 Jing Zhao
Jing Zhao Shuangzi Li
Shuangzi Li Ni Zhang3*
Ni Zhang3*
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 14 August 2024
Sec. Epilepsy
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1459392
Objective: Epilepsy-related stigma is a global problem, yet there has been an inadequate focus on children and adolescents. The purpose of this study was to determine the status quo of stigma and its determinants among children and adolescents with epilepsy in China.
Methods: A multicenter cross-sectional study was conducted across nine hospitals in eight cities within six provinces in China from 10 October 2023 to 15 June 2024. Participants included patients aged 8 to 18 years with epilepsy and their caregivers. Felt stigma was assessed with the Kilifi Stigma Scale for Epilepsy (KSSE). Social support and self-efficacy were collected through the Social Support Rating Scale (SSRS) and the Generalized Self-Efficacy Scale (GSES). The data were analyzed using t-tests, analysis of variance (ANOVA), Spearman correlation analysis, and multiple linear regression analysis.
Results: The study enrolled 281 children and adolescents, with a mean age of 12.25 years (SD = 2.56), including 46.6% females. A total of 35.6% participants had self-reported felt stigma. The mean KSSE score is 9.58 (SD = 7.11). Meanwhile, stigma scores correlated strongly with reduced social support (r = −0.55, p < 0.01) and self-efficacy (r = −0.43, p < 0.01). Place of residence (rural vs. non-rural), academic performance (average and above vs. fair or poor), region (western region vs. non-western region), duration of epilepsy (≤5 years vs. >5 years), drug-resistant epilepsy (yes vs. no), comorbidities (yes vs. no), social support and self-efficacy are major influencing factors among the complex factors influencing the felt stigma among children and adolescents.
Conclusion: Medical staff should be more aware of stigma among children and adolescents with epilepsy, especially those who live in rural and western areas, have poor academic performance, have epilepsy duration of more than 5 years, have drug-resistant epilepsy, and have comorbidities, who are at higher risk of stigma. It is recommended that effective measures be taken to alleviate stigma by improving children and adolescents’ self-efficacy and providing more social support for them and their families.
Epilepsy is one of the most common neurological disorders that affects around 70 million people worldwide (1). Epilepsy has a high incidence in early childhood, with approximately 75% of epilepsy begins in childhood (2). It affects neurological, cognitive, psychological and social domains and accounts for more than 0.75% of the global burden of disease (3, 4). However, clinical indicators of epilepsy such as seizure frequency do not fully reflect the disease burden, the stigma can be more frustrating than the seizures themselves. The World Health Organization (WHO) has identified stigma as a significant contributor to poor physical and mental health in individuals with epilepsy (5). Epilepsy stigma can be conceptualized as both “felt” and “enacted.” “Enacted stigma” refers to the actual instances of discrimination based on the diagnosis of epilepsy; whereas “felt stigma” refers to the shame, embarrassment or disgrace associated with epilepsy or the fear of being discriminated against (6). Either form can strongly impact a child’s life. However, felt stigma may cause more personal anguish and unhappiness than enacted (5).
Epilepsy-related stigma is a global problem, especially in China (7). A survey of 20 Chinese cities found that 64.9% of adolescents and young adults with epilepsy, as well as 64.0% of parents or caregivers, chose not to disclose the condition to others, potentially indicating a stigma surrounding epilepsy (8). In a community-based survey, a third of people with epilepsy of all ages identified stigma as the most difficult part of living with epilepsy (9). In Uganda, the prevalence of high-perceived stigma among children and adolescents with epilepsy was 34.0% (10). Stigma can disrupt the psychosocial development in children with epilepsy, leading to increased anxiety, depression, and poor quality of life (11). Stigma and discrimination were found to impact negatively on healthcare, education, employment and income, which can have an economic impact (12).
Several factors have been identified as influencing the stigma associated with epilepsy, including gender, age, duration of epilepsy, seizure frequency, severity and type of epilepsy (13), place of residence (14), educational attainment (6), anti-seizure medication (ASMs) (15), self-efficacy and social support (16). In addition, a study in Bulgaria found that 43.6% of people with drug-resistant epilepsy felt stigmatized (17). Children with epilepsy experience poor academic performance and school dropout due to bullying, alienation and stigma (18). Social support is a protective factor of subjective well-being. Individuals with good social support usually have an increased sense of control, which helps them cope better with adversity (16). Previous research shows that stigma is negatively associated with self-efficacy among adult with epilepsy (19). Successful epilepsy management, which necessitates strong social support and self-efficacy, is essential for individuals to regain their roles in school and social life, thereby enhancing their overall well-being (19).
Successful integration of children and adolescents with epilepsy into school and society is important goal in epilepsy care (20). The ability to overcome stigma is important determinants of successful integration. Yet the effect of stigma and its associated factors on children and adolescents populations are poorly understood. Therefore, the aim of this study is to assess the extent of felt stigma and its associated factors to fill this research gap. Furthermore, interventions aimed at reducing stigma and improving subjective well-being can be developed based on these findings.
A multicenter cross-sectional survey was conducted in China, covering nine tertiary children’s and comprehensive hospitals in different regions of China from 10 October 2023 to 15 June 2024. The managers of the neurology units in the survey gave their consent before the survey. All patients who were receiving neurologic services in the neurology outpatient or inpatients comprised the study population. The inclusion criteria were as follows: (i) the children and adolescents ranged in age from 8–18 years and were diagnosed according to 2017 classification and terminology of the International League Against Epilepsy (ILAE) for 2 months or longer (21); (ii) caregivers older than 18 years who provided care for children and adolescents with epilepsy, only one of the caregivers who was present with the child during the period of data collection was included in the study; (iii) both child and caregiver were able to read and understand the questionnaire independently or with the help of the researcher; (iv) they provided informed consent and voluntarily participated in this study. Exclusion criteria are as follows: (i) children and adolescents with intellectual impairment, and IQ score lower than 80 on the Wechsler Intelligence Scale were identified via medical records and caregiver consultations; (ii) caregivers were diagnosed with severe medical conditions, cognitive impairment, or mental illness.
Using questionnaires, we collected general demographic data, including children’s gender, age, height, weight, academic performance (standardized test scores and class ranks, normalized by class size), basic family information (e.g., only child status), and region of residence (based the National Bureau of Statistics of China). Socioeconomic indicators such as guardian education level, household income level based on the 2022 National Bureau of Statistics, and medical insurance status were included. Notably, China’s medical insurance system includes both social and commercial insurance schemes. The actual coverage rate is over 80% for inpatient medical expenses for pediatric patients. We also assessed family upbringing styles: authoritative (high expectations, supportive, promoting independence), permissive (nurturing, lenient, with minimal control), neglectful (low engagement, guidance lacking), and autocratic (strict, demanding, with punitive measures).
