
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Neurol. , 21 March 2024
Sec. Neurotrauma
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1347200
This article is part of the Research Topic Women in Neurotrauma 2023 View all 11 articles
 Sharada Kadaba Sridhar1,2
Sharada Kadaba Sridhar1,2 Jen Dysterheft Robb2
Jen Dysterheft Robb2 Rishabh Gupta2,3Scarlett Cheong1,2
Rishabh Gupta2,3Scarlett Cheong1,2 Rui Kuang1,4
Rui Kuang1,4 Uzma Samadani1,2,3,4,5*
Uzma Samadani1,2,3,4,5*Introduction: Normal Pressure Hydrocephalus (NPH) is a prominent type of reversible dementia that may be treated with shunt surgery, and it is crucial to differentiate it from irreversible degeneration caused by its symptomatic mimics like Alzheimer’s Dementia (AD) and Parkinson’s Disease (PD). Similarly, it is important to distinguish between (normal pressure) hydrocephalus and irreversible atrophy/degeneration which are among the chronic effects of Traumatic Brain Injury (cTBI), as the former may be reversed through shunt placement. The purpose of this review is to elucidate the structural imaging markers which may be foundational to the development of accurate, noninvasive, and accessible solutions to this problem.
Methods: By searching the PubMed database for keywords related to NPH, AD, PD, and cTBI, we reviewed studies that examined the (1) distinct neuroanatomical markers of degeneration in NPH versus AD and PD, and atrophy versus hydrocephalus in cTBI and (2) computational methods for their (semi-) automatic assessment on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI) scans.
Results: Structural markers of NPH and those that can distinguish it from AD have been well studied, but only a few studies have explored its structural distinction between PD. The structural implications of cTBI over time have been studied. But neuroanatomical markers that can predict shunt response in patients with either symptomatic idiopathic NPH or post-traumatic hydrocephalus have not been reliably established. MRI-based markers dominate this field of investigation as compared to CT, which is also reflected in the disproportionate number of MRI-based computational methods for their automatic assessment.
Conclusion: Along with an up-to-date literature review on the structural neurodegeneration due to NPH versus AD/PD, and hydrocephalus versus atrophy in cTBI, this article sheds light on the potential of structural imaging markers as (differential) diagnostic aids for the timely recognition of patients with reversible (normal pressure) hydrocephalus, and opportunities to develop computational tools for their objective assessment.
Normal pressure hydrocephalus (NPH), is a prominent type of dementia that is often reversible via ventricular shunt surgery, with earlier intervention leading to better outcomes (1). A notable discrepancy between the incidence (of patients who had surgical intervention) (2–4) and prevalence rates (5–7) suggests its under-recognition. This is substantiated by an estimate from the Hydrocephalus Association that 80% of patients with NPH remain unrecognized with most frequent misdiagnoses being Alzheimer’s Dementia (AD) or Parkinson’s Disease (PD) (8), which themselves significantly contribute to the global burden of neurological disorders (9). About half of the cases of NPH are estimated to be idiopathic, and the other half secondary to traumatic brain injury (TBI), tumor, meningitis, or infections (10, 11). Adding complexity to its recognition may be the fact that in the secondary NPH group, while tumors or infection linked to the disease can be detected definitively, a TBI-related origin may not be accurately identified due to incomplete medical history. Therefore, the accurate detection and treatment of NPH may inevitably depend on discerning it from irreversible atrophic pathologies like AD, PD, and post-traumatic degeneration.
In terms of structural neurodegeneration, hydrocephalic ventriculomegaly is the key marker of NPH (12). Idiopathic NPH and NPH secondary to TBI, may differ in their etiology, but remarkable improvement in symptoms of patients with both conditions have been demonstrated after ventricular shunting (1, 13). But because atrophy is a chronic effect of TBI which may cause secondary ventriculomegaly, and has been negatively correlated with shunt outcome, accurately discerning it from hydrocephalic ventriculomegaly on structural imaging (14) is paramount for shunt-surgery decision making. The structural degeneration in AD (15) and PD (16) is also characterized by atrophy. Both atrophy and hydrocephalus can give an appearance of ventricular enlargement, which may set a precedent for misdiagnosis if not examined carefully.
