 Yao Jiang
Yao Jiang Yingqiang Dang
Yingqiang Dang Qian Wu1
Qian Wu1 Lina Gao
Lina Gao Chongge You
Chongge You- 1Laboratory Medicine Center, The Second Hospital and Clinical Medical School, Lanzhou University, Lanzhou, China
- 2Department of Neurology, The Second Hospital and Clinical Medical School, Lanzhou University, Lanzhou, China
Objective: Acute ischemic stroke (AIS) is a heterogeneous condition. To stratify the heterogeneity, identify novel phenotypes, and develop Clinlabomics models of phenotypes that can conduct more personalized treatments for AIS.
Methods: In a retrospective analysis, consecutive AIS and non-AIS inpatients were enrolled. An unsupervised k-means clustering algorithm was used to classify AIS patients into distinct novel phenotypes. Besides, the intergroup comparisons across the phenotypes were performed in clinical and laboratory data. Next, the least absolute shrinkage and selection operator (LASSO) algorithm was used to select essential variables. In addition, Clinlabomics predictive models of phenotypes were established by a support vector machines (SVM) classifier. We used the area under curve (AUC), accuracy, sensitivity, and specificity to evaluate the performance of the models.
Results: Of the three derived phenotypes in 909 AIS patients [median age 64 (IQR: 17) years, 69% male], in phenotype 1 (N = 401), patients were relatively young and obese and had significantly elevated levels of lipids. Phenotype 2 (N = 463) was associated with abnormal ion levels. Phenotype 3 (N = 45) was characterized by the highest level of inflammation, accompanied by mild multiple-organ dysfunction. The external validation cohort prospectively collected 507 AIS patients [median age 60 (IQR: 18) years, 70% male]. Phenotype characteristics were similar in the validation cohort. After LASSO analysis, Clinlabomics models of phenotype 1 and 2 were constructed by the SVM algorithm, yielding high AUC (0.977, 95% CI: 0.961–0.993 and 0.984, 95% CI: 0.971–0.997), accuracy (0.936, 95% CI: 0.922–0.956 and 0.952, 95% CI: 0.938–0.972), sensitivity (0.984, 95% CI: 0.968–0.998 and 0.958, 95% CI: 0.939–0.984), and specificity (0.892, 95% CI: 0.874–0.926 and 0.945, 95% CI: 0.923–0.969).
Conclusion: In this study, three novel phenotypes that reflected the abnormal variables of AIS patients were identified, and the Clinlabomics models of phenotypes were established, which are conducive to individualized treatments.
Introduction
Acute ischemic stroke (AIS) is a highly heterogeneous disease characterized by a high risk of morbidity, disability, recurrence, and mortality (1, 2). It has been reported that the number of IS-related deaths is expected to increase further from 3.29 million in 2019 to 4.90 million by 2030 (3). Administration of antiplatelet and statin drugs in AIS patients is recommended by the American Heart Association (AHA) to reduce the risk of stroke recurrence and cardiovascular events (4). However, despite patients following the therapies of the guidelines, there is a substantial risk of recurrent stroke in AIS patients (5). A major barrier to intervention is the high heterogeneity of AIS. Therefore, stratifying the heterogeneity of AIS using multiple features can identify undescribed phenotypes that may respond differently to medication, making it possible to offer more personalized treatment to AIS patients. Recently, Ding et al. (6, 7) used unsupervised clustering algorithms to identify novel phenotypes with distinct traits in non-cardioembolic ischemic stroke (NCIS). Similarly, Chen et al. (8) and Schütz et al. (9) used the latent class analysis method to reveal the potential phenotypes of ischemic stroke with obstructive sleep apnea (OSA). Likewise, Lattanzi et al. (10) adopted the hierarchical cluster analysis to distinguish clinical phenotypes of the embolic stroke of an undetermined source. These studies elucidate the new tendency to discover potential phenotypes by understanding the heterogeneity of diseases based on a clustering algorithm.
The k-means clustering, as an unsupervised learning algorithm, can classify unlabeled data by maximizing the heterogeneity within different phenotypes (11) and also can identify similarities of potential phenotypes in a dataset (12). A large body of research work has shown that the k-means clustering algorithm can be used to reveal novel phenotypes of stroke (13), sepsis (14, 15), early-onset Alzheimer's disease (16), postoperative delirium symptoms (17), and coronary heart disease (CHD) (18), which can help to understand the potential pathogenesis and treatment respondence of diseases. For instance, with the availability of laboratory data, Guo et al. (15) used k-means clustering to categorize sepsis phenotype, reflecting the severity of sepsis and treatment effects. Similarly, Sriprasert et al. (18) classified postmenopausal women into different phenotypes based on nine metabolic laboratory indicators, revealing the relationship of subtypes to subclinical atherosclerosis.
Although clinical laboratories produce large amounts of laboratory results each day to assist clinical diagnosis (19), these data are not fully utilized (20). Hence, Wen et al. proposed a concept of clinical laboratory omics (Clinlabomics) using machine learning (ML) or deep learning algorithms to establish models based on clinical and laboratory data that can reveal valuable information hidden in a great deal of data (20).
Therefore, the objectives of this study were to investigate novel phenotypes of AIS patients based on clinical and laboratory data using a k-means clustering algorithm and maximizing the heterogeneity, compare the differences among phenotypes based on demographic, clinical, individual traits, physiological indices, and laboratory data, develop Clinlabomics models of AIS phenotypes, and evaluate the diagnostic performance of models, which have not been done previously.
Methods
Study design and population
This study consecutively enrolled AIS inpatients attending Lanzhou University Second Hospital between Dec 2019 and Dec 2022. Furthermore, we also prospectively collected AIS patients from January 2023 to January 2024 as an external validation dataset. The inclusion criteria were as follows: (1) age ≥18 years old; (2) first-ever AIS at admission within 24 h. Patients were excluded for malignant tumors, mental conditions, autoimmune diseases, intracranial hemorrhage, infection within 2 weeks before the onset of stroke, recurrent stroke, transient ischemic attacks (TIA), treated with anticoagulation or reperfusion, or missing data >5%. AIS, as defined by the World Health Organization (WHO), is a clinical syndrome with rapidly developing neurological deficit due to cerebrovascular cause, persisting for more than 24 h or death (21). The AIS was confirmed by computed tomography (CT) scan or diffusion weight imaging (DWI) on admission. Further, we also included a control group with 484 inpatients without any type of current or prior cerebral infarction but possessing clinical manifestations similar to AIS patients. This study was approved by the Ethics Committee of the Lanzhou University Second Hospital (IRB number: 2022A-710). Informed consent was obtained from all participants.
Clinical and laboratory data collection
Medical records provided routinely available clinical data, including demographic data (age, gender, nationality, education, marriage), individual traits (height, weight, body mass index), vascular risk factors (the history of hypertension, diabetes, atrial fibrillation, coronary disease, and unhealthy habits including smoking and drinking), physiological indices (heart rate, oxygen saturation, blood pressure), the National Institutes of Health Stroke Scale (NIHSS) score that evaluates the stroke severity, Glasgow coma scale (GCS) that determines the degree of coma, modified Rankin scale (mRS) that assesses the degree of disability caused by stroke, Trial of Org 10172 in Acute Stroke Treatment (TOAST) classification that classifies etiological subtypes, and CT or DWI results that confirm the location and numbers of lesions. Based on the NIHSS score, scores of 1–4, 5–15, 16–20, and 21–42 were regarded as mild, moderate, moderate-to-severe, and severe stroke, respectively (22). An experienced senior neurologist (BY) examined and verified the NIHSS score, GCS, mRS, and TOAST classification in all included patients. There was a green channel for patients suspected of AIS, whose blood collection and detection were conducted immediately upon admission. In general, the results of complete blood count (CBC), biochemical tests, and coagulation examinations needed to be reported in 10, 30, and 30 min, respectively. Laboratory test results on admission were collected from the laboratory information system (LIS).
