences between able-bodied individuals and SCI patients, compromising the accuracy and validity of experimental data.
HIET has been shown to improve training efficiency, reduce recovery time, and activate protective physiological mechanisms (19). However, no single treatment modality is sufficient for SCI recovery. HIET should be integrated with complementary therapies, such as cellular therapy, laser acupuncture, functional electrical stimulation, and brain-computer interfaces, to enhance therapeutic outcomes (77).
HIET, when improperly implemented, can lead to additional injuries. High-intensity interval training (HIIT) has been found to be more effective than continuous exercise in mitigating muscle fiber damage caused by sustained exertion. HIIT also enhances AMP-activated protein kinase (AMPK) phosphorylation, leading to increased expression and translocation of glucose transporter protein 4 (GLUT4) in skeletal muscles (50) (see Table 2 [9]). Consequently, intermittent exercise improves exercise capacity more effectively than continuous exercise. Based on the findings of various studies, HIIT is considered a preferred modality for SCI rehabilitation.
HIET is also associated with regulation of ROS and inflammatory mediators in the body. HIIT protocols should begin with moderate or low-intensity exercises, progressively increasing intensity to facilitate adaptation in both animal models and humans. During HIET, patients should aim to maintain their heart rate between 70 and 80% of their maximum heart rate, a target critical for achieving the desired exercise intensity while ensuring safety. Also, given the effects of medications on heart rate, patients can combine heart rate and exertion scales to control exercise intensity. This adaptability in training design enhances patient confidence and optimizes program effectiveness.
The use of exoskeletons in HIET programs can reduce exercise intensity; thus, reliance on such devices should be minimized, or exercise intensity should be increased proportionally (78). Additionally, training programs should prioritize restoring patients’ original functions rather than compensating for deficits. The design of exercises should replicate real-life scenarios, promoting convenience and efficiency to expedite reintegration into society.
Exercise training is inherently monotonous and exhausting, making patient autonomy a crucial element of rehabilitation. Cooperation and initiative from patients are essential, especially in HIET, which demands high levels of motivation to maintain adherence and maximize training outcomes (56).
To improve patient engagement, VR and other somatosensory technologies may be employed to enhance the entertainment value of training. These tools can provide immersive, professionally guided movement experiences, even within home settings. Medical staff should also encourage patients to overcome psychological barriers.
Community-based rehabilitation plays a pivotal role in post-hospitalization training. Medical institutions should collaborate with community organizations to strengthen patient education. Communities must also be equipped with adequate personnel and resources to support rehabilitation programs effectively.
In clinical research, the maximum heart rate values of individuals with SCI should be systematically investigated to refine exercise prescriptions. Structural changes in the body, pharmacological interventions, gender differences, and other relevant factors must be incorporated to ensure accurate monitoring during clinical trials. These considerations will optimize the intensity and modalities of exercise training, such as combining heart rate with perceived exertion scales, facilitating the clinical application of HIET for individuals with SCI. Furthermore, the integration of HIET with other therapeutic interventions could enhance the overall efficacy of SCI treatment.
In basic research related to SCI, the standardization of exercise intensity settings and progression protocols for animal experiments is essential. These protocols should align with the methodologies established for other disease models. Additionally, the effects and mechanisms of HIET on brain-derived neurotrophic factor (BDNF) merit focused investigation. Rather than merely promoting high levels of BDNF expression, it is critical to determine the optimal exercise intensity interval that achieves therapeutic benefits.
Moreover, the regulation of anti-inflammatory and pro-inflammatory factors during the inflammatory response induced by HIET warrants further study. This research could help minimize secondary injuries associated with SCI and create a favorable environment for spinal cord tissue repair.
