 Pedro Nogueira Fontana1,2*
Pedro Nogueira Fontana1,2* Vinícius Gomes da Silva1
Vinícius Gomes da Silva1 Roseli Corazzini1Natália Merten Athayde1
Roseli Corazzini1Natália Merten Athayde1 Ana Marina Dutra Ferreira da Silva1Igor Brockhausen1
Ana Marina Dutra Ferreira da Silva1Igor Brockhausen1 Carolina da Cunha Correia2
Carolina da Cunha Correia2 Cláudia Ferreira da Rosa Sobreira3Pedro José Tomaselli3Flávio Petean3
Cláudia Ferreira da Rosa Sobreira3Pedro José Tomaselli3Flávio Petean3 Rodrigo de Oliveira3
Rodrigo de Oliveira3 Pablo Vinícius Feitoza4
Pablo Vinícius Feitoza4 Michel Moraes Soane5Natália Saraiva5
Michel Moraes Soane5Natália Saraiva5 Rafaela Hidalgo5Cláudia Fideles5David Feder1
Rafaela Hidalgo5Cláudia Fideles5David Feder1 Alzira Alves de Siqueira Carvalho1*
Alzira Alves de Siqueira Carvalho1*- 1Neurosciences and Clinical Department, Centro Universitário ABC, Santo André, Brazil
- 2Faculty of Medical Sciences, Universidade de Pernambuco, Recife, Brazil
- 3Department of Neurosciences and Behavioral Sciences, Universidade de São Paulo - Ribeirão Preto, São Paulo, Brazil
- 4Department of Clinical Surgery, Faculty of Medicine, Universidade Federal do Amazonas, Manaus, Brazil
- 5EUROIMMUN Brazil, São Caetano do Sul, Brazil
Introduction: Differential diagnosis of rare idiopathic inflammatory myopathies (IIM) is mainly based on clinical aspects, muscle biopsy analysis, and auxiliary assays that determine myositis-specific and associated autoantibodies (MSA and MAA). While MSAs are considered specific for their respective IIM subclass, MAAs can be present in more than one subclass and in other conditions. This study compares results of a multispecific line blot assay with the final diagnosis of IIM patients based on clinical features and muscle biopsy to draw conclusions for the test's applicability in the diagnostic workflow.
Methods: Samples from patients (n = 50) diagnosed with various forms of IIM, including patients (n = 5) with other myopathies, were analyzed using the EUROLINE Autoimmune Inflammatory Myopathies 16 Ag (IgG), an anti-HMGCR (IgG) line blot, and the Anti-cN-1A ELISA (IgG, all EUROIMMUN).
Results: MSA and MAA were detected in 74.0% (37/50) of sera and were concordant with the final diagnosis in 64.8% (24/37), discordant in 16.2% (6/37) and not evaluable in 18.9% (7/37) of cases. In 100% (5/5) of patients with other myopathies, no MSA was found. MSA/MAA-co-positivity was observed in 18.0% (9/50) of patients. In 30.0% (15/50) of cases, the muscle biopsy analysis was essential to establish the final diagnosis.
Conclusion: The agreement between serodiagnostic results and final diagnosis highlights the applicability of the EUROIMMUN myositis-related diagnostic test as first line diagnostic tool in the IIM diagnosis workflow and suggests morphological analysis in cases of inconclusive or negative serology. However, results of diagnostic assays shall always be interpreted in combination with clinical features.
1 Introduction
Idiopathic inflammatory myopathies (IIM) are rare autoimmune diseases characterized by muscular weakness of varying severity and muscle inflammation. They are highly heterogeneous regarding phenotype, extra muscular involvement, creatine phosphokinase (CK) elevation and association with malignancies (1–3). Usually, the diagnosis is based on clinical aspects, muscle biopsy, and serodiagnostic assays of autoantibodies (AAbs) according to local availability.
The classification of IIM has evolved since the first description in 1975 by Bohan and Peter (4, 5). The advances of immunohistochemistry and the discovery of new myositis-specific antibodies (MSA) at the beginning of the 21st century led to a better understanding of the pathophysiology of IIM (6, 7). MSA have shown relevant clinical associations, e.g., with clinical phenotype, prognosis, risk of malignancy and treatment, providing better management of patients with IIM (8–10). Currently, IIM are divided into immune-mediated necrotizing myopathy (IMNM), dermatomyositis (DM), anti-synthetase syndrome (AsS), inclusion body myositis (IBM) and overlap myositis (OM) (1, 7, 11), based on clinical aspects, morphological findings and myositis-related antibodies [MSA and myositis associated antibodies (MAA)].
Anti-SRP and anti-HMGCR are associated with IMNM. They are related to myocarditis and malignancies, respectively. Also, seronegative cases should be screened for malignancies (12). Anti-Mi-2, anti-TIF1γ, anti-NXP2, anti-MDA5, and anti-SAE are characteristic MSA for DM with anti-TIF1γ, anti-NXP2, and anti-SAE1 related to malignancies (8, 10), and anti-MDA5 associated with severe interstitial lung disease (ILD) (8). Interferon type 1 activation is more distinguished in DM, while in AsS and IBM the interferon type 2 is more important (11). Since 2018, interferon type 1 signature is incorporated in DM diagnostic classification (13). Presence of anti-cN-1A is typical for IBM. However, anti-cN-1A has limited specificity as biomarker (14) because it can be detected in other autoimmune diseases, such as Sjögren's syndrome and systemic lupus erythematosus as well (15), making the muscle biopsy analysis important as diagnostic tool for this subgroup. Finally, AsS is a multisystem disease related to various MSA, such as, anti-Jo-1, anti-OJ, or anti-EJ, frequently in combination with ILD and with different therapeutic targets (16). It can present morphologically as a perimysial myopathy, which can suggest an AsS-specific antibody (Figure 1).
