 Xiuzhen Zhao
Xiuzhen Zhao Linxi Liu1,2†
Linxi Liu1,2†- 1The First Dongguan Affiliated Hospital, Guangdong Medical University, Dongguan, China
- 2Guangzhou University of Traditional Chinese Medicine, Guangzhou, China
- 3School of Rehabilitation Medicine, Gannan Medical University, Ganzhou, China
Background: Electroacupuncture (EA) has been employed to address the symptoms of constipation in individuals who have experienced a stroke. However, supporting evidence for its efficacy is lacking. This meta-analysis aims to investigate whether EA was effective in treating poststroke constipation.
Methods: We conducted a comprehensive search of eight databases, including four English-language databases (PubMed, Embase, Web of Science, and the Cochrane Library) and four Chinese-language databases (Chinese Biomedical Literature Database, China National Knowledge Infrastructure, VIP, and Wanfang), for randomized controlled trials (RCTs) published from inception through January 31, 2023. To assess treatment effectiveness, we calculated the risk ratio (RR) or mean difference (MD) with 95% confidence interval (CI).
Results: A total of 9 RCTs involving 601 participants were included. No heterogeneity was found across the included RCTs. The results of this meta-analysis indicated significant improvements in the total effective rate (RR = 1.39, 95% CI 1.27, 1.52), cure rates (RR 1.87, 95% CI 1.38, 2.54), constipation scoring system (MD = −2.51, 95% CI −3.05, −1.97), and quality of life (MD = −10.69, 95% CI −14.2, −7.17) in the EA group compared with the control group.
Conclusion: Current evidence indicates that EA may be recommended for patients experiencing poststroke constipation. The lack of thorough investigations has undermined the quality of the major findings.
1 Introduction
Stroke is a neurological abnormality brought on by cerebrovascular conditions such as cerebral infarction, cerebral hemorrhage, and subarachnoid hemorrhage, which cause localized damage to the central nervous system (1). This illness places a considerable financial strain on society and healthcare systems, consistently ranking as one of the leading causes of mortality, disability, and public health issues globally (2). In comparison to patients in the acute stage, convalescent patients experience a higher incidence of constipation, which detrimentally affects their quality of life (QoL), physical functioning, and recovery capacity (3). Previous systematic reviews have shown that the prevalence of constipation in stroke patients is approximately 48% (95% CI: 33–63%) (4). Due to limitations in physical activity and other factors, the prevalence of movement disorders is higher in stroke patients compared to healthy individuals (5). Poststroke constipation not only impacts patients’ QoL but also makes it more difficult for patients to recover and can even lead to the recurrence of cerebrovascular diseases (6).
In recent years, research has primarily concentrated on the incidence of poststroke constipation, while effective management strategies for these patients remain scarce (4, 7). Gastrointestinal (GI) illnesses are highly prevalent worldwide. Due to recurrent symptoms and the sometimes limited effectiveness of conventional treatments, patients with gastroesophageal reflux disease (8), functional dyspepsia (9), irritable bowel syndrome (10), and inflammatory bowel conditions (11) often turn to complementary therapies, including acupuncture. For thousands of years, Asian nations have used acupuncture as a form of medicine. Over the past few decades, acupuncture has also drawn more attention in western nations, with numerous studies examining its function in gastroenterology (12). Current drug therapies are often inadequate in alleviating symptoms and enhancing the quality of life for patients with constipation. The physiopathology of constipation can be complex, with various underlying mechanisms potentially contributing to treatment resistance. Therefore, there is a pressing need for simple and accurate diagnostic tools to identify specific subtypes of constipation that may respond to targeted therapies (13, 14). Additionally, adverse effects such as bloating (15), diarrhea (16), and nausea (17) are frequently reported. Therefore, we need to urgently look for effective treatment strategies with fewer side effects.
Traditional Chinese medicine (TCM) has long been used in China and globally due to its safety and long-lasting effects (18, 19). As a key component of complementary medicine, acupuncture is gaining popularity in numerous medical institutions for treating patients with poststroke constipation (20). Electroacupuncture (EA) is a therapeutic technique that combines the use of needles and electrical stimulation to prevent and treat various diseases. Low-frequency pulsed current is applied near the body’s bioelectric pathways, with the goal of eliciting therapeutic effects through the modulation of the body’s electrical signals and energy flows (21). This particular remedy has been employed to address several ailments including diarrhea, and abdominal pain (22, 23). According to preclinical research, EA stimulation of abdominal points has been shown to impact sympathetic innervation of the gastrointestinal tract, whereas stimulation of limb points can influence parasympathetic input (23, 24).
A systematic review has recommended EA as a treatment for poststroke constipation (25), and one study has indicated that EA may have some long-lasting effects (26). However, whether this evidence is applicable to the treatment of poststroke constipation remains unclear. EA can also stimulate the parasympathetic nerve, increase rectal pressure, and restore the sense of defecation (16). Despite the longstanding use of acupuncture as a potential treatment modality, there have been no rigorous qualitative or quantitative analyses evaluating the effects of EA on the abdomens of patients with stroke for the management of constipation. Overall, there is a paucity of evidence supporting the efficacy and safety of EA in the treatment of poststroke constipation. In this systematic review, we sought to comprehensively evaluate the existing literature to assess the efficacy and safety of EA for the management of constipation in the stroke population.
2 Methods
2.1 Study registration
This systematic review and meta-analysis was conducted and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) checklist (27) and the Cochrane Handbook for Systematic Reviews of Interventions (28). This study has also been registered on the PROSPERO website (ID: CRD42022375282).1
2.2 Database and search strategy
A comprehensive literature search was conducted across four English-language databases (PubMed, Embase, web of science, and the Cochrane central register of controlled trials) and four Chinese-language databases [Chinese biomedical literature database, China National Knowledge Infrastructure (CNKI), Chinese science and technology periodicals (VIP), and WANFANG digital periodicals (WANFANG)] for randomized controlled trials (RCTs) published from inception through January 31, 2023. The topic of this study is EA for the treatment of poststroke constipation; thus, the following medical subject words were used for the search: electroacupuncture AND stroke AND (constipation OR dysporia OR dysdefecation).
2.3 Study selection
Two independent reviewers (XZZ and LXL) conducted the study selection process, including screening of titles and abstracts, as well as assessing the full-text eligibility of potentially relevant studies. Any discrepancies were resolved through discussion or consultation with the corresponding author (CLM).