HIET has the potential to promote the repair of spinal cord tissue structure and function, enhance cardiorespiratory performance, mitigate central nervous system degeneration, modulate inflammatory responses, and reduce systemic complications associated with SCI. The underlying mechanisms include increasing BDNF levels, promoting oligodendrocyte production, decreasing pro-inflammatory factors, elevating anti-inflammatory factors and regulatory T-cells (Tregs), and improving biomarkers of cardiometabolic risk. However, it is important to note that excessive exercise intensity can cause secondary injuries. Such adverse effects may result from elevated pro-inflammatory and anti-inflammatory factors, necessitating careful monitoring of the psychological and physical state of patients during training and developing individualized HIET plans and conduct further research to validate the benefits and address the risks. The present study has certain limitations. First, due to the paucity of existing research, this study does not differentiate between complete and incomplete SCI, which are distinct in clinical practice. Future research should address these distinctions, considering the varying implications of different spinal cord segments. Second, the limited number of studies on HIET in SCI has necessitated reliance on findings from CNS diseases unrelated to SCI for certain inferences and hypotheses in this article. Consequently, explicit and in-depth exploration of exercise training methodologies for SCI is an urgent priority for future research.
XL: Conceptualization, Investigation, Methodology, Writing – original draft, Writing – review & editing. QL: Writing – original draft, Writing – review & editing. CL: Writing – original draft, Writing – review & editing. CZ: Writing – original draft, Writing – review & editing. JQ: Writing – review & editing, Methodology, Supervision. XZ: Writing – original draft, Writing – review & editing, Conceptualization, Funding acquisition, Investigation, Methodology, Project administration, Supervision.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the National Natural Science Foundation of China (no. 82202822) and the Fundamental Research Funds for the Central Universities (the Laboratory of Exercises Rehabilitation Science, no. 2024KFZX009).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Liu, P. Research Progress on treatment methods for spinal cord injury. J Mod Med Health. (2023) 39:1720–6. doi: 10.3969/j.issn.1009-5519.2023.10.022
2. Collaborators, GBDSCI. Global, regional, and National Burden of spinal cord injury, 1990-2019: a systematic analysis for the global burden of disease study 2019. Lancet Neurol. (2023) 22:1026–47. doi: 10.1016/S1474-4422(23)00287-9
3. Eli, I, Lerner, DP, and Ghogawala, Z. Acute traumatic spinal cord injury. Neurol Clin. (2021) 39:471–88. doi: 10.1016/j.ncl.2021.02.004
4. Cao, N, Feng, YP, and Xie, JX. Interpretation of “clinical guidelines for Neurorestorative in spinal cord injury (2021 China version)”. Chin J Contemp Ncurol Neurosurg. (2022) 22:655–61. doi: 10.3969/j.issn.1672-6731.2022.08.002
5. He, L, Chen, JS, Liu, S, and Luo, LY. The value of rehabilitation training for the recovery of neurological function and quality of life after spinal cord injury. Chinese Commun Phys. (2020) 36:173–4. doi: 10.3969/j.issn.1007-614x.2020.26.085
6. Zhang, FS, Xie, HX, Gao, DY, Yang, YH, Di, H, Zhang, J, et al. Survey and analysis of rehabilitation training for people with spinal cord injury in Shanghai. Chin J Rehab Med. (2020) 35:1403. doi: 10.3969/j.issn.1001-1242.2020.11.014
7. Xie, QF, Xie, YY, Hu, Q, Chen, XL, Lin, JW, and Ying, XW. Water treadmill training promotes the polar expression of aquaporin 4 and reduces tissue edema after spinal cord injury in rats. J Wenzhou Med Univ. (2023) 53:450–7. doi: 10.3969/j.issn.2095-9400.2023.06.003
