 Kathrine Jáuregui-Renaud1*
Kathrine Jáuregui-Renaud1* Dulce Maria García-Jacuinde2
Dulce Maria García-Jacuinde2 Simón Pedro Bárcenas-Olvera2Michael A. Gresty3Aralia Gutiérrez-Márquez2
Simón Pedro Bárcenas-Olvera2Michael A. Gresty3Aralia Gutiérrez-Márquez2- 1Unidad de Investigación Médica en Otoneurología, Instituto Mexicano del Seguro Social, Mexico City, Mexico
- 2Departamento de Audiología y Otoneurología, Hospital General del Centro Médico Nacional “La Raza”, Instituto Mexicano del Seguro Social, Mexico City, Mexico
- 3Division of Brain Sciences, Imperial College London, Charing Cross Hospital, London, United Kingdom
In subjects with peripheral vestibular disease and controls, we assessed: 1. The relationship between spatial anxiety and perceived stress, and 2. The combined contribution of spatial anxiety, spatial perspective-taking, and individual cofactors to dizziness-related handicap. 309 adults participated in the study (153 with and 156 without peripheral vestibular disease), including patients with bilateral vestibular deficiency, unilateral deficiency (evolution <3 or ≥3 months), Meniere’s disease, and Benign Paroxysmal Positional Vertigo. Assessments included: general health, personal habits, spatial anxiety (3-domains), perceived stress, spatial perspective-taking, dizziness-related handicap (3-domains), unsteadiness, sleep quality, motion sickness susceptibility, trait anxiety/depression, state anxiety, depersonalization/derealization. After bivariate analyses, analysis of covariance was performed (p ≤ 0.05). Spatial anxiety was related to unsteadiness and perceived stress, with an inverse relationship with trait anxiety (ANCoVA, adjusted R2 = 0.27–0.30, F = 17.945–20.086, p < 0.00001). Variability on perspective-taking was related to vestibular disease, trait and state anxiety, motion sickness susceptibility, and age (ANCoVA, adjusted R2 = 0.18, F = 5.834, p < 0.00001). All domains of spatial anxiety contributed to the Physical domain of dizziness-related handicap, while the Navigation domain contributed to the Functional domain of handicap. Handicap variability was also related to unsteadiness, spatial perspective-taking, quality of sleep, and trait anxiety/depression (ANCoVA, adjusted R2 = 0.66, F = 39.07, p < 0.00001). Spatial anxiety is related to perceived stress in adults both with and without vestibular disease, subjects with trait anxiety rated lower on spatial anxiety. State anxiety and acute stress could be helpful for recovery after peripheral vestibular lesion. Spatial anxiety and perspective-taking contribute to the Physical and Functional domains of dizziness-related handicap, possibly because it discourages behavior beneficial to adaptation.
1 Introduction
Spatial reasoning is an essential function for activities of daily life, which requires a variety of innate aptitudes, supplemented by learned (malleable) skills (1, 2). Spatial abilities include visualizing, mentally rotating, and transforming spatial information (3). Among these, the ability to imagine viewing a scene from another perspective (perspective-taking) can be impaired by aberrant vestibular stimulation (4); while uncompromised vestibular resources are needed for self-rotation estimates (5), mental body transformation (6), spatial awareness for location, directional heading, and movement through the environment (7). Consistently, vestibular dysfunction is related to impairments in spatial memory (8), visuospatial working memory (9), path integration (10), updating orientation (11), and spatial navigation (12). However, spatial abilities may vary according to multiple factors (13), including anxiety (14). Anxiety may also be provoked by vestibular dysfunction (15–18), as well as motion sickness susceptibility (19), and discordant visuo-vestibular interactions and postural instability may elicit fears associated to specific environments (20).
Anxiety implies responses to increase arousal modulate attentional processes and behavioral inhibition (21). It is related to a variety of factors, such as age (22), sex (23), and quality of sleep (24). Trait anxiety is a predisposition to express constant anxiety (25) and promotes the processing of environmental information preparing the organism for response (26). State anxiety refers to hypervigilance in anticipation of a threat; it can be triggered by acute stress and has a function on overcoming environmental challenges and facilitating memory consolidation (27). In potentially dangerous situations, trait anxiety increases the probability of state anxiety (25).
Spatial anxiety is the domain-specific anxiety that is related to spatial reasoning (28). It denotes the fear and apprehension felt when conducting spatial tasks (29), with negative effects on performance (29, 30). Although, spatial anxiety is related to both experience and performance (31), individual differences are partially explained by genetic and environmental factors, including education (32). In patients with bilateral vestibular hypofunction, spatial anxiety is related to impaired spatial memory and navigation performance (12).
Both vestibular dysfunction and anxiety are related to stress (33, 34). The hypothalamus-pituitary–adrenal axis, the cortico-limbic and the sympathetic systems interact with each other to coordinate the stress response (35). In animal models, unilateral vestibular deafferentation activates the stress axis (36), whereas cortisol administration may improve vestibular compensation (37, 38). In healthy human beings, vestibular caloric stimulation increases cortisol levels (39). Nonetheless, to adapt to challenging situations, stress responses include emotional arousal and altered perceptions (40, 41). Acute stress is a trigger of state anxiety, improving the chance to overcome challenges, facilitating memory of relevant information (27), and inducing focused attention (42). Contrariwise, dysregulation of the stress axis can underlie distorted perceptions, including primary dissociative conditions (43); while symptomatic vestibular disease may provoke dissociative misperceptions (44, 45).
Physiological impairment, anxiety, spatial anxiety, stress could all contribute to dizziness-related handicap. However, studies on their combined contribution to the handicap reported by patients with peripheral vestibular disease are scarce. The twofold purposes of this study were: to assess the relationship between spatial anxiety and perceived stress in adults seeking medical care due to peripheral vestibular disease, and to explore the combined contribution of spatial anxiety, perspective-taking, and individual cofactors to the variability of their dizziness-related handicap. Accordingly, we conducted a correlational study assessing spatial anxiety, perceived stress, perspective-taking, and handicap-related to dizziness in adults with/without peripheral vestibular disease, with the following cofactors: demographics, individual habits (alcohol, tobacco, and sleep), symptoms of unsteadiness, motion sickness susceptibility, and symptoms of common mental disorders (anxiety/depression and depersonalization/derealization).
2 Materials and methods
2.1 Participants
After approval by the institutional Research and Ethics Committees (IMSS R 2021-3601-219), in a specialized healthcare institutional system (Instituto Mexicano del Seguro Social, Mexico), 309 consecutive participants fulfilling the selection criteria gave their informed consent to participate in the study. They were 153 patients with diagnosed peripheral vestibular disease (18 to 87 years old, 109 women and 44 men) who were referred for specialized evaluation (Figure 1), and 156 volunteers with no history or clinical evidence of vestibular disease (18 to 85 years old, 97 women and 59 men), relatives or companions of patients attending the outpatient clinics. The selection of participants was performed according to the following criteria: no history or medical record of middle ear, retinal, neurological (including migraine), autoimmune or autonomic disorders, or hearing loss >40 dB nHL, or submission to psychiatric care or psychopharmacological treatment and to have completed at least nine years of formal school (secondary school). Three more patients fulfilling the criteria were excluded from the study due to symptoms of acute upper airways disease, at the time of evaluation. The sample size was calculated to assess a correlation value of at least ρ = 0.3, with type I error of 0.01 and type II error of 0.1.
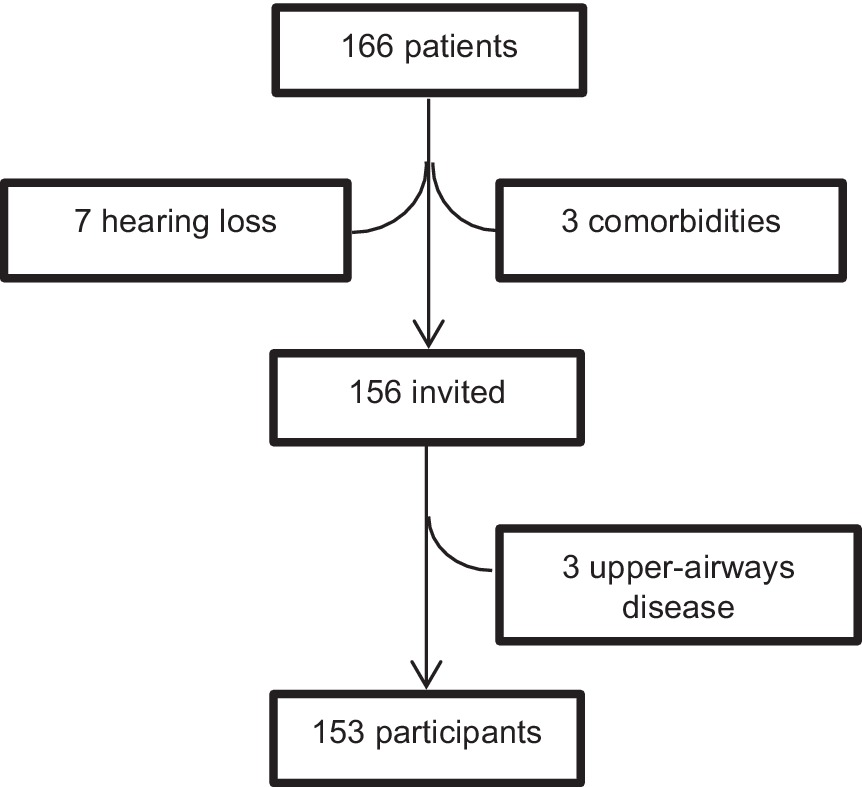
Figure 1. Selection of patients with peripheral vestibular disease.
The vestibular disease was confirmed at the neuro-otology clinic after at least: clinical assessment (including positional maneuvers), vestibular testing (caloric and/or rotatory tests), and audiological evaluation (middle ear impedance/audiometry/speech audiometry). The general characteristics of the participants are described in Table 1, according to the following groups: participants without history of vestibular disease and participants with diagnosed vestibular disease. Those with vestibular disease were classified by their clinical diagnoses in the following subgroups: bilateral vestibular deficiency, unilateral deficiency with <3 months of clinical evolution, unilateral deficiency with ≥3 months of clinical evolution, Meniere’s disease, and active Benign Paroxysmal Positional Vertigo (BPPV) (before treatment). The frequency of comorbidities in the two groups (without/with vestibular disease) is described in Table 2; compared to participants without vestibular disease, the frequency of corrected refraction errors was less than half in participants with vestibular disease, and no other differences were observed between the groups.
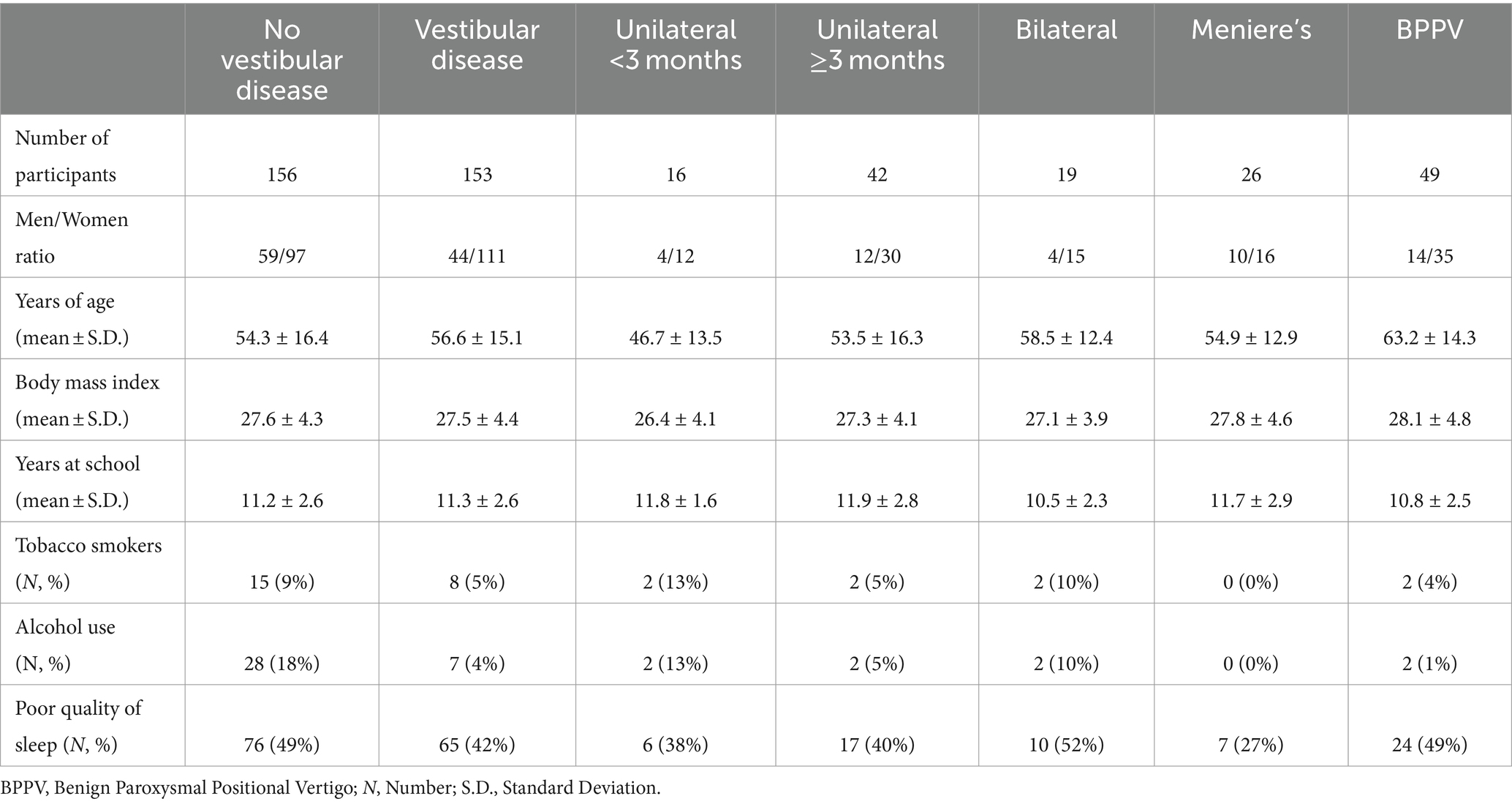
Table 1. General characteristics of 156 participants without and 153 with peripheral vestibular disease (by general diagnosis).
