 A. Özge
A. Özge B. Baykan
B. Baykan Ş. Bıçakçı3
Ş. Bıçakçı3 A. Ç. Atalar
A. Ç. Atalar N. Karlı
N. Karlı
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 13 June 2024
Sec. Headache and Neurogenic Pain
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1402569
Migraine, a prevalent neurological disorder, affects approximately 14.1% of the global population and disproportionately impacts females. This debilitating condition significantly compromises quality of life, productivity, and incurs high healthcare costs, presenting a challenge not only to individuals but to societal structures as a whole. Despite advances in our understanding of migraine pathophysiology, treatment options remain limited, necessitating ongoing research into effective therapies. This review delves into the complexity of migraine management, examining the roles of genetic predisposition, environmental influences, personalized treatment approaches, comorbidities, efficacy and safety of existing acute and preventive treatments. It further explores the continuum between migraine and tension-type headaches and discusses the intricacies of treating various migraine subtypes, including those with and without aura. We emphasize the recent paradigm shift toward trigeminovascular activation and the release of vasoactive substances, such as calcitonin gene-related peptide (CGRP), which offer novel therapeutic targets. We assess groundbreaking clinical trials, pharmacokinetic and pharmacodynamic perspectives, safety, tolerability, and the real-world application of CGRP monoclonal antibodies and gepants. In the face of persisting treatment barriers such as misdiagnosis, medication overuse headaches, and limited access to specialist care, we discuss innovative CGRP-targeted strategies, the high cost and scarcity of long-term efficacy data, and suggest comprehensive solutions tailored to Turkiye and developing countries. The review offers strategic recommendations including the formulation of primary care guidelines, establishment of specialized outpatient clinics, updating physicians on novel treatments, enhancing global accessibility to advanced therapies, and fostering patient education. Emphasizing the importance of lifestyle modifications and holistic approaches, the review underscores the potential of mass media and patient groups in disseminating critical health information and shaping the future of migraine management.
Migraine is a prevalent neurological disorder, affecting approximately 14.1% of the global population, with a higher incidence among females than males (1, 2). It is a debilitating condition that significantly impacts the patient’s quality of life, daily activities, productivity, and is associated with substantial healthcare costs (3, 4). The burden of migraine is not limited to the individual, but it also has a significant impact on their families and society as a whole, social psychological and economical (5). Despite substantial progress in understanding the pathophysiology of migraine, effective treatment options are still limited.
The complexity and heterogeneity of migraine’s etiology, pathophysiology, and treatment management pose significant challenges to developing effective therapies (6). Several factors, such as the interaction of genetic and environmental factors, hormonal changes, oxidative stress, inflammation, and neuronal hyperexcitability, have been implicated in migraine etiology and pathophysiology (7–9). It has been estimated that about 42% of migraines are inherited and relatives of cases with elevated pain scores, frequent attacks, early onset, migraine with aura faced a heightened risk (9). It is also hypothesized that tension type headache and migraine are two ends of the same spectrum in which transition in between can be seen (10–12) There are different subtypes of migraine, like migraine with and without aura, each with distinct clinical features and pathophysiology, which makes it challenging to treat (13). The drug treatment includes acute and preventive therapies, which aim to reduce the frequency, severity, and duration and burden of migraine attacks and improve the patient’s quality of life (14).
The understanding of the mechanisms underlying migraine has advanced in recent years and many potential targets for acute and preventive treatment have been identified (15, 16). The most recent hypothesis is the trigeminovascular activation resulting from the nociceptive signals originating from the meningeal vessels via trigeminal sensory branches which are then transmitted to cortical parts of the central nervous system. During this process several vasoactive substances including calcitonin gene-related peptide (CGRP) are released resulting in vasodilatation of the vessels and pain production. New therapeutic agents including CGRP monoclonal antibodies, anti-CGRP receptor antibodies, small-molecule CGRP receptor antagonists, gepants, ditans, and neuromodulation devices have shown promise in clinical trials (17–19). The development of these new treatments represent a significant unmet need in the field (20).
In this review article we aimed to;
• Explain the rationale of CGRP as the target of new migraine therapies.
• Review the major clinical trials, pharmacokinetic/dynamic insights, safety and tolerability profiles with real-world data (if available) of the CGRP monoclonal antibodies and gepants.
• Assess the clinical implications of new treatments targeting CGRP, opportunities and challenges for CGRP monoclonal antibodies and gepants launching.
• Provide specific recommendations for future treatment landscape in the context of Turkiye and developing countries.
An Expert Group Advisory Committee Meeting, involving 6 experts in neurology therapeutic area from Turkiye was convened in November 2022 to identify the scope of the literature search and to evaluate the resources. Each expert was either a member of an academic association, contributed to development of guidelines on the subject or published articles on migraine management. Prior to that meeting, a literature review was performed to highlight the evaluation of calcitonin gene-related peptide targeted therapies, current guidelines, obstacles to management and recommendations for effective migraine treatment from a global and regional Turkish perspective. To identify relevant articles, we searched the MEDLINE® (via the PubMed interface), Web of Science, Google Scholar and EMBASE databases. An electronic search of the literature published from 2000 to 2024 was conducted in these databases by using MeSH (Medical Subject Heading, Medline) and EMBASE terms, as well as free text words. The search included the terms “calcitonin gene-related peptide targeted therapies,” “current headache guidelines” “migraine management” and “migraine and Turkiye.” The inclusion criteria were: (1) peer-reviewed articles and scientific reports, (2) original articles, review articles and conference papers, including information about migraine management (3) publication between 2000 and 2024. The exclusion criteria were: (1) articles not published in either English or Turkish, and (2) case reports. The reference lists of all manuscripts were manually reviewed for additional eligible articles. Most recent and up to date publications were chosen. Relying upon this literature review, experts created a national perspective and developed brief recommendations for a future treatment landscape in Turkiye focused on migraine management.
Standard conventional migraine treatment can be divided in to acute and preventive strategies both still inholding significant unmet needs. These include suboptimal optimization, limited efficacy, excessive reliance on acute treatment agents leading to medication overuse headache (MOH) and the absence of suitable therapeutic options for all individuals (21). This brings the need for more effective, tolerable therapies with fewer contraindications. Recent clinical trials have demonstrated the effectiveness of monoclonal antibodies targeting CGRP or its receptor in reducing the frequency and severity of migraines (19). Other promising approaches include neuromodulation techniques, such as transcranial magnetic stimulation and vagus nerve stimulation, which have shown efficacy in reducing migraine frequency and severity (22, 23). In addition, non-pharmacological treatments, such as cognitive behavioral therapy and mindfulness-based interventions, have also shown promise in reducing migraine frequency and improving quality of life (24, 25). This article mainly concentrates on CGRP targets, as they dominate the mechanism of action of recent acute and preventive treatment options. Current migraine management approaches are summarized in Figure 1.
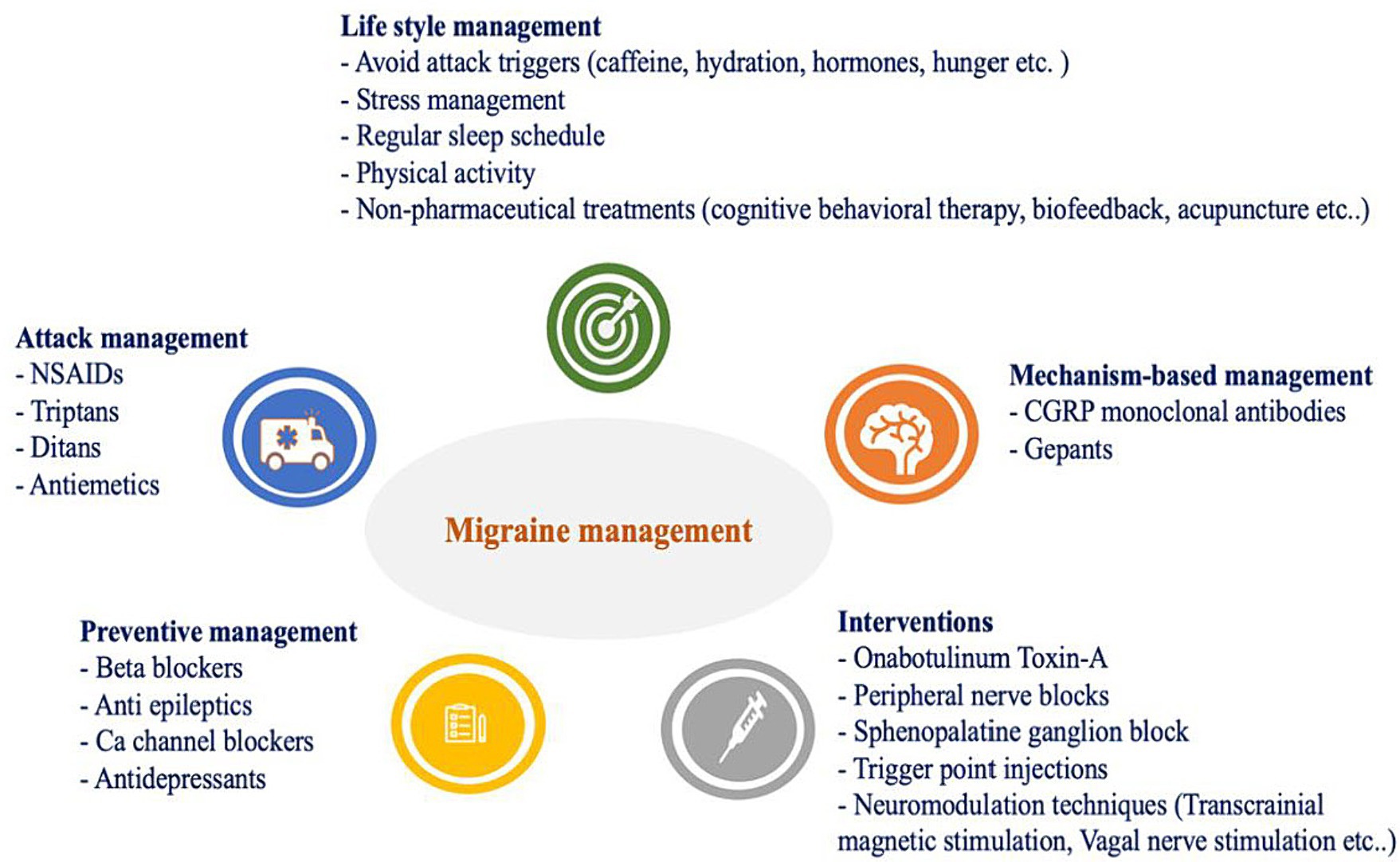
Figure 1. Current migraine management.
There are two main types of CGRP-targeted drugs (Figure 2): CGRP monoclonal antibodies, which are large-molecule CGRP receptor or ligand antagonists and gepants, which are small-molecule CGRP receptor antagonists (26).
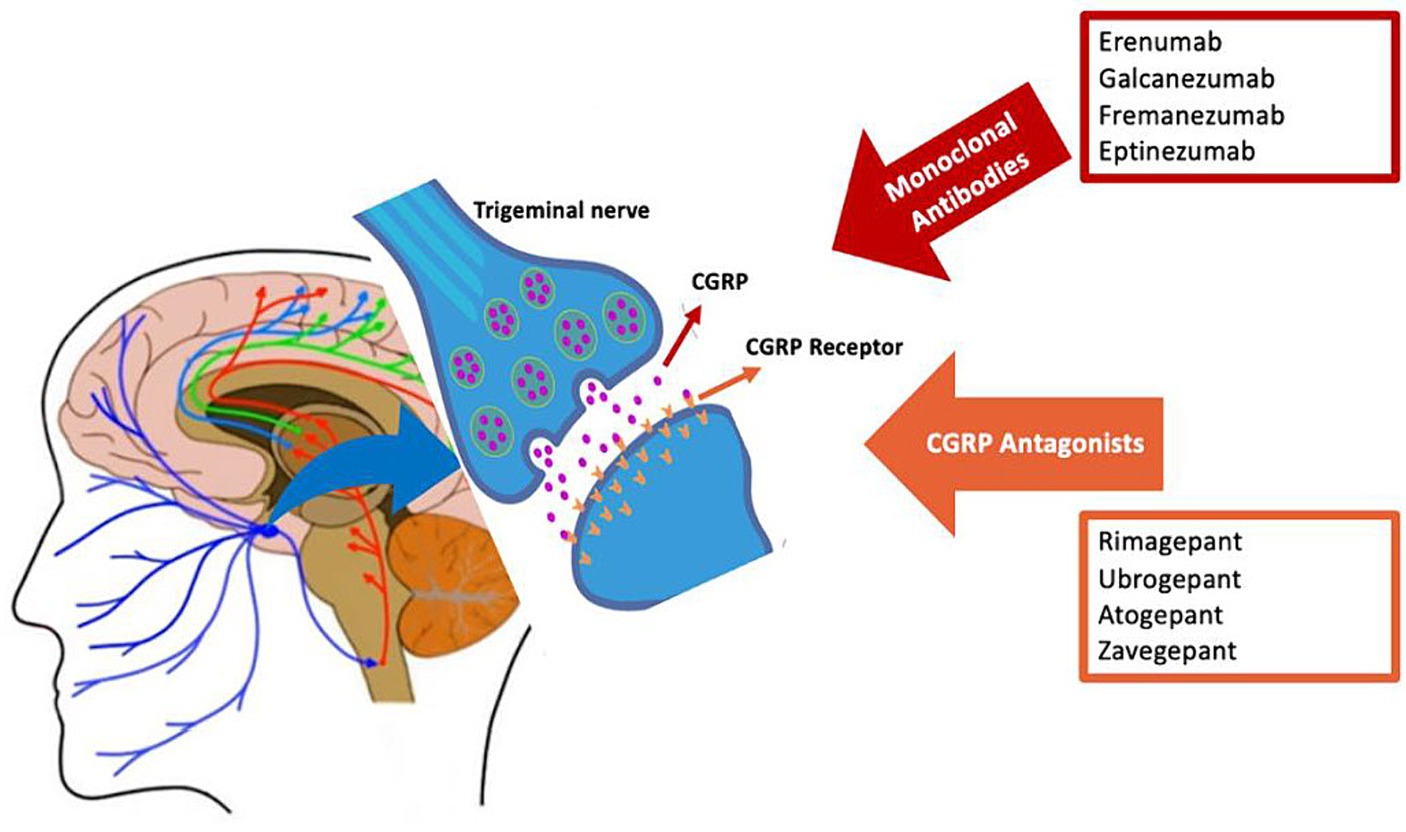
Figure 2. Calcitonin gene-related peptide (CGRP)-targeting drugs for migraine.
