 Franz-Simon Centner1
Franz-Simon Centner1 Holger Wenz2Mariella Eliana Oster1Franz-Joseph Dally1,3Johannes Sauter-Servaes1Tanja Pelzer1,4Jochen J. Schoettler1Bianka Hahn1
Holger Wenz2Mariella Eliana Oster1Franz-Joseph Dally1,3Johannes Sauter-Servaes1Tanja Pelzer1,4Jochen J. Schoettler1Bianka Hahn1 Amr Abdulazim5
Amr Abdulazim5 Katharian A. M. Hackenberg5Christoph Groden2Joerg Krebs1
Katharian A. M. Hackenberg5Christoph Groden2Joerg Krebs1 Manfred Thiel1Nima Etminan5
Manfred Thiel1Nima Etminan5 Máté E. Maros2,6*
Máté E. Maros2,6*- 1Department of Anesthesiology, Surgical Intensive Care Medicine and Pain Medicine, University Medical Center Mannheim, Medical Faculty Mannheim, University of Heidelberg, Mannheim, Germany
- 2Department of Neuroradiology, University Medical Center Mannheim, Medical Faculty Mannheim, University of Heidelberg, Mannheim, Germany
- 3Department of Orthopedics and Trauma Surgery, University Medical Center Mannheim, Medical Faculty Mannheim, University of Heidelberg, Mannheim, Germany
- 4Department of Neonatology, University Medical Center Mannheim, Medical Faculty Mannheim, University of Heidelberg, Mannheim, Germany
- 5Department of Neurosurgery, University Medical Center Mannheim, Medical Faculty Mannheim, University of Heidelberg, Mannheim, Germany
- 6Department of Biomedical Informatics at the Center for Preventive Medicine and Digital Health (CPD), University Medical Center Mannheim, Medical Faculty Mannheim, University of Heidelberg, Mannheim, Germany
Objective: Although sepsis and delayed cerebral ischemia (DCI) are severe complications in patients with aneurysmal subarachnoid hemorrhage (aSAH) and share pathophysiological features, their interrelation and additive effect on functional outcome is uncertain. We investigated the association between sepsis and DCI and their cumulative effect on functional outcome in patients with aSAH using current sepsis-3 definition.
Methods: Patients admitted to our hospital between 11/2014 and 11/2018 for aSAH were retrospectively analyzed. The main explanatory variable was sepsis, diagnosed using sepsis-3 criteria. Endpoints were DCI and functional outcome at hospital discharge (modified Rankin Scale (mRS) 0–3 vs. 4–6). Propensity score matching (PSM) and multivariable logistic regressions were performed.
Results: Of 238 patients with aSAH, 55 (23.1%) developed sepsis and 74 (31.1%) DCI. After PSM, aSAH patients with sepsis displayed significantly worse functional outcome (p < 0.01) and longer ICU stay (p = 0.046). Sepsis was independently associated with DCI (OR = 2.46, 95%CI: 1.28–4.72, p < 0.01). However, after exclusion of patients who developed sepsis before (OR = 1.59, 95%CI: 0.78–3.24, p = 0.21) or after DCI (OR = 0.85, 95%CI: 0.37–1.95, p = 0.70) this statistical association did not remain. Good functional outcome gradually decreased from 56.3% (76/135) in patients with neither sepsis nor DCI, to 43.8% (21/48) in those with no sepsis but DCI, to 34.5% (10/29) with sepsis but no DCI and to 7.7% (2/26) in patients with both sepsis and DCI.
Conclusion: Our study demonstrates a strong association between sepsis, DCI and functional outcome in patients with aSAH and suggests a complex interplay resulting in a cumulative effect towards poor functional outcome, which warrants further studies.
1 Introduction
Both sepsis and delayed cerebral ischemia (DCI) are severe complications in patients with aneurysmal subarachnoid hemorrhage (aSAH) and are significant determinants for poor outcome (1–4). Although sepsis and DCI share pathophysiological features (5–10), their interrelation is insufficiently understood (11). Therefore, we investigated the association between sepsis and DCI in a cohort of aSAH patients.
While the term DCI presents a pro-ischemic complication in patients who survive the initial aSAH ictus (12, 13), sepsis can also result in acute and long-term brain damage via cerebral ischemia (5, 6). Both sepsis and DCI are characterized by a dysregulation in vascular regulation and integrity (7, 8). DCI was mainly thought to be caused by cerebral vasospasm however, recent studies support the concept of a multifactorial pathophysiology, including microcirculatory disturbances due to microthrombosis and neuroinflammation (4, 9, 10). Microcirculatory dysfunction is also a key mechanism of septic organ dysfunction caused by direct effects of circulating mediators, capillary leak and microthrombus formation, which can affect any organ including the brain (5, 8). In this context, it was recently shown that systemic infection can amplify intracranial inflammatory responses in patients with aSAH (14).
Considering these overlapping pathophysiological features, we hypothesized that in aSAH patients the development of sepsis and DCI might be associated and may have an additive effect resulting in poor functional outcome. However, current data on the relation of sepsis and DCI in patients with aSAH are limited and inconclusive (11). Although nosocomial infection was independently associated with DCI in an exploratory analysis (11), two preceding studies did not find an association between sepsis and DCI (7, 15). These studies were, however, performed before 2016 (7, 15) and did not use the updated sepsis definition (sepsis-3), which focuses on septic organ dysfunction (16). Thus, we performed a comprehensive retrospective, single-center cohort study to investigate the association between sepsis and DCI and their potential cumulative effect on functional outcome in aSAH patients using current sepsis definition.
2 Materials and methods
2.1 Study design, setting and patient selection
This single-center retrospective cohort study was conducted at the 25-bed intensive care unit (ICU) of the Department of Anesthesiology, Surgical Intensive Care Medicine and Pain Medicine at the University Medical Center Mannheim, Germany, where aSAH patients were treated and managed in close collaboration with the Department of Neurosurgery. The Medical Ethics Commission II of Medical Faculty Mannheim, University of Heidelberg, approved the study design as well as reanalysis of neuroradiological reports and imaging data (reference number: 2019-1096R, 2017-825R-MA and 2017-828R-MA; date of approval: 01/10/2019). The need for informed consent was waived because of the retrospective nature of the study. Study design and reporting adhered to the STROBE guidelines [STrengthening the Reporting of OBservational studies in Epidemiology; (17)]. The study was registered at the German Clinical Trials Register (ID: DRKS00030748).
Data on all patients (age ≥ 18 years) treated in our ICU between 11/2014 and 11/2018 were extracted from an electronic health record database (Figure 1). Of 3,961 patients, 340 (8.6%) patients were preselected via ICD codes for spontaneous subarachnoid hemorrhage (code I60*). For 256 patients, aneurysmal subarachnoid hemorrhage on initial computed tomography (CT) scan was verified by an experienced neuroradiologist (H.W.). In a further step, 18 (7.0%) patients who did not receive aneurysm repair because of disease severity were excluded, resulting in 238 patients as final study cohort (Figure 1; Supplementary Table S1).