Disease-related characteristics involved epilepsy duration, the number of antiseizure medication (ASMs) types taken, seizure type, whether or not the diagnosis was drug resistant epilepsy (DRE) by neurologists (referring to the ILAE definition of DRE as “inadequate response to two appropriately chosen and used ASMs schedules”) (22), and seizure frequency in recent 3 months. These were mainly collected by medical records and self-report of caregivers.
The Kilifi Stigma Scale for Epilepsy (KSSE) is a three-point Likert 15-item scoring scale (23), which was used to measure felt stigma. The Chinese version of KSSE were translated and validated by Song et al. (24). The translated version exhibits good reliability and validity (Cronbach’s α = 0.93). The KSSE has been extensively validated in children and adolescents populations and has demonstrated cultural relevance and sensitivity in China (25). The total score ranges from 0 to 30. A score above the 66th percentile on the total scale is indicative of felt stigma, whereas a score below this threshold shows the absence of stigma.
The Social Support Rating Scale (SSRS) was used to measure the degree of support received from friends, relatives, and healthcare providers, which was developed by a Chinese researcher (26). It comprises 10 items designed to evaluate objective support (3 items), subjective support (4 items), and utilization of support (3 items). Objective support reflects an individual’s social network, material direct support, and emotional support. Subjective support refers to the feeling of being respected, supported, and understood. Utilization of support reflects the respondents to seek and use the degree of social support. The scale had good predictive validity and internal consistency among Chinese population [Cronbach’s α = 0.82, (27)]. The overall score ranges from 12 to 66. Higher scores indicate stronger social support.
The Generalized Self-Efficacy Scale (GSES) is a psychometric tool used to measure the level of generalized self-efficacy, developed by Jerusalem and Schwartz in 1979 (28). Self-efficacy is an individual’s belief in their ability to successfully manage different life situations (29). The Chinese version of GSES were translated and validated by Wang et al. (30). GSES has been translated into more than 28 languages and demonstrated strong reliability and validity (Cronbach’s α = 0.88) (31). The items are rated on a four-point scale, and possible total scores range from 10 to 40, with lower scores indicating lower self-efficacy.
Participation in this study was completely voluntary and anonymous. Before completing the questionnaire, the researchers obtained informed consent from the participants and their caregivers. This study was approved by the Medical Ethical Committee of Children’s Hospital of Chongqing Medical University (No. 2023-370).
Prior training was provided to all researchers working in a clinical setting. The questionnaire was distributed to neurology outpatient or inpatients. The participants were recruited using a convenient sampling method. Given the sensitivity of the stigma issue, measures were taken to ensure data authenticity. The researchers collected the information through a face-to-face interview, by providing participants with consistent instructions, instructions for completing the questionnaire, and links to access the questionnaire. Researchers obtained their informed consent before completing the questionnaire. For children and adolescents, consent was obtained from the legal guardian. Participants were informed that all data would be presented in statistical form to ensure anonymity and confidentiality. At the end of the survey, the data were checked for validity and completeness. If the questionnaire was incomplete, the respondent was asked to complete the missing items immediately. A total of eight cities in six provinces were surveyed in China, including the eastern, central and western regions. The division of regions was provided by the National Bureau of Statistics of China website. Finally, 302 children and adolescents with epilepsy and caregivers were recruited and completed the survey. A total of 281 valid questionnaires were recovered, with a 93.0% valid return rate.
We used SPSS 26.0 to accomplish all the statistical analyses. Demographic data and disease-related characteristics were summarized as means (standard deviations) and as frequency counts (percentages) for categorical variables. Comparisons of KSSE scores with demographic and clinical variables were analyzed using independent t-tests or one-way analysis of variance (ANOVA). Post-hoc comparisons for significant variables were performed using the Bonferroni correction. Correlation between stigma scores, epilepsy duration, social support, and self-efficacy using Spearman correlation. Multiple linear regression analyses of statistically significant independent variables were performed to derive factors influencing stigma in children and adolescents with epilepsy. Academic performance was coded as dummy variables. The results are reported as unstandardized (B) and standardized (β) regression coefficients, and the R-squared was reported for each outcome variable. All tests were two-sided with a significance level of p < 0.05.
A total of 281 children and adolescents with epilepsy and their caregivers were included. All patients’ demographic characteristics have been presented in Table 1. The mean age of children and adolescents with epilepsy was 12.25 years (SD = 2.56). One hundred and thirty one (46.6%) of them were female, and 88 patients (31.3%) lived in rural areas. Most families (87.9%) have medical insurance. One hundred and thirteen patients (40.2%) had a monthly household income of more than 5, 000 yuan. Only 32 mothers (11.4%) had attended university or above, while nearly 19.2% of fathers had attended university or above. One hundred and thirty-seven (48.7%) had below average academic performance. Table 2 shows the disease-related characteristics of patients. The mean duration of epilepsy since diagnosis was 3.52 years (SD = 2.95), and 113 (40.2%) took more than one type of ASMs. 148 (52.7%) of seizure type had focal onset. 20.3% of patients reported were drug-resistant epilepsy. Focal onset seizures were reported in 148 (52.7%) patients, and 20.3% of patients were diagnosed with drug-resistant epilepsy. Seizure freedom during the recent 3 months was noted in 100 (35.6%) patients, and 143 patients (50.9%) reported had comorbidities.

Table 1. Demographic characteristics of study patients.