Monoclonal antibodies are highly selective for CGRP and CGRP receptors, leading to fewer side effects and drug interactions (27). Currently, there are four monoclonal antibodies available for the preventive treatment of migraine: erenumab, eptinezumab, fremanezumab, and galcanezumab.
Erenumab, an IgG2 CGRP receptor blocker, is the first monoclonal antibody approved for the preventive treatment of migraine in adults (28, 29). In two Phase II trials erenumab was found to be effective and tolerable in chronic migraine patients along with the extension studies (30–33). Phase III STRIVE, ARISE and LIBERTY studies showed similar efficacy and adverse effects on episodic migraine (34–37). Erenumab also showed favorable results in efficacy and tolerability against topiramate in a phase IV comparative study (38). Adverse effects include constipation, injection site reactions, muscle spasms, and pruritus also shown in real world studies (RWS) (35, 39–44). Ongoing research on erenumab is investigating the efficacy and safety of the drug in pediatric patients with episodic and chronic migraine (NCT03836040, NCT03832998). Additionally, a Phase IV trial (NCT04592952) is investigating the efficacy of erenumab in high-frequency episodic headaches. Several RWS have investigated the safety and effectiveness of erenumab, with nearly all studies showing similar results of a reduction in monthly migraine days (MMD) with increased quality of life (40, 42, 45–48). A large RWS study on the impact of erenumab on absenteeism, healthcare resource use, and comorbidities has been completed, but the results have not yet been published (NCT05375097).
Fremanezumab is the second monoclonal antibody approved, available in monthly doses of 225 mg or quarterly doses of 675 mg (28, 49). Phase II and phase III HALO studies demonstrated successful results for both episodic and chronic migraine (50–53). The FOCUS trial also demonstrated favorable results (54). Recruiting studies of fremanezumab on sleep improvement (NCT04693533) and two other studies for the preventive treatment of episodic and chronic migraine in pediatric patients are still ongoing (NCT04530110, NCT04464707). RWS of fremanezumab have demonstrated its efficacy and tolerability regardless of migraine type or prior exposure to a different CGRP monoclonal antibody (55–57). RWS have also disclosed greater efficacy than randomized controlled trials (RCT), with rare treatment emergent adverse events, which were mostly mild conditions such as pain, rash or pruritus, flu-like symptoms, and hair loss (56, 58, 59). Additionally, significant reductions in antidepressant and anxiolytic medication use have been observed (60). The PEARL study is currently recruiting to investigate the effectiveness of fremanezumab (61).
Galcanezumab was approved in 2018 (28, 62). It is administered through subcutaneous (SC) injections, with a loading dose of 240 mg in the first month, followed by monthly 120 mg injections. Phase II and Phase III trials EVOLVE-1 and EVOLVE-2 studies showed efficacy and tolerability with similar results as REGAIN study (63–66). Two ongoing studies of galcanezumab are investigating its efficacy in children with chronic and episodic migraines (NCT04616326, NCT03432286). Another recruiting study is the pilot study of galcanezumab in vestibular migraine (NCT04417361). Several RWS are available all showing favorable results, some showing better results than the clinical trials (67–69). In a large RWS nearly 80.0% of the patients reported a decline in the frequency and in intensity of their headaches (70). Another study showed that galcanezumab was effective in chronic migraine regardless of medication overuse and poor responses were correlated with accompanying depression and everyday headache (68).
Eptinezumab has been approved as the first intravenous (iv.) monoclonal antibody (71, 72). Phase II and phase III PROMISE-1 and PROMISE-2 trials showed efficacy and tolerability (73–76). Long-term results of the PREVAIL and DELIVER studies also confirm the safety of eptinezumab (76, 77). There are ongoing studies for the efficacy in MOH (NCT05452239), also for children and adolescents with episodic and chronic migraine (NCT04965675, NCT05164172), as well as one for adult preventive treatment (NCT04921384). However, there is currently no RWS available yet. All monoclonal antibody and gepant drugs are listed in Table 1 and their studies are summarized in Table 2.
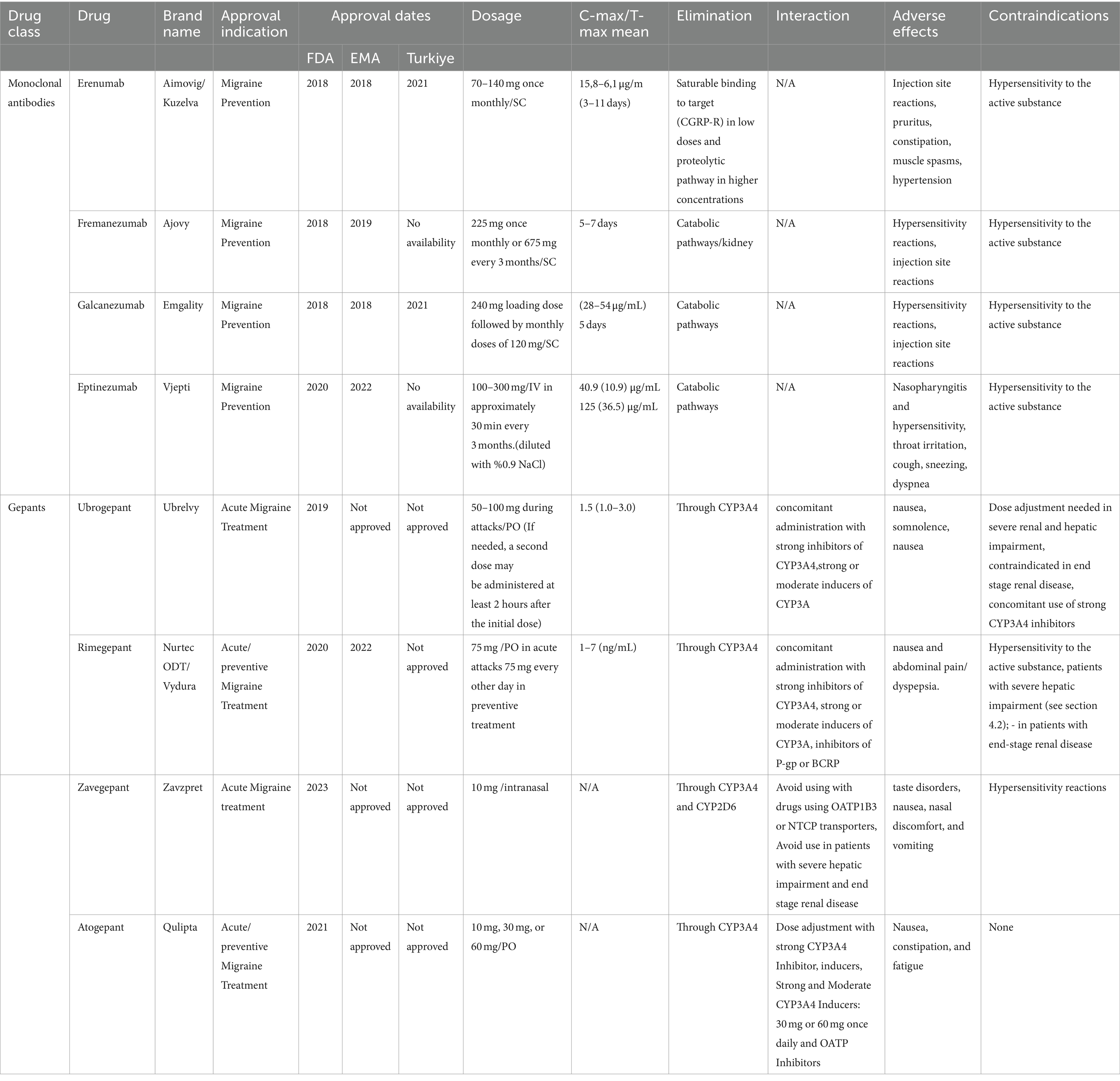
Table 1. Monoclonal antibodies and gepant drugs.
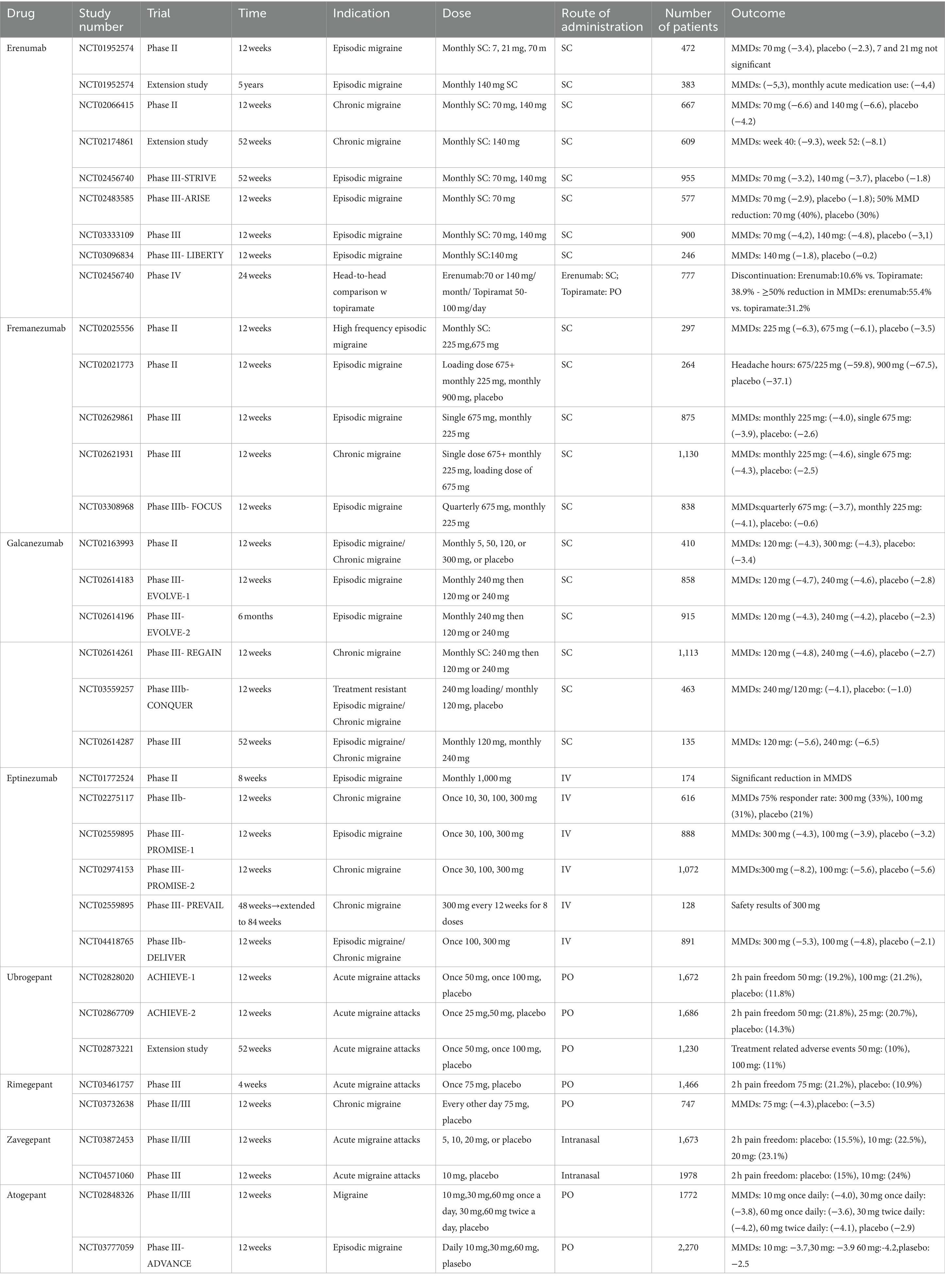
Table 2. Clinical studies of CGRP-targeted treatments.