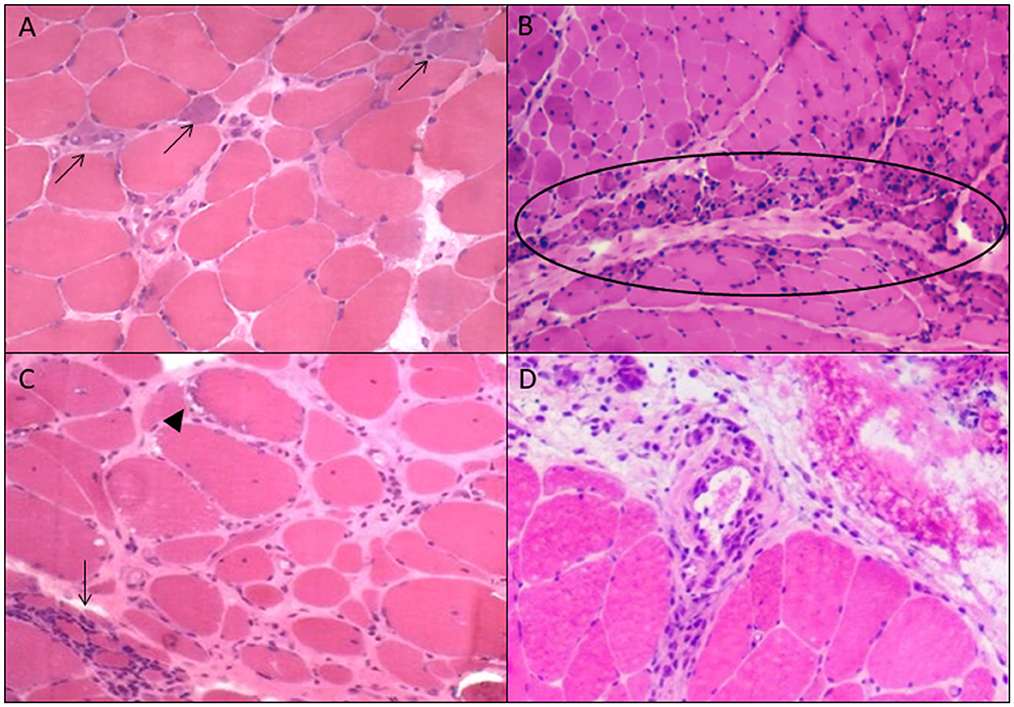
Figure 1. Morphological findings of each idiopathic inflammatory subgroup. (A) Immune-mediated necrotizing myopathy: necrosis and regeneration (arrows); (B) dermatomyositis: perifascicular atrophy (ellipse); (C) inclusion body myositis: rimmed vacuoles (arrowhead) and endomysial inflamation (arrow); (D) perimysial myopathy: perimysial inflammation and fragmentation.
MSA and MAA are detected mainly using immunoprecipitation (IP), ELISA, and line blot assays (17) with ELISA being the most used. IP is gold standard for myositis-related AAb detection applying native antigens. However, it is laborious and requires a high level of expertise, reducing its applicability as a routine test. ELISAs were developed for some antibodies, reaching a high agreement with IP. As new antibodies have been discovered, multispecific assays, such as line blots were developed. They allow easy accessibility and rapid and cost reduced processing but seem less sensitive and less specific (17).
The detection of myositis-related AAbs plays an important role corroborating the final diagnosis in IIM patients. This study aims to evaluate the performance and the clinical applicability of a multispecific line blot accompanied by an anti-HMGCR-specific line blot and an anti-cN-1A-specific ELISA compared to the final diagnosis of suspected IIM patients to draw conclusions for a diagnostic workflow.
2 Methods
2.1 Patients
This study included patients with IIM based on clinical symptoms and/or muscle biopsy showing typical inflammatory findings. Muscle biopsy samples were obtained according to standard methods (18) and analyzed using histochemistry and immunohistochemistry (IHC) assays. IHC was performed using the antibodies CD4 (Leica Biosystems, clone 4B12), CD8 (Leica Biosystems, clone 4B11), CD20 (Santa Cruz, clone D10 sc-393894), CD68 (Leica Biosystems, clone 514H12), C5b9 (Dako, clone aE11), MHC class I (Dako, clone W6/32) and p62 (Medaysis, clone MD61). The morphology was evaluated according to established criteria (6, 7, 19–22) by two different pathologists blinded to the serological result. Cases in which muscle biopsy analysis showed only MHC-I immunoexpression and no dystrophic changes were classified as immune-mediated myopathy (IMM).
2.2 Immunoassays
Patient sera were analyzed using the EUROLINE Autoimmune Inflammatory Myopathies 16 Ag (IgG) comprising the antigens Mi-2α, Mi-2β, -TIF1γ, MDA5, NXP2, SAE1, Ku, PM-Scl100, PM-Scl75, Jo-1, SRP, PL-7, PL-12, EJ, OJ, and Ro-52, a line blot for the detection of anti-HMGCR (IgG), and the anti-cN-1A (IgG) ELISA (all EUROIMMUN Medizinische Labordiagnostika AG, Germany). The assays were performed and evaluated according to the manufacturer's instructions with a sample being positive for presence of an individual antibody at moderate, strong, and very strong line intensities. For the anti-cN-1A (IgG) ELISA, the cut-off at a ratio ≥1.0 was applied. A sample was defined as co-positive when more than one AAb was present. In these cases, the muscle biopsy and clinical findings were considered to corroborate the respective AAb. A sample was defined as discordant when the serologic result differed from the classification based on clinical features and the muscle biopsy (for instance, IBM, DM, IMNM).
2.3 Statistical analysis
Fisher's exact test was used to verify the association between gender and serological status. The same test was used for immunosuppressant and serological status. Student's t test was used to verify the association between serological status and age at onset. The Mann-Whitney U test was used to verify the association between serological status and the non-normal quantitative variable CK levels.
2.4. Ethics
The study was approved by Clinical Research Ethics Committee of University Center Faculty of Medicine of ABC, CAAE: 49456021.9.0000.0082. Informed consent was obtained from all subjects according to the Declaration of Helsinki.
3 Results
3.1 Sample characterization
Fifty patients were included, being 18 males and 32 females, aged between 16 and 77 years (mean: 50.6 ± 15.7 years). Symptom onset ranged between age of 15–74 years (mean: 47 ± 15.5 years; median: 48 years; Table 1). At time of serum collection, 72% (36/50) of patients were on immunosuppressive therapy. Thirty-one patients were under corticosteroid treatment, 22 were using steroid-sparing agents, seven received intravenous immunoglobulin, one underwent plasmapheresis, one received rituximab and one abatacept.