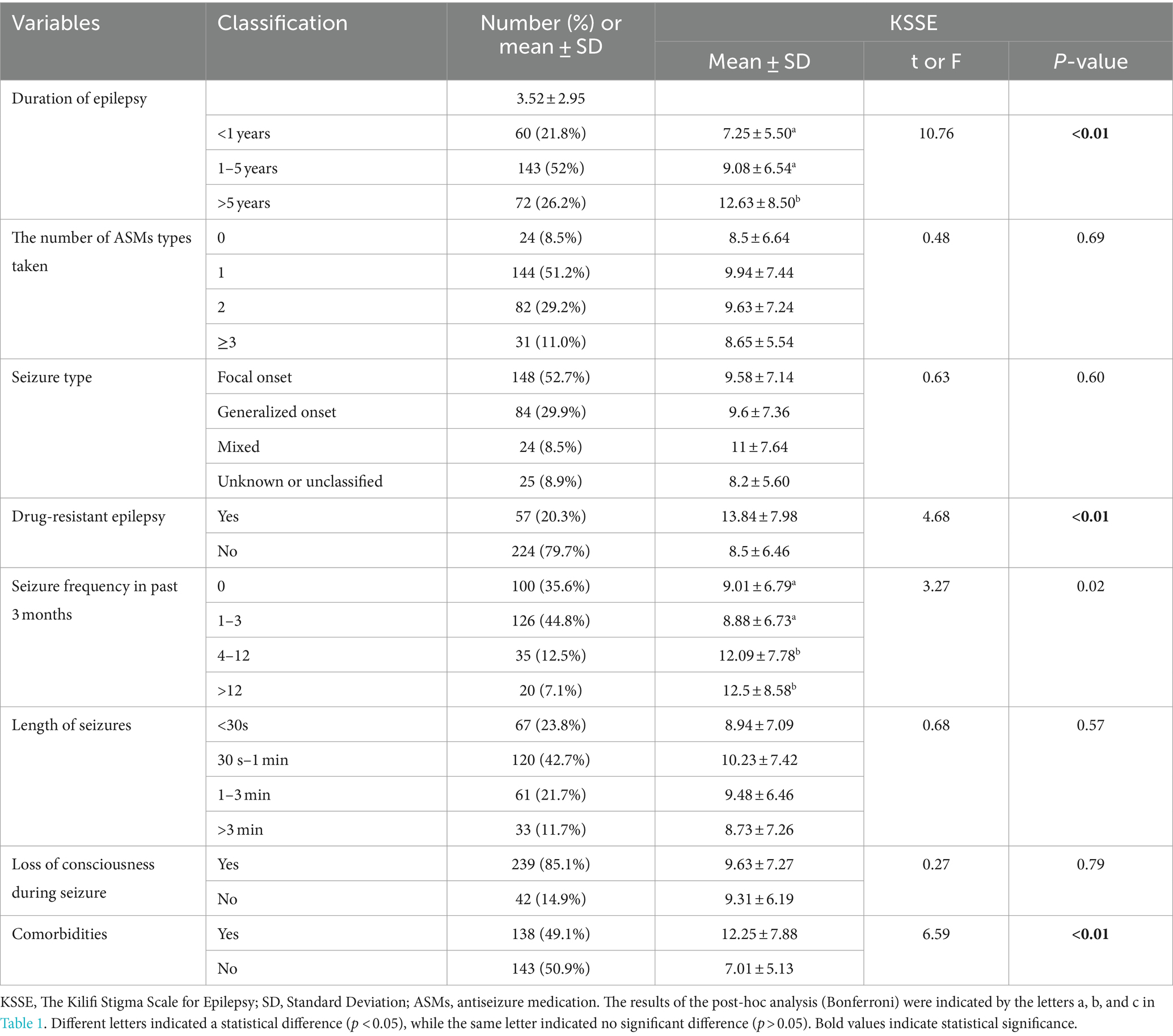
Table 2. Disease-related characteristics of study patients.
The mean KSSE score of 281 patients is 9.58 (SD = 7.11). Classification of the sample using the KSSE cut-off points revealed that 35.6% were at the threshold of feeling stigmatized. Through analysis, place of residence, monthly household income, difficulty of paying medical expenses, degree of mother’s and father’s education, children’s academic performance, family residence region, duration of epilepsy, drug-resistant epilepsy, seizure frequency in past 3 months, comorbidities have statistical significance (p < 0.05) with the stigma of children and adolescents in China, whereas different ages, gender, household type and the seizure type display no significant differences (p > 0.05). Details of post-hoc pairwise comparisons are shown in Tables 1, 2 and Figure 1.
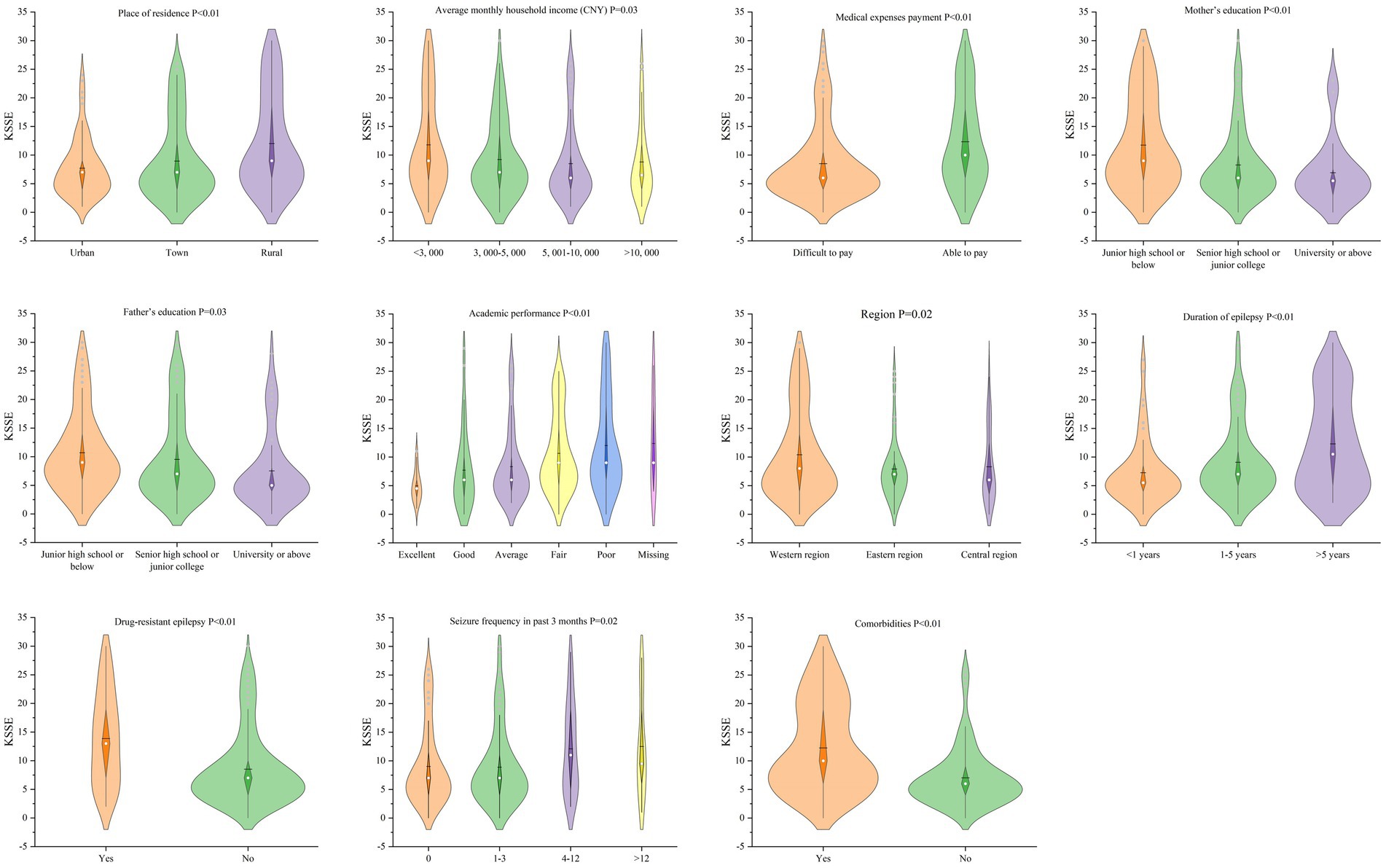
Figure 1. Violin plots of KSSE score in each group.
