 Davide Cardile
Davide Cardile Viviana Lo Buono*
Viviana Lo Buono* Francesco Corallo
Francesco Corallo Simona Cammaroto
Simona Cammaroto Caterina FormicaAngelo QuartaroneRocco Salvatore Calabrò
Caterina FormicaAngelo QuartaroneRocco Salvatore Calabrò- IRCCS Centro Neurolesi Bonino-Pulejo, Messina, Italy
Introduction: Body awareness (BA) is the process of gaining sensory awareness based on the physiological states and actions of the body. It is influenced by an individual’s attitudes, perceptions, beliefs, and experiences within the social and cultural contexts. Following a stroke, impairments in BA are thought to be widespread and could have a significant impact on recovery results. Regaining body awareness, however, is often neglected in the neurorehabilitation field. This study aimed to assess body image perception in two stroke patients and the potential effect of motor and cognitive rehabilitative treatments on possible improvement of BA.
Methods: Patients were evaluated through a multidimensional neuropsychological assessment before and after a 3-month motor and cognitive rehabilitative training. Sessions were scheduled 6 times per week with a total duration of 3 h per session.
Results: After the neurorehabilitative treatment, both patients showed an improvement in BA, cognition, mood, and motor skills. Differences emerged related to the progression and improvement of their respective performances.
Discussion: The causes of these differences could include the following: different brain areas affected, the ischemic or hemorrhagic nature of the stroke, age, and sex. Further research is needed to better understand the differences and similarities in the correlations between deficit and lesional sites. Structured and early multidisciplinary intervention can certainly guarantee a better functional recovery for patients after a stroke. However, in this study we show how complementary assessment methods (such as human figure drawing) may be highly informative in choosing treatment modalities and verifying rehabilitation outcomes.
1 Introduction
Body awareness (BA) is closely related to proprioception and is the sense that allows us to perceive the position, movement, and actions of our body parts, even without relying on visual input (1, 2). BA is considered to be an interactive process that includes awareness of the physiological states of the body, processes including pain and emotion, and activities, such as movement. Although this construct is predominantly thought of as related to the physical area, it is shaped by individuals’ attitudes, perceptions, beliefs, and social/cultural context experiences (3, 4). It involves receptors in muscles, tendons, and joints that send signals to the brain, allowing one to sense one’s own position of body in space (5). BA is a basic dimension in the concept of the body (6) and it develops from body schema and body image (7). Body image refers to the mental representation of one’s own body, arising from all sources of sensory and cognitive information, whereas body schema describes the unconscious use of sensory information by the motor system to maintain body posture and produce accurate movements. BA is the conceptualization of body image, and its conceptual realization, which is predicated on our perception of our experiences of bodies and our assessment of the data we gather from various sensorial sources (8).
Indeed, BA can be seen as the transition from objective to subjective sensory physiology (9). It is the interface between physiological body perception (i.e., visual, tactile, olfactory, gustatory, auditory, or kinesthetic as well as visceral perception) and cognitive-affective processing in the nervous system (10). Therefore, for effective processing and integration of this sensory information, the sensory pathways from the body to the brain must be intact. BA also subtends a visual representation of the body that can be investigated through the graphic representation of one’s own body. This, combined with the integration of multisensory neural inputs, makes BA an essential aspect of embodied self-awareness (11–13). Adding to the complexity of this construct are the involvement of different anatomical sites and the presence of higher order cognitive processes that decode and modulate these sensory inputs (14). For this reason, among the most used assessment instruments in literature there are tests such as the Multidimensional Assessment of Interoceptive Awareness (MAIA), the Body Perception Questionnaire (BPQ), and the Body Awareness Questionnaire (BAQ), which multidimensionally evaluate BA assessing motor awareness/perception, and the level of consciousness related to one’s internal sensations (15–17).
Serrada et al. (18) in their longitudinal study sought to investigate whether and how BA changed over time in a sample of more than 100 stroke patients, and to do so, they considered both the administration of the MAIA with that of the body perception disturbance (BPD) (19). In doing so, they smartly combined proprioceptive and interoceptive BA measures. Interoception is the perception of internal states, such as hunger, thirst, heartbeat, and visceral sensations, and is crucial for maintaining homeostasis and emotional regulation (20, 21). On the other hand, proprioception refers to the sense of the position and movement of body parts in space, mediated by mechanoreceptors in muscles, tendons, and joints, and is essential for coordinated motor control and balance (5, 22). These two constructs can be affected concomitantly or independently when conditions that impair BA occur, including several neurological conditions such as traumatic or vascular brain injury (23). Numerous people experience impairments in sensation and perception after a stroke which interrupts the representation of the body that is held in the brain (24). Clinically BA can be presented with distorted perception or reduced awareness of parts of the body or an impaired ability to localize them, feelings of strangeness, and illusory feelings of movement (25). After stroke, BA alterations are often associated with syndromes arising because of parietal lobe lesions (26). BA alterations may arise after a lesion in the posterior parietal cortex including the medial area, i.e., the precuneus, and more specifically the antero-dorsal precuneus (27). However, the neuroanatomical basis influencing BA includes an integrated system of brain regions and functional networks and involves the thalamus, insula, and cerebellum (3). Contrary to the general idea that BA alterations are predominantly associated with neglect and right hemisphere damage, literature data do not provide evidence for such hemispheric lateralization (28). BA training is crucial in patients who have suffered a stroke because focusing on both physical and cognitive functions it can improve clinical status helping regain the sense of their body in space and enhances their ability to control movements. For these patients, being able to recognize the position and movement of their limb enhances proprioception and facilitates better control and coordination of movements, positively impacting on daily activities and overall mobility (29–31). By improving body awareness, patients are better able to relearn motor skills and adapt to new movement patterns, which is crucial for regaining independence in daily life activities after a stroke (32). The improvement in BA also enhances balance, spatial awareness, and orientation, reducing the risk of falls (33). In addition, emotional regulation, anxiety, frustration, and pain management resulting from post-stroke physical limitations improve, as the rehabilitation process causes patients to regain confidence about their abilities and movements (17, 34).
Several authors have shown that recovery of BA is possible if patients are treated with adequate rehabilitation interventions (35–37). The limited available literature shows that BA in stroke patients is rarely addressed through stimulation or rehabilitation of both motor and cognitive abilities. Additionally, treatment outcomes related to BA are often considered only from a “physical” perspective such as improvements in walking, balance, or the movement of specific body parts, rather than from a proprioceptive standpoint. This study aimed to assess body image perception in two stroke patients and the potential effect of motor and cognitive rehabilitation on possible improvement of BA.
2 Clinical cases
This study included two stroke patients with BA impairments who were assessed and admitted to a rehabilitative program within 3 months after stroke onset. After being verbally informed in the presence of caregivers and all professionals involved in the rehabilitation process, verbal and written consent was obtained from both patients to enter the study and to publish the results.
2.1 Patients
At baseline, patients underwent neurological and neuropsychological examinations that revealed alterations in BA with fluctuating interoceptive and/or proprioceptive impairments. Patients did not present agnosia and neglect measured by the behavioral inattention test, and psychiatric history. Both patients were enrolled for specific rehabilitation training once they were medically stable, and the diagnosis of stroke was confirmed through MR imaging.
Case 1: A 65-year-old male right-handed, with obesity and hypertension, was affected by an ischemic stroke, occurring approximately 3 months before our observation (July 2021). Medical history was negative for other clinical events (i.e., previous stroke or heart diseases). At the neurological examination, the patient showed moderate upper left limb motor impairments, with muscle weakness, loss of dexterous movement, and sensory loss involving the tactile and proprioceptive modalities. No visual changes were recorded (NIHSS 13; Rankin Scale 3). The magnetic resonance image (MRI) showed a T2-weighted hyperintense lesion involving the right fronto-temporal–parietal area (Figure 1). The neuropsychological assessment showed a global cognitive decline and deficit in executive functions, visual–spatial ability, attention, and memory (Table 1). The patient also presented with severe anxiety and moderate depression disorders. The human figure drawing (HFD) showed alteration in BA. Indeed, the patient had a disturbance of the body schema characterized by a loss of ability to localize, recognize, and identify specific body parts to verbal commands. Both human figures represented (see Figures 2A,B) appeared incomplete in their corporal general characteristics. In particular, in Figure 2A the drawing was positioned at the left end of the sheet, and this could even be indicative of the presence of depressive feelings or an emotional state of introversion and withdrawal (38–40). The graphic stroke was weak and discontinuous; the basic elements that make up the human figure, such as the face (eyes, nose, mouth, and ears), hair, hands, and feet, were missing. The absence of the left arm seems to recall the patient’s left hemiplegia. In Figure 2B, no elements recall the features of a female human figure except for some features that evoke hair. The two lower limbs and the right upper limb were present, but the left upper limb was absent. The graphic stroke was weak and inaccurate.

