 Hao Feng1
Hao Feng1 Ruoran Wang
Ruoran Wang Fei Qiao
Fei Qiao- 1Department of Neurosurgery, Nanchong Central Hospital/The Second Clinical Medical College, North Sichuan Medical College, Nanchong, China
- 2Department of Neurosurgery, West China Hospital, Sichuan University, Chengdu, China
Background: The thrombocytopenia influences prognoses of critically ill patients. There are few studies exploring the prognostic value of thrombocytopenia among ICH patients. We perform this study to explore the correlation between thrombocytopenia at different timepoints of hospitalizations and mortality of ICH.
Methods: ICH patients recorded in the Medical Information Mart for Intensive Care-III were selected for this observational study. The thrombocytopenia, defined as platelet <150 × 109/L, was divided into three categories: baseline thrombocytopenia (thrombocytopenia occurred at admission), acquired thrombocytopenia (thrombocytopenia developed since the second day after admission), multiple thrombocytopenia (baseline thrombocytopenia + acquired thrombocytopenia). The main outcome in this study was the 30-day mortality of ICH patients. The univariate and multivariate logistic regression was sequentially performed to discover risk factors of mortality and confirm the correlation between thrombocytopenia groups and mortality of ICH.
Results: 66.5% of 902 ICH patients did not experience the thrombocytopenia since admission. 2.2, 14.5 and 16.7% ICH patients showed the baseline thrombocytopenia, acquired thrombocytopenia initial and multiple thrombocytopenia, respectively. The GCS did not show significant difference between thrombocytopenia groups (p = 0.118). The multiple thrombocytopenia group had the highest incidence of mechanical ventilation (p = 0.041), mortality (p < 0.001), and the longest length of ICU stay (p < 0.001), length of hospital stay (p < 0.001). The multivariate logistic regression found age (p < 0.001), GCS (p < 0.001), glucose (p = 0.013), mechanical ventilation (p = 0.002) was correlated with the mortality of ICH patients. Only the multiple thrombocytopenia group showed significant influence on the mortality of ICH (p = 0.002) in the multivariate logistic regression.
Conclusion: Single initial thrombocytopenia at admission dose not influence the mortality of ICH patients. ICH patients experiencing both initial thrombocytopenia and acquired thrombocytopenia have significantly higher mortality risk. The blood platelet level of ICH patients should be monitored continuously during hospitalizations to detect the thrombocytopenia and identify the high risk of poor prognosis.
1 Introduction
Accounting for nearly one third of stroke incidence, the intracerebral hemorrhage (ICH) leads poor prognosis of patients with the mortality more than 50% (1, 2). As the essential component of coagulation and hemostasis, the platelet plays an important role on the pathophysiological process of stroke. Both abnormalities of platelet function and number significantly may influence the bleeding events and prognoses of stroke patients (3, 4). The thrombocytopenia, commonly defined as the platelet level < 150 × 109/L, has been confirmed correlated with a serious of bleeding events, transufsion requirements and outcomes of critially ill patients (5, 6). While two studies, respectively, found the thrombocytopenia at admission was not related with the poor outcomes of ICH patients and ichemic stroke patients (7, 8). Another study discovered that only thrombocytopenia developed during ICU stay but not thrombocytopenia at admission was an indepdent risk factor for mortality of patients treated in the neurocritical care unit (9). And one recent study found the risk of hospital mortality in critically ill patients increased significantly with persistent thrombocytopenia but not transient thrombocytopenia (10). These findings lead us to make a hypothesis that thrombocytopenia at different timepoints since admission may exert different effects on prognoses of ICH patients. Therefore, we design this study to explore the prognostici value of thrombocytopenia at admission and thrombocytopenia developed during hospitalizations among ICH patients.
2 Materials and methods
2.1 Enrolled participants
ICH patients (confirmed using ICD-9 code-431) recorded in the Medical Information Mart for Intensive Care-III (MIMIC-III) (an intensive care database enrolling patients from the Beth Israel Deaconess Medical Center between 2001 and 2012) were selected for this observational study. A part of ICH patients were sequentially excluded from this study for four causes: (1) no records of platelet (n = 14); (2) no records of platelet at admission (n = 6); (3) records of platelet after day 1 ≤ 2 (n = 435); (4) no records of Glasgow Coma Scale (GCS) (n = 9). Nine hundred and two ICH patients were enrolled after the screening. The MIMIC-III deidentified personal information of patients and received ethical approvements from the Massachusetts Institute of Technology and Beth Israel Deaconess Medical Center.
