
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol. , 09 May 2024
Sec. Neurorehabilitation
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1359091
 Ignazio Leale1,2,3*
Ignazio Leale1,2,3* Vincenzo Di Stefano4
Vincenzo Di Stefano4 Carola Costanza5
Carola Costanza5 Filippo Brighina4
Filippo Brighina4 Michele Roccella3
Michele Roccella3 Antonio Palma1,3
Antonio Palma1,3 Giuseppe Battaglia1,3,6
Giuseppe Battaglia1,3,6Introduction: Charcot–Marie–Tooth disease (CMT) is an inherited neuropathy that affects the sensory and motor nerves. It can be considered the most common neuromuscular disease, with a prevalence of 1/2500.
Methods: Considering the absence of a specific medical treatment and the benefits shown by physical activity in this population, a systematic review was completed using several search engines (Scopus, PubMed, and Web of Science) to analyze the use, effectiveness, and safety of a training program performed in telecoaching (TC). TC is a new training mode that uses mobile devices and digital technology to ensure remote access to training.
Results: Of the 382 studies identified, only 7 met the inclusion criteria. The effects of a TC training program included improvements in strength, cardiovascular ability, and functional abilities, as well as gait and fatigue. However, the quality of the studies was moderate, the size of the participants in each study was small, and the outcome measured was partial.
Discussion: Although many studies have identified statistically significant changes following the administration of the TC training protocol, further studies are needed, with appropriate study power, better quality, and a higher sample size.
CMT also named hereditary motor and sensory neuropathy (HMSN) (1), encompasses a heterogeneous set of disorders affecting peripheral nerves. CMT is the most common inherited neuromuscular disorder with an estimated prevalence of 1 in 2500 (2, 3), caused by mutations in more than 80 genes (4, 5). In this disease, the most common subtypes are CMT1A, CMT1X, hereditary neuropathy with a predisposition to pressure paralysis (HNPP), CMT1B and CMT2A. The other identified subtypes represent less than 1% (6). CMT1 is characterized by a slow conduction speed in the motor nerves caused by a high demyelination process. According to Latour, the CMT1A is the most common form (76%), followed by CMT1X (11%), CMT1B (6%), and CMT1C (<6%) (7). CMT2 is characterized by a mutation in the MFN2 gene, which causes axonal neuropathy with onset in childhood. In general, patients with CMT show a high genetic heterogeneity but with a relatively homogeneous clinical component. Clinically the main symptoms include distal weakness, muscle atrophy, loss of proprioception, sensory loss, reduced reflexes, and skeletal deformities such as hollow foot (8, 9). The combination of these symptoms causes in patients an altered gait associated with difficulty in balance (10–13). It has also been shown that patients with CMT have anxiety and depression problems (14) with alteration of body composition (15) and low levels of physical activity (PA) (14, 16–18). A sedentary lifestyle increases body weight, muscle loss, and musculoskeletal pain, worsening the medical case of patients with CMT (19); this condition increases the risk of comorbidities such as metabolic syndrome or cardiovascular disease (20). The optimization of body composition profiles should be one of the main objectives to be achieved in patients with CMT. In fact, in these patients, a strong relationship between lean mass and physical functionality has been demonstrated (15). In addition, reduced fat mass is related to improved quality of life and reduced symptoms (15).
The current absence of specific medical treatment for several neurological diseases (21), and the need for new evidence for the use of drugs (22) emphasizes the importance of developing sustainable PA programs (8). Indeed, physical exercise might be an effective tool to improve quality of life and improve lifestyle in these patients, as well as slowing the progression of the disease. In particular, aerobic exercises, resistance training, and stretching appear to be the main training methods for CMT patients (23). However, it could be challenging to investigate new types of exercise in these patients, considering the potential benefits of PA but the difficulties in its practice in this population (24). Therefore, this systematic review aims to analyze the effectiveness and safety of TC training programs for CMT patients. Physical exercise in TC involves the use of technological and digital tools, such as computers and mobile devices, to remotely access training content (25).
Physical exercise in TC may be useful to reverse the sedentary lifestyle of CMT patients, allowing them to gain greater autonomy and independence, and improving their quality of life.
This systematic review was developed based on the favored reporting items for systematic reviews and meta-analyses (PRISMA) guidelines (26). The studies were selected through a database screening, such as PubMed (NLM) Web of Science (TS), and Scopus. The following keywords have been included to identify the articles: exercise, physical activity, telecoaching, tele-coaching, Charcot–Marie-Tooth, aerobic training, resistance training, and training. Terms were included in three different groups. In Group A the terms “telecoaching” and “tele-coaching” were inserted, in Group B the terms “exercise,” “physical activity,” “aerobic training,” “resistance training” and “training” were inserted. Finally, in Group C has been inserted the “Charcot–Marie-Tooth” term. To analyze the groups, Boolean operators “AND” and “OR” were used. Examples of matching included: Charcot–Marie-Tooth AND aerobic training OR telecoaching; resistance training AND Charcot–Marie-Tooth. All the founded articles were transferred into the Endnote software (Vers. X20 for Windows 11, © Thomson Reuters).
All studies that have the following criteria were included in this systematic review: (1) original research with full text written in the English language; (2) all study designs different than reviews, meta-analyses, letters to editors, and theses; (3) studies with training protocol in TC for patients with CMT. No gender differences between males and females were used for exclusion criteria. Articles from gray literature have not been investigated. The PICOS approach (Population, Intervention, Comparator, Outcomes, Study design) is explained in Table 1.
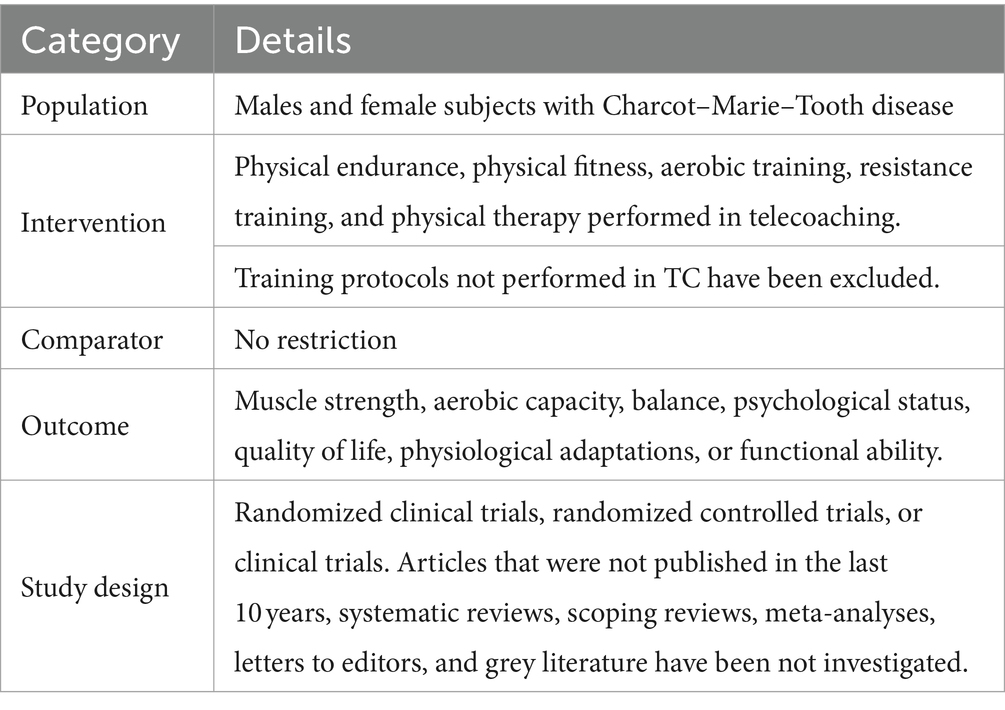
Table 1. Inclusion criteria according to the PICOS approach.
