 Yu Yao
Yu Yao
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol. , 19 April 2024
Sec. Stroke
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1386386
This article is part of the Research Topic Advances and controversies in ischemic stroke management: from prevention to diagnosis and acute treatment View all 95 articles
Background: This retrospective observational cohort study aimed to evaluate whether tenecteplase’s use for acute ischemic stroke (AIS) has time management advantages and clinical benefits.
Methods: 144 AIS patients treated with alteplase and 120 with tenecteplase were included. We compared baseline clinical characteristics, key reperfusion therapy time indices [onset-to-treatment time (OTT), door-to-needle time (DNT), and door-to-puncture time (DPT)] and clinical outcomes (24-h post-thrombolysis NIHSS improvement, and intracranial hemorrhage incidence) between the groups using univariate analysis. We assessed hospital stay durations and used binary logistic regression to examine tenecteplase’s association with DNT and DPT target times, NIHSS improvement, and intracranial hemorrhage.
Results: Baseline characteristics showed no significant differences except hyperlipidemia and atrial fibrillation. OTT (133 vs. 163.72, p = 0.001), DNT (36.5 vs. 50, p < 0.001) and DPT (117 vs. 193, p = 0.002) were significantly faster in the tenecteplase group. The rates of DNT ≤ 45 min (65.83% vs. 40.44%, p < 0.001) and DPT ≤ 120 min (59.09% vs. 13.79%, p = 0.001) were significantly higher in the tenecteplase group. Tenecteplase was an independent predictor of achieving target DNT (OR 2.951, 95% CI 1.732–5.030; p < 0.001) and DPT (OR 7.867, 95% CI 1.290–47.991; p = 0.025). Clinically, the proportion NIHSS improvement 24 h post-thrombolysis was higher in the tenecteplase group (64.17% vs. 50%, p = 0.024). No significant differences were observed in symptomatic intracranial hemorrhage (sICH) or any intracranial hemorrhage (ICH). Patients receiving tenecteplase had shorter hospital stays (6 vs. 8 days, p < 0.001). Tenecteplase was an independent predictor of NIHSS improvement at 24 h (OR 1.715, 95% CI 1.011–2.908; p = 0.045). There was no significant association between thrombolytic choice and sICH or any ICH.
Conclusion: Tenecteplase significantly reduced DNT and DPT. It was associated with early neurological function improvement (at 24 h), without compromising safety compared to alteplase. The findings support tenecteplase’s application in AIS.
Intravenous thrombolysis represents a safe and effective approach for acute ischemic stroke (AIS)'s ultra-early treatment. Following the 1996 US FDA approval of the recombinant tissue plasminogen activator (alteplase, rt-PA), extensive researches have confirmed that alteplase can significantly improve clinical outcomes. However, its specificity for fibrin is moderate and the risk of intracranial hemorrhage still exists. Alteplase has a short half-life (4–5 min), and its administration is complex, requiring intravenous bolus followed by a continuous infusion for 1 h; the efficiency of this ultra-early treatment workflow still needs improvement. Despite updates and iterations with alternatives such as recombinant human pro-urokinase (rhPro-UK), ancrod, and desmoteplase, a series of clinical trials have not demonstrated significant advantages in functional improvement. Moreover, these alternatives showed no significant difference, and in some cases, a slightly higher risk of hemorrhage, especially intracranial hemorrhage, compared to control drugs (1–4). This was the case until the advent of tenecteplase (TNK-tPA). Tenecteplase, a DNA variant of alteplase (5), exhibits enhanced fibrin specificity and greater resistance to plasminogen activator inhibitor-1 (PAI-1) (6), effectively targeting thrombi. Its improved fibrin specificity minimizes systemic fibrinogen consumption, substantially reducing hemorrhage risk. Additionally, tenecteplase’s extended plasma half-life (7, 8) permits a 5–10 s intravenous injection administration (9–11).
As a third-generation anti-fibrinolytic intravenous thrombolytic drug, tenecteplase boasts a well-characterized mechanism of action and significant practical advantages in administration, making it a promising candidate. Multiple studies have confirmed that its efficacy and safety may not be inferior to that of alteplase (12–17). And it has potential workflow advantages (18).
This study aims to evaluate whether tenecteplase’s use in routine clinical practice has time management advantages and corresponding clinical benefits, providing a basis for analyzing the rationale behind tenecteplase’s off-label application.
This study is a retrospective observational cohort study. We included AIS patients who received alteplase at the first affiliated Hospital of Ningbo University from January 2022 to February 2023 and those treated with tenecteplase (Mingfule, CSPC Recomgen Pharmaceutical [Guangzhou] Co., Ltd., China) from March 2023 to November 2023. Eligible patients were: (1) 18 years or older; (2) diagnosed with ischemic stroke per established criteria, with measurable neurological deficits; (3) treated within 4.5 h of symptom onset; (4) confirmed via CT or MRI to have no hemorrhage, extensive cerebral infarction, or other non-stroke pathologies; (5) provided informed consent, either personally or through family members (19). Exclusion criteria included standard contraindications to alteplase. The administered dosages were 0.9 mg/kg (maximum 90 mg) for alteplase and 0.25 mg/kg (maximum 25 mg) for tenecteplase. In March 2023, ethical considerations for clinical tenecteplase use and off-label usage were thoroughly addressed, in compliance with relevant regulations (ethical review number 2023-03-59). This study received approval from the Medical Ethics Committee of the First Affiliated Hospital of Ningbo University (ethics approval number 2023-175RS).
This study was performed in accordance with the Strengthening Reporting of Observational Studies in Epidemiology (STROBE) reporting guidelines (20).
Clinical data were obtained from the emergency and inpatient information management system. Baseline characteristics included gender, age, body mass index (BMI), hypertension, diabetes, hyperlipidemia, baseline National Institutes of Health Stroke Scale (NIHSS; a 42-point scale that quantifies neurologic deficits in 11 categories, with higher scores indicating more severe deficits) scores, and baseline modified Rankin scale (mRS; a seven point ordered classification scale reflecting functional neurological outcomes from 0 to 6, with 0 indicating no symptoms of neurological deficits and 6 indicating death) scores.