8. Zheng, Y, Mao, YR, Yuan, TF, Xu, DS, and Cheng, LM. Multimodal treatment for spinal cord injury: a sword of neuroregeneration upon neuromodulation. Neural Regen Res. (2020) 15:1437–50. doi: 10.4103/1673-5374.274332
9. Wu, J, Li, X, Wang, Q, Wang, S, He, W, Wu, Q, et al. LncRNA/miRNA/mRNA ceRNA network analysis in spinal cord injury rat with physical exercise therapy. PeerJ. (2022) 10:e13783. doi: 10.7717/peerj.13783
10. Chang, F, Zhang, Q, Xie, H, Yang, Y, Sun, M, Wu, A, et al. Effects of a rehabilitation program for individuals with chronic spinal cord injury in Shanghai, China. BMC Health Serv Res. (2020) 20:298. doi: 10.1186/s12913-020-05181-x
11. Lucas-Osma, AM, Schmidt, EKA, Vavrek, R, Bennett, DJ, Fouad, K, and Fenrich, KK. Rehabilitative training improves skilled forelimb motor function after cervical unilateral contusion spinal cord injury in rats. Behav Brain Res. (2022) 422:113731. doi: 10.1016/j.bbr.2021.113731
12. Li, NN, Yang, ZP, and Yang, WW. Effects of Core muscle group combined with limb linkage rehabilitation training on key muscle strength and balance ability of patients with lumbar segmental incomplete spinal cord injury. Henan Med Res. (2020) 29:3734–6. doi: 10.3969/j.issn.1004-437X.2020.20.033
13. Solinsky, R, Draghici, A, Hamner, JW, Goldstein, R, and Taylor, JA. High-intensity, whole-body exercise improves blood pressure control in individuals with spinal cord injury: a prospective randomized controlled trial. PLoS One. (2021) 16:e0247576. doi: 10.1371/journal.pone.0247576
14. Afshari, K, Ozturk, ED, Yates, B, Picard, G, and Taylor, JA. Effect of hybrid Fes exercise on body composition during the sub-acute phase of spinal cord injury. PLoS One. (2022) 17:e0262864. doi: 10.1371/journal.pone.0262864
15. Mahalakshmi, B, Maurya, N, Lee, SD, and Bharath, KV. Possible neuroprotective mechanisms of physical exercise in neurodegeneration. Int J Mol Sci. (2020) 21:5895. doi: 10.3390/ijms21165895
16. Alves, EDS, Dos Santos, RVT, de Lira, FS, Almeida, AA, Edwards, K, Benvenutti, M, et al. Effects of intensity-matched exercise at different intensities on inflammatory responses in able-bodied and spinal cord injured individuals. J Spinal Cord Med. (2021) 44:920–30. doi: 10.1080/10790268.2020.1752976
17. Fahey, M, Brazg, G, Henderson, CE, Plawecki, A, Lucas, E, Reisman, DS, et al. The value of high intensity locomotor training applied to patients with acute-onset neurologic injury. Arch Phys Med Rehabil. (2022) 103:S178–88. doi: 10.1016/j.apmr.2020.09.399
18. Hutchinson, MJ, and Goosey-Tolfrey, VL. Rethinking aerobic exercise intensity prescription in adults with spinal cord injury: time to end the use of "moderate to vigorous" intensity? Spinal Cord. (2022) 60:484–90. doi: 10.1038/s41393-021-00733-2
19. Jung, KS, Hutchinson, MJ, Chotiyarnwong, C, Kusumawardani, MK, Yoon, SH, Mikami, Y, et al. Dissonance in views between healthcare professionals and adults with a spinal cord injury with their understanding and interpretation of exercise intensity for exercise prescription. BMJ Open Sport Exerc Med. (2023) 9:e001487. doi: 10.1136/bmjsem-2022-001487
20. Dolbow, DR, Davis, GM, Welsch, M, and Gorgey, AS. Benefits and interval training in individuals with spinal cord injury: a thematic review. J Spinal Cord Med. (2022) 45:327–38. doi: 10.1080/10790268.2021.2002020
21. Huang, CL, Zhang, Y, Zhou, YY, Liu, WW, Zhao, MM, He, FC, et al. Effect of intensive rehabilitation nursing on cardiopulmonary function in patients with thoracolumbar spinal cord injury. Chin J Geriatr Care. (2020) 18:123–7. doi: 10.3969/j.issn.1672-2671.2020.03.049
22. Astorino, TA, Hicks, AL, and Bilzon, JLJ. Viability of high intensity interval training in persons with spinal cord injury-a perspective review. Spinal Cord. (2021) 59:3–8. doi: 10.1038/s41393-020-0492-9