The identification and elimination of duplicate studies were carried out by a single researcher. Subsequently, two authors analyzed independently the articles. Initially, the authors analyzed the title and abstracts of each study. Secondly the authors analyzed the full text to assess whether the selected studies agreed with the criteria of inclusion and exclusion.
The two authors discussed any dispute regarding their decisions; if the two authors did not agree on the inclusion or exclusion of a study, a third auditor was consulted. A Microsoft Excel spreadsheet (Microsoft Corp, Redmond, Washington) was used to report the following information related to the included studies: year of publication, sample age, gender, the aim of the study, and the TC protocol.
Two authors evaluated the quality and bias of all the studies included in this review, using a modified version of the checklist to measure the quality of RCTs and not RCTs written by Downs and Black (27). In the modified version of the checklist, item 27 (power) was changed from 0 to 5 to a score of 0–1, so that a study would receive a score of 0 in case the statistical power was below 80%, a score of 1 if the statistical power was above 80% (28). As a result, the final checklist score changed from 32 to 28. The quality of the studies was divided into four levels: excellent (26–28), good (20–25), fair (15–19), and poor (<14) (29, 30). The authors’ results were compared by an external researcher and discrepancies were resolved in a consensus meeting.
A total of 382 studies were identified through electronic databases. The titles and abstracts of 199 studies were analyzed after removing 183 duplicates. The full text of 17 studies has been examined of which only 7 articles agree with the inclusion and exclusion criteria. The PRISMA flowchart shows the entire selection process (Figure 1).
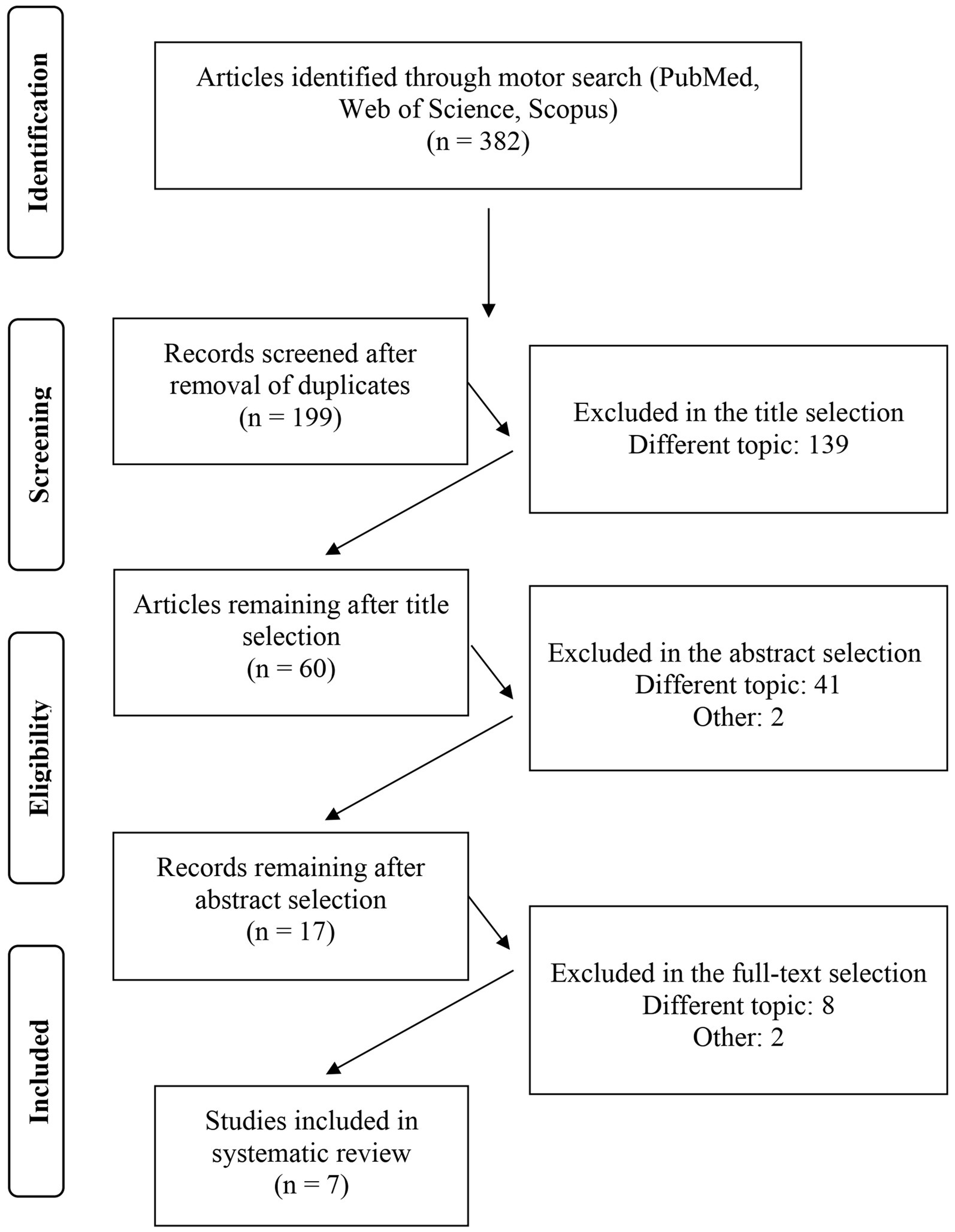
Figure 1. Flow diagram representing the selection process of manuscripts.
In detail, of the 7 included studies, 5 analyzed the effectiveness of a resistance training protocol in patients with CMT (31–35), while 2 studies analyzed the effectiveness of an interval training protocol on this target population (36, 37).
