 Glaucia Suzanna Jong-A-Liem1,2
Glaucia Suzanna Jong-A-Liem1,2 Talita Helena Martins Sarti1,2Mariusi Glasenapp dos Santos3Luciano Marcus Tirotti Giacon4
Talita Helena Martins Sarti1,2Mariusi Glasenapp dos Santos3Luciano Marcus Tirotti Giacon4 Raphael Wuo-Silva1Alex Machado Baeta5
Raphael Wuo-Silva1Alex Machado Baeta5 José Maria de Campos Filho2
José Maria de Campos Filho2 Feres Chaddad-Neto1,2*
Feres Chaddad-Neto1,2*- 1Department of Neurology and Neurosurgery, Universidade Federal de São Paulo, São Paulo, SP, Brazil
- 2Department of Neurosurgery, Hospital Beneficência Portuguesa de São Paulo, São Paulo, SP, Brazil
- 3Department of Neurosurgery, Universidade Federal de Santa Maria, Santa Maria, RS, Brazil
- 4Department of Neuroradiology, Hospital Beneficência Portuguesa de São Paulo, São Paulo, SP, Brazil
- 5Department of Neurology, Hospital Beneficência Portuguesa de São Paulo, São Paulo, SP, Brazil
Introduction: Mutations of the phosphatase and tensin homolog (PTEN) gene have been associated with a spectrum of disorders called PTEN hamartoma tumor syndrome, which predisposes the individual to develop various types of tumors and vascular anomalies. Its phenotypic spectrum includes Cowden syndrome (CS), Bannayan–Riley–Ruvalcaba syndrome (BRRS), Proteus syndrome, autism spectrum disorders (ASD), some sporadic cancers, Lhermitte–Duclos disease (LDD), and various types of associated vascular anomalies.
Clinical presentation: A previously healthy 27-year-old woman was experiencing visual scintillating scotomas and mild chronic headaches for the past 2 years. The initial computed tomographic (CT) and magnetic resonance imaging (MRI) scans did not reveal any abnormalities, but the possibility of pseudotumor cerebri was considered. Furthermore, a cerebral angiogram showed a posterior fossa dural arteriovenous fistula (dAVF), which was initially treated through embolization. However, in spite of proper treatment, this patient experienced multiple recurrent dAVFs in different locations, requiring multiple embolizations and surgeries. Despite exhibiting altered cerebral perfusion and hemodynamics, the patient did not display any significant symptoms until she experienced a sudden stroke resulting from deep venous thrombosis, which was not associated with any medical procedures or medication use. A comprehensive analysis was performed due to the aggressive nature of the dAVFs. Surprisingly, exome sequencing of a blood sample revealed a PTEN gene variant in chromosome 10, indicative of Cowden syndrome. However, no tumors or other vascular lesions were detected in other systems that would constitute Cowden syndrome.
Conclusion: The rapid formation of multiple and complex dAVFs, coupled with not meeting the criteria for any other PTEN-related syndrome, unequivocally leads to the presentation of a novel phenotype of the PTEN germline variant.
1 Introduction
The phosphatase and tensin homolog (PTEN) gene is a tumor suppressor gene that inhibits the PI3K/AKT/mTOR and vascular endothelial growth factor (VEGF) signaling pathways, which control cell growth, migration, apoptosis, and angiogenesis (1). Mutations of this gene have been associated with a spectrum of disorders called PTEN hamartoma tumor syndrome and predisposes the individual with the syndrome to develop various types of tumors and vascular anomalies. As this gene is expressed in almost all tissues and cell types, this condition usually involves multiple systems and, therefore, neurological anomalies are quite common.
These PTEN germline mutations are very rare, and their phenotypic spectrum includes Cowden syndrome (CS), Bannayan–Riley–Ruvalcaba syndrome (BRRS), Proteus syndrome, autism spectrum disorders (ASD), some sporadic cancers, Lhermitte–Duclos disease (LDD), and various types of vascular anomalies (2).
This case report, therefore, presents a novel phenotypic expression of the PTEN gene in a previously healthy adult with multiple and complex multiple dural arteriovenous fistulas (dAVFs).