Critical time points such as onset-to-treatment time (OTT), door-to-needle time (DNT), and door-to-puncture time (DPT) were calculated. The workflow outcomes comprised the proportion of patients treated within the recommended 45-min DNT as per international stroke guidelines (21, 22), and the proportion receiving bridging thrombectomy within the 120-min DPT, the standard time frame established by the Stroke Prevention and Treatment Project Committee of the National Health Commission for advanced stroke centers.
Post-thrombolysis 24-h NIHSS scores, cerebral imaging results (CT or MRI was performed before treatment and 22 to 36 h after thrombolysis treatment. Other CT scans were done if necessary.), and hospital stay durations were collected. Digital subtraction angiography (DSA) records of patients with large vessel occlusions (LVO) who received thrombectomy were also retrospected.
Clinical outcomes encompassed both efficacy and safety measures. Efficacy was assessed by the improvement in the NIHSS score at 24 h post-treatment. Safety outcomes included symptomatic intracranial hemorrhage (sICH), defined as any apparently extravascular blood in the brain or within the cranium that was associated with clinical deterioration, as defined by an increase of 4 points or more in the score on the NIHSS, or that led to death and that was identified as the predominant cause of the neurologic deterioration (23), and any intracranial hemorrhage (ICH).
Since tenecteplase has been applied to AIS in our hospital for a short period of time, we lack data of 90-day functional outcomes at present.
All statistical analyses were conducted using SPSS (version 23.0). Continuous data were presented as mean ± standard deviation or median (interquartile range), and categorical data as number (percentage). Univariate analysis was utilized to assess differences between groups. The Independent Student’s t-test was applied to normally distributed variables, and the Mann–Whitney test to non-normally distributed variables. Categorical variables were compared using Pearson’s chi-squared test or Fisher’s exact test. Variables that could potentially influence outcomes (age, hypertension, diabetes, baseline NIHSS, baseline mRS), those with a p-value < 0.05 in univariate analysis, and the type of thrombolytic drug were included in binary logistic regression models to identify independent predictors of outcomes. p-values <0.05 were considered statistically significant.
The study initially reviewed records of 124 patients treated with tenecteplase and 148 with alteplase. After 1 patient with incomplete data and 7 lost to follow-up being excluded, 120 patients treated with tenecteplase and 144 with alteplase were included in the study.
The demographic data (male [75.8% vs. 68.1%, p = 0.163] and age [66.5 vs. 67.75, p = 0.122]) and vascular risk factors (BMI [23.75 vs. 23.92, p = 0.727], hypertension [63.3% vs. 54.2%, p = 0.133], diabetes [14.2% vs. 19.4%, p = 0.256]) were comparable between groups. Significant differences were noted in the prevalence of hyperlipidemia (21.7% vs. 12.5%, p = 0.047) and atrial fibrillation (21.7% vs. 34%, p = 0.027) in the tenecteplase group. There were 38 patients in the tenecteplase group and 50 patients in the alteplase group had LVO (31.7% vs. 34.7%, p = 0.600). Baseline NIHSS (4.5 vs. 7, p = 0.155) and mRS (3 vs. 3.5, p = 0.633) scores, as well as the proportion undergoing bridging thrombectomy (20.0% vs. 22.9%, p = 0.566), did not significantly differ (Table 1).
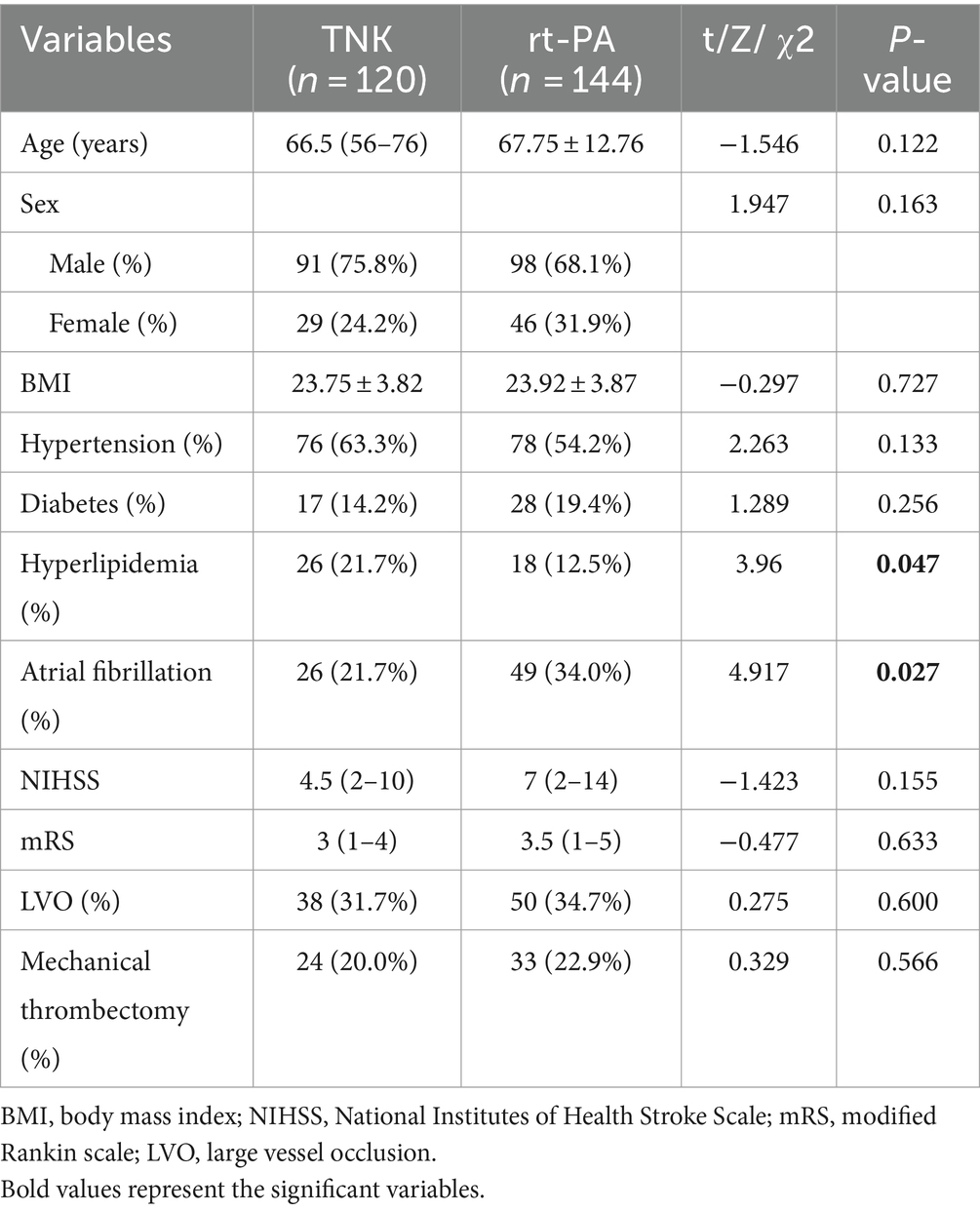
Table 1. Characteristics of the patients at baseline.
