
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 17 December 2024
Sec. Neuro-Otology
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1501561
This article is part of the Research Topic Bridging the Gap Between the Different Pillars of Tinnitus Research View all 6 articles
 Zhifeng Chen1,2,3†
Zhifeng Chen1,2,3† Yan Lu1,2†
Yan Lu1,2† Chenyu Chen4,5†Shaolian Lin1,2†Ting Xie6Xiaoyang Luo1,2
Chenyu Chen4,5†Shaolian Lin1,2†Ting Xie6Xiaoyang Luo1,2 Yanchun Lin1,2
Yanchun Lin1,2 Yuqing Chen1,2Yong Feng7Guanxia Xiong8Xiulan Ma9
Yuqing Chen1,2Yong Feng7Guanxia Xiong8Xiulan Ma9 Chaojun Zeng1,10,11*
Chaojun Zeng1,10,11* Chang Lin1,2,3*
Chang Lin1,2,3*Objective: The relationship between tinnitus in the elderly with hearing loss remains elusive. This study aimed to reveal the association between tinnitus and hearing impairment among older adults with age-related hearing loss (ARHL).
Methods: This cross-sectional study was conducted among a population of outpatients diagnosed with ARHL at four medical centers in different regions of China, from June 2020 to June 2023. ARHL patients were divided into two groups based on their self-reported tinnitus: tinnitus and non-tinnitus. Multivariable linear regression models were used to assess the association between tinnitus and hearing impairment in ARHL patients. Subgroup analyses, stratified by gender and age, were performed to further evaluate the association.
Results: A total of 418 older adults with ARHL were included in the study. Compared to the non-tinnitus group, ARHL patients with tinnitus had lower hearing thresholds (β = −5.07; 95% confidence interval (CI) −9.32 to −0.81; p = 0.020). On subgroup analyses stratified by gender and age, the male ARHL patients with tinnitus still had lower hearing thresholds compared to those without tinnitus (β = −6.96; 95% CI −12.70 to 1.22; p = 0.018). In females, tinnitus was not associated with hearing thresholds (β = −3.69; 95% CI −10.11 to 2.74, p = 0.262). There was no association between tinnitus and hearing thresholds in both the age group of ≥70 years (β = −4.31; 95% CI −9.65 to 1.03; p = 0.116) and the age group of <70 years (β = −3.54; 95% CI −9.96 to 2.89; p = 0.282).
Conclusion: Based on this multi-center cross-sectional study, we reveal that there is no evidence for the assumption that tinnitus may exacerbate hearing loss in the elderly for the first time. On the contrary, tinnitus is associated with better hearing in the male elderly with ARHL. More extensive longitudinal studies are needed to give a comprehensive insight of the present findings and the underlying mechanisms.
Age-related hearing loss (ARHL), commonly referred to as presbycusis, is a prevalent form of sensorineural hearing impairment predominantly observed in the elderly population (1). The Global Burden of Disease Study (GBD) estimates that in 2019, over 1.57 billion people were affected by hearing loss, with approximately 62.1% being over the age of 50. By 2050, the number of individuals with hearing loss is expected to exceed 2.45 billion (2). Additionally, hearing loss is the third leading cause of years lived with disability (YLDs) worldwide, accounting for 43.5 million YLDs (2). Hearing impairment leads to communication barriers, social isolation, depression, cognitive dysfunction, and other adverse effects (3–6), seriously affecting the physical and mental health and quality of life of older adults. However, there is no standardized and effective prevention and treatment of ARHL that can significantly restore or reverse the patient’s own hearing function currently (7). Thus, precise observation of the characteristics of the disease may contribute to a precise diagnosis and prompt treatment.
Tinnitus is characterized by the perception of sound without any external acoustic signal (8). It is often accompanied by hearing loss in the elderly, with an estimated overlap of around 80% (9). Its incidence and symptoms increase with increasing age and also with hearing loss, making it a particular disorder of older people (10). As a study reported that tinnitus affects approximately 14% of the world’s population (11), an estimated 740 million individuals, imposing a high economic burden on society. Tinnitus is often but not always related to hearing loss. It can occur independently or in conjunction with different hearing loss conditions (12). Although tinnitus patients account for the majority of ARHL patients, its intimate relationship with hearing impairment in the elderly remains poorly revealed.
The etiology and pathophysiological mechanism of tinnitus have not been fully elucidated. Studies have linked tinnitus to increased spontaneous firing and neuronal hyperactivity along the auditory pathway, which may be due to homeostatic plasticity, a compensatory mechanism that raises central neuronal gain to stabilize firing rates in the face of reduced auditory input (13, 14). Interestingly, Krauss et al. (15) proposed an alternative view, suggesting that stochastic resonance may be a primary driver of this hyperactivity, contributing to the onset and persistence of tinnitus. And their analysis of nearly 40,000 patients further showed that individuals with tinnitus generally had lower hearing thresholds in the low-frequency range compared to those without tinnitus (15). The emerging evidence suggests that the occurrence and progression of tinnitus are not only related to damage to the auditory pathway system, but also to structures of the limbic system, particularly the hippocampus, parahippocampal gyrus, and amygdala (16–22). The limbic system is known as the ‘sensory and reactive brain’ and can respond to emotional stimuli (23). Jastreboff suggested that the limbic system significantly contributes to the psychological responses associated with tinnitus, as it plays an important role in behavior and emotional expression (24). Overall, the association with tinnitus and hearing impairment still remains unclear.
Gender and age differences associated with tinnitus and hearing loss in the literature data are controversial. Previous research has produced mixed results regarding the influence of gender on tinnitus-related distress. Some studies reported that gender does not have a significant impact on the level of discomfort experienced by individuals with tinnitus, with both men and women experiencing similar levels of discomfort (25, 26). In contrast, other studies found gender differences. Some suggested that men report higher levels of annoyance from tinnitus, while others found that women experience greater discomfort (27, 28). Additionally, several studies showed that the prevalence of hearing loss and tinnitus increased with age (29, 30). Evidence indicated that the incidence and prevalence of tinnitus increases significantly in older adults compared to the general population. While tinnitus affected approximately 10–19% of the general adult population, the prevalence increases to 24–45% in older people (31). However, a cross-sectional study of 6,098 participants showed a comparable prevalence of hearing impairment in both the tinnitus and non-tinnitus groups in people over 54 years of age (32). These conflicting results highlight the need for further research to determine whether gender or age plays a consistent role in the perception and impact of tinnitus and to uncover possible factors that may contribute to gender or age-related differences in the association between tinnitus and hearing loss.
Therefore, this study aimed to assess the association between tinnitus and hearing impairment, especially among older adults with ARHL, and further explore the impact of different gender and age.