Variable selection
In total, we collected data on 97 variables, where 76 variables could be measured, detected, or calculated. The calculation formula of inflammatory biomarkers was as follows: neutrophil to lymphocyte ratio (NLR) = neutrophil (NEU)/lymphocyte (LYM); lymphocyte to monocyte ratio (LMR) = LYM/ monocyte (MON); monocyte to high-density lipoprotein-cholesterol ratio (MHR) = MON/ high-density lipoprotein-cholesterol (HDL-C) (23); neutrophil to high-density lipoprotein-cholesterol ratio (NHR) = NEU/HDL-C (23); systemic immune-inflammation index (SII) = platelet (PLT) × NLR (24); system inflammation response index (SIRI) = NUE × MON/LYM (24); multi-inflammatory index 1 (MII-1) = NLR × C-reaction protein (CRP) (25); multi-inflammatory index 2 (MII-2)=PLT/LYM × CRP (25); multi-inflammatory index 3 (MII-3) = (PLT × NLR) × CRP (25); red blood cell distribution width to platelet ratio (RPR) = red blood cell distribution width coefficient of variation (RDWCV)/PLT (26). Additionally, we used the ln [total triglyceride (TG) (mg/dL) × fasting blood glucose (FBG) (mg/dL)/2] formula to calculate the triglyceride-glucose (TyG) index (27). The corresponding lipid parameters of the atherogenic index of plasma (AIP), lipoprotein combine index (LCI), non-high-density lipoprotein-cholesterol (non-HDL-C), atherogenic coefficient (AC), Castelli's index-I (CRI-I), and Castelli's index-II (CRI-II) were calculated by lg (TG/HDL-C) (28), total cholesterol (TC) × TG × low-density lipoprotein-cholesterol (LDL-C)/HDL-C (29), TC–HDL-C (30), non-HDL-C/HDL-C (31), TC/HDL-C (31), and LDL-C/HDL-C (31), respectively. We classified the 76 variables into 11 domains according to their commonality, including non-invasive physiological indices, individual characteristics, inflammatory biomarkers, red blood cell-related parameters, lipid parameters, diabetes-related biomarkers, renal function indicators, ions, liver function-related indicators, myocardial injury markers, and coagulative markers. Categorical variables, such as gender and stroke severity, were excluded because of the requirements of clustering analysis.
Statistical analyses
A normal distribution of data was determined by the Kolmogorov-Smirnov test. The use of frequency counts and proportions (n%) expressed categorical variables that were compared using the Chi-square test and Fisher's exact test, if appropriate. Mean and standard deviation (SD), namely mean ± SD, was used to express normally distributed continuous variables, which were compared by a t-test. In contrast, non-normally distributed continuous variables were presented using median and interquartile range (IQR), namely M (Q1 - Q3), and compared by the Mann–Whitney U-test. The k-means clustering algorithm was used to identify novel phenotypes of AIS patients, where the optimal k was determined by the elbow method (32). The original data was transformed into standardized values (mean = 0, SD = 1) for clustering analysis. This clustering algorithm can partition observations into k clusters by assigning each observation to the nearest centroid (33). Once determined the phenotypes of AIS, we performed intergroup comparisons for the identification of significantly different variables. Further, a chord diagram was used to visualize abnormal variables classified by phenotype.
Before constructing models, we used the least absolute shrinkage and selection operator (LASSO) algorithm to perform variable selection for eliminating high multicollinearity variables (34). Subsequently, we used a random sampling method to divide patients in a 7:3 ratio into training and testing datasets. Next, a support vector machines (SVM) classifier was adopted to establish Clinlabomics predictive models, also regarded as phenotype classifiers, of AIS novel phenotypes. The SVM algorithm, which performs perfectly in dealing with both linear and non-linear data, can project training datasets into a multidimensional space, using a hyperplane to classify data (35), thus avoiding the overfitting problem (36). Receiver operating characteristic curves (ROC) were used to determine the optimal cut-off values of models, and the predictive performance of models was assessed by area under the receiver operating characteristic curve (AUC), accuracy, sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). All statistical analyses were performed on RStudio software (R version 4.3.0). A two-tailed p < 0.05 was regarded as statistical significance.
Results
Baseline characteristics of the study population
In total, we retrospectively included 909 AIS patients [median age: 64 (IQR: 17) years, 69% male] and 484 non-AIS subjects [median age: 66 (IQR: 15) years, 53% male]. In addition, we also prospectively collected 507 AIS patients [median age 60 (IQR: 18) years, 70% male] as validation dataset to verify the robustness of the k-means clustering algorithm. Figure 1 shows the detailed patient selection process and flow chart of this study. Table 1 summarizes the characteristics of the participants. There were no significant differences in age, nationality, marriage, history of atrial fibrillation (AF) and CHD, heart rate (HR), oxygen saturation in arterial blood (SaO2), body mass index (BMI), mean corpuscular hemoglobin (MCH), RDWCV, TC, LDL-C, non-HDL-C, urea, urea to creatinine ratio (UCR), calcium (Ca), total bilirubin (TBIL), indirect bilirubin (IBIL), aspartate aminotransferase (AST), albumin (ALB), creatine kinase (CK), international normalized ratio (INR), thrombin time (TT), and fibrin degradation products (FDP) between the two groups (all p > 0.05).
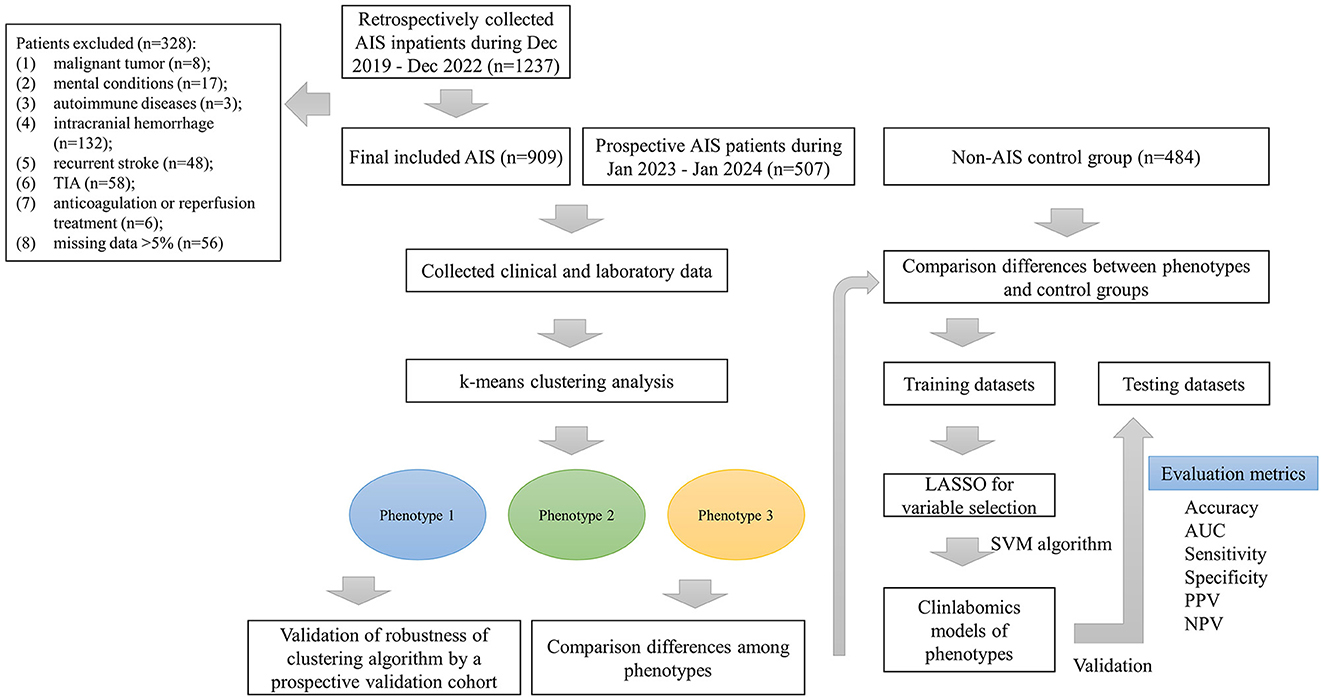
Figure 1. The patient selection process and flow chart. AIS, acute ischemic stroke; TIA, transient ischemic attack; LASSO, the least absolute shrinkage and selection operator; AUC, the area under curve; PPV, positive predictive value; NPV, negative predictive value.
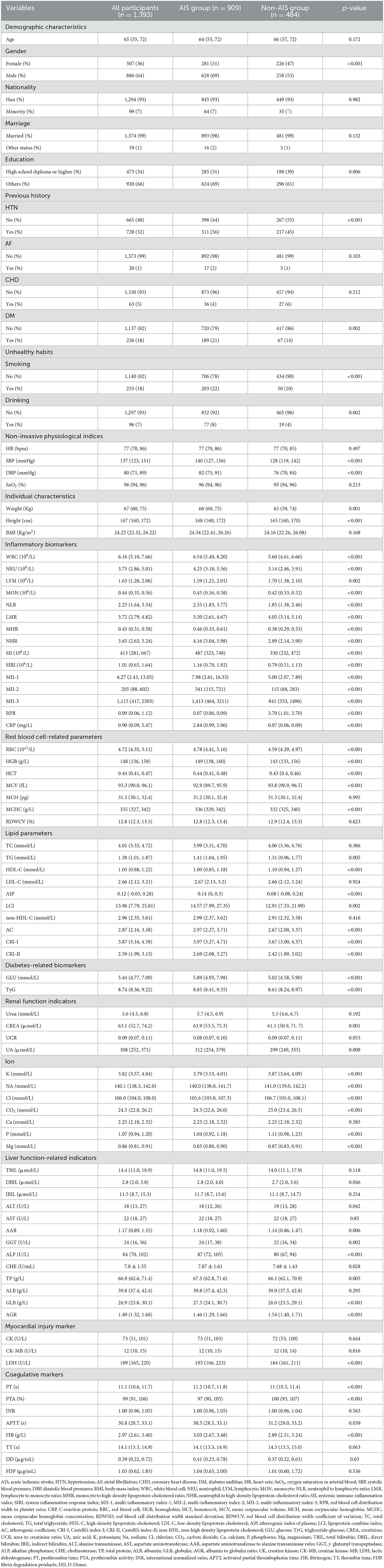
Table 1. Baseline characteristics of included participants in the retrospective cohort.