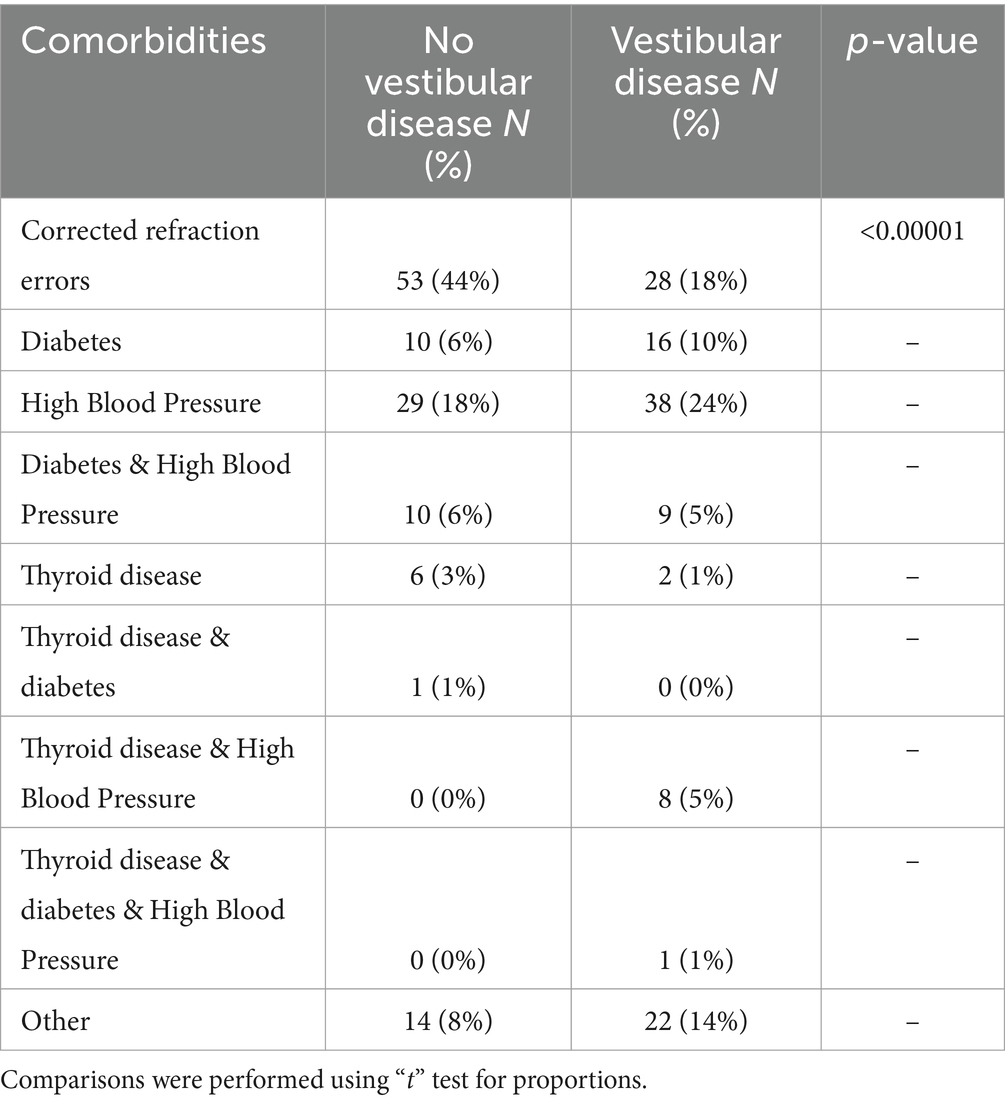
Table 2. Frequency of comorbidities in the 153 participants with and the 156 participants without peripheral vestibular disease.
2.2 Procedures
After all the participants reported their general health and personal habits (including alcohol and tobacco use) using an in-house questionnaire, the following instruments were administered for self-report:
2.2.1 Pittsburgh sleep quality index
Pittsburgh Sleep Quality Index (46) to assess sleep quality and sleep disturbances. The scale comprises 19 items to generate seven sub-scores on: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction. A total score is calculated by the sum of all sub-scores; an overall score of >5 indicates “poor” quality of sleep. The index has shown Cronbach’s alpha coefficient from 0.70 to 0.83 (47).
2.2.2 Motion sickness susceptibility questionnaire
Motion Sickness Susceptibility Questionnaire (short form) (48) to assess individual differences in motion sickness caused by a variety of stimuli (e.g., cars, boats, planes, trains, funfair rides). It contains 18-items, divided into two parts: part A to assess motion sickness during childhood, and part B to assess motion sickness during adulthood. Each sub-score ranges from 0 (no susceptibility) to 27 (maximum susceptibility), and a total score range from 0 to 54, higher scores indicate more susceptibility, with a Cronbach’s alpha coefficient of 0.87 (49).
2.2.3 Unsteadiness rating
Unsteadiness rating. A standardized questionnaire of symptoms related to unsteadiness (50) that includes nine items with no/yes responses. A “no” response is scored 0 points and a “yes” response is scored 1 point, except for vertigo that is scored 2 points. Frequent falls are considered only when ≥1 per month and frequent stumbles are considered only when ≥1 per week. A total score is obtained by summing the ratings for all the items (range 0 to 10). A score ≥4 points has been related to balance disorders (50).
2.2.4 Hospital anxiety and depression scale
Hospital Anxiety and Depression Scale (HADS) (51), which comprises 14 items, 7 for anxiety and 7 for depression, which are rated on a 4-point scale (0 to 3), each score ranges from 0 to 21, and a total score is obtained by summing the ratings for all the items. Cut-off scores of ≥8 (sub-scores) and ≥11 (total score) have shown sensitivities and specificities in the range of 0.70 to 0.90 for anxiety/ depression (51, 52), and Cronbach’s alpha coefficient from 0.67 to 0.93 (52).
2.2.5 State-trait anxiety inventory
The short version of the State-Trait Anxiety Inventory (53) to assess state anxiety, which comprises 6 items coded on a 4-point scale (from 0 to 3). A total score is calculated by the sum of the ratings for all the items (range from 0 to 18), higher scores are related to more anxiety (54).
2.2.6 Depersonalization/Derealization inventory
Depersonalization/Derealization Inventory (55), which comprises 28 items coded on a 5-point scale (from 0 to 4). A total score is obtained by the sum of the individual scores (range from 0 to 112), higher scores are related to more frequency/severity of depersonalization/derealization symptoms, with an internal consistency coefficient of 0.95 (55).
2.2.7 Perceived stress scale-10
Perceived Stress Scale-10 (56), which is a measure of global perceived stress. It contains 10 items that are coded on a 5-point scale (from 0 to 4). A total score ranging from 0 to 40 is computed by reverse scoring the four positively worded items and then summing the ratings for all the items, higher scores are related to more perceived stress, with a Cronbach’s alpha coefficient of 0.78 (57).
2.2.8 Spatial anxiety scale
Spatial Anxiety Scale (31), which includes three subscales assessing anxiety on spatial mental manipulation (8 items), spatial navigation (8 items), and spatial imagery (8 items). It comprises a total of 24 items that are scored on a 4-point scale (from 0 to 4). A total score is obtained by summing the ratings for all the items, higher scores are related to more spatial anxiety, with Cronbach’s alpha coefficient >0.8 (31).
2.2.9 Object perspective test
Object Perspective Test (58) in which participants rely on an egocentric frame of reference and form egocentric representations to solve the task. It is a pencil-and-paper test that comprises 12 items showing an array of objects and an “arrow circle”; participants are asked to imagine themselves facing a particular direction within the array, and then they are questioned about the direction between some of the objects. Absolute errors are calculated by the difference in degrees between the correct answer and what they draw in the “arrow circle.” Then a total score is obtained by the average for all the responses, higher scores indicate larger errors, with a total accuracy score of r = 0.77 (59).
2.2.10 Dizziness handicap inventory
Dizziness Handicap Inventory (60) to evaluate the self-perceived handicapping effects by dizziness and unsteadiness. It comprises 25 items that are scored on a 4-point scale (from 0 to 4). A total score is obtained by summing the ratings for all the items that were originally sub-grouped into three content domains, representing physical (7 items), emotional (9 items), and functional (9 items) aspects of handicap (60). Though, recent evidence suggests the need to reassess the factorial structure of the inventory (61, 62).
2.3 Experimental design and statistical analyses
A cross-sectional correlational study was designed. Assessment of data distribution was performed using the Kolmogorov Smirnov test. Accordingly, the bivariate analysis was performed using either: Mann Whitney U test or t-test (for means or for proportions); Spearman correlation or Pearson’s correlation coefficients; Kruskal Wallis analysis or analysis of variance (ANOVA) with Tukey honest significance test (HSD) for unequal N (Spjotvoll/Stoline test). The multivariate analysis was performed using analysis of covariance (ANCoVA), which was designed to compare participants with bilateral vestibular deficiency versus each of the other subgroups of participants. All the tests were performed using a two tailed significance level of 0.05.
3 Results
3.1 Bivariate analysis
3.1.1 Analysis by the general characteristics of the participants
Participants with/without vestibular disease had similar age and body mass index (p > 0.05) (Table 1). However, within the group of participants with vestibular disease, those with unilateral deficiency (either <3 months or ≥3 months of clinical evolution) were the youngest, while those with BPPV were the eldest (ANOVA, F = 5.397, p = 0.0004; Tukey HSD test for unequal N, p = 0.02). Linear correlation was observed between the age and the scores on: motion sickness susceptibility, perceived stress, quality of sleep and the anxiety sub-score of the HADS (Pearson r values from −0.12 to 0.20, p < 0.03).
The proportion of women was similar in the two main groups (with/without vestibular disease) and the mean years at formal school was the same for all subgroups (p > 0.05). Comparisons by sex on the instrument scores showed that, compared to men, women had higher scores on the symptoms related to unsteadiness (Mann Whitney U test, Z = −2.916, p = 0.003), the Navigation domain of spatial anxiety (Mann Whitney U test, Z − 2.315, p = 0.02), the three domains of the dizziness-related handicap instrument (Mann Whitney U test, Z from 1.963 to 2.099, p < 0.05), the sleep quality index (Mann Whitney U test, Z − 3.161, p = 0.001), and the sub-scores and total score of the HADS (Mann Whitney U test, Z from 1.963 to 2.577, p < 0.05). However, when a similar analysis by sex was performed just in the group of participants with vestibular disease, only the increased score on the sleep quality index in women (compared to men) persisted (Mann Whitney U test, Z − 2.749, p = 0.006), with a borderline result on the HADS depression sub-score (Mann Whitney U test, Z − 1.955, p = 0.0506).