This cross-sectional study was conducted among a population of outpatients diagnosed with ARHL at four clinical medical centers in different regions of China, from June 2020 to June 2023. The elderly with hearing loss as the chief complaint were included in this study. ARHL was diagnosed through pure tone audiometry and recognized diagnostic criteria (33). Each patient underwent an otoscopic examination along with a basic audiological evaluation. The inclusion criteria of patients were as follows: (1) age ≥ 60 years old; (2) bilateral sensorineural hearing loss with increasing thresholds for higher frequencies; (3) pure tone average (PTA) ≥ 20 dB HL in better ear. Otitis media, abnormal otoscopy, impacted cerumen, drug-deafness, noise-deafness, large asymmetric hearing loss, sudden hearing loss, abnormal tympanometry (peak pressure ≤ −150 da Pa; compliance ≤0.3 mL) at either ear, and severe cognitive impairment were excluded.
Tinnitus was defined as a constant tinnitus in the past year before the examination. We collected various demographic and clinical data from the patients, which included age (year), Body Mass Index (BMI) (kg/m2), gender (female/male), education level (less than primary school/primary school/junior high school/high school/more than high school), history of smoking (yes/no) and alcohol (yes/no), hearing threshold (dB HL), presence of constant of tinnitus in the past year (yes/no), dizziness (yes/no), and history of any surgery (yes/no). The presence of comorbidities such as hypertension (yes/no), diabetes mellitus (yes/no), and hyperlipidemia (yes/no) were also recorded.
This study was approved by the Ethics Committee of the First Affiliated Hospital of Fujian Medical University (No: IEC-FOM-013-2.0). Informed consent was obtained from all individual patients participated in the study.
Pure tone audiometry was carried out in a sound-isolated room, adhering to the GB/T 19885–2005 standards. This assessment utilized a clinical audiometer (AC40, Interacoustics). For air conduction audiometry, pure tone and masking signals were delivered via TDH39 supra-aural earphones, while bone conduction audiometry signals were provided by a B-71 bone vibrator. Air conduction testing covered the following frequencies: 0.25 kHz, 0.5 kHz, 1.0 kHz, 2.0 kHz, 4.0 kHz, and 8.0 kHz. Bone conduction testing was conducted at frequencies of 0.25 kHz, 0.5 kHz, 1.0 kHz, 2.0 kHz, and 4.0 kHz. According to the World Health Organization’s World Report on Hearing (12), hearing loss was defined as a threshold exceeding 20 dB HL. This definition was based on the better-ear PTA at frequencies of 0.5 kHz, 1 kHz, 2 kHz, and 4 kHz.
All statistical analyses were performed with SPSS (version 26.0) and R (version 4.3.0). p < 0.05 was considered statistically significant. Continuous data were expressed as mean (standard deviation, SD). Enumeration data were expressed as numbers (percentages). Student’s t-test and Satterthwaite t-test were used to analyze continuous data, and Chi-square test was used to analyze enumeration data.
Multivariate linear regression models were employed to examine the relationship between tinnitus and hearing thresholds. The association was evaluated using β coefficients and 95% confidence intervals (CI):
Model 1 served as the unadjusted baseline model. Model 2 was adjusted for age, BMI, gender, and education level. Model 3 included further adjustments for age, BMI, gender, education, surgery history, dizziness, hypertension, diabetes, and hyperlipidemia. Additionally, the associations were further analyzed in different subgroups based on gender and age. The analysis included an evaluation of the goodness of fit of the models based on the explained variance.
Figure 1 shows the screening process for eligible patients with ARHL. A total of 418 patients with ARHL were screened. The age of all ARHL patients was 69.9 ± 7.3 years. Table 1 demonstrates the characteristics of the ARHL patients with or without tinnitus. The prevalence of tinnitus in ARHL patients is 57.1% (239 / 418). The age of ARHL patients with tinnitus was 68.9 ± 6.3 years and those without tinnitus was 71.2 ± 8.4 years. There were also significant statistical differences between two groups according to age (p = 0.003), BMI (p = 0.049), PTA (p = 0.027), education (p = 0.049), surgery (p = 0.014), dizziness (p < 0.001), hypertension (p = 0.020), and diabetes (p = 0.018).
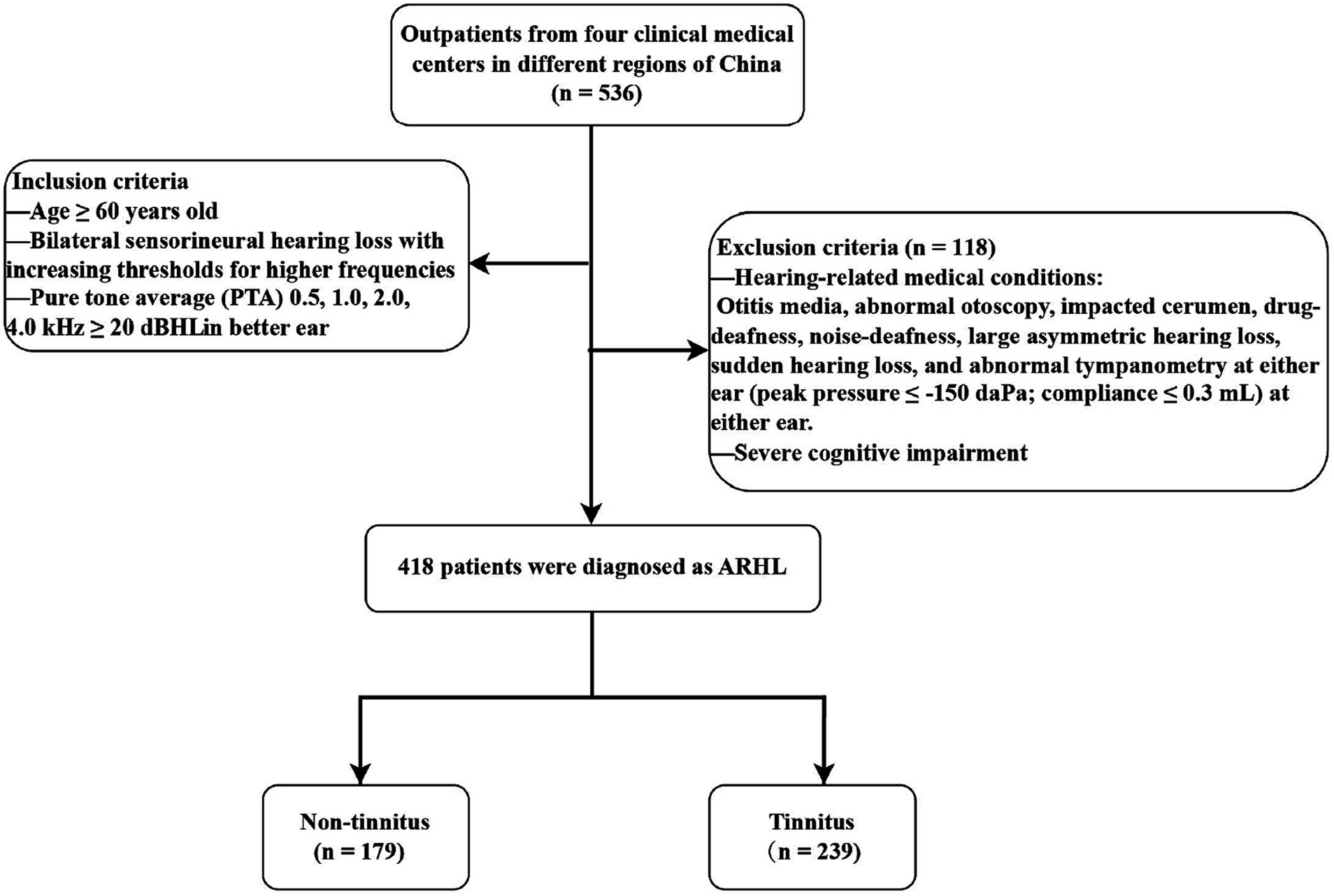
Figure 1. Flow chart of study population.