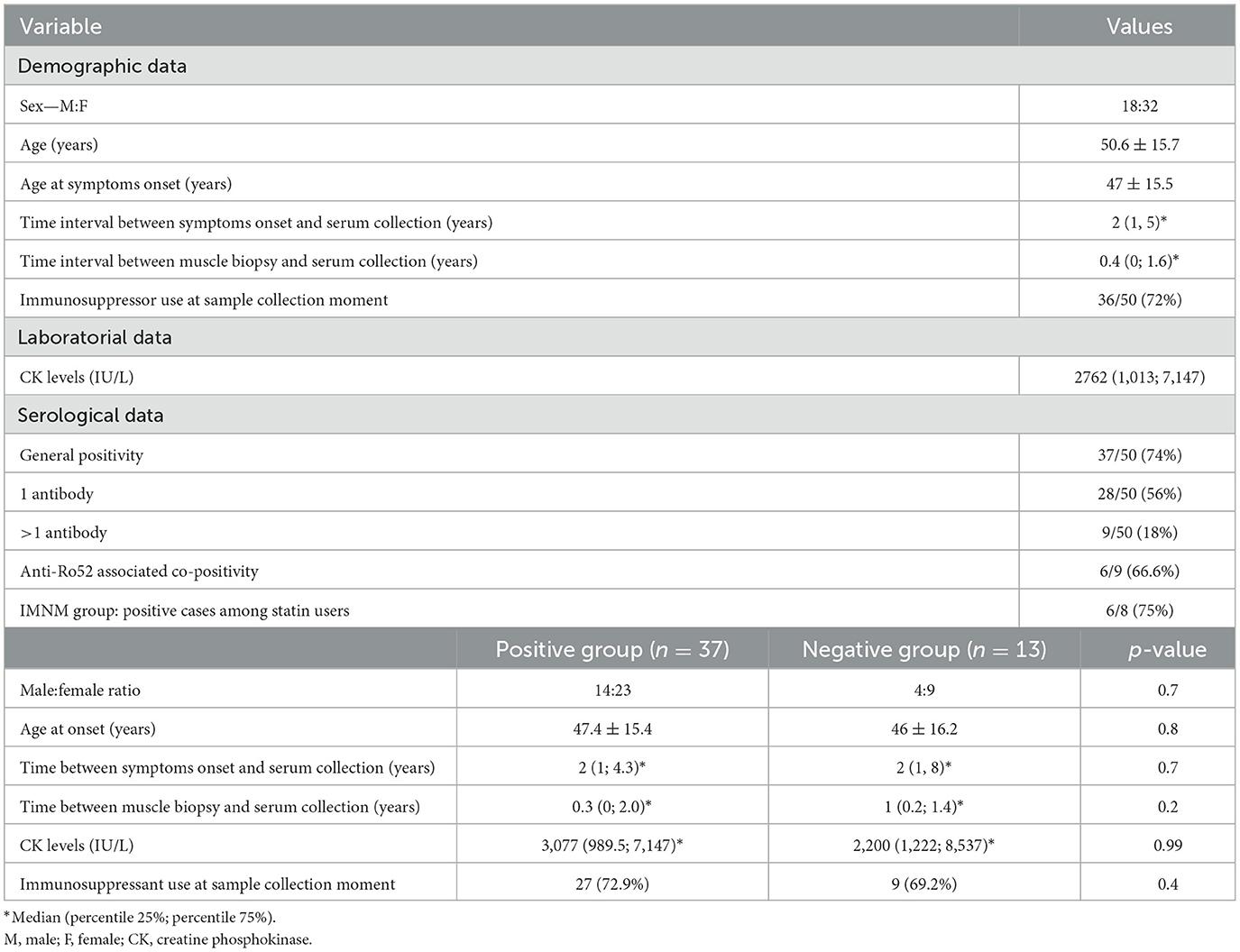
Table 1. Sample characterization.
3.2. Diagnosis according to clinic, histochemistry and immunohistochemistry
According to clinical picture and analysis of the muscle biopsy, 50 patients were diagnosed with IIM. The CK concentration in sera of these patients varied between 50 and 19,459 IU/L at a value considered as normal below 170 IU/L. In detail, IMNM in 21/50 (42%), of which eight were under statin use, DM in 8/50 (16%), immune-mediated myopathy (IMM) in 7/50 (14%), IBM in 5/50 (10%), and perimysial myopathy (PMM) in 4/50 (8%) patients. In five of 50 patients (10%), of which four were under statin use, other non-autoimmune mediated myopathies were found (cytoplasmic body myopathy, lipid storage myopathy, protein aggregate myopathy, nemaline myopathy and calpainopathy, Table 2).
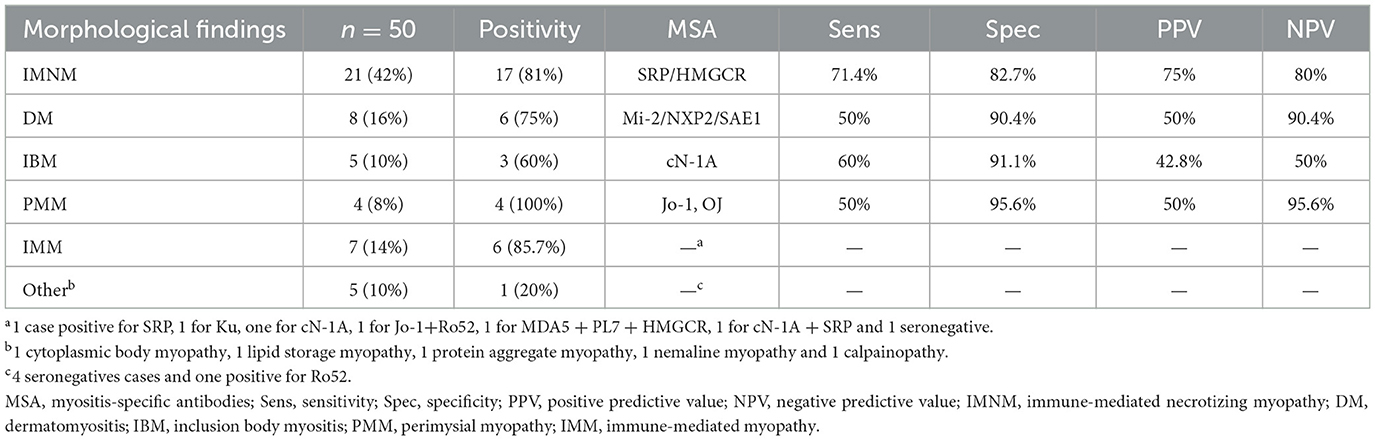
Table 2. Frequency of morphological and serological findings; sensitivity/specificity/PPV/NPV.