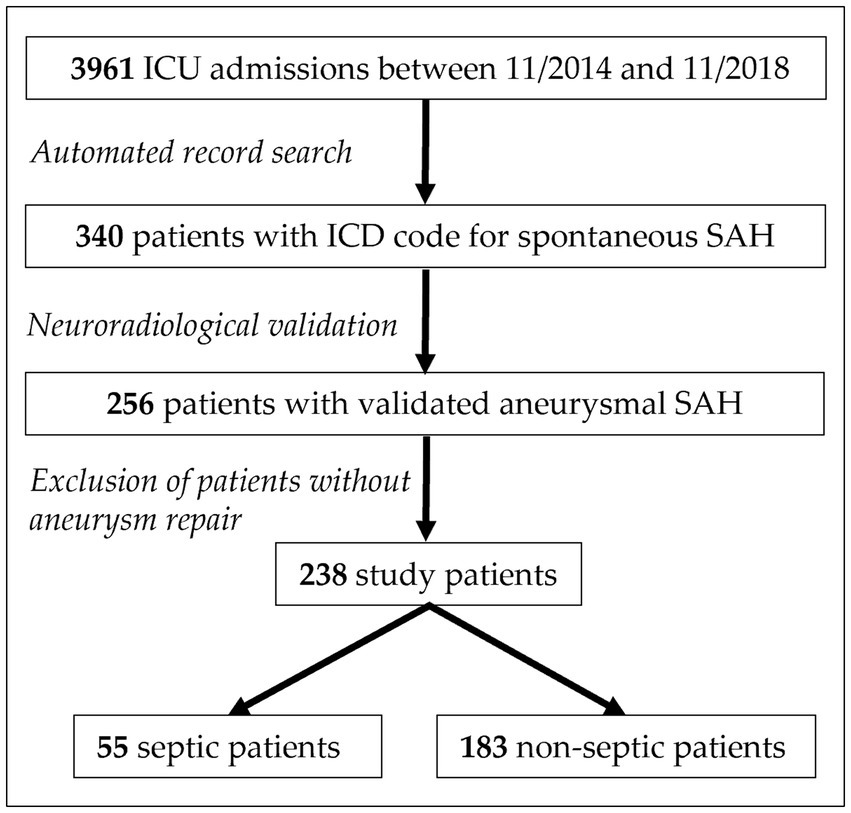
Figure 1. Flow diagram of study cohort selection. ICD indicates international classification of diseases. ICU, intensive care unit; SAH, subarachnoid hemorrhage.
2.2 Clinical assessment and management
All patients were screened for healthcare-associated infections according to center for disease control (CDC) criteria (18). For all patients who developed an infection, sequential organ failure assessment (SOFA) scores (19) were determined for 24-h periods by intensive care physicians. To ensure comparability of sepsis criteria application with the original approach of sepsis-3 definition (16), sepsis-3 criteria were applied using an automated algorithm as previously described (20). Baseline characteristics (age, sex, length of stay (LOS) in ICU and in-hospital mortality) were extracted from the electronic health records. Clinical parameters were extracted and verified by intensive care physicians: pre-existing illnesses, World Federation of Neurological Surgeons SAH grading scale (WFNS) at admission, placement of an external ventricular drainage (EVD), type of aneurysm repair and modified Rankin Scale (mRS) at hospital discharge. DCI as primary endpoint was defined as proposed by Vergouwen et al. (13) based on neuroimaging of cerebral infarction from DCI. Clinical management was performed as described in the Supplementary Text S1 and the procedures followed were in accordance with institutional guidelines (21). Since January 2016, an updated protocol for standardized detection and management of DCI was implemented by the Department of Neurosurgery in line with our previous studies (22, 23). We adjusted for these changes in DCI treatment protocol during all our analyses by incorporating a binary (yes/no) factor variable (DCI protocol). Patients with infections and sepsis were treated in accordance with current recommendations (24, 25). For enhanced hemodynamic and fluid management central venous access, PiCCO catheter (Pulsion Medical Systems, Munich, Germany) and foley catheter placement were routinely performed in all study patients.
2.3 Statistical analysis
Normally distributed variables were described using their means and standard deviations (SD), non-normally distributed variables with their medians, lower and upper quartile (LQ-UQ), while proportions were shown for categorical variables. All analyses were performed with the R statistics program™ (v.4.3.2, R Core Team 2023, Vienna Austria; RStudio IDE v. 2023.12.0 Build 554, Boston, MA, United States). Statistical analyses and their results were reported in accordance with the Statistical Analyses and Methods in the Published Literature (SAMPL) guidelines (26).
The main research question, and explanatory variable of interest, was the effect of sepsis on the development of DCI. Therefore, we first performed propensity score matching (PSM) to adjust for potential confounders between subgroups of sepsis positive and negative patients (27). Matching weights for sepsis-3 (nyes_sepis-3 = 55) subgroups were calculated using (the default settings of the matchit package) 1:1 nearest neighbor approach (Ntotal = 238; Nmatched = 110) without replacement based on propensity score distance estimated with logistic regression including the following covariates: age, sex, WFNS grading scale, intraventricular hemorrhage (IVH), DCI protocol and smoking status as well as presence of arterial hypertension. The target estimand was calculated based on the average treatment effect of the treated (ATT). Second, we applied an exploratory modeling approach using standard generalized linear models (base glm) on the original cohort (28, 29). For this, the primary and secondary endpoint variables were the development of DCI (yes vs. no) and functional outcome at hospital discharge (mRS 0–3 vs. 4–6), respectively. These endpoints were modeled by multivariable logistic regression (LR) adjusted for sepsis, age, smoking status, WFNS grading scale, EVD-placement and type of aneurysm repair. The target explanatory variable of interest was sepsis based on sepsis-3 criteria. As sensitivity analyses, interaction terms were added to the multivariable LR model to investigate if the main- and combination effects of DCI and sepsis stayed consistent within mRS outcomes. Data regarding the time-dependency of these research questions were lacking in the literature. Thus, the distributions of time of occurrences of sepsis and DCI were described using median, LQ-UQ. Between group comparisons of un- and matched PSM cohorts were performed using Chi-squared test for categorical variables (with continuity correction) and two-group t-test. In case of potentially non-normally distributed continuous variables (e.g., ICU days), the Kruskal–Wallis (global test) or for two-groups the Wilcoxon-Mann–Whitney tests whereas for categorical variables with small cell counts the Fisher’s exact test were used (30, 31). Due to the limited number of cases, it was not possible to evaluate complex multivariable models in time-varying regression frameworks (32). Additionally, post hoc power calculations were performed for 2 × 2 contingency tables with independent samples to estimate the power of our analyses given the proportion of good functional outcome at discharge in septic (yes vs. no) and DCI (yes vs. no) cohorts using two-sided =0.05 thresholds (power.exact.test function, Exact package). Figures were created using the ggplot2 grammar of graphics. p < 0.05 were considered significant. Due to the explorative nature of our analyses, p-values were not adjusted for multiple testing (31).