2.4 Type of studies
2.4.1 Participants
Adults who met the diagnostic standards (29) for post-stroke constipation were included in this study, which used EA as an intervention technique. We included all participants, without any restrictions on site of injury, type of injury, degree of constipation, or timing of the stroke, to include all pertinent articles.
2.4.2 Interventions
The main type of intervention included was the use of different forms of electrical stimulation to target the acupoints treating poststroke constipation. Relevant RCTs performing a comparison between EA plus conventional treatment (medication, manipulation, or any other treatment) and the same conventional treatment were included, regardless of blinding.
2.4.3 Outcomes
The primary outcome measures included the total effective rate, cure rate, and QoL following electroacupuncture (EA) treatment. Additionally, the patients’ clinical scores and QoL were evaluated using standardized tools such as the Constipation Scoring System (CSS), Patient Assessment of Constipation Quality of Life (PAC-QoL), or other relevant scales.
2.5 Exclusion criteria
Studies were excluded based on the following criteria: (1) studies with inappropriate randomization methods or incomplete data; (2) reviews, case reports, non-clinical studies, and animal studies; (3) studies lacking relevant data of interest; (4) studies with unclear or insufficient outcome measures; and (5) multiple publications reporting identical findings.
2.6 Data extraction and management
To identify the eligible RCTs, two authors (YXD and XZZ) independently examined the full texts of all articles retrieved from the databases. A third researcher (CLM) helped settle any disagreements regarding the studies that were chosen. The reviewers selected the studies after reviewing the exclusion and inclusion criteria and rigorously analyzing the titles and abstracts of all studies; after reading the studies, they decided which reserved documents to include. For each eligible study, the following items were extracted independently: author, year, randomization method, sample size, patient age, disease course, intervention, treatment course, total effective rate, cure rate, and adverse event records. Any differences during the extraction process were resolved by principal investigator (CLM). If missing data were found, the corresponding author was contacted by email for information. In cases of several studies describing the same trial, only one study was included.
2.7 Risk of bias assessment
The study quality was independently assessed by two investigators (YXD and XZZ) using the Cochrane system-recommended ROB assessment tools (RevMan 5.4) (28). The assessment was based on the following criteria: random sequence generation and allocation concealment (selection bias), blinding of participants and outcome assessors, handling of incomplete results, selective reporting, and other potential sources of bias. Each criterion was rated as having a high, low, or unclear risk of bias (ROB). In case of any disagreement between the assessors, one of the corresponding authors (CLM) was consulted for resolution. The overall risk of bias was determined based on the ratings of each criterion.
2.8 Data synthesis and statistical analysis
The data analysis was performed using the RevMan 5.4 software developed by the Cochrane Collaboration in the United Kingdom. For the main results of the studies that were included, we computed aggregate estimates with 95% CIs using RR for count data and MD with 95% CIs for measurement data. A significance level of p < 0.05 was deemed to have statistical significance. The heterogeneity among the studies included in the analysis was evaluated using a heterogeneity test. If there was no notable variation (I2 < 50%), the fixed-effects model was employed to merge the effect estimates. If there was a substantial amount of variation (I2 > 50%), the random-effects model was used instead (49). Any potential outliers or influential studies were discovered and addressed through the use of sensitivity analysis. If the data contained in the study could not be subjected to meta-analysis, a descriptive analysis was performed. Publication bias was evaluated by generating funnel plots using RevMan 5.4. The PRISMA principles were adhered to during the execution of all these procedures (30).
3 Results
3.1 Study identification and selection
We conducted an extensive search across eight electronic databases and found a total of 645 studies using the preset search tactics. After eliminating duplicate entries, there were 544 studies remaining. Out of these, a total of 522 studies were eliminated after reviewing their titles and abstracts because they did not match the predetermined criteria for inclusion. After thoroughly examining the complete texts of the remaining 22 investigations, an additional 13 studies were eliminated due to the predetermined exclusion criteria. Therefore, a grand number of nine RCTs were incorporated into the meta-analysis (31–39). For a comprehensive depiction of the research selection and inclusion process, please consult (Figure 1).
Figure 1. Flow chart of study search and selection process.
3.2 Characteristics of the included studies
Table 1 presents the attributes of the participants and the frequency of undesirable incidents in the studies that were included. The study included nine RCTs (31–39) with a total of 601 patients (344 men and 257 women). Among them, 315 patients were in the EA group and 286 patients were in the control group. The nine investigations were carried out only in China from 2008 to 2017, and the duration of the follow-up periods varied from 13 to 90 days. The experimental groups were administered conventional EA, while the control groups received either filiform needle acupuncture or medicine. All of the trials documented both the overall efficacy rate and the rates of complete recovery. Eight RCTs (31–37, 39) utilized the CCS to evaluate the patients’ scores, while only two investigations employed the PAC-QoL scale to examine the QoL. Table 2 provides a summary of the interventions’ characteristics, which include the treatment equipment, point selection site, and treatment prescription. The acupoints Tianshu (ST 25) and Daheng (SP 15) were the most commonly utilized in the investigations, with Tianshu being used in 88.9% of the studies (31–34, 36–39) and Daheng in 66.7% of the studies (31–35, 38, 39). The duration of the treatment varied between 2 and 4 weeks, with sessions occurring 6–7 times each week, lasting 30 min each. Table 3 provides a concise overview of the research’ objectives, criteria for inclusion, and key findings.
Table 1. Basic characteristics of EA treatment of poststroke constipation.

Table 2. Characteristics of EA parameters.
Table 3. The aim, primary findings, and conclusions of the studies included in this systematic review.
3.3 Methodological quality of the included trials
A risk assessment was performed to evaluate the methodological rigor of the studies that were included. Figure 2 presents the specific information regarding the assessment. All of the included experiments met the criterion for randomized sequence generation. Five studies (31, 32, 36–38) had an uncertain level of danger for both participants and assessors, while four studies (33–35, 39) had a high level of risk, and the quality of evaluations in these areas was subpar. Regarding data integrity, seven studies (31–36, 39) were evaluated as having a low risk, while the remaining two (37, 38) were considered to have a high risk. None of the studies revealed any additional bias.
Figure 2. Risk of bias summary.
