
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 16 February 2024
Sec. Sleep Disorders
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1360055
This article is part of the Research TopicSleep in Children with Rare Disorders Volume IIView all 4 articles
 Ilaria Frattale1*
Ilaria Frattale1* Rachele Sarnataro1
Rachele Sarnataro1 Martina Siracusano1,2
Martina Siracusano1,2 Assia Riccioni1
Assia Riccioni1 Cinzia Galasso1,3
Cinzia Galasso1,3 Massimiliano Valeriani3,4,5
Massimiliano Valeriani3,4,5 Giuseppina Conteduca6
Giuseppina Conteduca6 Domenico Coviello7Luigi Mazzone1,3
Domenico Coviello7Luigi Mazzone1,3 Romina Moavero3,4
Romina Moavero3,4Background: Sotos syndrome (SoS) is a rare overgrowth genetic disease caused by intragenic mutations or microdeletions of the NSD1 gene located on chromosome 5q35. SoS population might present cognitive impairment and a spectrum of behavioral characteristics, with a worse profile in patients with microdeletion. Although patients with SoS are known to have impaired sleep habits, very little data are available. The present study aimed to assess the prevalence of sleep disorders (SDs) in a pediatric cohort of patients with SoS and their correlation with neuropsychiatric profiles.
Methods: We included patients with a SoS diagnosis and age < 18 years; all patients underwent a comprehensive neuropsychological assessment, including evaluation of cognition, adaptive functions through the Adaptive Behavior Assessment System-Second Edition (ABAS-II), and behavioral problems using the Achenbach Child Behavior Checklist (CBCL) and Conners’ Parent Rating Scale-Revised (CPRS-R:L) questionnaire. To investigate the presence of SD parents, the Sleep Disturbance Scale for Children (SDSC) was completed.
Results: Thirty-eight patients (M 61%, F 39%, mean age 11.1 ± 4.65 years) were included in the study. Although only two had a prior SD diagnosis, 71.1% (N = 27) exhibited pathological scores on SDSC. No statistically significant associations were found between positive SDSC results and genetic microdeletion, intellectual disability (ID), or other medical conditions/treatments. However, a positive correlation emerged between SDSC scores and Conners’ Global Index (p = 0.048) and Restless/Impulsive (p = 0.01) scores, CBCL externalizing (p = 0.02), internalizing (p = 0.01), and total scores (p = 0.05). Conversely, a negative linear relationship was observed between the SDSC score and the ABAS GAC and ABAS CAD scores (p = 0.025).
Conclusion: We detected an SD in 71.1% of our sample, with a positive relation between SD and internalizing and externalizing symptom levels, especially hyperactivity and impulsivity. Our study demonstrated a high prevalence of SD in pediatric patients with SoS, highlighting that all patients should be screened for this problem, which has a great impact on the quality of life of patients and their families.
Sotos syndrome (SoS) is a rare overgrowth autosomal dominant syndrome with an incidence of approximately 1:14,000 live births (1). It is determined by intragenic mutations or microdeletions of the NSD1 gene (nuclear receptor set domain-containing protein 1) located on chromosome 5q35 (2); in 95% of cases, it is caused by a de novo mutation (3). Recent studies have demonstrated that NSD1 is involved in the MAPK/ERK pathway, an important regulator of cellular proliferation, differentiation, and apoptosis (4). The NSD1 gene product is expressed in several organs, including the brain, skeletal muscle, white blood cells, lung, spleen, kidney, and thymus, and it has a role in the regulation of gene transcription.
The syndrome was described for the first time in 1964 by Juan Sotos (5), but diagnostic criteria (facial features, overgrowth, and developmental delay/learning disability) were defined only later in 1994 by Cole and Hughes (6). Considering the features observed in 266 patients with mutations in the NSD1 gene, major characteristics, cardinals, and associated features were identified (Table 1).
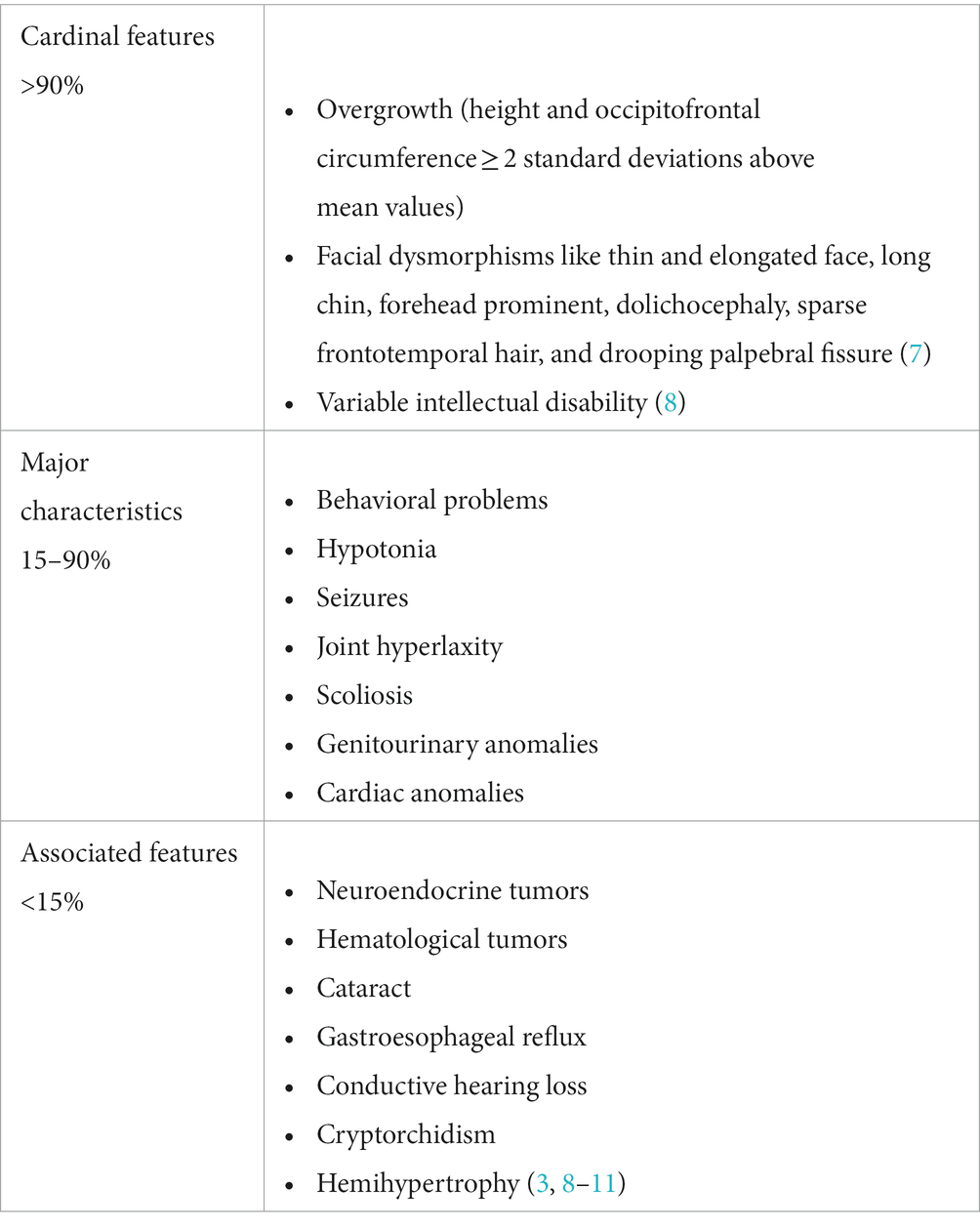
Table 1. Clinical features of SoS.