In AIS reperfusion therapy, key time metrics such as OTT, DNT, and DPT were significantly lower in the tenecteplase group (OTT: 133 vs. 163.72, p = 0.001; DNT: 36.5 vs. 50, p < 0.001; DPT: 117 vs. 193, p = 0.002). The proportions of patients in the tenecteplase group achieving DNT ≤ 45 min (65.83% vs. 40.44%, p < 0.001) and DPT ≤ 120 min (59.09% vs. 13.79%, p = 0.001) were significantly higher than in the alteplase group (Table 2). Binary logistic regression, incorporating baseline characteristics (age, hypertension, diabetes, hyperlipidemia, atrial fibrillation, baseline NIHSS, and baseline mRS) and thrombolytic drugs, indicated that tenecteplase was an independent predictor of meeting target times for DNT (OR 2.951, 95% CI 1.732–5.030; p < 0.001) and DPT (OR 7.867, 95% CI 1.290–47.991; p = 0.025; Table 3). Baseline characteristics such as NIHSS did not affect workflow outcomes (p > 0.05).
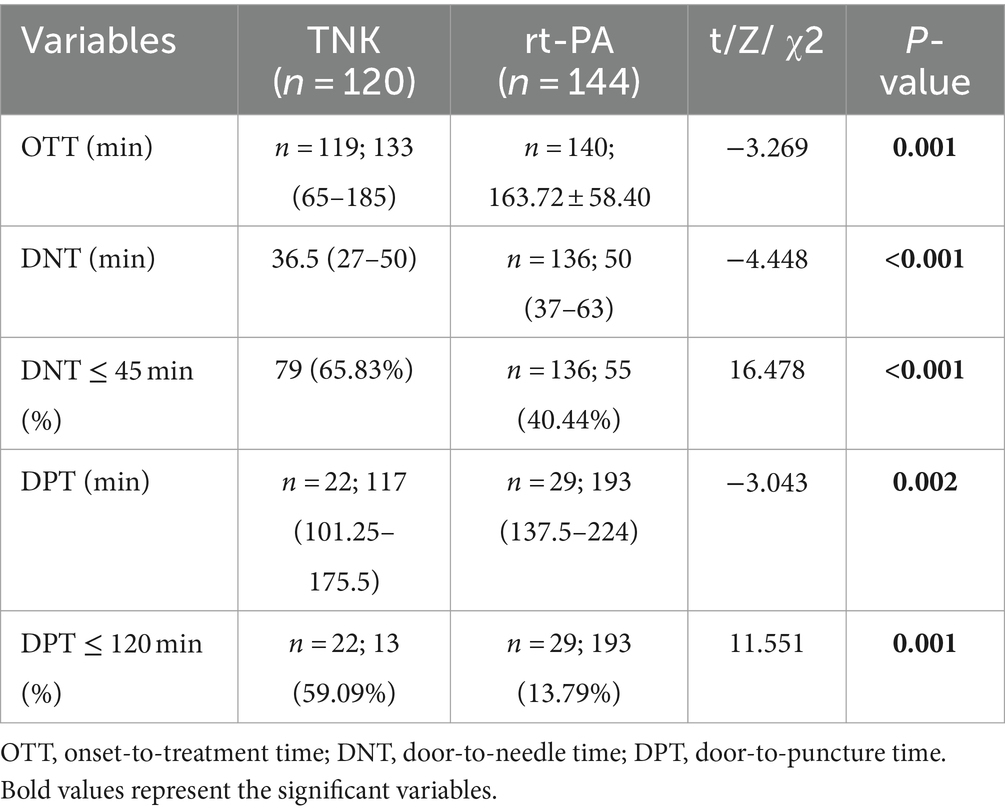
Table 2. Treatment-related timings.