The gepants are a class of small molecule CGRP antagonists that selectively target CGRP receptors. BIBN4096BS was the first gepant investigated in animal studies, followed by a phase I clinical study in 126 patients, which was found to be effective intravenously for acute attacks (78, 79). Olcegepant was the first gepant studied for acute treatment in migraine, showing superiority over placebo in achieving pain freedom within 2 h (80). However, due to severe paresthesia side effects and low bioavailability, it was no longer studied. Telcagepant was the first oral CGRP receptor antagonist found to be effective in RCTs showing promising results as triptans (81, 82). However, in 2014, telcagepant’s use in preventive treatment was halted due to elevations in transaminase levels (83).
Ubrogepant was approved by FDA in 2019 and EMA in 2022 (84, 85). The recommended doses are 50 mg or 100 mg, with an additional dose allowed at least 2 h after the initial dose if needed, and a maximum daily dose of 200 mg. Phase III ACHIEVE-1 study showed significant results with better relief of bothersome symptoms of migraine. Although elevated aminotransferase levels were detected in 6 patients, the liver safety board concluded that this finding was not related to adverse effects of ubrogepant (86). ACHIEVE-2 study also showed similar results (87). The most common adverse effects were nausea and dizziness (88). Safety results showed no treatment-emergent or cardiac adverse events in another post-hoc analysis in patients with major cardiovascular risk factors (89). Hepatic and renal insufficiency require dose adjustment, with a maximum daily dose of 100 mg, while end-stage renal failure is a contraindication. An extension trial of 52 weeks comparing the safety and tolerability of 50 mg and 100 mg ubrogepant in 1230 patients, revealed same results as previous studies. Upper respiratory tract infection and nausea were reported. Aminotransferase elevation was reported in 20 patients (90). A study comparing almotriptan and ubrogepant (NCT05214001) is still recruiting, and another study is underway to investigate the efficacy of ubrogepant in adolescents and children (NCT05125302). Also, the combination treatment of ubrogepant with atogepant is still being investigated (NCT05653986). Some combination studies have been completed considering ubrogepant and atogepant, but the data is not available to date (NCT05264129, NCT05653986). One small RWS found similar results to the RCTs concerning the efficacy of ubrogepant, but with higher adverse events (91).
Rimegepant is another CGRP receptor antagonist that received approval from both the FDA in 2020 and the EMA in 2022 for the acute and preventive treatment of migraine (72, 92). The maximum daily dose is 75 mg, and it should be avoided in patients with severe renal or hepatic failure (93). Two phase III trials showed favorable results in safety and tolerability for acute migraine treatment. The most common adverse effects were nausea and urinary tract infections, with no serious adverse effects (94, 95). Post-hoc analysis also confirmed these results along with the improved quality of life in patients (96). Long-term safety study showed 75 mg of rimegepant was safe and well-tolerated for the acute treatment of migraine (97). A phase IV study (NCT05211154) is ongoing. Another ongoing phase III study is investigating the long-term safety of rimegepant for the acute treatment of migraine in adolescents and children (NCT04743141). As a phase II/III compared rimegepant 75 mg taken every other day was safe and well-tolerated in the preventive treatment of migraine, it was approved by both the FDA and EMA for the preventive treatment after the studies (92, 98, 99). More investigations of rimegepant are continuing, including both the efficacy and tolerability of rimegepant for the acute and preventive treatment of migraine in adults (NCT05509400, NCT05518123) as well as RWS (NCT05709106). In a study comparing galcanezumab and rimegepant; galcanezumab was not found to be superior to rimegepant; however, both interventions demonstrated efficacy as preventive treatments (100). Another ongoing phase III RCT is evaluating the safety and tolerability of preventive migraine treatment in adolescents and children (NCT05156398). To date, no RWS has been published on the efficacy and safety of rimegepant.
Zavegepant, formerly known as vazegepant, is the first intranasally administered CGRP receptor antagonist that has been approved by the FDA in 2023 in acute migraine treatment (101). A completed phase II/III of zavegepant 10 mg and 20 mg were found to be more effective than placebo in both areas. The most common adverse effects were dysgeusia, nausea, and nasal discomfort No hepatotoxicity was detected (102). Another phase III trial showed favorable results in pain freedom and freedom from the most bothersome symptom (103). Long-term safety and tolerability results of zavegepant were shown by a phase II/III open-label trial (NCT04408794) (104). Another phase II/III study is currently recruiting, investigating the efficacy and safety of zavegepant in the preventive treatment of migraine (NCT04804033).
Atogepant is an FDA-approved oral CGRP receptor antagonist for the preventive treatment of episodic migraine, available in doses of 10 mg, 30 mg, or 60 mg (105). Mild-to-moderate renal and hepatic impairment does not require dose adjustment, while severe hepatic disease is a contraindication. In cases of severe renal impairment or concurrent use of CYP3A4 inhibitors, the maximum daily dose is limited to 10 mg. The first phase II/III trial showed favorable results considering mean decrease in MMDs (106). Nausea, constipation, and fatigue were the most common adverse events, and no liver toxicity was observed. The phase III ADVANCE study showed statistically significant reductions of MMDs (107). A phase III open RCT showed constipation in atogepant group (108). The extended results of the ADVANCE trial over 40 weeks demonstrated that 60 mg of atogepant daily was safe and well-tolerated (109). An observational diary study evaluating the real-world effectiveness of the acute treatment of migraine with ubrogepant when used in combination with atogepant for prevention is planned to finish in April 2024 (NCT05653986). Another study assessing the change in disease activity when ubrogepant and atogepant tablets are combined to treat migraine in adult participants is ongoing and planned to finish in April 2024 (COURAGE II; NCT05653986). There is currently no RWS available for atogepant.
Migraine treatment is guided by various international societies, including those from the International Headache Society (HIS), American Headache Society (AHS), European Headache Federation (EHF), and National Institute of Healthcare and Excellence (NICE). The development of new CGRP-based agents has led to significant changes in migraine treatment perspectives, resulting in the issuance of consensus statements and new treatment guidance by these societies (21, 110–112). In addition, the Health Services General Directorate of Turkiye Ministry of Health published guidelines for migraine treatment in 2020 and is planned to be rearranged (113).
The treatment guidelines for acute migraine vary among different organizations (Table 3). EHF recommendation is stepped care approach, while AHS recommendation is mostly a stratified approach (21, 114). British Association for the Study of Headache (BASH) and Turkiye recommend either a stratified therapy or a stepped care approach depending on the severity of the attack (111, 113). Even in the absence of nausea and vomiting, antiemetics are recommended by NICE and BASH. While EHF and NICE advice against oral ergot alkaloids, the AHS and Turkiye guidelines include ergot derivatives in the acute migraine treatment as patient-based decision in refractory cases. NICE suggests beginning triptan treatment with the least expensive available option, and all guidelines provide an alternative triptan if the primary one is ineffective. NICE and AHS also included neuromodulatory devices in selected cases which showed good tolerability and safety (112, 115, 116). The BASH, NICE, and Turkiye guidelines were established before the development of ditans and gepants; therefore, not yet included in the guidelines. There are ongoing preparations to incorporate gepants and ditans into these guidelines.
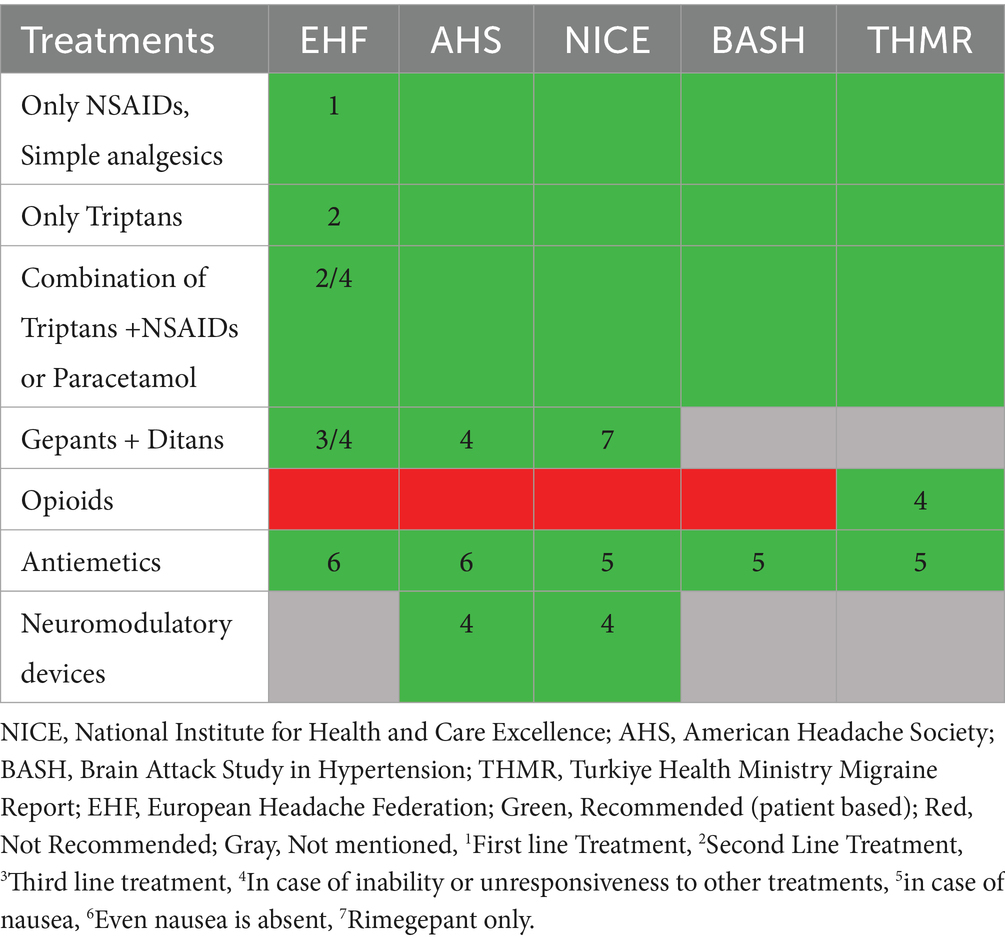
Table 3. Acute treatment recommendations in guidelines.
The preventive treatment guidelines for migraine differ across various medical societies, much like the acute treatment guidelines (Table 4) (21, 111, 112, 117). Up to date guidelines have not yet included eptinezumab and rimegepant for the preventive treatment, despite the fact that rimegepant is approved for migraine prevention by both FDA and EMA. NICE suggests the use of monoclonal antibodies in patients with four or more migraine days in a month who have an inadequate response to three preventive drug treatments. If the frequency does not reduce by 50% in episodic migraine or 30% in chronic migraine after 12 weeks, the treatment is recommended to be stopped. Transcranial magnetic stimulation is recommended in NICE for selected cases (118). AHS also suggests monoclonal agents in patients with four or more migraine days in a month. It is offered in cases of insufficient treatment with traditional agents for 8 weeks or more, if Migraine Disability Assessment (MIDAS) score is more than 11, headache impact test (HIT)-6 > 50 in episodic and chronic migraine, or chronic migraine patients who are unable to tolerate or show inadequate response to a minimum of two quarterly injections (6 months) of onabotulinumtoxinA. Although frovatriptan is not approved as a preventive therapy, it has been included as a preventive choice of medication in AHS guidelines, probably due to its long effect duration. EHF updated the recommendation on the use of monoclonal antibodies targeting the CGRP pathway for migraine prevention as they are effective and safe also in the long-term. The EHF expert panel provides the most detailed guide for CGRP monoclonal antibodies use in preventive treatment for migraine. Investigations and preparations for the new guideline are in progress in Turkiye.