2 Clinical presentation
A 27-year-old female lawyer was experiencing visual scintillating scotomas and subtle chronic headaches for the last 2 years. The patient had no comorbidities, no family history of cancer syndromes, and did not use continuous medication. An ophthalmologic investigation revealed her condition to be bilateral papilledema and the patient was referred to a neurologist. The initial computed tomographic (CT) and magnetic resonance imaging (MRI) scans were normal and raised the possibility of pseudotumor cerebri, which required supplemental analysis with digital subtracted angiography (DSA). In this examination, a dural arteriovenous fistula (dAVF) was detected in the posterior fossa, which was successfully embolized, resulting in occlusion without complications. The patient was discharged with no acquired deficit (mRS 1).
After 1 year, the headaches reoccurred, and the patient was readmitted. In DSA, a new and highly complex dAVF was detected in the supratentorial region, affecting meningeal branches of the external carotid artery, the meningohypophyseal trunk, the ascending pharyngeal and occipital arteries, and both transverse sinuses near the Torcula and superficial cortical veins (Figure 1). Therefore, she underwent a new session of embolization without any complications and was discharged without headaches (mRS 1).
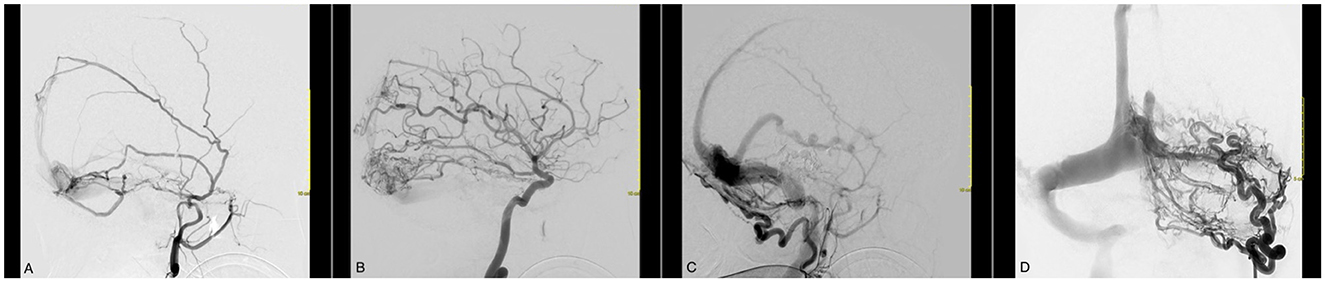
Figure 1. Cerebral angiography with a selective left external carotid artery (ECA) catheterization evidencing an AVF between branches of the external carotid artery and the superficial venous system. Venous congestion and reflux are evident in the Labbe vein and up until the posterior third of the superior sagittal sinus. (A) The meningeal branches of ECA in fistulous communication with the superior sagittal sinus and transverse sinus. (B) The cortical branches of the ICA in fistulous communication with the superior sagittal and transverse sinus. (C, D) A very enlarged occipital artery with multiple branches in fistulous communication with the transverse and sigmoid sinus.
Again, 1 month later, she was readmitted for the third time due to the emergence of a new symptom: tinnitus. A new DSA procedure revealed the presence of a new cortical dAVF in the patient, which was treated with another session of embolization without any complications. The patient was discharged and recovered from the tinnitus but continued to experience a mild headache. As the dAVF pattern changed and symptoms worsened over time, the patient underwent a fourth session of embolization after 3 months and a fifth session after 6 months for the same reasons.
Following the completion of the fifth session, the magnetic resonance angiography (MRA) analysis revealed the continued presence of multiple and intricate dAVFs. These dAVFs were supplied by arteries stemming from the right middle meningeal artery, right internal maxillary artery, and occipital artery (Figure 2). Additionally, these dAVFs were directly linked to the right transverse, sigmoid sinus, straight sinus, superior petrosal sinus, and superior sagittal sinus, all of which showed arterial flow. Furthermore, the deep venous drainage, medullary, and cortical veins exhibited signs of venous congestion and indirect indications of brain swelling.