A total of 170 patients with CMT were included in this review with an age between 11 and 45 years. Of the 7 studies, it is possible to identify two studies of El Mhandi et al. (36, 37) that included only male participants. The other five studies included both male and female participants. More detailed information on each study can be found in Table 2.
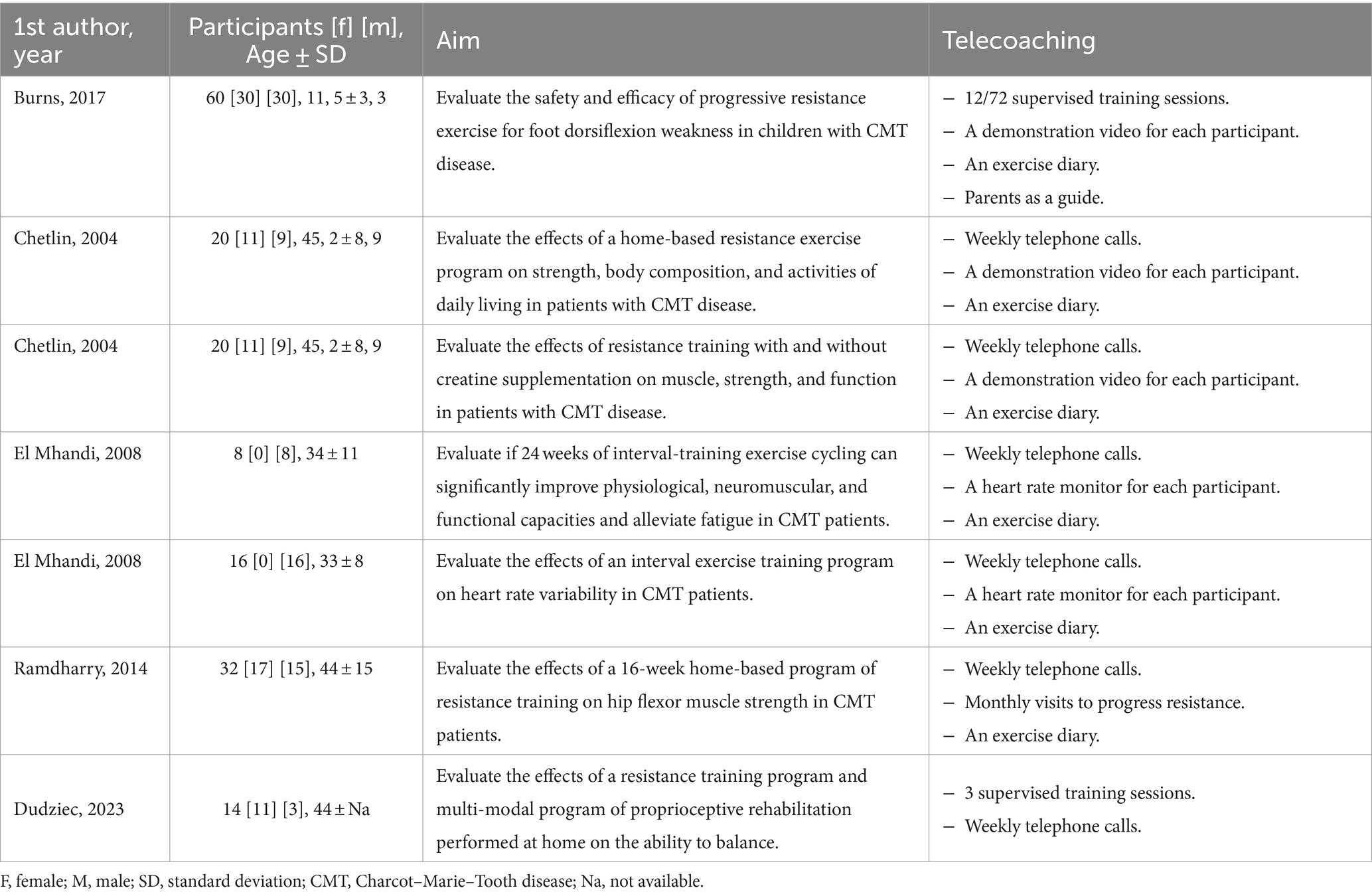
Table 2. The aim of the manuscripts and relative characteristics of the sample.
The methodological quality of the included studies was analyzed using the modified version of the Downs and Black checklist. Out of 7 studies, 1 study was evaluated as “good quality” (34), 3 studies as “fair quality” (31, 33, 35), and 3 studies were evaluated as “poor quality” studies (32, 36, 37). Some items of Downs and Black are difficult to use in studies with physical activity protocol, such as the use of a study design in double-blind.
Of the extrapolated studies, five used a TC resistance training protocol in patients with CMT (31–34). Among these, there is the study of Burns and colleagues (31); a randomized, double-blind, sham-controlled trial, in which the experimental group performed a TC training resistance exercise, while the control group performed a fictitious workout. The treatment team was the only one who knew about group assignment; participants, parents, caregivers, clinical evaluators, and other investigators were not informed of the group allocation. The experimental group, consisting of children, had performed a TC training program that aimed to improve the weakness in the dorsiflexion of the foot. Participants were trained using an adjustable ankle bracelet, designed to prevent slipping, three times a week or non-consecutive days, for 6 months with a protocol that provided an initial intensity of 50% and a progressive increase of up to 70% of one repetition maximum (1RM). The control group trained with the same procedure, including the same equipment, the same duration, the same frequency, the same series, and repetitions. However, the participants trained with a very low intensity, never exceeding 10% 1RM. Each parent was asked to help the child with the application of the bracelet and to supervise the training performed in TC. TC included the compilation of an exercise diary, the delivery of a video to be used as a familiarization, and the active participation of parents as a guide, as well as the execution of some supervised training sessions. The results indicated that after a 24-week intervention period, the experimental group had reduced the long-term progression of dorsiflexion weakness without side effects on muscle morphology; there were no signs of overwork fatigue. It has been shown that a TC training program is safe, valid, and effective in a pediatric population affected by CMT disease. A drop-out of 5 patients was detected, demonstrating high adherence to the training mode. Also Chetlin’s study (34) used a home-based resistance training program, for 12 weeks. This study aimed to evaluate the efficacy of resistance training with and without creatine supplementation on muscle strength and activities of daily living (ADL) in patients with CMT disease. ADL included getting up from the chair without using your arms, getting up from a supine position, and going up and down the stairs. The subjects were also timed while performing a lifting and moving test. Each test was performed from 3 to 6 times. In detail, 20 patients with CMT consumed 5 g/day creatine or placebo, while participating in a resistance training program. Resistance training consisted of 12 weeks of exercise performed in TC, divided into three phases (each phase of 4 weeks) with the amount of work increased systematically by adjusting the resistance or repetitions for each of the phases. For example, hand-grip exercises consisted of 3 sets of 4 repetitions, three times per week, with a 1-min rest period between each set. If the subjects failed to perform the number of repetitions, they used a lower resistance to complete the required program. More details can be found in Table 3. TC included the delivery of videos describing in detail the training techniques as well as supervised training sessions in which subjects knew the exercises to be performed.