Figure 1. Diffusion images (a,b) show a signal restriction in the right middle cerebral artery territory with involvement of the frontal, parietal temporal, and ipsilateral capsular nucleus regions. The hyperintensity in T1 (c) shows that the ischemic event is in the late subacute phase, while the T1 image (d) shows the edematous condition and the reduced representa of the subarachnoid spaces as well as the imprint on the ipsilateral ventricle system and more so on the frontal horn. Coronal section (e) show the lesional areas.
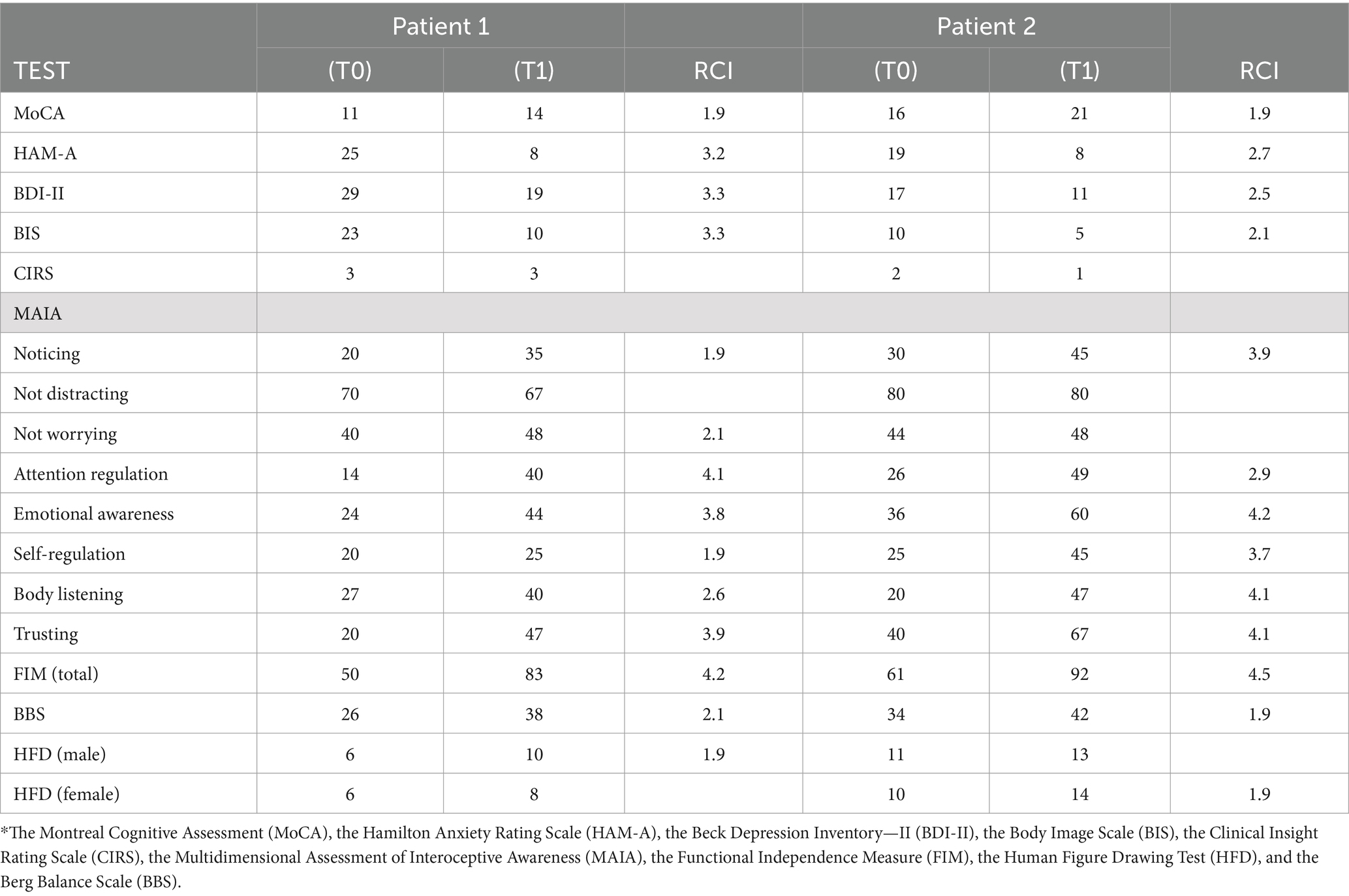
Table 1. Neuropsychological evaluation at admission to neurorehabilitative training (T0) and after 3 months (T1).
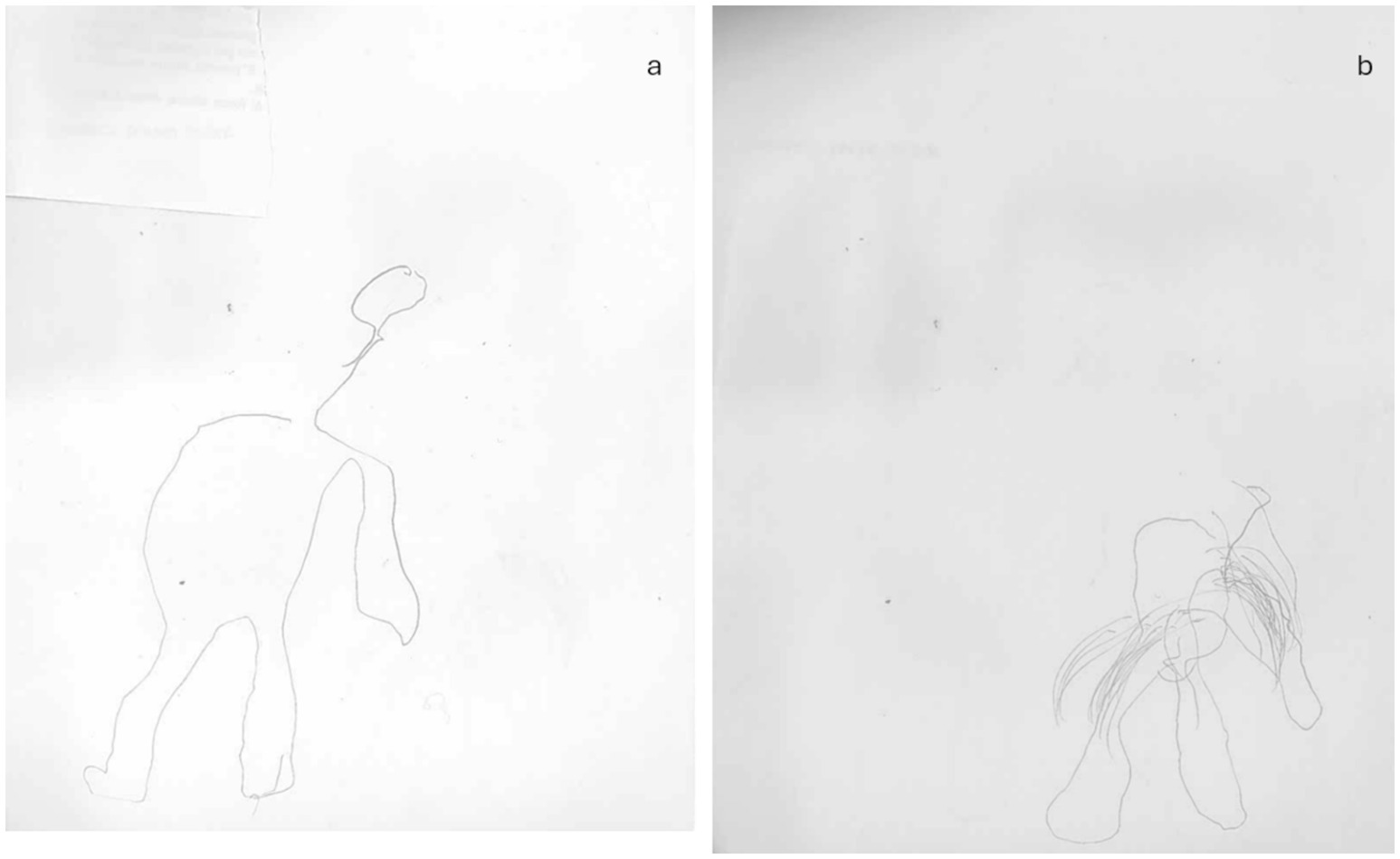
Figure 2. Graphical representation of the human figure of patient 1 at T0: (A) male representation; (B) female representation.
Case 2: A 55-year-old right-handed woman suffered a hemorrhagic stroke that occurred less than 3 months before our assessment (March 2022). The lesion involved the left side of the posterior inferior cerebellar artery (PICA) area. At the neurological examination, she presented with a postural deficit, ataxia during gait, and limb incoordination with moderate left hypoesthesia (NIHSS 15; Rankin Scale 3) (Figure 3). The patient reported vertigo. The neuropsychological evaluation revealed a poor global cognitive performance, with deficits in visuospatial planning, executive functions, and memory domains. No visual alterations were recorded. In the HFD, alterations in BA emerged (Figures 4A,B). The female representation (Figure 4A) had large dimensions and was represented in the center of the sheet. Although several details on the face were present, the absence of feet may indicate a sign of instability due to a lack of balance. The left side had a less fluid trait, probably related to the continuous sensations of dizziness referred by the patient. The male figure was abnormal in dimension (Figure 4B). The fact that his head and neck were wider than his lower body in the drawing could on the one hand reflect her difficulties in balance walking, but also be indicative of poor spatial planning. In addition, this patient reported important alterations in body perception referring to abnormal sensations of the left side of her body.