For participants, the report of tobacco or alcohol use was low, particularly among those with vestibular disease (Table 1); while one third to half of the participants of any group or subgroup reported bad quality of sleep (Sleep Quality Index >5) (Table 1).
3.1.2 Analysis by groups and subgroups
On the questionnaire of symptoms related to unsteadiness, participants without vestibular disease reported almost no symptoms (Table 3) and among the subgroups of participants with vestibular disease the total score was similar (p > 0.05) (Table 3). The most frequent symptom was vertigo, except for the group of patients with bilateral vestibular disease, which reported vertigo with half the frequency than the other four subgroups of patients; in contrast, less than one fifth of the patients with vestibular disease of any subgroup reported frequent stumbles or frequent falls (Figure 2). Contrariwise, more than two thirds of the patients with vestibular disease, of any subgroup, reported instability when moving the head rapidly, or when changing posture rapidly (Figure 2).
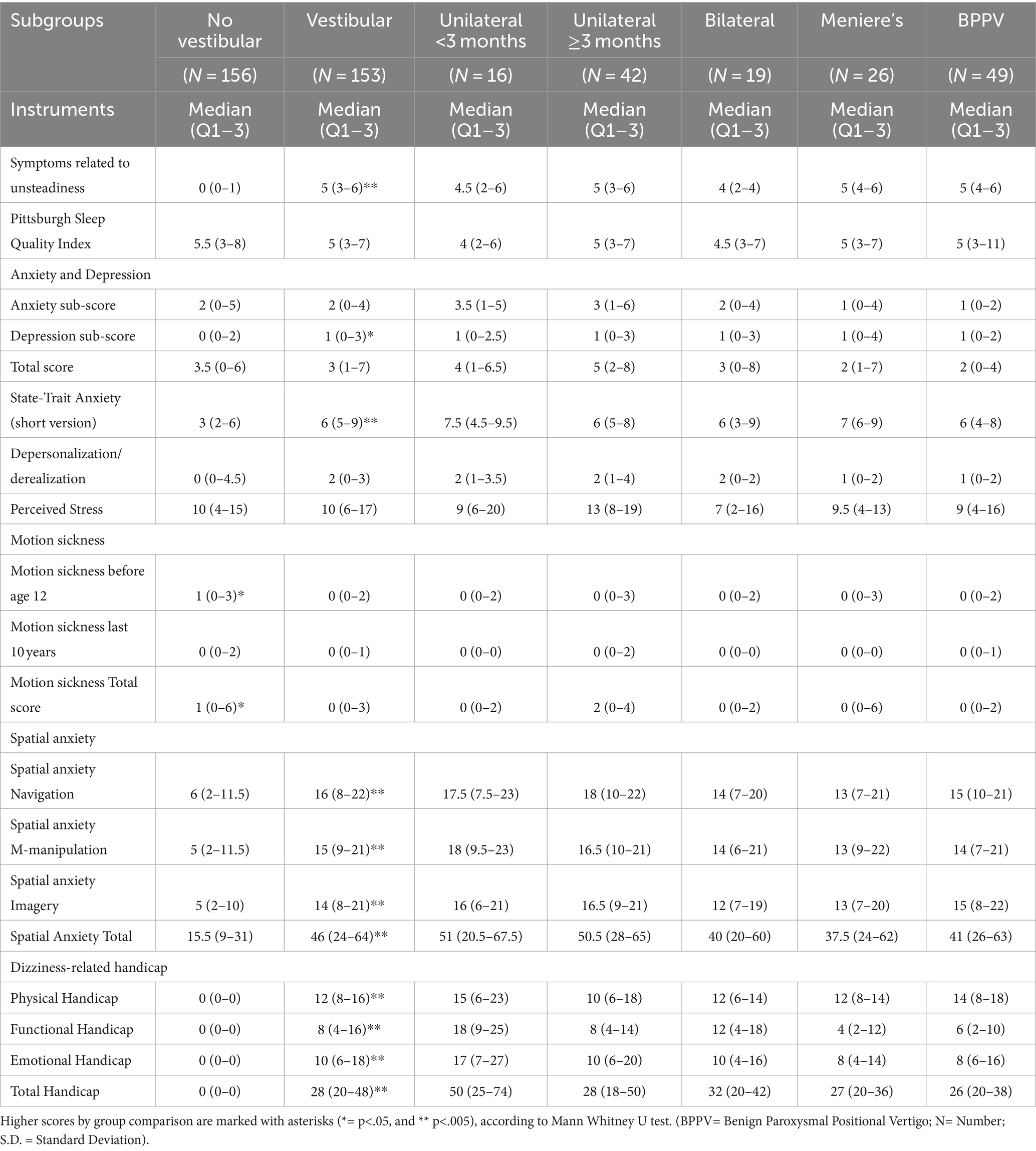
Table 3. Median and Quartiles 1 and 3 (Q1–Q3) of the scores on the instruments administered to 156 participants without and 153 with peripheral vestibular disease (by general diagnosis).
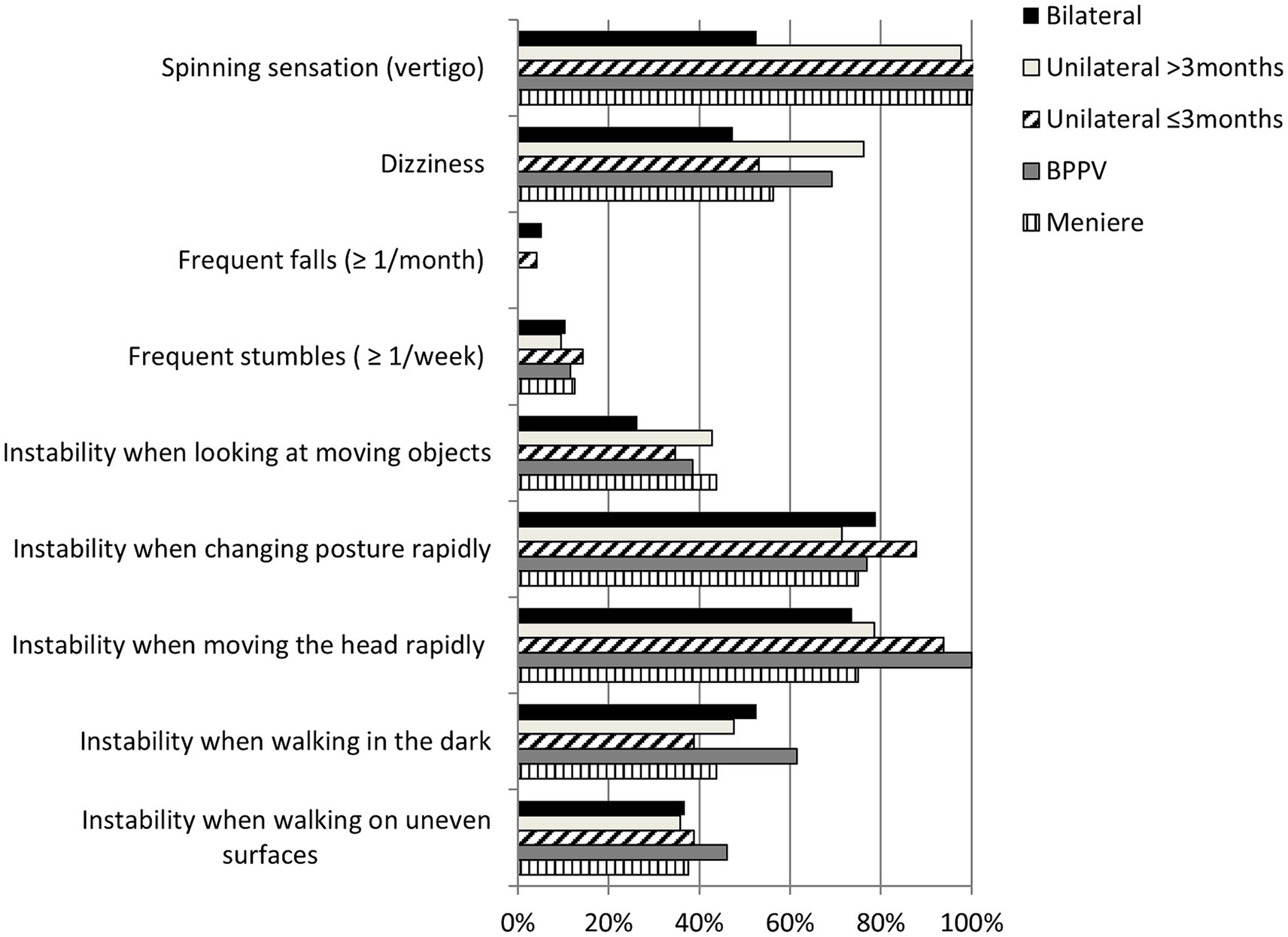
Figure 2. Frequency of symptoms related to unsteadiness of 153 patients by general diagnosis. (BPPV, Benign Paroxysmal Positional Vertigo).
Comparisons between the two groups (with/without vestibular disease) on the scores on symptoms of common mental disorders showed that the group with vestibular disease had higher scores on: state anxiety (Mann Whitney U test, adjusted Z = 7.514, p < 0.00001) and depression (HADS sub-score) (Mann Whitney U test, adjusted Z = 1.979, p = 0.04) (Table 3); with no differences among the subgroups of participants with vestibular disease (p > 0.05). For depersonalization/derealization, the score was similar among the groups and subgroups, but it was related to the scores on: anxiety/depression (HADS) (Spearman r values from 0.36 to 0.46, p < 0.00001), symptoms related to unsteadiness (Spearman r = 0.31, p < 0.00001), perceived stress (Spearman r = 0.31, p < 0.00001), motion sickness susceptibility (Spearman r values from 0.23 to 0.32, p < 0.00001), spatial anxiety (Spearman r values from 0.16 to 0.20, p < 0.05), and dizziness handicap (Spearman r values from 0.15 to 0.26, p < 0.01).
On the Motion Sickness Susceptibility Questionnaire, the participants with vestibular disease had lower scores than the participants without vestibular disease (Mann Whitney U test, adjusted Z = 2.041, p = 0.04). This score was related to the scores on: deviation of orientation on the object perspective test (Spearman r = −0.25, p < 0.00001), perceived stress (Spearman r = 0.24, p < 0.00001), and anxiety/depression (HADS) (Spearman r values from 0.17 to 0.34, p < 0.005).
On the Object Perspective Test, the participants without vestibular disease showed less total orientation deviation than the participants with vestibular disease (“t” test, t = 4.364, p = 0.0001). This difference was related to larger deviations in patients with either Meniere’s disease, and those with BPPV compared to participants without vestibular disease (ANOVA, F = 6.130, p < 0.0001; Tukey HSD test for unequal N, p < 0.05) (Figure 3). Among the participants with vestibular disease, patients with unilateral deficiency ≥3 months showed less deviation than those with BPPV (ANOVA, F = 3.872, p = 0.005; Tukey HSD test for unequal N, p = 0.01), with a borderline result when compared to patients with Meniere’s disease (Tukey HSD test for unequal N, p = 0.057). The deviation of orientation was related to the scores on: motion sickness susceptibility (Spearman r values from −0.25 to −0.22, p < 0.00002), dizziness handicap (Spearman r values from 0.19 to 0.23, p < 0.0005), state anxiety (Spearman r = 0.20, p < 0.0005), perceived stress (Spearman r = −0.11, p < 0.05), and spatial anxiety total score and the three sub-scores (Spearman r values from 0.11 to 0.15, p < 0.02).