3.3. Serodiagnostics of MSA and MAA
In 37/50 sera (74.0%), MSAs (n = 34, 91.9% of positive samples) and MAAs (n = 3, 8.1%) were present. In 28 cases, sera were positive for one individual antibody; nine sera showed co-positivity, being five cases MSA-MAA copositivity and four MSA-MSA copositivity (Supplementary Table 1).
In the IMNM panel, sera were positive for anti-HMGCR and anti-SRP in 6/21 and 7/21 samples, respectively. From eight IMNM patients under statin use, five were positive for anti-HMGCR and one for anti-SRP. Moreover, one sample each was positive for anti-Mi-2, anti-Ku, co-positive for anti-SRP/anti-Ro52, and co-positive for anti-cN-1A/anti-HMGCR/anti-Ro52. Four samples were negative for the MSAs and MAAs investigated here. In DM sera, one sample each was positive for anti-SRP, anti-Mi-2, anti-NXP2, anti-cN-1A, co-positive for anti-SAE1/anti-Ro52/anti-Ku, and co-positive for anti-SAE1/anti-Ro52 and two samples were negative for MSA and MAA. From the PMM patients, one each was positive for anti-HMGCR and anti-Mi-2 and two sera were positive for anti-Jo-1. In IMM patient sera, in one sample each anti-SRP, anti-Ku, anti-cN-1A, anti-Jo-1/Ro52, anti-MDA5/anti-PL7/anti-HMGCR, and anti-cN-1A/anti-SRP were detected. One sample was negative for MSA and MAA. Sera from patients with IBM were positive for anti-cN-1A, anti-cN-1A/Ro52, and anti-cN-1A/anti-SRP with two samples negative for the MSA and MAA investigated here.
In sera from patients diagnosed with other non-immune mediated myopathies, one sample was anti-Ro52 positive, all other samples were seronegative (Supplementary Table 1). Agreement between muscle biopsy and serology occurred in 64.8% (24/37). Based on sub-class characteristic MSA and MAA, IMNM, DM, IBM, and PMM were found with a sensitivity of 71.4% (15/21), 50.0% (4/8), 60.0% (3/5), and 50.0% (2/4) and a specificity of 82.7%, 90.4%, 91.1%, and 95.6%, respectively (Table 2, Supplementary Table 3). In 6/37 (16.2%) cases, the results were discordant (Supplementary Table 2). In 7/37 (18.9%) sera from patients with IMM, concordance or discordance could not be determined since a specific AAb could not be defined for this myositis subclass. In 5/5 (100.0%) sera from patients with other myopathies, no MSA was found (Table 2).
4 Discussion
This study describes the results of a cohort of patients with IIM using muscle biopsy associated with clinical features as the gold standard for diagnosis in order to compare them with serological results (MSA/MAA).
There is some disagreement between different authors about which antibodies should be considered myositis-specific or myositis-associated (23); however, ~70% of IIM patient carry some myositis-related antibody (24). In the present study, we found a general positivity of 74% (37/50) and a MSA positivity of 83.8% (31/37), similar to what was previously reported (25). The high prevalence of immunossuppressive treatment (72%) suggests that it did not influence the serological results. According our results, even in patients with long standing disease, the serology test can be useful.
Although the sensitivity of MSA/MAA is limited, our study showed a good specificity, suggesting that MSA/MAA panel is a useful tool in the diagnostic workup (Table 2 and Figure 2). Furthermore, in cases in which the muscle biopsy showed findings compatible with some subtypes of IIM but with no evident clinical features compatible, the identification of AAbs helped the diagnostic conclusion. In the P13, with anti-Ku positivity and compatible clinical syndrome, the muscle biopsy showed IMNM aspects. In this case, anti-Ku defined the diagnosis. This is in accordance with previous reports showing that IMNM can occur in other diseases as anti-Ku syndrome (26).
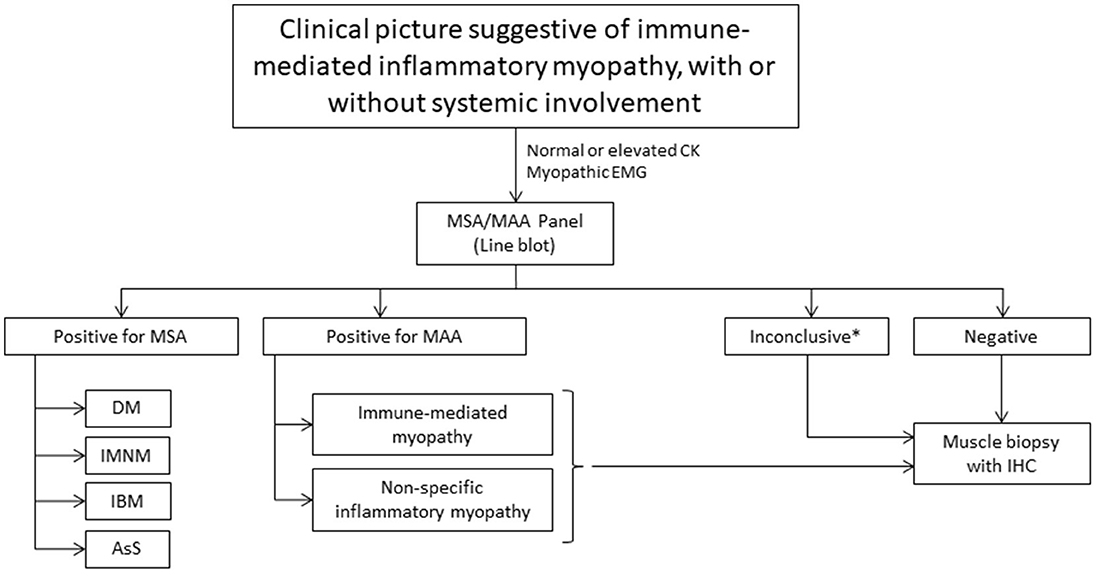
Figure 2. Diagnostic flowchart. CK, creatine phosphokinase; MSA, myositis-specific antibodies; MAA, myositis-associated antibodies; DM, dermatomyositis; IMNM, immune-mediated necrotizing myopathy; IBM, inclusion body myositis, AsS, anti-synthetase syndrome; IHC, immunohistochemistry. *Copositivity cases or clinical-serological discordance.