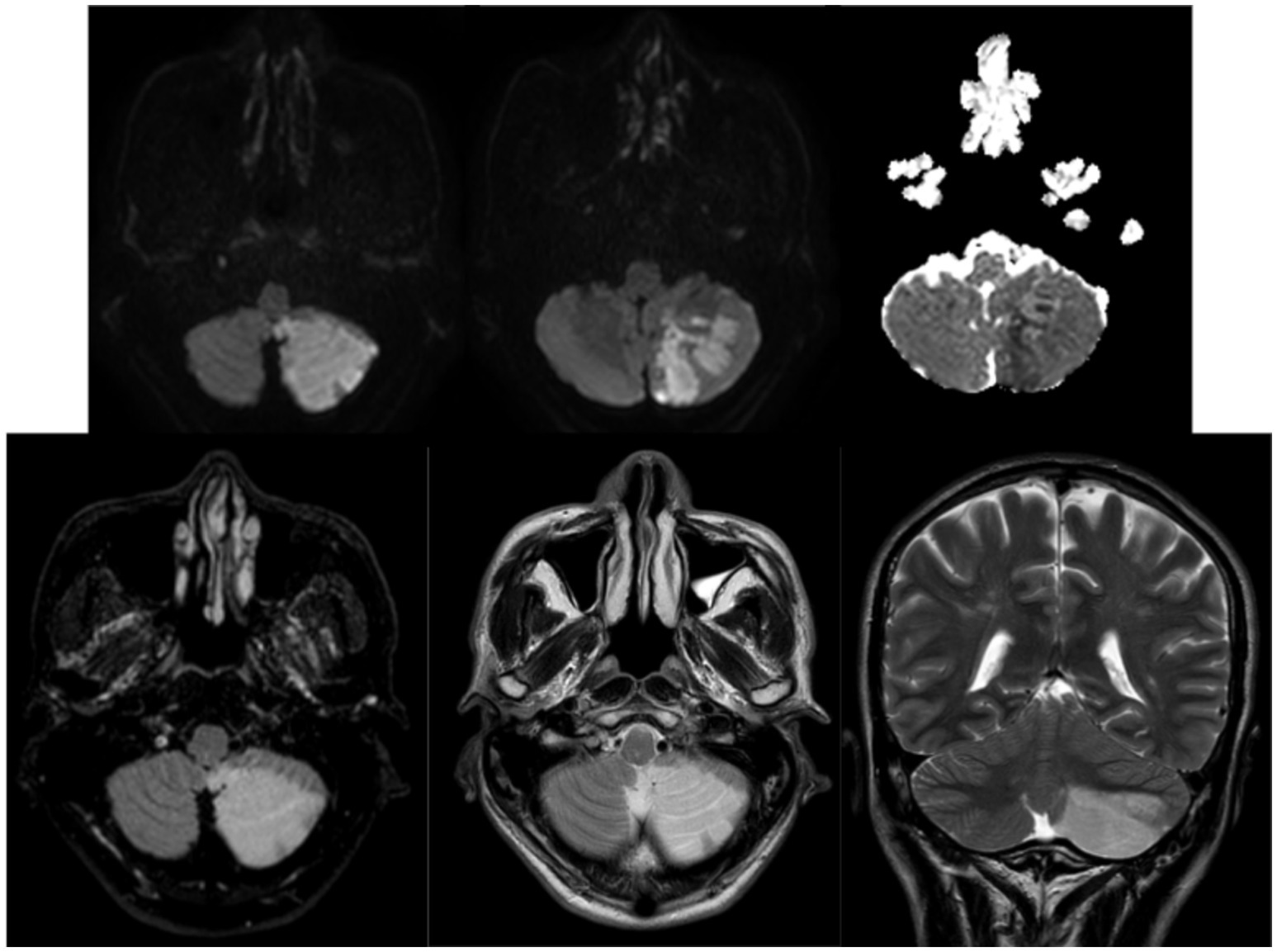
Figure 3. Case 2 MRI examination demonstrates the presence of an ischemic lesion in the left PICA area.
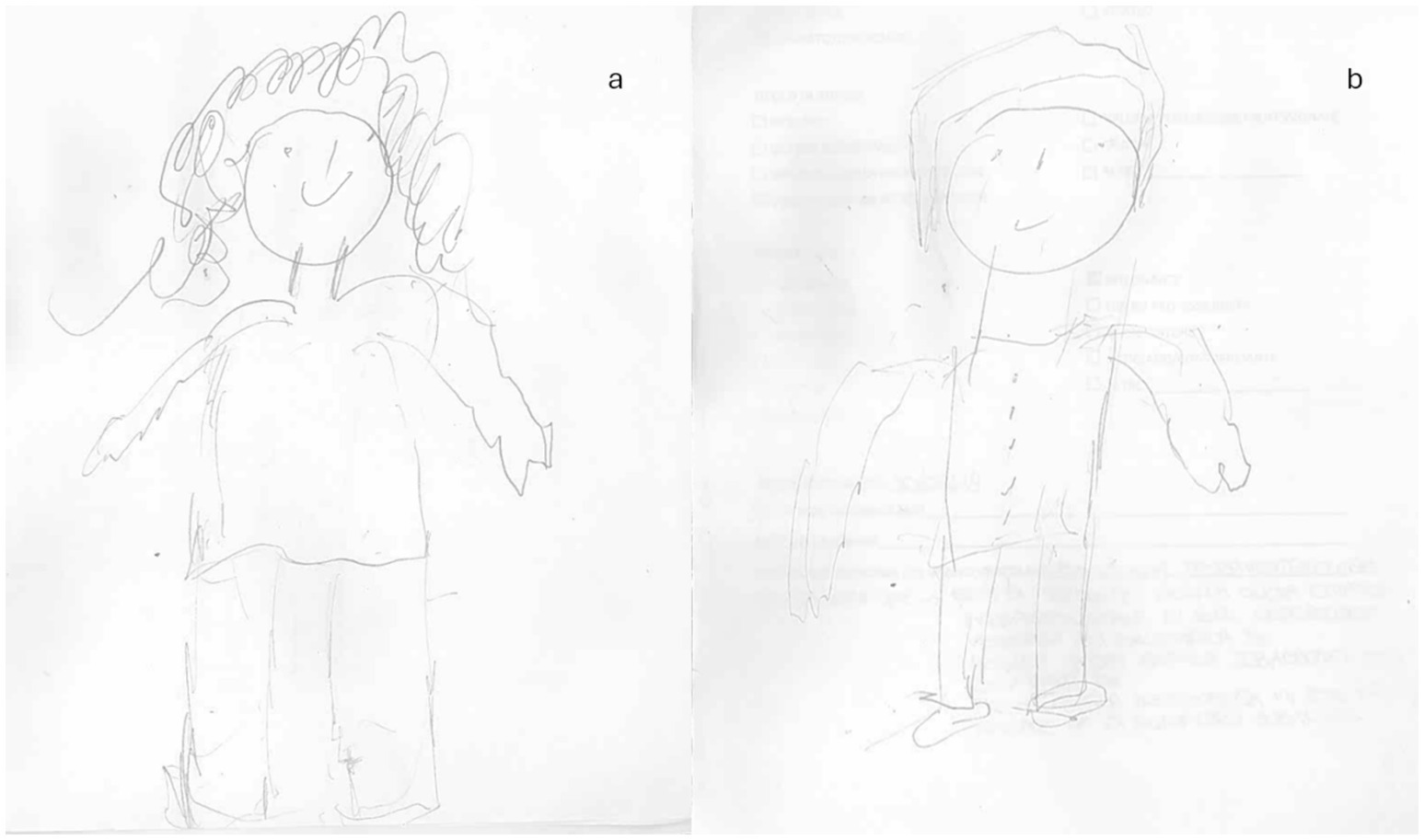
Figure 4. Graphical representation of the human figure of patient 2 at baseline T0: (A) female representation; (B) male representation.
2.2 Assessment and outcome measures
Given the importance of the early assessment of motor performance and cognitive functioning to develop an appropriate early rehabilitation program to maximize recovery, both patients were evaluated at admission to neurorehabilitation training (T0). After 3 months, a second evaluation was performed at the end of rehabilitative training (T1). To assess the actual significance of the improvements achieved by the patient (between T0 and T1) in all tests included in the neuropsychological assessment, we used the Reliable Change Index (RCI).
RCI is a standardized score used to determine whether a change in an individual (or group) performance is statistically significant based on the test–retest reliability of the measurement. RCI is calculated by dividing the change in the score of an individual by the standard error of the difference for the test being used. The cutoff value for statistical significance within the RCI is ≥1.96 (1.96 equates to the 95% confidence interval) (41).