The average social support score was 37.80 (SD = 9.25), and the score of subjective support dimension was the highest 21.94 (SD = 7.35). The self-efficacy score in children and adolescents with epilepsy was 26.77 (SD = 4.58). The result of the correlation analysis is shown in Figure 2. These analyses revealed stigma to be negatively correlated with social support (r = −0.55, p < 0.01) and self-efficacy (r = −0.43, p < 0.01).
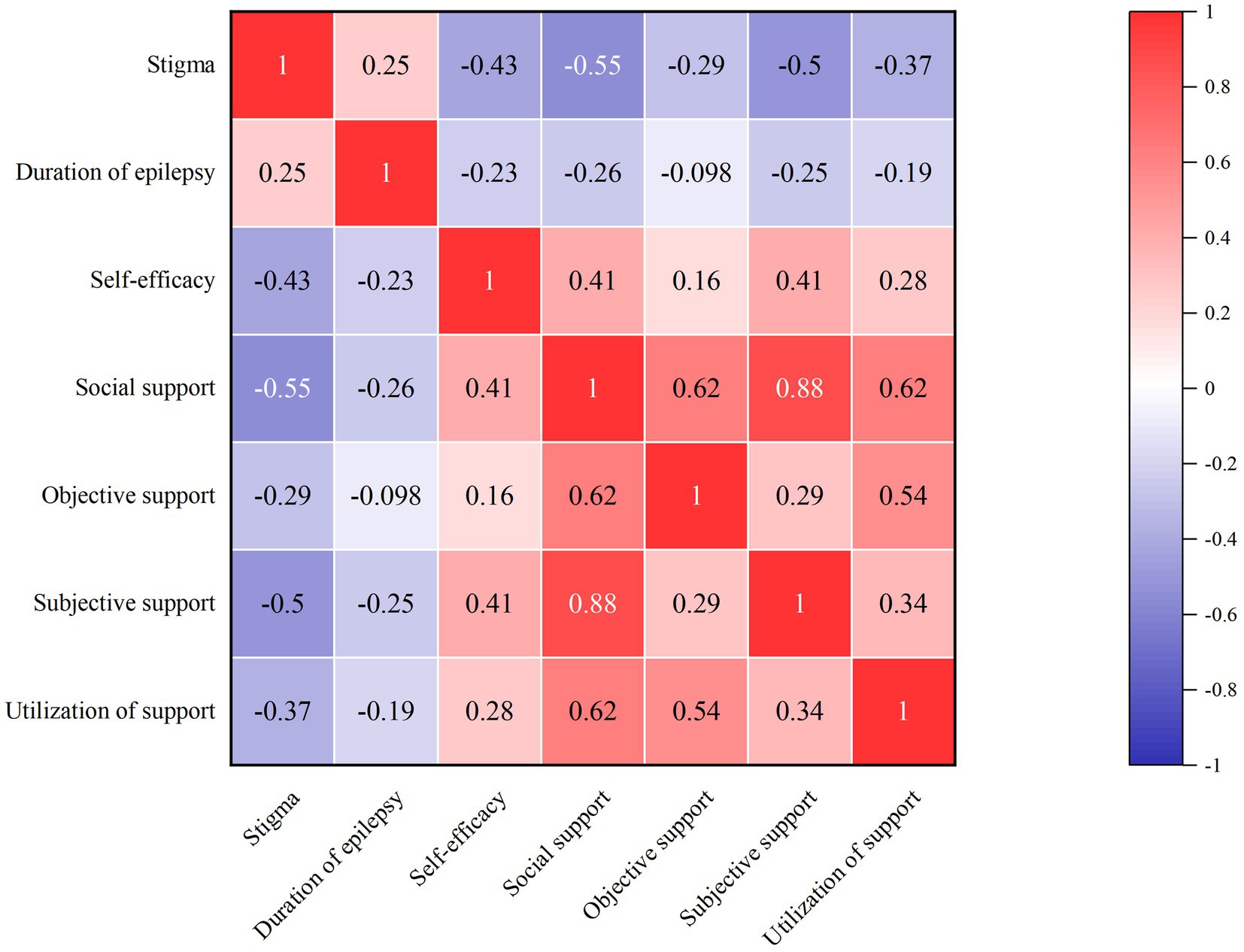
Figure 2. The correlation analysis of stigma, social support and self-efficacy.
The results of the variance analysis indicated that the discrepancy in stigma scores was primarily between rural and non-rural areas. Therefore, the place of residence was divided into rural and non-rural categories, This was done for other variables, like income, education, and so on. Factors with statistical significance in the univariate analysis and correlation analysis were regarded as independent variables; the KSSE scale score was taken as a dependent variable. The results of multiple linear regression on the KSSE are shown in Table 3. According to regression results, major influencing factors are comprised of place of residence, academic performance, region, duration of epilepsy, drug-resistant epilepsy, comorbidities, social support and self-efficacy, explaining 47.9% of the total variation in stigma scores among children and adolescents with epilepsy.