SoS population presents a heterogeneous neuropsychological profile, with possible cognitive impairment of various degrees and a spectrum of different neuropsychiatric manifestations, including autism spectrum disorder (ASD), hyperactivity (12–19), oppositive symptoms (20), separation anxiety (21), and self- and heteroaggressiveness (22). A recent study conducted by our research team on 64 patients with SoS suggested that 5q35 microdeletion is associated with a higher severity of neuropsychiatric symptoms (including cognitive skills and behavioral issues) compared to mutation (23).
Patients with SoS also present impaired sleep habits. The first information about sleep disorders was reported in 1991 by Rutter (20), but only 30 years later this problem was further investigated (24), probably due to the rarity of the syndrome and the limited number of samples to be studied.
The present study aimed to assess the prevalence of sleep disorders in a cohort of children and adolescents with SoS and evaluate a possible relationship with the behavioral symptoms.
The study involved patients who have been enrolled in the Child Neuropsychiatry Unit of Tor Vergata University Hospital of Rome. The population of this observational study is composed of SoS individuals included in a previous project conducted by our research team (23). The inclusion criteria of the present study were: a genetic diagnosis of SoS; age up to 18 years; and the availability to complete our questionnaires. In the context of our previous study (23), SoS patients underwent a complete neuropsychological standardized assessment, including cognitive intelligent quotient (IQ) evaluation through the non-verbal Leiter-R (Leiter international performance scale-revised), adaptive functioning (ABAS-II – Adaptive Behavior Assessment System-Second Edition), and parent-report behavioral questionnaire (CBCL, child behavior checklist; CPRS-R:L; Conners’ Parents Rating Scale-long form).
The Leiter-R is a standardized scale administered to children with communicational difficulties aged 2 to 20 years to evaluate their non-verbal cognitive abilities. The Leiter – R consists of 10 subtests: figure ground (FG), design analogies (DAs), form completion (FC), matching (M), sequential order (SO), repetitive pattern (RP), picture context (PC), classification (C), paper folding (PF), and figure rotation (FR), which make it possible to obtain a standardized non-verbal IQ score. In patients with more difficulties, it is possible to evaluate a brief IQ score through the FG, FC, So, and RP subtests (25).
The ABAS-II is a parent-report questionnaire available in two forms depending on the participant’s age: “0–5” and “5–21.” It provides information about the child’s adaptive functioning through the 241 parents’ answers for the “0–5″ form and 232 answers for the “5–21″ form, with scores ranging from 0 (“not able to”) to 3 (“able to do it and always performs it when needed”). The answers provide a way to define four skill domains: social (SAD), conceptual (CAD), practical (PAD), and General Adaptive Composite (GAC) scores deriving from the sum of other skill domains (26).
The typical score in the Leiter-R and ABAS-II is 100 ± 15 standard deviation, while the significant score is lower than 85.
The Achenbach Child Behavior Checklist (CBCL) is a parent-report questionnaire administrable in two forms depending on the child’s age: “18 months–5 years” and “6–18 years.” The answers provided by the parents allow us to obtain scores regarding behavioral problems and emotional symptoms using scores from 0 (not true) to 2 (often true). Considering the “18 months–5 years” form, the following areas are possible to detect: anxious/depressed, aggressive behavior, sleep problems, withdrawal, attention problems, emotional reactions, and somatic complaints. In the “6–18 years” form: withdrawn/depressed, social problems, somatic complaints, thought problems, aggressive behavior, rule-breaking behavior, anxious/depressed, and attention problems. Both forms have internalizing, externalizing, and total scores that can be considered unique scores for the statistical analysis. Considering the T-score, a behavior is considered borderline between 65 and 69, or significantly atypical, equal to or greater than 70 (27).
The Conners’ Parent Rating Scale-Revised (CPRS-R:L) is a parent-report questionnaire able to detect externalizing behavior constituted by 80 items organized in seven subscales (oppositional, social problems, anxious-shy, hyperactivity-impulsivity, perfectionism, and psychosomatic cognitive problems) (28). Total Conners’ Global Index (CGI), CGI Emotional Lability, CGI Restless-Impulsiveness, Diagnostic and Statistical Manual of Mental Disorders (DSM)-IV Total, DSM-IV Inattention, DSM-IV Hyperactive–Impulsive, and attention deficit hyperactivity disorder (ADHD) index scores are further detectable subscales (29). The T-score ranging from 61 to 69 is considered borderline, while it is significant if it is equal to or greater than 70 (28).
Parents were also asked to fill out an online survey that investigated medical comorbidities, with a focus on epilepsy and allergies, pharmacological treatment (including all neurological drugs and antihistaminics), rehabilitation therapy, instrumental examinations, and previous diagnoses of sleep disturbances.
Sleep quality was investigated through a thorough clinical history and the Sleep Disturbance Scale for Children (SDSC).
SDSC is a questionnaire validated by Bruni et al. in 1996 as a screening tool for pediatric sleep disorders. The answers to the 26 questions are converted into scores ranging from 1 to 5 depending on the frequency of the disturbance: 1 for never, 2 for occasionally, 3 for sometimes, 4 for often, and 5 for always (30).