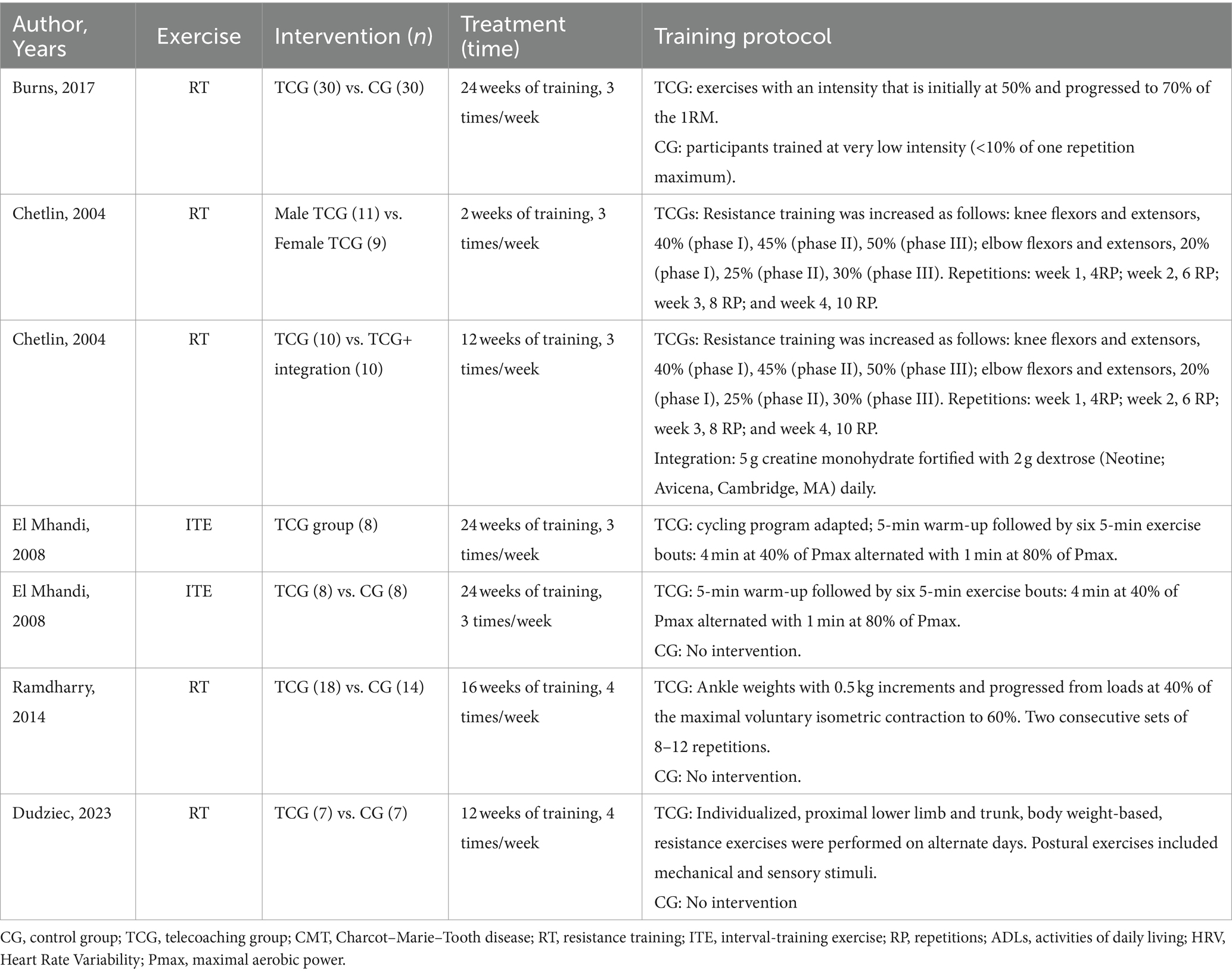
Table 3. Type of treatment and protocol in telecoaching.
The results indicated that for both groups, the type I muscle fiber diameter, and strength, were improved as well as the ADL. Overall, patients with CMT respond to resistance training performed in TC with muscle fiber adaptations, and with improvements in strength, and in the ADL. However, the use of Creatine was not beneficial. No drop-out has been detected.
The same research design has been applied by Chetlin and colleagues (32) to determine the effectiveness of a TC resistance training program on body composition, strength, and function of daily activities in men and women with CMT. The women’s group consisted of 11 participants while the men’s group of 9. At baseline, women had a normal percentage of strength (80%) in 4 out of 10 measurements, while men did not reach 80% of normal force in any measure. After resistance training, women reached 80% of normal strength in 8 out of 10 measurements, while men in 1 measurement. The functions of daily activities were improved after training without gender differences; moreover, men had significantly more fat-free mass (p < 0.05) before and after training compared to women.
Ramdharry and colleagues (33) used a randomized single-blind crossover design to assess the effectiveness of a physical exercise in TC on hip flexor muscle strength. Randomization was used to assign the subjects to one of two groups: group A with initial training, and group B with initial control period. The training protocol conformed with the guidelines of the American College of Sports Medicine (ACSM) and provided 16 weeks of training with 4 weekly training (38). Weights were used, positioned in the ankle, with periodic increments of 0.5 kg and oscillation from 40 to 60% of the maximum voluntary isometric contraction (MVC). Participants performed 2 sets of 8–12 repetitions, 4 days a week for 16 weeks. The exercise was performed in the supine position with load displacement from 10° in hip extension to 45° in hip flexion. After a period of familiarization, patients were monitored through an exercise diary, weekly phone calls, and monthly visits to improve protocol adherence. The results showed a significant increase in the strength of the hip flexor muscles to the left but not to the right, demonstrating that the resistance training was well-tolerated without evidence of weakness from overload. In addition, no drop-out was recorded, indicating high compliance with this training mode.
Finally, Dudziec and colleagues (35) used TC training protocol to assess the effectiveness of resistance training and multisensory balance training, delivered at home, on the ability to balance in patients with CMT. 14 patients were randomized into two groups: the TC group performed 12 weeks of strength training and multisensory balance; the control group performed the daily activities. The results showed high adherence to this training modality with 93% of patients completing the study. Posturography tests showed improvement in postural stability in favor of the intervention group, and the ability to balance and gait showed an improved elevated in the TC group. In the same group, partial improvements have been shown in the strength of the lower limbs.