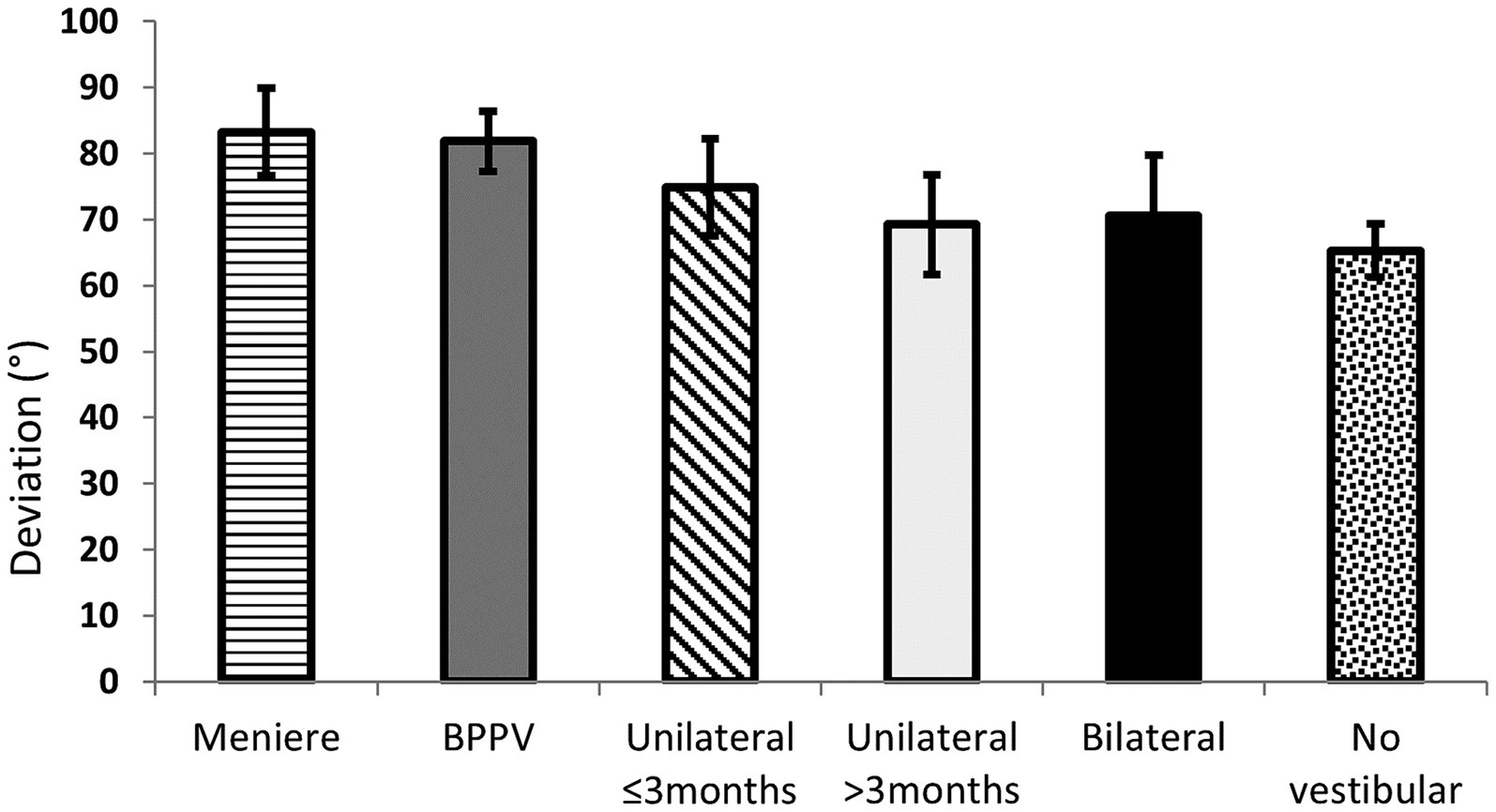
Figure 3. Mean and 95% Confidence Interval of the mean of the deviation on the Object Perspective Test of 153 patients (by general diagnosis) and 156 participants with no vestibular disease. (BPPV, Benign Paroxysmal Positional Vertigo).
On the Spatial Anxiety Scale, the three sub-scores and the total score were consistently higher in participants with vestibular disease compared to participants without vestibular disease (Table 3) (Mann Whitney U test, adjusted Z > 8.390, p < 0.00001). However, no significant difference was evident among the subgroups of participants with vestibular disease (p > 0.05) (Figure 4). Correlation between the scores (partial and total) on the Spatial Anxiety Scale and each of the other instrument scores is described in Table 4. Consistent correlations across the sub-scores and total score on spatial anxiety were observed on the scores on: symptoms related to unsteadiness (Spearman r values from 0.45 to 0.50; p < 0.00001), state anxiety (Spearman r values from 0.29 to 0.33, p < 0.00001), perceived stress (Spearman r values from 0.20 to 0.29, p > 0.0005), and the deviation of orientation on the object perspective test (Spearman r values from 0.11 to 0.15, p < 0.05).

Figure 4. Median of the sub-scores and total score on the spatial anxiety of 153 patients by general diagnosis. (BPPV, Benign Paroxysmal Positional Vertigo).
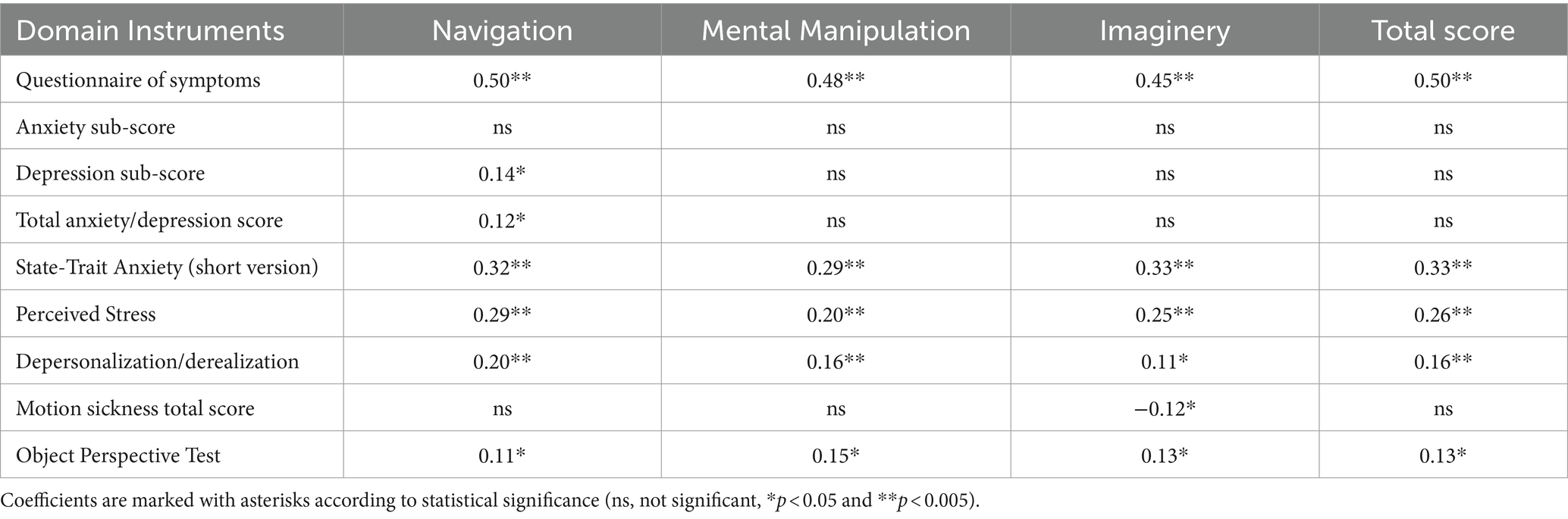
Table 4. Spearman rank correlation between the Spatial Anxiety Questionnaire sub-scores and total score, and the scores on the instruments to evaluate the study variables, of 309 participants (153 with and 156 without peripheral vestibular disorder).
On the Dizziness Handicap Inventory, among the subgroups of participants with vestibular disease, a difference was observed on the emotional domain, in which patients with unilateral deficiency <3 months showed the highest score among all subgroups (Kruskal Wallis, H = 11.115, p = 0.02) (Table 3). Correlation between the scores (partial and total) on the handicap related to dizziness and each of the other instrument scores is described in Table 5. Consistent correlations of the sub-scores and total score on handicap related to dizziness were observed with the scores on: symptoms related to unsteadiness (Spearman r values from 0.66 to 0.79; p < 0.00001), spatial anxiety (Spearman r values from 0.47 to 0.50, p < 0.0002), state anxiety (Spearman r values from 0.36 to 0.38, p < 0.00001), anxiety/depression (HADS) (Spearman r values from 0.14 to 0.30, p < 0.05), depersonalization/derealization (Spearman r values from 0.15 to 0.27, p < 0.005), and deviation of orientation on the object perspective test (Spearman r from 0.19 to 0.22, p < 0.005).
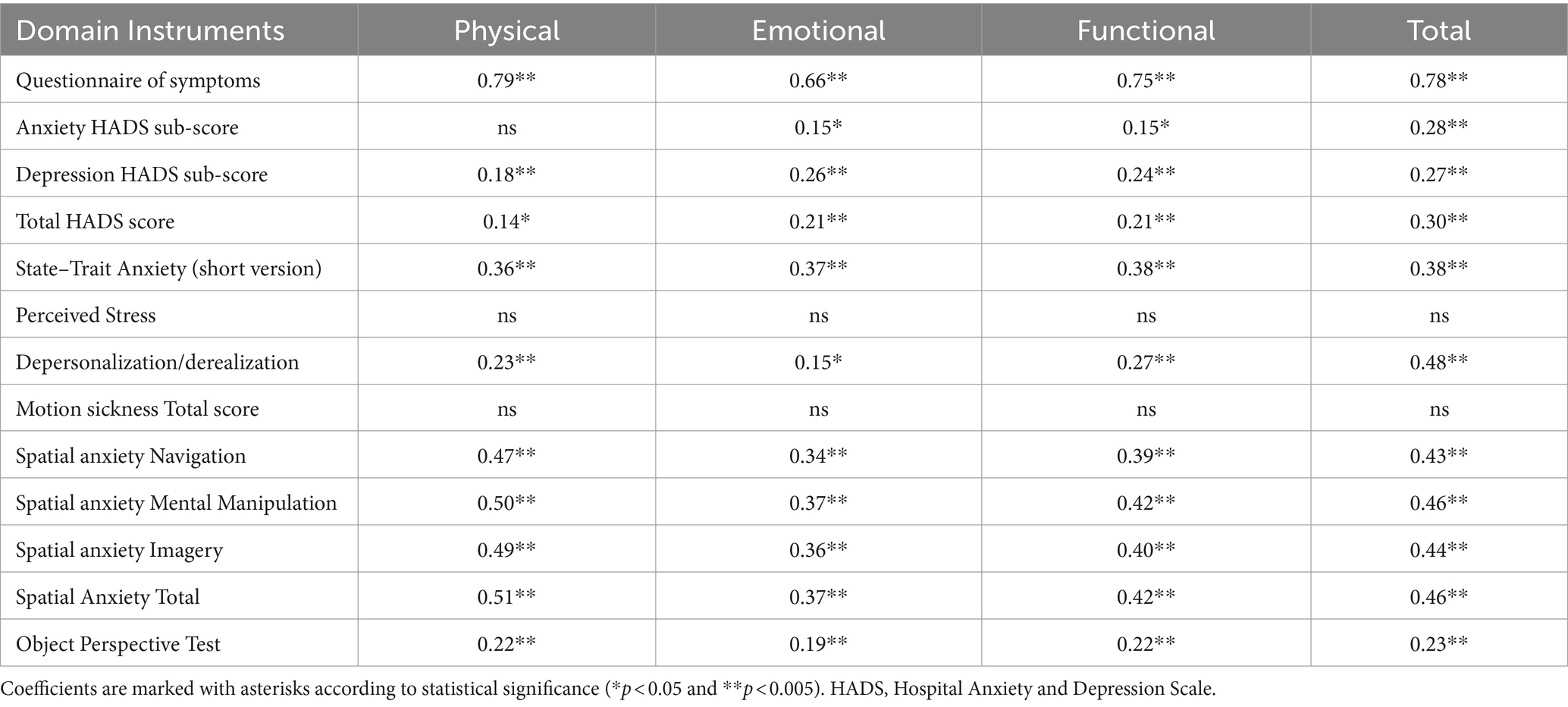
Table 5. Spearman rank correlation between the Dizziness Handicap Inventory (sub-scores and total score) and the evaluation instruments of 309 participants (153 with and 156 without peripheral vestibular disease).
3.2 Covariance analysis including cofactors
3.2.1 Analysis on spatial anxiety score
The covariance analysis including individual cofactors showed that the variables consistently contributing to the variance across the total score and sub-scores on spatial anxiety were (ANCoVA, adjusted multiple R2 from 0.27 to 0.30, F values from 17.945 to 20.086, p < 0.00001) (beta values by domain are described in Table 6): symptoms related to unsteadiness, perceived stress, and HADS score ≥11 points, besides the contrast between participants with bilateral vestibular deficiency versus those without vestibular disease. Participants with vestibular disease with a HADS total score ≥11 points showed lower spatial anxiety sub-scores and total score than those with a HADS total score <11 points, after controlling for covariates (ANCoVA, F = 5.854, p = 0.016) (Figure 5). Further exploratory analysis showed that this difference was evident in all the subgroups of patients and the result was reproducible on the HADS anxiety sub-score (≥8) (ANCoVA, F = 5.282, p = 0.02), but not on the depression sub-score (≥8) (p > 0.05).