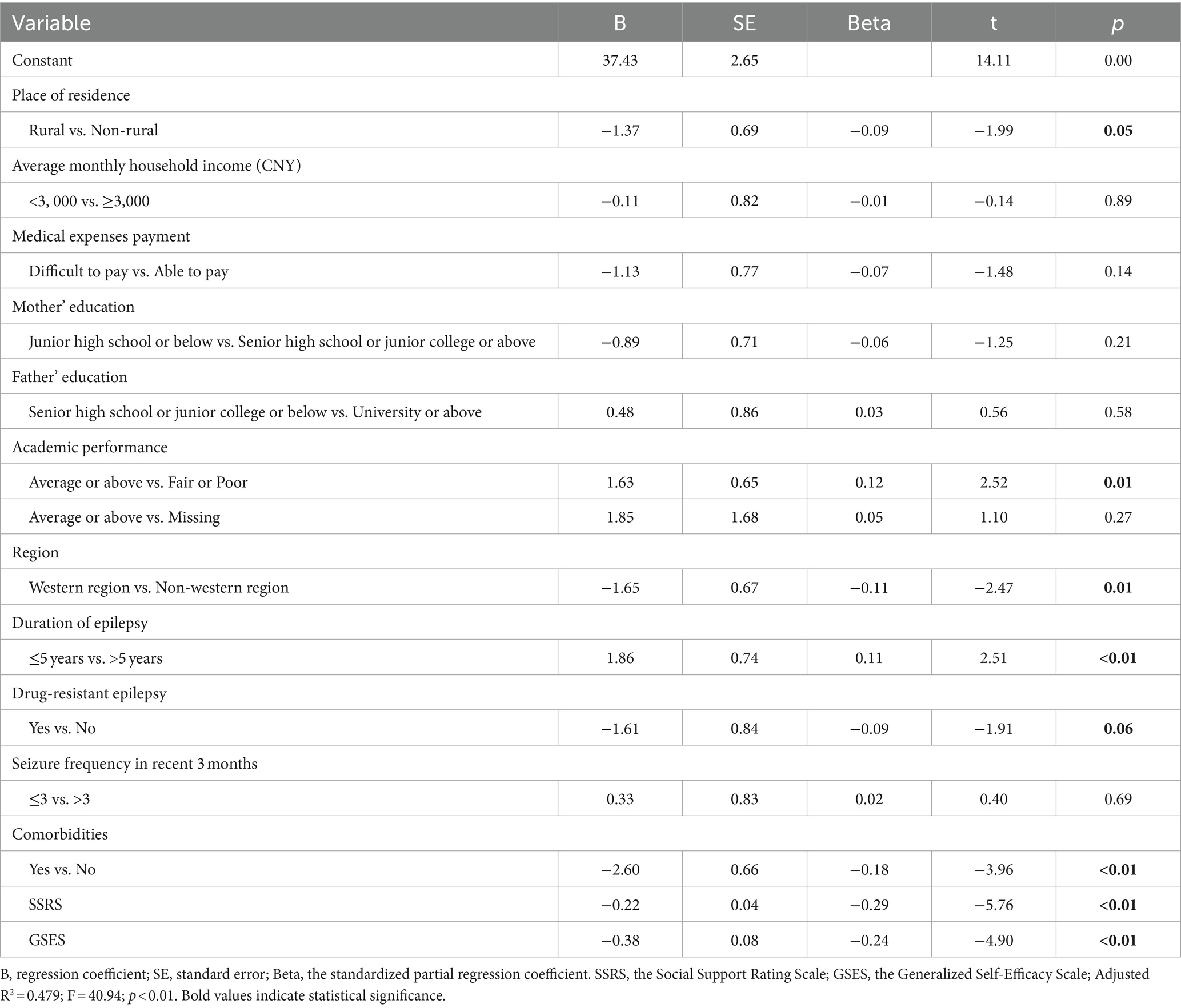
Table 3. Multiple linear regression for KSSE.
The present study utilized a multicenter cross-sectional design to investigate the degree of felt stigma and the influencing factors among children and adolescents with epilepsy in China. Results showed that 35.6% children and adolescents with epilepsy had felt stigma, which is higher than adults with epilepsy in China (32, 33), but significantly lower than the reported 44.7% in Ethiopia (34). Furthermore, this finding is closely similar to that of children and adolescents with epilepsy in Uganda (34.0%) (10). Differences in the incidence of stigma may be due to a complex array of sociocultural factors. The vulnerability to stigma during childhood and adolescence stems from underdeveloped coping mechanisms and limited social resources, making young individuals more prone to the effects of stigma compared to adults (12). Further research is needed to develop appropriate interventions to reduce stigma and improve health outcomes for children and adolescents.
Various factors may contribute to the stigma of epilepsy. The place of residence of the children and adolescents was found to have a statistically significant association with the level of perceived stigma. This finding is similar to the studies in Ethiopia that revealed that stigma is more prevalent among people with epilepsy in rural areas than in urban areas (35). People in rural areas with less education and lower socioeconomic status tend to have more negative attitudes toward epilepsy (36). Moreover, there is a huge treatment gap between urban and rural areas in China (1) This vast treatment gap is mainly driven by deficiencies in health care resources and the social stigma of epilepsy that is a result of cultural beliefs. The adverse effects of stigma on health conditions perpetuate a vicious cycle of social marginalization and deteriorating health (37).
The underdeveloped region of western China has a relatively weak social and economic foundation, resulting in a low level of social security (38). There is an uneven distribution of neurologists and healthcare resources between regions. In less developed areas, medical resources are scarce, especially in central and western China (38). This study showed that the western and non-western regions were statistically significant in the level of felt stigma. However, there is limited research on regional disparities in the stigma associated with epilepsy in China, and future studies with larger, multicenter samples are necessary for validation.
This study found that 48.7% of children with epilepsy performed below the average academic level, and this poor performance was linked to higher stigma. A Swedish study has also found that academic difficulties were common in schoolchildren with active epilepsy (39). A study that examined the Intelligence Quotient (IQ) screening and academic achievement testing of 173 children with epilepsy found that 48% of children had displayed learning disabilities (40). The stigma associated with epilepsy can negatively affect education, employment, income, and public opinion about resource allocation (41). The results indicate the need for intensive support and social care for children with epilepsy in educational settings.
The results of the study showed that children and adolescents with epilepsy for more than 5 years were more likely to feel stigmatized than those with epilepsy for less than 5 year, which is consistent with the previous studies (42). The chronicity of epilepsy may affect the child’s academic and social activities, leading to a wider gap with their peers, and this gap and isolation may exacerbate feelings of stigmatization (12). Children and adolescents undergo a critical developmental period that heightens their awareness of their illness and social status. The chronic and unpredictable nature of epilepsy can exacerbate their self-perception, leading to increased feelings of frustration and shame, and significantly affect emotional and psychological well-being (43). Therefore, appropriate education and advice should be provided to children and adolescents with a long duration of epilepsy to improve their self-management ability and establish correct disease perceptions.