The neuropsychological assessment included the administration of the following tests: the Montreal Cognitive Assessment (MoCA), the Beck Depression Inventory-II (BDI-II), the Hamilton Rating Scale for Anxiety (HAM-A), the Clinical Insight Rating Scale (CIRS), the Multidimensional Assessment of Interoceptive Awareness (MAIA), the Body Image Scale (BIS), the Human Figure Drawing Test (HFD), the Functional Independence Measure (FIM), and the Berg Balance Scale (BBS). The MoCA is a screening tool that evaluates several cognitive domains: attention and concentration, executive functions, memory, language, visuoconstructive skills, abstraction, computation, and orientation (42). The administration time is approximately 10 min and scores range from 0 to 30, with a score of 26 and above generally considered normal. BDI-II is a 21 multiple-choice item questionnaire used to measure the severity of depression in adults and adolescents at least 13 years old (43). HAM-A is a 14-item rating scale developed to measure the severity of anxiety symptoms. The test duration is short (10–15 min), and the total score goes from 0 to 56 allowing to discriminate between mild, moderate, and severe anxiety (44). CIRS is a standardized tool for evaluating awareness levels of cognitive and functional impairments and disease progression (45). MAIA is a tool that measures interoceptive awareness, the perception of sensation from inside the body including noticing, distracting, worrying, attention regulation, emotional awareness, self-regulation, body listening, and trusting (46). BIS is a 10-item Likert-scale questionnaire to assess body image concerns and changes over time (47). HFD is a test developed to evaluate the level of body awareness and that allows one to obtain a qualitative score about emotional status, personality traits, and the relationship between their body image perceived and self. Quantitative scoring was also performed according to other similar studies to compare pre-post performances (48). During the test, the patient is provided with a pencil and a blank sheet of paper, and he or she is required to draw a human figure. Subsequently, the patient must draw another human figure of the opposite sex of the first—scores obtainable range from 0 to 29 with lower scores indicating worse body perception (49). The Functional Independence Measure (FIM) scale was used to assess physical and cognitive disability (50). The scale includes 18 items, of which 13 items are physical domains and 5 items are cognition items. Each item is scored from 1 to 7 based on the level of independence, where 1 represents total dependence and 7 indicates complete independence. FIM total score can range from a minimum of 0 to a maximum of 126. The Berg Balance Scale (51) is a scale composed of 14 items of rapid administration (15 min) that aims to assess daily life movements such as the abilities to maintain and change positions, make movements with increasing speed, and perform tasks in unstable positions. Based on skill grades, each item is given a score from 0 to 4, where 0 is the minimum score and 4 is the maximum score. Summing the score obtained for all items gives a total score that will indicate the person’s state of mobilization: from 0 to 20, wheelchair; from 21 to 40, walks with assistance; and from 42 to 56, independent walking.
2.3 Rehabilitative program
Neurorehabilitative training was provided six times per week, and it included both motor and cognitive training. For both patients, motor training was performed by the same physiotherapist who is experienced and trained in the provision of physical therapy in patients with acquired brain injury. Motor training involved a series of exercises that targeted the learning of strategies to improve balance, coordination, flexibility, overall proprioceptive orientation, and gait training to improve mobility (52, 53). The sessions were aimed at sensorimotor skills relevant to basic daily functions, such as getting up from lying, sitting, rolling, and turning (54). Specifically, the following rehabilitation plan was established:
• Physical therapy with early mobilization of patients that included passive range-of-motion exercises to prevent joint stiffness and gradually progress to active-assisted and active exercises as the patients have gained strength.
• Proprioceptive training with weight-bearing exercises (standing, shifting weight from one leg to another) and balance exercises using a balance board and tandem walking.
• Strength and coordination exercises that required functional tasks such as reaching, grasping, and manipulating objects, and resistance training to improve muscle strength and endurance.
The cognitive training was delivered by an expert neuropsychologist who designed it as a combination of direct training of the impaired functions and metacognitive training to facilitate the development of compensatory strategies; it was based on cognitive and motivational techniques. The rehabilitative program was organized according to a predefined scheme. Attention training with exercises to improve focused, sustained, and divided attention; Memory exercises with tasks to enhance working memory, such as remembering and performing sequences of movements; executive function training including problem-solving tasks and planning activities that involve body movements; Motor imagery with the guided mental practice of movements to enhance motor planning and awareness.
Every day rehabilitative program was organized according to a predefined scheme: motor exercises (120 min) and cognitive exercises (60 min). The rehabilitation program lasted 12 weeks. Throughout the rehabilitation program, the difficulty of exercise progressively increased, ensuring a gradual advancement in both motor and cognitive abilities (Table 2). This structured approach remained consistent throughout the training period, with the complexity of tasks steadily rising over time.
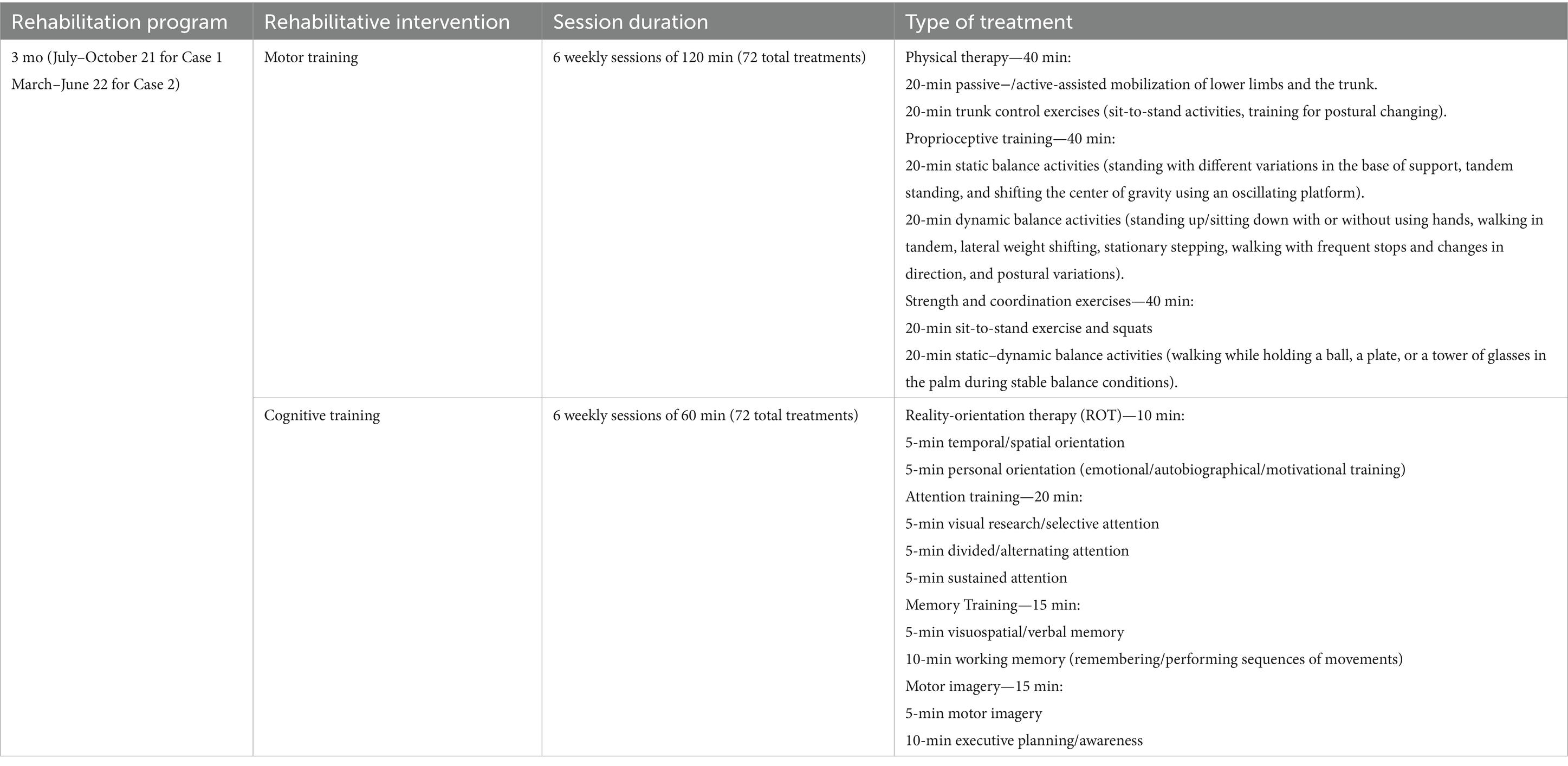
Table 2. Rehabilitation program description with cognitive and motor tasks.
3 Results
After the neurorehabilitative treatments, both patients improved in BA, cognition, mood, and motor skills (Table 1).