Our findings suggest that MSA/MAA panel is a useful diagnostic tool, in accordance with previously described (1, 6, 27, 28). The performance of multispecific line blot panels, being less invasive compared to muscle biopsy, makes this method an important ally as initial testing in the diagnostic evaluation of IIM. Our study, for the first time, showed 64.8% agreement between muscle biopsy findings and presence of antibodies, suggesting that the serological test can be used as a screening in IIM in order to avoid an invasive procedure. This high positivity led us to propose a diagnostic flowchart in IIM (Figure 2). Furthermore, the associations between MSA/MAA and clinical characteristics can guide specific therapeutic approaches, including malignancy screening and early management of ILD.
Malignancies are a factor of worse prognosis in IIM (29, 30). Classically, TIF1γ, NXP2 and SAE1 antibodies delimit a subset of subjects under a high risk of cancer, indicating the need for neoplastic screening and close monitoring, especially in the first 3 years after the onset of symptoms (27, 31–41). Although anti-HMGCR has been considered associated with neoplasia, some recent studies concluded the opposite and further investigations are necessary (42–44). Furthermore, seronegative IMNM subjects also are at higher risk of malignancies, which highlights the importance of serodiagnostics in this group of IIM (32). This predictive value is an advantage over muscle biopsy that, in general, cannot suggest a malignancy association. An exception to this are the punched out fibers in adult DM, found in TIF1γ cases (27); this pathological feature is particularly important in DM, since immunoblot have up to 50% of false-negativity for TIF1γ, and makes muscle biopsy important in seronegative DM (45). In addition, necrosis and regeneration, suggestive of IMNM, can be present in different neuromuscular disorders, so the presence of antibodies can guide the diagnostic approach.
Another important aspect of serology in DM subgroup is morphological similarity that can occur in both DM and AsS although with different pathophysiological mechanisms (46). The Mi2 positivity in one of our cases of perimysial myopathy (P31; Supplementary Table 2) is an example of this similarity. Also, in IMNM, serological diagnosis can help guide therapy, as individuals with refractory SRP positivity IMNM may have a good response to rituximab (19, 47, 48). In this context, MSA/MAA panels help to accelerate the diagnosis of IIM with a specific therapeutic target in a non-invasive way, allowing an early treatment.
The discovery of the role of interferon I and II in IIM (49) and the therapeutic effect of JAK/STAT inhibitor ruxolitinib in DM (9) brought new insights into the pathophysiology of IIM. In DM, there is an overexpression of genes induced by type I interferon (50, 51), making it a potential therapeutic target in this disease and paving the way for target-specific treatment.
Two cases were defined based on clinical features and serology but not by muscle biopsy (P24 and P48). The presence of eyelid rash and arthralgia (P24) along with Jo-1 allowed the diagnosis of AsS; although eyelid rash is considered typical of DM, it also can occur in AsS (52). A case with both SRP and cN1A (P48) could not be defined on pathological basis, but clinical features and CK levels were suggestive of IBM and in agreement with cN1A result (Supplementary Table 2).
In 15 (30%) cases (Supplementary Table 2), the muscle biopsy and clinical features were needed to define the final diagnosis, suggesting that the serology alone may not replace the clinical diagnosis and muscle biopsy. Disagreement between muscle biopsy and serology occurred in 16.2%. These cases had the final diagnosis defined by clinical features and muscle biopsy, suggesting that MSA can be found in different IIM; therefore, serology not always will determine the final diagnosis (Table 2), but is important as auxiliary diagnostic tool. Several reasons could explain this biopsy-antibody discordance, suggesting that serological tests should be used as screening or when the diagnostic workup was not conclusive. The different techniques available to detect AAbs in IIM can lead to different results (17, 19). The main methods used for AAbs detection are line blot, immunoprecipitation (IP) and ELISA (17), the former being the most used. IP, a conventional technology considered as a gold-standard for MSA and MAA detection, is laborious and require a high level of expertise, reducing its availability as a routine test. Thus, ELISA was developed for some antibodies, reaching a high agreement with IP. As new antibodies have been discovered, multispecific assays were developed, in order to be more accessible and cost reduced, although with lesser sensitivity and specificity (17). In the case of line blot, a multispecific assay, previous studies indicated that adjusting cutoff levels may be needed to increase specificity (53–55). Although imunoblot method has some limitations when compared to IP, several studies have demonstrated its usefulness in the current clinical practice as a screening tool (56, 57).
Co-positive cases represented a challenge to serological diagnosis of IIM. In 12% of cases, the responsible antibody was based on muscle biopsy diagnosis. Therefore, the muscle biopsy should not be the first exam in diagnostic workup of IIM. Nevertheless, serological testing remain useful in determine the prognosis and clinical approach in IIM.
This study shows a high agreement rate between serology (MSA/MSA) and morphological data, highlighting the importance and applicability of antibody testing as a screening test in IIM, being the muscle biopsy performed when serology is negative. Only in these cases, as well as in discordant cases, IP should be applied, as the higher costs and methodological issues limit its availability in the current clinical practice. Moreover, the serology is useful in determining prognosis and therapeutic approach. A limiting point of this study is the small sample size and, consequently, the low number of cases in some subgroups, common in rare diseases, which limits the interpretation of the results. A more robust sample would help to confirm our results, since a joint analysis of clinic, specific serology and muscle biopsy is not the daily reality of many services, and sometimes the patient is treated with an incomplete investigation. Nevertheless, our results show that clinical features remain the most important key point to reach the final diagnosis, regardless of isolated laboratorial tests.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Clinical Research Ethics Committee of University Center Faculty of Medicine of ABC. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants' legal guardians/next of kin.