Table 1. Descriptive statistics in two different groupsa.
The relationships between tinnitus and hearing thresholds in ARHL patients are shown in Table 2. Compared with non-tinnitus group, tinnitus was associated with lower β of hearing thresholds in ARHL patients (β = −5.07; 95% CI −9.32 to −0.81; p = 0.020), after adjustments for age, BMI, gender, education, surgery, dizziness, hypertension, diabetes, and hyperlipidemia.
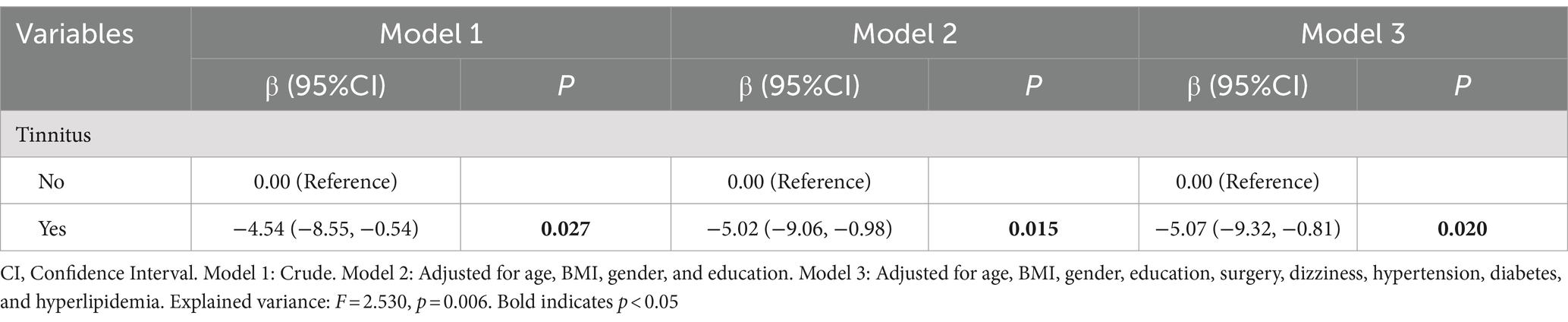
Table 2. Multivariate linear regression analysis: association of tinnitus with hearing thresholds.
Further analyses were carried out to investigate the association between tinnitus and hearing thresholds in different gender. As shown in Table 3, after stratification by gender, it is found that there were significant statistical differences in age (p = 0.08), PTA (p = 0.040), education (p = 0.010), dizziness (p < 0.001), hypertension (p = 0.005), and hyperlipidemia (p = 0.031) in males, but not in females (all p > 0.05). As multivariate linear regression analyses showed, tinnitus was still associated with lower hearing thresholds in male ARHL patients when compared with non-tinnitus group (β = −6.96; 95% CI -12.70 to −1.22; p = 0.018) (Table 4). However, among females, tinnitus was not related to hearing thresholds (β = −3.69; 95% CI −10.11 to 2.74; p = 0.262).

Table 3. Characteristics of ARHL patients stratified by gender.
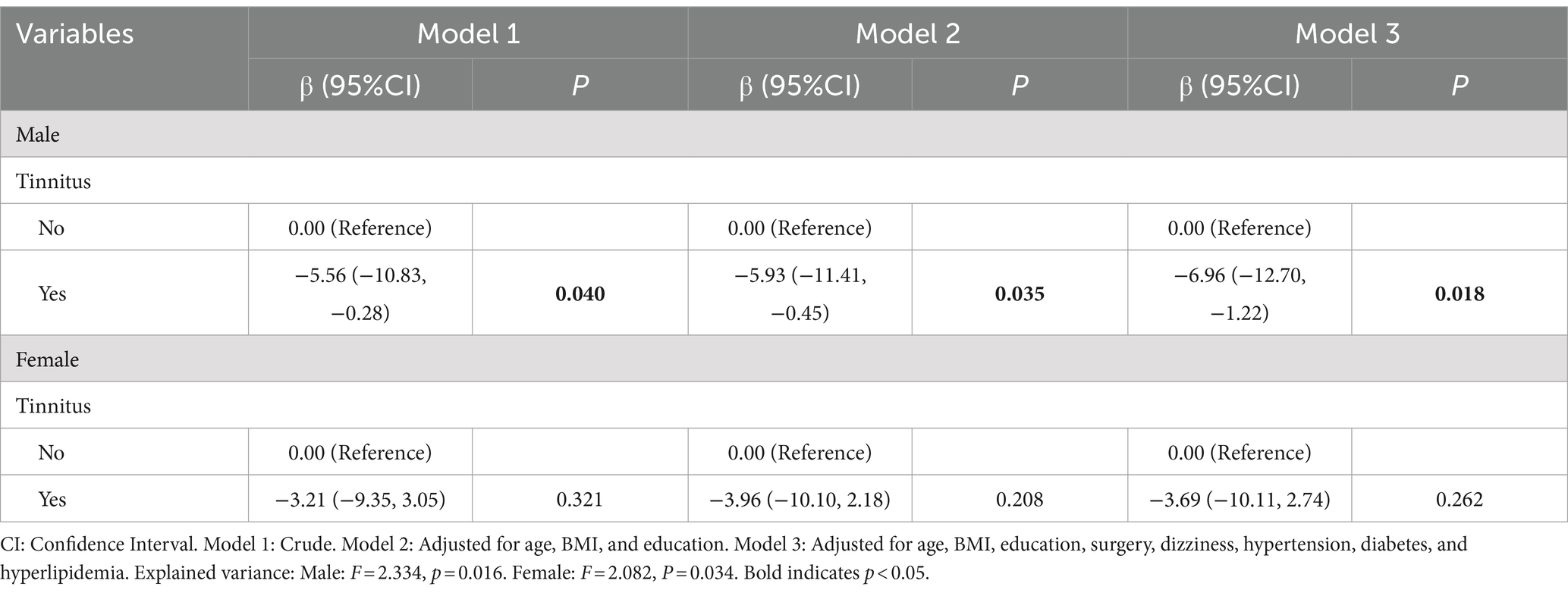
Table 4. Subgroup analyses stratified by gender.