Only two of the studies analyzed have used a TC protocol of interval training. El Mhandi and colleagues (37) have used this training program to assess if 24 weeks of interval training cycles could significantly improve physiological, neuromuscular, and functional abilities, as well as alleviate the perception of fatigue in patients with CMT. The training program included 24 weeks of training of which 12 were supervised and 12 telecoaching-independently at home. The single training session was 45 min and included 5 min of warm-up, 30 min of the middle phase, and 10 min of cool-down. No stretching activity was foreseen. The central phase consisted of 6 exercises of 5 min, of which 4 min at 40% of the maximum aerobic power (Pmax) and 1 min at 80% of Pmax. The exercise was made on stationary cycloergometers. TC period was performed with the same protocol, although several personal cycloergometers were used by subjects in their homes. Subjects were motivated and checked by weekly phone calls. The training period was well tolerated; no subjects reported adverse events or complications during the protocol. The results showed significant improvements in cardiorespiratory abilities, functional ability, and isokinetic strength, as well as in the scale of pain and fatigue during training. Also, benefits obtained at the end of the supervised period were maintained after the home period. However, the results also revealed that there was no effect on the production of isometric strength and indices of fatigue resistance after training.
The same training protocol was applied by El Mhandi and colleagues (36) to assess the effectiveness of interval training on heart rate variability (HRV) in patients with CMT. An experimental group and a healthy control group were included in this study. The HRV assessment was conducted at the baseline (T0) and the end of the 24-week study period (T1); in both evaluations, subjects were monitored through 24-h Holter electrocardiographic (ECG). The results showed that at the baseline all HRV indices of the experimental group were lower than the control group with a statistically significant difference for the pNN50 parameter. After the training program, the researchers found improvement in some time and frequency parameters in the experimental group; in some cases, the values of the experimental group at T1 exceeded the values of the control group at baseline (+8% mean R–R interval, +95% pNN50, 52% reduction in low/high-frequency ratio). These results suggest that interval training might improve dysautonomia in CMT, improving the activity of the parasympathetic nervous system.
The present review aimed to analyze the effectiveness of TC programs in patients with CMT disease. The topic is innovative and punctual, but there are still few studies in the literature. It has been found that this modality of exercise training can determine significant improvements in motor strength, functional abilities, heart rate variability, activities of daily life, as well as cardiorespiratory ability. However, due to the low number of randomized controlled trials, the low quality of the studies, the reduced number of participants within each training protocol, and the limited evidence of pre-post differences, the true effectiveness of TC in CMT disease remains unclear. Most of the studies analyzed examined the effectiveness of a TC resistance training program, showing positive changes in the indices of strength and muscle weakness, associating them with an increase in physiological abilities, neuromuscular and functional. Similarly, interval training showed significant improvements in HRV and the perception of fatigue, as well as an increase in cardiovascular ability.
In detail, Burns and colleagues (31) showed that 6 months of resistance training in TC preserved the strength of the dorsiflexion in the children; while over the weeks, likewise of an adult with CMT (39, 40), children have produced through resistance training, an overall gain of strength of 5% compared to a deterioration of 23% for the sedentary children, reflecting the normal course of the disease (41). Although creatine has not involved any more significant changes, the improvements induced by the training protocol of Chetlin and colleagues (32, 34), show the effectiveness of the TC training mode. The results obtained could be the result of muscle adaptation induced by resistance training. Indeed, post-workout, a hypertrophy of type 1 fibers was found, a condition consistent with what happens in healthy people after high-volume training (42). However, subjects with CMT are not able to train at the same intensities recommended for healthy sedentary subjects (8–12 repetitions to exhaustion or 67–80% of maximum strength) (43). Considering that the high intensity of training is associated with a decrease in performance and an increased risk of injury in patients with neuromuscular diseases (44), CMT patients needed to perform more repetitions, with less intensity, to equalize the recommended training volume. About creatine, it has been shown that oral intake increases muscle levels of creatine and phosphocreatine in healthy subjects, improving performance and post-exercise recovery (45–47). In detail, subjects who increase creatine levels by 17–30% get the biggest increases (48), while those who increase by 5% do not get any performance improvement (49). Conversely, although the initial levels of creatine are within the reference values for subjects with neuropathy (50), the lack of benefits induced by taking it might be caused by a low percentage of intake (5%).
Not increasing muscle creatine concentration in patients with CMT may be caused by the non-compliant use of the supplement or an alteration of the creatine transporter. Future studies could analyze the correct functioning of the creatine transporter in patients with CMT.
Moreover, the study by Ramdharry and colleagues (33), showed contrasting results, demonstrating a modest improvement in hip strength, but only to the left side. Overall, resistance training performed in TC would seem beneficial for this population, even if in the programming phase it should be considered that the muscles of CMT subjects do not physiologically respond to the training session due to chronic denervation (51). In addition, the sedentary lifestyle of CMT patients may be the cause of the improvements achieved by resistance training evidenced in other studies, as seen in healthy subjects (52); hence, it could be useful to extend the protocol administration period. Also, the protocol of El Mhandi and colleagues (36, 37) of interval training performed in TC was an effective strategy, aligning with other studies that demonstrate the effectiveness of regular and progressive dynamic activity in neuromuscular diseases (53–56). The numerous positive results obtained show that the program developed by researchers is perfectly in line with the needs and abilities of patients with CMT. A program that requires high functional abilities may be difficult to integrate into the daily routine, demotivating patients and causing a high risk of abandonment (57). A physical activity program should consider this aspect, especially if executed in TC; indeed, it has been shown that poor motivation becomes an obstacle to exercise for both the patient and the healthcare professional (58, 59). Moreover, recruitment is one of the main problems of studies conducted on CMT (60), because many patients with neuromuscular diseases do not undertake a physical activity program for lack of motivation and difficulties in shifts and logistics. Indeed, only one of the studies in this review has analyzed the sample size to ensure sufficient power in its study, to detect a statistically significant effect (33); the remaining studies did not use any reference to sample power. From this perspective, TC could be a training mode that helps this population by offering a practical and attainable approach. In addition, physical exercise in TC for patients with CMT should consider the age of participants. All studies included recruited adult participants with an average age of 40 years, except for the study conducted by Burnsand colleagues (31), in which participants were children between the ages of 6 and 17 years and an average age of 11.5 years. The age of the participants could influence both recruitment and results obtained; it is more likely that the main benefits induced by physical exercise in TC, are obtained at the disease onset, therefore in the early stages of the disease when the clinical burden is limited, and chronic complications have still not overcome.
A training program performed in TC has already been used in many other target populations, resulting in effective and risk-free (61, 62). From the analysis of these studies, it is possible to observe the main strengths and limitations of this new training approach. Indeed, the execution of physical exercise in TC has several advantages, among these we can identify the reduction of economic resources, the reduction of geographical limits, the freedom to train when you want as well as the possibility of training in a family environment and safe. In addition, this mode increases the autonomy and independence of the patient. However, TC has also negative factors, including social isolation, loss of contact between coach and patient, the high risk of abandonment, and the difficulty for the patient to understand the right execution technique of the exercises.