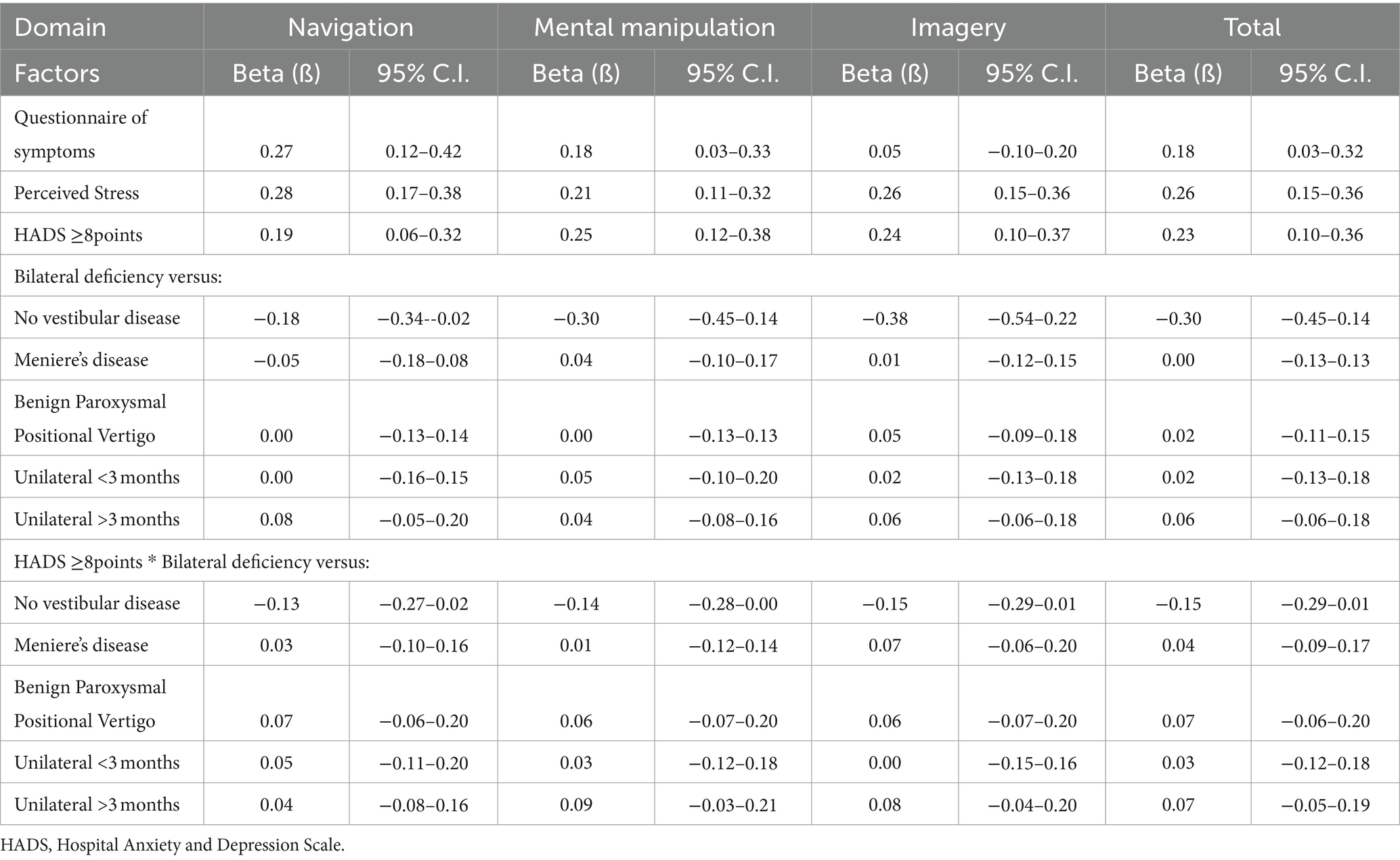
Table 6. Beta values and 95% Confidence Interval (C.I.) of the beta values of the variables included in the general linear model on the Spatial Anxiety score and subscores.
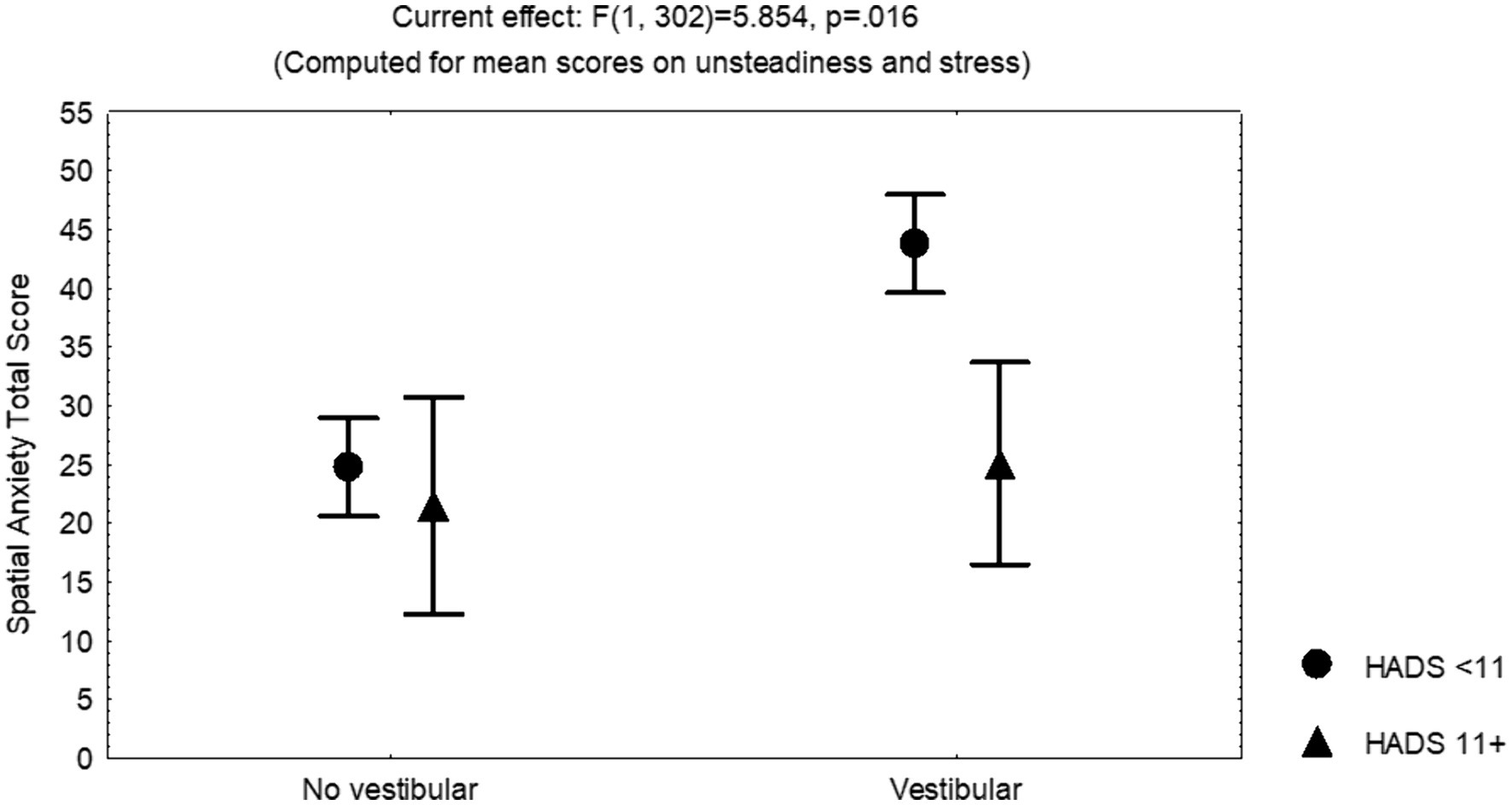
Figure 5. Least square means and standard error of the mean of the total score on the Spatial Anxiety Scale, corrected by the mean scores on symptoms of unsteadiness and perceived stress, of 156 participants without and 153 participants with vestibular disease. (HADS, Hospital Anxiety and Depression Scale).
3.2.2 Analysis on the orientation deviation score
The covariance analysis including individual cofactors showed that the variables consistently contributing to the variance on the orientation deviation were (ANCoVA, adjusted multiple R2 = 0.18, F = 5.834, p < 0.00001): vestibular disease (beta −0.23, 95% C.I. −0.40–0.05), HADS anxiety sub-score (≥8) (beta 0.22, 95% C.I. 0.09–0.34) (Figure 6), state anxiety (beta 0.20, 95% C.I. 0.08–0.31), motion sickness susceptibility (beta −0.15, 95% C.I. −0.25–0.04), and age (beta 0.11, 95% C.I. 0.001–0.21); however no interaction between the vestibular diagnose and HADS anxiety sub-score (≥8) was observed.
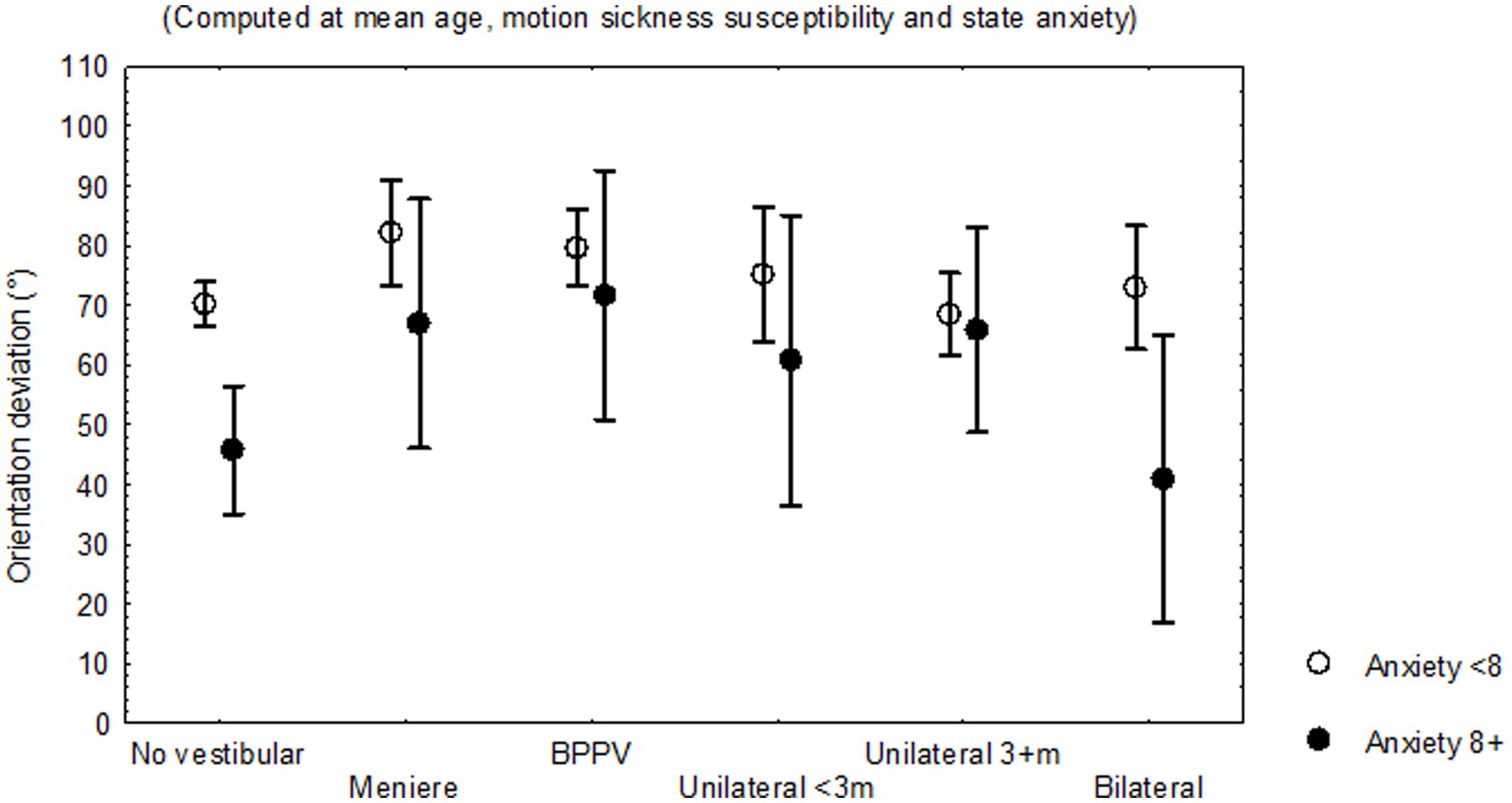
Figure 6. Least square means and standard error of the mean of the deviation of orientation on the Objective Perspective Test, according to the evidence of trait anxiety, corrected by the mean age, motion sickness susceptibility score and state anxiety score of 156 participants without and 153 participants with vestibular disease, by subgroup of diagnoses.