2.2 Variables collection
Demographic information (age, gale gender), comorbidities (hypertension, hyperlipidemia, diabetes, atrial fibrillation, coronary heart disease, chronic renal disease), vital signs at admission (mean blood pressure, heart rate), pulse oxygen saturation (SpO2) and GCS at admission were recorded. Laboratory examinations including white blood cell, hemoglobin, hematocrit, platelet, glucose, calcium, phosphate, prothrombin time, activated partial thromboplastin time, international normalized ratio (INR) were analyzed using the first blood sample after admission (within 24 h since admission). The subsequent platelet level after day 1 was also collected with the median frequency of 9 for measurements. The thrombocytopenia, defined as platelet <150 × 109/L, was divided into three categories: baseline thrombocytopenia (thrombocytopenia occurred at admission), acquired thrombocytopenia (thrombocytopenia developed since the second day after admission), multiple thrombocytopenia (baseline thrombocytopenia + acquired thrombocytopenia). The main outcome in this study was the 30-day mortality of ICH patients. The incidence of mechanical ventilation, length of ICU stay, length of hospital stay was also compared between different thrombocytopenia groups.
2.3 Statistical analyses
Variables with normal distribution or non-normal distribution were, respectively presented as mean ± standard or median (interquartile range). Kolmogorov–Smirnov test was used for testing the normal distribution of variables. Patients were divided into different groups according to the occurrence and timepoint of thrombocytopenia. Differences between these groups were compared using one way ANOVA (variables with normal distribution), Kruskal–Wallis (variables with non-normal distribution), or chi-square test (categorical variables). The univariate and multivariate logistic regression was sequentially performed to discover risk factors of mortality and confirm the correlation between thrombocytopenia groups and mortality of ICH. Two sides p-value <0.05 was set as statistically significant. All analyses and figures were performed using GraphPad Prism (GraphPad Software Inc., La Jolla, CA, United States) and SPSS 23.0 (SPSS, Inc., Chicago, IL).
3 Results
3.1 Comparison between thrombocytopenia groups of ICH patients
The occurrence of thrombocytopenia is concentrated in the first 10 days with the peak on the third day since admission (Figures 1A,B). Among 902 ICH patients, 66.5% (n = 600) of them did not experience the thrombocytopenia since admission (Table 1). 2.2% (n = 20) ICH patients showed the only initial thrombocytopenia at admission and 14.5% (n = 131) experienced acquired thrombocytopenia since the second day after admission. 16.7% (n = 151) ICH patients experienced both initial thrombocytopenia and acquired thrombocytopenia during hospitalizations (Table 1). Age (p = 0.002) and gender ratio (p = 0.006) showed significant difference among thrombocytopenia groups. The comorbidity atrial fibrillation was most prevalent in the baseline thrombocytopenia group (p = 0.029). The GCS did not show significant difference between thrombocytopenia groups though the multiple thrombocytopenia group had relatively lower GCS [9 (6–14)] (p = 0.118). Laboratory examination presented the multiple thrombocytopenia group had the lowest level of hemoglobin (p = 0.006), hematocrit (p = 0.003), platelet (p < 0.001), calcium (p < 0.001) and the highest level of prothrombin time (p < 0.001), activated partial thromboplastin time (p < 0.001), INR (p < 0.001). Furthermore, the multiple thrombocytopenia group had the highest incidence of mechanical ventilation (p = 0.041), mortality (p < 0.001) and the longest length of ICU stay (p < 0.001), length of hospital stay (p < 0.001).