For these aspects, physical exercise in TC requires telecoaches flexible and available to every need of the patient, constant weekly calls in order to supervise and control the progress of the exercise as well as an initial familiarization in order to learn and improve the execution of the exercises. Moreover, to optimize the effectiveness of this training modality, could be useful to provide each patient a clear and concise digital material that explains in detail the exercises to be performed, such as demo videos. Another important tool could be an exercise diary, in which to record when the training is carried out and any personal considerations in order to optimize PA.
Overall, this systematic review has found consistent results regarding the effectiveness and safety of a training protocol performed in TC, resulting in free of adverse events, with high adherence to the training mode and effective on all the variables analyzed. However, due to the low number of randomized controlled trials, the low quality of the studies, the reduced number of participants within each training protocol, and the limited evidence of pre-post differences, the true effectiveness of TC in CMT disease is still unclear. The TC training intervention allows researchers to develop new research strategies. Considering this, a multicenter study project involving a larger number of subjects could be the main intervention strategy to reduce these limits.
Further research is needed to verify the real benefits of a training protocol in TC and to organize and detail the training parameters such as volume, intensity, and density.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
IL: Conceptualization, Formal analysis, Methodology, Writing – original draft. VS: Conceptualization, Formal analysis, Methodology, Writing – original draft. CC: Formal analysis, Writing – original draft. FB: Supervision, Writing – review & editing. MR: Writing – review & editing. AP: Supervision, Writing – review & editing. GB: Conceptualization, Methodology, Supervision, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Dyck, PJ, and Lambert, EH. Lower motor and primary sensory neuron diseases with peroneal muscular atrophy: I. Neurologic, genetic, and Electrophysiologic findings in hereditary polyneuropathies. Arch Neurol. (1968) 18:603–18. doi: 10.1001/archneur.1968.00470360025002
2. Saporta, MA, and Shy, ME. Inherited peripheral neuropathies. Neurol Clin. (2013) 31:597–619. doi: 10.1016/j.ncl.2013.01.009
3. Barreto, LC, Oliveira, FS, Nunes, PS, de França Costa, IMP, Garcez, CA, Goes, GM, et al. Epidemiologic study of Charcot-Marie-tooth disease: a systematic review. Neuroepidemiology. (2016) 46:157–65. doi: 10.1159/000443706
4. Braathen, GJ. Genetic epidemiology of Charcot–Marie–tooth disease. Acta Neurol Scand. (2012) 126:iv–22. doi: 10.1111/ane.12013
5. Frasquet, M, Rojas-García, R, Argente-Escrig, H, Vázquez-Costa, JF, Muelas, N, Vílchez, JJ, et al. Distal hereditary motor neuropathies: mutation spectrum and genotype–phenotype correlation. Eur J Neurol. (2021) 28:1334–43. doi: 10.1111/ene.14700
6. Saporta, AS, Sottile, SL, Miller, LJ, Feely, SME, Siskind, CE, and Shy, ME. Charcot-Marie-tooth disease subtypes and genetic testing strategies. Ann Neurol. (2011) 69:22–33. doi: 10.1002/ana.22166
7. Latour, P, Gonnaud, PM, Ollagnon, E, Chan, V, Perelman, S, Stojkovic, T, et al. SIMPLE mutation analysis in dominant demyelinating Charcot-Marie-tooth disease: three novel mutations. J Peripher Nerv Syst. (2006) 11:148–55. doi: 10.1111/j.1085-9489.2006.00080.x
8. Pareyson, D, and Marchesi, C. Diagnosis, natural history, and management of Charcot-Marie-tooth disease. Lancet Neurol. (2009) 8:654–67. doi: 10.1016/S1474-4422(09)70110-3
9. Reilly, MM, and Shy, ME. Diagnosis and new treatments in genetic neuropathies. J Neurol Neurosurg Psychiatry. (2009) 80:1304–14. doi: 10.1136/jnnp.2008.158295
10. Ong, CF, Geijtenbeek, T, Hicks, JL, and Delp, SL. Predicting gait adaptations due to ankle plantarflexor muscle weakness and contracture using physics-based musculoskeletal simulations. PLoS Comput Biol. (2019) 15:e1006993. doi: 10.1371/journal.pcbi.1006993
11. The Cochrane CollaborationSackley, C, Disler, PB, Turner-Stokes, L, Wade, DT, Brittle, N, et al. Rehabilitation interventions for foot drop in neuromuscular disease. Cochrane Database Syst Rev. (2009) 3:Cd003908. doi: 10.1002/14651858.CD003908.pub3,
12. Kennedy, RA, McGinley, JL, Paterson, KL, Ryan, MM, and Carroll, K. Gait and footwear in children and adolescents with Charcot-Marie-tooth disease: a cross-sectional, case-controlled study. Gait Posture. (2018) 62:262–7. doi: 10.1016/j.gaitpost.2018.03.029
13. Kennedy, RA, Carroll, K, Hepworth, G, Paterson, KL, Ryan, MM, and McGinley, JL. Falls in paediatric Charcot-Marie-tooth disease: a 6-month prospective cohort study. Arch Dis Child. (2019) 104:535–40. doi: 10.1136/archdischild-2018-314890
14. Thomas, FP, Saporta, MA, Attarian, S, Sevilla, T, Sivera, R, Fabrizi, GM, et al. Patient-reported symptom burden of Charcot-Marie-tooth disease type 1A: findings from an observational digital lifestyle study. J Clin Neuromuscul Dis. (2022) 24:7–17. doi: 10.1097/CND.0000000000000426
15. Hackett, D, Roberts-Clarke, D, Jain, N, Mavros, Y, Wilson, GC, Halaki, M, et al. Body composition and its association with physical performance, quality of life, and clinical indictors in Charcot-Marie-tooth disease: a pilot study. Disabil Rehabil. (2019) 41:405–12. doi: 10.1080/09638288.2017.1395083