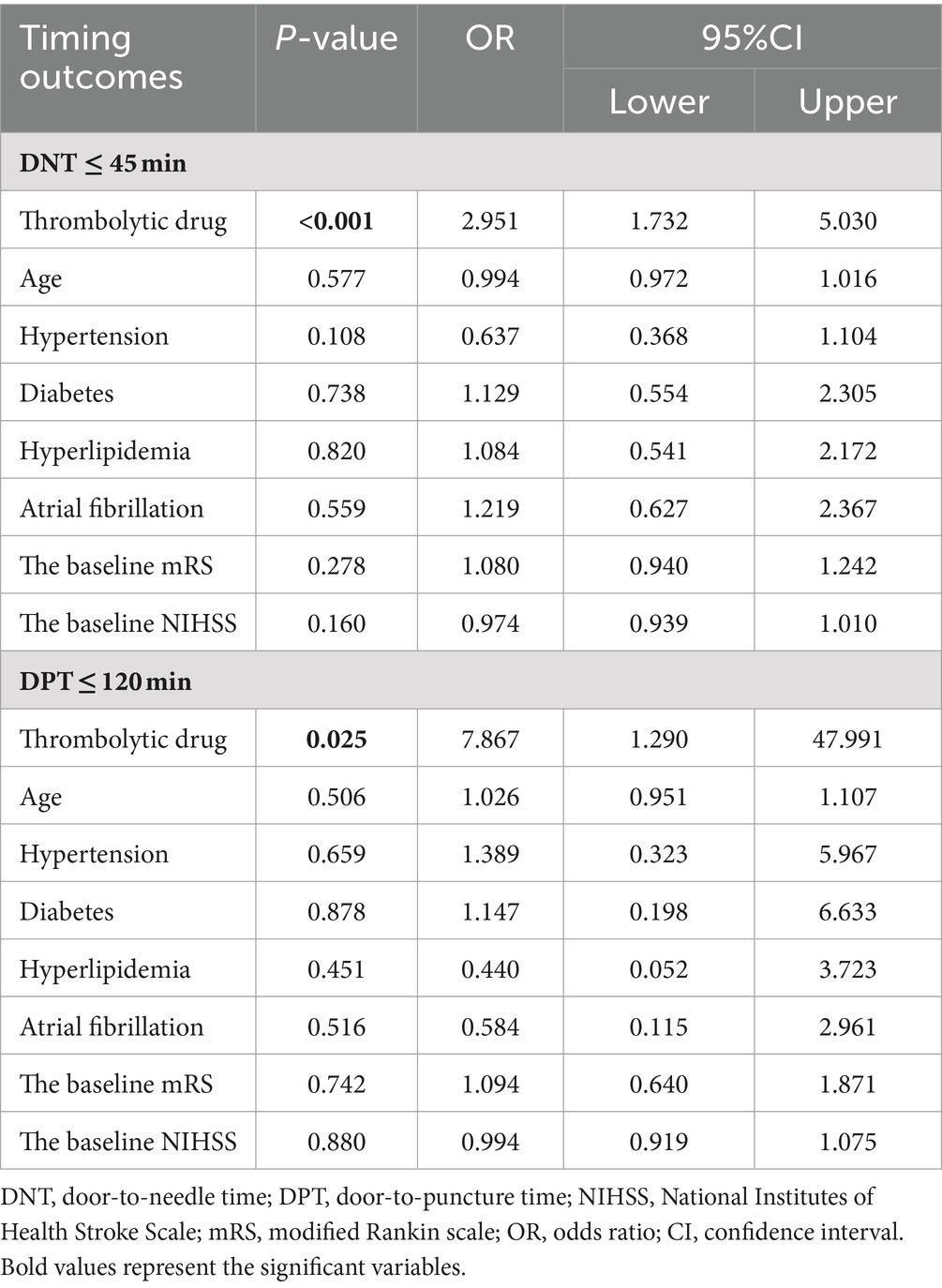
Table 3. Multivariate analysis of workflow outcomes.
Regarding clinical outcomes, the tenecteplase group showed a significantly higher percentage of NIHSS improvement 24 h post-thrombolysis (64.17% vs. 50%, p = 0.024). More patients with LVO who received thrombectomy (bridging therapy) in the tenecteplase group was showed partial recanalization at the first DSA (16.7% vs. 0%, p = 0.027). The incidences of sICH (3.33% vs. 4.86%, p = 0.536) or any ICH (13.3% vs. 15.28%, p = 0.654) did not differ significantly. Tenecteplase patients had shorter hospital stays (6 vs. 8, P<0.001; Table 4). Binary logistic regression revealed tenecteplase as an independent predictor of 24-h NIHSS improvement (OR 1.715, 95% CI 1.011–2.908; p = 0.045). Baseline NIHSS was identified as an independent risk factor for sICH (OR 1.082, 95% CI 1.020–1.147; p = 0.009) and any ICH (OR 1.065, 95% CI 1.026–1.106; p = 0.001). Atrial fibrillation was an independent risk factor for any ICH (OR 2.605, 95% CI 1.138–5.960; p = 0.023). Other baseline characteristics and thrombolytic drugs did not significantly impact safety outcomes (Table 5).
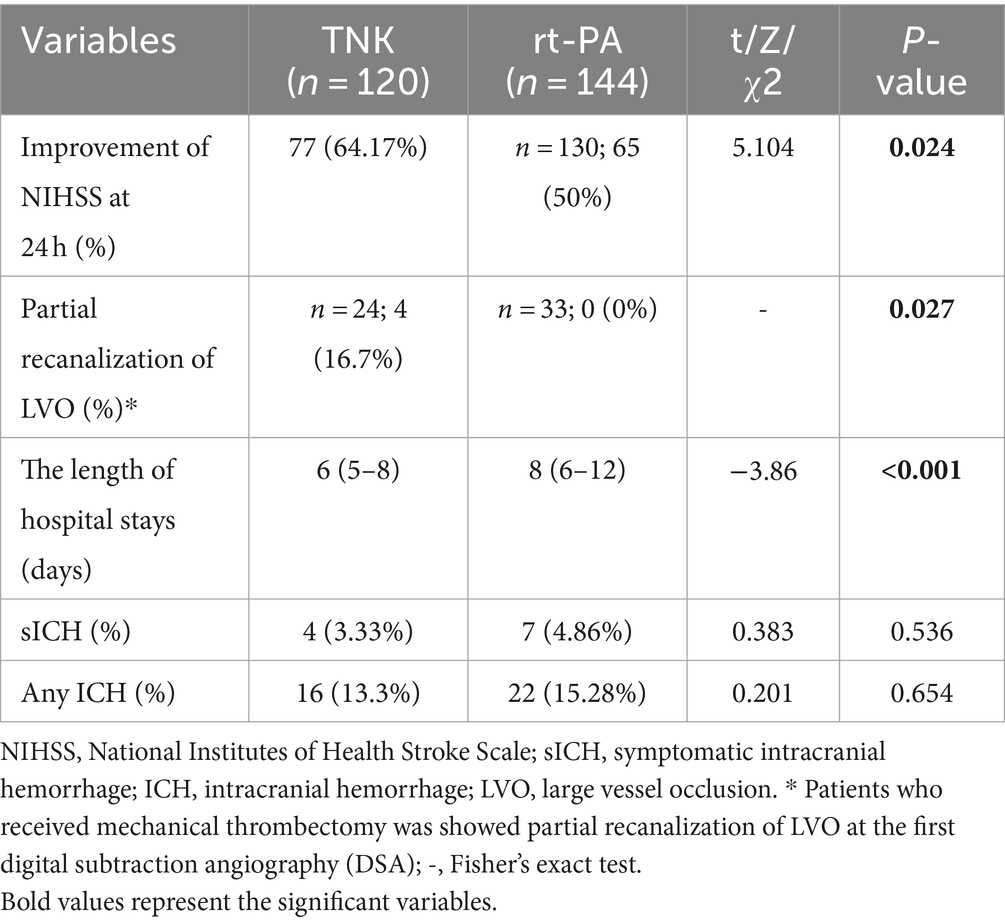
Table 4. Univariate analysis of clinical outcomes.