After stratification by age group, statistical differences in age (p = 0.004), PTA (p = 0.020), surgery (p = 0.021), and dizziness (p = 0.001) were found in the ≥70 years age group, but not in the <70 years age group (all p > 0.05) (Table 5). In addition, statistical differences in hypertension (p = 0.034) and diabetes (p = 0.041) were found in the age group ≥70 years, but not in the age group <70 years (all p > 0.05) (Table 5). However, further multivariate linear regression analyses showed that, upon adjustment of confounding variables, no significant association was found between tinnitus and hearing thresholds in the two different age groups (all p > 0.05) (Table 6).
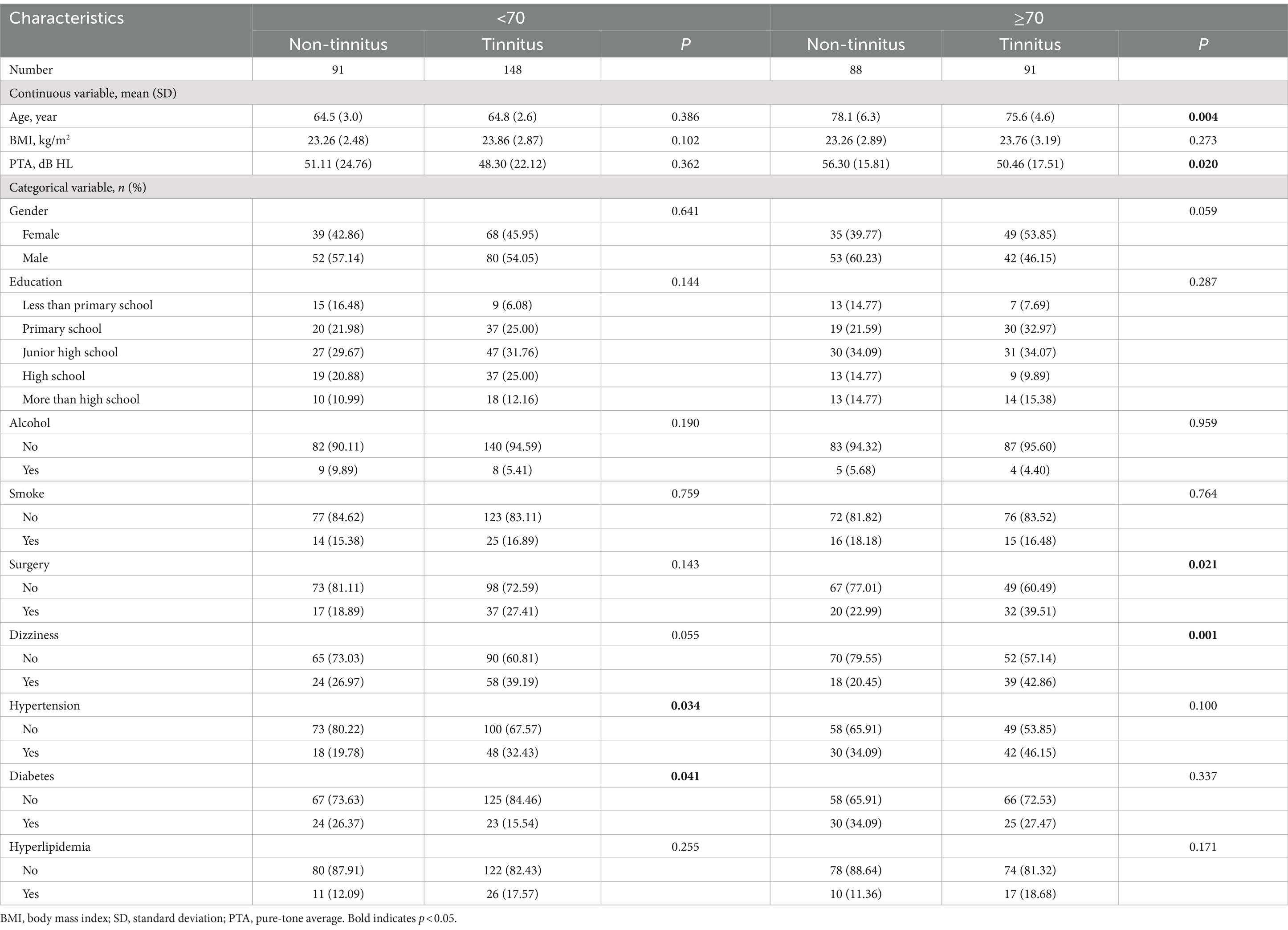
Table 5. Characteristics of ARHL patients stratified by age.
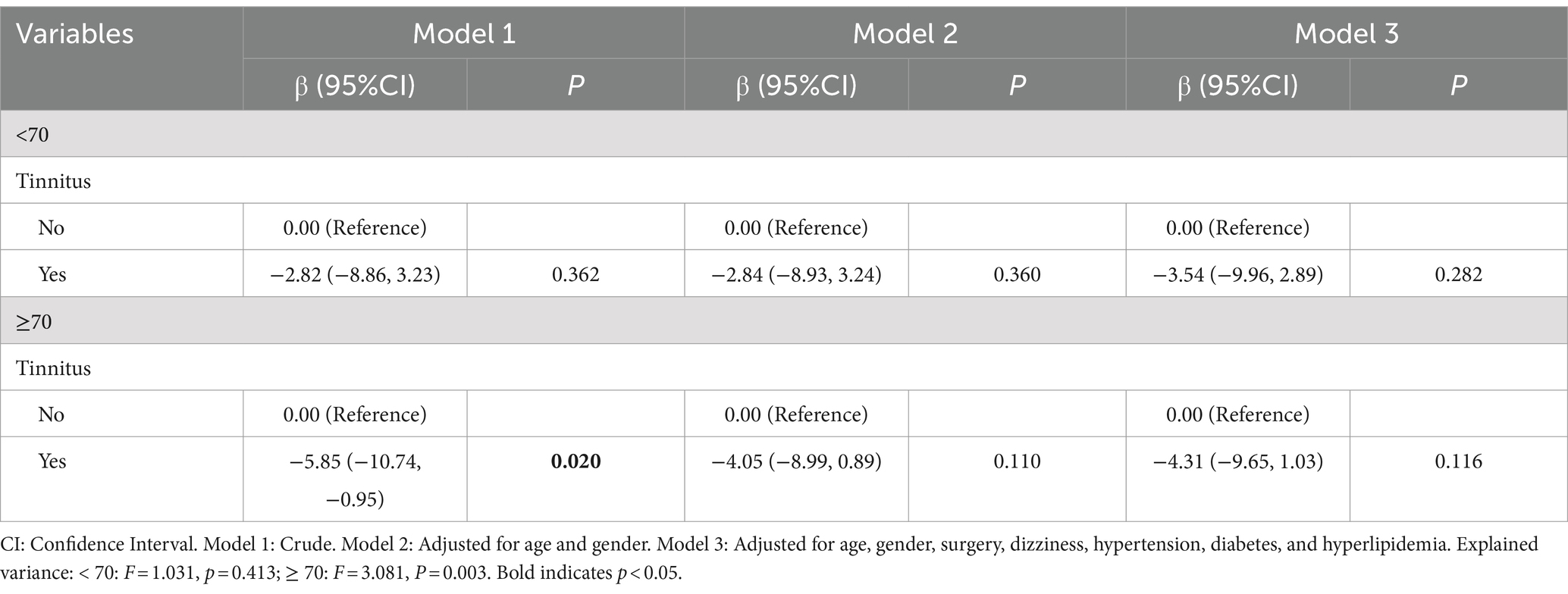
Table 6. Subgroup analyses stratified by age.