Drug-resistant epilepsy means that conventional anti-seizure medication (ASMs) cannot be effectively control seizures, and children may need to take multiple medications. Frequent seizures and long-term treatment process are prone to psychiatric comorbidities such as anxiety and depression (44). The complexity of the disease can exacerbate the stigma for children and adolescents. In a study of patients hospitalized for epilepsy in Hong Kong, more than half had physical or psychiatric comorbidities (45). It is clear that the double stigma associated with epilepsy and its comorbidities has a negative impact on prevention and care efforts (46). Double stigma poses a new challenge, making it even more important to invest energy and resources. Further robust data collection and monitoring to identify intervention points is urgently needed.
We found that felt stigma was negatively related to a level of self-efficacy and social support. DiIorio et al. (47) identified that self-management interventions aimed at improving self-efficacy can reduce stigma in people with epilepsy. Children and adolescents with epilepsy who possess high levels of self-efficacy often have better emotional regulation skills, which in turn makes them more likely to experience satisfaction and positive emotions (48). Furthermore, the labeling theory proposed by Link could help us further explain this result, suggesting that stigma impairs mental health by destroying the self-evaluation dimension, a concept which is mainly related to self-efficacy (49). At a family level, higher levels of social support in various forms may be a protective factor against stigma. Previous studies have indicated that social support was inversely associated with felt stigma (27, 50). Therefore, increasing social support may be an intervention strategy to prevent or reduce felt stigma among children and adolescents with epilepsy.
To our knowledge, this multicenter study is the first to examine multiple social determinants (parental education, region, academic performance, etc.) and disease characteristics (drug-resistant epilepsy, seizure frequency in past 3 months, comorbidities etc.) simultaneously in a population sample of children and adolescents with epilepsy. The results may provide the basis and direction for the prevention of stigma in children and adolescents with epilepsy. The study also has limitations. Firstly, it is a cross-sectional study, so causality cannot be determined between the variables. Follow-up researchers can conduct longitudinal studies to accumulate evidence of the causal relationship between felt stigma and various influencing factors. Secondly, although our sample size was multicenter, samples from the northeastern region of China were missing, which includes Heilongjiang, Jilin, and Liaoning provinces. This regional bias may affect the generalizability of our results. In future research, a more representative sample of all the regions in China will be needed to verify the results of this study. Thirdly, the traditional Chinese cultural and folk traditions, which influence the perception of epilepsy, may restrict the applicability of our findings in other cultural contexts. For example, the interpretation of epilepsy in Traditional Chinese Medicine, associating it with insanity and convulsion (7), could influence global understanding and research of the condition. Finally, other variables such as psychosocial issues, parental attitudes, school factors, and public attitudes and behaviors will be introduced into the research to discuss their impact on felt stigma in the future (51, 52).
This study indicates that stigma is a significant issue among children and adolescents with epilepsy in China. Meanwhile, place of residence, academic performance, region, duration of epilepsy, drug-resistant epilepsy, comorbidities, social support and self-efficacy are major influencing factors among the complex factors influencing the felt stigma among children and adolescents. It is crucial to integrate psychological counseling into clinical care, collaborate with schools to enhance academic support and reduce bullying, and engage policymakers to improve legislation and health insurance policies, particularly to extend coverage for epilepsy treatment in rural areas. These measures aim to mitigate the stigma and provide a more supportive environment for children and adolescents with epilepsy.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding authors.
The studies involving humans were approved by the Children’s Hospital of Chongqing Medical University. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
JZh: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Software, Validation, Visualization, Writing – original draft, Writing – review & editing. SL: Conceptualization, Funding acquisition, Project administration, Resources, Supervision, Writing – review & editing. NZ: Funding acquisition, Resources, Supervision, Writing – review & editing. CC: Supervision, Writing – review & editing. TW: Investigation, Writing – review & editing. MF: Investigation, Writing – review & editing. JZe: Visualization, Writing – review & editing. YX: Visualization, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work was supported by the Hospital of Chongqing Medical University Nursing Hospital Level Key Project (CHCQMU2023.02) and the China Association Against Epilepsy (CAAE) Epilepsy Care—Kang Zhe Foundation (CK-2024-053) the Chongqing Yuzhong District Science and Technology Commission Technology Foresight and Institutional Innovation Project (20180166).