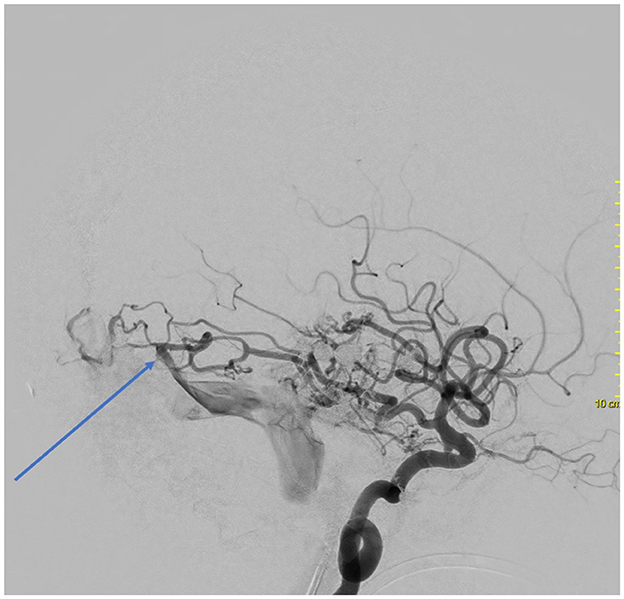
Figure 2. Cerebral angiography with a selective left internal carotid artery catheterization evidencing an AVF between branches of the posterior cerebral artery and the Labbe vein.
Therefore, the patient underwent a ventriculoperitoneal (VP) shunt with an initial threshold of 150 mmHg. The surgery was uneventful, and the patient was discharged with minor symptoms.
The patient suffered a generalized seizure and fell into a coma during a routine neuroimaging check-up 2 months later. New CT scans revealed a small infarct in the left frontal region with indications of hemorrhagic transformation. MR angiography and venography tests showed tortuous and partial thrombosis in the following veins: the right basal vein of Rosenthal, the sylvian superficial vein, the frontobasal vein, and the right internal jugular bulb. Despite the VP shunt being in the correct position, there were still signs of increased intracranial pressure (ICP).
The patient was kept under sedation for neuroprotection and presented with multiple neurological complications secondary to the mass cerebral venous thrombosis. Despite prolonged periods of anticoagulation therapy, she remained in a comatose condition. A new MRI evidenced the persistence of extensive brain swelling and ischemic parenchymal injury. Given the aggressiveness of the dAVFs and the poor outcome, the patient underwent rheumatologic, immunologic, hematologic, and genetic investigations. The first of these investigations was unremarkable. However, the genetic exome sequencing of her blood sample revealed a pathological variant in the PTEN gene compatible to Cowden syndrome. The patient underwent a full-body screening, which did not reveal any tumors or other vascular lesions in other systems.
The patient's family provided informed consent to publish this case, which was also authorized by the hospital's ethics committee.
3 Discussion
The most common neurological phenotypic expressions associated with the PTEN germline mutation manifest as follows.
Macrocephaly is a common finding (80%) in CS and happens to be 100% present in BRRS (3, 4). Lynch et al. studied BRRS in six children with extreme macrocephaly. Four parents of these children also carried the PTEN mutation and asymptomatic extreme macrocephaly as well (3). Hence, we affirm that macrocephaly of idiopathic cause can be an early marker for PTEN mutation-linked disorders (5). Developmental delay is also typical and associated with the macrocephalic finding. Children and adults in these cases have presented a lower intelligence quotient (IQ) score. Objectively, this intellectual disability, measured with an IQ score of 75, is also a minor criterion for the diagnosis of CS (6). ASD, remarkably in association with macrocephaly, has also been linked to PTEN mutation. One in five patients with ASD-macrocephalic have been diagnosed with a PTEN mutation. In these ASD cases, macrocephaly seems to be more severe compared to the non-PTEN-mutated group (7). Individuals with PTEN-related ASD also show anatomical differences, with an increase in cortical white matter and a distinctive neurocognitive and behavioral phenotype, including delayed language development, poor working memory and processing speed, and adaptive and sensory abnormalities (8, 9). Epilepsy has been mentioned in some cases (4, 10, 11) but is not as common in this population.
Lhermitte–Duclos disease (LDD) is the most common brain tumor that develops in adult CS patients. Once identified and confirmed, it is considered a pathognomonic finding for CS (6). This benign lesion occurs in around 35% of the CS patients, and only ~250 cases have been published (12). On T2-MRI, we identify a classic alternating pattern of high and low signal, giving it a striated appearance that is said to resemble “tiger stripes.” This tigroid appearance on T2 imaging distinguishes LDD from other more common primary cerebellar gliomas that destroy the delicate folial pattern of the cerebellum (13). These lesions are benign and progress through a slow growth. Surgical treatment is only required in symptomatic cases (12, 14). In the NIH Genetic Testing Registry, PTEN mutations have also been linked to the appearance of familial meningioma and other predisposing genes. There have been cases of CS associated with meningioma (10). However, whether the meningioma is genuinely associated with the PTEN mutation or is an incidental finding is unclear (15).