K-means clustering
We used the elbow method to determine the optimal k value of 3 (Figure 2A) and divided 909 AIS patients into three novel phenotypes (Figure 2B). Figure 3 describes the abnormal variables of three phenotypes. Patients in phenotype 1 (n = 401) were relatively young and obese and had significantly elevated levels of lipids. Phenotype 2 (n = 463) was associated with abnormal ion levels. Phenotype 3 (n = 45) was characterized by the highest level of inflammation, accompanied by mild multiple-organ dysfunction. Table 2 compares the statistical difference among phenotypes in demographic, clinical characteristics, and laboratory data.
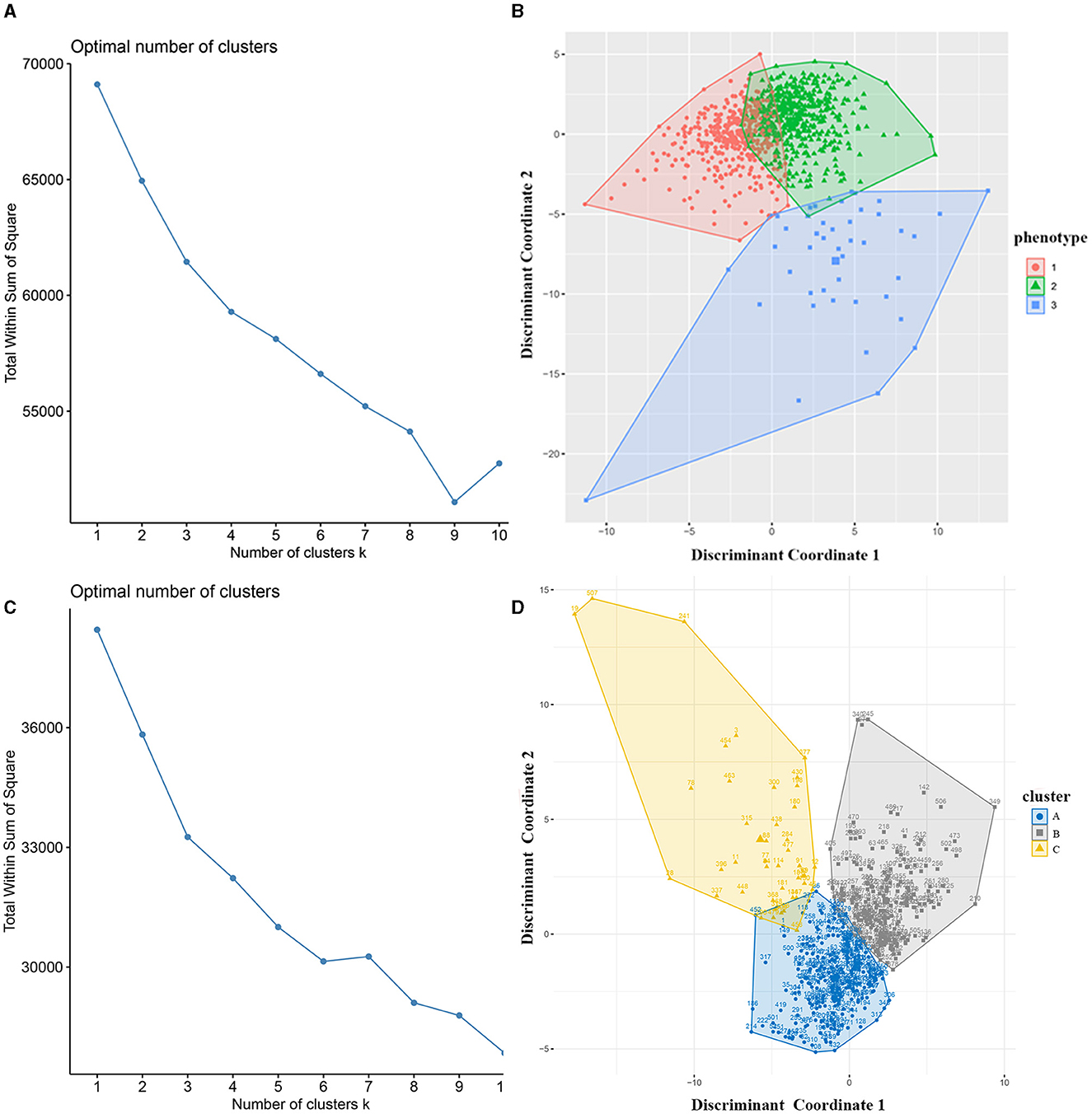
Figure 2. Identification of phenotypes of AIS patients using k-means clustering. (A) The optimal k value was determined using the elbow method; (B) Plotting of individual observations of each phenotype in discriminant component space; (C) The optimal k value in the validation cohort; (D) Individual observations of each cluster in discriminant component space in the validation dataset. AIS, acute ischemic stroke.
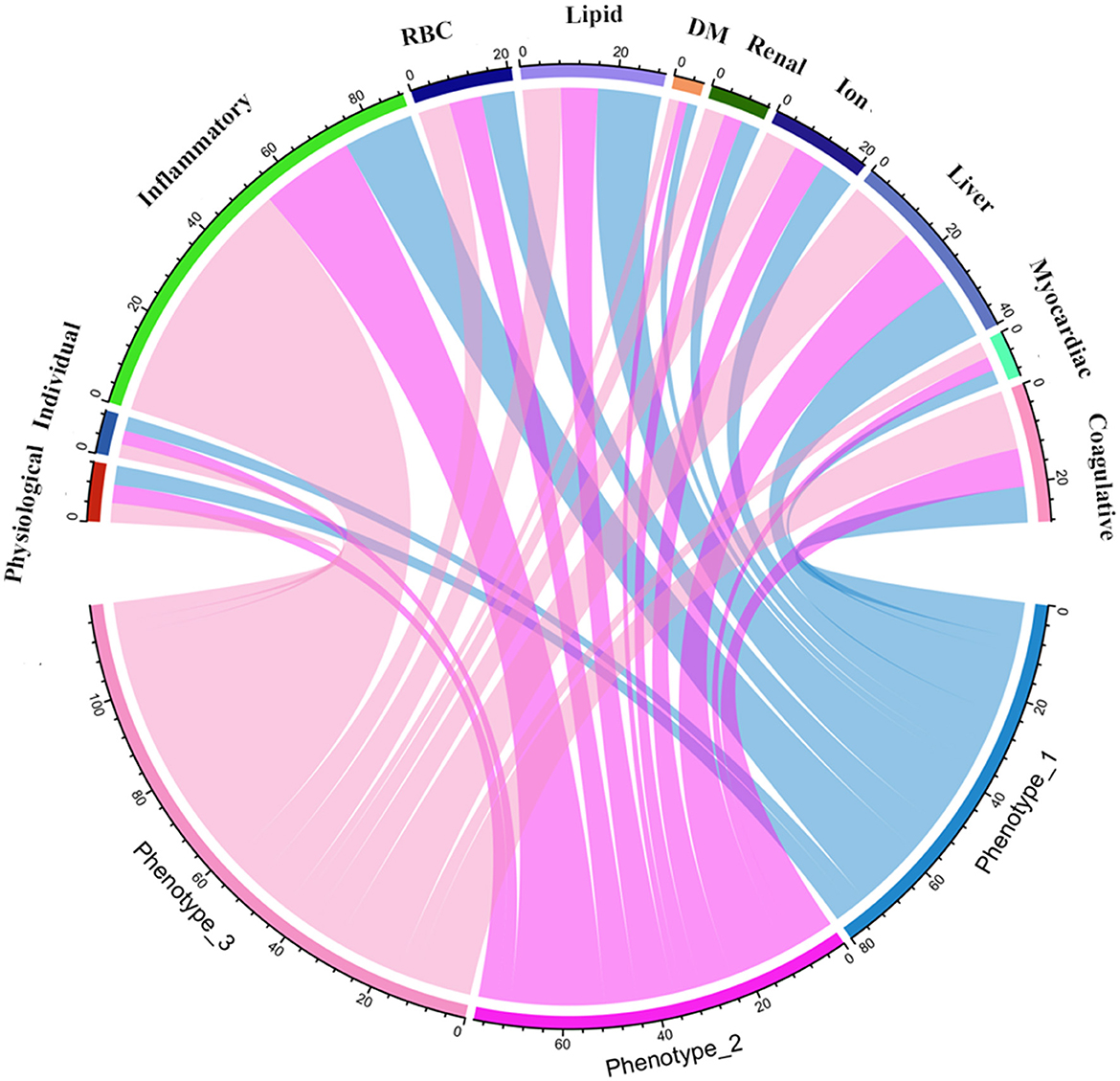
Figure 3. Chord diagrams show the relationships between phenotypes and 11 domains. RBC, red blood cell; DM, diabetes mellitus.