This study aimed to investigate the association between tinnitus and hearing impairment among older adults with ARHL. Interestingly, our findings showed that tinnitus was associated with lower hearing thresholds. Similar results were also demonstrated in male group. To the best of our knowledge, this is the first study to explore in some detail the association between tinnitus and hearing impairment in Chinese older adults with ARHL.
ARHL is the most common cause of hearing loss in older adults worldwide (34). According to the estimates of the World Health Organization (WHO) in 2012, approximately 164.5 million people over the age of 65 experience hearing impairment globally (35). With the current increase in age and life expectancy of the global population, it is projected that by 2025, more than 500 million people over the age of 60 will have ARHL (36). A wide range of evidence suggests that hearing loss is the most relevant etiologic factor in the development of tinnitus (37–39). According to previous literature, the prevalence of tinnitus among the elderly in China was 28.7 to 51.3% (40). In our study, the prevalence of tinnitus in ARHL patients is 57.1%, which was significantly higher than the prevalence in the general elderly population in China. Increasing age and hearing impairment have been identified as the most relevant risk factors for tinnitus (41), which leads to a higher prevalence of tinnitus in ARHL patients.
The association between tinnitus and hearing loss is not straightforward. Not everyone with hearing loss develops tinnitus, and not all people with tinnitus have abnormal hearing (37). Previous studies have found that the higher the prevalence of tinnitus, the higher the prevalence of hearing loss (42–44). However, in the cohort study of elderly patients, Bureš Z et al. (45) found no significant difference in hearing thresholds in ARHL patients with tinnitus than those without tinnitus. In our study, we identified a significant association between tinnitus and hearing impairment, for which tinnitus was associated with lower hearing thresholds. Most of the previous studies on the association between tinnitus and hearing loss have been based on patients’ self-reported hearing (46, 47). However, relying on self-reporting hearing may be inadequate for accurately detecting hearing loss (48). Our study used pure-tone audiometry to determine the hearing threshold, making the result more objective.
The etiology and pathophysiological mechanisms underlying tinnitus are still incompletely understood despite significant research progress. New evidence suggests that the onset and progression of tinnitus is not only related to damage to the auditory pathway, but is also associated with structural and functional changes in the limbic system (16–22). The limbic system is known to be involved in memory, especially on the parts associated with emotions (49). One recent study found an interesting and surprising result that among older adults without a Hispanic background, tinnitus combined with hearing loss resulted in better cognitive performance than hearing loss alone (50), suggesting that the presence of tinnitus may compensate for some of the known risk factors for cognitive impairment (51). In the context of this review, this may lead to the question of whether the hippocampus of the limbic system plays a role in tinnitus, where persistent auditory memory of tinnitus signals protects the hippocampus from functioning and prevents the previously demonstrated reduction in hippocampal neurogenesis in the presence of hearing loss (52). In our study, we found that tinnitus is associated with lower hearing thresholds in ARHL patients, which is consistent with the work of König et al. reporting better hearing thresholds in tinnitus patients compared to non-tinnitus patients (53). One possible reason is that tinnitus causes a constant updating of information between the hippocampus and the auditory cortex, which is effective in reducing the reduction of correspondence due to hearing loss. Another explanation could be stochastic resonance. This mechanism is able to at least partially restore hearing thresholds raised by noise trauma (15).
Previous studies have noted gender differences in the relation to tinnitus and hearing loss (54, 55). The 2009–2011 KNHANES revealed that the prevalence of tinnitus in participants over 12 years old was 17.7% for men and 21.7% for women, with the difference being statistically significant (56). It also has been shown that tinnitus in women is associated with greater psychological stress than in men (57). A previous cross-sectional study showed a statistically significant increase in the risk of attempted suicide in women with severe tinnitus, but not in men (58). These results are in contrast to other studies that have found a higher prevalence of tinnitus and hearing loss in men (59–61). However, some studies have found no relationship between gender and tinnitus after accounting for other factors (62, 63). In our study, we identified a gender-specific difference in the association between tinnitus and hearing thresholds. Male patients with tinnitus seemed to have better hearing than those without tinnitus. However, this association was not found in female ARHL patients. This gender discrepancy might be linked to differences in estrogen levels, cochlear structure, brain biochemistry, and the progression of age-related hearing loss between men and women (64). We also found that younger age, dizziness, hypertension, and hyperlipidemia may be risk factors for tinnitus in male patients with ARHL. These results are consistent with findings from previous studies (65–67).
Age differences related to tinnitus and hearing loss have been observed in many studies previously (56, 68, 69). In South Korea, about 27% of people aged 60 to 69 and 45% of people aged 70 and over suffer from subjective hearing loss (70). In a study of 14,178 participants in the US, Josef et al. (61) found the prevalence of tinnitus increased with age, reaching its highest rate of 14.3% in individuals aged 60 to 69 years. However, in a cross-sectional study of 6,098 eligible participants who underwent tinnitus and hearing assessment living in the Netherlands, Berthe et al. (32) found a similar prevalence of hearing impairment in both the tinnitus and non-tinnitus groups among individuals over the age of 54 years. This suggests that tinnitus may be independent of hearing loss and not related to the ageing process. While hearing loss is generally a significant risk factor for tinnitus, ARHL is unlikely to cause tinnitus (32). As ARHL is a slowly progressive disease of the auditory system, the brain has time to adapt to less and less input (71). Besides, several studies have found that the prevalence of tinnitus increases with age, but decreases after a certain age (72–74). It is assumed that with increasing age, the impact of tinnitus for the patient’s general health burden decreases, while the ability to treat the symptoms increases (75). In the present analysis, we did not identify an age-specific significant association between tinnitus and hearing thresholds in ARHL patients. Differences between studies are likely due to variations in factors such as demographic characteristics, sample size, or the confounding variables that were controlled in each study.
There remain limitations in our study. Firstly, the cross-sectional study design used in this research can only establish the correlations rather than causation. To validate the findings, it is crucial to conduct comprehensive prospective studies. Secondly, while efforts were made to adjust for hearing-related confounders, future studies should consider including additional unmeasured variables, such as marital status, income status, hearing aid use, etc. In addition, the nature and degree of tinnitus should be taken into account. Moreover, the exact mechanism linking hearing loss and tinnitus has not been fully explored. Lastly, since the data for this study were collected from different regions of China, caution should be exercised when generalizing the results to other countries or populations.