In addition to similar structural neurodegeneration, the cognitive and functional deficits such as dementia and gait impairment caused by these diseases often overlap, rendering misdiagnoses distressingly common. The stretching of the corticospinal tract (CST) in the corona radiata which conducts signal to the legs is thought to produce gait disturbance, a manifestation in most NPH cases, while radial shearing force exerted by enlarging ventricles leads to dementia (17). Loss of structural integrity leads to impairment of cognitive and executive function in AD which may affect gait due to divided attention (18). PD which is thought to arise in the substantia nigra and basal ganglia, is characterized by its motor symptoms including gait impairment (19). Its degenerative impact extends well into the cerebral cortex as atrophy leading to cognitive deficits (20). Chronic TBI (cTBI) also leads to cognitive and gait impairment through its degenerative effects (21, 22).
The neurostructural damage resulting from NPH manifests as distinct imaging markers capturable on Computed Tomography (CT) and Magnetic Resonance Imaging (MRI). CT-based markers have been included as a supporting factor in the diagnostic guidelines for NPH and acute TBI. However, they have not gained prominence relative to neurological, clinical, cerebrospinal fluid (CSF) and blood biomarkers, advanced MRI, and functional imaging, especially in AD, PD, and cTBI. Structural imaging markers may offer a noninvasive solution not only for the accurate detection of NPH, but also for its distinction from irreversible neurodegeneration in AD and PD; and distinguishing between atrophy and hydrocephalus in cTBI. There have been a handful of reviews that have elucidated imaging markers of NPH. Pyrgelis et al. (23) provided a review of functional and structural imaging markers for NPH and highlighted a limited number of them which distinguish it from AD and PD, and Yin et al. (24) presented a mini-review of NPH-specific features. But there have been no focused attempts to highlight the structural imaging markers of NPH along with those that can differentiate it from its mimics AD and PD and shed light on the interplay of atrophy and hydrocephalus in cTBI. This review also comments on the adoption of computational techniques for the objective assessment of these markers and highlights areas where further research is needed.
We searched PubMed for the keyword “normal pressure hydrocephalus” in combination with the keywords “Alzheimer” and “parkinson.” We also searched for “hydrocephalus” and “atrophy,” in combination with “traumatic brain injury.” Studies that used only structural neuroimaging modalities of (T1/T2/DTI) MRI and CT, and those that studied humans aged 19 years and above were retained. From the resultant set of articles, we present this review of structural imaging markers for NPH. For AD and PD, we provide a brief background of their burden, pathology, structural degenerative markers that differentiate NPH from them. The review of cTBI, and consequent atrophy and hydrocephalus is structured similarly. Articles where (semi) automatic image processing and machine (deep) learning have been applied to assess these features in MRI and CT modalities are also discussed. The key abbreviations and structural imaging marker definitions are in Tables 1, 2 respectively.