Table 2. Characteristics of three phenotypes based on the k-means clustering analysis.
In phenotype 1, the lipid parameters, including TC, TG, LDL-C, AIP, LCI, non-HDL-C, AC, CRI-I, and CRI-II, were significantly higher than the other two phenotypes (all p < 0.05). In phenotype 2, elevated levels of sodium (Na) and chloride (Cl) ions were found, compared to phenotype 1 and 3 (all p < 0.05). Nevertheless, patients in phenotype 3 had significant inflammation levels. They had abnormally increasing white blood cell (WBC), NEU, MON, NLR, MHR, NHR, SII, SIRI, MII-1, MII-2, MII-3, CRP, and lower levels of LYM and LMR inflammatory indicators, among the three phenotypes (all p < 0.05). Besides, phenotype 3 also had mild multiple-organ dysfunction, such as abnormal synthesis, secretion, coagulation, and excretion function occurring in the liver and renal, as well as myocardial injury. The basic characteristics of phenotypes and non-AIS control groups are displayed in Supplementary Table 1.
In the external validation dataset, 507 AIS patients were also divided into three clusters by the k-means cluster algorithm (Figures 2C, D), including clusters A (n = 251), B (n = 213), and C (n = 43). We compared the differences between the three groups in terms of clinical and laboratory data. Cluster A was characterized by abnormal ions, especially Na and Cl ions, corresponding to phenotype 2. Cluster B had high levels of lipid and BMI, which was equal to phenotype 1. Cluster C had mild organ dysfunction and severe levels of inflammation, with abnormal elevated and decreased inflammatory indicators, similar to phenotype 3. Supplementary Table 2 describes the detailed results.
Clinlabomics models of phenotypes
We used LASSO regression analysis to select 24 variables for the establishment of Clinlabomics model 1 of phenotype 1, including age, hypertension (HTN), smoking, systolic blood pressure (SBP), WBC, LYM, SII, MII-2, RPR, CRP, RBC, mean corpuscular volume (MCV), RDWCV, LDL-C, CRI-II, glucose (GLU), TyG, Cl, Ca, direct bilirubin (DBIL), alkaline phosphatase (ALP), cholinesterase (CHE), AGR, and PT (Figure 4A). For constructing predictive model 2 of phenotype 2 (Figure 4B), 23 variables, namely age, marriage, CHD, AF, drinking, HR, SBP, weight, LYM, NHR, SII, MII-2, RPR, CRP, TG, LCI, GLU, carbon dioxide (CO2), magnesium (Mg), ALB, AGR, INR, and TT were identified using a LASSO method. The predictive performance of the two phenotype classifiers established by the SVM algorithm was excellent, achieving high AUC values (ranging from 0.961 to 1.00), as shown in Figure 5 and Table 3. In particular, model 2 yielded higher accuracy (0.991 and 0.952), sensitivity (0.991 and 0.958), specificity (0.992 and 0.945), PPV (0.991 and 0.951), and NPV (0.992 and 0.952) both in training and testing datasets. Additionally, we selected a relatively important ranking of the top ten variables of models (Supplementary Figure 1). Notably, the inflammatory biomarkers CRP, RPR, and MII-2 were extremely important variables that ranked in the top three, both in model 1 and model 2. Furthermore, the calibration plots of the models showed a good agreement between the predicted probability and observed probability (Figure 6). Decision curve analysis (DCA) curves of two phenotype classifiers denoted optimal clinical efficacy (Figure 7).
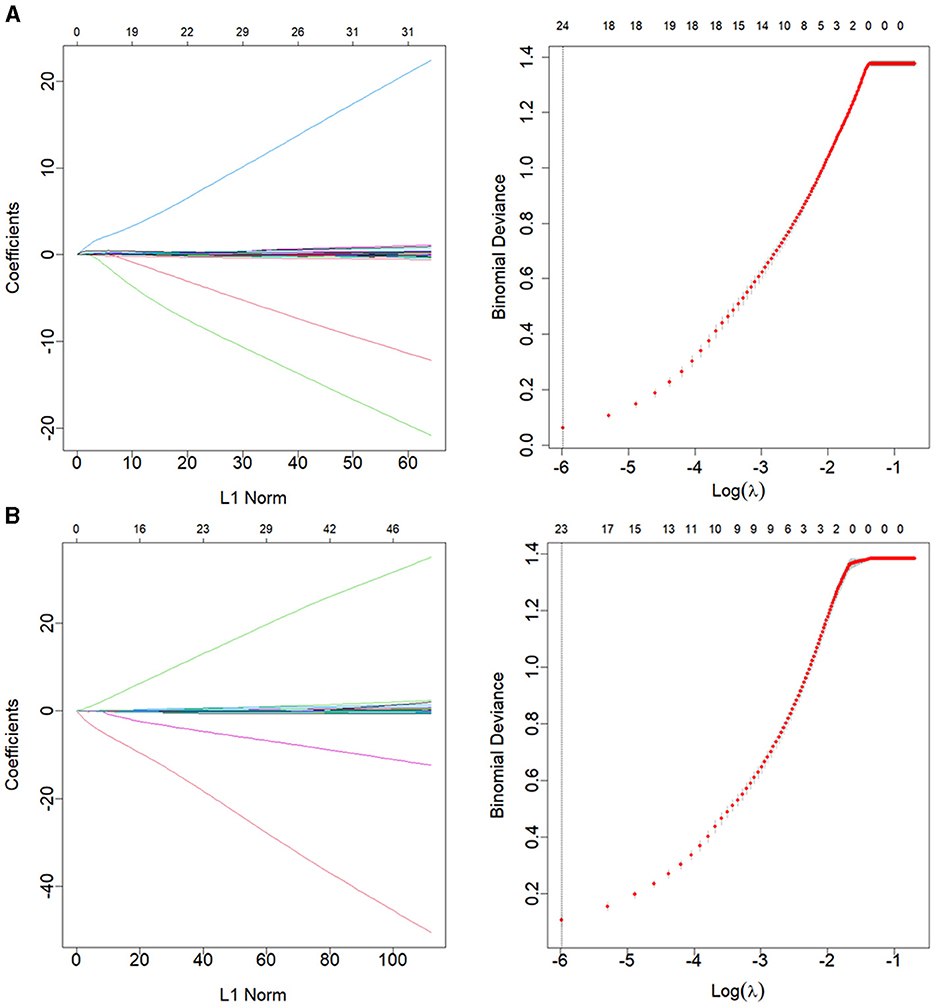
Figure 4. LASSO regression analysis for variable selection of (A) phenotype 1 and (B) phenotype 2. The LASSO coefficient profiles (left) and selection of the λ by 10-fold cross-validation in the LASSO analysis (right). LASSO, least absolute shrinkage, and selection operator.
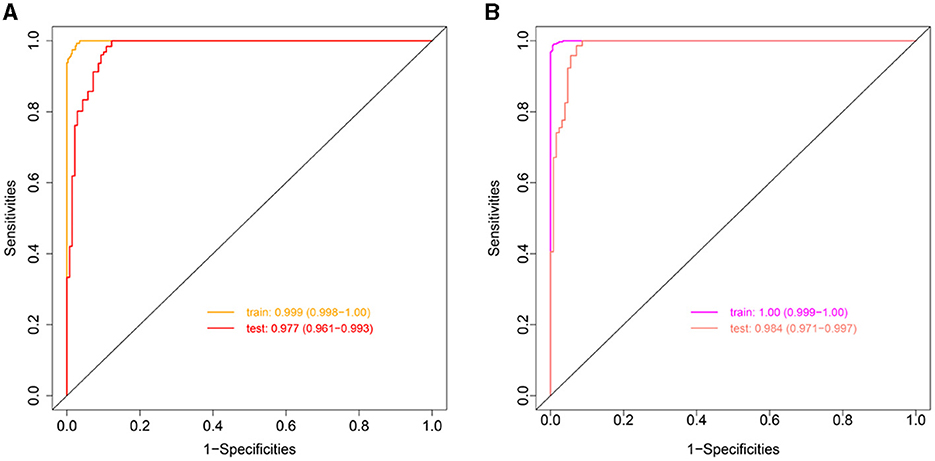
Figure 5. ROC curves of Clinlabomics (A) model 1 and (B) model 2. ROC, receiver-operating characteristic; AUC, the area under curve.