3.2.3 Analysis on the dizziness handicap inventory score and subscores
The covariance analysis including individual cofactors showed that the variables consistently contributing to the variance on the total Dizziness Handicap Inventory score were (ANCoVA, adjusted multiple R2 = 0.66, F = 39.07, p < 0.00001) (beta values are described in Table 7): symptoms related to unsteadiness; orientation deviation; quality of sleep score; HADS score ≥11 points, with higher handicap score in those with HADS score ≥11 points and either unilateral deficiency <3 months or BPPV; and the contrast between participants with bilateral vestibular deficiency versus those without vestibular disease, those with unilateral deficiency <3 months, and those with BPPV.
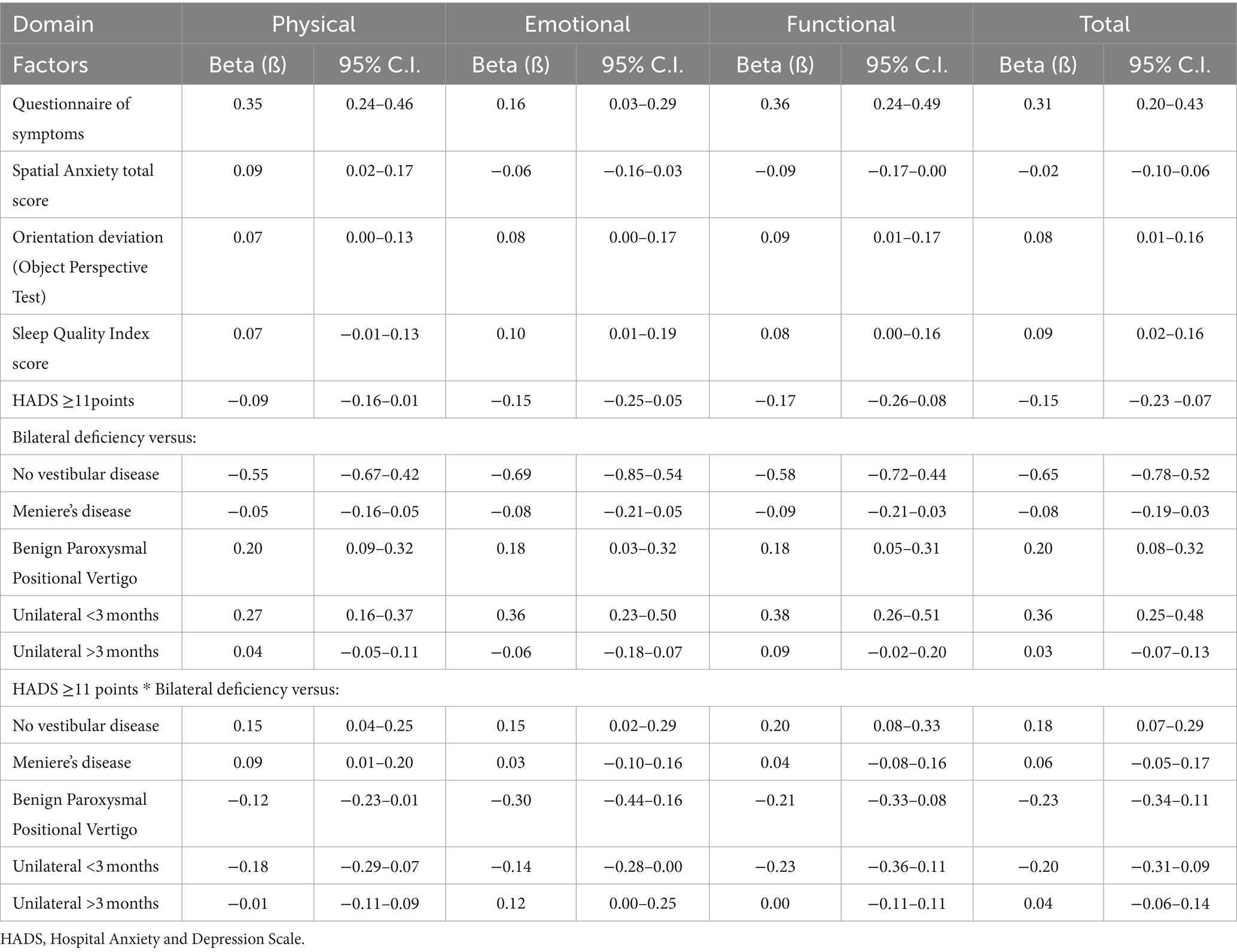
Table 7. Beta values and 95% Confidence Interval (C.I.) of the beta values of the variables included in the general linear model on the Dizziness Handicap Inventory score and sub-scores.
The covariance analysis on each domain of the Dizziness Handicap Inventory showed that the variables that consistently contributed to the variance on the Physical domain score were (ANCoVA, adjusted multiple R2 = 0.69, F = 44.77, p < 0.00001) (Table 7): symptoms related to unsteadiness, the orientation deviation, spatial anxiety (total score and sub-scores), quality of sleep, HADS score ≥11 points, and the contrast between participants with bilateral vestibular deficiency versus those without vestibular disease, those with unilateral deficiency <3 months, and those with BPPV. The variables that consistently contributed to the variance on the Emotional domain were (ANCoVA, adjusted multiple R2 = 0.52, F = 21.32, p < 0.00001) (Table 7): symptoms related to unsteadiness, quality of sleep, HADS score ≥11 points, and the contrast between participants with bilateral vestibular deficiency versus those without vestibular disease, and those with unilateral deficiency <3 months. The variables that consistently contributed to the variance on the Functional domain were (ANCoVA, adjusted multiple R2 = 0.60, F = 29.53, p < 0.00001) (Table 7): symptoms related to unsteadiness, orientation deviation, quality of sleep score, HADS score ≥11 points, and the contrast between participants with bilateral vestibular deficiency versus those without vestibular disease, and those with unilateral deficiency <3 months; however when the interaction between HADS ≥11 points and the vestibular diagnoses was considered, a significant result was also observed for the subgroup with BPPV. Additionally, the Navigation domain of the spatial anxiety questionnaire also contributed to the variance on the Functional domain of dizziness-related handicap (ANCoVA, F = 4.940, p = 0.027).
4 Discussion
In this study, spatial anxiety was related to the report of both symptoms of unsteadiness and perceived stress, but it was less in those with HADS anxiety sub-score ≥ 8 (Figure 5). The total score and the sub-scores on spatial anxiety contributed to the variability on the score of the Physical domain of the Dizziness Handicap Inventory, while just the score of the Navigation domain contributed to the functional domain of the handicap instrument. Other variables contributing to the variability on dizziness-related handicap were the report of symptoms of unsteadiness, the orientation deviation on the object perspective test, the quality of sleep, and anxiety/depression symptoms. Additionally, the orientation deviation was related to vestibular disease, the score on anxiety (both state anxiety and trait anxiety), the motion sickness susceptibility, and age (Figure 6).
The simultaneous relationship of spatial anxiety with symptoms of unsteadiness and perceived stress could be considered within the response to vestibular damage. Stress is a physiological reaction to a stimulus, improving the opportunity to overcome a stressor, which varies according to the stressor and the individual characteristics. Image studies support that down-regulation of the fear network may contribute to reduce distress during unpleasant body accelerations (63); while in patients with acute vestibular damage, acute stress facilitates vestibular compensation (33). However, repetitive exposure to stressors may induce adaptive changes in the brain circuits regulating the stress response (64), while removing the emotional arousal of novelty may abolish facilitation (65).
Chronic stress provokes circumscribed neurochemical changes in sub-regions of the hippocampus and the entorhinal and frontal cortices (66). In animal models, chronic stress is a cause of neuron atrophy in both the hippocampus and the prefrontal cortex, which are involved in memory, selective attention, and executive function, with hypertrophy of neurons in the amygdala that is involved in fear and anxiety, as well as aggression (67), and it also disturbs neurogenesis and survival of newly born neurons in the hippocampus (68); consequently, chronic stress alters the acute stress response on functions such as spatial memory (69). Consistently, patients with chronic bilateral vestibular deficits may report spatial anxiety (12), and display deficits on spatial abilities (12, 70, 71).
In this study, participants with peripheral vestibular disease and HADS anxiety sub-score ≥ 8 (symptoms of trait anxiety) showed lower spatial anxiety, compared to those with HADS anxiety sub-score < 8 (less symptoms of trait anxiety) (Figure 5), while participants with trait anxiety showed less orientation deviation on the object perspective test. These findings are consistent with studies in healthy adults within a threatening context, in which high levels of trait anxiety may improve the ability to retrace a route, whereas low levels of trait anxiety may be associated with worse performance under threat, supporting that the predisposition for emotional reaction could be helpful to overcome the apprehension provoked by the spatial task (26). Additionally, the interrelated neural circuits controlling stress and anxiety substantiate a bidirectional relationship (34); in subjects without psychiatric diagnosis, anxiety and depression have been associated with blunted or exaggerated cortisol responses to and recovery from stress (72).
It is frequently assumed that vestibular symptoms are provoked/heightened by anxiety and stress, but the results of this study support that state anxiety and the stress response could be helpful for recovery, whereas spatial anxiety can be detrimental. The results support that, in patients with peripheral vestibular disease, spatial anxiety may contribute to dizziness-related handicap. This contribution was evident particularly on the Physical domain of the handicap instrument, besides the distinct contribution of the Navigation domain of spatial anxiety to the Functional domain of the handicap inventory. These results are congruent with the design of the instruments administered for evaluation of these two variables. The Spatial Anxiety Questionnaire refers “to situations and experiences that may cause tension, apprehension, or anxiety” (31). In this study, the participants with peripheral vestibular disease consistently reported spatial anxiety related to performance of physical activities, including activities that may provoke dizziness/unsteadiness, which are evaluated by the Physical domain of the Dizziness Handicap Inventory (60); while anxiety related to navigation was deleterious for their daily life functioning, according to the limiting consequences of the symptoms reported by the Functional domain of the handicap inventory. These concepts are also classified in the International Classification of Functioning, Disability and Health (73) and described as: “activity limitations are difficulties an individual may have in executing activities,” and “participation restrictions are problems an individual may experience in involvement in life situations.” Yet, variability of limitations and restrictions related to health conditions may be influenced by contextual factors, including personal factors such as “fitness, lifestyle, habits, upbringing, coping styles, social background, education, profession, past and current experience (past life events and concurrent events), overall behavior pattern and character style, individual psychological assets and other characteristics” (73).
The contribution of the report of unsteadiness and symptoms of anxiety/depression (HADS) to the dizziness-related handicap is consistent with evidence towards worse scores on self-reported measurements on functioning increasing the severity of dizziness-related handicap (74), and the correlation between the report of symptoms of depression with both vestibular symptoms and the sense of disability (75). Consistently, after acute vestibular lesion, depression symptoms may persist while updating spatial orientation improves (45); whereas symptomatic peripheral vestibular disease has been related to increased risk for attempted suicide over a follow-up of 1 year, after adjusting for demographic related comorbidities (76). Although, adaptive changes may occur that could explain the differences among the subgroups of patients with variable clinical evolution. Additionally, the report of depersonalization/derealization symptoms was linearly related to multiple variables, including unsteadiness, perceived stress, and anxiety/depression, yet the multivariate analysis did not show an independent contribution to the variability of dizziness-related handicap.
The contribution of the orientation deviation to handicap, particularly in patients with episodic vertigo, can be explained by the relevance of the vestibular reference for egocentric mental transformations (77); though perspective-taking tests can be solved by both mentally reorienting oneself and mentally rotating the stimuli (78). Additionally, the orientation deviation had a negative relationship with the score on motion sickness susceptibility, which was less in patients with bilateral vestibular deficit. This result is consistent with the requirement of intact vestibular function for the provocation of motion sickness and to the association of motion sickness with mechanisms involved in adapting the spatial orientation system to strange environments (79).