Author contributions
PF: Data curation, Formal analysis, Validation, Writing – original draft. VS: Data curation, Formal analysis, Writing – review & editing. RC: Resources, Writing – review & editing. NA: Data curation, Investigation, Writing – review & editing. AF: Investigation, Resources, Writing – review & editing. IB: Investigation, Resources, Writing – review & editing. CC: Investigation, Writing – review & editing. CS: Investigation, Writing – review & editing. PJT: Investigation, Writing – review & editing. FP: Investigation, Writing – review & editing. RO: Investigation, Writing – review & editing. PF: Investigation, Writing – review & editing. MM: Funding acquisition, Resources, Validation, Writing – review & editing. NS: Resources, Validation, Writing – review & editing. RH: Resources, Validation, Writing – review & editing. CF: Resources, Validation, Writing – review & editing. DF: Investigation, Writing – review & editing. AC: Conceptualization, Funding acquisition, Project administration, Validation, Writing – review & editing.
Funding
The author(s) declares that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We thank to Anette Schulz MD, Beatrice Schmidt MSc and Flávio Morgado PhD for the support.
Conflict of interest
MM, NS, RH and CF were employed by company EUROIMMUN Brazil.
The serodiagnostic tests used in this study were provided by EUROIMMUN Brazil.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Generative AI statement
The author(s) declare that no Gen AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1504260/full#supplementary-material
References
1. Mariampillai K, Granger B, Amelin D, Guiguet M, Hachulla E, Maurier F, et al. Development of a new classification system for idiopathic inflammatory myopathies based on clinical manifestations and myositis-specific autoantibodies. JAMA Neurol. (2018) 75:1528–37. doi: 10.1001/jamaneurol.2018.2598
2. Schmidt J. Current classification and management of inflammatory myopathies. J Neuromuscul Dis. (2018) 5:109–29. doi: 10.3233/JND-180308
3. Selva-O'Callaghan A, Pinal-Fernandez I, Trallero-Araguás E, Milisenda JC, Grau-Junyent JM, Mammen AL. Classification and management of adult inflammatory myopathies. Lancet Neurol. (2018) 17:816–28. doi: 10.1016/S1474-4422(18)30254-0
4. Bohan A, Peter JB. Polymyositis and dermatomyositis (first of two parts). N Engl J Med. (1975) 292:344–7. doi: 10.1056/NEJM197502132920706
5. Bohan A, Peter JB. Polymyositis and dermatomyositis (second of two parts). N Engl J Med. (1975) 292:403–7. doi: 10.1056/NEJM197502202920807
6. Mammen AL. Autoimmune myopathies: autoantibodies, phenotypes and pathogenesis. Nat Rev Neurol. (2011) 7:343–54. doi: 10.1038/nrneurol.2011.63
7. Benveniste O, Stenzel W, Allenbach Y. Advances in serological diagnostics of inflammatory myopathies. Curr Opin Neurol. (2016) 29:662–73. doi: 10.1097/WCO.0000000000000376
8. Labrador-Horrillo M, Martinez MA, Selva-O'Callaghan A, Trallero-Araguas E, Balada E, Vilardell-Tarres M, et al. Anti-MDA5 antibodies in a large Mediterranean population of adults with dermatomyositis. J Immunol Res. (2014) 2014:290797. doi: 10.1155/2014/290797
9. Ladislau L, Suárez-Calvet X, Toquet S, Landon-Cardinal O, Amelin D, Depp M, et al. JAK inhibitor improves type I interferon induced damage: proof of concept in dermatomyositis. Brain. (2018) 141:1609–21. doi: 10.1093/brain/awy105
10. Aussy A, Boyer O, Cordel N. Dermatomyositis and immune-mediated necrotizing myopathies: a window on autoimmunity and cancer. Front Immunol. (2017) 8:992. doi: 10.3389/fimmu.2017.00992
11. Tanboon J, Uruha A, Stenzel W, Nishino I. Where are we moving in the classification of idiopathic inflammatory myopathies? Curr Opin Neurol. (2020) 33:590–603. doi: 10.1097/WCO.0000000000000855
12. Allenbach Y, Benveniste O, Stenzel W, Boyer O. Immune-mediated necrotizing myopathy: clinical features and pathogenesis. Nat Rev Rheumatol. (2020) 16:689–701. doi: 10.1038/s41584-020-00515-9
13. Mammen AL, Allenbach Y, Stenzel W, Benveniste O, ENMC 239th Workshop Study Group. 239th ENMC International Workshop: classification of dermatomyositis, Amsterdam, the Netherlands, 14-16 December 2018. Neuromuscul Disord. (2020) 30:70–92. doi: 10.1016/j.nmd.2019.10.005
14. Herbert MK, Pruijn GJ. Novel serology testing for sporadic inclusion body myositis: disease-specificity and diagnostic utility. Curr Opin Rheumatol. (2015) 27:595–600. doi: 10.1097/BOR.0000000000000216
15. Porcelli B, d'Alessandro M, Gupta L, Grazzini S, Volpi N, Bacarelli MR, et al. Anti-cytosolic 5'-nucleotidase 1A in the diagnosis of patients with suspected idiopathic inflammatory myopathies: an Italian real-life, single-centre retrospective study. Biomedicines. (2023) 11:1963. doi: 10.3390/biomedicines11071963
16. Opinc AH, Makowska JS. Antisynthetase syndrome - much more than just a myopathy. Semin Arthritis Rheum. (2021) 51:72–83. doi: 10.1016/j.semarthrit.2020.09.020
17. Damoiseaux J, Vulsteke JB, Tseng CW, Platteel ACM, Piette Y, Shovman O, et al. Autoantibodies in idiopathic inflammatory myopathies: clinical associations and laboratory evaluation by mono- and multispecific immunoassays. Autoimmun Rev. (2019) 18:293–305. doi: 10.1016/j.autrev.2018.10.004