The six most frequent types of disorder in adolescence and childhood are investigated: disorders in the initiation and maintenance of sleep (DIMS), sleep breathing disorders (SBDs), disorders of arousal (DA), sleep–wake transition disorders (SWTDs), disorders of excessive sleepiness (DOES), and night-time sweating (hyperhidrosis, SHY). The questionnaire is suggestive of sleep disturbances if the total score is equal to or greater than 39 and equal to or greater than 17 in the DIMS subscale, 7 in the SBD and SHY areas, 6 in DA, 14 in SWTD, and 13 in DOES.
Data from the clinical assessment and online survey were matched and included in a unique database for statistical analysis.
Demographical features considered for the purpose of the study were sex, age, intellectual disability (ID), genetic microdeletion, history and active epilepsy, other non-neurological comorbidities, antiseizure medication (ASM), other pharmacological treatments, and SD diagnosis.
An intellectual disability diagnosis was postulated considering the Leiter-R IQ score and the GAC score in the ABAS-II questionnaire.
The study protocol has been approved by the Ethical Committee of Tor Vergata University Hospital of Rome, Italy (#6022). All parents signed the informed consent form.
The SDSC questionnaire was proposed to the parents of 64 SoS patients enrolled in our previous project (23), with a 60% response rate and therefore a total of 38 valid questionnaires. The mean age at completion was 11.1 ± 4.65 years. Male individuals were 60.5% (n = 23). The demographic and clinical characteristics of our sample are summarized in Table 2.
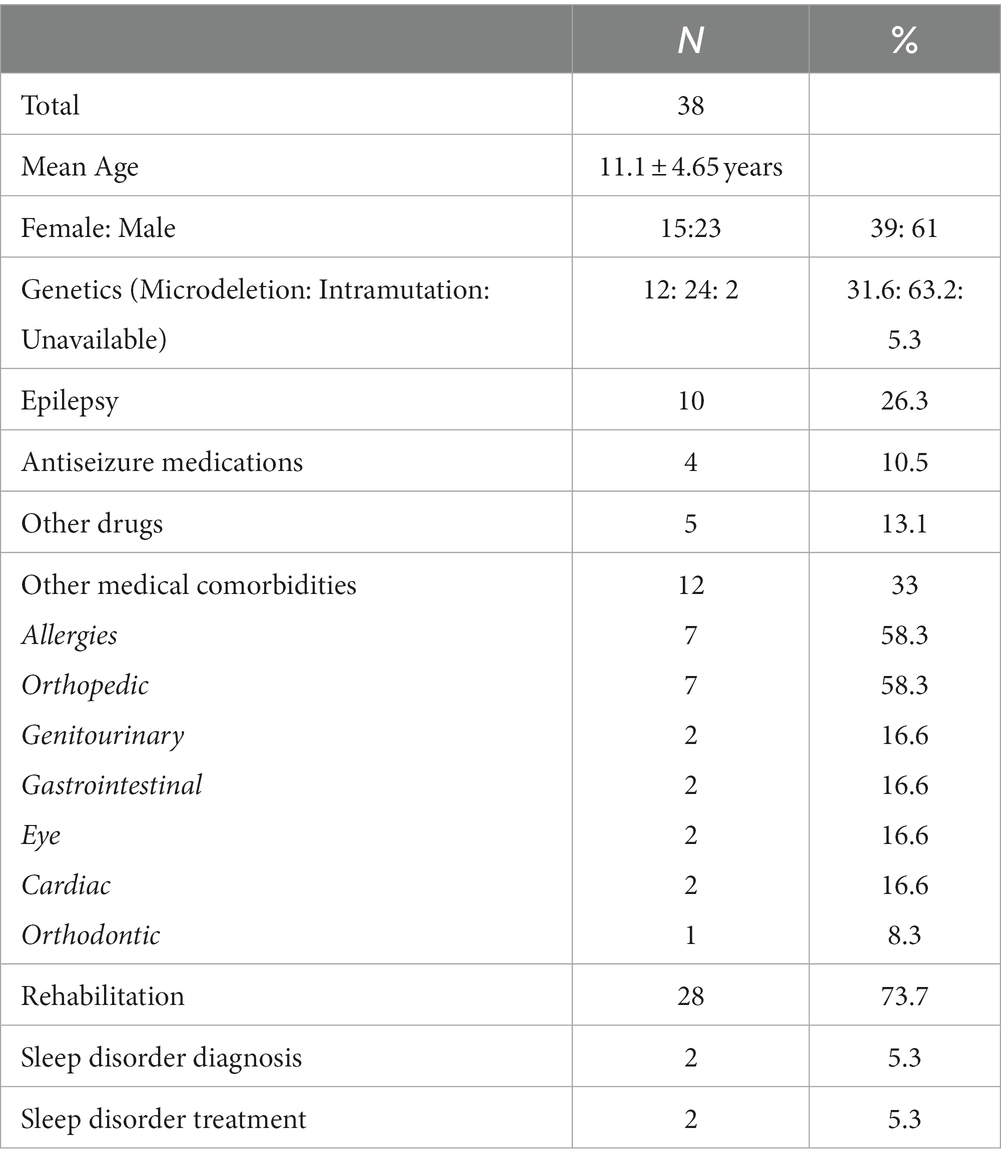
Table 2. Demographic and clinical characteristics of 38 participants.
Microdeletion of the NSD1 gene was detected in 31.6% (n = 12) of patients, while 63.2% (n = 24) presented an intragenic mutation. Genetic data were not available in 5.3% (n = 2).
Intellectual disability was diagnosed in 17 patients (44.7%). Ten patients had a history of epilepsy, of whom one had active epilepsy at the time of our evaluation (considering at least one seizure in the last year) and four were still on antiseizure medications. Among 12 individuals (31.6%), other non-neurologic medical conditions were present, with allergies (n = 7, 58.3%) being the most frequent one. Only two patients (5.3%) reported a previous diagnosis of sleep disorder.
A score above the cutoff was found in 71.1% (n = 27), and the overall mean total score was 45.2 ± 12.3 (range 28–80).
As for the subscales, 6 (15.8%) patients in the DIMS scale, 10 (26.3%) in SBD, 4 (10.5%) in DA, 10 (26.3%) in SWTD, 2 (5.2%) in DOES, and 7 (18.4%) in SHY obtained a score above the cutoff (Supplementary Figure 1).
The mean reported sleep onset latency was 15 min, while the mean total sleep time was 8–9 h.