The present study found that tinnitus might not exacerbate hearing loss in ARHL patients. Particularly, male patients with tinnitus have better hearing than those without tinnitus. The results of this study seem a challenge to part of the existing hypothesis that tinnitus may exacerbate hearing loss and will provide an interesting insight for future research.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethics Committee of the First Affiliated Hospital of Fujian Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ZC: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft, Writing – review & editing. YL: Data curation, Formal analysis, Writing – original draft. CC: Methodology, Software, Writing – original draft. SL: Data curation, Investigation, Writing – original draft. TX: Data curation, Validation, Writing – original draft. XL: Data curation, Writing – original draft. YCL: Investigation, Visualization, Writing – original draft. YC: Writing – original draft. YF: Data curation, Writing – review & editing. GX: Data curation, Writing – review & editing. XM: Data curation, Writing – review & editing. CZ: Resources, Supervision, Writing – original draft, Writing – review & editing. CL: Funding acquisition, Methodology, Project administration, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This research was supported by the Science and Technology Innovation Joint Funding Project of Fujian Province (Grant No. 2021Y9099), National Key Research and Development Project of China (Grant No. 2020YFC2005204), Fujian Provincial Clinical Medical Research Center for Ear, Nose, and Throat Difficulty Diseases (Grant No. EB-YJZX) under the Foundation Project to Fujian Provincial Science and Technology Innovation Platform (Grant NO. 2021Y2002), and Natural Science Foundation of Fujian Province (Grant No. 2022J01679).
The authors are grateful to all individual participants in the study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ninoyu, Y, and Friedman, RA. The genetic landscape of age-related hearing loss. Trends Genet. (2024) 40:228–37. doi: 10.1016/j.tig.2023.12.001
2. CGH, L. Hearing loss prevalence and years lived with disability, 1990-2019: findings from the global burden of disease Study 2019. Lancet. (2021) 397:996–1009. doi: 10.1016/s0140-6736(21)00516-x
3. Tu, NC, and Friedman, RA. Age-related hearing loss: unraveling the pieces. Laryngoscope Investig Otolaryngol. (2018) 3:68–72. doi: 10.1002/lio2.134
4. Loughrey, DG, Kelly, ME, Kelley, GA, Brennan, S, and Lawlor, BA. Association of age-Related Hearing Loss with Cognitive Function, cognitive impairment, and dementia: a systematic review and Meta-analysis. JAMA Otolaryngol Head Neck Surg. (2018) 144:115–26. doi: 10.1001/jamaoto.2017.2513
5. Livingston, G, Huntley, J, Sommerlad, A, Ames, D, Ballard, C, Banerjee, S, et al. Dementia prevention, intervention, and care: 2020 report of the lancet commission. Lancet. (2020) 396:413–46. doi: 10.1016/s0140-6736(20)30367-6
6. Lin, FR, Pike, JR, Albert, MS, Arnold, M, Burgard, S, Chisolm, T, et al. Hearing intervention versus health education control to reduce cognitive decline in older adults with hearing loss in the USA (ACHIEVE): a multicentre, randomised controlled trial. Lancet. (2023) 402:786–97. doi: 10.1016/s0140-6736(23)01406-x
7. Tanael, M. A novel therapy for Presbycusis. Rejuvenation Res. (2021) 24:3–5. doi: 10.1089/rej.2020.2322
8. McCormack, A, Edmondson-Jones, M, Somerset, S, and Hall, D. A systematic review of the reporting of tinnitus prevalence and severity. Hear Res. (2016) 337:70–9. doi: 10.1016/j.heares.2016.05.009
9. Baguley, D, McFerran, D, and Hall, D. Tinnitus. Lancet. (2013) 382:1600–7. doi: 10.1016/S0140-6736(13)60142-7
10. Biswas, R, and Hall, DA. Prevalence, incidence, and risk factors for tinnitus. Curr Top Behav Neurosci. (2021) 51:3–28. doi: 10.1007/7854_2020_154
11. Jarach, CM, Lugo, A, Scala, M, van den Brandt, PA, Cederroth, CR, Odone, A, et al. Global prevalence and incidence of tinnitus: a systematic review and Meta-analysis. JAMA Neurol. (2022) 79:888–900. doi: 10.1001/jamaneurol.2022.2189
12. Shapiro, SB, Noij, KS, Naples, JG, and Samy, RN. Hearing loss and tinnitus. Med Clin North Am. (2021) 105:799–811. doi: 10.1016/j.mcna.2021.05.003
13. Wu, C, Stefanescu, RA, Martel, DT, and Shore, SE. Tinnitus: maladaptive auditory–somatosensory plasticity. Hear Res. (2016) 334:20–9. doi: 10.1016/j.heares.2015.06.005
14. Zhang, J. Auditory cortex stimulation to suppress tinnitus: mechanisms and strategies. Hear Res. (2013) 295:38–57. doi: 10.1016/j.heares.2012.05.007
15. Krauss, P, Tziridis, K, Metzner, C, Schilling, A, Hoppe, U, and Schulze, H. Stochastic resonance controlled upregulation of internal noise after hearing loss as a putative cause of tinnitus-related neuronal hyperactivity [hypothesis and theory]. Front Neurosci. (2016) 10:10. doi: 10.3389/fnins.2016.00597
16. Vanneste, S, and To WTDe Ridder, D. Tinnitus and neuropathic pain share a common neural substrate in the form of specific brain connectivity and microstate profiles. Prog Neuro-Psychopharmacol Biol Psychiatry. (2019) 88:388–400. doi: 10.1016/j.pnpbp.2018.08.015
17. Cai, WW, Li, ZC, Yang, QT, and Zhang, T. Abnormal spontaneous neural activity of the central auditory system changes the functional connectivity in the tinnitus brain: a resting-state functional MRI Study. Front Neurosci. (2019) 13:1314. doi: 10.3389/fnins.2019.01314
18. Mazurek, B, Boecking, B, and Brueggemann, P. Association between stress and tinnitus-new aspects. Otol Neurotol. (2019) 40:e467–73. doi: 10.1097/mao.0000000000002180
19. Davies, JE, Gander, PE, and Hall, DA. Does chronic tinnitus Alter the emotional response function of the amygdala?: a sound-evoked fMRI Study. Front Aging Neurosci. (2017) 9:31. doi: 10.3389/fnagi.2017.00031