23. Farrow, M, Maher, J, Deere, R, Spellanzon, B, Williams, S, Thompson, D, et al. Effect of high-intensity interval training on cardiometabolic component risks in persons with paraplegia: results of a randomized controlled trial. Exp Physiol. (2024) 109:1253–66. doi: 10.1113/EP091803
24. Hortobagyi, T, Vetrovsky, T, Balbim, GM, Sorte Silva, NCB, Manca, A, Deriu, F, et al. The impact of aerobic and resistance training intensity on markers of neuroplasticity in health and disease. Ageing Res Rev. (2022) 80:101698. doi: 10.1016/j.arr.2022.101698
25. Shi, XH. Research Progress on the mechanism of sports training promoting the repair of spinal cord injury. Chongqing Med. (2021) 50:3389–94. doi: 10.3969/j.issn.1671-8348.2021.19.032
26. Leech, KA, and Hornby, TG. High-intensity locomotor exercise increases brain-derived neurotrophic factor in individuals with incomplete spinal cord injury. J Neurotrauma. (2017) 34:1240–8. doi: 10.1089/neu.2016.4532
27. Kiss, K, Bacova, M, Kisucka, A, Gálik, J, Ileninova, M, Kuruc, T, et al. Impact of endurance training on regeneration of axons, glial cells, and inhibitory neurons after spinal cord injury: a link between functional outcome and regeneration potential within the lesion site and in adjacent spinal cord tissue. Int J Mol Sci. (2023) 24:616. doi: 10.3390/ijms24108616
28. An, LB, Liu, CH, Zhao, BL, Zhou, XH, and Li, WT. Effects of body weight support treadmill training with different exercise intensities on expressions of Trkb and Bdnf proteins in spinal cord tissue and its promotion effect on motor function recovery of rats with spinal cord injury. J Jilin Univ. (2019) 45:1389–94. doi: 10.13481/j.1671-587x.20190633
29. Zhan, ZX. Study of effect of treadmill exercise on Mtor pathway and motor function recovery in mice with spinal cord injury [master's thesis]. Chongqing: Chong Qing Medical University (2022).
30. Anjum, A, Yazid, MD, Fauzi, M, Idris, J, Ng, AMH, Selvi, A, et al. Spinal cord injury: pathophysiology, multimolecular interactions, and underlying recovery mechanisms. Int J Mol Sci. (2020) 21:7533. doi: 10.3390/ijms21207533
31. Zhou, HY, Cui, F, and Shuang, WB. The role and mechanism of mitochondrial dysfunction in progression of spinal cord injury. China Med Eng. (2020) 28:33–8. doi: 10.19338/j.issn.1672-2019.2020.09.009
32. Zhou, L. Salvia Divinorum attenuates the inflammatory damage of Β-amyloid in ad brain and its mechanism [Master's thesis]. Hunan: Central South University (2014).
33. Zhang, ZY, Kang, WM, Zhang, S, and Bo, H. High-intensity interval training-induced neuroprotection of Hippocampus in app/Ps1 transgenic mice via upregulation of mitophagy. Chin J Rehab Med. (2020) 35:670–5. doi: 10.3969/j.issn.1001-1242.2020.06.005
34. Gao, ZRD. Research Progress of mechanism and monitoring of neuromuscular function remodeling and regeneration in sprint training. Bullet Sport Sci Technol. (2023) 31:219–23,65. doi: 10.19379/j.cnki.issn.1005-0256.2023.03.061
35. Liu, XX, and Zhou, MW. Structural changes and functional remodeling of the brain after spinal cord injury. Chin J Rehab Med. (2021) 36:1026–30. doi: 10.3969/j.issn.1001-1242.2021.08.025
36. Zhao, C, Bao, SS, Xu, M, and Rao, JS. Importance of brain alterations in spinal cord injury. Sci Prog. (2021) 104:368504211031117. doi: 10.1177/00368504211031117
37. Li, Y, Cao, T, Ritzel, RM, He, J, Faden, AI, and Wu, J. Dementia, depression, and associated brain inflammatory mechanisms after spinal cord injury. Cells. (2020) 9:1420. doi: 10.3390/cells9061420
38. Li, Y, Ritzel, RM, Khan, N, Cao, T, He, J, Lei, Z, et al. Delayed microglial depletion after spinal cord injury reduces chronic inflammation and neurodegeneration in the brain and improves neurological recovery in male mice. Theranostics. (2020) 10:11376–403. doi: 10.7150/thno.49199
39. Sun, P, Ye, XM, Tian, L, Li, JB, and Cheng, RD. Effect of spinal cord injury on the expression of C-Fos in hypothalamus and neuronal apoptosis. China Modern Doctor. (2020) 58:45–8.