The chi-square test did not reveal a statistically significant association between a positive score in SDSC and genetic microdeletion (p = 0.63), sex (p = 1), ID (p = 1), epilepsy history (p = 0.7), active epilepsy (p = 0.3), ASM (p = 1), other drug intakes (p = 1), rehabilitation (p = 0.4), and other non-neurological comorbidities (p = 0.4).
Twenty-nine patients (83%) achieved values above the cutoff in ABAS (mean score 68.6), 27 (84%) in CBCL (mean score 58.7), and 9 (26%) in Conners (mean score 61.6). The scores for all the subscales are reported in Table 3.
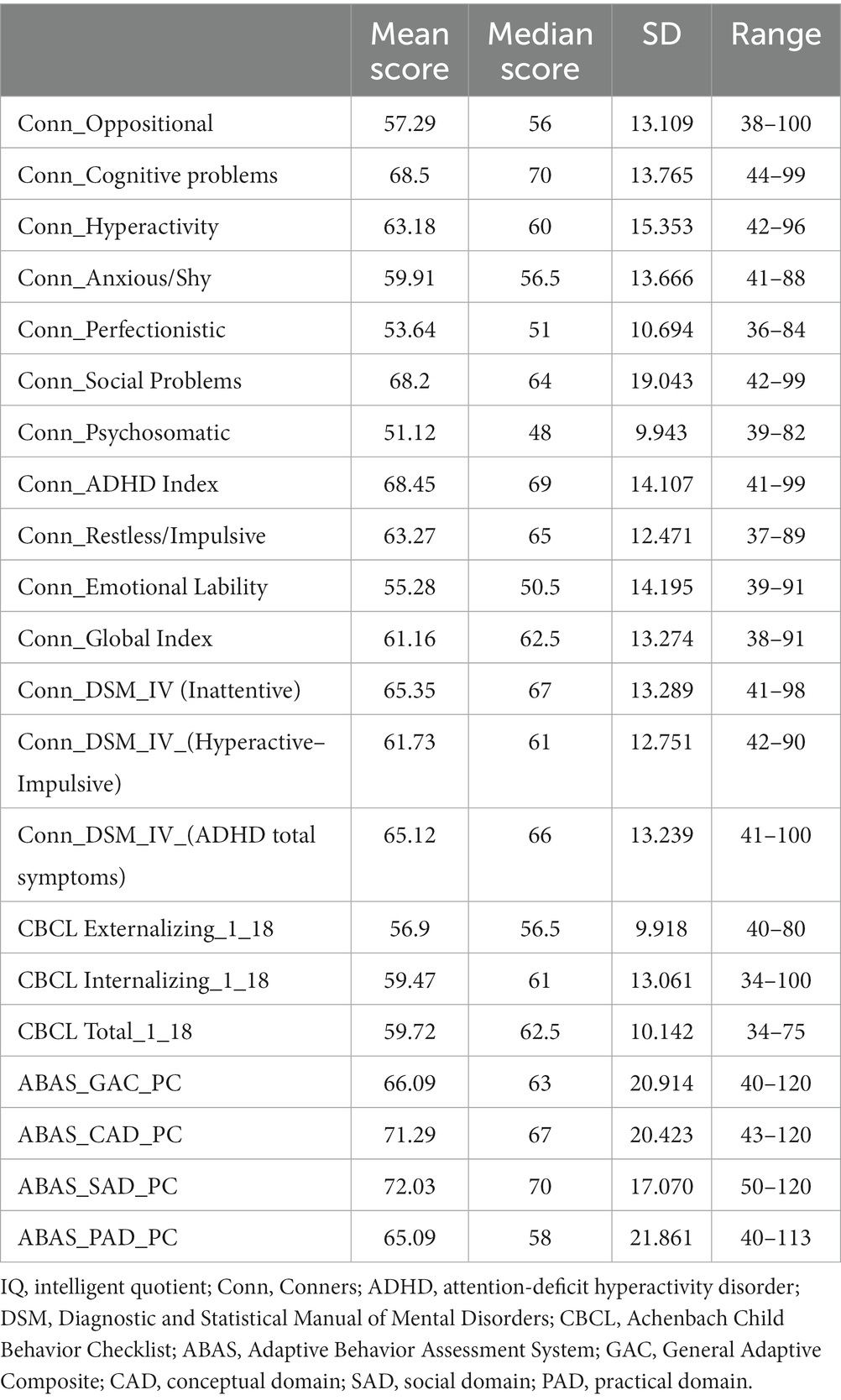
Table 3. Conners’, CBCL, and ABAS scores.
The application of a two-tailed Student’s t-test for independent samples revealed no significant differences in mean scores of Conners, CBCL, and ABAS between subjects with and without an SD (Table 4).
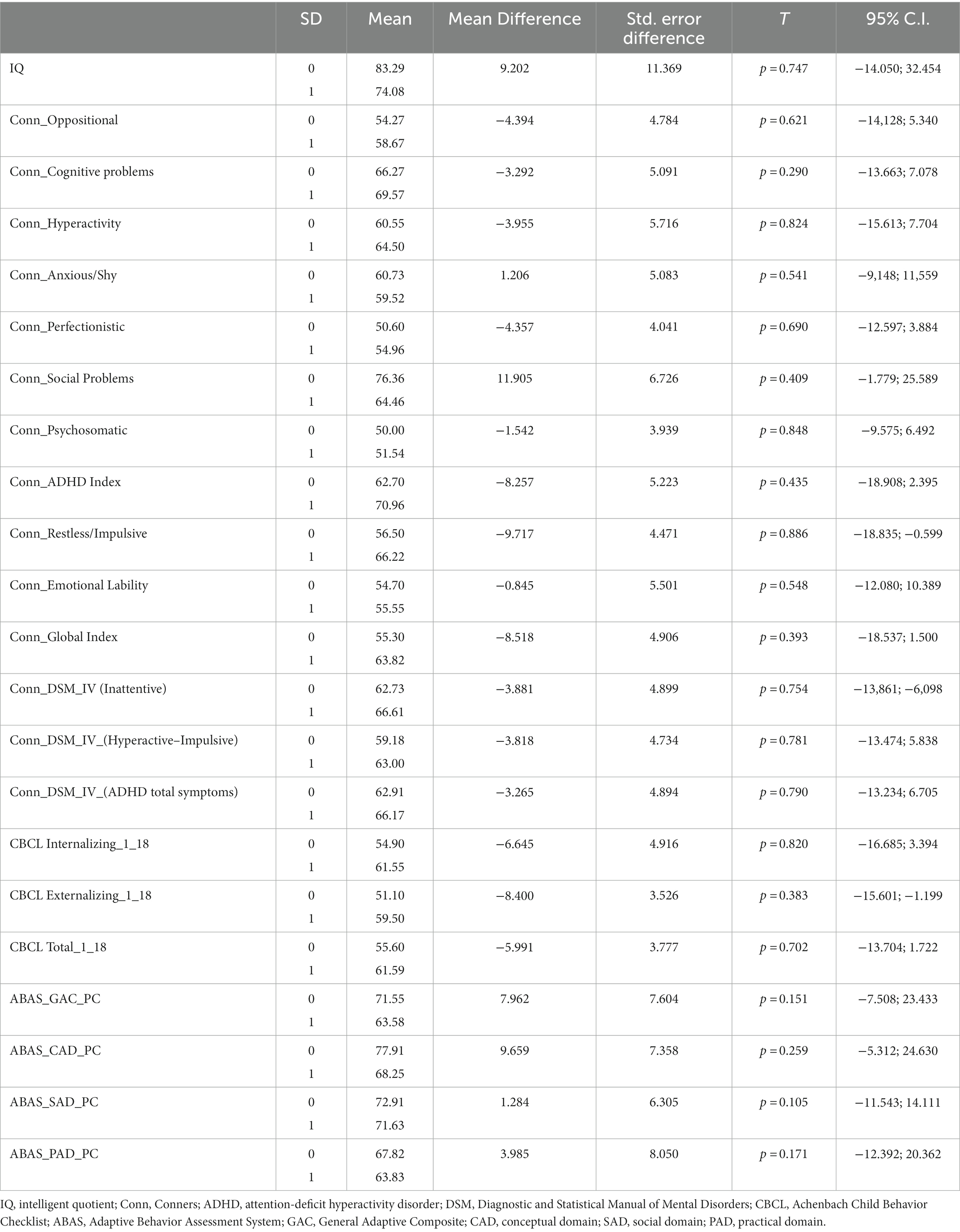