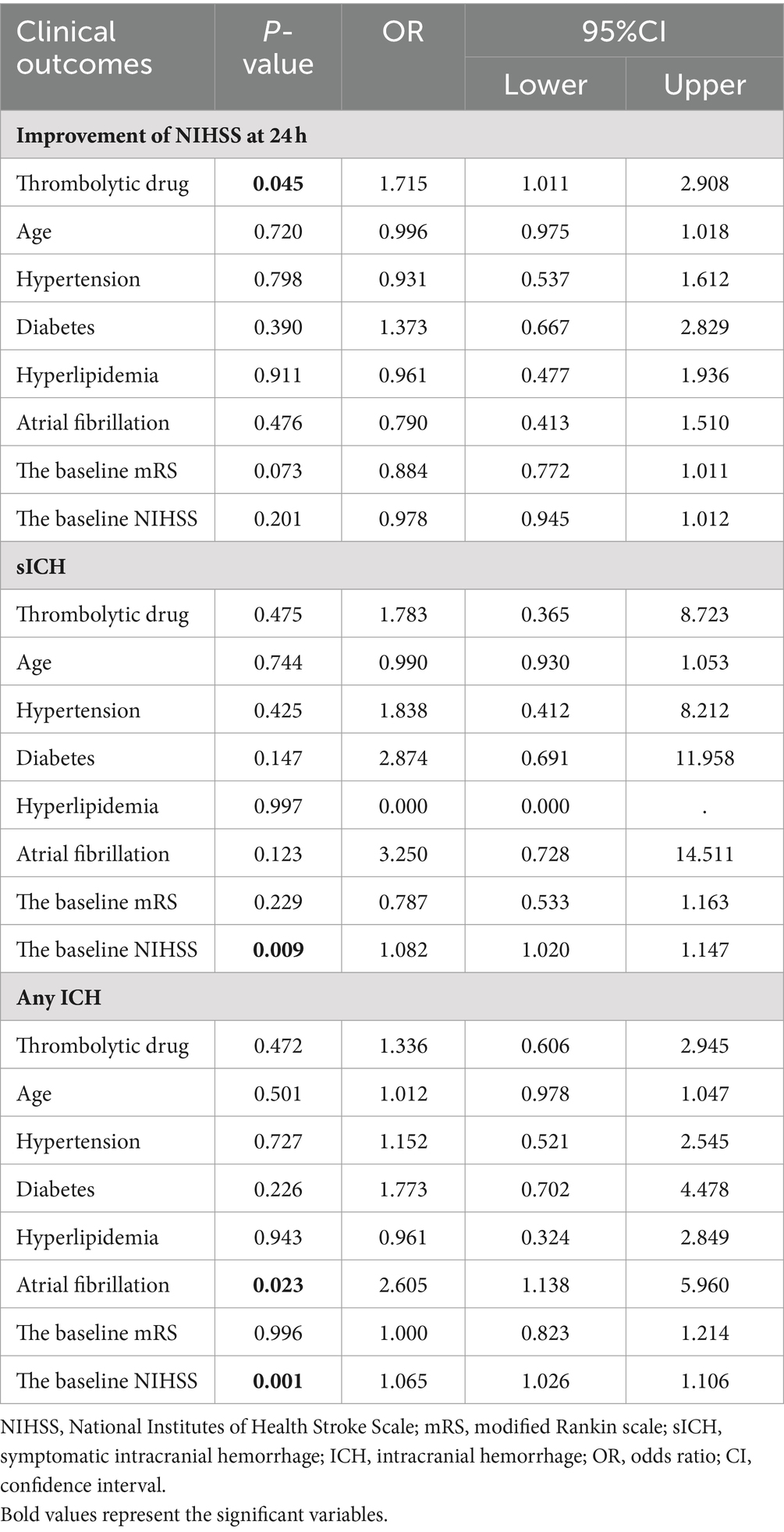
Table 5. Multivariate analysis of clinical outcomes.
Our study is the first retrospective study on the application of tenecteplase in AIS in the real world from China. The study demonstrated that intravenous thrombolysis with tenecteplase is a feasible treatment for AIS, associated with early clinical improvement, enhanced ultra-early treatment workflow efficiency, and reduced hospital stays. Its safety outcomes paralleled those of alteplase.