3.4 Meta-analysis outcomes
3.4.1 Total effective rate
All nine studies provided information on the overall efficacy of EA in comparison to conventional treatment. Subgroup analysis was performed based on the outcome measures used as the criteria for grouping. The findings of the heterogeneity test suggested that the EA may be the main cause of heterogeneity. The findings demonstrated that EA is a highly successful treatment for poststroke constipation, as illustrated in Figure 3. The study included nine RCTs (31–39), with a total of 601 patients. These trials evaluated the overall effectiveness of EA in patients with poststroke constipation, comparing it to healthy individuals. The combined findings of these studies indicated that EA had a significant positive effect on the overall effective rate (RR = 1.29, 95% CI = [1.07, 1.55], I2 = 81%, p < 0.05). The subgroup analyses of the EA were conducted to compare the effectiveness of EA versus medication. The results showed a RR of 1.47, with a 95% CI ranging from 1.07 to 2.01. The heterogeneity of the studies, as measured by I2, was 86%. The p-value was less than 0.001, indicating statistical significance. The EA vs. filiform needle comparison yielded a RR of 1.12, with a 95% CI of [1.02, 1.25]. The heterogeneity (I2) was 0% and the p-value was less than 0.05. This information is presented in Figure 3.
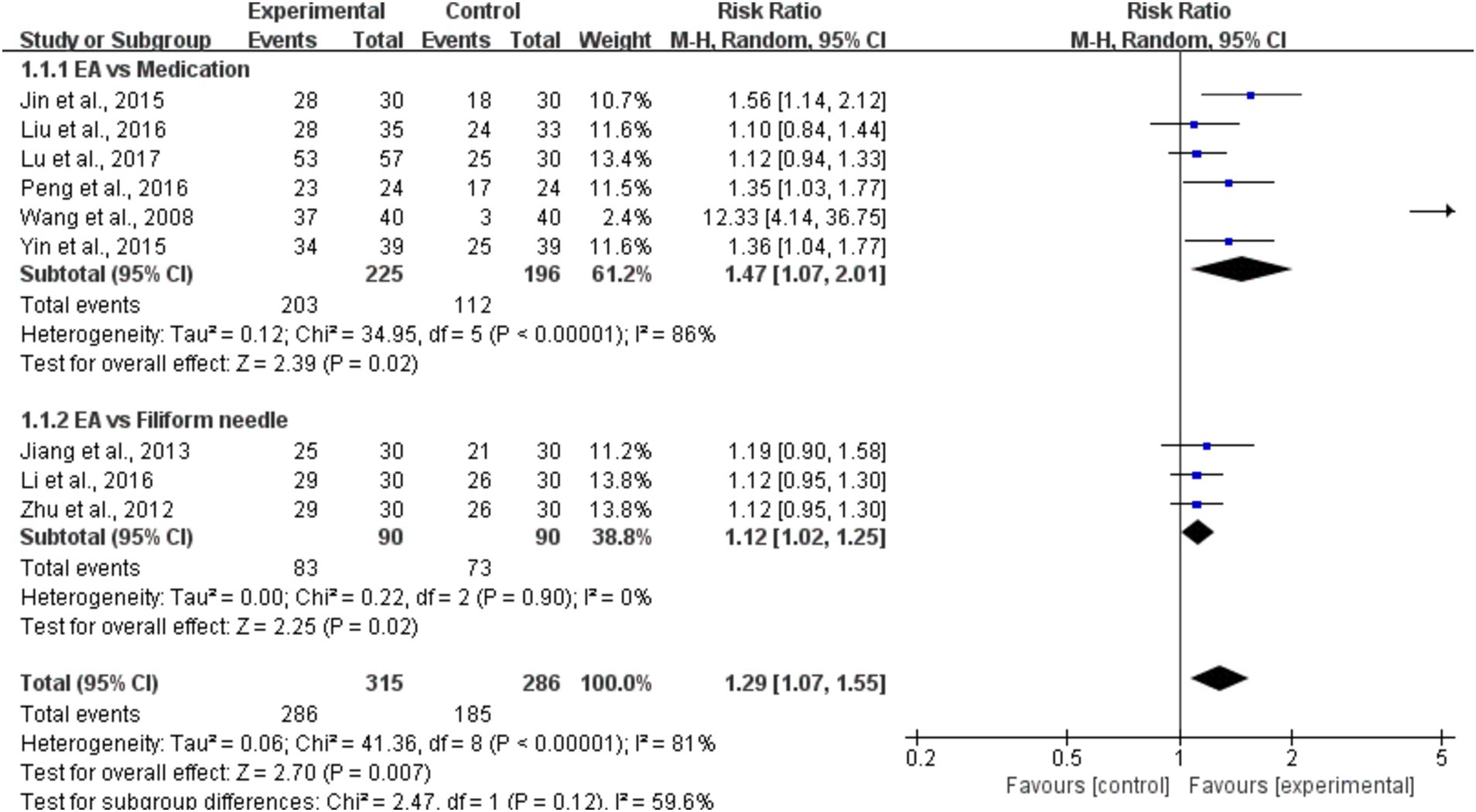
Figure 3. A forest plot of the subgroup analysis of the included studies comparing EA group and control group in changes of the total effective rate.
3.4.2 Cure rate
We conducted subgroup analyses to further investigate the effect of EA on cure rates in patients with poststroke constipation compared to healthy individuals (31–39). The aggregated results demonstrated that EA significantly improved cure rates overall (RR = 1.87, 95% CI = [1.38, 2.54], I2 = 0%, p < 0.001), indicating a nearly twofold increase in the likelihood of cure with EA when compared to control treatments. In the subgroup analysis comparing EA to medication, the results also showed a significant improvement in cure rates for EA (RR = 1.86, 95% CI = [1.33, 2.59], I2 = 0%, p < 0.001). This suggests that EA is more effective than medication in improving cure rates, with an 86% higher likelihood of cure in the EA group. However, for the subgroup comparing EA to the use of filiform needles (a type of acupuncture technique), the results were not statistically significant (RR = 1.93, 95% CI = [0.88, 4.27], I2 = 0%, p > 0.05). Although the relative risk suggests that EA might be more effective than filiform needle therapy, the wide confidence interval and the p-value greater than 0.05 indicate that this result is not conclusive, and more studies would be necessary to determine if EA truly surpasses filiform needle therapy in terms of cure rates (Figure 4).

Figure 4. A forest plot of the subgroup analysis of the included studies comparing EA group and control group in changes of the cure rate.
3.4.3 CCS
Eight studies (31–39), which included a total of 523 subjects, used the CCS to evaluate patients’ clinical outcomes. The aggregated results of these studies suggested that EA significantly improved the constipation score (MD = −2.51, 95% CI = [−3.05, −1.97], I2 = 2%, p < 0.001). Subgroup analyses of the EA, for the subgroup of EA vs. medication (MD = −2.15, 95% CI = [−2.84, −1.47], I2 = 1%, p < 0.001). For the EA vs. filiform needle (MD = −3.06, 95% CI = [−3.93, −2.19], I2 = 0%, p < 0.001) (Figure 5).