Table 4. Two-tailed Student’s t-test for independent samples.
Linear regression reveals a positive relationship between the SDSC scores and Conners’ and CBCL subscales regarding externalizing and internalizing symptoms (Conners’ CGI Total and Conners’ restless/impulsive, CBCL externalizing, internalizing, and total score). This indicates that an increase in these values is associated with an increased SDSC score. Furthermore, there is a negative linear relationship between the SDSC score and ABAS subscales.
In the logistic regression model including IQ, Conners’, CBCL’s, and ABAS’s subscale independent variables, none of them appeared to be a significant risk factor for positive SDSC. All the statistical linear regression test scores and logistic regression model scores are reported in Table 5.
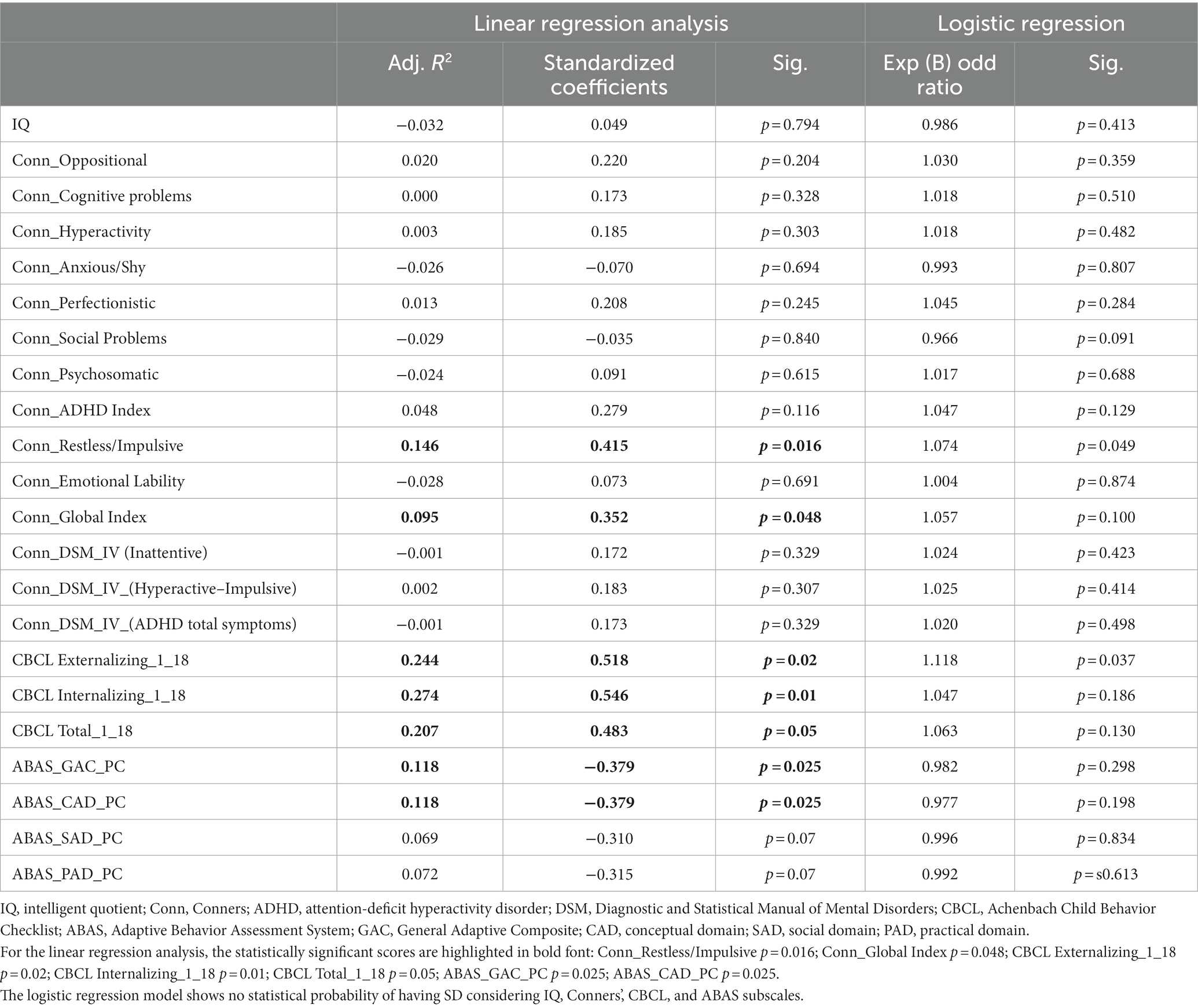
Table 5. Linear regression analysis and logistic regression model.