3 Results
3.1 Cohort characteristics
The 238 patients with aSAH had a median age of 56 years (Q1-Q3: 50–64; Table 1) and 69.7% (166/238) were female. 116 (48.7%) patients developed any infection. When applying sepsis-3 criteria, 55 patients were diagnosed as septic, resulting in a sepsis frequency of 47.4% (55/116) in patients with an infection and 23.1% (55/238) in relation to the total cohort. This resulted in a mortality rate of 14.5% (8/55) within the septic subpopulation. Of all patients 31.1% (74/238) developed DCI, while 47.3% (26/55) with sepsis also developed DCI. The diagnosis of sepsis preceded the diagnosis of DCI in 65.4% (17/26) by a median of 43 h. A total of 129 patients (54.2%) had a poor functional outcome at hospital discharge (mRS >3) and the overall in-hospital mortality was 14.7% (35/238, Table 1).
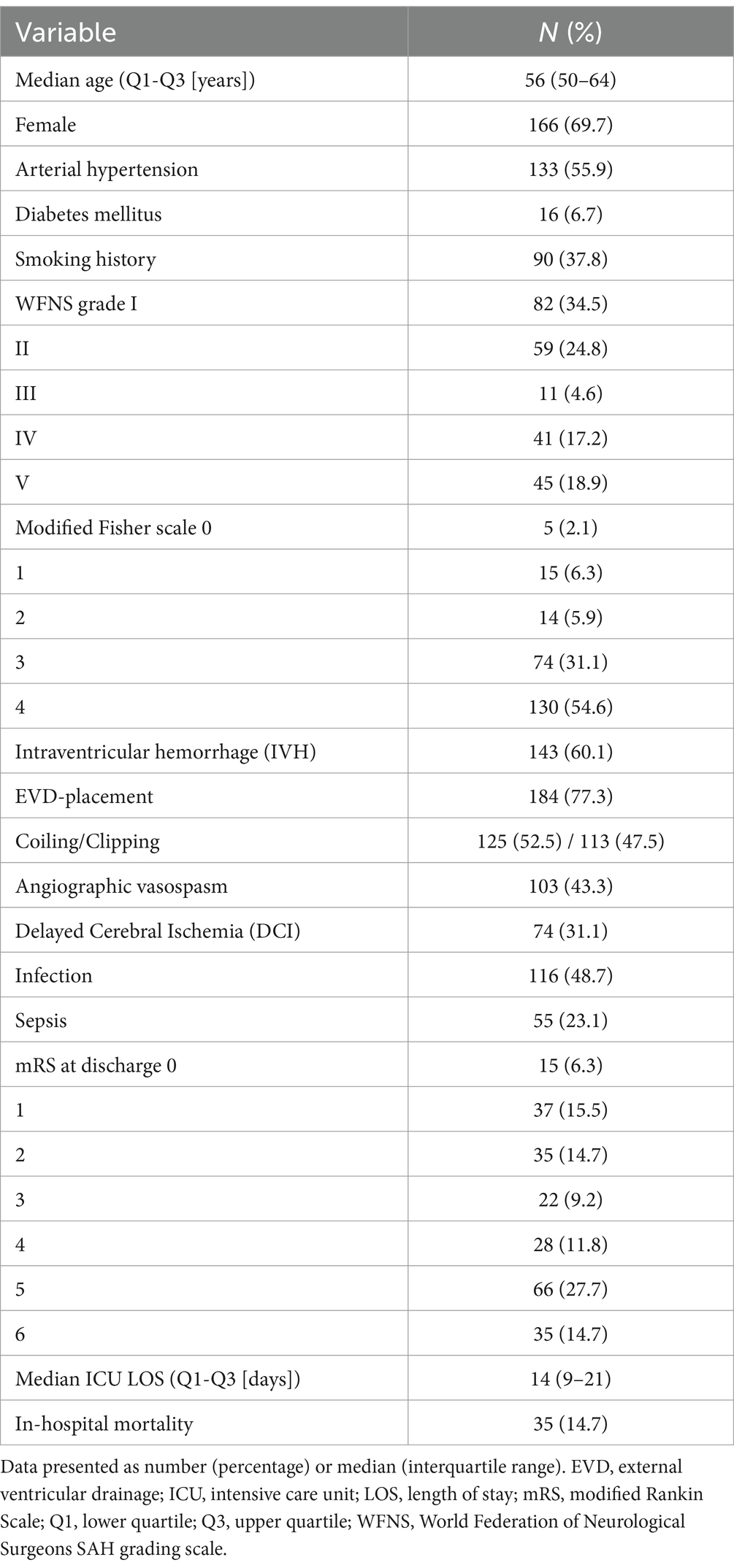
Table 1. Clinical and treatment characteristics of the total cohort with aneurysmal subarachnoid hemorrhage (N = 238).
3.2 Propensity score matching
PSM was performed for the development of sepsis. Variables included established risk factors for DCI (33, 34) such as smoking, sex, diabetes and arterial hypertension. Unmatched control cases were excluded from univariate analyses (n = 128).
Before PSM (n = 238, Table 2) diabetes, modified Fisher, IVH, EVD-placement, DCI, infection, functional outcome and ICU LOS were significantly different between septic and non-septic patients. After propensity score matching (n = 110), infection (p < 0.01) and ICU LOS (p = 0.046) remained significant and among the 55 matched patients without sepsis, 27 (49.1%) had poor functional outcomes, contrasting with 43 patients (78.2%) who developed sepsis (p < 0.01, Table 2).
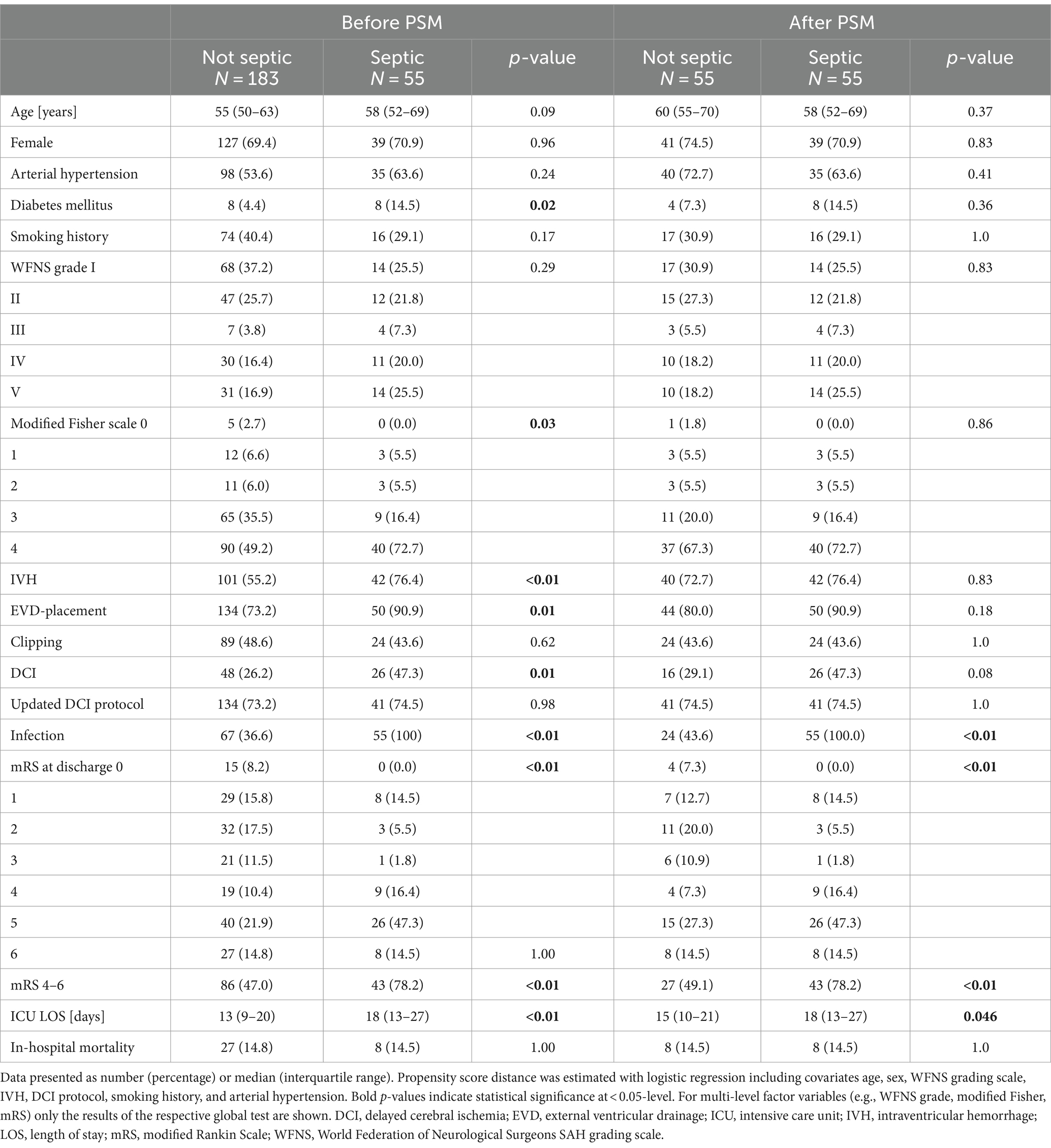
Table 2. Clinical and treatment characteristics before and after propensity score matching (PSM) for cases with sepsis.