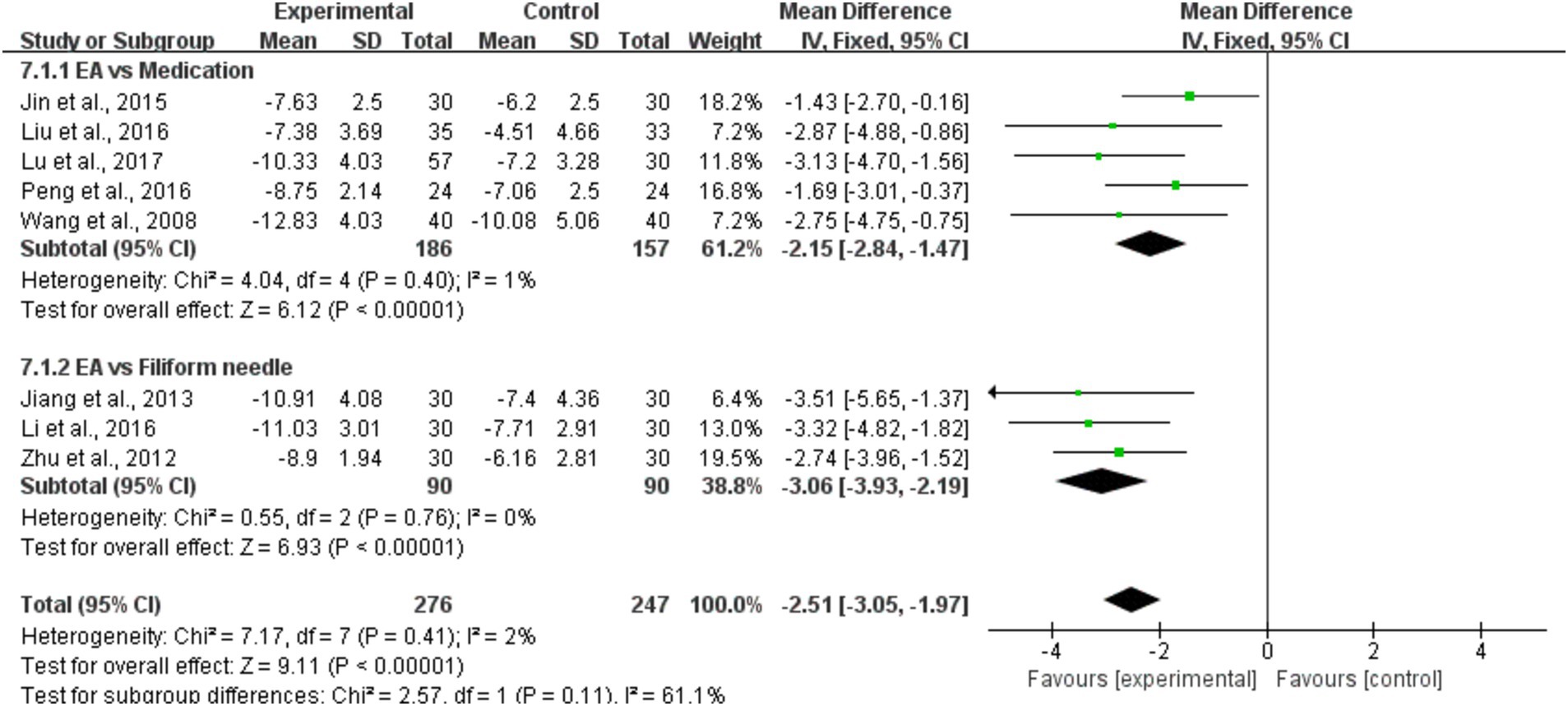
Figure 5. A forest plot of the subgroup analysis of the included studies comparing EA group and control group in changes of the CCS.
3.4.4 PAC-QoL
The QoL in the target population was reported in just two research (34, 36). A grand number of 147 patients were evaluated. The QoL analysis utilized a fixed-effects model due to the absence of heterogeneity. The findings demonstrated that EA had a substantial positive impact on the QoL of patients with poststroke constipation, as compared to the control group (MD = −10.69, 95% CI = [−14.2, −7.17], p < 0.001) (Figure 6).

Figure 6. A Forest plot of EA group vs. control group: PAC-QoL.
3.4.5 Adverse events
None of the studies showed any negative effects in the treatment of poststroke constipation, suggesting that EA can be utilized as a secure and efficient traditional Chinese medicine approach in the therapeutic management of poststroke constipation.
3.4.6 Publication Bias
The RevMan 5.4 software was utilized to generate funnel plots for the identification of publication bias (Figure 7). The clinical efficacy analysis results and funnel plots indicated the presence of asymmetry and significant bias.