Our study highlighted early neurological improvement in patients undergoing intravenous thrombolysis, identifying tenecteplase as an independent predictor of 24-h NIHSS improvement, aligning with findings from the TASTE-A trial. Patients treated with tenecteplase at Melbourne mobile stroke units exhibited significantly smaller perfusion lesion volumes upon hospital arrival than those treated with alteplase, indicating a higher early reperfusion rate (13). Multiple studies in clinical practice have suggested that tenecteplase offers substantial clinical benefits. In AIS patients with acute large vessel occlusion (LVO), tenecteplase treatment resulted in higher initial angiography reperfusion rates (17), enhanced 24-h reperfusion and clinical improvement (16), and improved 90-day functional outcomes (17). For all AIS patients eligible for thrombolysis, the tenecteplase group achieved non-inferior rates of long-term functional prognosis (mRS score of 0–1 at 90 days) (12, 14, 15). These benefits are attributable to tenecteplase’s optimized pharmacological properties. As a DNA variant of alteplase, tenecteplase undergoes molecular changes at three sites (T at site 103, N at site 117, and K at sites 296 to 299) (5), enhancing its specificity by 10–14 times compared to alteplase. It directly activates plasminogen into plasmin upon contact with thrombi and exhibits 80 times increased resistance to plasminogen activator inhibitor-1 (PAI-1) (6), thus effectively acting on thrombi with lower dosage but improved efficacy.
Regarding safety outcomes, the incidence of sICH (3.33% in the tenecteplase group and 4.86% in the alteplase group) and any ICH (13.33% in the tenecteplase group and 15.28% in the alteplase group) in the study was consistent with previous studies (14, 15, 23, 24). The incidences of sICH and any ICH were not significantly different between two groups, corroborating previous research (12–15). It is worth mentioning that as for sICH, our results with lower risk of Tenecteplase was similar to the experience from the CERTAIN registry, a large international dataset of early adopters in tenecteplase (25). This safety profile is due to tenecteplase’s fibrin specificity (6), which minimizes systemic fibrinogen consumption and significantly reduces hemorrhage risk.
Supported by high-quality clinical trials, the use of tenecteplase in AIS treatment has been incorporated into several national AIS management guidelines (19, 21, 26). The application of tenecteplase in the real world also increased. Several stroke centers in New Zealand have changed to routine off-label intravenous tenecteplase from July 2018. A retrospective analysis showed that routine use of tenecteplase for stroke thrombolysis was feasible since there was no difference between tenecteplase and alteplase in 90-day functional independence (mRS score, 0–2), and it had comparable safety outcome to alteplase (27). Then on 2 March 2020, the New Zealand Central Region Hyper-Acute Stroke Network collectively switched to tenecteplase. The initiative was also successful that researchers found evidence of benefit and no evidence of harm (28). The 2022 European Stroke Organization Conference (ESOC) highlighted two register studies. Canadian researcher Katsanos, drawing on the international SITS-ISTR registry and the French multicenter TETRIS registry, demonstrated superior 90-day mRS score distributions, lower all-cause mortality, and no increased risk of sICH in the tenecteplase group. This supports the judicious use of tenecteplase in AIS treatment.
In addition to efficacy and safety, tenecteplase was found to enhance key time metrics in AIS treatment, aligning with recent prospective (18) and retrospective studies (29). Its half-life of 20–24 min enables a prolonged effective blood concentration (7, 8), allowing for a rapid 5–10 s intravenous injection, bypassing the need for infusion pumps required for alteplase’s hour-long infusion (9–11). Tenecteplase can quickly initiate treatment without the need for infusion pumps or additional equipment, significantly reducing DNT. The efficacy of intravenous thrombolysis is time-sensitive, with delays diminishing its benefits. DNT, a controllable hospital metric, is crucial for predicting the prognosis of AIS patients receiving thrombolysis (30, 31). It is also a key indicator for establishing efficient stroke pathways. For patients with large vessel occlusion (LVO), current guidelines recommend a bridging treatment approach combining intravenous thrombolysis and arterial embolectomy when criteria for both are met, rather than proceeding directly to endovascular treatment (EVT). Different from alteplase, tenecteplase does not require standard infusion pumps for a one-hour intravenous infusion. This facilitates quicker patient transfer after start of thrombolysis, enhancing stroke green channel management processes and significantly reducing DPT. EVT’s effectiveness is similarly time-dependent (32). Shortening DPT and achieving prompt reperfusion of occluded vessels are linked to improved clinical outcomes (33). But at the same time, it is important to note that intrinsic of tenecteplase, is that one of the strengths is speed of administration but also the lack of opportunity to stop administration in case of adverse reactions. This may be a defect, but considering its low incidence of adverse reactions, tenecteplase is still worth promoting.
Novelly, our study observed a shorter length of hospital stay for patients in the tenecteplase group compared to the alteplase group, suggesting potential savings in medical resources. This may be related to the higher proportion of early neurological function improvement in the tenecteplase group, which accelerates patients’ recovery. Tenecteplase, being less expensive, showed a greater net benefit in overall hospital cost analyses, primarily due to lower hospitalization costs (18). This may also be due to the shortened length of hospitalization. This reduction in drug costs is crucial in cost–benefit analysis and could potentially enhance the savings and quality-adjusted life years in the healthcare system.
However, our study has limitations. (1) It was based on data from a single center, and it is uncertain if similar results would be replicated in other centers or regions. (2) Thrombolytic treatment assignment was neither randomized nor blinded and, therefore, subject to biases in management decisions and outcome assessments. Fortunately, there was not much difference in the baseline characteristics, and we attempted to attenuate this limitation by binary logistic regression. (3) The clinical outcomes reported were early-stage, and further exploration is needed to assess long-term neurological function improvement. Yet, these early indicators have been shown to predict 90-day mRS scores (34), validating their use. (4) Most participants had mild to moderate stroke, the impact of tenecteplase on more severe stroke outcomes remains to be investigated. Future research will aim to expand the sample size and extend follow-up duration to provide more detailed data, such as 90-day mRS scores.
In conclusion, tenecteplase, as a new-generation thrombolytic drug, demonstrated a higher rate of early clinical improvement in AIS treatment and safety comparable to alteplase. Its ease of administration and management significantly enhanced target DNT and DPT achievement rates. Although confirmation in larger multicenter studies and ongoing randomized trials is needed, this study supports the use of tenecteplase in AIS intravenous thrombolysis.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Medical Ethics Committee of the First Affiliated Hospital of Ningbo University. The studies were conducted in accordance with the local legislation and institutional requirements. The ethics committee/institutional review board waived the requirement of written informed consent for participation from the participants or the participants' legal guardians/next of kin due to the retrospective nature of the study.