3.3 Association between sepsis and DCI
In multivariable LR fitted on complete cases (n = 238, Table 1) of the original cohort, sepsis demonstrated an independent association with the occurrence of DCI (adjusted odds ratio (aOR) = 2.46, 95%CI: 1.28–4.72, p = 0.007; Table 3; Figure 2A). The history of smoking slightly missed statistical significance with DCI (p = 0.054; Figure 2A).
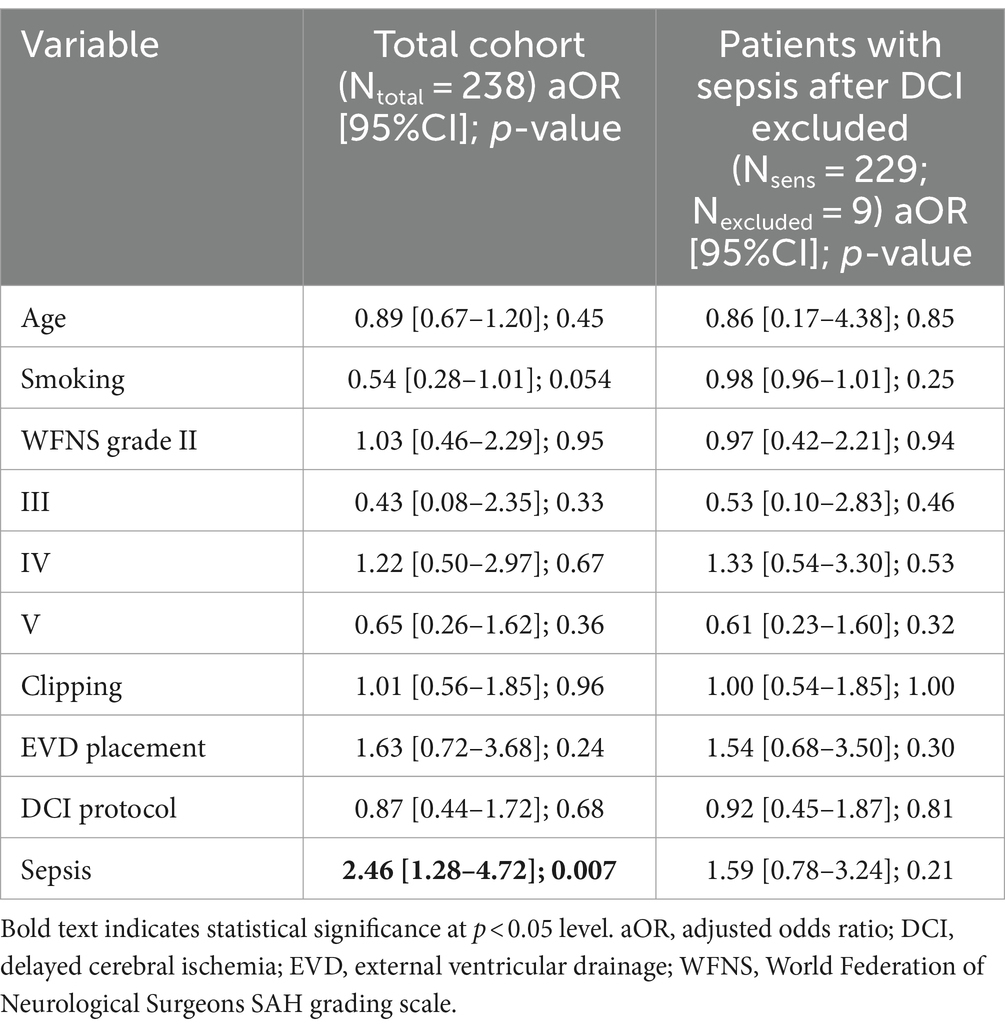
Table 3. Multivariable logistic regression models including sensitivity analysis for the primary endpoint delayed cerebral ischemia (DCI).