40. He, LW, Guo, XJ, Zhao, C, and Rao, JS. Rehabilitation training after spinal cord injury affects brain structure and function: from mechanisms to methods. Biomedicines. (2023) 12:10041. doi: 10.3390/biomedicines12010041
41. Redondo-Castro, E, and Navarro, X. Peripheral nerve alterations after spinal cord injury in the adult rat. Spinal Cord. (2013) 51:630–3. doi: 10.1038/sc.2013.57
42. Sabatier, MJ, Redmon, N, Schwartz, G, and English, AW. Treadmill training promotes axon regeneration in injured peripheral nerves. Exp Neurol. (2008) 211:489–93. doi: 10.1016/j.expneurol.2008.02.013
43. Brennan, FH, Li, Y, Wang, C, Ma, A, Guo, Q, Li, Y, et al. Microglia coordinate cellular interactions during spinal cord repair in mice. Nat Commun. (2022) 13:4096. doi: 10.1038/s41467-022-31797-0
44. Tian TaL, X. Problems and challenges in regeneration and repair of spinal cord injury. Chinese J Tissue Eng Res. (2021) 25:3039–48.
45. Walsh, CM, Gull, K, and Dooley, D. Motor rehabilitation as a therapeutic tool for spinal cord injury: new perspectives in immunomodulation. Cytokine Growth Factor Rev. (2023) 69:80–9. doi: 10.1016/j.cytogfr.2022.08.005
46. Sutor, TW, Kura, J, Mattingly, AJ, Otzel, DM, and Yarrow, JF. The effects of exercise and activity-based physical therapy on bone after spinal cord injury. Int J Mol Sci. (2022) 23:608. doi: 10.3390/ijms23020608
47. Zhang, JL, Sou, L, Li, XZ, Yin, JJ, Wu, QF, and Wang, HX. Effects of different intensities of exercises on spasticity and concentration of serum brain-derived neurotrophic factor in patients with incomplete spinal cord injury. Chin J Rehab Med. (2022) 37:80–4. doi: 10.3870/zgkf.2022.02.003
48. Chen, ZG, Ding, HL, Li, L, and Wang, C. Changes of bone metabolism after different intensity endurance exercises in growing rats. Chin J Tissue Eng Res. (2020) 24:3382–5588. doi: 10.3969/j.issn.2095-4344.2918
49. Gong, XW. Study on whether high-intensity interval training can promote skeletal muscle anabolism. Contemp Sports Technol. (2022) 12:1–4. doi: 10.16655/j.cnki.2095-2813.2201-1579-9022
50. Zhang, LM, Liu, JJ, Lin, XY, Liu, L, and Lu, J. Mechanism by which high-intensity intermittent exercise improves skeletal muscle injury and enhances exercise capacity in rats. Chin J Tissue Eng Res. (2023) 27:5603–9. doi: 10.12307/2023.890
51. Fang, L. Research on the effect of exercise training on spasticity and its mechanism in rats after spinal cord injury [Master’s thesis]. Nanjing: Nanjing Medical University (2018).