In particular, at T1 concerning BA, the analysis of human figures (see Figures 5A,B) of patient 1 showed a better representation of all body elements with an overall increase in performance between 6.9 and 13.8%. Although in the drawing, it was still missing the left arm, it shows more harmonious proportions between the different parts of the body. The graphic stroke appears more careful and precise (shading of the hair). Cognitively, the score at MOCA increased at T1 (Table 1), while emotionally, the scores markedly decreased at both HAM-A (8) and BDI-II (19).
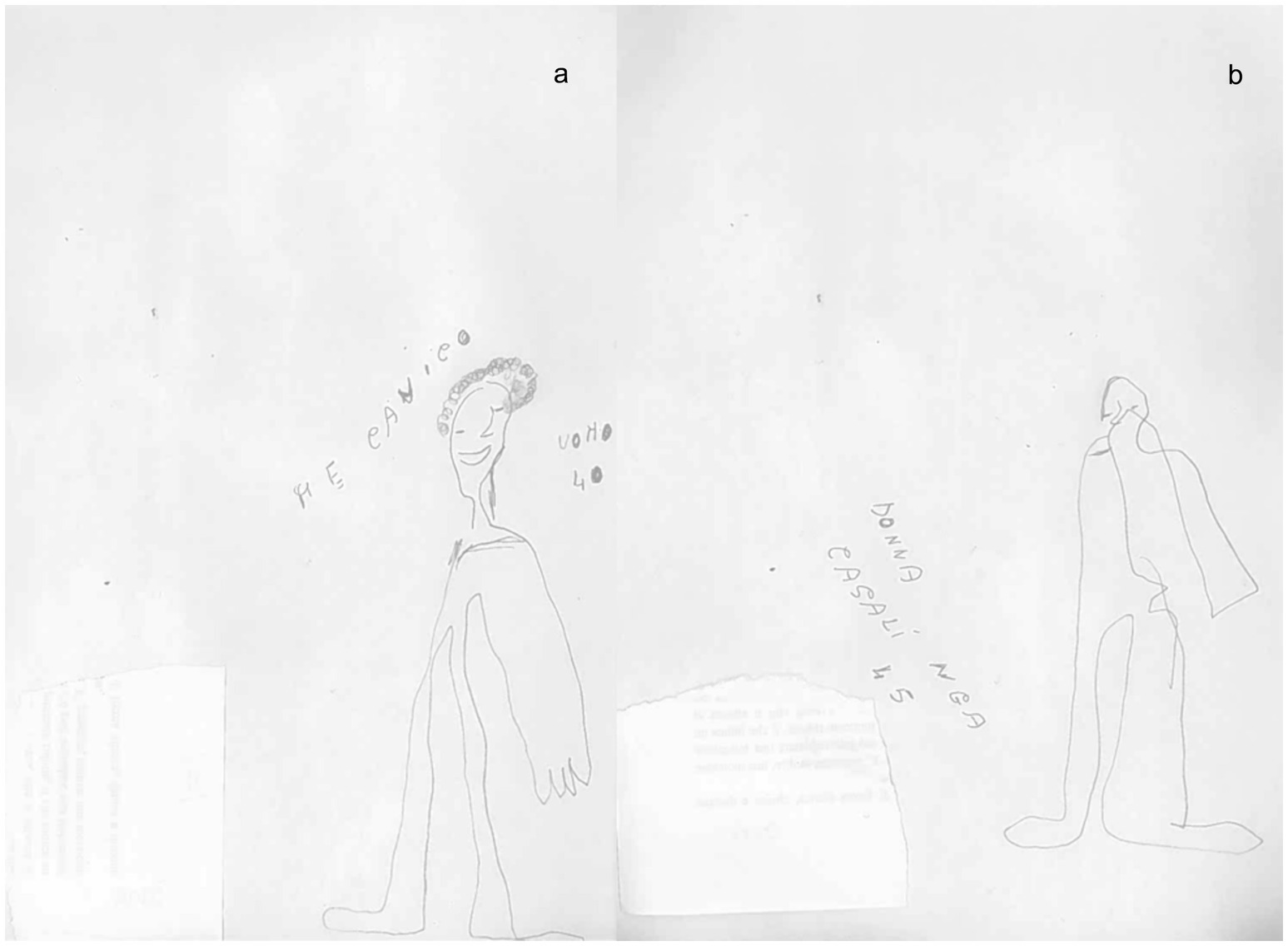
Figure 5. Graphical representation of the human figure of patient 1 after rehabilitative training T1: (A) male representation; (B) female representation.
In addition to this improvement, also balance and autonomy improved, as revealed by scores recorded at the BBS and FIM. The MAIA test showed better performance (between 13 and 27% more), especially in the areas of noticing, attention regulation, emotional awareness, body listening, and trusting.
After neurorehabilitative training, patient 2 improved in BA with an overall increase in performance between 6.9 and 13.8%. At T1 (see Figures 6A,B), the dimensions of both figures were improved. The female figure was represented by more details concerning the male representation. This could indicate a clear sex identification of the patient. Although she started with higher scores on average, even in the second patient there was an increase in the score on the MoCA at T1. Moreover, there was a notable decrease in scores on both the HAM-A (8) and the BDI-II (11). Balance and autonomy scores improved, and the MAIA test revealed greater enhancements in the same areas as patient 1, with a performance between 23 and 27% better. In particular, also self-regulation showed an important increase (20%).
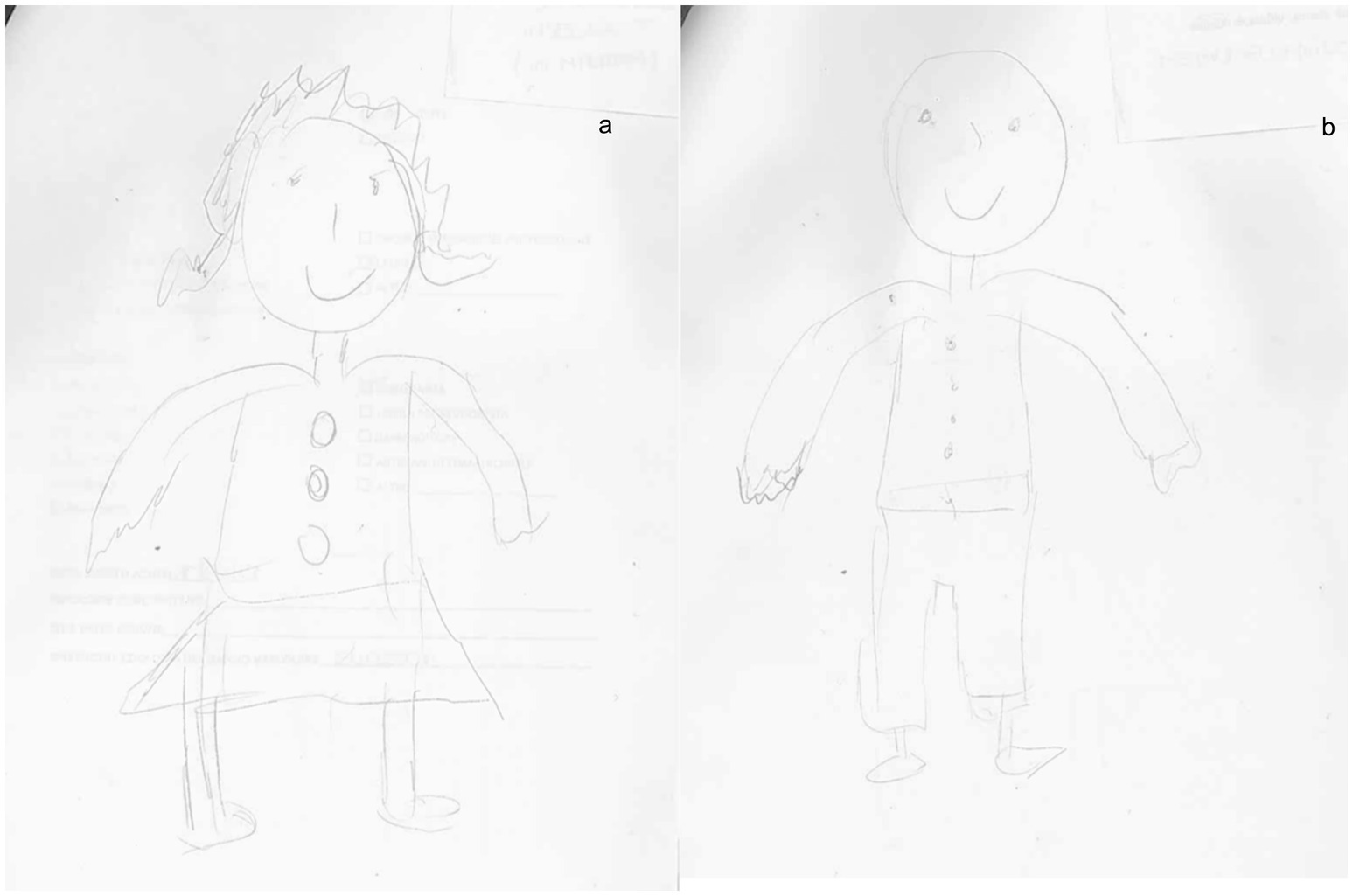
Figure 6. Graphical representation of the human figure of patient 2 at T1: (A) female representation; (B) male representation.