20. Billig, AJ, Lad, M, Sedley, W, and Griffiths, TD. The hearing hippocampus. Prog Neurobiol. (2022) 218:102326. doi: 10.1016/j.pneurobio.2022.102326
21. Elmer, S, Schmitt, R, Giroud, N, and Meyer, M. The neuroanatomical hallmarks of chronic tinnitus in comorbidity with pure-tone hearing loss. Brain Struct Funct. (2023) 228:1511–34. doi: 10.1007/s00429-023-02669-0
22. Zimmerman, BJ, Abraham, I, Schmidt, SA, Baryshnikov, Y, and Husain, FT. Dissociating tinnitus patients from healthy controls using resting-state cyclicity analysis and clustering. Netw Neurosci. (2019) 3:67–89. doi: 10.1162/netn_a_00053
23. Hu, J, Cui, J, Xu, J-J, Yin, X, Wu, Y, and Qi, J. The neural mechanisms of tinnitus: a perspective from functional magnetic resonance imaging. Front Neurosci. (2021) 15:621145. doi: 10.3389/fnins.2021.621145
24. Jastreboff, PJ, and Hazell, JW. A neurophysiological approach to tinnitus: clinical implications. Br J Audiol. (1993) 27:7–17. doi: 10.3109/03005369309077884
25. Pinto, PC, Sanchez, TG, and Tomita, S. The impact of gender, age and hearing loss on tinnitus severity. Braz J Otorhinolaryngol. (2010) 76:18–24. doi: 10.1590/s1808-86942010000100004
26. Vanneste, S, Joos, K, and De Ridder, D. Prefrontal cortex based sex differences in tinnitus perception: same tinnitus intensity, same tinnitus distress, different mood. PLoS One. (2012) 7:e31182. doi: 10.1371/journal.pone.0031182
27. Hiller, W, and Goebel, G. Factors influencing tinnitus loudness and annoyance. Arch Otolaryngol Head Neck Surg. (2006) 132:1323–30. doi: 10.1001/archotol.132.12.1323
28. Seydel, C, Haupt, H, Olze, H, Szczepek, AJ, and Mazurek, B. Gender and chronic tinnitus: differences in tinnitus-related distress depend on age and duration of tinnitus. Ear Hear. (2013) 34:661–72. doi: 10.1097/AUD.0b013e31828149f2
29. Aazh, H, Lammaing, K, and Moore, BCJ. Factors related to tinnitus and hyperacusis handicap in older people. Int J Audiol. (2017) 56:677–84. doi: 10.1080/14992027.2017.1335887
30. Schecklmann, M, Landgrebe, M, and Langguth, B. Phenotypic characteristics of hyperacusis in tinnitus. PLoS One. (2014) 9:e86944. doi: 10.1371/journal.pone.0086944
31. Sindhusake, D, Mitchell, P, Newall, P, Golding, M, Rochtchina, E, and Rubin, G. Prevalence and characteristics of tinnitus in older adults: the Blue Mountains hearing Study. Int J Audiol. (2003) 42:289–94. doi: 10.3109/14992020309078348
32. Oosterloo, BC, Croll, PH, Baatenburg de Jong, RJ, Ikram, MK, and Goedegebure, A. Prevalence of tinnitus in an aging population and its relation to age and hearing loss. Otolaryngol Head Neck Surg. (2021) 164:859–68. doi: 10.1177/0194599820957296
33. World Health Organization. World report on hearing. Geneva, Switzerland: World Health Organization (2021).
34. Yang, W, Zhao, X, Chai, R, and Fan, J. Progress on mechanisms of age-related hearing loss. Front Neurosci. (2023) 17:1253574. doi: 10.3389/fnins.2023.1253574
35. Sheffield, AM, and Smith, RJH. The epidemiology of deafness. Cold Spring Harb Perspect Med. (2019) 9, 9:a033258. doi: 10.1101/cshperspect.a033258
36. Wang, J, and Puel, JL. Presbycusis: an update on Cochlear mechanisms and therapies. J Clin Med. (2020) 9:9. doi: 10.3390/jcm9010218
37. Langguth, B, Kreuzer, PM, Kleinjung, T, and De Ridder, D. Tinnitus: causes and clinical management. Lancet Neurol. (2013) 12:920–30. doi: 10.1016/s1474-4422(13)70160-1
38. Shore, SE, Roberts, LE, and Langguth, B. Maladaptive plasticity in tinnitus--triggers, mechanisms and treatment. Nat Rev Neurol. (2016) 12:150–60. doi: 10.1038/nrneurol.2016.12
39. Møller, AR. Epidemiology of tinnitus in adults. Textbook of tinnitus. (2011) 5:29–37. doi: 10.1007/978-1-60761-145-5_5
40. Zhang, D, Xu, Q, Caimino, C, and Baguley, D. The prevalence of tinnitus in China: a systematic review of the literature. J Laryngol Otol. (2021) 135:3–9. doi: 10.1017/S002221512000256X
41. Arriaga, MA. Tinnitus: theory and management. Otol Neurotol. (2005) 26:315–6. doi: 10.1097/00129492-200503000-00036
42. Yakunina, N, and Nam, EC. Does the tinnitus pitch correlate with the frequency of hearing loss? Acta Otolaryngol. (2021) 141:163–70. doi: 10.1080/00016489.2020.1837394
43. Ristovska, L, Jachova, Z, and Stojcheska, V. Psychoacoustic characteristics of tinnitus in relation to audiometric profile. Arch Acoust. (2019) 44:419–28. doi: 10.24425/aoa.2019.129258
44. Chung, SH, Kim, SS, Kim, SH, and Seung, GY. Comparisons of Audiologic characteristics in patients with continuous and intermittent tinnitus. Clin Pract. (2024) 14:1383–90. doi: 10.3390/clinpract14040111
45. Bureš, Z, Profant, O, Svobodová, V, Tóthová, D, Vencovský, V, and Syka, J. Speech comprehension and its relation to other auditory parameters in elderly patients with tinnitus. Front Aging Neurosci. (2019) 11:219. doi: 10.3389/fnagi.2019.00219
46. Michikawa, T, Nishiwaki, Y, Kikuchi, Y, Saito, H, Mizutari, K, Okamoto, M, et al. Prevalence and factors associated with tinnitus: a community-based study of Japanese elders. J Epidemiol. (2010) 20:271–6. doi: 10.2188/jea.je20090121
47. Oiticica, J, and Bittar, RSM. Tinnitus prevalence in the city of São Paulo. Braz J Otorhinolaryngol. (2015) 81:167–76. doi: 10.1016/j.bjorl.2014.12.004
48. Noreña, AJ. An integrative model of tinnitus based on a central gain controlling neural sensitivity. Neurosci Biobehav Rev. (2011) 35:1089–109. doi: 10.1016/j.neubiorev.2010.11.003
49. Rauschecker, JP, Leaver, AM, and Mühlau, M. Tuning out the noise: limbic-auditory interactions in tinnitus. Neuron. (2010) 66:819–26. doi: 10.1016/j.neuron.2010.04.032
50. Hamza, Y, and Zeng, F-G. Tinnitus is associated with improved cognitive performance in non-hispanic elderly with hearing loss. Front Neurosci. (2021) 15:735950. doi: 10.3389/fnins.2021.735950
51. Lin, FR, Yaffe, K, Xia, J, Xue, Q-L, Harris, TB, Purchase-Helzner, E, et al. Hearing loss and cognitive decline in older adults. JAMA Intern Med. (2013) 173:293–9. doi: 10.1001/jamainternmed.2013.1868