16. Kennedy, RA, Carroll, K, Paterson, KL, Ryan, MM, Burns, J, Rose, K, et al. Physical activity of children and adolescents with Charcot-Marie-tooth neuropathies: a cross-sectional case-controlled study. PLoS One. (2019) 14:e0209628. doi: 10.1371/journal.pone.0209628
17. di Stefano, V, Battaglia, G, Giustino, V, Gagliardo, A, D’Aleo, M, Giannini, O, et al. Significant reduction of physical activity in patients with neuromuscular disease during COVID-19 pandemic: the long-term consequences of quarantine. J Neurol. (2021) 268:20–6. doi: 10.1007/s00415-020-10064-6
18. Leale, I, Giustino, V, Trapani, P, Alonge, P, Rini, N, Cutrò, I, et al. Physical activity in patients with neuromuscular disease three years after COVID-19, a longitudinal survey: the after-effects of the quarantine and the benefits of a return to a healthier life-style. J Clin Med. (2024) 13:265. doi: 10.3390/jcm13010265
19. Tremblay, MS, Colley, RC, Saunders, TJ, Healy, GN, and Owen, N. Physiological and health implications of a sedentary lifestyle. Appl Physiol Nutr Metab. (2010) 35:725–40. doi: 10.1139/H10-079
20. Aitkens, S, Kilmer, DD, Wright, NC, and McCrory, MA. Metabolic syndrome in neuromuscular disease. Arch Phys Med Rehabil. (2005) 86:1030–6. doi: 10.1016/j.apmr.2004.09.012
21. Pareyson, D, Saveri, P, and Pisciotta, C. New developments in Charcot-Marie-Tooth neuropathy and related diseases. Curr Opin Neurol. (2017) 30:471–80. doi: 10.1097/WCO.0000000000000474
22. di Stefano, V, Thomas, E, Alonge, P, Giustino, V, Pillitteri, G, Leale, I, et al. Patisiran enhances muscle mass after nine months of treatment in ATTRv amyloidosis: a study with bioelectrical impedance analysis and handgrip strength. Biomedicines. (2023) 11:62. doi: 10.3390/biomedicines11010062
23. Sman, AD, Hackett, D, Fiatarone Singh, M, Fornusek, C, Menezes, MP, and Burns, J. Systematic review of exercise for Charcot-Marie-tooth disease. J Peripher Nerv Syst. (2015) 20:347–62. doi: 10.1111/jns.12116
24. Menotti, F, Felici, F, Damiani, A, Mangiola, F, Vannicelli, R, and Macaluso, A. Charcot-Marie-tooth 1A patients with low level of impairment have a higher energy cost of walking than healthy individuals. Neuromuscul Disord. (2011) 21:52–7. doi: 10.1016/j.nmd.2010.09.008
25. Colorado-State-University. (2016). Telecoaching emerges as tool in nutrition and medicine. Available at: https://source.colostate.edu/telecoaching-emerges-as-tool-in-nutrition-and-medicine/.
26. Shamseer, L, Moher, D, Clarke, M, Ghersi, D, Liberati, A, Petticrew, M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ. (2015) 349:g7647. doi: 10.1136/bmj.g7647
27. Downs, SH, and Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J Epidemiol Community Health. (1998) 52:377–84. doi: 10.1136/jech.52.6.377
28. Chuter, V, Spink, M, Searle, A, and Ho, A. The effectiveness of shoe insoles for the prevention and treatment of low back pain: a systematic review and meta-analysis of randomised controlled trials. BMC Musculoskelet Disord. (2014) 15:140. doi: 10.1186/1471-2474-15-140
29. Pas, HI, Reurink, G, Tol, JL, Weir, A, Winters, M, and Moen, MH. Efficacy of rehabilitation (lengthening) exercises, platelet-rich plasma injections, and other conservative interventions in acute hamstring injuries: an updated systematic review and meta-analysis. Br J Sports Med. (2015) 49:1197–205. doi: 10.1136/bjsports-2015-094879
30. Hooper, P, Jutai, JW, Strong, G, and Russell-Minda, E. Age-related macular degeneration and low-vision rehabilitation: a systematic review. Can J Ophthalmol. (2008) 43:180–7. doi: 10.3129/i08-001
31. Burns, J, Sman, AD, Cornett, KMD, Wojciechowski, E, Walker, T, Menezes, MP, et al. Safety and efficacy of progressive resistance exercise for Charcot-Marie-tooth disease in children: a randomised, double-blind, sham-controlled trial. Lancet Child Adolesc Health. (2017) 1:106–13. doi: 10.1016/S2352-4642(17)30013-5
32. Chetlin, RD, Gutmann, L, Tarnopolsky, M, Ullrich, IH, and Yeater, RA. Resistance training effectiveness in patients with Charcot-Marie-tooth disease: recommendations for exercise prescription. Arch Phys Med Rehabil. (2004) 85:1217–23. doi: 10.1016/j.apmr.2003.12.025
33. Ramdharry, GM, Pollard, A, Anderson, C, Laurá, M, Murphy, SM, Dudziec, M, et al. A pilot study of proximal strength training in Charcot-Marie-tooth disease. J Peripher Nerv Syst. (2014) 19:328–32. doi: 10.1111/jns.12100
34. Chetlin, RD, Gutmann, L, Tarnopolsky, MA, Ullrich, IH, and Yeater, RA. Resistance training exercise and creatine in patients with Charcot-Marie-tooth disease. Muscle Nerve. (2004) 30:69–76. doi: 10.1002/mus.20078
35. Dudziec, MM, Lee, LE, Massey, C, Tropman, D, Skorupinska, M, Laurá, M, et al. Home-based multi-sensory and proximal strengthening program to improve balance in Charcot-Marie-tooth disease type 1A: a proof of concept study. Muscle Nerve. (2024) 69:354–61. doi: 10.1002/mus.28032
36. El Mhandi, L, Pichot, V, Calmels, P, Gautheron, V, Roche, F, and Féasson, L. Exercise training improves autonomic profiles in patients with Charcot-Marie-tooth disease. Muscle Nerve. (2011) 44:732–6. doi: 10.1002/mus.22150
37. El Mhandi, L, Millet, GY, Calmels, P, Richard, A, Oullion, R, Gautheron, V, et al. Benefits of interval-training on fatigue and functional capacities in Charcot-Marie-tooth disease. Muscle Nerve. (2008) 37:601–10. doi: 10.1002/mus.20959
38. ACMs Medicine. ACSM's guidelines for exercise testing and prescription. Baltimore, MD: Lippincott Williams and Wilkins (2009).