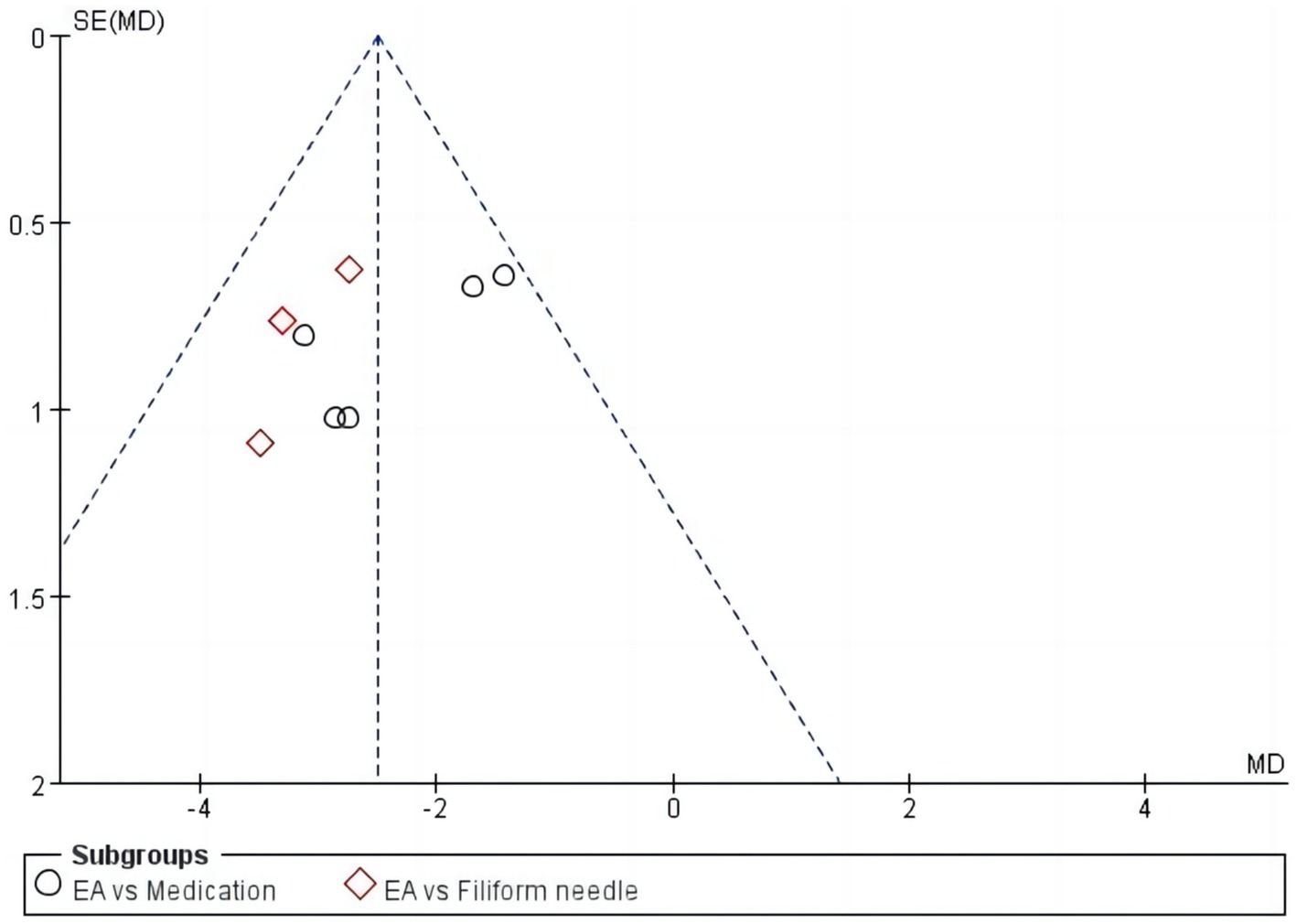
Figure 7. Funnel chart of clinical efficacy.
4 Discussion
This study is the initial comprehensive research and meta-analysis to consolidate the findings on the therapeutic impact of EA in individuals suffering from poststroke constipation. We conducted a thorough assessment of 9 randomized controlled trials (RCTs) in order to assess the effectiveness and safety of EA treatments in patients suffering from constipation after a stroke. Our study revealed a shortage of high-quality RCTs investigating therapies in this area. Tianshu (ST 25) and Daheng (SP 15) have been commonly chosen as acupoints for treating constipation in numerous investigations, resulting in positive therapeutic outcomes. As a result, they are favored in clinical practice.
When analyzing the results of the meta-analysis on the efficacy of abdominal EA therapy for poststroke constipation, it is crucial to take into account potential sources of bias and limitations in the studies that were included. Publication bias, selective reporting bias, and financing prejudice are potential causes of bias that could have impacted the overall findings. These biases can result in an inflated evaluation of the treatment impact and manipulate the body of data. Furthermore, it is important to consider constraints such as limited sample sizes, variations among the research, and the possibility of publication bias. These factors can influence the accuracy and applicability of the findings.
According to current medical theory, the objective of acupuncture treatment for poststroke constipation is to reestablish the patient’s physiological equilibrium by controlling the enteric nervous system, sympathetic and parasympathetic nervous systems, and the central nervous system (40). Multiple investigations have demonstrated that acupuncture has the ability to modulate the gastrointestinal functions of the body (41, 42). The afferent impulse of acupuncture travels to the brain centers at all levels, through the spinal cord, and out through the autonomic nervous system and humoral pathways to affect gastrointestinal function via the somatic nerve and vascular wall nerve plexus pathways (6, 43).
In order to improve the body’s ability to self-regulate and potentially expedite the healing process, certain sites along the meridians are physically stimulated by methods such as needle insertion, heat application, or pressure. Most acupuncture methods utilize single-use stainless-steel needles, each of which has a little larger diameter than the average human hair. The needles penetrate the “acupuncture points” on the skin. The needle that is inserted can be subjected to heat or electrical current, rotated, or moved vertically and horizontally at different rates and depths. The precise method by which EA affects poststroke constipation is not yet understood. Several factors, including as the mix of acupoints, meticulous selection of acupoints, and the depth of EA, can influence the effectiveness of EA. Further research and network meta-analyses are necessary to investigate the efficacy of different EA approaches. There is no medical treatment that can entirely erase the subjective sensations of patients. Conducting placid acupuncture is necessary to validate the impartiality of EA’s efficacy. Prior research has indicated that abdominal EA activates particular acupuncture points, such as Quchi (LI 11) or Shangjuxu (ST 37), which can regulate the equilibrium between the parasympathetic and sympathetic nervous systems. It is theorized that this stimulation enhances the movement of the gastrointestinal tract, therefore relieving symptoms of constipation. Additional research on the neurophysiological and biochemical mechanisms associated with abdominal EA therapy could enhance our understanding of how it works.
According to the findings of this meta-analysis, we saw significant improvements in the total effective rate, cure rate, CCS score, and PAC-QoL. These results provide confirmation of the usefulness of EA to a certain degree. This procedure may entail several treatment strategies. EA can enhance the patients’ symptoms through many means. Cui and colleagues conducted a study using 50 male Wistar rats to investigate the impact of various EA frequencies (ST25) on the time it takes for the first black stool to be excreted, as well as the electromyography of the colon, vasoactive intestinal peptide (VIP), and substance P immune activity in rats with slow transit constipation (44). The down-regulation of VIP immune activity and up-regulation of substance P immune activity in the colon tissue may have caused the electromyographic observation that EA enhanced colon activity. The therapeutic effects of 100 Hz-EA were less effective compared to those of 2 Hz/100 Hz-EA and 2 Hz-EA. In a separate research investigation, Liang and his team divided a total of 50 mice into two distinct groups. The first group, known as the model group (n = 40), did not get any form of treatment. On the other hand, the second group, referred to as the EA group, was subjected to a frequency range of 2–15 Hz with an amplitude of 1 mA at ST 37 for a duration of 15 min every day over a span of 3 consecutive days (45). An additional six mice formed a control group that did not experience constipation. This work provides evidence that the application of EA stimulation at acupoint ST 37 can partially reinstate the functionality of enteric neurons and ameliorate the impairment of intestinal motility. The enteric nervous system can impact changes in intestinal motility by affecting inhibitory neurons. In another study, Zhu and colleagues employed immunohistochemistry methods to identify the presence of protein gene product 9.5 and neuronal nitric oxide synthase in the muscle tissue of the jejunum, ileum, and proximal colon. Electrically activating acupuncture point ST 37 has been found to alleviate intestine motor dysfunction and partially restore intestinal neuron function, according to the research findings (43). The enteric nervous system can influence alterations in intestinal motility by impacting inhibitory neurons. The preceding description supports our findings, which suggest that using EA to stimulate the Tianshu, Daheng, and Shangjuxu points may be a more effective treatment for poststroke constipation in patients. Nevertheless, variations in the research findings may arise due to the limited duration of the follow-up periods and the absence of conscious analysis.