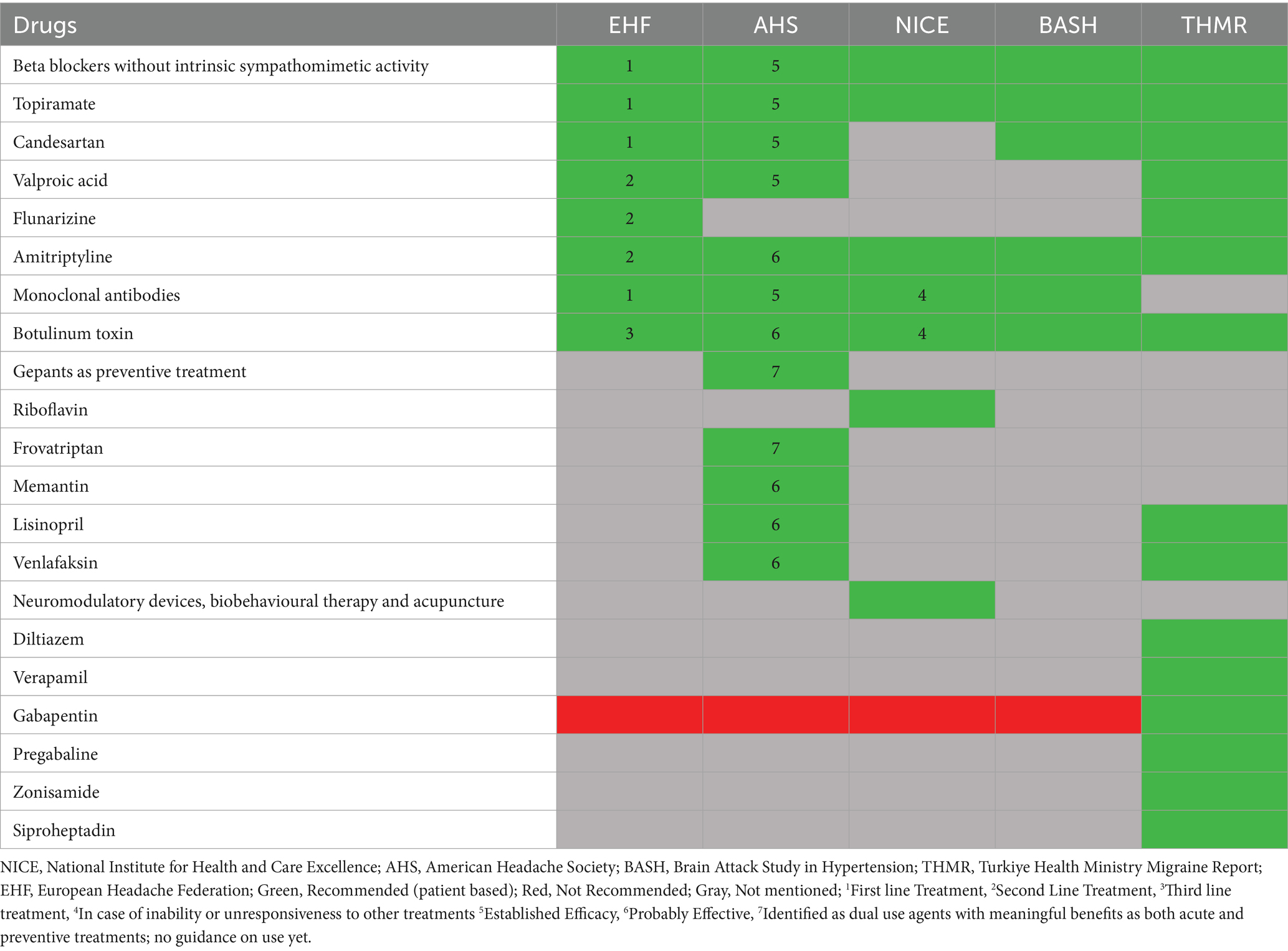
Table 4. Preventive treatment recommendations in guidelines.
Population-based studies as CaMEO and OVERCOME studies have demonstrated that the majority of migraine patients lack an accurate diagnosis and appropriate treatment (119, 120). In a study conducted in Turkiye, it was reported that 22.8% of patients with a definitive diagnosis of migraine had previously been diagnosed with tension-type headache, and 37.1% of patients diagnosed with tension-type headache had previously been diagnosed with sinusitis (121). In another study conducted in our country, 40.9% of migraine patients stated that they had previously been diagnosed with tension-type headache. Possible explanations for this difference include the symptoms not meeting definitive migraine diagnostic criteria in previous physician evaluations, the variable nature of migraine, or the alternation between migraine and tension-type headache (122). In Turkiye, headache treatment is offered through governmental hospitals, university hospitals free of charge for individuals covered by social security, as well as private hospitals. Unlike some other countries, patients in Turkiye, have the ability to directly consult a neurologist for headache complaints, although visit durations are typically very brief within the social security system. The neurology consultation periods are shortened due to intense patients load, the initial diagnosis and management of numerous migraine patients is believed to be incomplete. The MIRA-Neurology study group stated that headache complaint caused at least 1/3 of all neurological outpatient visits in Turkiye and 2/3 of all patients admitted to neurology clinics had headache (123). This suggests that awareness of migraine in our society may have grown over time, leading to a shift in patient preference toward consulting neurologists. Such a trend is highly beneficial as it promotes early initiation of appropriate treatment for migraine patients, potentially lowering rates of chronicity. Examining the global data from the “My Migraine Voice” health survey, it was found that the initial healthcare provider sought by patients was typically a general practitioner (53%) (124). This contrasts with the trends observed in Türkiye, possibly due to the emphasis on encouraging patients to seek care from primary health services, a distinction from healthcare policies in other nations. In terms of workforce loss, the rates of patients reporting that migraine affects their professional lives were notably higher in Türkiye compared to global data (125). While the burden of migraine in Türkiye is similar to other countries, the remarkable high number of emergency room visits compared to other countries imposes a significant financial and operational strain on the “free” healthcare system provided by the social security system. To alleviate this burden, it is necessary to create special guidelines for primary care physicians, thus the diagnosis and treatment of migraine patients will not be initiated only by neurologists. Additionally, these guidelines may outline algorithms for determining when patients should be referred to specialized centers. The existing guidelines and algorithms for neurologists in Turkiye, encompassing all the latest treatments, should be revised and updated. Regular and standardized effective trainings are crucial to keep neurologists well-informed and updated about the diagnosis and treatment of migraine. Furthermore, there is a necessity to enhance the scientific content available to doctors on social media platforms, ensuring it is both increased and kept current. It is strongly advisable for hospitals to establish headache outpatient clinics with specialized physicians if they are not already in place. This helps prevent inaccurate or incomplete diagnoses and ensures optimal patient care.
Studies from Turkiye showed only 43.1% of the patients were using medications under the supervision of a physician and only 2.9% of them were using migraine specific medication during acute attacks (121). Migraine-specific treatments are subject to prescription limits in some countries similar to Turkiye leading to inadequate access and treatment with triptans. This results in patients transitioning to other over-the-counter (OTC) analgesics, leading to OTC related MOH (125, 126). Although ergot alkaloids are not used in Europe and United States, they are still being prescribed for moderate–severe attacks in selected cases. Despite this, patients tend to use “cheap” drugs regardless of the attack severity in Turkiye. Furthermore, commercial availability of many triptans is restricted, greatly reducing the effectiveness of acute attack treatments. On the contrary, unlike many countries the available triptans can be purchased without prescription which may lead to MOH eventually. Despite the licensing of erenumab, and galcanezumab in Turkiye, obtaining these drugs remains challenging for patients due to lack of insurance coverage, it creates a significant barrier to access to medicines for patients in need. Efforts should be made to enhance accessibility to all acute treatment agents in our country. Effective treatment of not only the acute attack of migraine but also the accompanying symptoms is important for the quality of life of patients. Patients, hindered by photophobia are unable to drive and may find themselves in distressing situations due to nausea. To avert such scenarios, there is a need for treatments that can swiftly and effectively halt the migraine attack. The drugs to be used during acute attack treatment should not have the potential for side effects that could affect the daily life of patients.
Research indicates that only 10% of individuals receive preventive treatment, despite the fact that preventive medication could benefit over 40% of episodic migraine sufferers (127). Similarly, it was reported that only 4.9% of the patients received prophylactic treatment in Turkiye, although the monthly number of attacks was four and above in more than half of the patients with migraine (121). The timely initiation of preventive treatment in eligible patients will also serve to mitigate MOH resulting from excessive drug usage. Preventive treatments that are rapidly effective, devoid of potential side effects, and do not necessitate a wash-out period are in demand.
CGRP antagonists, the sole migraine-specific compounds at present, seem to be currently positioned at the bottom among all available treatments. The reason for this is primarily attributed to their high cost and the absence of reimbursement policies, which significantly limit access for many individuals. Furthermore, the long-term effects of most molecules are unknown, and speculation suggests that long-term CGRP suppression with the injectable molecules may have negative effects on cardiovascular health, bone density, and immune function (128). Erenumab and galcanezumab have been approved for use in Turkiye, patients continue to have difficulty accessing these drugs because of the lack of full coverage of these drugs by social security agency and private insurance companies. These obstacles suggest a need for more streamlined and affordable migraine treatment options in Turkiye. Advancements in technology allow for a clearer understanding of the mechanisms behind existing treatments, and ongoing studies on migraine pathophysiology have the potential to contribute significantly to the development of more targeted and specific treatments for migraines.
Tailoring treatment plans to individual patient characteristics remains a challenge. Every treatment modality should be evaluated closely, particularly in chronic migraine patients. The discontinuation of migraine prophylaxis is also an important consideration in this context. It is crucial to individually assess the response to treatment, any encountered adverse effects, and the overall efficacy of the preventive therapy in managing migraine symptoms, taking into account the specific needs of the patient (129).
Many genetic and environmental factors are involved in the etiology of migraine. It has been stated that hereditary factors contribute to the etiology of migraine in the range of 34 to 57%. However, the genetic background is not well defined due to its inherent heterogeneity. Studies suggest that the 5-HTR2C rs3813929 and TNF-a-308G/A polymorphism can be a genetic risk factor for migraine in the Turkish population (130, 131). Pain perception and response mechanisms also differ among individuals and in HEAD-MENAA study, lifetime pain duration of the patients admitted to neurology clinics was significantly longer in the Middle East and Turkiye than in the other regions (132). Through advancements in precision medicine, healthcare providers aim to craft treatment plans that optimize efficacy while minimizing side effects for each patient. This approach extends beyond focusing solely on symptom relief, encompassing the broader aspects of a patient’s life, including their emotional well-being and daily functioning and aims to improve quality of life.
Migraine often coexists with other conditions and diseases, such as mood disorders, sleep disturbances and cardiovascular events (133). In addition to medical interventions for sleep disorders and stress, patients can be guided toward cognitive-behavioral treatments. Integrating comprehensive care that addresses these comorbidities is a key unmet need. Managing and treating the underlying comorbid conditions play a significant role in minimizing migraine attacks and enhancing the efficacy of treatments.
Involves addressing not only the acute symptoms but also considering the broader aspects of a patient’s physical, emotional, and social well-being. Holistic care includes lifestyle modifications, stress management, dietary considerations, and other non-pharmacological interventions alongside traditional medical treatments. As migraine is a condition characterized by multi-aspect and complex pathophysiology, its treatment should not be confined solely to neurologists. Instead, a multidisciplinary assessment involving other physicians is essential, considering the underlying psychosocial conditions. Support from non-medical professionals, such as dietitians, psychologists, and life coaches, is valuable to provide comprehensive care (134). In addition to the patient’s adherence to migraine treatment, patient’s treatment response is likely to improve with lifestyle modifications, including addressing sleep issues, managing screen exposure, practicing stress management, engaging in regular exercise, and adjusting diet.
Social determinants, geographic and geo-economic disparities, economic burden, cultural misconceptions, limited resources and overburdened healthcare services, and stigma are the main factors in difficulty to access to migraine treatment by taking into account a local and global scale (135, 136). Economically, disparities in income and healthcare coverage significantly impact individuals’ ability to access headache treatment. Despite Turkiye providing free access to public healthcare systems and diagnostic examinations, prolonged waiting periods may ensue due to the large influx of patients. Disparities in headache diagnosis, treatment, and management become particularly apparent, especially in rural regions lacking sufficient healthcare resources. Furthermore, the absence of insurance coverage for certain medications including CGRP monoclonal antibodies and specialized treatments presents a barrier for low-income patients seeking adequate treatment. Hence, patient education and awareness is also an essential component of migraine management. In a study, adding patient education to routine migraine medical treatment resulted in a reduction in mean headache days per month and a greater reduction in functionally incapacitating headache days per month, less analgesic overuse, increased adherence therapy, and made fewer headache-related calls to the clinic (137). Patients, in particular, ought to trust their physicians and adhere to the prescribed treatments consistently. In Turkiye, patients frequently rely on medications suggested by their social circle, and some opt to directly visit the pharmacy instead of consulting a doctor. They purchase medications and use them inconsistently. Empowering patients with education enable them to make informed decisions about their health and engage more effectively in their treatment plans. The establishment of migraine-specific patient associations and support groups is essential. Health authorities and associations should disseminate accurate information through brochures, social media, and TV announcements to enhance awareness and support.