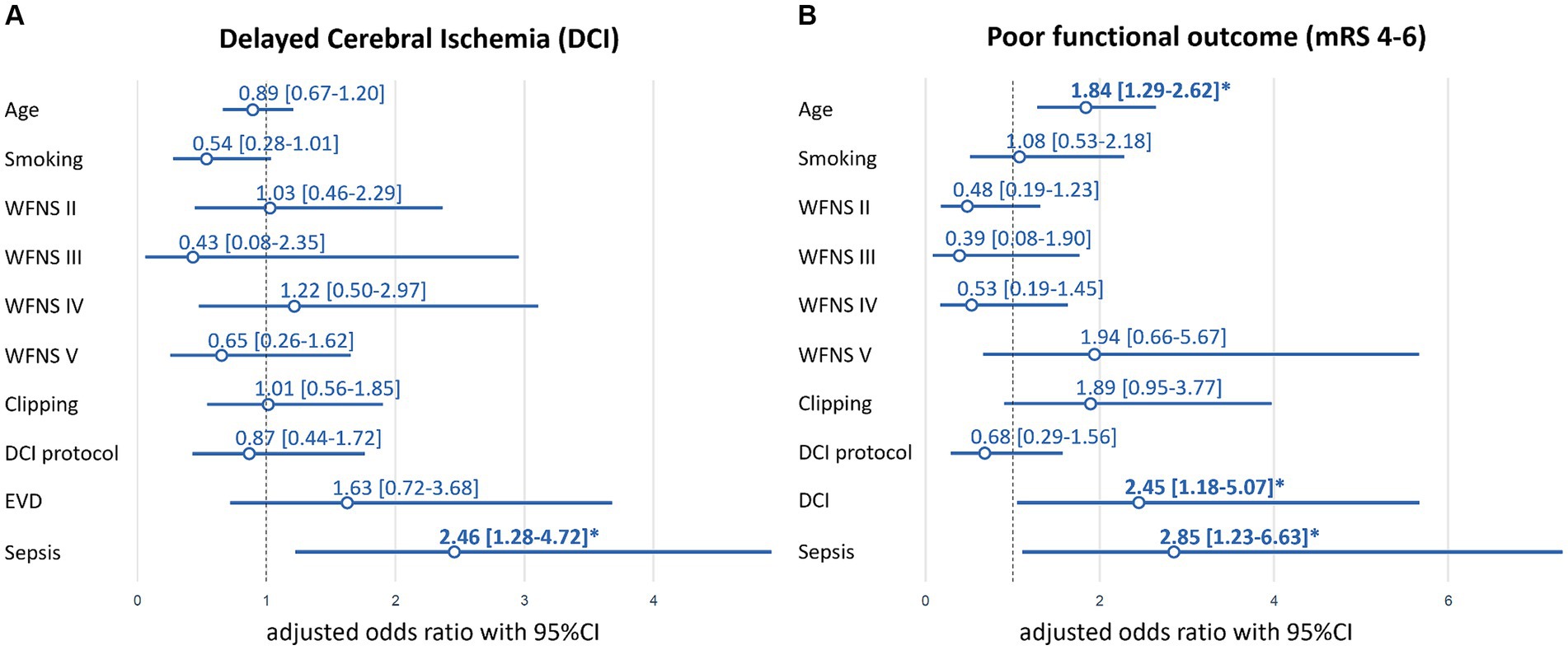
Figure 2. Multivariable logistic regression model-based adjusted odds ratios (aOR) for DCI (A) and poor (mRS 4–6) functional outcome (B). EVD for mRS 4–6 is not shown due to cleaner visibility and out of range point estimates and confidence intervals (aOR = 21.87, 95%CI:6.76–70.77, p < 0.01). Bold font and *indicate significance at p < 0.05-level. DCI indicates delayed cerebral ischemia. EVD, external ventricular drainage; mRS, modified Rankin Scale; WFNS, World Federation of Neurological Surgeons SAH grading scale.
To further scrutinize the link between DCI and sepsis, we performed three sensitivity analyses. First, we excluded patients who developed sepsis after DCI (n = 9) from the cohort, only focusing on cases in whom sepsis preceded DCI. This LR model indicated a trend towards increased odds of DCI if sepsis was diagnosed (aOR = 1.59, 95%CI: 0.78–3.24, p = 0.21; Table 3). Second, patients who developed sepsis before DCI (n = 17) were excluded, focusing on cases in whom DCI preceded sepsis. In this LR analysis, there was no apparent association between DCI and sepsis (aOR = 0.85, 95%CI: 0.37–1.95, p = 0.70; Supplementary Table S2). Third, to differentiate whether a change in vital parameters was due to neuroinflammation caused by the SAH ictus (10) or sepsis, sepsis as variable of interest in the primary multivariable model (Figure 2A; Table 3) was replaced with quick SOFA (qSOFA) independent from the infectious status. There was no association between qSOFA and DCI when applied independently from an infection (aOR = 0.85, 95%CI: 0.43–1.68, p = 0.65; Supplementary Figure S1; Supplementary Table S3).
3.4 Association between sepsis and DCI with functional outcome
In multivariable LR models containing all cases (n = 238) of the original cohort, sepsis was independently associated with poor functional outcome (mRS >3) at hospital discharge with an aOR = 2.85 (95%CI: 1.23–6.63, p = 0.02; Figure 2B; Supplementary Table S4). Age (aOR = 1.84, 95%CI: 1.29–2.62, p < 0.01), EVD-placement (aOR = 21.87, 95%CI: 6.76–70.77, p < 0.01) and DCI (aOR = 2.45, 95%CI: 1.18–5.07, p = 0.02) were additional predictors of poor functional outcome.
Furthermore, we evaluated the effects of potential interactions between sepsis and DCI regarding functional outcome (Supplementary Table S5). Sepsis showed an interaction with DCI (aOR = 11.05, 95%CI: 1.31–93.27, p = 0.03) and neither of these variables remained independently associated (p = 0.53 for sepsis and p = 0.27 for DCI) in the interaction model (Supplementary Table S5). Thus, indicating that the main effect of sepsis and DCI on functional outcome could not be independently interpreted from each other.
The proportion of patients with good functional outcome (mRS 0–3) gradually decreased in subgroups of patients from 56.3% (76/135) in those with neither sepsis nor DCI, to 43.8% (21/48) in those with no sepsis but DCI, to 34.5% (10/29) in patients with sepsis but no DCI and to 7.7% (2/26) in those with both sepsis and DCI. To quantify the potential effect of small numbers of patients in some subgroups of the latter results, we performed post hoc power analyses. If identical proportions (i.e., probabilities) of poor outcome (mRS 4–6) were assumed for a study between non-septic (p1 = 0.46, n1 = 183) and septic (p2 = 0.78, n2 = 55) patients using two-sided =0.05, this would result in a power of 99.0%. Additionally, 10–20% variations of the above proportions (p1 vs. p2) within the identically sized two groups for 0.46 versus 0.68 and 0.36 versus 0.58 resulted both in a power of 79.9%, respectively.
4 Discussion
The primary aim of the present study was to investigate the association between sepsis and DCI and a potential cumulative effect of sepsis and DCI on functional outcome in a cohort of patients with aSAH using current sepsis definition. Because of overlapping pathophysiological features, we hypothesized that sepsis and DCI might be associated and have a cumulative effect on poor functional outcome. In our cohort of aSAH patients, sepsis was independently associated with DCI. However, when patients that developed sepsis before or after DCI were excluded, this association did not remain. If sepsis preceded DCI, we found a trend towards a higher probability of developing DCI, which was probably limited by the sample size. Nonetheless, sepsis was confirmed as an independent risk factor for poor functional outcome in patients with aSAH. The worst functional outcome was observed in patients who suffered from both sepsis and DCI.
Robust data on the association between sepsis and DCI in patients with aSAH are limited and inconclusive (11). A previous study by Foreman et al. described an independent association between nosocomial infection and DCI (11). However, in their study no differentiation between localized and systemic infection was made (11). Jeon et al. reported that sepsis was neither associated with DCI nor with mRS > 3 at 3 months after SAH (15). In a relatively small cohort of 98 aSAH patients, Budohosky et al. found a trend towards increased odds of DCI in patients with sepsis (OR = 4.4, 95%CI: 0.08–25.2; p = 0.095) (7). Although the used sepsis operationalization was shown to be important in studies on sepsis-associated outcomes in critically ill patients in general (20, 35) and in patients with aSAH specifically (2, 36), neither of the aforementioned studies included details about the utilized sepsis definition. Additionally, both studies were performed before 2016 (7, 15) and did not apply the updated sepsis-3 definition that focuses on septic organ dysfunction (16). To our knowledge, this is the first study evaluating sepsis-3 criteria for the association between sepsis and DCI in patients with aSAH.