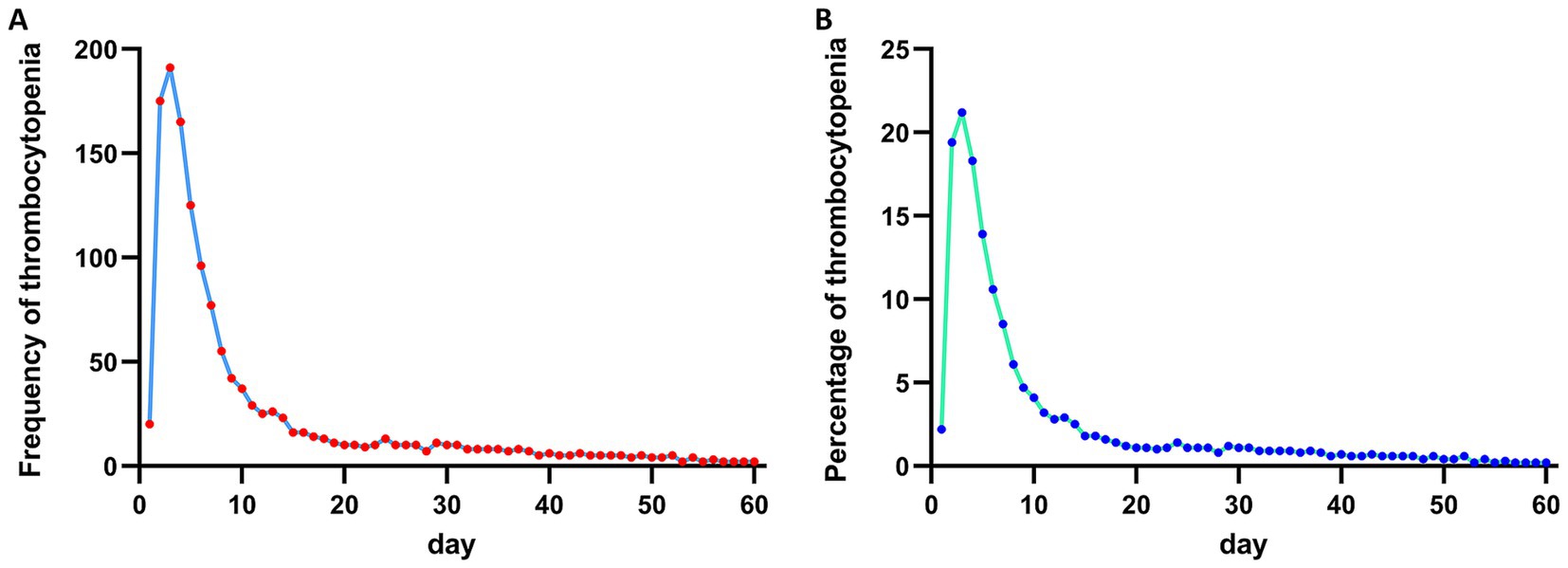
Figure 1. (A) Frequency of thrombocytopenia during hospitalizations in ICH patients. (B) Percentage of thrombocytopenia during hospitalizations in ICH patients.