Barriers to achieve optimal migraine treatment and suggestions to improve treatment management in migraine, respectively, presented in Figures 3, 4.
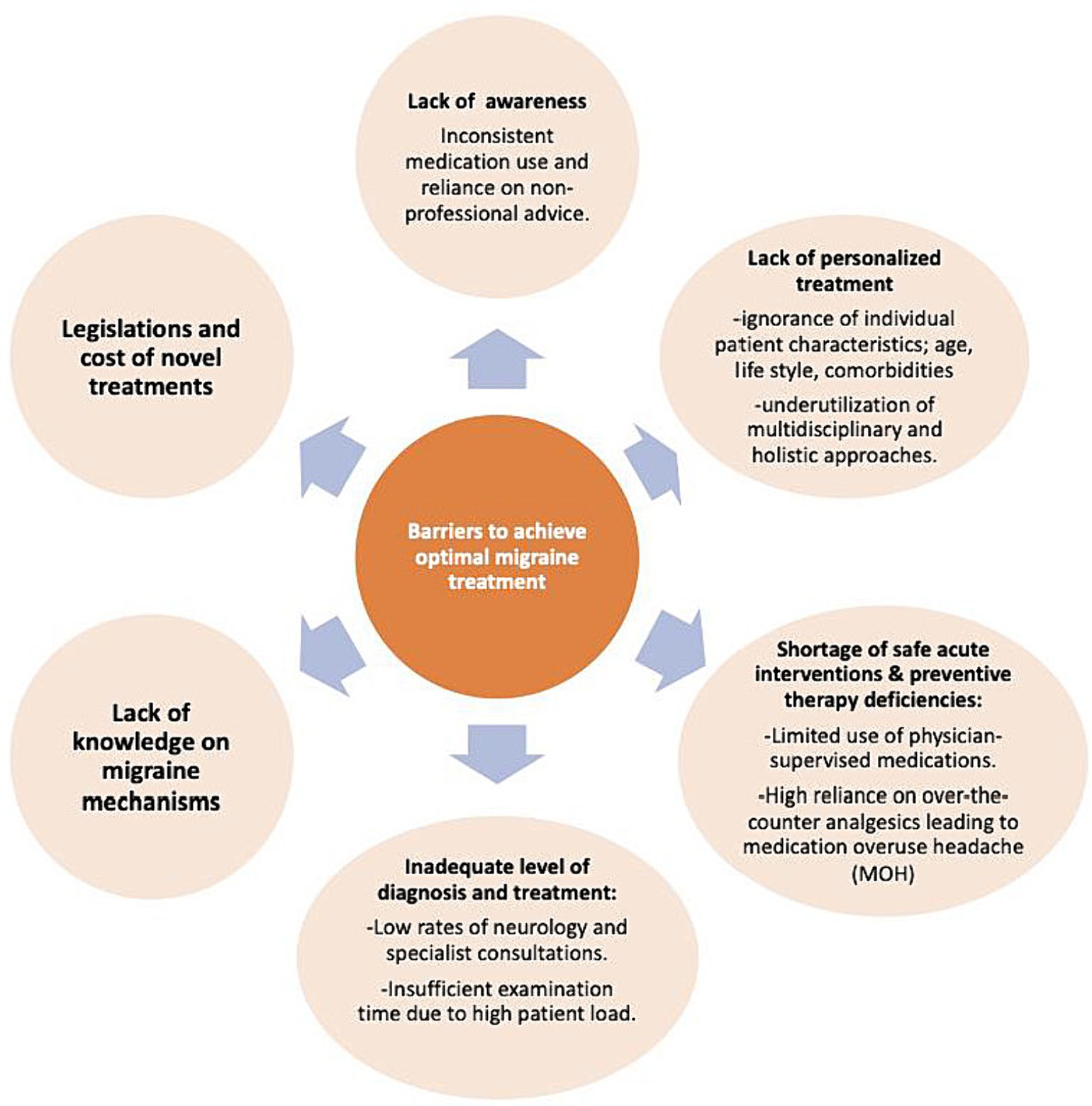
Figure 3. Barriers to achieve optimal migraine treatment.
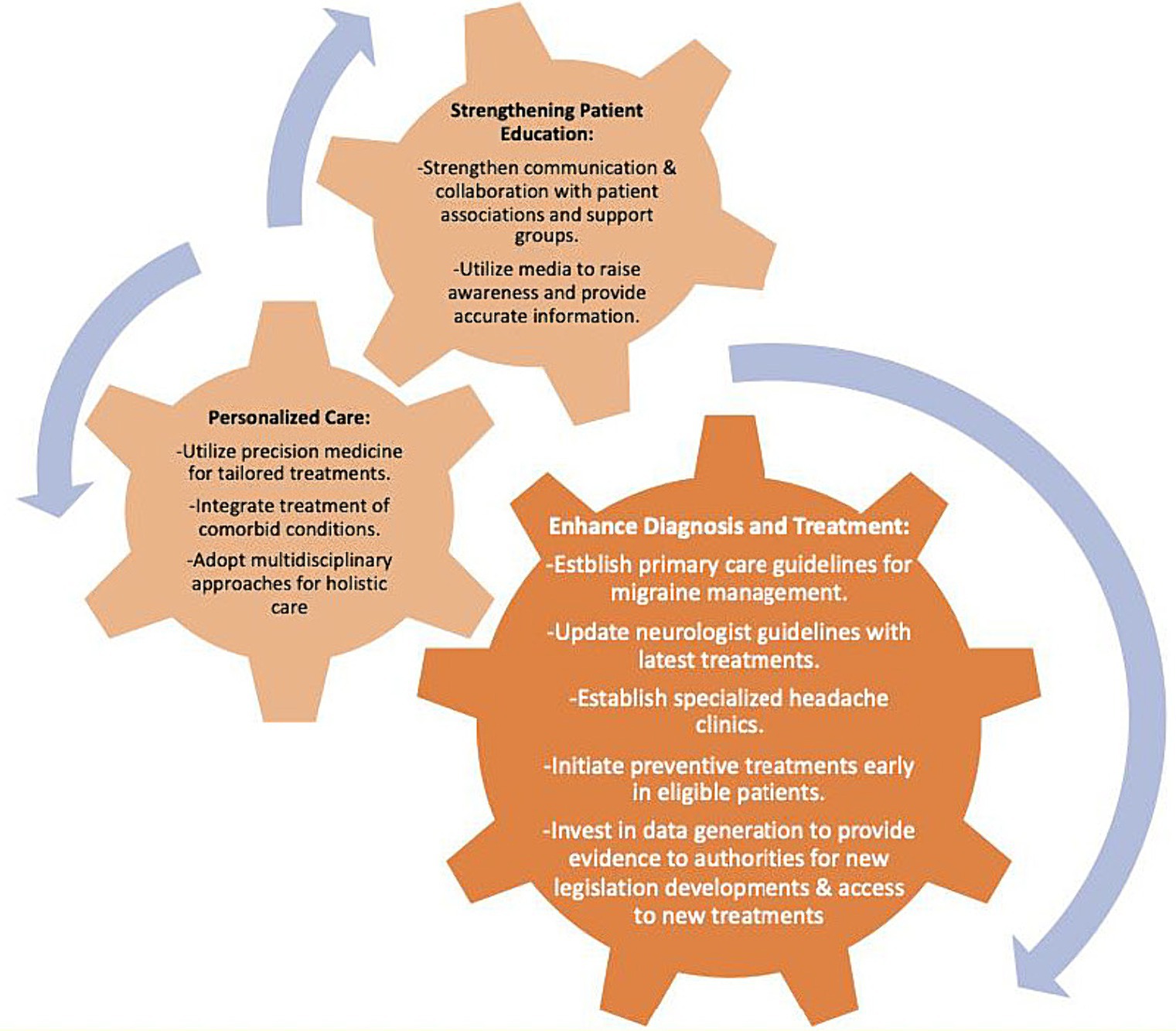
Figure 4. Suggestions to improve treatment management in migraine.
In light of recent advancements in migraine research and treatment modalities, it is imperative to engage in a comprehensive discussion regarding the challenges of managing migraine in the contemporary healthcare landscape. Personal viewpoints play a pivotal role in shaping the discourse surrounding migraine management, as they provide insights into individual experiences, preferences, and treatment outcomes. By fostering a more engaging dialog, healthcare professionals can collaboratively explore the multifaceted challenges encountered in migraine care, including medication adherence, treatment efficacy, and the impact of comorbidities on overall management strategies. Furthermore, addressing patient-specific concerns and incorporating patient perspectives into treatment decisions are essential components of a patient-centered approach to migraine care. Through open and transparent communication, coupled with a thorough understanding of the evolving therapeutic landscape, healthcare providers can navigate the complexities of migraine management more effectively, ultimately improving patient outcomes and quality of life.
Obstacles in migraine treatment include poor specification in migraine therapies, lack of tailored treatment plans, accurate diagnosis and appropriate treatment eventually leading to MOH, inadequate time in evaluation due to high rate of outpatient clinic visit numbers, limited access to specialists, unavailability of some of the new treatment options for effective acute and preventive treatment. Researchers have sought innovative strategies for migraine specified therapies such as CGRP-targeting drugs. However, high costs and limited long-term data on these drugs present challenges to widespread adoption. Other strategies to overcome the aforementioned obstacles can be listed as establishing guidelines and algorithms for primary care physicians, establishing diseases specified outpatient clinics in available centers, sharing the latest scientific content with doctors and help them keep updated with the new medications, efforts in enhancing accessibility of new treatment options in all countries, education of patients about treatment options, changes of life style and holistic approaches. Also creating patient groups and informative messages through mass media by the health authorities can be useful.
AÖ: Writing – review & editing. BB: Writing – review & editing. ŞB: Writing – review & editing. ME: Writing – review & editing. AA: Writing – review & editing. SG: Writing – review & editing. NK: Writing – review & editing.
The authors declare that this study received funding from Pfizer to cover the cost of Remedium Consulting Group. Pfizer was not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication. Remedium Consulting Group were involved in medical writing assistance, project and author coordination support and submission assistance.
Medical writing assistance, project and author coordination support including submission assistance was provided by Ayşe Özlem Yılmaz and Ferda Kızıltaş at Remedium Consulting Group.