We observed a strong association between sepsis and DCI in the total cohort. When patients who developed sepsis after DCI were excluded from the analysis, thereby focusing on the effect of sepsis preceding DCI, the association between sepsis and DCI was no longer statistically significant but indicated a potential trend towards a positive association with DCI. Thus, we assume that a larger, potentially multi-centric cohort could improve statistical power and underscore their temporal association. This notion was also supported by the sensitivity analysis focusing on patients who developed sepsis after DCI, in which no relevant association between sepsis and DCI could be identified. These findings hint to a rather complex interplay between sepsis and DCI.
The observed association between sepsis and DCI in the present study might be explained by overlapping pathophysiological effects of sepsis in the brain and DCI. Both conditions are characterized by vascular dysfunction including dysregulation of cerebral vascular tone and impairment of vascular autoregulation (3, 7, 36). While DCI can occur independently from cerebral vasospasm, there is still a strong association between angiographic vasospasm with neurological worsening, cerebral infarction, and poor outcome (12). Simultaneously, in contrast to systemic vasodilation in early sepsis, vasoconstriction of the resistance arterioles in the brain occurs in patients with sepsis-associated encephalopathy (37). It is noteworthy that the titration of the systemic circulation to a specific blood pressure target with vasopressors will not automatically restore cerebral perfusion in septic patients (38). In recent years, new evidence has been established for both sepsis-associated encephalopathy and DCI that factors beyond a disturbed macrocirculation of cerebral blood vessels play an important role in the pathophysiology including microcirculatory disturbances due to endothelial dysfunction, neuroinflammation and microthrombosis with consecutive disruption of the blood–brain barrier and cellular injury (9, 10, 39, 40).
While DCI is defined as cerebral ischemia due to sequelae of SAH (13), sepsis can cause cerebral ischemia via the multifactorial pathophysiological processes described above (5, 6, 39). Hence, both sepsis and DCI are associated with derangements of vascular tone and integrity, microthrombosis formation and neuroinflammation resulting in cerebral ischemia (4, 6, 9, 10, 39). These pathophysiological effects are concordant with the results of the present study in that both sepsis and DCI were independent risk factors for poor functional outcome in our cohort of aSAH patients. Sepsis is known to be independently associated with persistent new cognitive impairment and functional disability among survivors in general populations (41) and might contribute to brain dysfunction after SAH as a second hit to an already vulnerable brain (1). Accordingly, the relevance of sepsis on the functional outcome in patients with aSAH was shown before (1, 42, 43) and confirmed in the present study. Interestingly, our analysis revealed a significant interaction between sepsis and DCI and showed that their effects on functional outcome could not be interpreted independently from each other. Furthermore, sensitivity analyses suggested that temporal characteristics of sepsis and DCI occurrence are of relevance. In line with this, we observed a gradual decrease of the proportion of patients with good functional outcome in the presence of DCI and sepsis. Only 7.7% of patients who suffered from sepsis and DCI achieved an mRS 0–3 outcome, which underlines a cumulative effect that warrants further research. In this context, it has been recently shown that systemic infection can increase intracranial inflammatory responses in patients with aSAH (14), which might be a promising approach to explore the here established associations between sepsis, DCI and functional outcome. Further investigating the temporal course of sepsis, the systemic immune response and the development of DCI could be helpful to better define the relationship (11).
4.1 Limitations
Our study has several limitations: The data are derived from a single-center retrospective cohort study. However, the retrospective nature permitted the inclusion of all available information independent from temporal occurrence and for the comprehensive description of infectious complications. Concurrently, the retrospective design prevented conclusions about cause–effect inferences. Our analyses are based on a cohort, which was extracted up to 11/2018. This was due to a data lockdown within the research project Scientific Computing for Improved Detection and Therapy of Sepsis (SCIDATOS (44, 45), funded by the Klaus Tschira Foundation, grant number 00.277.2015) and a consecutive elaborate data annotation and validation process by several experts from multiple medical disciplines. Nonetheless, this is, to our knowledge, among the largest cohorts in that the association between sepsis and DCI in aSAH patients was analyzed (7, 11, 15). Functional outcome at hospital discharge, as the endpoint of this study, cannot capture long-term outcomes. As demonstrated in a previous study of SAH patients, sepsis was identified as an independent risk factor for both poor functional outcome at hospital discharge and in the long term (1). It is tempting to speculate that the here established association between sepsis and DCI may also be relevant for long-term functional outcome, warranting investigation in future studies.
5 Conclusion
In conclusion, the present study is, to our knowledge, the first to demonstrate a significant association between sepsis and DCI in aSAH patients and indicate the relevance of their temporal association. Sepsis was confirmed as an independent risk factor for poor functional outcome at hospital discharge. Furthermore, the co-occurrence of sepsis and DCI led to a cumulative effect towards poor functional outcome. Our analyses highlight the significant impact of sepsis on the disease course of aSAH patients suggesting a complex interplay between sepsis and DCI, which warrants further research on this topic.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Medical Ethics Commission II of the Medical Faculty Mannheim, University of Heidelberg. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants’ legal guardians/next of kin due to the observational and retrospective nature of the study.
Author contributions
F-SC: Writing – original draft, Validation, Project administration, Methodology, Investigation, Data curation, Conceptualization. HW: Writing – review & editing, Validation, Resources, Investigation, Data curation. MO: Writing – review & editing, Validation, Software, Resources, Formal analysis, Data curation. F-JD: Writing – review & editing, Investigation. JS-S: Writing – review & editing, Investigation. TP: Writing – review & editing, Investigation. JS: Writing – review & editing, Investigation. BH: Writing – review & editing, Software, Formal analysis, Data curation. AA: Writing – review & editing, Investigation. KH: Writing – review & editing, Investigation. CG: Writing – review & editing, Resources. JK: Writing – review & editing, Validation, Resources. MT: Writing – review & editing, Supervision, Resources, Project administration, Funding acquisition. NE: Writing – review & editing, Validation, Resources. MM: Writing – original draft, Visualization, Validation, Software, Resources, Project administration, Methodology, Funding acquisition, Formal analysis, Data curation.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. F-SC, JS, and MT report funding from the Klaus Tschira Stiftung, grant number 00.277.2015. MM reports funding from the German Ministry for Education and Research (BMBF) within the framework of the Medical Informatics Initiative (MII) MIRACUM Consortium (Medical Informatics for Holistic Disease Models in Personalized and Preventive Medicine, MIDorAI; 01ZZ2020). For the publication fee, we acknowledge the financial support from the Open Access Publication Funding of Heidelberg University and the German Research Foundation (DFG).