4 Discussion
This study sought to investigate body image perception in two stroke patients and the potential effect of motor and cognitive rehabilitative treatments in improving BA and functional deficits after stroke. Both patients involved in this study had similar issues related to BA with fluctuating interoceptive and/or proprioceptive impairments, although such alterations were caused by a completely different site of the lesion. The first patient presented a brain lesion in the right front-parietal–temporal area while the second one in the left side of the PICA. In line with other studies in literature, we found that motor and cognitive improvement was correlated with improvement in BA scores. Battesha et al. (55) and Sengar et al. (56) indeed treated stroke patients with treatments that considered both motor and cognitive aspects. In the former case (55), patients received physical rehabilitation in addition to maze control training. Specifically, patients were standing on a platform that had a motion, and they were asked to follow a set of targets through a maze. The participant moved a cursor to each target as it blinked and did not let the cursor touch a wall of the maze. On the other hand, in Sengar et al. (56) patients received dual-task balance training with postural (step forward, backward, and sideways) and cognitive tasks (remembering words and counting forward and backward by adding 3 to the digits). Both studies treated patients with middle cerebral artery stroke and found that combined (motor and cognitive) treatment improved physical awareness of limb or body part proprioception/position, balance, and autonomy. In this regard, Perfetti in his neurocognitive rehabilitation theory argues that the learning (or re-learning) of interaction patterns with their surroundings activates cognitive processes that produce sensory–motor recovery (57, 58). Salles et al. (59) relying on this theory, proposed an interesting cognitive therapeutic protocol that considered an individual’s motor, sensory, and cognitive characteristics using both kinesthetic and tactile tasks.
Although our results have been reflected by those in literature, to the best of our knowledge, this is the first study where the level of BA is not only assessed by motor and neuropsychological parameters but also by using HFD, a test that provides information about the patient’s representation and awareness of his/her body. The details in drawings, indeed, offer insights into BA and cognitive status (60, 61), with a particular focus on visuospatial and constructive impairments (62). In addition, drawing can serve as a qualitative tool to investigate also emotional status and mood disorders, it can be particularly suitable for assessing BA after a stroke. After the neurorehabilitation training, both patients presented a better graphical representation of themselves. Specifically, concerning HFD we observed more details and a better-defined trait in the human figure, especially about the figures of case 2 (Figure 6). In case 1, at T1, we observed little improvement in cognitive functions, and in details of HFD; however, the left upper limb remains unrepresented in all drawings (Figure 5). It is possible that the difficulty of hemiplegic upper limb recovery was related to a deficit in recognition of this part of the body in HFD. In addition to the improvement in balance and autonomy, the patient was more able to sustain and control attention to body sensations consciously. This would suggest that the rehabilitation training has produced cascading effects not only on the patient’s attention but also on the patient’s cognitive, emotional, and functional aspects. On the other hand, in case 2, we not only observed a greater improvement in cognitive domains and BA (Figure 6) but also a better ability to regulate anxiety and distress by paying mindful attention to bodily sensations. This led patient 2 to experience her body as more secure and trustworthy, which positively reinforced her attempts at attentional focus on body districts and sensations. Chiaramonte et al. (63) in one of their studies focused on patients’ characteristics and improvement to combined traditional rehabilitation exercises with goal-oriented proprioceptive exercises to improve not only motor performance but also representation of the body and its movements in space.
In case 1, lesions involved the parietal lobe and it is well known that this area has an important role in the function and processing of sensory information, understanding spatial orientation, and BA (64). In case 2 strokes hit cerebellar areas. Although BA deficits are most often associated with right parietal and temporo-parietal lesions, they may sometimes occur in association with lesions of the cerebellum and brainstem (65–67). Cerebellar damage frequently gives rise to a diverse range of cognitive dysfunctions, via the cerebrocerebellar loop; however, cerebellar networks are endowed with great plastic potential supporting a variety of learning mechanisms (68). This plasticity in the corticocerebellar system emphasizes the therapeutic potential of the cerebellar system for the enhancement of stroke recovery (69).
The ability to continuously observe, update, and provide input regarding one’s body’s position and movement in space is what makes BA so important. Accurate bodily information is crucial for the exact control of motions as it is the primary process utilized to integrate information for perception, decision-making, and action (24).
It is crucial to remember that the BA receives input from both external and internal senses. Gomez-Andres et al. (70) used auditory feedback-based rehabilitation via real-time provided to the patient supplementary information about his/her body position. While walking, alterations in frequency spectra of footstep sounds were induced via a system that selectively amplifies and equalizes the signal to generate distorted auditory feedback in the presence of an error. Their results show that feedback increased movement, coordination, and BA.
The limbic system provides affective and memory input related to body image, while the language and spatial portions of the parietal lobes in each hemisphere provide input related to semantic and lexical features. The ability of the person to maintain motor function and recuperate after a stroke is greatly aided by their intact BA, and this is what makes assessment and rehabilitation so important (71). However, after a stroke, many people report deficits in sensation and perception, which disrupts the representation of the brain of the body and significantly affects a person’s BA (72). Inaccurate perception of the body is caused by changed motor and sensory cortical processing, and it makes it more difficult to move with accuracy and control as it affects postural control, dynamic balance, coordination, and the person’s capacity to safely explore their immediate surroundings. It thus impacts one’s functional capacities, ability to carry out everyday tasks, and quality of life (73). Depending on the type of injury, rehabilitation can take a considerable amount of time (74, 75). Additionally, fluctuating or persistent alterations in neurocognitive performance make rehabilitation particularly challenging. As BA is often impaired in stroke patients and not always recovers spontaneously, neurorehabilitation is necessary to elicit and sustain it (76). Moreover, the length of rehabilitation and the destination of discharge are frequently hampered by decreased BA. Structured and early multidisciplinary intervention can certainly guarantee a better functional recovery for patients after a stroke. However, in this study we show how complementary assessment methods (such as HFD) can also be highly informative in choosing treatment modalities and verifying rehabilitation outcomes.
Unfortunately, we cannot draw important conclusions from our study (although the RCI was high for many items concerning BA and cognition outcomes), as it is based only on two case reports that have different etiology, and what is more, the lack of an adequate follow up prevents us to state to what extent the post-training effect lasts. However, BA deficit is poorly investigated in literature, and this overlooked problem may seriously affect post-stroke functional recovery and then deserve future investigation.
5 Conclusion
With this study, we showed the relationship between BA training and motor and neuropsychological rehabilitative outcomes and that the same type of treatment could be applied with positive results in patients with BA due to different brain lesions (i.e., fronto-temporo-parietal and cerebellar). Further studies should better investigate the role of the cerebellum in body image and cognitive functions, trying to better understand the neurophysiological connection with the main brain areas subtending BA. Moreover, more specific tests as well as the drawing test should be validated as qualitative tools to provide useful information about body image representation in patients with stroke and to monitor the progress of the motor and cognitive rehabilitative treatments.