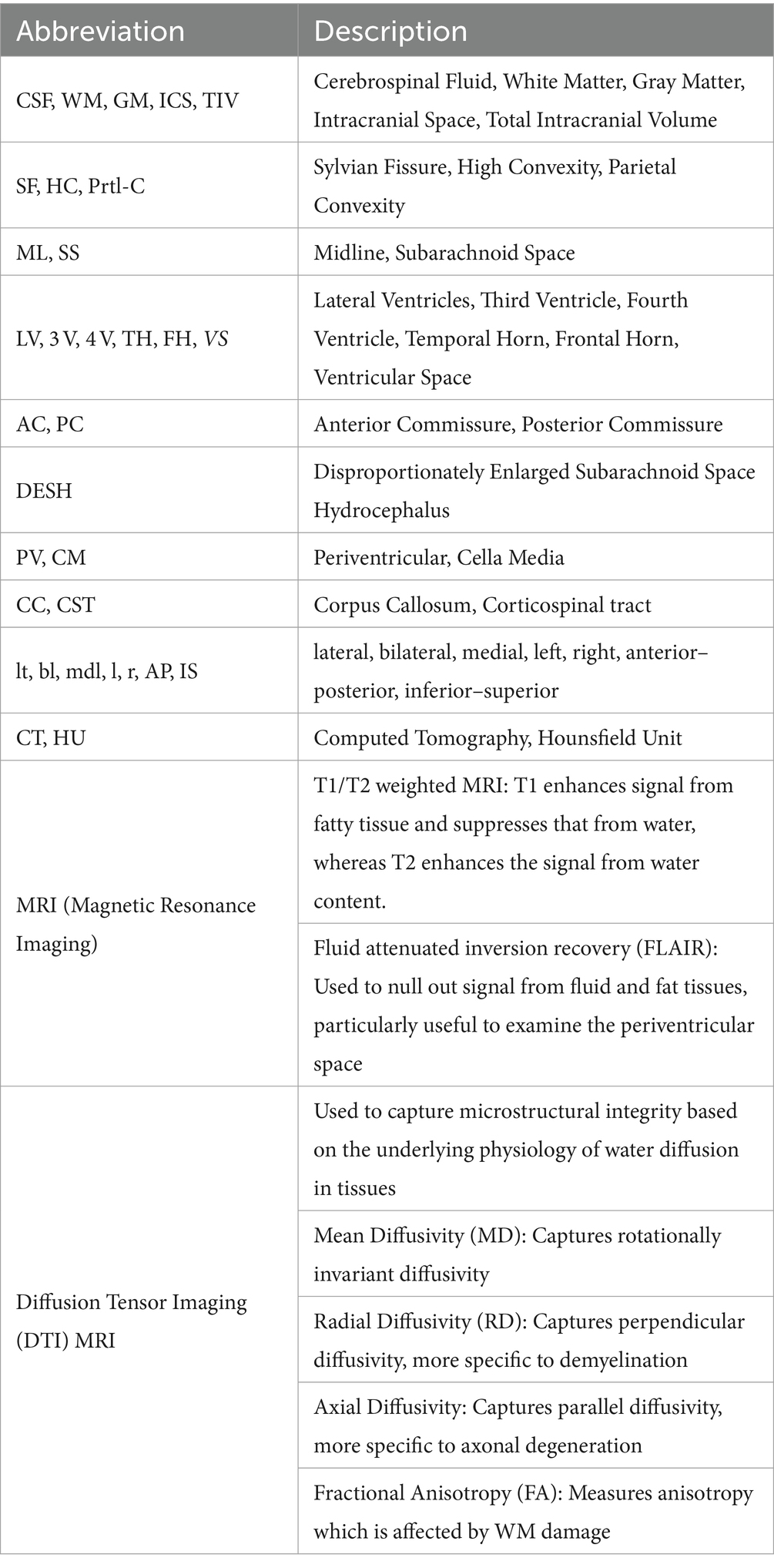
Table 1. Key abbreviations.