The authors are particularly grateful to the Pediatric Neurology Care Professional Committee of the Chinese Pediatric Nursing Union and all nursing managers for their support of this study. The authors thank all participants for their valuable contributions.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Ding, D, Zhou, D, Sander, JW, Wang, W, Li, S, and Hong, Z. Epilepsy in China: major progress in the past two decades. Lancet Neurol. (2021) 20:316–26. doi: 10.1016/s1474-4422(21)00023-5
2. Symonds, JD, Elliott, KS, Shetty, J, Armstrong, M, Brunklaus, A, Cutcutache, I, et al. Early childhood epilepsies: epidemiology, classification, aetiology, and socio-economic determinants. Brain. (2021) 144:2879–91. doi: 10.1093/brain/awab162
3. Groover, O, Morton, ML, Janocko, NJ, Teagarden, DL, Villarreal, HK, Drane, DL, et al. Mind the gap: health disparities in families living with epilepsy are significant and linked to socioeconomic status. Epileptic Disord. (2020) 22:782–9. doi: 10.1684/epd.2020.1229
4. Trinka, E, Kwan, P, Lee, B, and Dash, A. Epilepsy in Asia: disease burden, management barriers, and challenges. Epilepsia. (2019) 60:7–21. doi: 10.1111/epi.14458
5. World Health Organization. Epilepsy: A public health imperative World health organization (2019). https://www.who.int/publications/i/item/epilepsy-a-public-health-imperative
6. Kwon, CS, Jacoby, A, Ali, A, Austin, J, Birbeck, GL, Braga, P, et al. Systematic review of frequency of felt and enacted stigma in epilepsy and determining factors and attitudes toward persons living with epilepsy-report from the international league against epilepsy task force on stigma in epilepsy. Epilepsia. (2022) 63:573–97. doi: 10.1111/epi.17135
7. Li, S, Wu, J, Wang, W, Jacoby, A, de Boer, H, and Sander, JW. Stigma and epilepsy: the Chinese perspective. Epilepsy Behav. (2010) 17:242–5. doi: 10.1016/j.yebeh.2009.12.015
8. Yu, P-m, Ding, D, Zhu, G-x, and Hong, Z. International Bureau for Epilepsy survey of children, teenagers, and young people with epilepsy: data in China. Epilepsy Behav. (2009) 16:99–104. doi: 10.1016/j.yebeh.2009.06.013
9. Fisher, RS. Epilepsy from the Patient's perspective: review of results of a community-based survey. Epilepsy Behav. (2000) 1:S9–s14. doi: 10.1006/ebeh.2000.0107
10. Kirabira, J, Nakawuki, M, Fallen, R, and Zari, RG. Perceived stigma and associated factors among children and adolescents with epilepsy in south western Uganda: a cross sectional study. Seizure. (2018) 57:50–5. doi: 10.1016/j.seizure.2018.03.008
11. Mar Htwe, Z, Lae Phyu, W, Zar Nyein, Z, and Aye, KA. Correlation between depression and perceived stigma among people living with epilepsy. Epilepsy Behav. (2023) 146:109372. doi: 10.1016/j.yebeh.2023.109372
12. Earnshaw, VA, Watson, RJ, Eaton, LA, Brousseau, NM, Laurenceau, JP, and Fox, AB. Integrating time into stigma and health research. Nat Rev Psychol. (2022) 1:236–47. doi: 10.1038/s44159-022-00034-2
13. Elafros, MA, Sakubita-Simasiku, C, Atadzhanov, M, Haworth, A, Chomba, E, and Birbeck, GL. Stigma and psychiatric morbidity among mothers of children with epilepsy in Zambia. Int Health. (2013) 5:288–94. doi: 10.1093/inthealth/iht028
14. Yang, TW, Kim, YS, Kim, DH, Yeom, JS, and Kwon, OY. Felt stigma proportion in people living with epilepsy: a systematic review. Seizure. (2023) 111:87–97. doi: 10.1016/j.seizure.2023.07.025
15. Kirabira, J, Forry, JB, Kinengyere, AA, Adriko, W, Amir, A, Rukundo, GZ, et al. A systematic review protocol of stigma among children and adolescents with epilepsy. Syst Rev. (2019) 8:21. doi: 10.1186/s13643-019-0940-9
16. Karakaş, N, Sarıtaş, S, Aktura, S, Karabulutlu, EY, and Oruç, FG. Investigation of factors associated with stigma and social support in patients with epilepsy in Turkey: a cross-sectional study. Epilepsy Behav. (2022) 128:108572. doi: 10.1016/j.yebeh.2022.108572
17. Viteva, E. Stigmatization of patients with epilepsy: a review of the current problem and assessment of the perceived stigma in Bulgarian patients. Epilepsy Behav. (2012) 25:239–43. doi: 10.1016/j.yebeh.2012.07.018
18. Biset, G, Abebaw, N, Gebeyehu, NA, Estifanos, N, Birrie, E, and Tegegne, KD. Prevalence, incidence, and trends of epilepsy among children and adolescents in Africa: a systematic review and meta-analysis. BMC Public Health. (2024) 24:771. doi: 10.1186/s12889-024-18236-z
19. Elliott, JO, Jacobson, MP, and Seals, BF. Self-efficacy, knowledge, health beliefs, quality of life, and stigma in relation to osteoprotective behaviors in epilepsy. Epilepsy Behav. (2006) 9:478–91. doi: 10.1016/j.yebeh.2006.07.007
20. Mula, M, and Sander, JW. Psychosocial aspects of epilepsy: a wider approach. BJPsych Open. (2016) 2:270–4. doi: 10.1192/bjpo.bp.115.002345
21. Fisher, RS, Cross, JH, French, JA, Higurashi, N, Hirsch, E, Jansen, FE, et al. Operational classification of seizure types by the international league against epilepsy: position paper of the ILAE Commission for Classification and Terminology. Epilepsia. (2017) 58:522–30. doi: 10.1111/epi.13670
22. Kwan, P, Arzimanoglou, A, Berg, AT, Brodie, MJ, Allen Hauser, W, Mathern, G, et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc task force of the ILAE commission on therapeutic strategies. Epilepsia. (2010) 51:1069–77. doi: 10.1111/j.1528-1167.2009.02397.x
23. Mbuba, CK, Ngugi, AK, Fegan, G, Ibinda, F, Muchohi, SN, Nyundo, C, et al. Risk factors associated with the epilepsy treatment gap in Kilifi, Kenya: a cross-sectional study. Lancet Neurol. (2012) 11:688–96. doi: 10.1016/s1474-4422(12)70155-2
24. Song, J, Li, Z, Li, H, and Sheng, Y. The level and influence factors of stigma in people living epilepsy. Chin J Nurs. (2016) 51:40–4.
25. Austin, JK, Birbeck, G, Parko, K, Kwon, CS, Fernandes, PT, Braga, P, et al. Epilepsy-related stigma and attitudes: systematic review of screening instruments and interventions—report by the international league against epilepsy task force on stigma in epilepsy. Epilepsia. (2022) 63:598–628. doi: 10.1111/epi.17133
26. Xiao, S. The theoretical basis and applications of social support rating scale(SSRS). J Clin Psychiatry. (1994) 4:98–100.
27. Wu, Y, Yan, Z, Fornah, L, Zhao, J, and Wu, S. The mediation effect of social support between stigma and social alienation in patients with stroke. Front Public Health. (2023) 11:1290177. doi: 10.3389/fpubh.2023.1290177
28. Luszczynska, A, Gutiérrez-Doña, B, and Schwarzer, R. General self-efficacy in various domains of human functioning: evidence from five countries. Int J Psychol. (2005) 40:80–9. doi: 10.1080/00207590444000041
29. Dahlberg, K, Stenberg, E, Liang, Y, Nilsson, U, and Jaensson, M. The general self-efficacy scale in a population planned for bariatric surgery in Sweden: a psychometric evaluation study. BMJ Open. (2022) 12:e061509. doi: 10.1136/bmjopen-2022-061509
30. Wang, C, Hu, Z, and Liu, Y. Evidences for reliability and validity of the Chinese version of general self efficacy scale. Chin J Appl Psychol. (2001) 1:37–40.