52. Ardestani, MM, Henderson, CE, Salehi, SH, Mahtani, GB, Schmit, BD, and Hornby, TG. Kinematic and neuromuscular adaptations in incomplete spinal cord injury after high- versus low-intensity locomotor training. J Neurotrauma. (2019) 36:2036–44. doi: 10.1089/neu.2018.5900
53. Chen, L, Lei, J, and Yu, HJ. Progress of research on the mechanism and treatment of pathologic pain after spinal cord injury. Chin J Pain Med. (2022) 28:843–8. doi: 10.3969/j.issn.1006-9852.2022.11.008
54. Palandi, J, Bobinski, F, de Oliveira, GM, and Ilha, J. Neuropathic pain after spinal cord injury and physical exercise in animal models: a systematic review and meta-analysis. Neurosci Biobehav Rev. (2020) 108:781–95. doi: 10.1016/j.neubiorev.2019.12.016
55. Li, X, Wang, Q, Ding, J, Wang, S, Dong, C, and Wu, Q. Exercise training modulates glutamic acid Decarboxylase-65/67 expression through TRKB signaling to ameliorate neuropathic pain in rats with spinal cord injury. Mol Pain. (2020) 16:1744806920924511. doi: 10.1177/1744806920924511
56. Sterling, MK, Wouda, MF, and Lahelle, AF. A qualitative interview study on how people with incomplete spinal cord injury experience high-intensity walking exercise. Spinal Cord Ser Cases. (2021) 7:92. doi: 10.1038/s41394-021-00456-9
57. Graham, K, Yarar-Fisher, C, Li, J, McCully, KM, Rimmer, JH, Powell, D, et al. Effects of high-intensity interval training versus moderate-intensity training on cardiometabolic health markers in individuals with spinal cord injury: a pilot study. Top Spinal Cord Inj Rehabil. (2019) 25:248–59. doi: 10.1310/sci19-00042
58. McLeod, JC, Diana, H, and Hicks, AL. Sprint interval training versus moderate-intensity continuous training during inpatient rehabilitation after spinal cord injury: a randomized trial. Spinal Cord. (2020) 58:106–15. doi: 10.1038/s41393-019-0345-6
59. Hou, S, and Rabchevsky, AG. Autonomic consequences of spinal cord injury. Compr Physiol. (2014) 4:1419–53. doi: 10.1002/cphy.c130045
60. Hubscher, CH, Montgomery, LR, Fell, JD, Armstrong, JE, Poudyal, P, Herrity, AN, et al. Effects of exercise training on urinary tract function after spinal cord injury. Am J Physiol Renal Physiol. (2016) 310:F1258–68. doi: 10.1152/ajprenal.00557.2015
61. Ouyang, S, Wang, X, Chen, Y, Deng, L, Yang, X, Hu, S, et al. Swimming training combined with fecal microbial transplantation protects motor functions in rats with spinal cord injury by improving the intestinal system. Neurosci Lett. (2023) 799:137104. doi: 10.1016/j.neulet.2023.137104
62. Zhan, Z, Pan, L, Zhu, Y, Wang, Y, Zhao, Q, Liu, Y, et al. Moderate-intensity treadmill exercise promotes Mtor-dependent motor cortical neurotrophic factor expression and functional recovery in a murine model of crush spinal cord injury (Sci). Mol Neurobiol. (2023) 60:960–78. doi: 10.1007/s12035-022-03117-6
63. Zhu, ZH, Zou, HJ, Song, ZW, and Liu, JB. Cellular microenvironment in nerve repair after spinal cord injury. Chin J Tissue Eng Res. (2023) 27:114–20. doi: 10.12307/2022.971
64. Bai, J, Geng, B, Wang, X, Wang, S, Yi, Q, Tang, Y, et al. Exercise facilitates the M1-to-M2 polarization of microglia by enhancing autophagy via the Bdnf/Akt/Mtor pathway in neuropathic pain. Pain Physician. (2022) 25:E1137–51.