In our sample, we were able to detect sleep disorders in 71.1% of patients through a comprehensive collection of detailed clinical histories and the administration of the SDSC. This finding demonstrates that these disorders are much more prevalent in children and adolescents with SoS than in the general pediatric population, where the prevalence is 20–30% (31–33).
The most commonly identified sleep problems were SBD and SWTD, both occurring in 26.3%, possibly linked to the high incidence of congenital malformations of the neck and head in this population, such as general hypotonia, including weakness in the muscles of swallowing, macroglossia, high arched palates, alveolar cleft and cleft lip, and palate, which could contribute to respiratory and feeding difficulties (34). Regarding the other subscales, we observed a score above the cutoff for SHY at 18.4% and for DIMS at 15.8%.
In our sample, SD is not significantly associated with genetic microdeletion, ID, or other medical conditions and treatments.
However, the SDSC score is related to the level of internalizing and externalizing symptoms, particularly in the hyperactivity and impulsivity domains. According to our findings, better adaptive functioning is correlated with lower SDSC scores. This is noteworthy despite all the adaptive functioning scores identified with ABAS-II being significantly pathological, indicating an adaptive functioning level below the normal range.
Behavioral problems within the SoS spectrum are among the major characteristics, with a prevalence ranging from 15 to 90%, depending on the examined study group. It is important to note that, being a rare syndrome, literature data often refer to case reports or small studies.
In 1991, Rutter first described sleep problems related to early awakenings in a small sample of 11 SoS subjects (20). In a recent study, 40 patients with a mean age of 11 years (1.3–30 years) and genetic, possible, and probable diagnoses of SoS were compared with data from healthy subjects in the literature. The study showed increased resistance at bedtime, anxiety surrounding sleep, nocturnal awakenings, parasomnias, daytime sleepiness, and evidence of sleep-disordered breathing (SDB). The authors compared their population with one presenting intellectual and developmental disabilities, and they found that patients with SoS more frequently presented SBDs and parasomnias (24). These studies have certain limitations. Rutter (20) employed a non-standardized parent report. In the study conducted by Stafford et al. (24), participants with probable, possible, and genetically diagnosed SoS were included. They completed the Children’s Sleep Habits Questionnaire (CHSQ), validated for children aged 4 to 10 years, to establish a standardized parameter for all included patients, regardless of age (1.3 to 30 years old).
Sleep issues are prevalent across all stages of childhood, encompassing infants, toddlers, preschoolers, school-age children, and adolescents. During children’s brain development, sleep plays a key role, necessary for typical synaptic development and maturation of brain areas (35). Poor sleep can have significant repercussions on the cognitive side, and, due to the involvement of the prefrontal cortex, it can also lead to alterations in executive functions (36–38). It is also associated with behavioral disturbances, particularly a tendency toward externalizing disorders (39), irritability, and difficulty modulating emotions and impulses (39–41). Several studies have demonstrated the correlation between good sleep and a positive impact on future behavioral and socioemotional aspects lasting into adulthood (39, 42, 43). Chronic poor sleep habits, particularly short sleep durations, can also increase the risk of obesity and metabolic diseases (44–46). Sleep-related breathing disorders, ranging from habitual snoring to obstructive sleep apnea syndrome, can significantly affect emotional intelligence, cardiovascular functions, orofacial thrive, and the neuroendocrine and central nervous systems (47).
Furthermore, studies have shown that caregivers of patients with sleep disturbances experience high levels of distress (48–50), and stress levels improve when the child’s sleep habits improve (51, 52).
Therefore, early identification of an SD is crucial to prevent repercussions on the cognitive, emotional, and behavioral spheres, especially in a population that is genetically predisposed. It is essential to support families in managing this condition. Clinicians should specifically evaluate this aspect, as in our population, only two patients have already had a diagnosis of SD.
Our study does have some limitations. Not all patients responded to our questionnaires, and it is likely that parents of those with sleep disturbances were more likely to respond, potentially influencing the final rate of SD detected in our population. Moreover, a comprehensive physical examination of all study participants to correlate with the high prevalence of sleep disorders in SBD and SWTD areas was not feasible. Nonetheless, it is well established that the SoS phenotype encompasses head and neck malformations.
To the best of our knowledge, this is the first study attempting to correlate the presence of sleep disorders with behavioral symptoms in the pediatric SoS population. Internalizing and externalizing symptoms, especially in the hyperactivity and impulsivity domains, are directly related to more severe sleep symptoms, whereas typical adaptive behaviors are associated with milder sleep problems. Early detection of sleep disorders is crucial for enabling prompt treatment, reducing the onset of internalizing and externalizing problems, and preventing adverse impacts on the quality of life for caregivers.
Additionally, addressing behavioral symptoms may positively impact sleep, given the bidirectional connection between the two.
The high prevalence of SD in our population underscores the need to include an investigation of sleep habits and quality in the clinical evaluations of these patients to identify and manage them correctly.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethical Committee of Tor Vergata University Hospital of Rome, Italy. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements. Written informed consent was obtained from the minor(s)’ legal guardian/next of kin for the publication of any potentially identifiable images or data included in this article.
IF: Data curation, Formal analysis, Writing – original draft. RS: Investigation, Writing – review & editing. MS: Writing – review & editing. AR: Writing – review & editing. CG: Writing – review & editing. MV: Writing – review & editing. GC: Writing – review & editing. DC: Writing – review & editing. LM: Writing – review & editing. RM: Conceptualization, Data curation, Formal analysis, Supervision, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the Italian Ministry of Health with Current Research funds.