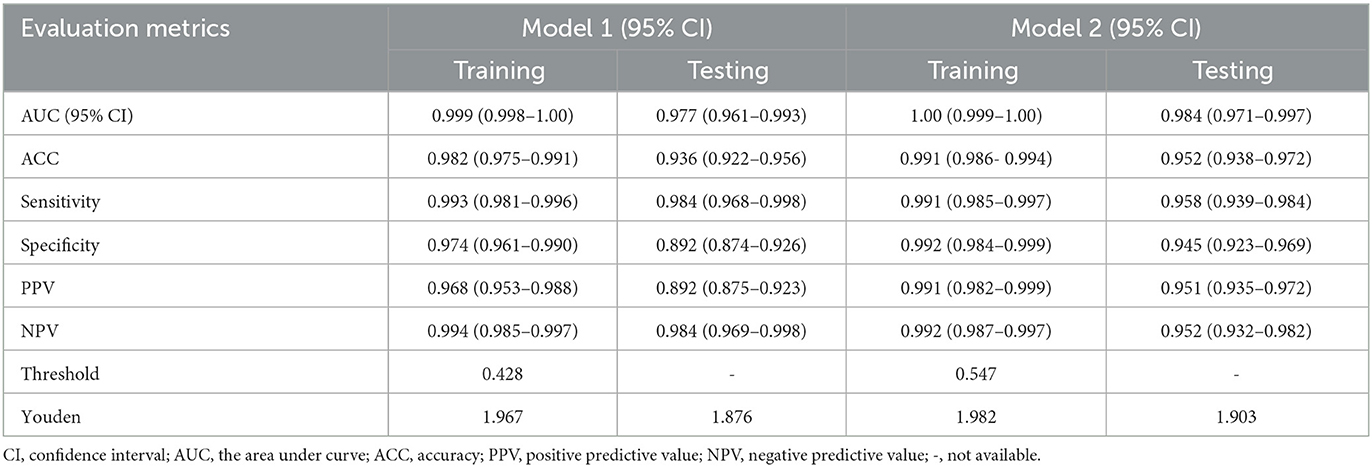
Table 3. Evaluation metrics assess the predictive performance of Clinlabomics models.
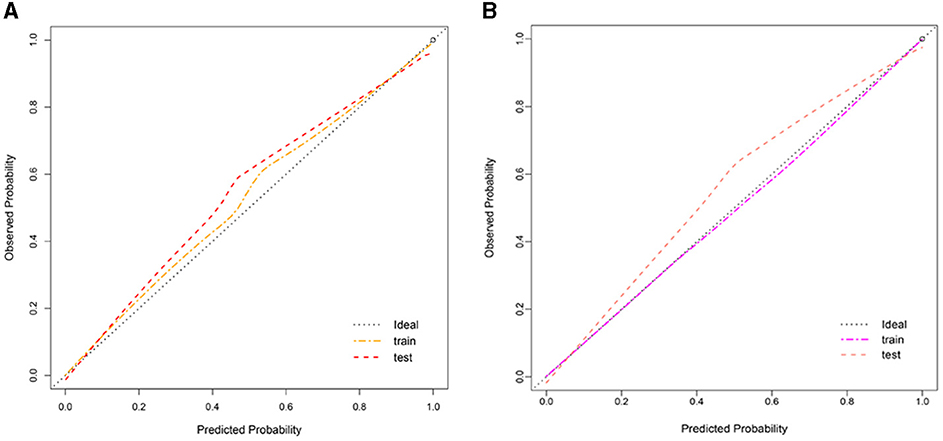
Figure 6. Calibration plot of Clinlabomics (A) model 1 and (B) model 2.
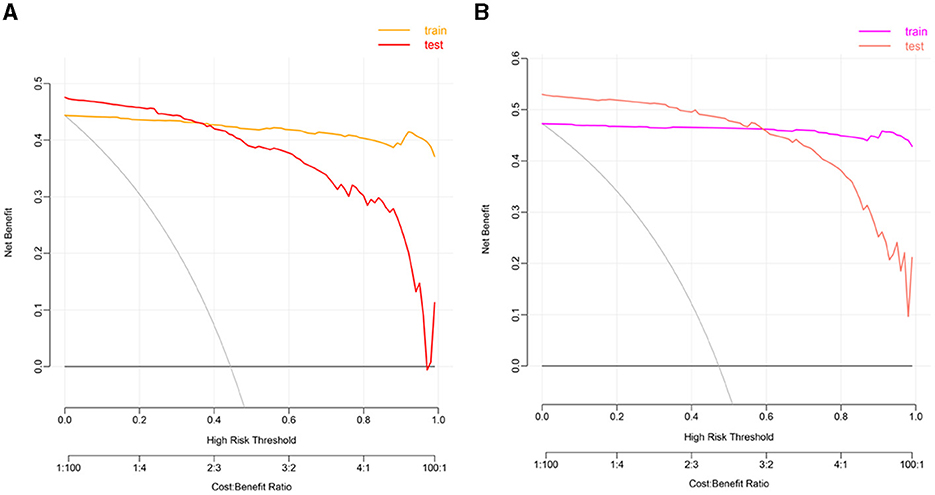
Figure 7. The DCA plots of Clinlabomics (A) model 1 and (B) model 2. DCA, decision curve analysis.
Discussion
In this retrospective analysis of data from AIS patients, we classified them into three novel phenotypes with distinct clinical characteristics and significantly different laboratory data. This stratification of AIS patients may provide evidence of potential pathophysiology mechanisms of diseases and can help clinicians make clinical decisions about the intervention of stroke.
Of the three novel phenotypes, phenotype 3, which had only ~5% of the overall population sample size, was closely related to the older adult population and had the highest level of inflammation and mild multiple-organ dysfunction, containing abnormal liver, kidney function, and coagulative status. While phenotype 2 was characterized by a mild increase in inflammatory markers, it had the lowest lipid levels. Interestingly, the serum ions, such as potassium (K), NA, Cl, CO2, and phosphorus (P), were observed to be increased in phenotype 2. In contrast, phenotype 1 had a relatively young but high BMI population, who had significantly elevated levels of lipids.
We also compared with other phenotypes of ischemic stroke (Table 4). For instance, Chen and Chen (8) and Lattanzi et al. (10) revealed a clinical phenotype with dyslipidemia in embolic stroke of undetermined source (ESUS) and ischemic stroke with OSA, respectively. Likewise, Ding et al. (6, 7) also identified the phenotypes of abnormal inflammation and lipid metabolism of NCIS patients, which demonstrated that inflammatory and lipid alterations were closely associated with the occurrence of ischemic stroke. In our study, we found a distinct phenotype with abnormal ions for the first time, which may provide new insight into targeted treatments of AIS patients.
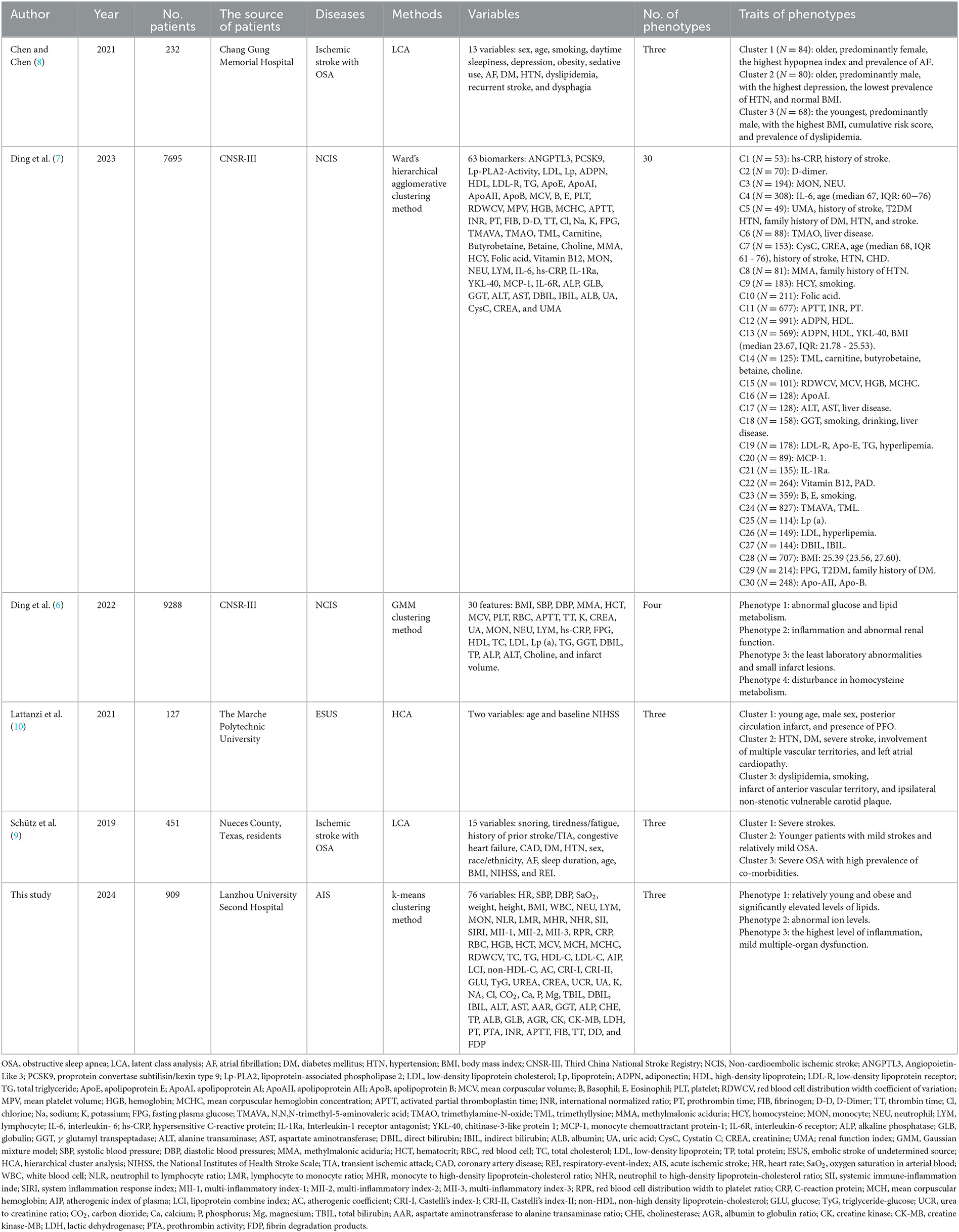
Table 4. Comparison with other phenotypes of ischemic stroke.