Asymptomatic cavernous malformations (cavernoma or cavernous angioma) and developmental venous anomalies (venous angioma) are common, and many cases were reported with these conditions in patients with CS (10). One case of a giant ruptured fusiform middle cerebral artery aneurysm was also reported in a CS patient; however, the PTEN gene mutation was not confirmed because the patient and his family did not consent to genetic testing (16). Two cases of spinal AVF associated with LDD have been reported. Rupture or steal phenomena of the AVF in a cervical location can have devastating clinical consequences. Both cases were very similar in feeding and drainage patterns and could represent a different phenotype (17–19). Non-neurological AVM has been reported in many CS and BRRS cases (20). Real intracranial AVM has not been reported yet. A French CS multicenter study found six patients (in a series of 20) harboring vascular malformation (10). Therefore, the association of PTEN mutations and vascular anomalies is consistent with the growing evidence that PTEN modulates angiogenesis (20).
The literature review for the present study revealed that only a limited number of cases identified a correlation between the PTEN variant and dAVFs. These few cases exhibited the syndromes mentioned earlier. An adult with classic CS experienced a generalized seizure caused by bleeding from multiple dural and epidural high-flow AVFs. This patient underwent five sessions of embolization uneventfully but unfortunately passed away due to severe status epilepticus (21). Another study reported that a 14-year-old with BRRS, who manifested with diplopia and papilledema, was diagnosed with pseudotumor cerebri, similar to the reported case in our study. Despite the signs of increased ICP, no MRI or MR angiogram abnormalities were noted. Because the patient in our study worsened over time, new studies identified dAVF connecting meningeal branches of the middle meningeal artery to the transverse sinus bilaterally. She underwent two sessions of embolization and had a good recovery (22). Acquired dAVF has also been reported in CS in a postop of a brainstem cavernoma. In this case, the manipulated dura underwent neovascularization, creating anomalous communications between dural arteries and cerebellar cortical veins. This patient was reapproached to treat the dAVF. This case suggests that postoperative angiogenesis may cause AVF in patients with CS (23). Determining whether PTEN insufficiency alone or other molecular factors in the PI3K/Akt/VEGF signaling contribute to these angiogenic formations is difficult (24).
Our case, different from the ones mentioned in the literature, did not meet the criteria for any PTEN gene syndrome. Whole-body screening did not identify any cutaneous or visceral lesions, which would fulfill the criteria for CS. She was normocephalic and had no history of developmental delay. Because she was a lawyer, we deduce that the patient previously had an average IQ. Additionally, this case has a unique presentation of rapidly formed multiple and new dAVFs. Despite compromised venous drainage, venous congestion, and chronic perfusion shortages, the patient remained relatively asymptomatic. She only progressed to a more severe neurological state when experiencing acute bleeding secondary to venous thrombosis. Interestingly, her cerebral perfusion adapted rapidly to the collaterals and responded highly to hemodynamic changes after every embolization. This complex formation of dAVF corroborates with the suspicion of physiopathology that PTEN modulates angiogenesis.
It is important to emphasize that this mutation is relatively rare (25).
Of the few cases previously published associated with dAVF, typical PTEN syndromic patients were involved. Hence, we advocate the novelty of this case: (1) Despite the PTEN variant, the patient did not fulfill the criteria for any syndrome; and (2) the rapid and aggressive formation of new dAVFs is not typical. More studies are necessary to understand how to manage patients who present with such dAVFs.
4 Conclusion
The previously reported dAVF cases with PTEN variant were linked to syndromic PTEN mutations. We describe a case of a previously healthy adult with multiple and complex dAVFs as a new phenotype.