YYa: Conceptualization, Data curation, Formal analysis, Writing – original draft, Writing – review & editing. YW: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing. XZ: Formal analysis, Methodology, Writing – original draft. CL: Data curation, Writing – original draft. LC: Data curation, Writing – original draft. YYi: Data curation, Writing – original draft. JY: Conceptualization, Formal analysis, Methodology, Supervision, Writing – review & editing, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was supported by Ningbo Top Medical and Health Research Program, China (project code: 2022020304), and Ningbo Science and Technology Plan Project, China (project code: 2022S023).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Hennerici, MG, Kay, R, Bogousslavsky, J, Lenzi, GL, Verstraete, M, Orgogozo, JM, et al. Intravenous ancrod for acute ischaemic stroke in the European stroke treatment with Ancrod trial: a randomised controlled trial. Lancet. (2006) 368:1871–8. doi: 10.1016/S0140-6736(06)69776-6
2. Hacke, W, Albers, G, Al-Rawi, Y, Bogousslavsky, J, Davalos, A, Eliasziw, M, et al. The Desmoteplase in acute ischemic stroke trial (DIAS)—a phase II MRI-based 9-hour window acute stroke thrombolysis trial with intravenous desmoteplase. Stroke. (2005) 36:66–73. doi: 10.1161/01.STR.0000149938.08731.2c
3. Albers, GW, von Kummer, R, Truelsen, T, Jensen, J-KS, Ravn, GM, Gronning, BA, et al. Safety and efficacy of desmoteplase given 3-9 h after ischaemic stroke in patients with occlusion or high-grade stenosis in major cerebral arteries (DIAS-3): a double-blind, randomised, placebo-controlled phase 3 trial. Lancet Neurol. (2015) 14:575–84. doi: 10.1016/S1474-4422(15)00047-2
4. Michels, H, Windeler, B, and Hopkins, F. A double-blind multicenter comparison of the efficacy and safety of Saruplase and Urokinase in the treatment of acute myocardial infarction: report of the SUTAMI study group. J Thromb Thrombolysis. (1995) 2:117–24. doi: 10.1007/BF01064379
5. Behrouz, R . Intravenous tenecteplase in acute ischemic stroke: an updated review. J Neurol. (2014) 261:1069–72. doi: 10.1007/s00415-013-7102-0
6. Huber, K . Plasminogen activator inhibitor type-1 (part two): role for failure of thrombolytic therapy. PAI-1 resistance as a potential benefit for new fibrinolytic agents. J Thromb Thrombolysis. (2001) 11:195–202. doi: 10.1023/A:1011952602122
7. Warach, SJ, Dula, AN, and Milling, TJ Jr. Tenecteplase thrombolysis for acute ischemic stroke. Stroke. (2020) 51:3440–51. doi: 10.1161/STROKEAHA.120.029749
8. Tanswell, P, Modi, N, Combs, D, and Danays, T. Pharmacokinetics and pharmacodynamics of tenecteplase in fibrinolytic therapy of acute myocardial infarction. Clin Pharmacokinet. (2002) 41:1229–45. doi: 10.2165/00003088-200241150-00001
9. Keyt, BA, Paoni, NF, Refino, CJ, Berleau, L, Nguyen, H, Chow, A, et al. A faster-acting and more potent form of tissue plasminogen activator. Proc Natl Acad Sci USA. (1994) 91:3670–4. doi: 10.1073/pnas.91.9.3670
10. Modi, NB, Fox, NL, Clow, FW, Tanswell, P, Cannon, CP, Van de Werf, F, et al. Pharmacokinetics and pharmacodynamics of tenecteplase: results from a phase II study in patients with acute myocardial infarction. J Clin Pharmacol. (2000) 40:508–15. doi: 10.1177/00912700022009125
11. Stewart, RJ, Fredenburgh, JC, Leslie, BA, Keyt, BA, Rischke, JA, and Weitz, JI. Identification of the mechanism responsible for the increased fibrin specificity of TNK-tissue plasminogen activator relative to tissue plasminogen activator. J Biol Chem. (2000) 275:10112–20. doi: 10.1074/jbc.275.14.10112
12. Logallo, N, Novotny, V, Assmus, J, Kvistad, CE, Alteheld, L, Ronning, OM, et al. Tenecteplase versus alteplase for management of acute ischaemic stroke (NOR-TEST): a phase 3, randomised, open-label, blinded endpoint trial. Lancet Neurol. (2017) 16:781–8. doi: 10.1016/S1474-4422(17)30253-3
13. Bivard, A, Zhao, H, Churilov, L, Campbell, BCV, Coote, S, Yassi, N, et al. Comparison of tenecteplase with alteplase for the early treatment of ischaemic stroke in the Melbourne Mobile stroke unit (TASTE-A): a phase 2, randomised, open-label trial. Lancet Neurol. (2022) 21:520–7. doi: 10.1016/S1474-4422(22)00171-5
14. Menon, BK, Buck, BH, Singh, N, Deschaintre, Y, Almekhlafi, MA, Coutts, SB, et al. Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, non-inferiority trial. Lancet. (2022) 400:161–9. doi: 10.1016/S0140-6736(22)01054-6
15. Wang, Y, Li, S, and Pan, Y. Tenecteplase versus alteplase in acute ischaemic cerebrovascular events (TRACE-2): a phase 3, multicentre, open-label, randomised controlled, non-inferiority trial. Lancet. (2023) 401:1078–8. doi: 10.1016/S0140-6736(22)02600-9
16. Parsons, M, Spratt, N, Bivard, A, Campbell, B, Chung, K, Miteff, F, et al. A randomized trial of Tenecteplase versus Alteplase for acute ischemic stroke. N Engl J Med. (2012) 366:1099–107. doi: 10.1056/NEJMoa1109842