The contribution of the quality of sleep to dizziness-related handicap corresponds to the evidence on the interaction of sleep with vestibular function and balance (80–82). Sleep and wakefulness are regulated by the aminergic, cholinergic brainstem and hypothalamic systems with involvement of immune homeostatic regulating mechanisms (83). In rats, vestibular damage can affect the sleep-wakefulness cycle with up-regulation of the level of autophagy in hypothalamic tissue (84). In humans, epidemiologic evidence supports that adults with vertigo have a higher risk for abnormal sleep duration (85); conversely, in patients with sleep complains, sleep architecture variation has been associated with vestibular symptoms (86). Additionally, clinical studies have shown that persistent sleep disturbance after vestibular rehabilitation is related to handicap severity (87), while rehabilitation for unilateral vestibular disease is associated to improvement of the quality of sleep (88). However, these variables interact with stress, with a bidirectional relation between stress and sleep quantity, in which worse sleep quantity and continuity may predict higher next-day stress (89).
The findings of this study may support future studies, including the design of clinical studies on spatial anxiety and chronic stress in adults with peripheral vestibular disease, to assess their spatial abilities, according to their clinical characteristics. Of relevance to rehabilitation, it is possible that spatial anxiety, specifically apprehension about moving in situations which would provoke unpleasant, vestibular symptoms, could prevent a patient from actively engaging with challenging circumstances to encourage adaptation.
The results of this study should be interpreted in the context of its limitations. The cross-sectional design prevents discussion of any causal relationship. The sample size was calculated to assess moderate to strong correlations; thus, we cannot deny weaker relationships. The study was limited to the most obvious factors influencing the results. Enrolment was limited to patients receiving specialized medical care without comorbidities that could interfere with the assessed relationships, so the results may be different in other clinical settings. However, the strengths of the study include the prospective collection of the data by trained health professionals, the variety of cofactors that were evaluated, and the consistency of the results.
5 Conclusion
In adults both with and without vestibular disease, spatial anxiety can be related to both unsteadiness and perceived stress and may be less in those with symptoms of trait anxiety (HADS anxiety sub-score ≥ 8). Spatial anxiety and impairment of perspective-taking, along with poor quality of sleep and trait anxiety may contribute to the Physical and Functional domains of dizziness-related handicap. Whereas follow-up studies are required to assess if a degree of anxiety and stress could be beneficial to encourage rehabilitation, specific spatial anxiety can be detrimental, possibly because it limits behavior beneficial to adaptation.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Instituto Mexicano del Seguro Social. IMSS R 2021-3601-219. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
KJ-R: Conceptualization, Formal analysis, Investigation, Methodology, Project administration, Resources, Supervision, Visualization, Writing – original draft, Writing – review & editing. DG-J: Data curation, Investigation, Validation, Writing – review & editing. SB-O: Data curation, Investigation, Validation, Writing – review & editing. MG: Visualization, Writing – review & editing. AG-M: Investigation, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
2. Buckley, J, Seery, N, and Canty, D. A heuristic framework of spatial ability: a review and synthesis of spatial factor literature to support its translation into STEM education. Educ Psychol Rev. (2018) 30:947–72. doi: 10.1007/s10648-018-9432-z
3. Linn, MC, and Petersen, AC. Emergence and characterization of sex differences in spatial ability: a meta-analysis. Child Dev. (1985) 56:1479–98. doi: 10.2307/1130467
4. Gardner, MR, Stent, C, Mohr, C, and Golding, JF. Embodied perspective-taking indicated by selective disruption from aberrant self-motion. Psychol Res. (2017) 81:480–9. doi: 10.1007/s00426-016-0755-4
5. Israël, I, Sievering, D, and Koenig, E. Self-rotation estimate about the vertical axis. Acta Otolaryngol. (1995) 115:3–8. doi: 10.3109/00016489509133338
6. Allum, JHJ, Langewitz, W, Sleptsova, M, Welge-Luessen, A, Honegger, F, Schatz, TH, et al. Mental body transformation deficits in patients with chronic balance disorders. J Vestib Res. (2017) 27:113–25. doi: 10.3233/VES-170613
7. Shinder, ME, and Taube, JS. Differentiating ascending vestibular pathways to the cortex involved in spatial cognition. J Vestib Res. (2010) 20:3–23. doi: 10.3233/VES-2010-0344
8. Brandt, T, Schautzer, F, Hamilton, DA, Bruning, R, Markowitsch, HJ, Kalla, R, et al. Vestibular loss causes hippocampal atrophy and impaired spatial memory in humans. Brain. (2005) 128:2732–41. doi: 10.1093/brain/awh617
9. Guidetti, G, Guidetti, R, Manfredi, M, and Manfredi, M. Vestibular pathology and spatial working memory. Acta Otorhinolaryngol Ital. (2020) 40:72–8. doi: 10.14639/0392-100X-2189
10. Mast, FW, Preuss, N, Hartmann, M, and Grabherr, L. Spatial cognition, body representation and affective processes: the role of vestibular information beyond ocular reflexes and control of posture. Front Integr Neurosci. (2014) 8:44. doi: 10.3389/fnint.2014.00044
11. Jáuregui-Renaud, K, Sang, YPF, Gresty, MA, Green, DA, and Bronstein, AM. Depersonalization/derealization symptoms and updating orientation in patients with vestibular disease. J Neurol Neurosurg Psychiatry. (2008) 79:276–83. doi: 10.1136/jnnp.2007.122119
12. Kremmyda, O, Hüfner, K, Flanagin, VL, Hamilton, DA, Linn, J, Strupp, M, et al. Beyond dizziness: virtual navigation, spatial anxiety and hippocampal volume in bilateral vestibulopathy. Front Hum Neurosci. (2016) 10:139. doi: 10.3389/fnhum.2016.00139
13. Uttal, DH, Meadow, NG, Tipton, E, Hand, LL, Alden, AR, Warren, C, et al. The malleability of spatial skills: a meta-analysis of training studies. Psychol Bull. (2013) 139:352–402. doi: 10.1037/a0028446
14. Thoresen, JC, Francelet, R, Coltekin, A, Richter, KF, Fabrikant, SI, and Sandi, C. Not all anxious individuals get lost: trait anxiety and mental rotation ability interact to explain performance in map-based route learning in men. Neurobiol Learn Mem. (2016) 132:1–8. doi: 10.1016/j.nlm.2016.04.008
15. Balaban, CD, and Thayer, JF. Neurological bases for balance-anxiety links. J Anxiety Disord. (2001) 15:53–79. doi: 10.1016/S0887-6185(00)00042-6
16. Eckhardt-Henn, A, Best, C, Bense, S, Breuer, P, Diener, G, Tschan, R, et al. Psychiatric comorbidity in different organic vertigo syndromes. J Neurol. (2008) 255:420–8. doi: 10.1007/s00415-008-0697-x
17. Decker, J, Limburg, K, Henningsen, P, Lahmann, C, Brandt, T, and Dieterich, M. Intact vestibular function is relevant for anxiety related to vertigo. J Neurol. (2019) 266:89–92. doi: 10.1007/s00415-019-09351-8
18. Yuan, Q, Yu, L, Shi, D, Ke, X, and Zhang, H. Anxiety and depression among patients with different types of vestibular peripheral vertigo. Medicine (Baltimore). (2015) 94:e453. doi: 10.1097/MD.0000000000000453
19. Mittelstaedt, JM. Individual predictors of the susceptibility for motion-related sickness: a systematic review. J Vestib Res. (2020) 30:165–93. doi: 10.3233/VES-200702
20. Coehlo, CM, and Balaban, CD. Visuo-vestibular contributions to anxiety and fear. Neurosci Biobehav Rev. (2015) 48:148–59. doi: 10.1016/j.neubiorev.2014.10.023
21. Gray, JA. A neuropsychological theory of anxiety. In emotions in personality and psychopathology Boston. Springer US: MA (1979).
22. Faravelli, C, Scarpato, MA, Castellini, G, and Lo, SC. Gender differences in depression and anxiety: the role of age. Psychiatry Res. (2013) 210:1301–3. doi: 10.1016/j.psychres.2013.09.027
23. Altemus, M, Sarvaiya, N, and Epperson, C. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. (2014) 35:320–30. doi: 10.1016/j.yfrne.2014.05.004
24. Cox, RC, and Olatunji, BO. A systematic review of sleep disturbance in anxiety and related disorders. J Anxiety Disor. (2016) 37:104–29. doi: 10.1016/j.janxdis.2015.12.001
25. Spielberger, CD. State-trait anxiety inventory for adults (STAI-AD). Washington, D.C.: APA PsycTests (1983).
26. Bublatzky, F, Allen, P, and Riemer, M. Spatial navigation under threat: aversive apprehensions improve route retracing in higher versus lower trait anxious individuals. Front Psychol. (2023) 14:1166594. doi: 10.3389/fpsyg.2023.1166594
27. Roozendaal, B, Schelling, G, and McGaugh, JL. Corticotropin-releasing factor in the basolateral amygdala enhances memory consolidation via an interaction with the β-adrenoceptor–cAMP pathway: dependence on glucocorticoid receptor activation. J Neurosci. (2008) 28:6642–51. doi: 10.1523/JNEUROSCI.1336-08.2008
28. Alvarez-Vargas, D, Abad, C, and Pruden, SM. Spatial anxiety mediates the sex difference in adult mental rotation test performance. Cogn Res Princ Implic. (2020) 5:31. doi: 10.1186/s41235-020-00231-8
29. Lawton, CA. Gender differences in way-finding strategies: relationship to spatial ability and spatial anxiety. Sex Roles. (1994) 30:765–79. doi: 10.1007/BF01544230
30. Hund, AM, and Minarik, JL. Getting from Here to there: spatial anxiety, wayfinding strategies, direction type, and wayfinding efficiency. Spatial Cogn Comput. (2006) 6:179–201. doi: 10.1207/s15427633scc0603_1
31. Lyons, IM, Ramirez, G, Maloney, EA, Rendina, DN, and Levine, SC. Beilock SL spatial anxiety: a novel questionnaire with subscales for measuring three aspects of spatial anxiety. J Numeric Cognit. (2018) 4:526–53. doi: 10.5964/jnc.v4i3.154
32. Malanchini, M, Rimfeld, K, Shakeshaft, NG, Rodic, M, Schofield, K, Selzam, S, et al. The genetic and environmental aetiology of spatial, mathematics and general anxiety. Sci Rep. (2017) 7:42218. doi: 10.1038/srep42218
33. Saman, Y, Bamiou, DE, Gleeson, M, and Dutia, MB. Interactions between stress and vestibular compensation – a review. Front Neurol. (2012) 3:00116. doi: 10.3389/fneur.2012.00116
34. Daviu, N, Bruchas, MR, Moghaddamc, B, Sandid, C, and Beyelere, A. Neurobiological links between stress and anxiety. Neurobiol Stress. (2019) 11:100191. doi: 10.1016/j.ynstr.2019.100191
35. Gunnar, M, and Quevedo, K. The neurobiology of stress and development. Annu Rev Psychol. (2007) 58:145–73. doi: 10.1146/annurev.psych.58.110
36. Gliddon, CM, Darlington, CL, and Smith, PF. Activation of the hypothalamic–pituitary-adrenal axis following vestibular deafferentation in pigmented guinea pig. Brain Res. (2003) 964:306–10. doi: 10.1016/S0006-8993(02)04086-6
37. Igarashi, M, Ishikawa, K, Ishii, M, and Schmidt, KA. Effect of ACTH-(4–10) on equilibrium compensation after unilateral labyrinthectomy in the squirrel monkey. Eur J Pharmacol. (1985) 119:239–42. doi: 10.1016/0014-2999(85)90302-4
38. Gilchrist, DP, Smith, PF, and Darlington, CL. ACTH (4–10) accelerates ocular motor recovery in the guinea pig following vestibular deafferentation. Neurosci Lett. (1990) 118:14–6. doi: 10.1016/0304-3940(90)90237-4
39. Dagilas, A, Kimiskidis, V, Aggelopoulou, M, Kapaki, E, Fitili, C, Libitaki, G, et al. Changes in Blood Neurotransmitter and Steroid Levels During Evoked Vertigo. Otol Neurotol. (2005) 26:476–80. doi: 10.1097/01.mao.0000169785.15083.28
40. Sachar, EJ, Hellman, L, Roffwarg, HP, Halpern, FS, Fukushima, DK, and Gallagher, TF. Disrupted 24-hour patterns of cortisol secretion in psychotic depression. Arch Gen Psychiarty. (1973) 28:19–24. doi: 10.1001/archpsyc.1973.01750310011002
41. Koopman, C, Classen, C, Cardeña, E, and Spiegel, D. When disaster strikes, acute stress disorder may follow. J Trauma Stress. (1995) 8:29–46. doi: 10.1007/BF02105405
42. Joels, M, Pu, Z, Wiegert, O, Oitzl, MS, and Krugers, HJ. Learning under stress: how does it work? Trends Cogn Sci. (2006) 10:152–8. doi: 10.1016/j.tics.2006.02.002
43. Simeon, D, Guralnik, O, Knutelska, M, Hollander, E, and Schmeidler, J. Hypothalamic-pituitary-adrenal axis dysregulation in depersonalization disorder. Neuropsychopharmacology. (2001) 25:793–5. doi: 10.1016/S0893-133X(01)00288-3
44. Sang, YPF, Jáuregui-Renaud, K, Green, DA, Bronstein, AM, and Gresty, MA. Depersonalization/ derealization symptoms in vestibular disease. J Neurol Neurosurg Psychiatry. (2006) 77:760–6. doi: 10.1136/jnnp.2005.075473
45. Gómez-Alvarez, FB, and Jáuregui-Renaud, K. Psychological symptoms and spatial orientation during the first 3 months after acute unilateral vestibular lesion. Arch Med Res. (2011) 42:97–103. doi: 10.1016/j.arcmed.2011.03.004
46. Buysse, DJ, Reynolds, CF III, Monk, TH, Berman, SR, and Kupfer, DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. (1989) 28:193–213. doi: 10.1016/0165-1781(89)90047-4
47. Mollayeva, T, Thurairajah, P, Burton, K, Mollayeva, S, Shapiro, CM, and Colantonio, A. The Pittsburgh sleep quality index as a screening tool for sleep dysfunction in clinical and non-clinical samples: a systematic review and meta-analysis. Sleep Med Rev. (2016) 25:52–73. doi: 10.1016/j.smrv.2015.01.009
48. Golding, JF. Predicting individual differences in motion sickness susceptibility by questionnaire. Pers Individ Dif. (2006) 41:237–48. doi: 10.1016/j.paid.2006.01.012
49. Golding, JF. Motion sickness susceptibility. Auton Neurosci. (2006) 129:67–76. doi: 10.1016/j.autneu.2006.07.019
50. Jáuregui-Renaud, K, Gutiérrez, MA, Viveros, RL, and Villanueva, PL. Síntomas de inestabilidad corporal y enfermedad vestibular. Rev Med Instit Mex Seg Soc. (2003) 41:373–8.