Data availability statement
The datasets presented in this article are not readily available because of ethical and privacy restrictions. Requests to access the datasets should be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by the Ethics and Research Committee of the Federal University of São Paulo. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author contributions
GJ-A-L: Conceptualization, Investigation, Writing – original draft, Writing – review & editing. TS: Formal analysis, Investigation, Writing – review & editing. MS: Data curation, Methodology, Writing – review & editing. LG: Data curation, Methodology, Writing – review & editing. RW-S: Writing – review & editing. AB: Data curation, Investigation, Writing – review & editing. JC: Resources, Validation, Writing – review & editing. FC-N: Project administration, Supervision, Validation, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
We would like to thank all the microvascular fellows for their support with this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Plamper M, Gohlke B, Woelfle J. PTEN hamartoma tumor syndrome in childhood and adolescence-a comprehensive review and presentation of the German pediatric guideline. Mol Cell Pediatr. (2022) 9:3. doi: 10.1186/s40348-022-00135-1
2. Tan WH, Baris HN, Burrows PE, Robson CD, Alomari AI, Mulliken JB, et al. The spectrum of vascular anomalies in patients with PTEN mutations: implications for diagnosis and management. J Med Genet. (2007) 44:594–602. doi: 10.1136/jmg.2007.048934
3. Lynch NE, Lynch SA, McMenamin J, Webb D. Bannanyan-Riley-Ruvalcaba syndrome: a cause of extreme macrocephaly and neurodevelopmental delay. Arch Dis Child. (2009) 94:553–4. doi: 10.1136/adc.2008.155663
4. Hendriks YMC, Verhallen JTCM, van der Smagt JJ, Kant SG, Hilhorst Y, Hoefsloot L, et al. Bannanyan-Riley-Ruvalcaba syndrome: further delineation of the phenotype and management of PTEN mutation-positive cases. Fam Cancer. (2003) 2:79–85. doi: 10.1023/A:1025713815924
5. Starink TM, van der Veen JP, Arwert F, de Waal LP, de Lange GG, Gille JJ, et al. The Cowden syndrome: a clinical and genetic study in 21 patients. Clin Genet. (1986) 29:222–33. doi: 10.1111/j.1399-0004.1986.tb00816.x
6. Pilarski R, Burt R, Kolman W, Pho L, Shannon KM, Swisher E. Cowden syndrome and the PTEN hamartoma tumor syndrome: systematic review and revised diagnostic. J Natl Cancer Inst. (2013) 105:1607–16. doi: 10.1093/jnci/djt277
7. Mester JL, Tilot AK, Rybicki LA, Frazier TW, Eng C. Analysis of prevalence and degree of macrocephaly in patients with germline PTEN mutations and of brain weight in Pten knock-in murine model. Eur J Hum Genet. (2011) 19:763–8. doi: 10.1038/ejhg.2011.20
8. Busch RM, Srivastava S, Hogue O, Frazier TW, Klaas P, Hardan A, et al. Developmental synaptopathies consortium. Transl Psychiatry. (2019) 9:253. doi: 10.1038/s41398-019-0588-1
9. Frazier TW, Embacher R, Tilot AK, Koenig K, Mester J, Eng C. Molecular and phenotypic abnormalities in individuals with germline heterozygous PTEN mutations and autism. Mol Psychiatry. (2015) 20:1132–8. doi: 10.1038/mp.2014.125
10. Lok C, Viseux V, Francoise M, Richard MA, Gondry-Jouet C, Deramond H, et al. Brain magnetic resonance imaging in patients with Cowden syndrome. Medicine. (2005) 84:129–36. doi: 10.1097/01.md.0000158792.24888.d2
11. Prats-Sánchez LA, Hervás-García JV, Becerra JL, Lozano M, Castaño C, Munuera J, et al. Multiple intracranial arteriovenous fistulas in Cowden Syndrome. J Stroke Cerebrovasc Dis. (2016) 25:e93–4. doi: 10.1016/j.jstrokecerebrovasdis.2016.03.048
12. Khandput U, Huntoon K, Smith-Cohn M, Shaw A, Elder JB. Bilateral recurrent dysplastic cerebellar gangliocytoma (Lhermitte-Duclos Disease) in Cowden Syndrome: a case report and literature review. World Neurosurg. (2019) 127:319–25. doi: 10.1016/j.wneu.2019.03.131
13. Zhang HW, Zhang YQ, Liu XL, Mo YQ, Lei Y, Lin F, et al. MR imaging features of Lhermitte-Duclos disease: case reports and literature review. Medicine. (2022) 101:e28667. doi: 10.1097/MD.0000000000028667
14. Joo G, Doumanian J. Radiographic findings of dysplastic cerebellar gangliocytoma (Lhermitte-Duclos Disease) in a woman with Cowden Syndrome: a case study and literature review. J Radiol Case Rep. (2020) 14:1–6. doi: 10.3941/jrcr.v14i3.3814
15. Yehia L, Eng C, Adam MP, Feldman J, Mirzaa GM, Pagon RA, et al. PTEN Hamartoma Tumor Syndrome. In: Bean LJH, Gripp KW, Amemiya A, , editors. GeneReviews. Seattle, WA: University of Washington, Seattle (2001).