The study was conducted in collaboration with the Italian Association of Sotos Syndrome (ASSI Gulliver).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1360055/full#supplementary-material
1. Tatton-Brown, K , and Rahman, N . Clinical features of NSD1-positive Sotos syndrome. Clin Dysmorphol. (2004) 13:199–04. doi: 10.1097/00019605-200410000-00001
2. Kurotaki, N , Harada, N , Yoshiura, K , Sugano, S , Niikawa, N , and Matsumoto, N . Molecular characterization of NSD1, a human homologue of the mouse Nsd1 gene. Gene. (2001) 279:197–04. doi: 10.1016/S0378-1119(01)00750-8
3. Tatton-Brown, K , Cole, TR , and Rahman, N . Sotos Syndrome. In: MP Adam, GM Mirzaa, RA Pagon, SE Wallace, LJ Bean, and KW Gripp, et al., Gene reviews® Seattle (WA): University of Washington, Seattle (2004)
4. Kim, EK , and Choi, EJ . Pathological roles of MAPK signaling pathways in human diseases. Biochim Biophys Acta (BBA) - Mol Basis Dis. (2010) 1802:396–05. doi: 10.1016/j.bbadis.2009.12.009
5. Sotos, JF , Dodge, PR , Muirhead, D , Crawford, JD , and Talbot, NB . Cerebral gigantism in childhood: a syndrome of excessively rapid growth with Acromegalic features and a nonprogressive neurologic disorder. N Engl J Med. (1964) 271:109–16. doi: 10.1056/NEJM196407162710301
6. Cole, TR , and Hughes, HE . Sotos syndrome: a study of the diagnostic criteria and natural history. J Med Genet. (1994) 31:20–32. doi: 10.1136/jmg.31.1.20
7. Allanson, JE , and Cole, TRP . Sotos syndrome: evolution of facial phenotype subjective and objective assessment. Am J Med Genet. (1996) 65:13–20. doi: 10.1002/(SICI)1096-8628(19961002)65:1<13::AID-AJMG2>3.0.CO;2-Z
8. Tatton-Brown, K , Douglas, J , Coleman, K , Baujat, G , Cole, TRP , Das, S, et al. Genotype-phenotype associations in Sotos syndrome: an analysis of 266 individuals with NSD1 aberrations. Am J Hum Genet. (2005) 77:193–04. doi: 10.1086/432082
9. Tatton-Brown, K . Multiple mechanisms are implicated in the generation of 5q35 microdeletions in Sotos syndrome. J Med Genet. (2005) 42:307–13. doi: 10.1136/jmg.2004.027755
10. Edmondson, A , and Kalish, J . Overgrowth syndromes. J Pediatr Genet. (2015) 4:136–43. doi: 10.1055/s-0035-1564440
11. Gracia Bouthelier, R , and Lapunzina, P . Follow-up and risk of tumors in overgrowth syndromes. J Pediatr Endocrinol Metab. (2005) 18:1227–35. doi: 10.1515/JPEM.2005.18.S1.1227/html
12. Gajre, M , Mhatre, P , and Vijaykumar, R . Sotos syndrome with developmental co-ordination disorder; report of a case. J Taibah Univ Med Sci. (2014) 10:234–7. doi: 10.1016/j.jtumed.2014.05.007
13. Gosalakkal, JA . Sotos syndrome (cerebral gigantism): a review of neurobehavioral, developmental and neurological manifestations. Int Pediatr. (2004) 19:147–51.
14. Mouridsen, SE , and Hansen, MB . Neuropsychiatric aspects of Sotos syndrome. A review and two case illustrations. Eur Child Adolesc Psychiatry. (2002) 11:43–8. doi: 10.1007/s007870200007
15. Jellinek, M , Trad, PV , Schlefer, E , Hertzig, M , and Kernberg, PF . Treatment strategies for a case of concurrent pervasive developmental disorder and cerebral gigantism. J Am Acad Child Adolesc Psychiatry. (1991) 30:499–06. doi: 10.1097/00004583-199105000-00024
16. de Boer, L , Röder, I , and Wit, J . Psychosocial, cognitive, and motor functioning in patients with suspected Sotos syndrome: a comparison between patients with and without NSD1 gene alterations. Dev Med Child Neurol. (2006) 48:582–8. doi: 10.1017/S0012162206001228
17. Finegan, JAK , Cole, TRP , Kingwell, E , Smith, ML , Smith, M , and Sitarenios, G . Language and behavior in children with Sotos syndrome. J Am Acad Child Adolesc Psychiatry. (1994) 33:1307–15. doi: 10.1097/00004583-199411000-00013
18. Mauceri, L , Sorge, G , Baieli, S , Rizzo, R , Pavone, L , and Coleman, M . Aggressive behavior in patients with sotos syndrome. Pediatr Neurol. (2000) 22:64–7. doi: 10.1016/S0887-8994(99)00105-8
19. Varley, CK , and Crnic, K . Emotional, behavioral, and cognitive status of children with cerebral gigantism. J Dev Behav Pediatr JDBP. (1984) 5:132–4.
20. Rutter, SC , and Cole, TRP . Psychological characteristics of sotos syndrome. Dev Med Child Neurol. (1991) 33:898–02. doi: 10.1111/j.1469-8749.1991.tb14799.x
21. Sarimski, K . Behavioural and emotional characteristics in children with Sotos syndrome and learning disabilities. Dev Med Child Neurol. (2003) 45:172–8.
22. Sheth, K , Moss, J , Hyland, S , Stinton, C , Cole, T , and Oliver, C . The behavioral characteristics of Sotos syndrome. Am J Med Genet A. (2015) 167:2945–56. doi: 10.1002/ajmg.a.37373
23. Siracusano, M , Riccioni, A , Frattale, I , Arturi, L , Dante, C , Galasso, C, et al. Cognitive, adaptive and behavioral profile in Sotos syndrome children with 5q35 microdeletion or intragenic variants. Am J Med Genet A. (2023) 191:1836–48. doi: 10.1002/ajmg.a.63211
24. Stafford, CF , Ward, C , Ward, SLD , and Sanchez-Lara, PA . Characterization of sleep habits of children with Sotos syndrome. Am J Med Genet A. (2021) 185:2815–20. doi: 10.1002/ajmg.a.62212
25. Roid, GH , and Miller, LJ . Leiter international performance scale-revised: examiner’s manual. Roid G H and Miller L. J (Eds.), (1997). Stoelting.
26. Oakland, T . Adaptive behavior assessment system. Kreutzer J. S, de Luca J, and Caplan B (Eds.), (2011). (2nd ed.) Springer.
27. Achenbach, TM , and Rescorla, LA . Manual for the ASEBA preschool forms & profiles. (2000). University of Vermont.
28. Conners, CK , Sitarenios, G , Parker, JDA , and Epstein, JN . The revised Conners’ parent rating scale (CPRS-R): factor structure, reliability, and criterion validity. J Abnorm Child Psychol. (1998) 26:257–68. doi: 10.1023/A:1022602400621
29. Gurley, JR . Conners’ parent rating scales – revised In: S Goldstein and JA Naglieri, editors. Encyclopedia of child behavior and development. Boston, MA: Springer US (2011)
30. Bruni, O , Ottaviano, S , Guidetti, V , Romoli, M , Innocenzi, M , Cortesi, F, et al. The sleep disturbance scale for children (SDSC) construct ion and validation of an instrument to evaluate sleep disturbances in childhood and adolescence. J Sleep Res. (1996) 5:251–61. doi: 10.1111/j.1365-2869.1996.00251.x
31. Mindell, JA , Kuhn, B , Lewin, DS , Meltzer, LJ , and Sadeh, AAmerican Academy of Sleep Medicine. Behavioral treatment of bedtime problems and night wakings in infants and young children. Sleep. (2006) 29:1263–76.