AÖ board member of IHS, current president of GMPS, advisory board of TEVA, Abbvie, Lilly and Pfizer Pharmaceuticals; lecturer for additionally İlko, Abdi İbrahim, Biofarma, Drogsan Pharmaceuticals and have loyalty from Springer books. BB has acted in advisory board of Takeda and Pfizer Pharmaceuticals and has received speaker honorarium from Lilly and Novartis. ŞB has acted in advisory board of Novartis, Amgen, Pfizer Pharmaceuticals, and has received speaker honorarium from Novartis. AA has acted in advisory board of Pfizer Pharmaceuticals. ME has acted in advisory board of Novartis and Pfizer Pharmaceuticals, and has received speaker honorarium from Novartis, Lilly, Abdi İbrahim Pharmaceuticals and Ali Raif Pharmaceuticals. SG is an employee of Pfizer. NK has acted in advisory board of Novartis, AbbVie, Amgen, Lilly and Pfizer Pharmaceuticals, and has received speaker honorarium from Novartis.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Safiri, S, Pourfathi, H, Eagan, A, Mansournia, MA, Khodayari, MT, Sullman, MJM, et al. Global, regional, and national burden of migraine in 204 countries and territories, 1990 to 2019. Pain. (2022) 163:e293–309. doi: 10.1097/j.pain.0000000000002275
2. Baykan, B, Ertas, M, Karlı, N, Uluduz, D, Uygunoglu, U, Ekizoglu, E, et al. Migraine incidence in 5 years: a population-based prospective longitudinal study in Turkey. J Headache Pain. (2015) 16:103. doi: 10.1186/s10194-015-0589-2
3. Lipton, RB, Bigal, ME, Diamond, M, Freitag, F, Reed, ML, and Stewart, WF. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology. (2007) 68:343–9. doi: 10.1212/01.wnl.0000252808.97649.21
4. Buse, DC, Manack, AN, Fanning, KM, Serrano, D, Reed, ML, Turkel, CC, et al. Chronic migraine prevalence, disability, and sociodemographic factors: results from the American migraine prevalence and prevention study. Headache. (2012) 52:1456–70. doi: 10.1111/j.1526-4610.2012.02223.x
5. Burch, RC, Buse, DC, and Lipton, RB. Migraine: epidemiology, burden, and comorbidity. Neurol Clin. (2019) 37:631–49. doi: 10.1016/j.ncl.2019.06.001
6. Dodick, DW. A phase-by-phase review of migraine pathophysiology. Headache. (2018) 58:4–16. doi: 10.1111/head.13300
7. Charles, A. The pathophysiology of migraine: implications for clinical management. Lancet Neurol. (2018) 17:174–82. doi: 10.1016/S1474-4422(17)30435-0
8. Goadsby, PJ, Holland, PR, Martins-Oliveira, M, Hoffmann, J, Schankin, C, and Akerman, S. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev. (2017) 97:553–622. doi: 10.1152/physrev.00034.2015
9. Grangeon, L, Lange, KS, Waliszewska-Prosół, M, Onan, D, Marschollek, K, Wiels, W, et al. Genetics of migraine: where are we now? J Headache Pain. (2023) 24:12. doi: 10.1186/s10194-023-01547-8
10. Oguz Akarsu, E, Baykan, B, Ertas, M, Zarifoglu, M, Orhan, EK, Saip, S, et al. The persistence versus interchangeability of migraine and tension-type headaches in a 5-year population-based validated survey. Cephalalgia: Int J Headache. (2020) 40:39–48. doi: 10.1177/0333102419852359
11. Vargas, BB. Tension-type headache and migraine: two points on a continuum? Curr Pain Headache Rep. (2008) 12:433–6. doi: 10.1007/s11916-008-0073-7
12. Karli, N, Bican, A, and Zarifoğlu, M. Course of adolescent headache: 4-year annual face-to-face follow-up study. J Headache Pain. (2010) 11:327–34. doi: 10.1007/s10194-010-0228-x
13. Dodick, DW. Migraine. Lancet (London, England). (2018) 391:1315–30. doi: 10.1016/S0140-6736(18)30478-1
14. Silberstein, SD. Preventive migraine treatment. Continuum (Minneapolis, Minn). (2015) 21:973–89. doi: 10.1212/CON.0000000000000199
15. Pietrobon, D, and Striessnig, J. Neurobiology of migraine. Nature reviews. Neuroscience. (2003) 4:386–98. doi: 10.1038/nrn1102
16. Ashina, M, Hansen, JM, Do, TP, Melo-Carrillo, A, Burstein, R, and Moskowitz, MA. Migraine and the trigeminovascular system-40 years and counting. Lancet Neurol. (2019) 18:795–804. doi: 10.1016/S1474-4422(19)30185-1
17. Charles, A, and Pozo-Rosich, P. Targeting calcitonin gene-related peptide: a new era in migraine therapy. Lancet (London, England). (2019) 394:1765–74. doi: 10.1016/S0140-6736(19)32504-8
18. Schoenen, J, Vandersmissen, B, Jeangette, S, Herroelen, L, Vandenheede, M, Gérard, P, et al. Migraine prevention with a supraorbital transcutaneous stimulator: a randomized controlled trial. Neurology. (2013) 80:697–704. doi: 10.1212/WNL.0b013e3182825055
19. Karlı, N, Bıçakçı, Ş, and Mehtar, BM. CGRP: new Focus in migraine. Turkish J Neurol. (2022) 28:1–5. doi: 10.4274/tnd.2022.88027
20. Burch, R. Preventive migraine treatment. Continuum (Minneapolis, Minn). (2021) 27:613–32. doi: 10.1212/CON.0000000000000957
21. Eigenbrodt, AK, Ashina, H, Khan, S, Diener, HC, Mitsikostas, DD, Sinclair, AJ, et al. Diagnosis and management of migraine in ten steps. Nat Rev Neurol. (2021) 17:501–14. doi: 10.1038/s41582-021-00509-5
22. Tassorelli, C, Grazzi, L, de Tommaso, M, Pierangeli, G, Martelletti, P, Rainero, I, et al. Noninvasive vagus nerve stimulation as acute therapy for migraine: the randomized PRESTO study. Neurology. (2018) 91:e364–73. doi: 10.1212/WNL.0000000000005857
23. Lan, L, Zhang, X, Li, X, Rong, X, and Peng, Y. The efficacy of transcranial magnetic stimulation on migraine: a meta-analysis of randomized controlled trails. J Headache Pain. (2017) 18:86. doi: 10.1186/s10194-017-0792-4
24. Wells, RE, Burch, R, Paulsen, RH, Wayne, PM, Houle, TT, and Loder, E. Meditation for migraines: a pilot randomized controlled trial. Headache. (2014) 54:1484–95. doi: 10.1111/head.12420
25. Andrasik, F, Grazzi, L, D'Amico, D, Sansone, E, Leonardi, M, Raggi, A, et al. Mindfulness and headache: a "new" old treatment, with new findings. Cephalalgia: Int J Headache. (2016) 36:1192–205. doi: 10.1177/0333102416667023
26. Edvinsson, L. CGRP and migraine: from bench to bedside. Rev Neurol. (2021) 177:785–90. doi: 10.1016/j.neurol.2021.06.003
27. de Vries, T, Villalón, CM, and MaassenVanDenBrink, A. Pharmacological treatment of migraine: CGRP and 5-HT beyond the triptans. Pharmacol Ther. (2020) 211:107528. doi: 10.1016/j.pharmthera.2020.107528
28. Novel Drug Approvals for 2018. (2018). Available at: https://www.fda.gov/NewsEvents/Newsroom/PressAnnouncements/ucm608120.htm
29. Agency, EM. Erenumab Approval (2018). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/aimovig#authorisation-details-section
30. Sun, H, Dodick, DW, Silberstein, S, Goadsby, PJ, Reuter, U, Ashina, M, et al. Safety and efficacy of AMG 334 for prevention of episodic migraine: a randomised, double-blind, placebo-controlled, phase 2 trial. Lancet Neurol. (2016) 15:382–90. doi: 10.1016/S1474-4422(16)00019-3
31. Tepper, S, Ashina, M, Reuter, U, Brandes, JL, Doležil, D, Silberstein, S, et al. Safety and efficacy of erenumab for preventive treatment of chronic migraine: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. (2017) 16:425–34. doi: 10.1016/S1474-4422(17)30083-2
32. Ashina, M, Goadsby, PJ, Reuter, U, Silberstein, S, Dodick, DW, Xue, F, et al. Long-term efficacy and safety of erenumab in migraine prevention: results from a 5-year, open-label treatment phase of a randomized clinical trial. Eur J Neurol. (2021) 28:1716–25. doi: 10.1111/ene.14715
33. Tepper, SJ, Ashina, M, Reuter, U, Brandes, JL, Doležil, D, Silberstein, SD, et al. Long-term safety and efficacy of erenumab in patients with chronic migraine: results from a 52-week, open-label extension study. Cephalalgia: Int J Headache. (2020) 40:543–53. doi: 10.1177/0333102420912726
34. Goadsby, PJ, Reuter, U, Hallström, Y, Broessner, G, Bonner, JH, Zhang, F, et al. A controlled trial of Erenumab for episodic migraine. New England J Med. (2017) 377:2123–32. doi: 10.1056/NEJMoa1705848
35. Dodick, DW, Ashina, M, Brandes, JL, Kudrow, D, Lanteri-Minet, M, Osipova, V, et al. ARISE: a phase 3 randomized trial of erenumab for episodic migraine. Cephalalgia. (2018) 38:1026–37. doi: 10.1177/0333102418759786
36. Reuter, U, Goadsby, PJ, Lanteri-Minet, M, Wen, S, Hours-Zesiger, P, Ferrari, MD, et al. Efficacy and tolerability of erenumab in patients with episodic migraine in whom two-to-four previous preventive treatments were unsuccessful: a randomised, double-blind, placebo-controlled, phase 3b study. Lancet (London, England). (2018) 392:2280–7. doi: 10.1016/S0140-6736(18)32534-0
37. Goadsby, PJ, Reuter, U, Lanteri-Minet, M, da Silva, P, Lima, G, Hours-Zesiger, P, et al. Long-term efficacy and safety of Erenumab: results from 64 weeks of the LIBERTY study. Neurology. (2021) 96:e2724–35. doi: 10.1212/WNL.0000000000012029
38. Reuter, U, Ehrlich, M, Gendolla, A, Heinze, A, Klatt, J, Wen, S, et al. Erenumab versus topiramate for the prevention of migraine - a randomised, double-blind, active-controlled phase 4 trial. Cephalalgia: Int J Headache. (2022) 42:108–18. doi: 10.1177/03331024211053571
39. Kanaan, S, Hettie, G, Loder, E, and Burch, R. Real-world effectiveness and tolerability of erenumab: a retrospective cohort study. Cephalalgia: Int J Headache. (2020) 40:1511–22. doi: 10.1177/0333102420946725
40. Scheffler, A, Messel, O, Wurthmann, S, Nsaka, M, Kleinschnitz, C, Glas, M, et al. Erenumab in highly therapy-refractory migraine patients: first German real-world evidence. J Headache Pain. (2020) 21:84. doi: 10.1186/s10194-020-01151-0
41. Becker, WJ, Spacey, S, Leroux, E, Giammarco, R, Gladstone, J, Christie, S, et al. A real-world, observational study of erenumab for migraine prevention in Canadian patients. Headache. (2022) 62:522–9. doi: 10.1111/head.14291
42. Khalil, M, Moreno-Ajona, D, Villar-Martínez, MD, Greenwood, F, Hoffmann, J, and Goadsby, PJ. Erenumab in chronic migraine: experience from a UK tertiary Centre and comparison with other real-world evidence. Eur J Neurol. (2022) 29:2473–80. doi: 10.1111/ene.15364
43. Guerzoni, S, Baraldi, C, Pensato, U, Favoni, V, Lo Castro, F, Cainazzo, MM, et al. Chronic migraine evolution after 3 months from erenumab suspension: real-world-evidence-life data. Neurolog Sci: Official J Italian Neurolog Society Italian Society of Clin Neurophysiol. (2022) 43:3823–30. doi: 10.1007/s10072-022-05870-x
44. Gantenbein, AR, Agosti, R, Kamm, CP, Landmann, G, Meier, N, Merki-Feld, GS, et al. Swiss QUality of life and healthcare impact assessment in a real-world Erenumab treated migraine population (SQUARE study): interim results. J Headache Pain. (2022) 23:142. doi: 10.1186/s10194-022-01515-8
45. Russo, A, Silvestro, M, Scotto di Clemente, F, Trojsi, F, Bisecco, A, Bonavita, S, et al. Multidimensional assessment of the effects of erenumab in chronic migraine patients with previous unsuccessful preventive treatments: a comprehensive real-world experience. J Headache Pain. (2020) 21:69. doi: 10.1186/s10194-020-01143-0
46. Raffaelli, B, Kalantzis, R, Mecklenburg, J, Overeem, LH, Neeb, L, Gendolla, A, et al. Erenumab in chronic migraine patients who previously failed five first-line Oral prophylactics and OnabotulinumtoxinA: a dual-center retrospective observational study. Front Neurol. (2020) 11:417. doi: 10.3389/fneur.2020.00417
47. Cheng, S, Jenkins, B, Limberg, N, and Hutton, E. Erenumab in chronic migraine: an Australian experience. Headache. (2020) 60:2555–62. doi: 10.1111/head.13968
48. Troy, E, Shrukalla, AA, Buture, A, Conaty, K, Macken, E, Lonergan, R, et al. Medium-term real-world data for erenumab in 177 treatment resistant or difficult to treat chronic migraine patients: persistence and patient reported outcome measures after 17-30 months. J Headache Pain. (2023) 24:5. doi: 10.1186/s10194-022-01536-3
49. EMA. Approval of Fremanezumab. (2019). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/ajovy
50. Bigal, ME, Dodick, DW, Rapoport, AM, Silberstein, SD, Ma, Y, Yang, R, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of high-frequency episodic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2b study. Lancet Neurol. (2015) 14:1081–90. doi: 10.1016/S1474-4422(15)00249-5