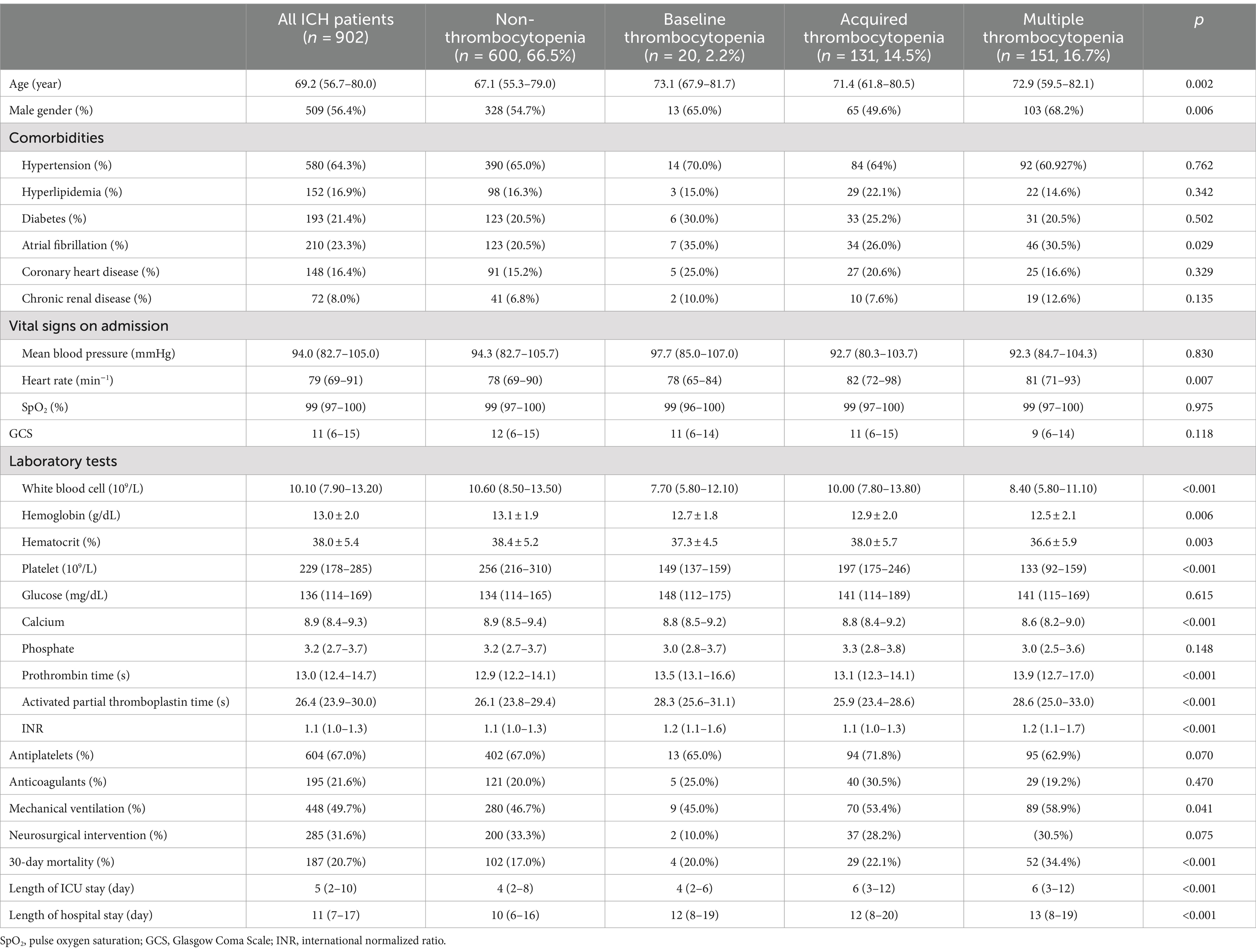
Table 1. Comparison between groups of ICH patients divided by the thrombocytopenia.
3.2 Correlation between thrombocytopenia and 30-day mortality of ICH patients
The univariate logistic regression presented age (p < 0.001), atrial fibrillation (p = 0.005), chronic renal disease (p = 0.016), mean blood pressure (p = 0.021), GCS (p < 0.001), hemoglobin (p = 0.001), hematocrit (p = 0.002), glucose (p < 0.001), mechanical ventilation (p < 0.001) was correlated with the mortality of ICH patients (Table 2). Only the multiple thrombocytopenia group (p < 0.001) showed statistical significance on influencing the mortality of ICH in the univariate logistic regression (Figure 2A). The multivariate logistic regression found age (p < 0.001), GCS (p < 0.001), glucose (p = 0.013), mechanical ventilation (p = 0.002) was correlated with the mortality of ICH patients. The multiple thrombocytopenia still showed statistical significance (p = 0.002) in the multivariate logistic regression while other thrombocytopenia groups did not correlate with the mortality of ICH patients (Figure 2B).

Table 2. Univariate and multivariate logistic regression analysis of correlation between thrombocytopenia and 30-day mortality of intracerebral hemorrhage patients.