32. Staples, AD , Bates, JE , and Petersen, IT . Ix. Bedtime routines in early childhood: prevalence, consistency, and associations with NIGHTTIME sleep: bedtime routines. Monogr Soc Res Child Dev. (2015) 80:141–59. doi: 10.1111/mono.12149
33. Turnbull, K , Reid, GJ , and Morton, JB . Behavioral sleep problems and their potential impact on developing executive function in children. Sleep. (2013) 36:1077–84. doi: 10.5665/sleep.2814
34. Danis, DO , Bodamer, O , and Levi, JR . The otolaryngologic manifestations of Sotos syndrome 1: a systematic review. Int J Pediatr Otorhinolaryngol. (2021) 143:110649. doi: 10.1016/j.ijporl.2021.110649
35. Hirata, I , Mohri, I , Kato-Nishimura, K , Tachibana, M , Kuwada, A , Kagitani-Shimono, K, et al. Sleep problems are more frequent and associated with problematic behaviors in preschoolers with autism spectrum disorder. Res Dev Disabil. (2016) 49-50:86–99. doi: 10.1016/j.ridd.2015.11.002
36. Bernier, A , Beauchamp, MH , Bouvette-Turcot, AA , Carlson, SM , and Carrier, J . Sleep and cognition in preschool years: specific links to executive functioning. Child Dev. (2013) 84:1542–53. doi: 10.1111/cdev.12063
37. Nelson, TD , Nelson, JM , Kidwell, KM , James, TD , and Espy, KA . Preschool sleep problems and differential associations with specific aspects of executive control in early elementary school. Dev Neuropsychol. (2015) 40:167–80. doi: 10.1080/87565641.2015.1020946
38. Sadeh, A . Consequences of sleep loss or sleep disruption in children. Sleep Med Clin. (2007) 2:513–20. doi: 10.1016/j.jsmc.2007.05.012
39. Touchette, É , Petit, D , Séguin, JR , Boivin, M , Tremblay, RE , and Montplaisir, JY . Associations between sleep duration patterns and behavioral/cognitive functioning at school entry. Sleep. (2007) 30:1213–9. doi: 10.1093/sleep/30.9.1213
40. Ednick, M , Cohen, AP , McPhail, GL , Beebe, D , Simakajornboon, N , and Amin, RS . A review of the effects of sleep during the first year of life on cognitive, psychomotor, and temperament development. Sleep. (2009) 32:1449–58. doi: 10.1093/sleep/32.11.1449
41. Scharf, RJ , Demmer, RT , Silver, EJ , and Stein, REK . Nighttime sleep duration and externalizing behaviors of preschool children. J Dev Behav Pediatr. (2013) 34:384–91. doi: 10.1097/DBP.0b013e31829a7a0d
42. Hale, L , Berger, LM , LeBourgeois, MK , and Brooks-Gunn, J . A longitudinal study of preschoolers’ language-based bedtime routines, sleep duration, and well-being. J Fam Psychol. (2011) 25:423–33. doi: 10.1037/a0023564
43. Wong, MM , Brower, KJ , and Zucker, RA . Childhood sleep problems, early onset of substance use and behavioral problems in adolescence. Sleep Med. (2009) 10:787–96. doi: 10.1016/j.sleep.2008.06.015
44. Knutson, KL . Does inadequate sleep play a role in vulnerability to obesity? Am J Hum Biol. (2012) 24:361–71. doi: 10.1002/ajhb.22219
45. Leproult, R , and Van Cauter, E . Role of sleep and sleep loss in hormonal release and metabolism In: S Loche, M Cappa, L Ghizzoni, M Maghnie, and MO Savage, editors. Endocrine Development (2010) 17:11–21. doi: 10.1159/000262524
46. Miller, MA , Kruisbrink, M , Wallace, J , Ji, C , and Cappuccio, FP . Sleep duration and incidence of obesity in infants, children, and adolescents: a systematic review and meta-analysis of prospective studies. Sleep. (2018) 41. doi: 10.1093/sleep/zsy018/4833233
47. Operto, FF , Precenzano, F , Bitetti, I , Lanzara, V , Fontana, ML , Pastorino, GMG, et al. Emotional intelligence in children with severe sleep-related breathing disorders. Behav Neurol. (2019) 2019:1–6. doi: 10.1155/2019/6530539
48. Schlieber, M , and Han, J . The role of sleep in young Children’s development: a review. J Genet Psychol. (2021) 182:205–17. doi: 10.1080/00221325.2021.1908218
49. Hiscock, H , and Wake, M . Infant sleep problems and postnatal depression: a community-based study. Pediatrics. (2001) 107:1317–22. doi: 10.1542/peds.107.6.1317
50. Meltzer, LJ , and Mindell, JA . Relationship between child sleep disturbances and maternal sleep, mood, and parenting stress: a pilot study. J Fam Psychol. (2007) 21:67–73. doi: 10.1037/0893-3200.21.1.67
51. Hiscock, H , Bayer, J , Gold, L , Hampton, A , Ukoumunne, OC , and Wake, M . Improving infant sleep and maternal mental health: a cluster randomised trial. Arch Dis Child. (2007) 92:952–8. doi: 10.1136/adc.2006.099812
Keywords: sleep, genetics, behavior, Sotos syndrome, children, pediatrics
Citation: Frattale I, Sarnataro R, Siracusano M, Riccioni A, Galasso C, Valeriani M, Conteduca G, Coviello D, Mazzone L and Moavero R (2024) Sleep disturbances and behavioral symptoms in pediatric Sotos syndrome. Front. Neurol. 15:1360055. doi: 10.3389/fneur.2024.1360055
Edited by:
Karen Spruyt, Institut National de la Santé et de la Recherche Médicale (INSERM), FranceReviewed by:
Montida Veeravigrom, The University of Chicago, United StatesCopyright © 2024 Frattale, Sarnataro, Siracusano, Riccioni, Galasso, Valeriani, Conteduca, Coviello, Mazzone and Moavero. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ilaria Frattale, aWxhcmlhZnJhdHRhbGVAbGliZXJvLml0
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.