Due to the poor quality of the studies included and the overall lack of high-quality research on the use of EA for treating poststroke constipation, the findings of our analysis cannot be substantiated by the available literature. In addition, none of the studies included in the analysis have been registered in the Chinese Clinical Trial Registry, which prevents us from determining whether there has been any selective reporting of the study results. The randomization procedures, double blinding, adverse responses, and follow-up of the included studies exhibit significant faults, rendering the assessment of long-term treatment outcomes unfeasible. Furthermore, it is highly probable that there is selection bias, implementation bias, and measurement bias in the process due to the lack of universal diagnostic and efficacy evaluation criteria utilized in the literature, and the failure to adhere to internationally accepted standards (46). Effective use of blinding or masking techniques can significantly mitigate measurement bias and placebo effects. Out of the research that were analyzed, the double-blind principle was determined to have an unclear level of risk in 5 studies (31, 32, 36–38), high risk in 2 studies (33, 35) and low risk in 2 studies (34, 39). In five of the studies (31, 32, 36–38), the assessors were blind assessed as unknown risk. Due of the crucial role of communication between the therapist and patient in acupuncture, achieving double blindness is challenging.
A thorough and systematic review and analysis (47), pertaining to our research, was carried out to assess the efficacy and safety of acupuncture in treating constipation following a stroke. The study incorporated several RCTs and using the RoB 2.0 tool to evaluate the methodological quality. The meta-analysis was conducted using RevMan 5.3 and Stata 15.1 software, and the quality of evidence was evaluated using the GRADE approach. In addition, the study employed the Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) standards to evaluate the quality of reporting for acupuncture interventions. By contrasting the findings of the meta-analysis with our own study, we may discern many parallels and contrasts that are pivotal for a thorough examination of the current data on acupuncture for post-stroke constipation. Firstly, the two studies may have discrepancies in their inclusion criteria and search methodologies. The study incorporated nine RCTs sourced from diverse databases, however the meta-analysis might have utilized distinct databases and a dissimilar time frame. These disparities may lead to inequalities in the quantity of research included and the characteristics of the patient population. Both studies evaluated several outcome measures including overall responder rate, constipation symptom scores, SP levels, latency to first bowel movement, serum VIP levels, and Bristol Stool Scale (BSS) scores. The findings of the two investigations shown congruency in some dimensions. Both studies demonstrated that acupuncture, whether used alone or in conjunction with conventional therapy, was superior to conventional therapy alone in enhancing the overall responder rate, decreasing constipation symptom scores, elevating SP levels, accelerating the time to the first bowel movement, and reducing VIP levels. Nevertheless, there were disparities in the outcomes pertaining to BSS scores. When acupuncture was used together with conventional therapy, it was found to be better than conventional therapy alone based on BSS scores. However, when acupuncture was used alone, there were no statistically significant differences compared to conventional therapy. The results of this meta-analysis have significant implications for the practical use of abdominal EA therapy in treating poststroke constipation. Incorporating abdominal EA into rehabilitation programs for stroke patients has the potential to provide a beneficial additional treatment method. Abdominal EA therapy has the potential to improve the QoL and overall recovery of poststroke patients by boosting gastrointestinal motility and alleviating constipation symptoms. Furthermore, the therapy is appealing for clinical practice due to its relatively affordable price and little negative effects.
EA has been recognized as a treatment method that provides benefits compared to other therapies and shows efficacy in treating constipation (25). Recognizing the constraints of our research is crucial. Initially, despite attempts to incorporate extensive datasets, it is not possible to completely eliminate the potential for publication bias. Furthermore, the studies that were considered may have intrinsic limitations, such as having small sample numbers or variances in study methods. Moreover, the variability among the trials may contribute to a certain level of ambiguity in the combined findings. Finally, this meta-analysis only considered papers written in English and Chinese languages, which may introduce a linguistic bias. It is important to consider these constraints while analyzing the results. In order to encourage the worldwide adoption of EA and assure the efficient implementation of medical scientific research findings, future RCTs should adhere to universal diagnostic criteria and efficacy evaluation criteria, guided by evidence-based medicine (48). In order to improve the quality of EA research, it is crucial to focus on patients’ TCM symptoms and apply tailored EA methods. Furthermore, in the process of conducting clinical research, it is essential to guarantee the appropriate randomization of cases in order to assure the comparability of the observation and control groups. However, researchers frequently neglect the extraction and analysis of TCM syndrome differentiation data while assessing the equilibrium of fundamental data sets. Since EA is based on TCM syndrome differentiation, the lack of data on syndrome differentiation makes it difficult to determine the comparability across groups. In clinical controlled research, the inclusion of a blank control group can aid in the unbiased evaluation of the effectiveness of acupuncture.