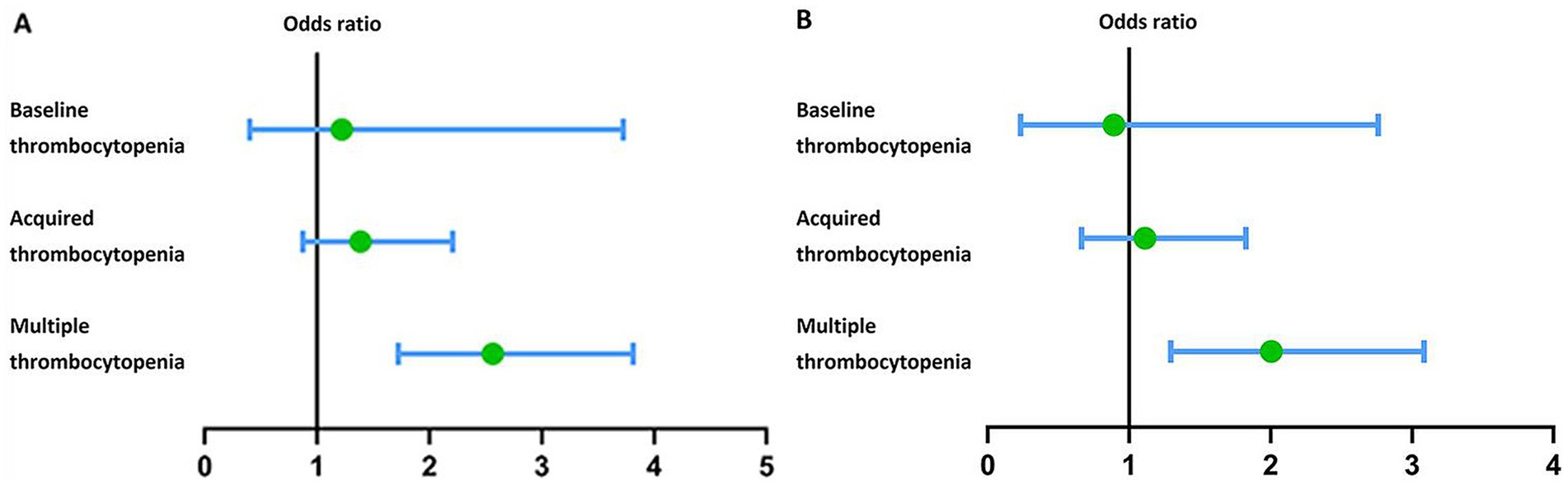
Figure 2. (A) Forest plot showing the correlation between different types of thrombocytopenia and mortality of ICH patients analyzed by the univariate logistic regression. (B) Forest plot showing the correlation between different types of thrombocytopenia and mortality of ICH patients analyzed by the multivariate logistic regression.
4 Discussion
As a disorder of coagulative system, the thrombocytopenia is prevalent among hospitalized patients with the incidence ranging from 8.3 to 67.6% (6). Some studies have explored risk factors for the thrombocytopenia including age, gender, sepsis, liver dysfunction, bleeding, disease severity reflected by the sequential organ failure score (6, 11, 12). While the effect of thrombocytopenia on the prognosis of various patients has not been confirmed. Some studies found the thrombocytopenia were related with the mortality risk of various patients including sepsis, COVID-19, seasonal influenza, systemic lupus erythematosus, cancer (12–18). While one study showed the thrombocytopenia at admission was not related with poor outcomes of ichemic stroke patients (8). Another study implied that the thrombocytopenia did not influence rates of hematoma enlargement and functional status of ICH patients, regardless of the prior antiplatelet therapy (7). It is noteworthy that only thrombocytopenia developed during ICU stay but not thrombocytopenia at admission was confirmed an indepdent risk factor for mortality of patients treated in the neurocritical care unit (9). This fact indicated that the thrombocytopenia at different timepoints since admission may exert different effects on prognoses of crtically ill patients. Consistent with the finding, results of our study implied ICH patients complicated with thrombocytopenia both at admission and developed during hospitalizations had significanly higher mortality while the ICH patients with thrombocytopenia only at admission did not show higher mortaliy risk than non-thrombocytopenia ICH patients.