17. Campbell, BCV, Mitchell, PJ, Churilov, L, Yassi, N, Kleinig, TJ, Dowling, RJ, et al. Tenecteplase versus Alteplase before Thrombectomy for ischemic stroke. N Engl J Med. (2018) 378:1573–82. doi: 10.1056/NEJMoa1716405
18. Warach, SJ, Dula, AN, Milling, TJ, Miller, S, Allen, L, Zuck, ND, et al. Prospective observational cohort study of Tenecteplase versus Alteplase in routine clinical practice. Stroke. (2022) 53:3583–93. doi: 10.1161/STROKEAHA.122.038950
19. Berge, E, Whiteley, W, Audebert, H, Marchis, GMD, Fonseca, AC, Padiglioni, C, et al. European stroke organisation (ESO) guidelines on intravenous thrombolysis for acute ischaemic stroke. Eur Stroke J. (2021) 6:I–LXII. doi: 10.1177/2396987321989865
20. von Elm, E, Altman, DG, Egger, M, Pocock, SJ, Gotzsche, PC, Vandenbroucke, JP, et al. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Lancet. (2007) 370:1453–7. doi: 10.1016/S0140-6736(07)61602-X
21. Powers, WJ, Rabinstein, AA, Ackerson, T, Adeoye, OM, Bambakidis, NC, Becker, K, et al. Guidelines for the early Management of Patients with Acute Ischemic Stroke: 2019 update to the 2018 guidelines for the early Management of Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2019) 50:E344–418. doi: 10.1161/STR.0000000000000211
22. Powers, WJ, Rabinstein, AA, Ackerson, T, Adeoye, OM, Bambakidis, NC, Becker, K, et al. 2018 guidelines for the early Management of Patients with Acute Ischemic Stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2018) 49:E46–E110. doi: 10.1161/STR.0000000000000158
23. Hacke, W, Kaste, M, Bluhmki, E, Brozman, M, Davalos, A, Guidetti, D, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. (2008) 359:1317–29. doi: 10.1056/NEJMoa0804656
24. Hacke, W, Kaste, M, Fieschi, C, von Kummer, R, Davalos, A, Meier, D, et al. Randomised double-blind placebo-controlled trial of thrombolytic therapy with intravenous alteplase in acute ischaemic stroke (ECASS II). Lancet. (1998) 352:1245–51. doi: 10.1016/S0140-6736(98)08020-9
25. Warach, SJJ, Ranta, A, Kim, J, Song, SSS, Wallace, A, Beharry, J, et al. Symptomatic intracranial hemorrhage with Tenecteplase vs Alteplase in patients with acute ischemic stroke the comparative effectiveness of routine Tenecteplase vs Alteplase in acute ischemic stroke (CERTAIN) collaboration. JAMA Neurol. (2023) 80:732–8. doi: 10.1001/jamaneurol.2023.1449
26. Liu, L, Chen, W, Zhou, H, Duan, W, Li, S, Huo, X, et al. Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of ischaemic cerebrovascular diseases. Stroke Vasc Neurol. (2020) 5:159–76. doi: 10.1136/svn-2020-000378
27. Zhong, CS, Beharry, J, Salazar, D, Smith, K, Withington, S, Campbell, BCV, et al. Routine use of Tenecteplase for thrombolysis in acute ischemic stroke. Stroke. (2021) 52:1087–90. doi: 10.1161/STROKEAHA.120.030859
28. Mahawish, K, Gommans, J, Kleinig, T, Lallu, B, Tyson, A, and Ranta, A. Switching to Tenecteplase for stroke thrombolysis real-world experience and outcomes in a regional stroke network. Stroke. (2021) 52:E590–3. doi: 10.1161/STROKEAHA.121.035931
29. Jillian, H, Jesse, MT, Mark, H, Lauren, T, Terri, Y, Taylor, S, et al. Tenecteplase improves door-to-needle time in real-world acute stroke treatment. Stroke Vasc Interv Neurol. (2021) 1:e000102. doi: 10.1161/SVIN.121.000102
30. Saver, JL, Fonarow, GC, Smith, EE, Reeves, MJ, Grau-Sepulveda, MV, Pan, W, et al. Time to treatment with intravenous tissue plasminogen activator and outcome from acute ischemic stroke. JAMA. (2013) 309:2480–8. doi: 10.1001/jama.2013.6959
31. Fonarow, GC, Smith, EE, Saver, JL, Reeves, MJ, Bhatt, DL, Grau-Sepulveda, MV, et al. Timeliness of tissue-type plasminogen activator therapy in acute ischemic stroke patient characteristics, hospital factors, and outcomes associated with door-to-needle times within 60 minutes. Circulation. (2011) 123:750–8. doi: 10.1161/CIRCULATIONAHA.110.974675
32. Goyal, M, Menon, BK, van Zwam, WH, Dippel, DWJ, Mitchell, PJ, Demchuk, AM, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. (2016) 387:1723–31. doi: 10.1016/S0140-6736(16)00163-X
33. Jahan, R, Saver, JL, Schwamm, LH, Fonarow, GC, Liang, L, Matsouaka, RA, et al. Association between time to treatment with endovascular reperfusion therapy and outcomes in patients with acute ischemic stroke treated in clinical practice. JAMA. (2019) 322:252–63. doi: 10.1001/jama.2019.8286
Keywords: acute ischemic stroke, tenecteplase, alteplase, early improvement, door-to-needle time
Citation: Yao Y, Wu Y, Zhang X, Liu C, Cai L, Ying Y and Yang J (2024) Real-world data of tenecteplase vs. alteplase in the treatment of acute ischemic stroke: a single-center analysis. Front. Neurol. 15:1386386. doi: 10.3389/fneur.2024.1386386
Edited by:
Matteo Foschi, Azienda Unità Sanitaria Locale (AUSL) della Romagna, ItalyReviewed by:
Maria Giulia Mosconi, University of Perugia, ItalyCopyright © 2024 Yao, Wu, Zhang, Liu, Cai, Ying and Yang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jianhong Yang, 13705743956@139.com
†These authors have contributed equally to this work and share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.