51. Bigal, ME, Edvinsson, L, Rapoport, AM, Lipton, RB, Spierings, EL, Diener, HC, et al. Safety, tolerability, and efficacy of TEV-48125 for preventive treatment of chronic migraine: a multicentre, randomised, double-blind, placebo-controlled, phase 2b study. Lancet Neurol. (2015) 14:1091–100. doi: 10.1016/S1474-4422(15)00245-8
52. Dodick, DW, Silberstein, SD, Bigal, ME, Yeung, PP, Goadsby, PJ, Blankenbiller, T, et al. Effect of Fremanezumab compared with placebo for prevention of episodic migraine: a randomized clinical trial. JAMA. (2018) 319:1999–2008. doi: 10.1001/jama.2018.4853
53. Silberstein, SD, Dodick, DW, Bigal, ME, Yeung, PP, Goadsby, PJ, Blankenbiller, T, et al. Fremanezumab for the preventive treatment of chronic migraine. N Engl J Med. (2017) 377:2113–22. doi: 10.1056/NEJMoa1709038
54. Ferrari, MD, Diener, HC, Ning, X, Galic, M, Cohen, JM, Yang, R, et al. Fremanezumab versus placebo for migraine prevention in patients with documented failure to up to four migraine preventive medication classes (FOCUS): a randomised, double-blind, placebo-controlled, phase 3b trial. Lancet (London, England). (2019) 394:1030–40. doi: 10.1016/S0140-6736(19)31946-4
55. Driessen, MT, Cohen, JM, Thompson, SF, Patterson-Lomba, O, Seminerio, MJ, Carr, K, et al. Real-world effectiveness after initiating fremanezumab treatment in US patients with episodic and chronic migraine or difficult-to-treat migraine. J Headache Pain. (2022) 23:56. doi: 10.1186/s10194-022-01415-x
56. Barbanti, P, Egeo, G, Aurilia, C, Torelli, P, Finocchi, C, d'Onofrio, F, et al. Early and sustained efficacy of fremanezumab over 24-weeks in migraine patients with multiple preventive treatment failures: the multicenter, prospective, real-life FRIEND2 study. J Headache Pain. (2023) 24:30. doi: 10.1186/s10194-023-01561-w
57. McAllister, P, Lamerato, L, Krasenbaum, LJ, Cohen, JM, Tangirala, K, Thompson, S, et al. Real-world impact of fremanezumab on migraine symptoms and resource utilization in the United States. J Headache Pain. (2021) 22:156. doi: 10.1186/s10194-021-01358-9
58. Argyriou, AA, Dermitzakis, EV, Xiromerisiou, G, Rallis, D, Soldatos, P, Litsardopoulos, P, et al. Efficacy and safety of fremanezumab for migraine prophylaxis in patients with at least three previous preventive failures: prospective, multicenter, real-world data from a Greek registry. Eur J Neurol. (2023) 30:1435–42. doi: 10.1111/ene.15740
59. Driessen, MT, Cohen, JM, Patterson-Lomba, O, Thompson, SF, Seminerio, M, Carr, K, et al. Real-world effectiveness of fremanezumab in migraine patients initiating treatment in the United States: results from a retrospective chart study. J Headache Pain. (2022) 23:47. doi: 10.1186/s10194-022-01411-1
60. Krasenbaum, LJ, Pedarla, VL, Thompson, SF, Tangirala, K, Cohen, JM, and Driessen, MT. A real-world study of acute and preventive medication use, adherence, and persistence in patients prescribed fremanezumab in the United States. J Headache Pain. (2022) 23:54. doi: 10.1186/s10194-022-01413-z
61. Ashina, M, Amin, FM, Kokturk, P, Cohen, JM, Konings, M, Tassorelli, C, et al. PEARL study protocol: a real-world study of fremanezumab effectiveness in patients with chronic or episodic migraine. Pain Manag. (2021) 11:647–54. doi: 10.2217/pmt-2021-0015
62. EMA. Galcanezumuab approval (2018). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/emgality
63. Dodick, DW, Goadsby, PJ, Spierings, EL, Scherer, JC, Sweeney, SP, and Grayzel, DS. Safety and efficacy of LY2951742, a monoclonal antibody to calcitonin gene-related peptide, for the prevention of migraine: a phase 2, randomised, double-blind, placebo-controlled study. Lancet Neurol. (2014) 13:885–92. doi: 10.1016/S1474-4422(14)70128-0
64. Stauffer, VL, Dodick, DW, Zhang, Q, Carter, JN, Ailani, J, and Conley, RR. Evaluation of Galcanezumab for the prevention of episodic migraine: the EVOLVE-1 randomized clinical trial. JAMA Neurol. (2018) 75:1080–8. doi: 10.1001/jamaneurol.2018.1212
65. Skljarevski, V, Matharu, M, Millen, BA, Ossipov, MH, Kim, B-K, and Yang, JY. Efficacy and safety of galcanezumab for the prevention of episodic migraine: results of the EVOLVE-2 phase 3 randomized controlled clinical trial. Cephalalgia. (2018) 38:1442–54. doi: 10.1177/0333102418779543
66. Detke, HC, Goadsby, PJ, Wang, S, Friedman, DI, Selzler, KJ, and Aurora, SK. Galcanezumab in chronic migraine: the randomized, double-blind, placebo-controlled REGAIN study. Neurology. (2018) 91:e2211–21. doi: 10.1212/WNL.0000000000006640
67. Silvestro, M, Tessitore, A, Orologio, I, De Micco, R, Tartaglione, L, Trojsi, F, et al. Galcanezumab effect on "whole pain burden" and multidimensional outcomes in migraine patients with previous unsuccessful treatments: a real-world experience. J Headache Pain. (2022) 23:69. doi: 10.1186/s10194-022-01436-6
68. Lee, HC, Cho, S, and Kim, BK. Predictors of response to galcanezumab in patients with chronic migraine: a real-world prospective observational study. Neurolog Sci: Official J Italian Neurolog Society Italian Society of Clin Neurophysiol. (2023) 44:2455–63. doi: 10.1007/s10072-023-06683-2
69. Kwon, S, Gil, YE, and Lee, MJ. Real-world efficacy of galcanezumab for the treatment of migraine in Korean patients. Cephalalgia: Int J Headache. (2022) 42:705–14. doi: 10.1177/03331024221076481
70. Yalinay Dikmen, P, Baykan, B, Uludüz, D, Özge, A, Ilgaz Aydınlar, E, Polat, B, et al. Real-life experiences with galcanezumab and predictors for treatment response in Turkey. BMC Neurol. (2023) 23:418. doi: 10.1186/s12883-023-03467-1
71. EMA. Eptinezumab approval. (2020). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/vyepti
72. FDA. Novel aprovals in 2020. (2020). Available at: https://www.fda.gov/drugs/new-drugs-fda-cders-new-molecular-entities-and-new-therapeutic-biological-products/novel-drug-approvals-2020
73. Dodick, DW, Goadsby, PJ, Silberstein, SD, Lipton, RB, Olesen, J, Ashina, M, et al. Safety and efficacy of ALD403, an antibody to calcitonin gene-related peptide, for the prevention of frequent episodic migraine: a randomised, double-blind, placebo-controlled, exploratory phase 2 trial. Lancet Neurol. (2014) 13:1100–7. doi: 10.1016/S1474-4422(14)70209-1
74. Lipton, RB, Goadsby, PJ, Smith, J, Schaeffler, BA, Biondi, DM, Hirman, J, et al. Efficacy and safety of eptinezumab in patients with chronic migraine: PROMISE-2 Neurol. (2020). 94:e1365–e1377. doi: 10.1212/WNL.0000000000009169
75. Ashina, M, Saper, J, Cady, R, Schaeffler, BA, Biondi, DM, Hirman, J, et al. Eptinezumab in episodic migraine: A randomized, double-blind, placebo-controlled study (PROMISE-1). Cephalalgia. (2020) 40:241–54. doi: 10.1177/0333102420905132
76. Kudrow, D, Cady, RK, Allan, B, Pederson, SM, Hirman, J, Mehta, LR, et al. Long-term safety and tolerability of eptinezumab in patients with chronic migraine: a 2-year, open-label, phase 3 trial. BMC Neurol. (2021) 21:126. doi: 10.1186/s12883-021-02123-w
77. Ashina, M, Lanteri-Minet, M, Pozo-Rosich, P, Ettrup, A, Christoffersen, CL, Josiassen, MK, et al. Safety and efficacy of eptinezumab for migraine prevention in patients with two-to-four previous preventive treatment failures (DELIVER): a multi-arm, randomised, double-blind, placebo-controlled, phase 3b trial. Lancet Neurol. (2022) 21:597–607. doi: 10.1016/S1474-4422(22)00185-5
78. Doods, H, Hallermayer, G, Wu, D, Entzeroth, M, Rudolf, K, Engel, W, et al. Pharmacological profile of BIBN4096BS, the first selective small molecule CGRP antagonist. Br J Pharmacol. (2000) 129:420–3. doi: 10.1038/sj.bjp.0703110
79. Iovino, M, Feifel, U, Yong, CL, Wolters, JM, and Wallenstein, G. Safety, tolerability and pharmacokinetics of BIBN 4096 BS, the first selective small molecule calcitonin gene-related peptide receptor antagonist, following single intravenous administration in healthy volunteers. Cephalalgia: Int J Headache. (2004) 24:645–56. doi: 10.1111/j.1468-2982.2004.00726.x
80. Hewitt, DJ, Aurora, SK, Dodick, DW, Goadsby, PJ, Ge, YJ, Bachman, R, et al. Randomized controlled trial of the CGRP receptor antagonist MK-3207 in the acute treatment of migraine. Cephalalgia: Int J Headache. (2011) 31:712–22. doi: 10.1177/0333102411398399
81. Ho, TW, Mannix, LK, Fan, X, Assaid, C, Furtek, C, Jones, CJ, et al. Randomized controlled trial of an oral CGRP receptor antagonist, MK-0974, in acute treatment of migraine. Neurology. (2008) 70:1304–12. doi: 10.1212/01.WNL.0000286940.29755.61
82. Ho, TW, Ferrari, MD, Dodick, DW, Galet, V, Kost, J, Fan, X, et al. Efficacy and tolerability of MK-0974 (telcagepant), a new oral antagonist of calcitonin gene-related peptide receptor, compared with zolmitriptan for acute migraine: a randomised, placebo-controlled, parallel-treatment trial. Lancet (London, England). (2008) 372:2115–23. doi: 10.1016/S0140-6736(08)61626-8
83. Ho, TW, Connor, KM, Zhang, Y, Pearlman, E, Koppenhaver, J, Fan, X, et al. Randomized controlled trial of the CGRP receptor antagonist telcagepant for migraine prevention. Neurology. (2014) 83:958–66. doi: 10.1212/WNL.0000000000000771
84. EMA. Ubrogepant approval. (2019). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/vydura
85. FDA. Novel drug approval (2019). Available at: https://www.fda.gov/drugs/new-drugs-fda-cders-new-molecular-entities-and-new-therapeutic-biological-products/novel-drug-approvals-2019
86. Dodick, DW, Lipton, RB, Ailani, J, Lu, K, Finnegan, M, Trugman, JM, et al. Ubrogepant for the treatment of migraine. N Engl J Med. (2019) 381:2230–41. doi: 10.1056/NEJMoa1813049
87. Lipton, RB, Dodick, DW, Ailani, J, Lu, K, Finnegan, M, Szegedi, A, et al. Effect of Ubrogepant vs placebo on pain and the Most bothersome associated symptom in the acute treatment of migraine: the ACHIEVE II randomized clinical trial. JAMA. (2019) 322:1887–98. doi: 10.1001/jama.2019.16711
88. Goadsby, PJ, Blumenfeld, AM, Lipton, RB, Dodick, DW, Kalidas, K, M Adams, A, et al. Time course of efficacy of ubrogepant for the acute treatment of migraine: clinical implications. Cephalalgia: Int J Headache. (2021) 41:546–60. doi: 10.1177/0333102420970523
89. Hutchinson, S, Silberstein, SD, Blumenfeld, AM, Lipton, RB, Lu, K, Yu, SY, et al. Safety and efficacy of ubrogepant in participants with major cardiovascular risk factors in two single-attack phase 3 randomized trials: ACHIEVE I and II. Cephalalgia: Int J Headache. (2021) 41:979–90. doi: 10.1177/03331024211000311
90. Blumenfeld, AM, Goadsby, PJ, Dodick, DW, Hutchinson, S, Liu, C, Finnegan, M, et al. Efficacy of ubrogepant based on prior exposure and response to triptans: a post hoc analysis. Headache. (2021) 61:422–9. doi: 10.1111/head.14089
91. Chiang, CC, Arca, KN, Dunn, RB, Girardo, ME, Quillen, JK, Dodick, DW, et al. Real-world efficacy, tolerability, and safety of ubrogepant. Headache. (2021) 61:620–7. doi: 10.1111/head.14062
92. EMA. Rimegepant approval. (2022). Available at: https://www.ema.europa.eu/en/medicines/human/EPAR/vydura
93. Altamura, C, Brunelli, N, Marcosano, M, Fofi, L, and Vernieri, F. Gepants - a long way to cure: a narrative review. Neurolog Sci: Official J Italian Neurolog Society Italian Society of Clinical Neurophysiol. (2022) 43:5697–708. doi: 10.1007/s10072-022-06184-8
94. Croop, R, Goadsby, PJ, Stock, DA, Conway, CM, Forshaw, M, Stock, EG, et al. Efficacy, safety, and tolerability of rimegepant orally disintegrating tablet for the acute treatment of migraine: a randomised, phase 3, double-blind, placebo-controlled trial. Lancet (London, England). (2019) 394:737–45. doi: 10.1016/S0140-6736(19)31606-X
95. Lipton, RB, Croop, R, Stock, EG, Stock, DA, Morris, BA, Frost, M, et al. Rimegepant, an Oral calcitonin gene–related peptide receptor antagonist, for migraine. (2019);381:142–149.