Recent works have shown that inflammation plays a vital role in the pathogenesis of AIS, which may increase the risk of stroke and exacerbate ischemic lesions (37–39). When ischemia occurs in the cerebrum, peripheral circulating leukocytes and their subsets, including neutrophils, monocytes, and lymphocytes, are recruited to the cerebral ischemic region. These cells produce, secrete, and activate inflammatory mediators, such as cytokines, chemokines, adhesion molecules, etc., and even interact with inflammatory cells to contribute to the progression and sustenance of inflammation (40, 41). Inflammatory responses participate in the process of thrombosis, which, in turn, can generate a thrombotic inflammatory response via the recruitment of leukocytes, leading to tissue organ damage and influencing the clinical outcome of AIS patients (42). One collaborative analysis of 31,245 patients who received statin therapy revealed that residual inflammatory risk (RIR), namely LDL-C <70 mg/dL and high-sensitivity C-reactive protein (hs-CRP) level ≥ 2 mg/L, can effectively predict cardiovascular events and death, and all-cause death (43). Similarly, RIR was strongly associated with the poor functional outcome of AIS patients and could predict the risk of recurrent stroke for AIS or TIA patients (44). Therefore, an anti-inflammatory strategy is recognized as a potential treatment to reduce the recurrence of stroke and other vascular events after the onset of IS (45, 46).
Furthermore, we found that the levels of traditional lipid parameters, including TC, TG, HDL-C, and LDL-C, and non-traditional lipid parameters, such as AIP, LCI, non-HDL-C, AC, CRI-I, and CRI-II, were significantly increased in the phenotype 1, which had 46% carotid plaque occurrence rate in all AIS population. Abnormal lipid metabolism and inflammatory responses are involved in the pathological progression of atherosclerosis, which is initiated by oxidation of LDL-C, activated by endothelium, and mediated by macrophages (47). Hyperlipidemia can recruit pro-inflammatory monocytes, which infiltrate into atherosclerotic lesions and ultimately form foam cells. They also can activate the innate immune response by triggering the production of many pro-inflammatory cytokines. Importantly, inflammation and hyperlipidemia had similar future atherothrombotic risks in the population without receiving statins (43). Thus, it is important to understand the vital roles of inflammation and lipids in the atherosclerosis process for better intervention of IS. Currently, statin therapy is recommended to reduce cardiovascular event risk among people with atherosclerosis in primary or secondary prevention, based on the randomized trials that demonstrated the efficacy of statin to decline the occurrence of cardiovascular events in patients with high levels of LDL-C (48) and hs-CRP (49). In addition, other lipid-lowering therapies, including ezetimibe, bempedoic acid, proprotein convertase subtilisin-kexin type 9 (PCSK9) inhibitors, angiopoietin-like 3 protein (ANGPTL3) inhibitors, and inclisiran were also observed to reduce cardiovascular event rates (50–52). A parallel-group trial elucidated that a target LD-L cholesterol <70 mg/dL in IS or TIA patients with atherosclerosis had lower cardiovascular risk (53).
Interestingly, both inflammation biomarkers and lipid levels were found to be the lowest in phenotype 2, but the levels of K, NA, Cl, and P ions were increased. After the onset of cerebral ischemia, endogenous Na+/K+-ATPase (NKA) inhibitors that damaged the innate NKA activity were released to the peripheral circulation (54), leading to ATP depletion, which in turn exacerbated anoxic damage (55, 56). Besides, abnormal metabolic changes occurred in extracellular and intracellular environments, namely, reductions in ATP and cytosolic K+, as well as increases in ROS produced by mitochondria and intracellular Ca2+. These changes activated the nucleotide-binding oligomerization domain (NOD)-like receptor (NLR) family pyrin domain-containing 3 (NLRP3) inflammasome and subsequent pro-caspase-1 self-cleaved into caspase-1, mediating pyroptosis and ultimately causing neuronal death (57). In addition, the decline of intracellular K+ could also stimulate the activation of NLRP3 inflammasome and trigger inflammation cascades (58). Therefore, restoring the activity of NKA may reduce inflammasome activation, relieve neuronal death, and attenuate ischemic injury (59), which may be a distinct therapeutic target for AIS.
In this study, a total of 24 and 23 variables were selected to construct Clinlabomics models of phenotype 1 and phenotype 2, respectively. The SVM generally presented a similar or superior ability to the logistic regression (LR) method in the classification of diseases (60). We tried to use the LR algorithm to construct the Clinlabomics models of phenotypes, but the results were disappointing with the fitted probabilities numerically 0 or 1. Thus, we established the phenotype classifiers using the SVM algorithm, which showed excellent predictive performance for phenotypes of AIS patients. Both in models 1 and 2, CRP, RPR, and MII-2 inflammatory biomarkers were the most important predictors. Kitagawa et al. (61) revealed that a low level of CRP (<1 mg/L) reduced 32% recurrent stroke and TIA compared to patients with CRP ≥ 1 mg/L. In addition, elevated CRP was observed to be strongly correlated to a 3-month worse outcome of stroke patients without infection (62). The RPR, as a new inflammatory index, was closely related to the risk of mortality among AIS patients (63, 64). Furthermore, an increase in RPR could also predict early neurological deterioration after intravenous thrombolysis in patients with AIS (65). It remains unclear whether any relationship exists between the MII-2 indicator and AIS patients, but a recent study elucidated that the MII-1 and MII-2 inflammatory markers were capable of predicting the occurrence of acute symptomatic seizures after IS (66). With advances in algorithms to develop prediction models by combining multiple variables, we can optimize models to identify the hidden complex relationships among variables, which may be of great utility in clinical practice.
However, we should consider limitations on the interpretation of our findings. First, this is a single-center, small sample-size study that needs further validation in a large-scale study. Second, we also need to investigate more advanced ML algorithms to better predict the phenotypes of AIS patients based on multicenter and large-scale research. Third, due to the small population (n = 45), we did not establish the predictive phenotype classifiers of phenotype 3, which is required to explore the underlying mechanism of mild organ damage and dysfunction in the future. Interestingly, although a large quantity of ML-based models exists to predict AIS, they are not effectively utilized in clinical practice, which is ascribed to the complicated data mining algorithms and abstruse formulas. Therefore, it is imperative to solve this problem to better apply these models by clinicians.
Conclusion
In conclusion, we identified three novel phenotypes that connected with different clinical variables using k-means clustering analysis. We constructed the Clinlabomics models of phenotypes in AIS patients that are conducive to clinical decision-making and personalized medicine.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by the Ethics Committee of the Lanzhou University Second Hospital (IRB number: 2022A-710). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
YJ: Data curation, Formal analysis, Methodology, Writing—original draft, Visualization, Writing—review & editing. YD: Formal analysis, Investigation, Methodology, Validation, Visualization, Writing—original draft. QW: Methodology, Validation, Visualization, Writing—review & editing. BY: Software, Supervision, Writing—review & editing. LG: Funding acquisition, Writing—review & editing. CY: Conceptualization, Writing—review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Cuiying Scientific and Technological Innovation Program of Lanzhou University Second Hospital (CY2020-BJ05).