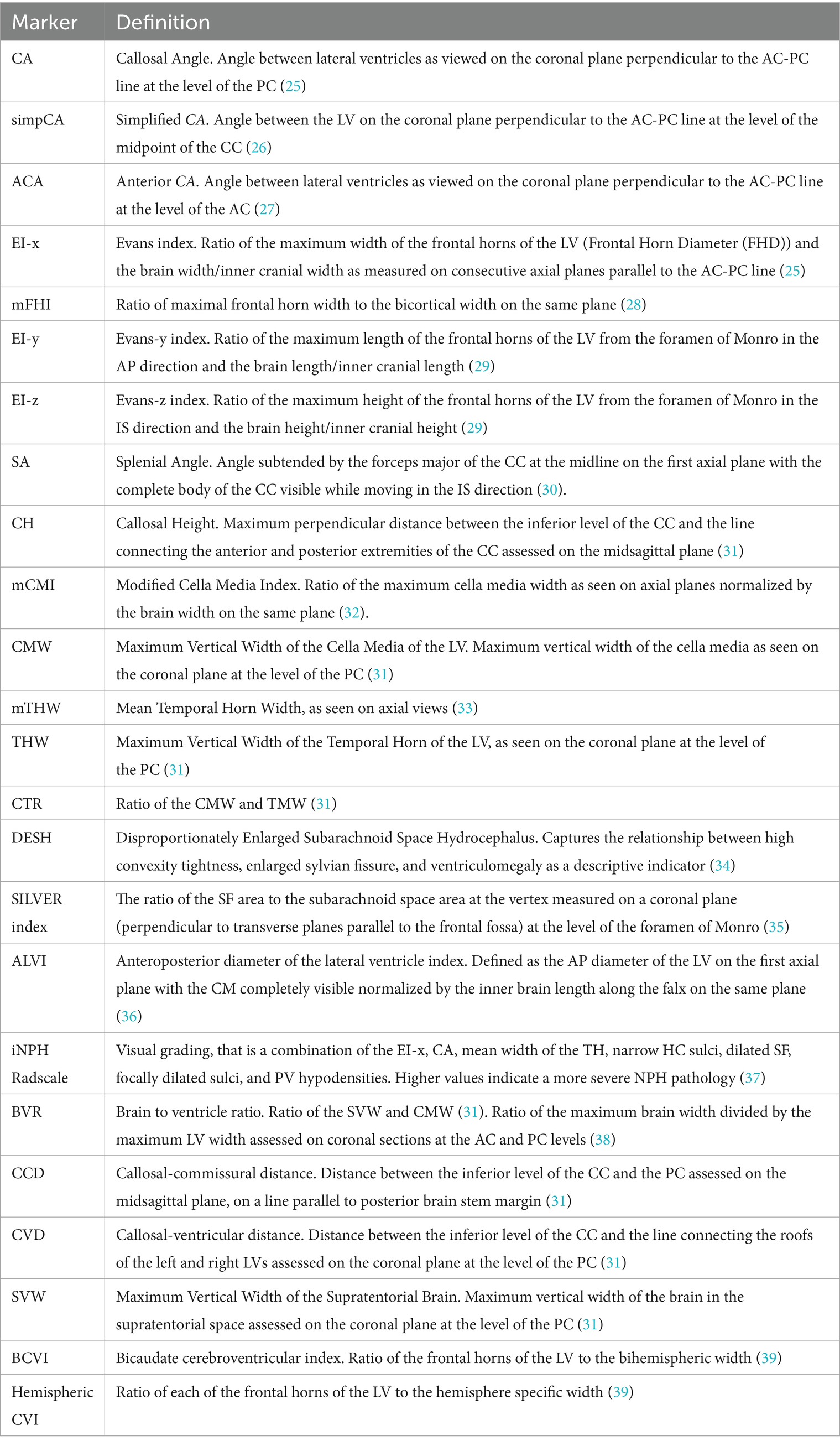
Table 2. Structural imaging markers and definitions.
Hakim and Adams, first explained the mechanism of NPH using Pascal’s law. Presently, at least 700,000 older adults in the US are estimated to be afflicted by the condition (40). Excessive buildup of CSF in the ventricles leads to their enlargement and impingement on the surrounding brain tissue. And due to the compliance of the surrounding brain tissue, intracranial pressure (ICP), remains “normal” (12). Recent studies suggest that the pathogenesis of NPH is complex and is potentially related to CSF dynamics, CSF – interstitial fluid exchange, cortical subarachnoid space (SS) morphology, and venous congestion (41). It is clinically characterized by the Hakim triad which is a combination of gait impairment, urinary incontinence, and cognitive impairment.