51. Zigmond, AS, and Snaith, RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
52. Bjelland, I, Dahl, AA, Haug, TT, and Neckelmann, D. The validity of the hospital anxiety and depression scale. An updated literature review. J Psychosom Res. (2002) 52:69–77. doi: 10.1016/S0022-3999(01)00296-3
53. Marteau, TM, and Bekker, H. The development of a six-item short-form of the state scale of the Spielberger state-trait anxiety inventory (STAI). Br J Clin Psychol. (1992) 31:301–6. doi: 10.1111/j.2044-8260.1992.tb00997.x
54. Bayrampour, H, McDonald, S, Fung, T, and Tough, S. Reliability and validity of three shortened versions of the state anxiety inventory scale during the perinatal period. J Psychosom Obstet Gynecol. (2014) 35:101–7. doi: 10.3109/0167482x.2014.950218
55. Cox, BJ, and Swinson, RP. Instrument to assess depersonalization-derealization in panic disorder. Depress Anxiety. (2002) 15:172–5. doi: 10.1002/da.10051
56. Cohen, S, and Williamson, G. Perceived stress in a probability sample of the United States. S Spacapam and S Oskamp (eds); The social psychology of health. Newbury Park, CA: Sage (1988)
57. Baik, SH, Fox, RS, Mills, SD, Roesch, SC, Sadler, GR, Klonoff, EA, et al. Reliability and validity of the perceived stress Scale-10 in Hispanic Americans with English or Spanish language preference. J Health Psychol. (2019) 24:628–39. doi: 10.1177/1359105316684938
58. Kozhevnikov, M. Hegarty M a dissociation between object manipulation spatial ability and spatial orientation ability. Memory Cognition. (2001) 29:745–56. doi: 10.3758/BF03200477
59. Mazman, GZ, and Altun, A. Individual differences in spatial orientation performances: an eye tracking study. World J Educat Technol. (2013) 5:266–80.
60. Jacobson, GP, and Newman, CW. The development of the dizziness handicap inventory. Arch Otolaryngol Head Neck Surg. (1990) 116:424–7. doi: 10.1001/archotol.1990.01870040046011
61. Kurre, A, Bastiaenen, CH, van Gool, CJ, Gloor-Juzi, T, de Bruin, ED, and Straumann, D. Exploratory factor analysis of the dizziness handicap inventory (German version). BMC Ear Nose Throat Disord. (2010) 10:3. doi: 10.1186/1472-6815-10-3
62. Ma, HP, Ong, JR, Ou, JC, Chiang, YH, and Lian, SY. Comparison of dizziness factors for mild traumatic brain injury patients with and without dizziness: a factor analysis and propensity score model study. Comput Math Methods Med. (2021) 2021:5571319. doi: 10.1155/2021/5571319
63. Neumann, N, Fullana, MA, Radua, J, Brandt, T, Dieterich, M, and Lotze, M. Common neural correlates of vestibular stimulation and fear learning: an fMRI meta-analysis. J Neurol. (2023) 270:1843–56. doi: 10.1007/s00415-023-11568-7
64. Lyons, DM, Parker, KJ, and Schatzberg, AF. Animal models of early life stress: implications for understanding resilience. Dev Psychobiol. (2010) 52:402–10. doi: 10.1002/dev.20429
65. Okuda, S, Roozendaal, B, and McGaugh, JL. Glucocorticoid effects on object recognition memory require training-associated emotional arousal. Proc Natl Acad Sci USA. (2004) 101:853–8. doi: 10.1073/pnas.0307803100
66. Goddard, M, Zheng, Y, Darlington, CL, and Smith, PF. Monoamine transporter and enzyme expression in the medial temporal lobe and frontal cortex following chronic bilateral vestibular loss. Neurosci Lett. (2008) 437:107–10. doi: 10.1016/j.neulet.2008.03.073
67. McEwen, BS, and Chattarji, S. Molecular mechanisms of neuroplasticity and pharmacological implications: the example of tianeptine. Eur Neuropsychopharmacol. (2004) 14:S497–502. doi: 10.1016/j.euroneuro.2004.09.008
68. Gould, E, Tanapat, P, Rydel, T, and Hastings, N. Regulation of hippocampal neurogenesis in adulthood. Biol Psychiatry. (2000) 48:715–20. doi: 10.1016/S0006-3223(00)01021-0
69. Conrad, CD. What is the functional significance of chronic stress induced CA3 dendritic retraction within the hippocampus? Behav Cogn Neurosci Rev. (2006) 5:41–60. doi: 10.1177/1534582306289043
70. Popp, P, Wulff, M, Finke, K, Rühl, M, Brandt, T, and Dieterich, M. Cognitive deficits in patients with a chronic vestibular failure. J Neurol. (2017) 264:554–63. doi: 10.1007/s00415-016-8386-7
71. Anson, E, Ehrenburg, MR, Simonsick, EM, and Agrawal, Y. Association between vestibular function and rotational spatial orientation perception in older adults. J Vestib Res. (2021) 31:469–78. doi: 10.3233/VES-201582
72. Fiksdal, A, Hanlin, L, Kuras, Y, Gianferante, D, Chen, X, Thoma, MV, et al. Associations between symptoms of depression and anxiety and cortisol responses to and recovery from acute stress. Psychoneuroendocrinol. (2019) 102:44–52. doi: 10.1016/j.psyneuen.2018.11.035
73. World Health Organization (2001). Geneva, Switzerland: World Health Organization; ICF: International Classification of Functioning, Disability and Health. Available at: https://www.who.int/standards/classifications/international-classification-of-functioning-disability-and-health. Accessed on 23 February 2023.
74. Kristiansen, L, Magnussen, LH, Wilhelmsen, KT, Maeland, S, Nordahl, SHG, Hovland, A, et al. Self-reported measures have a stronger association with dizziness-related handicap compared with physical tests in persons with persistent dizziness. Front Neurol. (2022) 13:850986. doi: 10.3389/fneur.2022.850986
75. Ketola, S, Havia, M, Appelberg, B, and Kentala, E. Depressive symptoms underestimated in vertiginous patients. Otolaryngol Head Neck Surg. (2007) 137:312–5. doi: 10.1016/j.otohns.2007.03.037
76. Yang, TH, Xirasagar, S, Cheng, YF, Chen, CS, and Lin, HC. Does peripheral vestibular disorder increase the risk of attempted suicide: a retrospective cohort study. J Affective Disord. (2023) 341:12–6. doi: 10.1016/j.jad.2023.08.110
77. Grabherr, L, Cuffel, C, Guyot, JP, and Mast, FW. Mental transformation abilities in patients with unilateral and bilateral vestibular loss. Exp Brain Res. (2011) 209:205–14. doi: 10.1007/s00221-011-2535-0
78. Wraga, M, Shephard, JM, Church, JA, Inati, S, and Kosslyn, SM. Imagined rotations of self versus objects: an fMRI study. Neuropsychol. (2005) 43:1351–61. doi: 10.1016/j.neuropsychologia.2004.11.028
79. Guedry, FE, Rupert, AR, and Reschke, MF. Motion sickness and development of synergy within the spatial orientation system. A hypothetical unifying concept. Brain Res Bull. (1998) 47:475. doi: 10.1016/S0361-9230(98)00087-2
80. Katzenberger, B, Brosch, F, Besnard, S, and Grill, E. Chronic vestibular hypofunction is associated with impaired sleep: results from the dizzy Reg patient registry. J Clin Med. (2023) 12:5903. doi: 10.3390/jcm12185903
81. Robillard, R, Prince, F, Boissonneault, M, Filipini, D, and Carrier, J. Effects of increased homeostatic sleep pressure on postural control and their modulation by attentional resources. Clin Neurophysiol. (2011) 122:1771–8. doi: 10.1016/j.clinph.2011.02.010
82. Besnard, S, Tighilet, B, Chabbert, C, Hitier, M, Toulouse, J, Le Gall, A, et al. The balance of sleep: role of the vestibular sensory system. Sleep Med Rev. (2018) 42:220–8. doi: 10.1016/j.smrv.2018.09.001
83. Han, KS, Kim, L, and Shim, I. Stress and sleep disorder. Exp Neurobiol. (2012) 21:141–50. doi: 10.5607/en.2012.21.4.141
84. Yan, G, Li, F, Tao, Z, Xing, X, Zhou, Z, Wang, X, et al. Effects of vestibular damage on the sleep and expression level of orexin in the hypothalamus of rats and its correlation with autophagy and Akt tumor signal pathway. J Oncol. (2022) 2022:2514555. doi: 10.1155/2022/2514555
85. Albathi, M, and Agrawal, Y. Vestibular vertigo is associated with abnormal sleep duration. J Vestib Res. (2017) 27:127–35. doi: 10.3233/VES-170617
86. Altena, E, Buguet, E, Higginson, C, Lee, E, Douglass, A, Spitale, N, et al. Vestibular symptoms are related to the proportion of REM sleep in people with sleep complaints: a preliminary report. J Vestib Res. (2023) 33:165–72. doi: 10.3233/VES-220113
87. Sugaya, N, Arai, M, and Goto, F. The effect of vestibular rehabilitation on sleep disturbance in patients with chronic dizziness. Acta Otolaryngol. (2017) 137:275–8. doi: 10.1080/00016489.2016.1244859
88. Micarelli, A, Viziano, A, Arena, M, Misici, I, Di Benedetto, A, Carbini, V, et al. Changes in sleep performance and chronotype behaviors after vestibular rehabilitation in unilateral vestibular hypofunction. J Laryngol Otol. (2022) 137:1349–58. doi: 10.1017/S0022215122002602
Keywords: spatial anxiety, spatial orientation, stress, vestibular, handicap
Citation: Jáuregui-Renaud K, García-Jacuinde DM, Bárcenas-Olvera SP, Gresty MA and Gutiérrez-Márquez A (2024) Spatial anxiety contributes to the dizziness-related handicap of adults with peripheral vestibular disease. Front. Neurol. 15:1365745. doi: 10.3389/fneur.2024.1365745
Edited by:
Paul Smith, University of Otago, New ZealandReviewed by:
Diego Kaski, University College London, United KingdomDavid Herdman, St George’s University Hospitals NHS Foundation Trust, United Kingdom
Copyright © 2024 Jáuregui-Renaud, García-Jacuinde, Bárcenas-Olvera, Gresty and Gutiérrez-Márquez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Kathrine Jáuregui-Renaud, a2F0aHJpbmUuamF1cmVndWlAaW1zcy5nb2IubXg=