65. Zhang, X, Yu, B, and Cai, BT. Effects of exercise intensities on expression of hypoxia inducible factor-1α Mrna in the skeletal muscle of rats. Chin J Orthop Trauma. (2006) 8:453–7. doi: 10.3760/cma.j.issn.1671-7600.2006.05.014
66. Zhou, XH. Study on the effect of weight-loss walking training on sperm quality in male rats with spinal cord injury [Master’s thesis]. Jilin: Jilin University (2020).
67. ACSM. Acsm’s guidelines for exercise testing and prescription. 9th ed. Beijing: Beijing Sport University Press (2015).
68. McMillan, DW, Maher, JL, Jacobs, KA, Nash, MS, and Bilzon, JLJ. Physiological responses to moderate intensity continuous and high-intensity interval exercise in persons with paraplegia. Spinal Cord. (2021) 59:26–33. doi: 10.1038/s41393-020-0520-9
69. Goosey-Tolfrey, VL, Hutchinson, M, and Sharpe, L. Infographic. Field-based methods for assessing exercise intensity in adults with spinal cord injury. Br J Sports Med. (2023) 57:203–4. doi: 10.1136/bjsports-2022-106226
70. Tsai, SW, Huang, YH, Chen, YW, and Ting, CT. Influence of Β-blockers on heart rate recovery and rating of perceived exertion when determining training intensity for cardiac rehabilitation. J Chin Med Assoc. (2015) 78:520–5. doi: 10.1016/j.jcma.2015.05.009
71. Fenrich, KK, Hallworth, BW, Vavrek, R, Raposo, PJF, Misiaszek, JE, Bennett, DJ, et al. Self-directed rehabilitation training intensity thresholds for efficient recovery of skilled forelimb function in rats with cervical spinal cord injury. Exp Neurol. (2021) 339:113543. doi: 10.1016/j.expneurol.2020.113543
72. Jannings, W, and Pryor, J. The experiences and needs of persons with spinal cord injury who can walk. Disabil Rehabil. (2012) 34:1820–6. doi: 10.3109/09638288.2012.665126
73. Jordan, MM, Berkowitz, D, Hannold, E, Velozo, CA, and Behrman, AL. Thinking through every step: how people with spinal cord injuries relearn to walk. Qual Health Res. (2013) 23:1027–41. doi: 10.1177/1049732313494119
74. Maggio, MG, Bonanno, M, Manuli, A, Onesta, MP, de, R, Quartarone, A, et al. Do individuals with spinal cord injury benefit from semi-immersive virtual reality cognitive training? Preliminary results from an exploratory study on an underestimated problem. Brain Sci. (2023) 13:945. doi: 10.3390/brainsci13060945
75. Ding, W, Hu, S, Wang, P, Kang, H, Peng, R, Dong, Y, et al. Spinal cord injury: the global incidence, prevalence, and disability from the global burden of disease study 2019. Spine. (2022) 47:1532–40. doi: 10.1097/BRS.0000000000004417
76. Liu, J, Gao, H, and Li, JJ. Epidemiology of patients with traumatic spinal cord injury and study on the influencing factors of hospitalization costs. Chin J Rehab. (2020) 35:139–42. doi: 10.3870/zgkf.2020.03.006
77. Neurorestoratology IAoNaCAo. Interpretation of clinical Neurorestorative therapeutic guidelines for spinal cord injury (Ianr/Canr version 2019). Med J West China. (2020) 32:790–802. doi: 10.3969/j.issn.1672-3511.2020.06.003
Keywords: athletic training, spinal cord injury, exercise intensity, high-intensity training, functional recovery
Citation: Li X, Li Q, Li C, Zhang C, Qian J and Zhang X (2025) Effect of high-intensity exercise training on functional recovery after spinal cord injury. Front. Neurol. 16:1442004. doi: 10.3389/fneur.2025.1442004
Edited by:
Giorgio Scivoletto, Santa Lucia Foundation (IRCCS), ItalyReviewed by:
Simon O’Carroll, The University of Auckland, New ZealandCopyright © 2025 Li, Li, Li, Zhang, Qian and Zhang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Xin Zhang, YXNobGV5X3poeGluQDE2My5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.