52. Berger, JI, Billig, AJ, Sedley, W, Kumar, S, Griffiths, TD, and Gander, PE. What is the role of the hippocampus and parahippocampal gyrus in the persistence of tinnitus? Hum Brain Mapp. (2024) 45:e26627. doi: 10.1002/hbm.26627
53. König, O, Schaette, R, Kempter, R, and Gross, M. Course of hearing loss and occurrence of tinnitus. Hear Res. (2006) 221:59–64. doi: 10.1016/j.heares.2006.07.007
54. Aqeel, M, Ammar, A, and Akhtar, T. The mediating role of tinnitus perception between hearing impairment and development of psychological problems in male and female tinnitus patients. Int J Hum Rights Healthc. (2017) 10:332–43. doi: 10.1108/IJHRH-05-2017-0017
55. Flores, LS, Teixeira, AR, Rosito, LP, Seimetz, BM, and Dall'Igna, C. Pitch and loudness from tinnitus in individuals with noise-induced hearing loss. Int Arch Otorhinolaryngol. (2016) 20:248–53. doi: 10.1055/s-0035-1562935
56. Park, KH, Lee, SH, Koo, JW, Park, HY, Lee, KY, Choi, YS, et al. Prevalence and associated factors of tinnitus: data from the Korean National Health and nutrition examination survey 2009-2011. J Epidemiol. (2014) 24:417–26. doi: 10.2188/jea.je20140024
57. Schlee, W, Hall, DA, Edvall, NK, Langguth, B, Canlon, B, and Cederroth, CR. Visualization of global disease burden for the optimization of patient management and treatment. Front Med. (2017) 4:86. doi: 10.3389/fmed.2017.00086
58. Lugo, A, Trpchevska, N, Liu, X, Biswas, R, Magnusson, C, Gallus, S, et al. Sex-specific association of tinnitus with suicide attempts. JAMA Otolaryngol Head Neck Surg. (2019) 145:685–7. doi: 10.1001/jamaoto.2019.0566
59. Baigi, A, Oden, A, Almlid-Larsen, V, Barrenäs, M-L, and Holgers, K-M. Tinnitus in the general population with a focus on noise and stress: a public health study. Ear Hear. (2011) 32:787–9. doi: 10.1097/AUD.0b013e31822229bd
60. Stouffer, J, and Tyler, RS. Characterization of tinnitus by tinnitus patients. J Speech Hear Disord. (1990) 55:439–53. doi: 10.1044/jshd.5503.439
61. Shargorodsky, J, Curhan, GC, and Farwell, WR. Prevalence and characteristics of tinnitus among US adults. Am J Med. (2010) 123:711–8. doi: 10.1016/j.amjmed.2010.02.015
62. Wallhäußer-Franke, E, Brade, J, Balkenhol, T, D'Amelio, R, Seegmüller, A, and Delb, W. Tinnitus: distinguishing between subjectively perceived loudness and tinnitus-related distress. PLoS One. (2012) 7:e34583. doi: 10.1371/journal.pone.0034583
63. Fujii, K, Nagata, C, Nakamura, K, Kawachi, T, Takatsuka, N, Oba, S, et al. Prevalence of tinnitus in community-dwelling Japanese adults. J Epidemiol. (2011) 21:299–304. doi: 10.2188/jea.je20100124
64. Xia, F, and Ren, Y. Association between caffeine intake from foods and beverages in the diet and hearing loss in United States adults [original research]. Front Neurol. (2024) 15:15. doi: 10.3389/fneur.2024.1436238
65. Sutbas, A, Yetiser, S, Satar, B, Akcam, T, Karahatay, S, and Saglam, K. Low-cholesterol diet and antilipid therapy in managing tinnitus and hearing loss in patients with noise-induced hearing loss and hyperlipidemia. Int Tinnitus J. (2007) 13:143–9.
66. Musleh, A, Alshehri, S, and Qobty, A. Hyperlipidemia and its relation with tinnitus: cross-sectional approach. Niger J Clin Pract. (2022) 25:1046–9. doi: 10.4103/njcp.njcp_1465_21
67. Ramatsoma, H, and Patrick, SM. Hypertension associated with hearing loss and tinnitus among hypertensive adults at a tertiary Hospital in South Africa. Front Neurol. (2022) 13:857600. doi: 10.3389/fneur.2022.857600
68. Mo, F, Zhu, S, Jia, H, Xia, Y, Lang, L, Zheng, Q, et al. Trends in prevalence of hearing loss in adults in the USA 1999-2018: a cross-sectional study. BMC Public Health. (2024) 24:976. doi: 10.1186/s12889-024-18426-9
69. Clifford, RE, and Ryan, AF. The interrelationship of tinnitus and hearing loss secondary to age, noise exposure, and traumatic brain injury. Ear Hear. (2022) 43:1114–24. doi: 10.1097/aud.0000000000001222
70. Cho, Y-S, Choi, S-H, Park, KH, Park, HJ, Kim, J-W, Moon, IJ, et al. Prevalence of otolaryngologic diseases in South Korea: data from the Korea national health and nutrition examination survey 2008. Clin Exp Otorhinolaryngol. (2010) 3:183–93. doi: 10.3342/ceo.2010.3.4.183
71. Sedley, W. Tinnitus: does gain explain? Neuroscience. (2019) 407:213–28. doi: 10.1016/j.neuroscience.2019.01.027
72. Stohler, NA, Reinau, D, Jick, SS, Bodmer, D, and Meier, CR. A study on the epidemiology of tinnitus in the United Kingdom. Clin Epidemiol. (2019) 11:855–71. doi: 10.2147/clep.S213136
73. Martinez, C, Wallenhorst, C, McFerran, D, and Hall, DA. Incidence rates of clinically significant tinnitus: 10-year trend from a cohort study in England. Ear Hear. (2015) 36:e69–75. doi: 10.1097/AUD.0000000000000121
74. Gopinath, B, McMahon, CM, Rochtchina, E, Karpa, MJ, and Mitchell, P. Incidence, persistence, and progression of tinnitus symptoms in older adults: the Blue Mountains hearing Study. Ear Hear. (2010) 31:407–12. doi: 10.1097/AUD.0b013e3181cdb2a2
Keywords: tinnitus, age-related hearing loss, pure-tone average, gender, elderly, association
Citation: Chen Z, Lu Y, Chen C, Lin S, Xie T, Luo X, Lin Y, Chen Y, Feng Y, Xiong G, Ma X, Zeng C and Lin C (2024) Association between tinnitus and hearing impairment among older adults with age-related hearing loss: a multi-center cross-sectional study. Front. Neurol. 15:1501561. doi: 10.3389/fneur.2024.1501561
Edited by:
Alice Lisa Burghard, UCONN Health, United StatesReviewed by:
Andrea Migliorelli, University Hospital of Ferrara, ItalyCopyright © 2024 Chen, Lu, Chen, Lin, Xie, Luo, Lin, Chen, Feng, Xiong, Ma, Zeng and Lin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chaojun Zeng, NzI3NTk5MjU0QHFxLmNvbQ==; Chang Lin, bGluYzMwMUBzaW5hLmNvbQ==
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.