39. Lindeman, E, Leffers, P, Spaans, F, Drukker, J, Reulen, J, Kerckhoffs, M, et al. Strength training in patients with myotonic dystrophy and hereditary motor and sensory neuropathy: a randomized clinical trial. Arch Phys Med Rehabil. (1995) 76:612–20. doi: 10.1016/S0003-9993(95)80629-6
40. Smith, CA, Chetlin, RD, Gutmann, L, Yeater, RA, and Alway, SE. Effects of exercise and creatine on myosin heavy chain isoform composition in patients with Charcot-Marie-tooth disease. Muscle Nerve. (2006) 34:586–94. doi: 10.1002/mus.20621
41. Burns, J, Ouvrier, R, Estilow, T, Shy, R, Laurá, M, Pallant, JF, et al. Validation of the Charcot-Marie-tooth disease pediatric scale as an outcome measure of disability. Ann Neurol. (2012) 71:642–52. doi: 10.1002/ana.23572
42. Taaffe, DR, Pruitt, L, Pyka, G, Guido, D, and Marcus, R. Comparative effects of high- and low-intensity resistance training on thigh muscle strength, fiber area, and tissue composition in elderly women. Clin Physiol. (1996) 16:381–92. doi: 10.1111/j.1475-097X.1996.tb00727.x
43. American College of Sports Medicine Position Stand. The recommended quantity and quality of exercise for developing and maintaining cardiorespiratory and muscular fitness, and flexibility in healthy adults. Med Sci Sports Exerc. (1998) 30:975–91. doi: 10.1249/00005768-199806000-00032
44. Kilmer, DD. Response to resistive strengthening exercise training in humans with neuromuscular disease. Am J Phys Med Rehabil. (2002) 81:S121–6. doi: 10.1097/00002060-200211001-00013
45. Wang, CC, Fang, CC, Lee, YH, Yang, MT, and Chan, KH. Effects of 4-week Creatine supplementation combined with complex training on muscle damage and sport performance. Nutrients. (2018) 10:1640. doi: 10.3390/nu10111640
46. Wax, B, Kerksick, CM, Jagim, AR, Mayo, JJ, Lyons, BC, and Kreider, RB. Creatine for exercise and sports performance, with recovery considerations for healthy populations. Nutrients. (2021) 13:1915. doi: 10.3390/nu13061915
47. Hall, M, Manetta, E, and Tupper, K. Creatine supplementation: an update. Curr Sports Med Rep. (2021) 20:338–44. doi: 10.1249/JSR.0000000000000863
48. Persky, AM, and Brazeau, GA. Clinical pharmacology of the dietary supplement creatine monohydrate. Pharmacol Rev. (2001) 53:161–76. doi: 10.1124/pharmrev1
49. Greenhaff, PL. Creatine and its application as an ergogenic aid. Int J Sport Nutr. (1995) 5:S100–10. doi: 10.1123/ijsn.5.s1.s100
50. Tarnopolsky, MA, and Parise, G. Direct measurement of high-energy phosphate compounds in patients with neuromuscular disease. Muscle Nerve. (1999) 22:1228–33. doi: 10.1002/(SICI)1097-4598(199909)22:9<1228::AID-MUS9>3.0.CO;2-6
51. Lewis, RA, Li, J, Fuerst, DR, Shy, ME, and Krajewski, K. Motor unit number estimate of distal and proximal muscles in Charcot-Marie-tooth disease. Muscle Nerve. (2003) 28:161–7. doi: 10.1002/mus.10419
52. Deschenes, MR, and Kraemer, WJ. Performance and physiologic adaptations to resistance training. Am J Phys Med Rehabil. (2002) 81:S3–S16. doi: 10.1097/00002060-200211001-00003
53. Florence, JM, and Hagberg, JM. Effect of training on the exercise responses of neuromuscular disease patients. Med Sci Sports Exerc. (1984) 16:460–5. doi: 10.1249/00005768-198410000-00007
54. Wright, NC, Kilmer, DD, McCrory, MA, Aitkens, SG, Holcomb, BJ, and Bernauer, EM. Aerobic walking in slowly progressive neuromuscular disease: effect of a 12-week program. Arch Phys Med Rehabil. (1996) 77:64–9. doi: 10.1016/S0003-9993(96)90222-1
55. Voorn, EL, Koopman, FS, Nollet, F, and Brehm, MA. Individualized aerobic exercise in neuromuscular diseases: a pilot study on the feasibility and preliminary effectiveness to improve physical fitness. Phys Ther. (2021) 101:pzaa213. doi: 10.1093/ptj/pzaa213
56. Oorschot, S, Brehm, MA, van Groenestijn, AC, Koopman, FS, Verhamme, C, Eftimov, F, et al. Efficacy of a physical activity programme combining individualized aerobic exercise and coaching to improve physical fitness in neuromuscular diseases (I'M FINE): study protocol of a randomized controlled trial. BMC Neurol. (2020) 20:184. doi: 10.1186/s12883-020-01725-0
57. Bakker, M, Schipper, K, Koopman, FS, Nollet, F, and Abma, TA. Experiences and perspectives of patients with post-polio syndrome and therapists with exercise and cognitive behavioural therapy. BMC Neurol. (2016) 16:23. doi: 10.1186/s12883-016-0544-0
58. Phillips, M, Flemming, N, and Tsintzas, K. An exploratory study of physical activity and perceived barriers to exercise in ambulant people with neuromuscular disease compared with unaffected controls. Clin Rehabil. (2009) 23:746–55. doi: 10.1177/0269215509334838
59. Voorn, EL, Koopman, F, Nollet, F, and Brehm, MA. Aerobic exercise in adult neuromuscular rehabilitation: a survey of healthcare professionals. J Rehabil Med. (2019) 51:518–24. doi: 10.2340/16501977-2567
60. Abresch, RT, Carter, GT, Han, JJ, and McDonald, CM. Exercise in neuromuscular diseases. Phys Med Rehabil Clin N Am. (2012) 23:653–73. doi: 10.1016/j.pmr.2012.06.001
61. de Vasconcelos, HCA, Lira Neto, JCG, de Araújo, MFM, Carvalho, GCN, de Souza Teixeira, CR, de Freitas, RWJF, et al. Telecoaching programme for type 2 diabetes control: a randomised clinical trial. Br J Nurs. (2018) 27:1115–20. doi: 10.12968/bjon.2018.27.19.1115
62. Snoek, JA, Meindersma, EP, Prins, LF, van’t Hof, AWJ, de Boer, MJ, Hopman, MT, et al. The sustained effects of extending cardiac rehabilitation with a six-month telemonitoring and telecoaching programme on fitness, quality of life, cardiovascular risk factors and care utilisation in CAD patients: the TeleCaRe study. J Telemed Telecare. (2021) 27:473–83. doi: 10.1177/1357633X19885793
Keywords: Charcot-Marie-Tooth, adapted physical activity, telecoaching, exercise, neuropathy
Citation: Leale I, Di Stefano V, Costanza C, Brighina F, Roccella M, Palma A and Battaglia G (2024) Telecoaching: a potential new training model for Charcot-Marie-Tooth patients: a systematic review. Front. Neurol. 15:1359091. doi: 10.3389/fneur.2024.1359091
Edited by:
Andrea Martinuzzi, Eugenio Medea (IRCCS), ItalyReviewed by:
Luca Leonardi, Sapienza University of Rome, ItalyCopyright © 2024 Leale, Di Stefano, Costanza, Brighina, Roccella, Palma and Battaglia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ignazio Leale, aWduYXppby5sZWFsZUB1bmlwYS5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.