31. Cayır, A, and Ulupınar, S. The relationship among educational skills, general self-efficacy perceptions and performance in nursing instructors. Nurse Educ Today. (2021) 107:105129. doi: 10.1016/j.nedt.2021.105129
32. Wei, Z, Wang, X, Ren, L, Liu, C, Liu, C, Cao, M, et al. Using machine learning approach to predict depression and anxiety among patients with epilepsy in China: a cross-sectional study. J Affect Disord. (2023) 336:1–8. doi: 10.1016/j.jad.2023.05.043
33. Wei, Z, Ren, L, Yang, L, Liu, C, Cao, M, Yang, Q, et al. The relationship between social anxiety and felt stigma in patients with epilepsy: a network analysis. Seizure. (2021) 92:76–81. doi: 10.1016/j.seizure.2021.08.014
34. Fite, RO, and Guta, MT. Stigma and associated factors among people with epilepsy in Ethiopia: a systematic review and meta-analysis. Epilepsy Behav. (2021) 117:107872. doi: 10.1016/j.yebeh.2021.107872
35. Tegegne, MT, and Awoke, AA. Perception of stigma and associated factors in people with epilepsy at Amanuel specialized mental hospital, Addis Ababa, Ethiopia. Int J Psychiatry Clin Pract. (2017) 21:58–63. doi: 10.1080/13651501.2016.1223315
36. Tiamkao, S, Sawanyawisuth, K, Singhpoo, K, Ariyanuchitkul, S, and Ngamroop, R. Differences of knowledge, attitudes, and behaviors towards epilepsy between populations in municipal and nonmunicipal areas. Psychol Res Behav Manag. (2013) 6:111–6. doi: 10.2147/prbm.S50842
37. Gavan, L, Hartog, K, Koppenol-Gonzalez, GV, Gronholm, PC, Feddes, AR, Kohrt, BA, et al. Assessing stigma in low- and middle-income countries: a systematic review of scales used with children and adolescents. Soc Sci Med. (2022) 307:115121. doi: 10.1016/j.socscimed.2022.115121
38. Lin, Y, Hu, S, Hao, X, Duan, L, Wang, W, Zhou, D, et al. Epilepsy centers in China: current status and ways forward. Epilepsia. (2021) 62:2640–50. doi: 10.1111/epi.17058
39. Reilly, C, Atkinson, P, Das, KB, Chin, RF, Aylett, SE, Burch, V, et al. Academic achievement in school-aged children with active epilepsy: a population-based study. Epilepsia. (2014) 55:1910–7. doi: 10.1111/epi.12826
40. Fastenau, PS, Jianzhao, S, Dunn, DW, and Austin, JK. Academic underachievement among children with epilepsy: proportion exceeding psychometric criteria for learning disability and associated risk factors. J Learn Disabil. (2008) 41:195–207. doi: 10.1177/0022219408317548
41. Sharac, J, McCrone, P, Clement, S, and Thornicroft, G. The economic impact of mental health stigma and discrimination: a systematic review. Epidemiol Psichiatr Soc. (2010) 19:223–32. doi: 10.1017/s1121189x00001159
42. Bielen, I, Friedrich, L, Sruk, A, Prvan, MP, Hajnšek, S, Petelin, Z, et al. Factors associated with perceived stigma of epilepsy in Croatia: a study using the revised epilepsy stigma scale. Seizure. (2014) 23:117–21. doi: 10.1016/j.seizure.2013.10.008
43. Chong, L, Jamieson, NJ, Gill, D, Singh-Grewal, D, Craig, JC, Ju, A, et al. Children's experiences of epilepsy: a systematic review of qualitative studies. Pediatrics. (2016) 138:658. doi: 10.1542/peds.2016-0658
44. Nigussie, K, Lemma, A, Sertsu, A, Asfaw, H, Kerebih, H, and Abdeta, T. Depression, anxiety and associated factors among people with epilepsy and attending outpatient treatment at primary public hospitals in Northwest Ethiopia: a multicenter cross-sectional study. PLoS One. (2021) 16:e0256236. doi: 10.1371/journal.pone.0256236
45. Chen, Z, Liew, D, and Kwan, P. Excess mortality and hospitalized morbidity in newly treated epilepsy patients. Neurology. (2016) 87:718–25. doi: 10.1212/wnl.0000000000002984
46. Mula, M. Depression in epilepsy. Curr Opin Neurol. (2017) 30:180–6. doi: 10.1097/wco.0000000000000431
47. DiIorio, C, Reisinger, EL, Yeager, KA, and McCarty, F. A telephone-based self-management program for people with epilepsy. Epilepsy Behav. (2009) 14:232–6. doi: 10.1016/j.yebeh.2008.10.016
48. Xu, Z, Rüsch, N, Huang, F, and Kösters, M. Challenging mental health related stigma in China: systematic review and meta-analysis. I. Interventions among the general public. Psychiatry Res. (2017) 255:449–56. doi: 10.1016/j.psychres.2017.01.008
49. Link, BG, Phelan, JC, Bresnahan, M, Stueve, A, and Pescosolido, BA. Public conceptions of mental illness: labels, causes, dangerousness, and social distance. Am J Public Health. (1999) 89:1328–33. doi: 10.2105/ajph.89.9.1328
50. Qin, Y, Dai, M, Chen, L, Zhang, T, Zhou, N, and Chen, X. The relationship between ecological executive function and stigma among patients with epilepsy: the mediating effect of social support. Epilepsy Res. (2022) 182:106919. doi: 10.1016/j.eplepsyres.2022.106919
51. Lee, HJ, Choi, EK, Park, HB, and Yang, S-H. Risk and protective factors related to stigma among people with epilepsy: an integrative review. Epilepsy Behav. (2020) 104:106908. doi: 10.1016/j.yebeh.2020.106908
Keywords: children and adolescents, epilepsy, stigma, social support, cross-sectional
Citation: Zhao J, Li S, Zhang N, Cui C, Wang T, Fan M, Zeng J and Xie Y (2024) Felt stigma and associated factors in children and adolescents with epilepsy: a multicenter cross-sectional study in China. Front. Neurol. 15:1459392. doi: 10.3389/fneur.2024.1459392
Edited by:
Daichi Sone, Jikei University School of Medicine, JapanReviewed by:
Izumi Kuramochi, Saitama Medical University, JapanCopyright © 2024 Zhao, Li, Zhang, Cui, Wang, Fan, Zeng and Xie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Shuangzi Li, MTIwODEyMzUxOEBxcS5jb20=; Ni Zhang, MTEzNDY5OTI3MEBxcS5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.