Data availability statement
The datasets presented in this article are not readily available because of ethical and privacy restrictions. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
DC: Conceptualization, Writing – original draft, Writing – review & editing. VLB: Writing – original draft, Writing – review & editing. FC: Conceptualization, Investigation, Visualization, Writing – review & editing. SC: Data curation, Software, Validation, Writing – review & editing. CF: Writing – review & editing. AQ: Supervision, Validation, Visualization, Writing – review & editing. RSC: Data curation, Supervision, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This research was supported by Current Research Funds 2024, Ministry of Health, Italy.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ahn, SN. Differences in body awareness and its effects on balance function and independence in activities of daily living for stroke. J Phys Ther Sci. (2018) 30:1386–9. doi: 10.1589/jpts.30.1386
2. Sarıçan, Y, Erdoğanoğlu, Y, and Pepe, M. The effect of body awareness on trunk control, affected upper extremity function, balance, fear of falling, functional level, and level of independence in patients with stroke. Top Stroke Rehabil. (2023) 30:681–90. doi: 10.1080/10749357.2023.2185995
3. Serrada, I, Hordacre, B, and Hillier, S. Recovery of body awareness after stroke: an observational study. Front Neurol. (2021) 12:745964. doi: 10.3389/fneur.2021.745964
4. Oz, M, and Ulger, O. Body awareness disturbances in patients with low back pain: a systematic review. Acta Neurol Belg. (2024). doi: 10.1007/s13760-024-02554-5
5. Proske, U, and Gandevia, SC. The proprioceptive senses: their roles in signaling body shape, body position and movement, and muscle force. Physiol Rev. (2012) 92:1651–97. doi: 10.1152/physrev.00048.2011
6. Corbetta, M, Kincade, MJ, Lewis, C, Snyder, AZ, and Sapir, A. Neural basis and recovery of spatial attention deficits in spatial neglect. Nat Neurosci. (2005) 8:1603–10. doi: 10.1038/nn1574
7. Sattin, D, Parma, C, Lunetta, C, Zulueta, A, Lanzone, J, Giani, L, et al. An overview of the body schema and body image: theoretical models, methodological settings and pitfalls for rehabilitation of persons with neurological disorders. Brain Sci. (2023) 13:1410. doi: 10.3390/brainsci13101410
8. Mayer, A, Kudar, K, Bretz, K, and Tihanyi, J. Body schema and body awareness of amputees. Prosthetics Orthot Int. (2008) 32:363–82. doi: 10.1080/03093640802024971
9. Posner, MI, Walker, JA, Friedrich, FJ, and Rafal, RD. Effects of parietal injury on covert orienting of attention. J Neurosci. (1984) 4:1863–74. doi: 10.1523/JNEUROSCI.04-07-01863.1984
10. Mesulam, MM. Spatial attention and neglect: parietal, frontal and cingulate contributions to the mental representation and attentional targeting of salient extrapersonal events. Philos Trans R Soc Lond B Biol Sci. (1999) 354:1325–46. doi: 10.1098/rstb.1999.0482
11. Guidetti, S, Asaba, E, and Tham, K. The lived experience of recapturing self-care. Am J Occup Ther. (2007) 61:303–10. doi: 10.5014/ajot.61.3.303
12. Lindvall, MA, Anderzén Carlsson, A, and Forsberg, A. Basic body awareness therapy for patients with stroke: experiences among participating patients and physiotherapists. J Bodyw Mov Ther. (2016) 20:83–9. doi: 10.1016/j.jbmt.2015.06.004
13. Mehling, WE, Wrubel, J, Daubenmier, JJ, Price, CJ, Kerr, CE, Silow, T, et al. Body awareness: a phenomenological inquiry into the common ground of mind-body therapies. Philos Ethics Humanit Med. (2011) 6:6. doi: 10.1186/1747-5341-6-6
14. Craig, AD. Interoception: the sense of the physiological condition of the body. Curr Opin Neurobiol. (2003) 13:500–5. doi: 10.1016/s0959-4388(03)00090-4
15. Shields, SA, Mallory, ME, and Simon, A. The body awareness questionnaire: reliability and validity. J Pers Assess. (1989) 53:802–15. doi: 10.1207/s15327752jpa5304_16
16. Cerritelli, F, Galli, M, Consorti, G, D’Alessandro, G, Kolacz, J, and Porges, SW. Body perception questionnaire--short form; Italian version (BPQ-I) [database record] APA PsycTests (2021).
17. Mehling, WE, Price, C, Daubenmier, JJ, Acree, M, Bartmess, E, and Stewart, A. The multidimensional assessment of interoceptive awareness (MAIA). PLoS One. (2012) 7:e48230. doi: 10.1371/journal.pone.0048230
18. Serrada, I, Fryer, C, Hordacre, B, and Hillier, S. Can body awareness training improve recovery following stroke: a study to assess feasibility and preliminary efficacy. Clin Rehabil. (2022) 36:650–9. doi: 10.1177/02692155221083492
19. Ten Brink, AF, Halicka, M, Vittersø, AD, Jones, HG, Stanton, TR, and Bultitude, JH. Validation of the Bath CRPS body perception disturbance scale. J Pain. (2021) 22:1371–84. doi: 10.1016/j.jpain.2021.04.007
20. Craig, AD. How do you feel? Interoception: the sense of the physiological condition of the body. Nat Rev Neurosci. (2002) 3:655–66. doi: 10.1038/nrn894
21. Khalsa, SS, Rudrauf, D, Feinstein, JS, and Tranel, D. Interoception and mental health: a roadmap. Biol Psychol. (2018) 133:1–3. doi: 10.1016/j.biopsycho.2018.01.012
22. Sherrington, CS. The integrative action of the nervous system. In Scientific and Medical Knowledge Production. Routledge (1906). p. 217–253.
23. Alawieh, A, Zhao, J, and Feng, W. Factors affecting post-stroke motor recovery: implications on neurotherapy after brain injury. Behav Brain Res. (2018) 340:94–101. doi: 10.1016/j.bbr.2016.08.029
24. Stott, H, Cramp, M, McClean, S, and Turton, A. ‘Somebody stuck me in a bag of sand’: lived experiences of the altered and uncomfortable body after stroke. Clin Rehabil. (2021) 35:1348–59. doi: 10.1177/02692155211000740
25. Pisella, L, Havé, L, and Rossetti, Y. Body awareness disorders: dissociations between body-related visual and somatosensory information. Brain. (2019) 142:2170–3. doi: 10.1093/brain/awz187
26. Roth, M. Disorders of the body image caused by lesions of the right parietal lobe. Brain. (1949) 72:89–111. doi: 10.1093/brain/72.1.89
27. Herbet, G, Lemaitre, AL, Moritz-Gasser, S, Cochereau, J, and Duffau, H. The antero-dorsal precuneal cortex supports specific aspects of bodily awareness. Brain. (2019) 142:2207–14. doi: 10.1093/brain/awz179
28. Kortte, K, and Hillis, AE. Recent advances in the understanding of neglect and anosognosia following right hemisphere stroke. Curr Neurol Neurosci Rep. (2009) 9:459–65. doi: 10.1007/s11910-009-0068-8
29. Carey, LM, Oke, LE, and Matyas, TA. Impaired limb position sense after stroke: a quantitative test for clinical use. Arch Phys Med Rehabil. (1996) 77:1271–8. doi: 10.1016/s0003-9993(96)90192-6
30. Johansson, BB. Current trends in stroke rehabilitation. A review with focus on brain plasticity. Acta Neurol Scand. (2010) 123:147–59. doi: 10.1111/j.1600-0404.2010.01417.x
31. Schmalzl, L, Crane-Godreau, MA, and Payne, P. Movement-based embodied contemplative practices: definitions and paradigms. Front Hum Neurosci. (2014) 8:205. doi: 10.3389/fnhum.2014.00205
32. Morone, G, Paolucci, S, and Iosa, M. The efficacy of balance training with the use of a robotic device in stroke patients: a randomized clinical trial. J Neuroeng Rehabil. (2017) 14:13. doi: 10.1186/s12984-017-0224-2
33. Dean, CM, and Shepherd, RB. Task-related training improves performance of seated reaching tasks after stroke: a randomized controlled trial. Stroke. (1997) 28:722–8. doi: 10.1161/01.str.28.4.722
34. Perrin, P, Perrin, C, Bene, MC, Nicolas, JP, and Wolf, JE. Improvement of postural control after vestibular rehabilitation. Neurophysiologie Clinique/Clinical Neurophysiology. (1997) 27:1–9.
35. Moore, MJ, Vancleef, K, Riddoch, MJ, Gillebert, CR, and Demeyere, N. Recovery of visuospatial neglect subtypes and relationship to functional outcome six months after stroke. Neurorehabil Neural Repair. (2021) 35:823–35. doi: 10.1177/15459683211032977
36. Demeyere, N, and Gillebert, CR. Ego- and allocentric visuospatial neglect: dissociations, prevalence, and laterality in acute stroke. Neuropsychology. (2019) 33:490–8. doi: 10.1037/neu0000527
37. Durfee, AZ, and Hillis, AE. Unilateral spatial neglect recovery poststroke. Stroke. (2023) 54:10–9. doi: 10.1161/STROKEAHA.122.041710
38. Deng, X, Mu, T, Wang, Y, and Xie, Y. The application of human figure drawing as a supplementary tool for depression screening. Front Psychol. (2022) 13:865206. doi: 10.3389/fpsyg.2022.865206
39. Corallo, F, Tarda, D, Coppola, V, Bonanno, L, Lo Buono, V, Palmeri, R, et al. The relationship between body image and emotional and cognitive impairment after brain damage: a preliminary study. Brain Behav. (2021) 11:e02181. doi: 10.1002/brb3.2181
40. Opalić, P. Human figure test in the research of psychopathological state of refugees and somatically traumatized. Srp Arh Celok Lek. (2005) 133:21–8. doi: 10.2298/sarh0502021o
41. Jacobson, NS, and Truax, P. Clinical significance: a statistical approach to defining meaningful change in psychotherapy research. J Consult Clin Psychol. (1991) 59:12–9. doi: 10.1037//0022-006X.59.1.12
42. Conti, S, Bonazzi, S, Laiacona, M, Masina, M, and Coralli, MV. Montreal cognitive assessment (MoCA)-Italian version: regression-based norms and equivalent scores. Neurol Sci. (2015) 36:209–14. doi: 10.1007/s10072-014-1921-3
43. Beck, AT, Ward, CH, Mendelson, M, Mock, J, and Erbaugh, J. An inventory for measuring depression. Arch Gen Psychiatry. (1961) 4:561–71. doi: 10.1001/archpsyc.1961.01710120031004
44. Hamilton, M. The assessment of anxiety states by rating. Br J Med Psychol. (1959) 32:50–5. doi: 10.1111/j.2044-8341.1959.tb00467.x
45. Tondelli, M, Galli, C, Vinceti, G, Fiondella, L, Salemme, S, Carbone, C, et al. Anosognosia in early- and late-onset dementia and its association with neuropsychiatric symptoms. Front Psych. (2021) 12:658934. doi: 10.3389/fpsyt.2021.658934
46. Mehling, WE, Acree, M, Stewart, A, Silas, J, and Jones, A. The multidimensional assessment of interoceptive awareness, version 2 (MAIA-2). PLoS One. (2018) 13:e0208034. doi: 10.1371/journal.pone.0208034
47. Cheli, S, Agostini, A, Herd-Smith, A, Caligiani, L, Martella, F, and Fioretto, L. (2016). Body Image Scale--Italian Version. Psicoterapia Cognitiva e Comportamentale.