96. Johnston, K, Harris, L, Powell, L, Popoff, E, Coric, V, L'Italien, G, et al. Monthly migraine days, tablet utilization, and quality of life associated with Rimegepant - post hoc results from an open label safety study (BHV3000-201). J Headache Pain. (2022) 23:10. doi: 10.1186/s10194-021-01378-5
97. Croop, R, Berman, G, Kudrow, D, Mullin, K, Thiry, A, et al. open-label long-term safety study of rimegepant for the acute treatment of migraine. Cephalalgia. 44:3331024241232944. doi: 10.1177/03331024241232944
98. FDA. Rimegepant approval. (2021). Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/212728s006lbl.pdf
99. Croop, R, Lipton, RB, Kudrow, D, Stock, DA, Kamen, L, Conway, CM, et al. Oral rimegepant for preventive treatment of migraine: a phase 2/3, randomised, double-blind, placebo-controlled trial. Lancet (London, England). (2021) 397:51–60. doi: 10.1016/S0140-6736(20)32544-7
100. Schwedt, TJ, Myers Oakes, TM, Martinez, JM, Vargas, BB, Pandey, H, Pearlman, EM, et al. Comparing the efficacy and safety of Galcanezumab versus Rimegepant for prevention of episodic migraine: results from a randomized. Controlled Clin Trial Neurol Therapy. (2024) 13:85–105. doi: 10.1007/s40120-023-00562-w
101. FDA. Novel drug approvals 2023. (2023). Available at: https://www.fda.gov/drugs/novel-drug-approvals-fda/novel-drug-approvals-2023
102. Croop, R, Madonia, J, Stock, DA, Thiry, A, Forshaw, M, Murphy, A, et al. Zavegepant nasal spray for the acute treatment of migraine: a phase 2/3 double-blind, randomized, placebo-controlled, dose-ranging trial. Headache. (2022) 62:1153–63. doi: 10.1111/head.14389
103. Lipton, RB, Croop, R, Stock, DA, Madonia, J, Forshaw, M, Lovegren, M, et al. Safety, tolerability, and efficacy of zavegepant 10 mg nasal spray for the acute treatment of migraine in the USA: a phase 3, double-blind, randomised, placebo-controlled multicentre trial. Lancet Neurol. (2023) 22:209–17. doi: 10.1016/S1474-4422(22)00517-8
104. Berman, G, Mullin, K, Pavlovic, J, Smith, T, Croop, R, Madonia, J, et al. Long-term safety and tolerability of Zavegepant 10 mg nasal spray during concomitant use of CGRP monoclonal antibodies: results from a 1-year open-label safety trial (P10-12.009) (2023) 100:4312. doi: 10.1212/WNL.0000000000203893
105. FDA. novel drug approval. (2021). Available at: https://www.fda.gov/drugs/novel-drug-approvals-fda/novel-drug-approvals-2021
106. Goadsby, PJ, Dodick, DW, Ailani, J, Trugman, JM, Finnegan, M, Lu, K, et al. Safety, tolerability, and efficacy of orally administered atogepant for the prevention of episodic migraine in adults: a double-blind, randomised phase 2b/3 trial. Lancet Neurol. (2020) 19:727–37. doi: 10.1016/S1474-4422(20)30234-9
107. Ailani, J, Lipton, RB, Goadsby, PJ, Guo, H, Miceli, R, Severt, L, et al. Atogepant for the preventive treatment of migraine. N Engl J Med. (2021) 385:695–706. doi: 10.1056/NEJMoa2035908
108. Ashina, M, Tepper, S, Reuter, U, Blumenfeld, A, Hutchinson, S, Xia, J, et al. Long-term safety and tolerability of atogepant 60 mg following once daily dosing over 1 year for the preventive treatment of migraine (2664), American J Neurolo. (2021) 96:15. doi: 10.1212/WNL.96.15_supplement.2664
109. Klein, BC, Miceli, R, Severt, L, McAllister, P, Mechtler, L, McVige, J, et al. Safety and tolerability results of atogepant for the preventive treatment of episodic migraine from a 40-week, open-label multicenter extension of the phase 3 ADVANCE trial. Cephalalgia: Int J Headache. (2023) 43:033310242211282. doi: 10.1177/03331024221128250
110. National Institute for health and care excellence: Guidelines. Headaches in over 12s: Diagnosis and management. London: National Institute for Health and Care Excellence (NICE Guideline, No. 150.) Available at: https://www.ncbi.nlm.nih.gov/books/NBK553317/.
111. Guidelines, B.. BASH Guidelines for headache. (2019). Available at: https://headache.org.uk/landing-page/for-clinicians/the-common-primary-headaches/migraine-for-clinicians/
112. Ailani, J, Burch, RC, and Robbins, MS. The American Headache Society Consensus Statement: Update on integrating new migraine treatments into clinical practice. Headache Rev. (2021) 61:1021–39. doi: 10.1111/head.14153
113. Health TMO. Migren Klinik Protokolu. (2020). Available at: https://dosyamerkez.saglik.gov.tr/Eklenti/38083,migrenkp20200720pdf.pdf?0
114. Silberstein, SD. Practice parameter: evidence-based guidelines for migraine headache (an evidence-based review): report of the quality standards Subcommittee of the American Academy of neurology. Neurology. (2000) 55:754–62. doi: 10.1212/WNL.55.6.754
115. NICE. Transcutaneous electrical stimulation of the supraorbital nerve for treating and preventing migraine. (2022). Available at: https://www.nice.org.uk/guidance/ipg740/resources/transcutaneous-electrical-stimulation-of-the-supraorbital-nerve-for-treating-and-preventing-migraine-pdf-1899876273639109
116. Sacco, S, Lampl, C, Amin, FM, Braschinsky, M, Deligianni, C, Uludüz, D, et al. European headache federation (EHF) consensus on the definition of effective treatment of a migraine attack and of triptan failure. J Headache Pain. (2022) 23:133. doi: 10.1186/s10194-022-01502-z
117. Sacco, S, Bendtsen, L, Ashina, M, Reuter, U, Terwindt, G, Mitsikostas, DD, et al. European headache federation guideline on the use of monoclonal antibodies acting on the calcitonin gene related peptide or its receptor for migraine prevention. J Headache Pain. (2019) 20:6. doi: 10.1186/s10194-018-0955-y
118. NICE. Transcranial magnetic stimulation for treating and preventing migraine. (2014). Available at: https://www.nice.org.uk/guidance/ipg477/resources/transcranial-magnetic-stimulation-for-treating-and-preventing-migraine-pdf-1899869936447941
119. Adams, AM, Serrano, D, Buse, DC, Reed, ML, Marske, V, Fanning, KM, et al. The impact of chronic migraine: the chronic migraine epidemiology and outcomes (CaMEO) study methods and baseline results. Cephalalgia: Int J Headache. (2015) 35:563–78. doi: 10.1177/0333102414552532
120. Lipton, RB, Nicholson, RA, Reed, ML, Araujo, AB, Jaffe, DH, Faries, DE, et al. Diagnosis, consultation, treatment, and impact of migraine in the US: results of the OVERCOME (US) study. Headache. (2022) 62:122–40. doi: 10.1111/head.14259
121. Ertas, M, Baykan, B, Kocasoy Orhan, E, Zarifoglu, M, Karli, N, Saip, S, et al. One-year prevalence and the impact of migraine and tension-type headache in Turkey: a nationwide home-based study in adults. J Headache Pain. (2012) 13:147–57. doi: 10.1007/s10194-011-0414-5
122. Ertaş, M, Saip, S, Karadaş, Ö, Öztürk, V, Uygunoğlu, U, Özge, A, et al. A comprehensive assessment of headache characteristics, management and burden of migraine in comparison with tension type headache in Turkey: Results of a cross-sectional survey of adult patients. Research Square (2022). doi: 10.21203/rs.3.rs-1755769/v1
123. Baykan, B, Ertas, M, Karli, N, Akat-Aktas, S, Uzunkaya, O, Zarifoglu, M, et al. The burden of headache in neurology outpatient clinics in Turkey. Pain Pract. (2007) 7:313–23. doi: 10.1111/j.1533-2500.2007.00154.x
124. Martelletti, P, Schwedt, TJ, Lanteri-Minet, M, Quintana, R, Carboni, V, Diener, H-C, et al. My migraine voice survey: a global study of disease burden among individuals with migraine for whom preventive treatments have failed. J Headache Pain. (2018) 19:1–10. doi: 10.1186/s10194-018-0946-z
125. Atalar, AÇ, Bozkurt, M, Çalişkan, Z, Vo, P, and Ertaş, M. Living with burden of migraine: the analysis of “my migraine voice” survey results in Turkey. Noro Psikiyatr Ars. (2021) 58:115. doi: 10.29399/npa.24780
126. Lipton, RB, Buse, DC, Serrano, D, Holland, S, and Reed, ML. Examination of unmet treatment needs among persons with episodic migraine: results of the American migraine prevalence and prevention (AMPP) study. Headache. (2013) 53:1300–11. doi: 10.1111/head.12154
127. Katsarava, Z, Mania, M, Lampl, C, Herberhold, J, and Steiner, TJ. Poor medical care for people with migraine in Europe - evidence from the Eurolight study. J Headache Pain. (2018) 19:10. doi: 10.1186/s10194-018-0839-1
128. Majima, M, Ito, Y, and Hosono, K. CGRP/CGRP receptor antibodies: potential adverse effects due to blockade of neovascularization? Trends Pharmacol Sci. (2019) 40:11–21. doi: 10.1016/j.tips.2018.11.003
129. Al-Hassany, L, Lyons, HS, Boucherie, DM, Farham, F, Lange, KS, Marschollek, K, et al. The sense of stopping migraine prophylaxis. J Headache Pain. (2023) 24:9. doi: 10.1186/s10194-023-01539-8
130. Yücel, Y, Coşkun, S, Cengiz, B, Özdemir, HH, Uzar, E, Çim, A, et al. Association of Polymorphisms within the serotonin receptor genes 5-HTR1A, 5-HTR1B, 5-HTR2A and 5-HTR2C and migraine susceptibility in a Turkish population. Clin Psychopharmacol Neurosci: Official Scientific J Korean College of Neuropsychopharmacol. (2016) 14:250–5. doi: 10.9758/cpn.2016.14.3.250
131. Ates, O, Kurt, S, Altinisik, J, Karaer, H, and Sezer, S. Genetic variations in tumor necrosis factor alpha, interleukin-10 genes, and migraine susceptibility. Pain Med (Malden, Mass). (2011) 12:1464–9. doi: 10.1111/j.1526-4637.2011.01200.x
132. Genc, H, Baykan, B, Bolay, H, Uluduz, D, Unal-Cevik, I, Kissani, N, et al. Cross-sectional, hospital-based analysis of headache types using ICHD-3 criteria in the Middle East, Asia, and Africa: the head-MENAA study. J Headache Pain. (2023) 24:24. doi: 10.1186/s10194-023-01555-8
133. Buse, DC, Reed, ML, Fanning, KM, Bostic, R, Dodick, DW, Schwedt, TJ, et al. Comorbid and co-occurring conditions in migraine and associated risk of increasing headache pain intensity and headache frequency: results of the migraine in America symptoms and treatment (MAST) study. J Headache Pain. (2020) 21:23. doi: 10.1186/s10194-020-1084-y
134. Rathier, LA, Buse, DC, Nicholson, RA, and Andrasik, FJH. Multidisciplinary approach to patients with migraine. Trends Pharmacol Sci. (2013) 7:100–12. doi: 10.1002/9781118678961.ch7
135. Tana, C, Raffaelli, B, Souza, MNP, de la Torre, ER, Massi, DG, Kisani, N, et al. Health equity, care access and quality in headache - part 1. J Headache Pain. (2024) 25:12. doi: 10.1186/s10194-024-01712-7
136. Raffaelli, B, Rubio-Beltrán, E, Cho, SJ, De Icco, R, Labastida-Ramirez, A, Onan, D, et al. Health equity, care access and quality in headache - part 2. J Headache Pain. (2023) 24:167. doi: 10.1186/s10194-023-01699-7
Keywords: CGRP-targeted therapies, migraine management, clinical implications, gepants, monoclonal antibodies, personalized treatment
Citation: Özge A, Baykan B, Bıçakçı Ş, Ertaş M, Atalar AÇ, Gümrü S and Karlı N (2024) Revolutionizing migraine management: advances and challenges in CGRP-targeted therapies and their clinical implications. Front. Neurol. 15:1402569. doi: 10.3389/fneur.2024.1402569
Edited by:
Tsubasa Takizawa, Keio University, JapanReviewed by:
Marta Waliszewska-Prosół, Wroclaw Medical University, PolandCopyright © 2024 Özge, Baykan, Bıçakçı, Ertaş, Atalar, Gümrü and Karlı. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: A. Özge, ZmVyZGEua2l6aWx0YXNAcmVtZWRpdW1jZy5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.