Acknowledgments
The authors would like to thank the participants of the study.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1366307/full#supplementary-material
References
1. GBD 2016 Stroke Collaborators. Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. (2019) 18:439–58. doi: 10.1016/S1474-4422(19)30034-1
2. Wang YJ Li ZX, Gu HQ, Zhai Y, Jiang Y, Zhao XQ, et al. China Stroke Statistics 2019: A report from the national center for healthcare quality management in neurological diseases, china national clinical research center for neurological diseases, the Chinese stroke association, national center for chronic and non-communicable disease control and prevention, Chinese center for disease control and prevention and institute for global neuroscience and stroke collaborations. Stroke Vasc Neurol. (2020) 5:211–39. doi: 10.1136/svn-2020-000457
3. Fan J, Li X, Yu X, Liu Z, Jiang Y, Fang Y, et al. Global burden, risk factor analysis, and prediction study of ischemic stroke, 1990-2030. Neurology. (2023) 101:e137–e50. doi: 10.1212/WNL.0000000000207387
4. Powers WJ, Rabinstein AA, Ackerson T, Adeoye OM, Bambakidis NC, Becker K, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American heart association/American stroke association. Stroke. (2019) 50:e344–418. doi: 10.1161/STR.0000000000000211
5. Wang Y. Residual recurrence risk of ischaemic cerebrovascular events: concept, classification and implications. Stroke Vasc Neurol. (2021) 6:155–7. doi: 10.1136/svn-2021-000885
6. Ding L, Mane R, Wu Z, Jiang Y, Meng X, Jing J, et al. Data-driven clustering approach to identify novel phenotypes using multiple biomarkers in acute ischaemic stroke: a retrospective, multicentre cohort study. EClinicalMedicine. (2022) 53:101639. doi: 10.1016/j.eclinm.2022.101639
7. Ding L, Liu Y, Meng X, Jiang Y, Lin J, Cheng S, et al. Biomarker and genomic analyses reveal molecular signatures of non-cardioembolic ischemic stroke. Sig Trans Targ Ther. (2023) 8:222. doi: 10.1038/s41392-023-01465-w
8. Chen CY, Chen CL. Recognizable clinical subtypes of obstructive sleep apnea after ischemic stroke: a cluster analysis. Nat Sci Sleep. (2021) 13:283–90. doi: 10.2147/NSS.S301668
9. Schütz SG, Lisabeth LD, Shafie-Khorassani F, Case E, Sanchez BN, Chervin RD, et al. Clinical phenotypes of obstructive sleep apnea after ischemic stroke: a cluster analysis. Sleep Med. (2019) 60:178–81. doi: 10.1016/j.sleep.2019.04.004
10. Lattanzi S, Rinaldi C, Pulcini A, Corradetti T, Angelocola S, Zedde ML, et al. Clinical phenotypes of embolic strokes of undetermined source. Neurol Sci. (2021) 42:297–300. doi: 10.1007/s10072-020-04700-2
11. Hennig C, Meila M, Murtagh F, Rocci RE. Handbook of Cluster Analysis, 1st Edn. New York, NY: Chapman and Hall/CRC (2015).
12. Ren Z, Fu X. Stroke risk factors in United States: an analysis of the 2013-2018 national health and nutrition examination survey. Int J Gen Med. (2021) 14:6135–47. doi: 10.2147/IJGM.S327075
13. Miller JB, Nowak RM, Reed BP, DiSomma S, Nanayakkara P, Moyer M, et al. Hemodynamic characteristics of suspected stroke in the emergency department. Am J Emerg Med. (2017) 35:1915–8. doi: 10.1016/j.ajem.2017.08.017
14. Seymour CW, Kennedy JN, Wang S, Chang CH, Elliott CF, Xu Z, et al. Derivation, validation, and potential treatment implications of novel clinical phenotypes for sepsis. JAMA. (2019) 321:2003–17. doi: 10.1001/jama.2019.5791
15. Guo F, Zhu X, Wu Z, Zhu L, Wu J, Zhang F. Clinical applications of machine learning in the survival prediction and classification of sepsis: coagulation and heparin usage matter. J Transl Med. (2022) 20:265. doi: 10.1186/s12967-022-03469-6
16. Pollet M, Skrobala E, Lopes R, Kuchcinski G, Bordier C, Rollin-Sillaire A, et al. A multimodal, longitudinal study of cognitive heterogeneity in early-onset Alzheimer's disease. Eur J Neurol. (2021) 28:3990–8. doi: 10.1111/ene.15097
17. Sri-Iesaranusorn P, Sadahiro R, Murakami S, Wada S, Shimizu K, Yoshida T, et al. Data-driven categorization of postoperative delirium symptoms using unsupervised machine learning. Front Psychiatry. (2023) 14:1205605. doi: 10.3389/fpsyt.2023.1205605
18. Sriprasert I, Mack WJ, Hodis HN, Allayee H, Brinton RD, Karim R. Effect of ApoE4 genotype on the association between metabolic phenotype and subclinical atherosclerosis in postmenopausal women. Am J Cardiol. (2019) 124:1031–7. doi: 10.1016/j.amjcard.2019.06.022
19. Bayot ML, Lopes JE, Zubair M, Naidoo P. Clinical Laboratory [Updated 2022 Dec 19]. Treasure Island: StatPearls Publishing (2023).
20. Wen X, Leng P, Wang J, Yang G, Zu R, Jia X, et al. Clinlabomics: leveraging clinical laboratory data by data mining strategies. BMC Bioinformatics. (2022) 23:387. doi: 10.1186/s12859-022-04926-1
21. Aho K, Harmsen P, Hatano S, Marquardsen J, Smirnov VE, Strasser T. Cerebrovascular disease in the community: results of a WHO collaborative study. Bullet WHO. (1980) 58:113–30.
22. Islam MS, Hussain I, Rahman MM, Park SJ, Hossain MA. Explainable artificial intelligence model for stroke prediction using EEG signal. Sensors. (2022) 22:589. doi: 10.3390/s22249859
23. Gkantzios A, Tsiptsios D, Karapepera V, Karatzetzou S, Kiamelidis S, Vlotinou P, et al. Monocyte to HDL and neutrophil to HDL ratios as potential ischemic stroke prognostic biomarkers. Neurol Int. (2023) 15:301–17. doi: 10.3390/neurolint15010019
24. Huang L. Increased systemic immune-inflammation index predicts disease severity and functional outcome in acute ischemic stroke patients. Neurologist. (2023) 28:32–8. doi: 10.1097/NRL.0000000000000464
25. Demirel ME, Akunal Türel C. The role of the multi-inflammatory index as a novel predictor of hospital mortality in acute ischemic stroke. Cureus. (2023) 15:e43258. doi: 10.7759/cureus.43258
26. Chen B, Ye B, Zhang J, Ying L, Chen Y. RDW to platelet ratio: a novel noninvasive index for predicting hepatic fibrosis and cirrhosis in chronic hepatitis B. PLoS One. (2013) 8:e68780. doi: 10.1371/journal.pone.0068780
27. Wang X, Feng B, Huang Z, Cai Z, Yu X, Chen Z, et al. Relationship of cumulative exposure to the triglyceride-glucose index with ischemic stroke: a 9-year prospective study in the Kailuan cohort. Cardiovasc Diabetol. (2022) 21:66. doi: 10.1186/s12933-022-01510-y
28. Dobiásová M, Frohlich J. The plasma parameter log (TG/HDL-C) as an atherogenic index: correlation with lipoprotein particle size and esterification rate in apoB-lipoprotein-depleted plasma (FER(HDL)). Clin Biochem. (2001) 34:583–8. doi: 10.1016/S0009-9120(01)00263-6
29. Si Y, Liu J, Han C, Wang R, Liu T, Sun L. The correlation of retinol-binding protein-4 and lipoprotein combine index with the prevalence and diagnosis of acute coronary syndrome. Heart Vessels. (2020) 35:1494–501. doi: 10.1007/s00380-020-01627-8
30. Wu J, Chen S, Liu L, Gao X, Zhou Y, Wang C, et al. Non-high-density lipoprotein cholesterol vs low-density lipoprotein cholesterol as a risk factor for ischemic stroke: a result from the Kailuan study. Neurol Res. (2013) 35:505–11. doi: 10.1179/1743132813Y.0000000206
31. Guo J, Wang A, Wang Y, Liu X, Zhang X, Wu S, et al. Non-traditional lipid parameters as potential predictors of asymptomatic intracranial arterial stenosis. Front Neurol. (2021) 12:679415. doi: 10.3389/fneur.2021.679415
32. Lugner M, Gudbjörnsdottir S, Sattar N, Svensson AM, Miftaraj M, Eeg-Olofsson K, et al. Comparison between data-driven clusters and models based on clinical features to predict outcomes in type 2 diabetes: nationwide observational study. Diabetologia. (2021) 64:1973–81. doi: 10.1007/s00125-021-05485-5
33. MacQueen J. Some methods for classification and analysis of multivariate observations. In: Proceedings of the Sixth Berkeley Symposium on Mathematical Statistics and Probability (1967).
34. Dai P, Chang W, Xin Z, Cheng H, Ouyang W, Luo A. Retrospective study on the influencing factors and prediction of hospitalization expenses for chronic renal failure in China based on random forest and LASSO regression. Front Publ Health. (2021) 9:678276. doi: 10.3389/fpubh.2021.678276
35. Vapnik V. The Support Vector Method of Function Estimation. In:Suykens JAK, Vandewalle J, editors. Nonlinear Modeling: Advanced Black-Box Techniques. Boston, MA: Springer US (1998). p. 55–85.