48. Lo Buono, V, Corallo, F, Bonanno, L, Quartarone, A, De Cola, MC, and De Cola, MC. Body image and emotional status in patients with acquired brain injury. J Clin Med. (2023) 12:4070. doi: 10.3390/jcm12124070
49. Rubio, KB, and Van Deusen, J. Relation of perceptual and body image dysfunction to activities of daily living of persons after stroke. Am J Occup Ther. (1995) 49:551–9. doi: 10.5014/ajot.49.6.551
50. Hamilton, BB, Laughlin, JA, Fiedler, RC, and Granger, CV. Interrater reliability of the 7-level functional independence measure (FIM). Scandinavian journal of rehabilitation medicine (2020) 26:115–119.
51. Miranda-Cantellops, N, and Tiu, TK. Berg balance testing In: StatPearls [internet]. Treasure Island. FL: StatPearls Publishing (2023)
52. Bang, DH, and Cho, HS. Effect of body awareness training on balance and walking ability in chronic stroke patients: a randomized controlled trial. J Phys Ther Sci. (2016) 28:198–201. doi: 10.1589/jpts.2016.198
53. Lindvall, MA, and Forsberg, A. Body awareness therapy in persons with stroke: a pilot randomized controlled trial. Clin Rehabil. (2014) 28:1180–8. doi: 10.1177/0269215514527994
54. Batson, G, and Deutsch, JE. Effects of Feldenkrais awareness through movement on balance in adults with chronic neurological deficits following stroke: a preliminary study. Complement Health Pract Rev. (2005) 10:203–10. doi: 10.1177/1533210105285516
55. Battesha, HHM, Wadee, AN, Shafeek, MM, Tawfick, AM, and Ibrahim, HM. Maze control training on kinesthetic awareness in patients with stroke: a randomized controlled trial. Rehabil Res Pract. (2022) 2022:5063492–7. doi: 10.1155/2022/5063492
56. Sengar, S, Raghav, D, Verma, M, Alghadir, AH, and Iqbal, A. Efficacy of dual-task training with two different priorities instructional sets on gait parameters in patients with chronic stroke. Neuropsychiatr Dis Treat. (2019) 15:2959–69. doi: 10.2147/NDT.S197632
57. Perfetti, C. El ejercicio terapéutico cognoscitivo para la reeducación motora del hemipléjico adulto. Barcelona: Edikamed (1999).
58. Rodríguez-Larrad, A, Rizzello, C, and Perfetti, C. Ejercicio terapéutico cognoscitivo In: R Cano-de-la-Cuerda and S Collado Vázquez, editors. Neurorehabilitación: Métodos específicos de valoración y tratamiento. Madrid, Spain: Médica Panamericana (2012). 307–21.
59. Sallés, L, Martín-Casas, P, Gironès, X, Durà, MJ, Lafuente, JV, and Perfetti, C. A neurocognitive approach for recovering upper extremity movement following subacute stroke: a randomized controlled pilot study. J Phys Ther Sci. (2017) 29:665–72. doi: 10.1589/jpts.29.665
60. Skybo, T, Ryan-Wenger, N, and Su, YH. Human figure drawings as a measure of children's emotional status: critical review for practice. J Pediatr Nurs. (2007) 22:15–28. doi: 10.1016/j.pedn.2006.05.006
61. Abell, SC, Heiberger, AM, and Johnson, JE. Cognitive evaluations of young adults by means of human figure drawings: an empirical investigation of two methods. J Clin Psychol. (1994) 50:900–5. doi: 10.1002/1097-4679(199411)50:6<900::aid-jclp2270500614>3.0.co;2-3
62. Thurm, BE, Pereira, ES, Fonseca, CC, de Siqueira Cagno, MJ, and Gama, EF. Neuroanatomical aspects of the body awareness. J Morphol Sci. 28:(2011).
63. Chiaramonte, R, D'Amico, S, Caramma, S, Grasso, G, Pirrone, S, Ronsisvalle, MG, et al. The effectiveness of goal-oriented dual task proprioceptive training in subacute stroke: a retrospective observational study. Ann Rehabil Med. (2024) 48:31–41. doi: 10.5535/arm.23086
64. Nawrot, M, and Rizzo, M. Motion perception deficits from midline cerebellar lesions in humans. Vis Res. (1995) 35:723–31. doi: 10.1016/0042-6989(94)00168-l
65. Benghanem, S, Mazeraud, A, Azabou, E, Chhor, V, Shinotsuka, CR, Claassen, J, et al. Brainstem dysfunction in critically ill patients. Crit Care. (2020) 24:5. doi: 10.1186/s13054-019-2718-9
66. Habib, SH, and Habib, SS. Auditory brainstem response: an overview of neurophysiological implications and clinical applications—a narrative review. J Pak Med Assoc. (2021) 71:2230–6. doi: 10.47391/JPMA.03-432
67. Burello, L, De Bartolo, P, Gelfo, F, Foti, F, Angelucci, F, and Petrosini, L. Functional recovery after cerebellar damage is related to GAP-43-mediated reactive responses of pre-cerebellar and deep cerebellar nuclei. Exp Neurol. (2012) 233:273–82. doi: 10.1016/j.expneurol.2011.10.016
68. Wessel, MJ, and Hummel, FC. Non-invasive cerebellar stimulation: a promising approach for stroke recovery? Cerebellum. (2018) 17:359–71. doi: 10.1007/s12311-017-0906-1
69. Olgiati, E, Maravita, A, Spandri, V, Casati, R, Ferraro, F, Tedesco, L, et al. Body schema and corporeal self-recognition in the alien hand syndrome. Neuropsychology. (2017) 31:575–84. doi: 10.1037/neu0000359
70. Gomez-Andres, A, Grau-Sánchez, J, Duarte, E, Rodriguez-Fornells, A, and Tajadura-Jiménez, A. Enriching footsteps sounds in gait rehabilitation in chronic stroke patients: a pilot study. Ann N Y Acad Sci. (2020) 1467:48–59. doi: 10.1111/nyas.14276
71. Bonanno, M, De Luca, R, Torregrossa, W, Tonin, P, and Calabrò, RS. Moving toward appropriate motor assessment tools in people affected by severe acquired brain injury: a scoping review with clinical advices. Healthcare (Basel, Switzerland). (2022) 10:1115. doi: 10.3390/healthcare10061115
72. Carey, LM, Matyas, TA, and Baum, C. Effects of somatosensory impairment on participation after stroke. Am J Occup Ther. (2018) 72:7203205100p1–7203205100p10. doi: 10.5014/ajot.2018.025114
73. Hazelton, C, Thomson, K, Todhunter-Brown, A, Campbell, P, Chung, CS, Dorris, L, et al. Interventions for perceptual disorders following stroke. Cochrane Database Syst Rev. (2022) 2022:CD007039. doi: 10.1002/14651858.CD007039.pub3
74. Ko, SB, and Yoon, BW. Mechanisms of functional recovery after stroke. Front Neurol Neurosci. (2013) 32:1–8. doi: 10.1159/000346405
75. De Luca, R, Bonanno, M, Vermiglio, G, Trombetta, G, Andidero, E, Caminiti, A, et al. Robotic Verticalization plus music therapy in chronic disorders of consciousness: promising results from a pilot study. Brain Sci. (2022) 12:1045. doi: 10.3390/brainsci12081045
Keywords: body awareness, body image, neurorehabilitation, stroke, cognition, mood
Citation: Cardile D, Lo Buono V, Corallo F, Cammaroto S, Formica C, Quartarone A and Calabrò RS (2024) The importance of recovering body awareness in post-stroke rehabilitation: insights from clinical case reports. Front. Neurol. 15:1467181. doi: 10.3389/fneur.2024.1467181
Edited by:
Victor W. Mark, University of Alabama at Birmingham, United StatesReviewed by:
Monika Zawadka-Kunikowska, Nicolaus Copernicus University in Toruń, PolandJena Blackwood, University of Minnesota Twin Cities, United States
Copyright © 2024 Cardile, Lo Buono, Corallo, Cammaroto, Formica, Quartarone and Calabrò. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Viviana Lo Buono, dml2aWFuYS5sb2J1b25vQGlyY2NzbWUuaXQ=