The American-European diagnostic guidelines classify NPH into possible and probable subgroups based on clinical evaluation for the Hakim triad, an invasive CSF tap-test with opening CSF pressure of 5–18 mm Hg, medical history, and radiographic assessment of lateral ventricle (LV) enlargement (42). Enlarged temporal horns (TH) and periventricular intensity changes unattributable to ischemia or demyelination are also considered. While they do not endorse a classification of patients with definite NPH based on positive shunt response, the Japanese guidelines take that approach, and include evaluation of sulcal tightness at the high-convexity (HC) of the brain and dilation at the sylvian fissures (SF) (43). Age at onset and presence of other comorbidities are also considered in both guidelines (44). Irrespective of different approaches to classification, a vast majority of patients saw favorable outcomes following shunt surgery (45) and early surgical intervention was found to significantly affect functional outcomes (46). And despite reports of complications (47), advances in surgical procedures guided by computer aided neuronavigation, and infection reduction strategies suggest a promising future for complete reversal of symptoms in NPH (48).
Radiological markers are significantly factored in the clinical diagnosis of NPH. Diagnostic standard measures of ventriculomegaly in NPH diagnosis include the callosal angle (CA), Evans-x index (EI-x), and the Disproportionately Enlarged Subarachnoid Space Hydrocephalus (DESH) (42, 43). Several other structural markers describing the effects of NPH on the ventricular and CSF spaces, white matter (WM), and gray matter (GM) structures have been described over the years. The prominent features described in this section are summarized in Table 3.
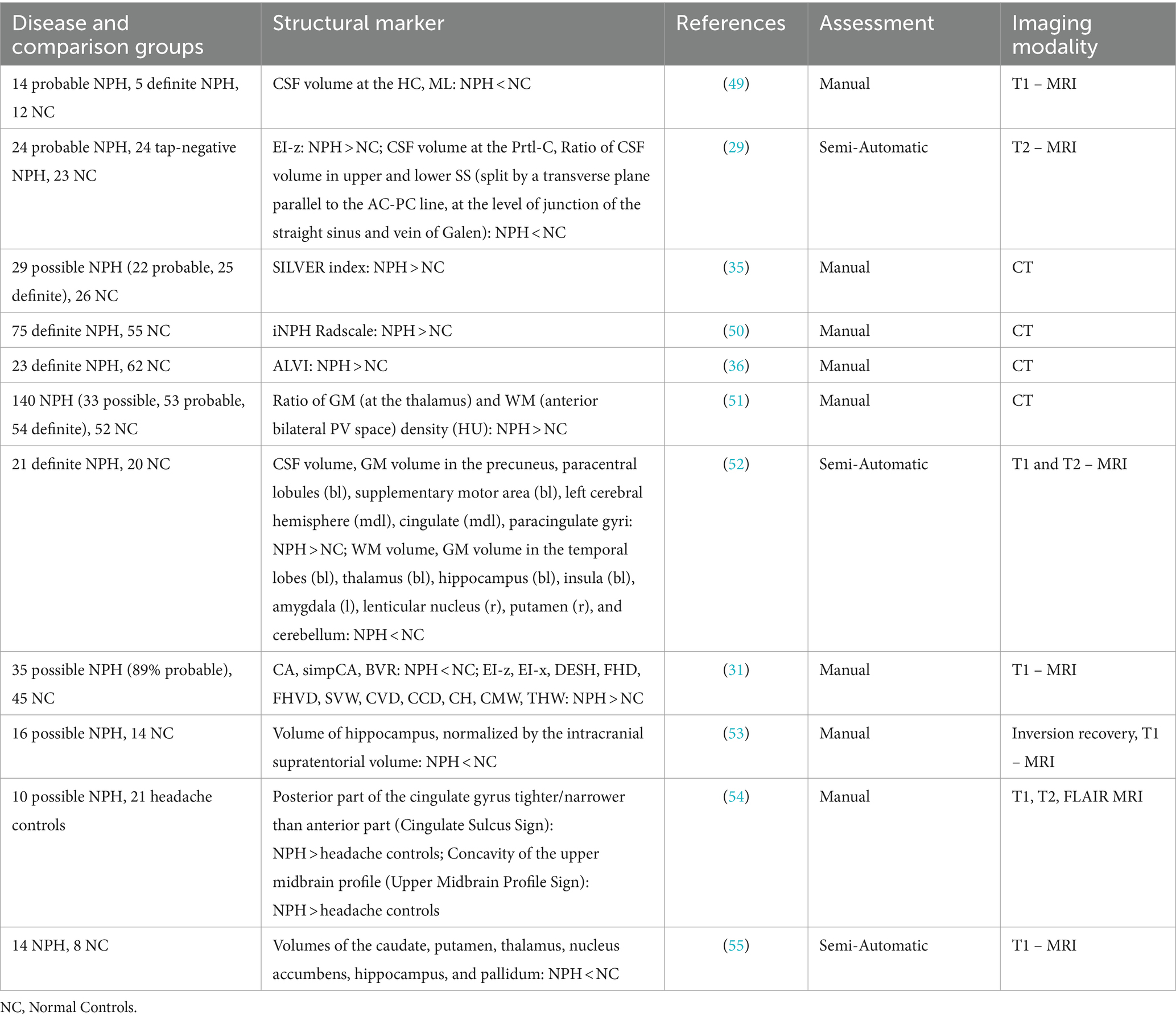
Table 3. Structural imaging markers of NPH.
As CSF spaces are the most distinctly deformed anatomy in NPH, features describing its volume and morphology have been extensively studied and applied in the detection of NPH. A 2007 study of 14 patients with probable NPH (3.5% with shunt response) patients on MRI scans indicated that visually apparent narrowing of CSF spaces at the HC and midline (ML) accurately separated them from age-matched