5 Conclusion
Overall, the findings of this meta-analysis indicate that EA as a therapeutic intervention enhances the overall effectiveness, rate of complete recovery, CCS, and QoL in stroke patients suffering from constipation, without causing any additional negative effects. Nevertheless, due to the absence of rigorous studies, the primary conclusions have been compromised in terms of their quality. In order to address the limitations of current research and provide strong evidence for the clinical use and recommendations of various types of EA, it is necessary to conduct further well-designed and high-quality trials with large sample sizes.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
XZ: Writing – original draft. LL: Writing – original draft. YD: Writing – original draft. CM: Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Footnotes
References
1. Sacco, RL, Kasner, SE, Broderick, JP, Caplan, LR, Connors, JJ, Culebras, A, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2013) 44:2064–89. doi: 10.1161/STR.0b013e318296aeca
2. Zhang, Q, Fu, Y, Lu, Y, Zhang, Y, Huang, Q, Yang, Y, et al. Impact of virtual reality-based therapies on cognition and mental health of stroke patients: systematic review and meta-analysis. J Med Internet Res. (2021) 23:e31007. doi: 10.2196/31007
3. Shang, J, He, Y, Wang, R, Xu, Y, and Xu, J. Comparison of therapeutic effects of different acupuncture and moxibustion therapies on constipation after stroke treatment: a protocol for systematic review and network meta-analysis. Medicine. (2021) 100:e27397. doi: 10.1097/md.0000000000027397
4. Lim, SF, and Childs, C. A systematic review of the effectiveness of bowel management strategies for constipation in adults with stroke. Int J Nurs Stud. (2013) 50:1004–10. doi: 10.1016/j.ijnurstu.2012.12.002
5. Li, J, Yuan, M, Liu, Y, Zhao, Y, Wang, J, and Guo, W. Incidence of constipation in stroke patients: a systematic review and meta-analysis. Medicine. (2017) 96:e7225. doi: 10.1097/md.0000000000007225
6. Zhang, T, Wang, G, Li, B, Wang, L, Guo, J, Hu, J, et al. Effect of acupuncture for constipation after ischemic stroke: study protocol for a randomized controlled trial. Trials. (2018) 19:454. doi: 10.1186/s13063-018-2750-0
7. Su, Y, Zhang, X, Zeng, J, Pei, Z, Cheung, RTF, Zhou, Q(P), et al. New-onset constipation at acute stage after first stroke: incidence, risk factors, and impact on the stroke outcome. Stroke. (2009) 40:1304–9. doi: 10.1161/strokeaha.108.534776
9. Ford, AC, Mahadeva, S, Carbone, MF, Lacy, BE, and Talley, NJ. Functional dyspepsia. Lancet. (2020) 396:1689–702. doi: 10.1016/s0140-6736(20)30469-4
10. Chey, WD, Kurlander, J, and Eswaran, S. Irritable bowel syndrome: a clinical review. JAMA. (2015) 313:949–58. doi: 10.1001/jama.2015.0954
11. Zhang, YZ, and Li, YY. Inflammatory bowel disease: pathogenesis. World J Gastroenterol. (2014) 20:91–9. doi: 10.3748/wjg.v20.i1.91
12. Rabitti, S, Giovanardi, CM, and Colussi, D. Acupuncture and related therapies for the treatment of gastrointestinal diseases. J Clin Gastroenterol. (2021) 55:207–17. doi: 10.1097/mcg.0000000000001455
13. Basilisco, G Italian Society of Neurogastroenterology Motility (SINGEM) Study Group. Patient dissatisfaction with medical therapy for chronic constipation or irritable bowel syndrome with constipation: analysis of N-of-1 prospective trials in 81 patients. Aliment Pharmacol Ther. (2020) 51:629–36. doi: 10.1111/apt.15657
14. Chiarioni, G, Lambiase, C, Whitehead, WE, Rettura, F, Morganti, R, Popa, SL, et al. Difficult defecation in constipated patients: diagnosis by minimally invasive diagnostic tests. Dig Liver Dis. (2024) 56:429–35. doi: 10.1016/j.dld.2023.06.004
15. DiPalma, JA, Cleveland, MV, McGowan, J, and Herrera, JL. A randomized, multicenter, placebo-controlled trial of polyethylene glycol laxative for chronic treatment of chronic constipation. Am J Gastroenterol. (2007) 102:1436–41. doi: 10.1111/j.1572-0241.2007.01199.x
16. Zhang, C, Guo, L, Guo, X, Li, G, and Guo, X. Short and long-term efficacy of combining Fuzhengliqi mixture with acupuncture in treatment of functional constipation. J Trad Chin Med. (2013) 33:51–9. doi: 10.1016/s0254-6272(13)60100-4
17. Li, Y, An, L, and Tian, H. Diabetic constipation treated with acupoint embedding therapy and forlax: a randomized controlled trial. Zhongguo Zhen Jiu. (2016) 36:124–8.
18. Wang, L, Wu, F, Hong, Y, Shen, L, Zhao, LJ, and Lin, X. Research progress in the treatment of slow transit constipation by traditional Chinese medicine. J Ethnopharmacol. (2022) 290:115075. doi: 10.1016/j.jep.2022.115075
19. Yuan, QL, Guo, TM, Liu, L, Sun, F, and Zhang, YG. Traditional Chinese medicine for neck pain and low back pain: a systematic review and meta-analysis. PLoS One. (2015) 10:e0117146. doi: 10.1371/journal.pone.0117146
20. Tack, J, and Müller-Lissner, S. Treatment of chronic constipation: current pharmacologic approaches and future directions. Clin Gastroenterol Hepatol. (2009) 7:502–8. doi: 10.1016/j.cgh.2008.12.006
21. Liu, AJ, Li, JH, Li, HQ, Fu, DL, Lu, L, Bian, ZX, et al. Electroacupuncture for acute ischemic stroke: a meta-analysis of randomized controlled trials. Am J Chin Med. (2015) 43:1541–66. doi: 10.1142/s0192415x15500883
22. Wang, Y, Zhou, M, Shen, J, Wang, D, Xu, N, Song, Y, et al. Effect of electroacupuncture on chemotherapy-induced diarrhea: study protocol for a randomized controlled trial. Transl Cancer Res. (2021) 10:2516–24. doi: 10.21037/tcr-20-3400
23. Kee Jang, D, Kyu Lee, J, Yung Jung, C, Ho Kim, K, Ra Kang, H, Sun Lee, Y, et al. Electroacupuncture for abdominal pain relief in patients with acute pancreatitis: a three-arm randomized controlled trial. J Integr Med. (2023) 21:537–42. doi: 10.1016/j.joim.2023.10.004
24. Li, YQ, Zhu, B, Rong, PJ, Ben, H, and Li, YH. Neural mechanism of acupuncture-modulated gastric motility. World J Gastroenterol. (2007) 13:709–16. doi: 10.3748/wjg.v13.i5.709
25. Jie, L, Shiping, L, Yue, X, and Fuli, Z. Efficacy and safety of electroacupuncture for secondary constipation: a systematic review and meta-analysis. Int J Color Dis. (2023) 38:196. doi: 10.1007/s00384-023-04487-6
26. Liu, Z, Yan, S, Wu, J, He, L, Li, N, Dong, G, et al. Acupuncture for chronic severe functional constipation: a randomized trial. Ann Intern Med. (2016) 165:761–9. doi: 10.7326/m15-3118
27. Page, MJ, McKenzie, JE, Bossuyt, PM, Boutron, I, Hoffmann, TC, Mulrow, CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst Rev. (2021) 10:89. doi: 10.1186/s13643-021-01626-4
28. Cumpston, M, Li, T, Page, MJ, Chandler, J, Welch, VA, Higgins, JPT, et al. Updated guidance for trusted systematic reviews: a new edition of the Cochrane handbook for systematic reviews of interventions. Cochrane Database Syst Rev. (2019) 10:Ed000142. doi: 10.1002/14651858.Ed000142
29. Tang, OF, Huang, SM, Ye, XX, Liu, QX, Chen, TT, and Zhan, CJ. Effect of acupuncture and moxibustion on post-stroke constipation: a network Meta-analysis. Zhongguo Zhen Jiu. (2020) 40:1011–6. doi: 10.13703/j.0255-2930.20190717-k0008
30. Liberati, A, Altman, DG, Tetzlaff, J, Mulrow, C, Gotzsche, PC, Ioannidis, JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate healthcare interventions: explanation and elaboration. BMJ. (2009) 339:b2700. doi: 10.1136/bmj.b2700
31. Wang, DS, SW, LL, Kong, WYW, and Cui, XM. Clinical observation on abdominal electroacupuncture for treatment of post-stroke constipation. Zhongguo Zhen Jiu. (2008) 1:7–9.