The insignificance of baseline thrombocytopenia indicated that it may just act as a reflection of initial stroke severity or prior use of antiplatelets. The transient effect of low platelet level at admission may not play a critical role on the prognoses of ICH patients. Only our stated multiple thrombocytopenia which meant persistent thrombocytopenia lasting from the admission to subsequent hospitalization significantly influence the mortality of ICH patients. This finding was consistent with one previous study showing that the mortality of critically ill patients begins to significantly increase only when the thrombocytopenia lasts more than 2 days and the mortality is positively associated with the duration of thrombocytopenia (10). The persistent or multiple thrombocytopenia could be caused by many factors including blood dilution, decreased platelet production, increased platelet consumption, and drugs (19, 20). As for ICH patients, the excessive consumption caused by coagulation, intraoperative blood loss and intracranial progressive hemorrhage may both contribute to the persistent state of low platelet level.
Due to the prognostic effect of multiple thrombocytopenia, the platelet level after ICH should be monitored constantly especially during the first 10 days of hospitalizations. And preventive measures for the trend of reduced platelet level including appropriate platelet transfusion should be provided after ICH. Certainly, the detailed schedule and indications of platelet transfusion for ICH patients has not been decided though studies have been performed to validate the efficiency and safety of platelet transfusion in ICH patients especially those with prior antiplatelet use (21–26). Though most of available evidence showed no benefit of platelet transfusion for ICH patients with prior antiplatelet use, the efficacy of platelet transfusion for the general ICH patients receiving surgical intervention has not been confirmed. The discovered effect of thrombocytopenia at different timepoints in our study may be helpful for researchers to design clinical trials exploring the indication of platelet transfusion among ICH patients in the future.
Some limitations were not avoidable in this study. First, this observational study collects patients from the single American Medical Center. The selection bias is not avoidable and the finding should be further confirmed by future studies in other medical centers from other countries. Second, some confounding factors influencing the correlation between thrombocytopenia and mortality may not be included such as platelet transfusion, coagulants transfusion. Third, the low number of baseline thrombocytopenia group would influence the reliability of our findings, which should be verified by future studies with larger sample sizes. Fourth, only the occurrence and timepoints of thrombocytopenia were analyzed but not the severity of thrombocytopenia. The severity of low platelet level may also influence the correlation between thrombocytopenia and mortality of ICH. Future studies should be designed to further analyze the comprehensive effect of severity and timepoint of thrombocytopenia on the prognoses of ICH patients. Fifth, prognostic effect of thrombocytopenia on outcome was analyzed while the effect of correcting thrombocytopenia by platelet transfusion was not analyzed due to the inherent limitation of observational study. Randomized controlled studies are worthy to confirm therapeutic effect of platelet transfusion at different timepoints of hospitalizations on platelet level and prognosis. Finally, other outcomes such as functional status and rebleeding events of ICH patients were not analyzed due to the incomplete record of the database. Future studies could be designed to verify relationships between these outcomes and thrombocytopenia. Although these limitations, the strength of our study is exploring the diverse prognostic effect of the thrombocytopenia at different timepoints among ICH patients after admission.
5 Conclusion
Initial thrombocytopenia at admission is not associated with the mortality of ICH patients. ICH patients experiencing both initial thrombocytopenia and acquired thrombocytopenia have significantly higher mortality risk. The platelet level of ICH patients should be monitored constantly during hospitalizations to detect the thrombocytopenia and identify high mortality risk.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: mimic.physionet.org.
Ethics statement
Ethical review and approval was not required for the study on human participants in accordance with the local legislation and institutional requirements. Written informed consent from the patients/participants or patients/participants’ legal guardian/next of kin was not required to participate in this study in accordance with the national legislation and the institutional requirements.