16. Toh K, Suzuki K, Miyaoka R, Kitagawa T, Saito T, Nakano Y, et al. Giant cerebral aneurysm in a patient with Cowden syndrome treated with surgical clipping. World Neurosurg. (2019) 126:336–40. doi: 10.1016/j.wneu.2019.02.245
17. Almubarak AO, Haq AU, Alzahrani I, Shail EA. Lhermitte-duclos disease with cervical arteriovenous fistula. J Neurol Surg A Cent Eur Neurosurg. (2019) 80:134–7. doi: 10.1055/s-0038-1670636
18. Akiyama Y, Ikeda J, Ibayashi Y, Nonaka T, Asai Y, Houkin K. Lhermitte-Duclos disease with cervical paraspinal arteriovenous fistula. Neurol Med Chir. (2006) 46:446–9. doi: 10.2176/nmc.46.446
19. Bae BG, Kim HJ, Lee SG, Choi JR, Hwang C, Lee JH, et al. A novel PTEN mutation in a Korean patient with Cowden syndrome and vascular anomalies. Acta Derm Venereol. (2011) 91:88–90. doi: 10.2340/00015555-0994
20. Turnbull MM, Humeniuk V, Stein B, Suthers GK. Arteriovenous malformations in Cowden syndrome. J Med Genet. (2005) 42:e50. doi: 10.1136/jmg.2004.030569
21. Srinivasa RN, Burrows PE. Dural arteriovenous malformation in a child with Bannayan-Riley-Ruvalcaba Syndrome. Am J Neuroradiol. (2006) 27:1927–9.
22. Moon K, Ducruet AF, Crowley RW, Klas K, Bristol R, Albuquerquer FC. Complex dural arteriovenous fistula in Bannayan-Riley-Ruvalcaba syndrome. J Neurosurg Pediatr. (2013) 12:87–92. doi: 10.3171/2013.3.PEDS12551
23. Sadahiro H, Ishihara H, Goto H, Oka F, Shirao S, Yoneda H, et al. Postoperative dural arteriovenous fistula in a patient with Cowden disease: a case report. J Stroke Cerebrovasc Dis. (2014) 23:572–5. doi: 10.1016/j.jstrokecerebrovasdis.2013.04.021
24. Kar S, Samii A, Bertalanffy H. PTEN/PI3K/Akt/VEGF signaling and the cross talk to KRIT1, CCM2, and PDCD10 proteins in cerebral cavernous malformations. Neurosurg Rev. (2015) 38:229–36. doi: 10.1007/s10143-014-0597-8
Keywords: pseudotumor cerebri, gene variant, AV fistulas, dural arteriovenous fistula (DAVF), PTEN gene mutation
Citation: Jong-A-Liem GS, Sarti THM, dos Santos MG, Giacon LMT, Wuo-Silva R, Baeta AM, de Campos Filho JM and Chaddad-Neto F (2024) Case report: Association between PTEN-gene variant and an aggressive case of multiple dAVFs. Front. Neurol. 15:1347289. doi: 10.3389/fneur.2024.1347289
Received: 30 November 2023; Accepted: 14 March 2024;
Published: 08 April 2024.
Edited by:
Huifang Shang, Sichuan University, ChinaReviewed by:
Qiheng He, Capital Medical University, ChinaValeria Capra, Giannina Gaslini Institute (IRCCS), Italy
Copyright © 2024 Jong-A-Liem, Sarti, dos Santos, Giacon, Wuo-Silva, Baeta, de Campos Filho and Chaddad-Neto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Feres Chaddad-Neto, ZmVyZXNjaGFkZGFkQGhvdG1haWwuY29t