18. Dubowitz V, Sewry CA, Oldfors A. Muscle Biopsy - A Practical Approach, 5th Edn. Amsterdam: Elsevier (2020).
19. Allenbach Y, Mammen AL, Benveniste O, Stenzel W, Immune-Mediated Necrotizing Myopathies Working Group. 224th ENMC International Workshop: Clinico-sero-pathological classification of immune-mediated necrotizing myopathies Zandvoort, The Netherlands, 14-16 October 2016. Neuromuscul Disord. (2018) 28:87–99. doi: 10.1016/j.nmd.2017.09.016
20. Hilton-Jones D, Brady S. Diagnostic criteria for inclusion body myositis. J Intern Med. (2016) 280:52–62. doi: 10.1111/joim.12480
21. Pestronk A. Acquired immune and inflammatory myopathies: pathologic classification. Curr Opin Rheumatol. (2011) 23:595–604. doi: 10.1097/BOR.0b013e32834bab42
22. Allenbach Y, Benveniste O, Goebel HH, Stenzel W. Integrated classification of inflammatory myopathies. Neuropathol Appl Neurobiol. (2017) 43:62–81. doi: 10.1111/nan.12380
23. Satoh M, Tanaka S, Ceribelli A, Calise SJ, Chan EK. A comprehensive overview on myositis-specific antibodies: new and old biomarkers in idiopathic inflammatory myopathy. Clin Rev Allergy Immunol. (2017) 52:1–19. doi: 10.1007/s12016-015-8510-y
24. Betteridge Z, McHugh N. Myositis-specific autoantibodies: an important tool to support diagnosis of myositis. J Intern Med. (2016) 280:8–23. doi: 10.1111/joim.12451
25. Gunawardena H, Betteridge ZE, McHugh NJ. Myositis-specific autoantibodies: their clinical and pathogenic significance in disease expression. Rheumatology. (2009) 48:607–12. doi: 10.1093/rheumatology/kep078
26. Oyama M, Holzer MT, Ohnuki Y, Saito Y, Nishimori Y, Suzuki S, et al. Pathologic features of anti-ku myositis. Neurology. (2024) 102:e209268. doi: 10.1212/WNL.0000000000209268
27. Tanboon J, Inoue M, Saito Y, Tachimori H, Hayashi S, Noguchi S, et al. Dermatomyositis: muscle pathology according to antibody subtypes. Neurology. (2022) 98:e739–49. doi: 10.1212/WNL.0000000000013176
28. Anquetil C, Boyer O, Wesner N, Benveniste O, Allenbach Y. Myositis-specific autoantibodies, a cornerstone in immune-mediated necrotizing myopathy. Autoimmun Rev. (2019) 18:223–30. doi: 10.1016/j.autrev.2018.09.008
29. Hočevar A, Viršček A, Krošel M, Gradišnik S, Rotar Ž, Tomšič M, et al. Survival of patients with idiopathic inflammatory myopathies in Slovenia. Front Med. (2021) 8:801078. doi: 10.3389/fmed.2021.801078
30. Jiang W, Shi J, Yang H, Tian X, Yang H, Chen Q, et al. Long-term outcomes and prognosis factors in patients with idiopathic inflammatory myopathies based on myositis-specific autoantibodies: a single cohort study. Arthritis Care Res. (2023) 75:1175–82. doi: 10.1002/acr.24993
31. Yang H, Peng Q, Yin L, Li S, Shi J, Zhang Y, et al. Identification of multiple cancer-associated myositis-specific autoantibodies in idiopathic inflammatory myopathies: a large longitudinal cohort study. Arthritis Res Ther. (2017) 19:259. doi: 10.1186/s13075-017-1469-8.
32. Allenbach Y, Keraen J, Bouvier AM, Jooste V, Champtiaux N, Hervier B, et al. High risk of cancer in autoimmune necrotizing myopathies: usefulness of myositis specific antibody. Brain. (2016) 139(Pt 8):2131–5. doi: 10.1093/brain/aww054
33. Kadoya M, Hida A, Hashimoto Maeda M, Taira K, Ikenaga C, Uchio N, et al. Cancer association as a risk factor for anti-HMGCR antibody-positive myopathy. Neurol Neuroimmunol Neuroinflamm. (2016) 3:e290. doi: 10.1212/NXI.0000000000000290
34. Aussy A, Fréret M, Gallay L, Bessis D, Vincent T, Jullien D, et al. The IgG2 isotype of anti-transcription intermediary factor 1γ autoantibodies is a biomarker of cancer and mortality in adult dermatomyositis. Arthritis Rheumatol. (2019) 71:1360–70. doi: 10.1002/art.40895
35. Fiorentino DF, Chung LS, Christopher-Stine L, Zaba L, Li S, Mammen AL, et al. Most patients with cancer-associated dermatomyositis have antibodies to nuclear matrix protein NXP-2 or transcription intermediary factor 1γ. Arthritis Rheum. (2013) 65:2954–62. doi: 10.1002/art.38093
36. Oldroyd A, Sergeant JC, New P, McHugh NJ, Betteridge Z, Lamb JA, et al. The temporal relationship between cancer and adult onset anti-transcriptional intermediary factor 1 antibody-positive dermatomyositis. Rheumatology. (2019) 58:650–5. doi: 10.1093/rheumatology/kez329
37. Trallero-Araguás E, Rodrigo-Pendás JÁ, Selva-O'Callaghan A, Martínez-Gómez X, Bosch X, Labrador-Horrillo M, et al. Usefulness of anti-p155 autoantibody for diagnosing cancer-associated dermatomyositis: a systematic review and meta-analysis. Arthritis Rheum. (2012) 64:523–32. doi: 10.1002/art.33379
38. Albayda J, Pinal-Fernandez I, Huang W, Parks C, Paik J, Casciola-Rosen L, et al. Antinuclear matrix protein 2 autoantibodies and edema, muscle disease, and malignancy risk in dermatomyositis patients. Arthritis Care Res. (2017) 69:1771–6. doi: 10.1002/acr.23188
39. Muro Y, Sugiura K, Nara M, Sakamoto I, Suzuki N, Akiyama M. High incidence of cancer in anti-small ubiquitin-like modifier activating enzyme antibody-positive dermatomyositis. Rheumatology. (2015) 54:1745–7. doi: 10.1093/rheumatology/kev247
40. Albayda J, Mecoli C, Casciola-Rosen L, Danoff SK, Lin CT, Hines D, et al. A North American cohort of anti-SAE dermatomyositis: clinical phenotype, testing, and review of cases. ACR Open Rheumatol. (2021) 3:287–94. doi: 10.1002/acr2.11247
41. Ge Y, Lu X, Shu X, Peng Q, Wang G. Clinical characteristics of anti-SAE antibodies in Chinese patients with dermatomyositis in comparison with different patient cohorts. Sci Rep. (2017) 7:188. doi: 10.1038/s41598-017-00240-6