Author contributions
HF: Conceptualization, Writing – original draft. XL: Data curation, Formal analysis, Writing – original draft. AF: Writing – review & editing. RW: Data curation, Formal analysis, Methodology, Resources, Software, Writing – original draft. FQ: Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Krishnamurthi, RV, Moran, AE, Forouzanfar, MH, Bennett, DA, Mensah, GA, Lawes, CMM, et al. The global burden of hemorrhagic stroke: a summary of findings from the GBD 2010 study. Glob Heart. (2014) 9:101–6. doi: 10.1016/j.gheart.2014.01.003
2. GBD 2019 Stroke Collaborators . Global, regional, and national burden of stroke and its risk factors, 1990–2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet Neurol. (2021) 20:795–820. doi: 10.1016/S1474-4422(21)00252-0
3. Ziai, WC, Torbey, MT, Kickler, TS, Oh, S, Bhardwaj, A, and Wityk, RJ. Platelet count and function in spontaneous intracerebral hemorrhage. J Stroke Cerebrovasc Dis. (2003) 12:201–6. doi: 10.1016/S1052-3057(03)00075-2
4. Ciolli, L, Lelli, N, Rosafio, F, Maffei, S, Sacchetti, F, Vandelli, L, et al. Platelet function monitoring performed after carotid stenting during endovascular stroke treatment predicts outcome. J Stroke Cerebrovasc Dis. (2021) 30:105800. doi: 10.1016/j.jstrokecerebrovasdis.2021.105800
5. Jonsson, AB, Rygård, SL, Hildebrandt, T, Perner, A, Møller, MH, and Russell, L. Thrombocytopenia in intensive care unit patients: a scoping review. Acta Anaesthesiol Scand. (2021) 65:2–14. doi: 10.1111/aas.13699
6. Hui, P, Cook, DJ, Lim, W, Fraser, GA, and Arnold, DM. The frequency and clinical significance of thrombocytopenia complicating critical illness: a systematic review. Chest. (2011) 139:271–8. doi: 10.1378/chest.10-2243
7. Mrochen, A, Sprügel, MI, Gerner, ST, Sembill, JA, Lang, S, Lücking, H, et al. Thrombocytopenia and clinical outcomes in intracerebral hemorrhage: a retrospective multicenter cohort study. Stroke. (2021) 52:611–9. doi: 10.1161/STROKEAHA.120.031478
8. Wang, YR, Yang, LY, Lee, CH, Chang, SH, Chen, PH, and Jhou, HJ. Is thrombocytopenia an in-hospital mortality risk factor among patients with acute ischemic stroke? A propensity score-matched analysis from the MIMIC-IV database. J Clin Med. (2023) 12:580. doi: 10.3390/jcm12020580
9. Zhou, D, Li, Z, Wu, L, Shi, G, and Zhou, J. Thrombocytopenia and platelet course on hospital mortality in neurological intensive care unit: a retrospective observational study from large database. BMC Neurol. (2020) 20:220. doi: 10.1186/s12883-020-01794-1
10. Jiang, X, Zhang, W, Ma, X, and Cheng, X. Risk of hospital mortality in critically ill patients with transient and persistent thrombocytopenia: a retrospective study. Shock. (2022) 58:471–5. doi: 10.1097/SHK.0000000000002005
11. Anthon, CT, Pène, F, Perner, A, Azoulay, E, Puxty, K, van de Louw, A, et al. Thrombocytopenia and platelet transfusions in ICU patients: an international inception cohort study (PLOT-ICU). Intensive Care Med. (2023) 49:1327–38. doi: 10.1007/s00134-023-07225-2
12. Williamson, DR, Lesur, O, Tétrault, JP, Nault, V, and Pilon, D. Thrombocytopenia in the critically ill: prevalence, incidence, risk factors, and clinical outcomes. Can J Anaesth. (2013) 60:641–51. doi: 10.1007/s12630-013-9933-7
13. Sherban, A, Hussen, R, Gafter-Gvili, A, Atamna, A, Bishara, J, Raanani, P, et al. The impact of thrombocytopenia and lymphopenia on mortality in patients infected with influenza virus—a retrospective cohort study. Acta Haematol. (2023) 146:481–9. doi: 10.1159/000533466
14. Yang, X, Yang, Q, Wang, Y, Wu, Y, Xu, J, Yu, Y, et al. Thrombocytopenia and its association with mortality in patients with COVID-19. J Thromb Haemost. (2020) 18:1469–72. doi: 10.1111/jth.14848