Acknowledgments
We are grateful to Prof. Dr. Gabriel J. E. Rinkel for his valuable comments and helpful advice.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1393989/full#supplementary-material
References
1. Gonçalves, B, Kurtz, P, Turon, R, Santos, T, Prazeres, M, Righy, C, et al. Incidence and impact of sepsis on long-term outcomes after subarachnoid hemorrhage: a prospective observational study. Ann Intensive Care. (2019) 9:94. doi: 10.1186/s13613-019-0562-3
2. Centner, FS, Oster, ME, Dally, FJ, Sauter-Servaes, J, Pelzer, T, Schoettler, JJ, et al. Comparative analyses of the impact of different criteria for Sepsis diagnosis on outcome in patients with spontaneous subarachnoid hemorrhage. J Clin Med. (2022) 11:3873. doi: 10.3390/jcm11133873
3. Eagles, ME, Tso, MK, and Macdonald, RL. Cognitive impairment, functional outcome, and delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. World Neurosurg. (2019) 124:e558–62. doi: 10.1016/j.wneu.2018.12.152
4. Abdulazim, A, Heilig, M, Rinkel, G, and Etminan, N. Diagnosis of delayed cerebral ischemia in patients with aneurysmal subarachnoid hemorrhage and triggers for intervention. Neurocrit Care. (2023) 39:311–9. doi: 10.1007/s12028-023-01812-3
5. Pan, S, Lv, Z, Wang, R, Shu, H, Yuan, S, Yu, Y, et al. Sepsis-induced brain dysfunction: pathogenesis, diagnosis, and treatment. Oxidative Med Cell Longev. (2022) 2022:1328729–13. doi: 10.1155/2022/1328729
6. Sharshar, T, Annane, D, de la Grandmaison, GL, Brouland, JP, Hopkinson, NS, and Françoise, G. The neuropathology of septic shock. Brain Pathol. (2004) 14:21–33. doi: 10.1111/j.1750-3639.2004.tb00494.x
7. Budohoski, KP, Czosnyka, M, Smielewski, P, Kasprowicz, M, Helmy, A, Bulters, D, et al. Impairment of cerebral autoregulation predicts delayed cerebral ischemia after subarachnoid hemorrhage: a prospective observational study. Stroke. (2012) 43:3230–7. doi: 10.1161/strokeaha.112.669788
8. Lelubre, C, and Vincent, JL. Mechanisms and treatment of organ failure in sepsis. Nat Rev Nephrol. (2018) 14:417–27. doi: 10.1038/s41581-018-0005-7
9. Suzuki, H, Kanamaru, H, Kawakita, F, Asada, R, Fujimoto, M, and Shiba, M. Cerebrovascular pathophysiology of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. Histol Histopathol. (2021) 36:143–58. doi: 10.14670/hh-18-253
10. McBride, DW, Blackburn, SL, Peeyush, KT, Matsumura, K, and Zhang, JH. The role of Thromboinflammation in delayed cerebral ischemia after subarachnoid hemorrhage. Front Neurol. (2017) 8:555. doi: 10.3389/fneur.2017.00555
11. Foreman, PM, Chua, M, Harrigan, MR, Fisher, WS 3rd, Vyas, NA, Lipsky, RH, et al. Association of nosocomial infections with delayed cerebral ischemia in aneurysmal subarachnoid hemorrhage. J Neurosurg. (2016) 125:1383–9. doi: 10.3171/2015.10.Jns151959
12. Vergouwen, MD, Ilodigwe, D, and Macdonald, RL. Cerebral infarction after subarachnoid hemorrhage contributes to poor outcome by vasospasm-dependent and-independent effects. Stroke. (2011) 42:924–9. doi: 10.1161/STROKEAHA.110.597914
13. Vergouwen, MD, Vermeulen, M, van Gijn, J, Rinkel, GJ, Wijdicks, EF, Muizelaar, JP, et al. Definition of delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage as an outcome event in clinical trials and observational studies: proposal of a multidisciplinary research group. Stroke. (2010) 41:2391–5. doi: 10.1161/STROKEAHA.110.589275
14. Coelembier, C, Venet, F, Demaret, J, Viel, S, Lehot, JJ, Dailler, F, et al. Impact of ventilator-associated pneumonia on cerebrospinal fluid inflammation during immunosuppression after subarachnoid hemorrhage: a pilot study. J Neurosurg Anesthesiol. (2022) 34:e57–62. doi: 10.1097/ana.0000000000000732
15. Jeon, SB, Choi, HA, Badjatia, N, Schmidt, JM, Lantigua, H, Claassen, J, et al. Hyperoxia may be related to delayed cerebral ischemia and poor outcome after subarachnoid haemorrhage. J Neurol Neurosurg Psychiatry. (2014) 85:1301–7. doi: 10.1136/jnnp-2013-307314
16. Singer, M, Deutschman, CS, Seymour, CW, Shankar-Hari, M, Annane, D, Bauer, M, et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA. (2016) 315:801–10. doi: 10.1001/jama.2016.0287
17. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gøtzsche, PC, and Vandenbroucke, JP. The Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
18. Horan, TC, Andrus, M, and Dudeck, MA. CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. (2008) 36:309–32. doi: 10.1016/j.ajic.2008.03.002
19. Vincent, J-L, Moreno, R, Takala, J, Willatts, S, De Mendonça, A, Bruining, H, et al. The SOFA (Sepsis-related organ failure assessment) score to describe organ dysfunction/failure. Intensive Care Med. (1996) 22:707–10. doi: 10.1007/BF01709751
20. Centner, F-S, Schoettler, JJ, Fairley, A-M, Lindner, HA, Schneider-Lindner, V, Weiss, C, et al. Impact of different consensus definition criteria on sepsis diagnosis in a cohort of critically ill patients—insights from a new mathematical probabilistic approach to mortality-based validation of sepsis criteria. PLoS One. (2020) 15:e0238548. doi: 10.1371/journal.pone.0238548
21. Abdulazim, A, Küppers, C, Hackenberg, KAM, Neumaier-Probst, E, Alzghloul, MM, Krebs, J, et al. Multidisciplinary and standardized management of patients with delayed cerebral ischemia after aneurysmal subarachnoid hemorrhage. Acta Neurochir. (2022) 164:2917–26. doi: 10.1007/s00701-022-05347-y
22. Etminan, N, Beseoglu, K, Heiroth, H-J, Turowski, B, Steiger, HJ, and Hänggi, D. Early perfusion computerized tomography imaging as a radiographic surrogate for delayed cerebral ischemia and functional outcome after subarachnoid hemorrhage. Stroke. (2013) 44:1260–6. doi: 10.1161/STROKEAHA.111.675975
23. Etminan, N, Beseoglu, K, Eicker, SO, Turowski, B, Steiger, H-J, and Hänggi, D. Prospective, randomized, open-label phase II trial on concomitant intraventricular fibrinolysis and low-frequency rotation after severe subarachnoid hemorrhage. Stroke. (2013) 44:2162–8. doi: 10.1161/STROKEAHA.113.001790
24. Dellinger, RP, Levy, MM, Rhodes, A, Annane, D, Gerlach, H, Opal, SM, et al. Surviving Sepsis campaign: international guidelines for management of severe sepsis and septic shock, 2012. Intensive Care Med. (2013) 39:165–228. doi: 10.1007/s00134-012-2769-8