32. Liu, HF, Fengjun, S, and Ye, BH. Therapeutic observation of acupuncture at He-Sea and front-mu points for post-stroke constipation. Shanghai J Acupunct Moxib. (2016) 35:160–1.
33. Jiang, DW. Clinical observation of treating constipation after apoplex with abdominal electroacupuncture. [master’s thesis]. [Heilongjiang (China)]: Heilongjiang University of Traditional Chinese Medicine. (2013).
34. Jin, HG. Clinical observation on treatment of constipation after stroke with electric acupuncture combined with drug. [master’s thesis]. [Heilongjiang (China)]: Heilongjiang University of Traditional Chinese Medicine. (2015).
35. Li, CR. Clinical observations on the treatment of constipation after apoplexy with abdominal electroacupuncture. [master’s thesis]. [Heilongjiang (China)]: Heilongjiang University of Traditional Chinese Medicine. (2016).
36. Lu, L. Clinical observation of electroacupuncture at Tianshu (ST25) with deep needling for post-stroke constipation and its regulatory effects on SP, VIP in the blood-serum. [master’s thesis]. [Nanjing (China)]: Nanjing University of Traditional Chinese Medicine. (2017)
37. Peng, YJ, and Li, ZR. Clinical observation of deep needling at Tianshu (ST25) with Electroacupuncture for post-stroke constipation. Shanghai J Acupunct Moxib. (2016) 35:1181–3.
38. Yin, YX, Wang, YL, Zhang, KX, Zhang, SQ, Zhang, XL, Liu, WJ, et al. Therapeutic effect of electroacupuncture combined with bifidobacterium in the treatment of constipation after acute stroke. J Color Anal Surgery. (2015) 21:106.
39. Zhu, ZM. Clinical observation on abdominal electroacupuncture for treating deficiency constipation in post-stroke patients. [master’s thesis]. [Heilongjiang (China)]: Heilongjiang University of Traditional Chinese Medicine. (2012).
40. Chavez, LM, Huang, SS, MacDonald, I, Lin, JG, Lee, YC, and Chen, YH. Mechanisms of acupuncture therapy in ischemic stroke rehabilitation: a literature review of basic studies. Int J Mol Sci. (2017) 18:2270. doi: 10.3390/ijms18112270
41. Li, HY, Chen, Y, Hu, ZY, Chen, P, Li, RL, Jiang, JW, et al. Meta-analysis of acupuncture and moxibustion for the therapeutic effect on postoperative gastrointestinal dysfunction of gastric cancer. Zhongguo Zhen Jiu. (2022) 42:595–602. doi: 10.13703/j.0255-2930.20210214-0003
42. Wang, XY, Wang, H, Guan, YY, Cai, RL, and Shen, GM. Acupuncture for functional gastrointestinal disorders: a systematic review and meta-analysis. J Gastroenterol Hepatol. (2021) 36:3015–26. doi: 10.1111/jgh.15645
43. Zhu, X, Liu, Z, Qu, H, Niu, W, Gao, L, Wang, Y, et al. The effect and mechanism of electroacupuncture at LI11 and ST37 on constipation in a rat model. Acupunct Med. (2016) 34:194–200. doi: 10.1136/acupmed-2015-010897
44. Cui, MX, Sun, YP, Li, XF, Zhang, XP, Xu, XK, Gao, F, et al. Effect of electroacupuncture of “Tianshu”(ST25) at different frequencies on electromyography and immunoactivity of SP and VIP of colon in rats with slow transit constipation. Zhen Ci Yan Jiu. (2022) 47:710–4. doi: 10.13702/j.1000-0607.20210638
45. Liang, C, Wang, K, Xu, B, and Yu, Z. Electroacupuncture at acupoint ST 37(Shangjuxu) improves function of the enteric nervous system in a novel mouse constipation model. BMC Complement Altern Med. (2016) 16:392. doi: 10.1186/s12906-016-1377-5
46. Huang, X, Shen, Y, and Li, XH. Systematic review on the treatment of functional constipation with electroacupuncture and gastro-kinetic drugs. Zhen Ci Yan Jiu. (2020) 45:592–8. doi: 10.13702/j.1000-0607.180765
47. Sun, T, Wang, K, Li, L, Yan, M, Zou, L, Zhang, M, et al. Efficacy and safety of acupuncture in post-stroke constipation: a systematic review and meta-analysis. Front Neurosci. (2023) 17:1275452. doi: 10.3389/fnins.2023.1275452
48. Critchley, JA, Zhang, Y, Suthisisang, CC, Chan, TYK, and Tomlinson, B. Alternative therapies and medical science: designing clinical trials of alternative/complementary medicines--is evidence-based traditional Chinese medicine attainable? J Clin Pharmacol. (2000) 40:462–7. doi: 10.1177/00912700022009224
Keywords: stroke, constipation, electroacupuncture, rehabilitation, meta-analysis
Citation: Zhao X, Liu L, Diao Y and Ma C (2024) Effectiveness of abdominal electroacupuncture therapy for poststroke constipation: a meta-analysis. Front. Neurol. 15:1480681. doi: 10.3389/fneur.2024.1480681
Edited by:
Massimo Bellini, University of Pisa, ItalyCopyright © 2024 Zhao, Liu, Diao and Ma. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chunling Ma, eXhiYTIwQDE2My5jb20=
†These authors share first authorship