15. Zhao, H, Li, S, and Yang, R. Thrombocytopenia in patients with systemic lupus erythematosus: significant in the clinical implication and prognosis. Platelets. (2010) 21:380–5. doi: 10.3109/09537101003735564
16. Koyama, K, Katayama, S, Muronoi, T, Tonai, K, Goto, Y, Koinuma, T, et al. Time course of immature platelet count and its relation to thrombocytopenia and mortality in patients with sepsis. PLoS One. (2018) 13:e0192064. doi: 10.1371/journal.pone.0192064
17. Peng, W, Li, C, Zhang, X, Wen, T, and Chen, Z. The impact of thrombocytopenia on prognosis of HBV-related small hepatocellular carcinoma: a propensity score matching analysis. World J Surg Oncol. (2021) 19:46. doi: 10.1186/s12957-021-02160-2
18. Yang, F, Tian, J, Peng, L, Zhang, L, Liu, J, Tian, X, et al. Thrombocytopenia is an independent risk factor for the prognosis of thrombotic microangiopathy in Chinese patients with systemic lupus erythematosus. Front Med. (2021) 8:772607. doi: 10.3389/fmed.2021.772607
19. Pluta, J, and Trzebicki, J. Thrombocytopenia: the most frequent haemostatic disorder in the ICU. Anaesthesiol Intensive Ther. (2019) 51:56–63. doi: 10.5603/AIT.2019.0011
20. Greinacher, A, and Selleng, S. How I evaluate and treat thrombocytopenia in the intensive care unit patient. Blood. (2016) 128:3032–42. doi: 10.1182/blood-2016-09-693655
21. Baharoglu, MI, Cordonnier, C, Salman, RAS, de Gans, K, Koopman, MM, Brand, A, et al. Platelet transfusion versus standard care after acute stroke due to spontaneous cerebral haemorrhage associated with antiplatelet therapy (PATCH): a randomised, open-label, phase 3 trial. Lancet. (2016) 387:2605–13. doi: 10.1016/S0140-6736(16)30392-0
22. Lin, Y, Liu, Y, Liu, L, Zhang, L, Lin, Y, Yu, J, et al. Platelet transfusion for spontaneous intracerebral hemorrhage with prior antiplatelet: a systematic review and meta-analysis. Medicine. (2023) 102:e36072. doi: 10.1097/MD.0000000000036072
23. Morris, NA, Patel, N, Galvagno, SM Jr, Ludeman, E, Schwartzbauer, GT, Pourmand, A, et al. The effect of platelet transfusion on functional independence and mortality after antiplatelet therapy associated spontaneous intracerebral hemorrhage: a systematic review and meta-analysis. J Neurol Sci. (2020) 417:117075. doi: 10.1016/j.jns.2020.117075
24. Mengel, A, Stefanou, MI, Hadaschik, KA, Wolf, M, Stadler, V, Poli, K, et al. Early Administration of desmopressin and platelet transfusion for reducing hematoma expansion in patients with acute antiplatelet therapy associated intracerebral hemorrhage. Crit Care Med. (2020) 48:1009–17. doi: 10.1097/CCM.0000000000004348
25. Arnone, GD, Kumar, P, Wonais, MC, Esfahani, DR, Campbell-Lee, SA, Charbel, FT, et al. Impact of platelet transfusion on intracerebral hemorrhage in patients on antiplatelet therapy-an analysis based on intracerebral hemorrhage score. World Neurosurg. (2018) 111:e895–904. doi: 10.1016/j.wneu.2018.01.006
Keywords: intracerebral hemorrhage, thrombocytopenia, platelet, mortality, hemorrhagic stroke
Citation: Feng H, Luo X, Fu A, Wang R and Qiao F (2024) Prognostic value of thrombocytopenia during hospitalizations in intracerebral hemorrhage patients. Front. Neurol. 15:1429988. doi: 10.3389/fneur.2024.1429988
Edited by:
Luis Rafael Moscote-Salazar, Colombian Clinical Research Group in Neurocritical Care, ColombiaReviewed by:
Nikoloz Tsiskaridze, Pineo Medical Ecosystem, GeorgiaLi Zhang, Nanjing University, China
Copyright © 2024 Feng, Luo, Fu, Wang and Qiao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Fei Qiao, cWlhb2ZlaXd4eEAxNjMuY29t