36. Raghavendra NS, Deka PC. Support vector machine applications in the field of hydrology: a review. Applied Soft Comp. (2014) 19:372–86. doi: 10.1016/j.asoc.2014.02.002
37. Tirandi A, Sgura C, Carbone F, Montecucco F, Liberale L. Inflammatory biomarkers of ischemic stroke. Intern Emerg Med. (2023) 18:723–32. doi: 10.1007/s11739-023-03201-2
38. Bitencourt ACS, Timóteo RP, Bazan R, Silva MV, da Silveira Filho LG, Ratkevicius CMA, et al. Association of proinflammatory cytokine levels with stroke severity, infarct size, and muscle strength in the acute phase of stroke. J Stroke Cerebrovasc Dis. (2022) 31:106187. doi: 10.1016/j.jstrokecerebrovasdis.2021.106187
39. Ray MJ, Walters DL, Bett JN, Cameron J, Wood P, Aroney CN. Platelet-monocyte aggregates predict troponin rise after percutaneous coronary intervention and are inhibited by Abciximab. Int J Cardiol. (2005) 101:249–55. doi: 10.1016/j.ijcard.2004.03.033
40. Han L, Wang Z, Yuan J, He J, Deng Y, Zhu DS, et al. Circulating Leukocyte as an Inflammatory Biomarker: Association with Fibrinogen and Neuronal Damage in Acute Ischemic Stroke. J Inflamm Res. (2023) 16:1213–26. doi: 10.2147/JIR.S399021
41. Nakamura A, Otani K, Shichita T. Lipid mediators and sterile inflammation in ischemic stroke. Int Immunol. (2020) 32:719–25. doi: 10.1093/intimm/dxaa027
42. Wang MQ, Sun YY, Wang Y, Yan XL, Jin H, Sun X, et al. Platelet-to-neutrophil ratio after intravenous thrombolysis predicts unfavorable outcomes in acute ischemic stroke. Curr Neurovasc Res. (2020) 17:411–9. doi: 10.2174/1567202617666200517111802
43. Ridker PM, Bhatt DL, Pradhan AD, Glynn RJ, MacFadyen JG, Nissen SE. Inflammation and cholesterol as predictors of cardiovascular events among patients receiving statin therapy: a collaborative analysis of three randomised trials. Lancet. (2023) 401:1293–301. doi: 10.1016/S0140-6736(23)00215-5
44. Li J, Pan Y, Xu J, Li S, Wang M, Quan K, et al. Residual inflammatory risk predicts poor prognosis in acute ischemic stroke or transient ischemic attack patients. Stroke. (2021) 52:2827–36. doi: 10.1161/STROKEAHA.120.033152
45. Kelly PJ, Murphy S, Coveney S, Purroy F, Lemmens R, Tsivgoulis G, et al. Anti-inflammatory approaches to ischaemic stroke prevention. J Neurol Neurosurg Psychiatry. (2018) 89:211–8. doi: 10.1136/jnnp-2016-314817
46. Coveney S, McCabe JJ, Murphy S, O'Donnell M, Kelly PJ. Anti-inflammatory therapy for preventing stroke and other vascular events after ischaemic stroke or transient ischaemic attack. Cochrane Database Syst Rev. (2020) 5:CD012825. doi: 10.1002/14651858.CD012825.pub2
47. Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. (2005) 352:1685–95. doi: 10.1056/NEJMra043430
48. Fulcher J, O'Connell R, Voysey M, Emberson J, Blackwell L, Mihaylova B, et al. Efficacy and safety of LDL-lowering therapy among men and women: meta-analysis of individual data from 174,000 participants in 27 randomised trials. Lancet. (2015) 385:1397–405. doi: 10.1016/S0140-6736(14)61368-4
49. Ridker PM, Danielson E, Fonseca FA, Genest J, Gotto AM, Kastelein JJ, et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med. (2008) 359:2195–207. doi: 10.1056/NEJMoa0807646
50. Nurmohamed NS, Navar AM, Kastelein JJP. New and emerging therapies for reduction of LDL-cholesterol and apolipoprotein B: JACC focus seminar 1/4. J Am Coll Cardiol. (2021) 77:1564–75. doi: 10.1016/j.jacc.2020.11.079
51. Tokgözoglu L, Libby P. The dawn of a new era of targeted lipid-lowering therapies. Eur Heart J. (2022) 43:3198–208. doi: 10.1093/eurheartj/ehab841
52. Byrne P, Demasi M, Jones M, Smith SM, O'Brien KK, DuBroff R. Evaluating the association between low-density lipoprotein cholesterol reduction and relative and absolute effects of statin treatment: a systematic review and meta-analysis. JAMA Intern Med. (2022) 182:474–81. doi: 10.1001/jamainternmed.2022.0134
53. Amarenco P, Kim JS, Labreuche J, Charles H, Abtan J, Béjot Y, et al. A comparison of two LDL cholesterol targets after ischemic stroke. N Engl J Med. (2020) 382:9. doi: 10.1056/NEJMoa1910355
54. De Angelis C, Haupert GT. Hypoxia triggers release of an endogenous inhibitor of Na(+)-K(+)-ATPase from midbrain and adrenal. Am J Physiol. (1998) 274:F182–8. doi: 10.1152/ajprenal.1998.274.1.F182
55. Magnani ND Dada LA, Queisser MA, Brazee PL, Welch LC, Anekalla KR, et al. HIF and HOIL-1L-mediated PKCζ degradation stabilizes plasma membrane Na,K-ATPase to protect against hypoxia-induced lung injury. Proc Natl Acad Sci U S A. (2017) 114:E10178–e86. doi: 10.1073/pnas.1713563114
56. Comellas AP Dada LA, Lecuona E, Pesce LM, Chandel NS, Quesada N, et al. Hypoxia-mediated degradation of Na,K-ATPase via mitochondrial reactive oxygen species and the ubiquitin-conjugating system. Circ Res. (2006) 98:1314–22. doi: 10.1161/01.RES.0000222418.99976.1d
57. Xu Q, Zhao B, Ye Y, Li Y, Zhang Y, Xiong X, et al. Relevant mediators involved in and therapies targeting the inflammatory response induced by activation of the NLRP3 inflammasome in ischemic stroke. J Neuroinflammation. (2021) 18:123. doi: 10.1186/s12974-021-02137-8
58. Zhu M, Sun H, Cao L, Wu Z, Leng B, Bian J. Role of Na(+)/K(+)-ATPase in ischemic stroke: in-depth perspectives from physiology to pharmacology. J Mol Med. (2022) 100:395–410. doi: 10.1007/s00109-021-02143-6
59. Shi M, Cao L, Cao X, Zhu M, Zhang X, Wu Z, et al. DR-region of Na(+)/K(+) ATPase is a target to treat excitotoxicity and stroke. Cell Death Dis. (2018) 10:6. doi: 10.1038/s41419-018-1230-5
60. Lin Y, Lee Y, Wahba G. Support vector machines for classification in nonstandard situations. Mach Learn. (2002) 46:191–202. doi: 10.1023/A:1012406528296
61. Kitagawa K, Hosomi N, Nagai Y, Kagimura T, Ohtsuki T, Maruyama H, et al. Cumulative effects of LDL cholesterol and CRP levels on recurrent stroke and TIA. J Atheroscler Thromb. (2019) 26:432–41. doi: 10.5551/jat.45989
62. Wang L, Li Y, Wang C, Guo W, Liu M. C-reactive protein, infection, and outcome after acute ischemic stroke: a registry and systematic review. Curr Neurovasc Res. (2019) 16:405–15. doi: 10.2174/1567202616666191026122011
63. Xu N, Peng C. Association between red cell distribution width-to-platelet ratio and short-term and long-term mortality risk in patients with acute ischemic stroke. BMC Neurol. (2023) 23:191. doi: 10.1186/s12883-023-03219-1
64. He K, Xie X, Duan X, Zhou Q, Wu J. Red cell distribution width-to-platelet count ratio: a promising predictor of in-hospital all-cause mortality in critically ill patients with acute ischemic stroke. Cerebrovas Dis. (2023) 2:1–8. doi: 10.1159/000529184
65. Jiang M, Shen J, Muhammad B, Geng D. Red blood cell distribution width to platelet ratio predicts early neurological deterioration in acute ischemic stroke patients receiving intravenous thrombolysis. J Stroke Cerebrovasc Dis. (2023) 32:107146. doi: 10.1016/j.jstrokecerebrovasdis.2023.107146
Keywords: acute ischemic stroke, novel phenotypes, machine learning, clustering algorithms, Clinlabomics models
Citation: Jiang Y, Dang Y, Wu Q, Yuan B, Gao L and You C (2024) Using a k-means clustering to identify novel phenotypes of acute ischemic stroke and development of its Clinlabomics models. Front. Neurol. 15:1366307. doi: 10.3389/fneur.2024.1366307
Received: 06 January 2024; Accepted: 11 March 2024;
Published: 27 March 2024.
Edited by:
Raffaele Ornello, University of L'Aquila, ItalyReviewed by:
Murat Kirisci, Istanbul University-Cerrahpasa, TürkiyeYuanfang Ren, University of Florida, United States
Copyright © 2024 Jiang, Dang, Wu, Yuan, Gao and You. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Chongge You, eW91Y2hnQGx6dS5lZHUuY24=
†These authors have contributed equally to this work