42. Shelly S, Beecher G, Milone M, Liewluck T, Ernste F, Triplett J, et al. Cancer and immune-mediated necrotizing myopathy: a longitudinal referral case-controlled outcomes evaluation. Rheumatology. (2022) 62:281–9. doi: 10.1093/rheumatology/keac144
43. Mammen AL. Paraneoplastic myopathies. Handb Clin Neurol. (2024) 200:327–32. doi: 10.1016/B978-0-12-823912-4.00022-0
44. Khoo T, Chinoy H. Anti-HMGCR immune-mediated necrotising myopathy: addressing the remaining issues. Autoimmun Rev. (2023) 22:103468. doi: 10.1016/j.autrev.2023.103468
45. Mariscal A, Milán M, Baucells A, Martínez MA, Guillen AG, Trallero-Araguás E, et al. Anti-TIF-1γ antibody detection using a commercial kit vs in-house immunoblot: usefulness in clinical practice. Front Immunol. (2021) 11:625896. doi: 10.3389/fimmu.2020.625896
46. Inoue M, Tanboon J, Okubo M, Theerawat K, Saito Y, Ogasawara M, et al. Absence of sarcoplasmic myxovirus resistance protein A (MxA) expression in antisynthetase syndrome in a cohort of 194 cases. Neuropathol Appl Neurobiol. (2019) 45:523–4. doi: 10.1111/nan.12551
47. Valiyil R, Casciola-Rosen L, Hong G, Mammen A, Christopher-Stine L. Rituximab therapy for myopathy associated with anti-signal recognition particle antibodies: a case series. Arthritis Care Res. (2010) 62:1328–34. doi: 10.1002/acr.20219
48. Pinal-Fernandez I, Parks C, Werner JL, Albayda J, Paik J, Danoff SK, et al. Longitudinal course of disease in a large cohort of myositis patients with autoantibodies recognizing the signal recognition particle. Arthritis Care Res. (2017) 69:263–70. doi: 10.1002/acr.22920
49. Bolko L, Jiang W, Tawara N, Landon-Cardinal O, Anquetil C, Benveniste O, et al. The role of interferons type I, II and III in myositis: a review. Brain Pathol. (2021) 31:e12955. doi: 10.1111/bpa.12955
50. Rigolet M, Hou C, Baba Amer Y, Aouizerate J, Periou B, Gherardi RK, et al. Distinct interferon signatures stratify inflammatory and dysimmune myopathies. RMD Open. (2019) 5:e000811. doi: 10.1136/rmdopen-2018-000811
51. Pinal-Fernandez I, Casal-Dominguez M, Derfoul A, Pak K, Plotz P, Miller FW, et al. Identification of distinctive interferon gene signatures in different types of myositis. Neurology. (2019) 93:e1193–204. doi: 10.1212/WNL.0000000000008128
52. Hamaguchi Y, Fujimoto M, Matsushita T, Kaji K, Komura K, Hasegawa M, et al. Common and distinct clinical features in adult patients with anti-aminoacyl-tRNA synthetase antibodies: heterogeneity within the syndrome. PLoS ONE. (2013) 8:e60442. doi: 10.1371/journal.pone.0060442
53. Bundell C, Rojana-Udomsart A, Mastaglia F, Hollingsworth P, McLean-Tooke A. Diagnostic performance of a commercial immunoblot assay for myositis antibody testing. Pathology. (2016) 48:363–6. doi: 10.1016/j.pathol.2016.03.012
54. Lecouffe-Desprets M, Hémont C, Néel A, Toquet C, Masseau A, Hamidou M, et al. Clinical contribution of myositis-related antibodies detected by immunoblot to idiopathic inflammatory myositis: a one-year retrospective study. Autoimmunity. (2018) 51:89–95. doi: 10.1080/08916934.2018.1441830
55. To F, Ventín-Rodríguez C, Elkhalifa S, Lilleker JB, Chinoy H. Line blot immunoassays in idiopathic inflammatory myopathies: retrospective review of diagnostic accuracy and factors predicting true positive results. BMC Rheumatol. (2020) 4:28. doi: 10.1186/s41927-020-00132-9
56. Mahler M, Betteridge Z, Bentow C, Richards M, Seaman A, Chinoy H, et al. Comparison of three immunoassays for the detection of myositis specific antibodies. Front Immunol. (2019) 10:848. doi: 10.3389/fimmu.2019.00848
57. Angeli F, Pedretti E, Garrafa E, Fredi M, Ceribelli A, Franceschini F, et al. Comparison of lineblot and immunoprecipitation methods in the detection of myositis-specific and myositis-associated antibodies in patients with idiopathic inflammatory myopathies: consistency with clinical diagnoses. Diagnostics. (2024) 14:2192. doi: 10.3390/diagnostics14192192
Keywords: idiopathic inflammatory myopathies, myositis-specific antibodies, muscle biopsy, dermatomyositis, immune-mediated necrotizing myopathy, anti-synthetase syndrome, inclusion body myositis, myositis-associated antibodies
Citation: Fontana PN, da Silva VG, Corazzini R, Athayde NM, Ferreira da Silva AMD, Brockhausen I, Correia CdC, Sobreira CFdR, Tomaselli PJ, Petean F, de Oliveira R, Feitoza PV, Moraes Soane M, Saraiva N, Hidalgo R, Fideles C, Feder D and Carvalho AAdS (2025) Applicability of a serodiagnostic line blot for idiopathic inflammatory myopathy: the muscle biopsy is not all. Front. Neurol. 15:1504260. doi: 10.3389/fneur.2024.1504260
Received: 30 September 2024; Accepted: 11 December 2024;
Published: 06 January 2025.
Edited by:
Pritikanta Paul, University of California, San Francisco, United StatesReviewed by:
Georgios E. Manousakis, University of Minnesota, United StatesShiri Keret, Technion Israel Institute of Technology, Israel
Copyright © 2025 Fontana, da Silva, Corazzini, Athayde, Ferreira da Silva, Brockhausen, Correia, Sobreira, Tomaselli, Petean, de Oliveira, Feitoza, Moraes Soane, Saraiva, Hidalgo, Fideles, Feder and Carvalho. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pedro Nogueira Fontana, cGVkcm9ub2d1ZWlyYWZvbnRhbmFAZ21haWwuY29t; Alzira Alves de Siqueira Carvalho, YWx6aXJhc2lxdWVpcmFjYXJ2YWxob0BnbWFpbC5jb20=