controls (49). Another study of 24 patients with probable NPH who had functional improvement after a CSF-tap test (tap positive), 24 tap negative patients, and 23 age matched controls using on (T2) MRI scans showed that 3 newly proposed metrics – CSF volume at the parietal convexity (Prtl-C), the Evans-z index (EI-z), and upper to lower SS ratio were optimal diagnostic indices of iNPH as they had the highest area under the curve of receiver operating characteristics (AUCROC) in distinguishing between tap-positive and tap-negative patients. Absolute and normalized (by intracranial volume) volumes of the total ventricle and bilateral ventricle spaces, the Evans-y index (EI-y), EI-x, maximum ventricle to brain lengths (in the 3 orthogonal directions), CA, CSF volumes of the SS at the frontal and parietal convexity, SF and basal cistern, and posterior fossa were also among the evaluated features (29).
Changin et al. proposed a simplified CA (simpCA) measure to overcome the need for extensive image processing to obtain the CA and showed that it was significantly lowered in NPH patients as seen on MRI sequences (27). To mitigate nonuniformity and examination of multiple slices required to measure the EI-x, another quantitative measure called the anteroposterior diameter of the lateral ventricle index (ALVI) on a fixed a standard plane was demonstrated to be better correlated with ventricular volume as compared to the EI-x, and a threshold of 0.5 could detect patients with ventriculomegaly in definite NPH when compared to healthy controls on CT (36). A comprehensive study of interpretable measures of the CSF spaces on MRI evaluated the frontal horn diameter (FHD), DESH, CA, simpCA, maximum vertical width of the supraventricular brain (SVW), cella media width (CMW), temporal horn width (THW), frontal horn vertical diameter (FHVD), callosal ventricular distance (CVD), callosal commissural distance (CCD), callosal height (CH), EI-x, EI-z, cella media to temporal horn ratio (CTR: CMW/THW), and brain to ventricle ratio (BVR: SVW/CMW), showed that all features except the CTR were able capture significant differences between probable NPH and normal controls. However, the capacity of these features in predicting shunt response were not evaluated in the study (31).