25. Rhodes, A, Evans, LE, Alhazzani, W, Levy, MM, Antonelli, M, Ferrer, R, et al. Surviving sepsis campaign: international guidelines for management of sepsis and septic shock: 2016. Intensive Care Med. (2017) 43:304–77. doi: 10.1007/s00134-017-4683-6
26. Lang, TA, and Altman, DG. Basic statistical reporting for articles published in biomedical journals: the “statistical analyses and methods in the published literature” or the SAMPL guidelines. Int J Nurs Stud. (2015) 52:5–9. doi: 10.1016/j.ijnurstu.2014.09.006
27. Flottmann, F, van Horn, N, Maros, ME, Leischner, H, Bechstein, M, Meyer, L, et al. More retrieval attempts are associated with poorer functional outcome after unsuccessful Thrombectomy. Clin Neuroradiol. (2022) 32:361–8. doi: 10.1007/s00062-021-01054-w
28. Christoffersen, B.. Comparing Methods for Time Varying Logistic Models. (2017). Available at: http://cran.nexr.com/web/packages/dynamichazard/vignettes/Comparing_methods_for_logistic_models.pdf. (Accessed January 27, 2024)
29. Therneau, T, Crowson, C, and Atkinson, E. Using Time Dependent Covariates and Time Dependent Coefficients in the Cox Model. (2023). Available at: https://cran.r-project.org/web/packages/survival/vignettes/timedep.pdf. (Accessed January 27, 2024)
30. Yoshida, K, Bartel, A, Chipman, JJ, Bohn, J, DAgostino McGowan, L, Barrett, M, et al. Create ‘Table 1’ to Describe Baseline Characteristics with or Without Propensity Score Weights. (2022). Available at: https://cran.r-project.org/web/packages/tableone/tableone.pdf. (Accessed February 28, 2024)
31. Wenz, H, Maros, ME, Meyer, M, Förster, A, Haubenreisser, H, Kurth, S, et al. Image quality of 3rd generation spiral cranial dual-source CT in combination with an advanced model iterative reconstruction technique: a prospective intra-individual comparison study to standard sequential cranial CT using identical radiation dose. PLoS One. (2015) 10:e0136054. doi: 10.1371/journal.pone.0136054
32. Weyer, V, Maros, ME, Kronfeld, A, Kirschner, S, Groden, C, Sommer, C, et al. Longitudinal imaging and evaluation of SAH-associated cerebral large artery vasospasm in mice using micro-CT and angiography. J Cereb Blood Flow Metab. (2020) 40:2265–77. doi: 10.1177/0271678x19887052
33. de Rooij, NK, Rinkel, GJ, Dankbaar, JW, and Frijns, CJ. Delayed cerebral ischemia after subarachnoid hemorrhage: a systematic review of clinical, laboratory, and radiological predictors. Stroke. (2013) 44:43–54. doi: 10.1161/strokeaha.112.674291
34. Ya, X, Zhang, C, Zhang, S, Zhang, Q, Cao, Y, Wang, S, et al. The relationship between smoking and delayed cerebral ischemia after intracranial aneurysm rupture: a systematic review and Meta-analysis. Front Neurol. (2021) 12:625087. doi: 10.3389/fneur.2021.625087
35. Verboom, DM, Frencken, JF, Ong, DS, Horn, J, van der Poll, T, Bonten, MJ, et al. Robustness of sepsis-3 criteria in critically ill patients. J Intensive Care. (2019) 7:46. doi: 10.1186/s40560-019-0400-6
36. Flinspach, AN, Konczalla, J, Seifert, V, Zacharowski, K, Herrmann, E, Balaban, Ü, et al. Detecting Sepsis in patients with severe subarachnoid hemorrhage during critical care. J Clin Med. (2022) 11:4229. doi: 10.3390/jcm11144229
37. Szatmári, S, Végh, T, Csomós, A, Hallay, J, Takács, I, Molnár, C, et al. Impaired cerebrovascular reactivity in sepsis-associated encephalopathy studied by acetazolamide test. Crit Care. (2010) 14:R50. doi: 10.1186/cc8939
38. van den Brule, JMD, Stolk, R, Vinke, EJ, van Loon, LM, Pickkers, P, van der Hoeven, JG, et al. Vasopressors do not influence cerebral critical closing pressure during systemic inflammation evoked by experimental Endotoxemia and Sepsis in humans. Shock. (2018) 49:529–35. doi: 10.1097/shk.0000000000001003
39. Taccone, FS, Scolletta, S, Franchi, F, Donadello, K, and Oddo, M. Brain perfusion in sepsis. Curr Vasc Pharmacol. (2013) 11:170–86. doi: 10.2174/1570161111311020007
40. Ren, C, Yao, RQ, Zhang, H, Feng, YW, and Yao, YM. Sepsis-associated encephalopathy: a vicious cycle of immunosuppression. J Neuroinflammation. (2020) 17:14. doi: 10.1186/s12974-020-1701-3
41. Iwashyna, TJ, Ely, EW, Smith, DM, and Langa, KM. Long-term cognitive impairment and functional disability among survivors of severe sepsis. JAMA. (2010) 304:1787–94. doi: 10.1001/jama.2010.1553
42. Frontera, JA, Fernandez, A, Schmidt, JM, Claassen, J, Wartenberg, KE, Badjatia, N, et al. Impact of nosocomial infectious complications after subarachnoid hemorrhage. Neurosurgery. (2008) 62:80–7. doi: 10.1227/01.NEU.0000311064.18368.EA
43. Hammer, A, Ranaie, G, Erbguth, F, Hohenhaus, M, Wenzl, M, Killer-Oberpfalzer, M, et al. Impact of complications and comorbidities on the intensive care length of stay after aneurysmal subarachnoid Haemorrhage. Sci Rep. (2020) 10:1–9. doi: 10.1038/s41598-020-63298-9
44. Schamoni, S, Lindner, HA, Schneider-Lindner, V, Thiel, M, and Riezler, S. Leveraging implicit expert knowledge for non-circular machine learning in sepsis prediction. Artif Intell Med. (2019) 100:101725. doi: 10.1016/j.artmed.2019.101725
Keywords: delayed cerebral ischemia, sepsis, subarachnoid hemorrhage, sepsis criteria, propensity score (PS) matching (PSM)
Citation: Centner F-S, Wenz H, Oster ME, Dally F-J, Sauter-Servaes J, Pelzer T, Schoettler JJ, Hahn B, Abdulazim A, Hackenberg KAM, Groden C, Krebs J, Thiel M, Etminan N and Maros ME (2024) Sepsis and delayed cerebral ischemia are associated and have a cumulative effect on poor functional outcome in aneurysmal subarachnoid hemorrhage. Front. Neurol. 15:1393989. doi: 10.3389/fneur.2024.1393989
Edited by:
Mu Li, Huazhong University of Science and Technology, ChinaReviewed by:
J. Javier Provencio, University of Virginia, United StatesDaniel Dubinski, University Hospital Rostock, Germany
Copyright © 2024 Centner, Wenz, Oster, Dally, Sauter-Servaes, Pelzer, Schoettler, Hahn, Abdulazim, Hackenberg, Groden, Krebs, Thiel, Etminan and Maros. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Máté E. Maros, bWFyb3NAdW5pLWhlaWRlbGJlcmcuZGU=