Structural imaging markers that predict shunt response in NPH have not been reliably established. A larger study of probable NPH (n = 229) patients contrasted with a non-NPH group, manually examined volumes of the LVs, basal cisterns, and SS superior to and at the level of the SF. They also manually evaluated DESH, focally dilated sulci, aqueductal CSF flow void sign, medial temporal lobe atrophy, WM changes, mean temporal horn width (mTHW), EI-x, CA, and the modified cella media index (mCMI) (33). They found that NPH diagnosis was more likely in patients with higher disproportion of the SF-level SS as compared to the supra-SF SS space, and narrower THs (lower mTHW) but concluded that none of the radiological markers could predict shunt response. Given that this study only included patients with EI-x > 0.3, the finding of narrower THs in NPH may be due to patients with atrophic enlargement of the TH being grouped in the non-NPH group.
A quantification of DESH on CT scans was proposed using the SILVER index defined as the ratio of the SF area to the SS area at the vertex, which had an AUC of 0.9 in distinguishing NPH from controls, but there was no significant difference between shunt responders and non-responders (35). Another retrospective study that tried to relate various manually evaluated MRI measures including notable ones such as DESH (HC sulcal tightness and SF dilation), the CA, EI-x, maximum 3 V width, maximum width of the TH, maximum anteroposterior diameter of the 4 V, aqueductal flow-void sign, and inter-hemispheric fissure width found no significant differences between shunt responders and non-responders (56). Consolidating several markers of ventriculomegaly and CSF space morphology, Kockum et al. (37) proposed the iNPH Radscale in 2018. They demonstrated that this measure showed consistency when measured on MRI and CT (57), and had a positive correlation with expert radiologist evaluations and classified shunt-responsive NPH patients from healthy controls (50) using CT scans. However, there is also evidence that the Radscale cannot predict shunt response amidst symptomatic individuals and recommended against its sole for shunt-surgery selection (58).
A novel measure called the Splenial Angle (SA), defined on Diffusion Tensor Imaging (DTI) MRI Fractional Anisotropy maps as the angle subtended by the forceps major of the corpus callosum (CC) on axial slices, to capture the effect of ventricular distention on the CC at the ML in probable NPH was shown to have high sensitivity in distinguishing it from controls (30). Left ear extinction in NPH possibly associated with the upward elevation and thinning of the CC was found to be alleviated among patients with NPH post shunting, indicating the range of impairments that may be reversed with surgery (59). Confirming the previous findings of loss of WM integrity in NPH on CT scans, a recent study showed that the ratio of GM density at the thalamus to the WM density at anterior periventricular regions was lower in NPH and could be used to distinguish it from healthy controls. Even though their NPH cohort included definite NPH patients, they were unable to demonstrate the utility of this measure in distinguishing between shunt response in symptomatic patients (51). Hippocampal atrophy was shown to correlate with patients who have higher rates of cognitive impairment in NPH (53). But GM degradation had not been detailed in NPH until recently. Lv et al. (52) compared definite NPH patients with controls using MRI scans and found regional variations in GM volume that were significantly different in the NPH group. GM volume was lowered in specific temporal areas, thalamus, hippocampus, and the cerebellum. Contrarily, it was increased in medial and parietal regions. Global reduction in WM volumes and increase in CSF volumes were also found (52).
A 2013 study on MRI scans of 16 NPH patients who improved after shunt surgery showed that recovery after surgery was correlated with lower brain deformation before surgery as seen on MRI (60). They captured the ratio of ventricular and SF enlargement to the HC/ML tightness in a single measure of deformity, reflective of DESH, which was shown to improve post-surgery. It is important to note from this study that there may be a threshold to structural damage which may indicate irreparable loss when breached. And as new therapies emerge, it would be critical to accurately identify patients with this type of reversible dementia to optimize care for them. This is where differential diagnosis for NPH including the accurate identification of AD and PD comes to the forefront. The prominent features capturing the difference between NPH and AD/PD are summarized in Table 4.
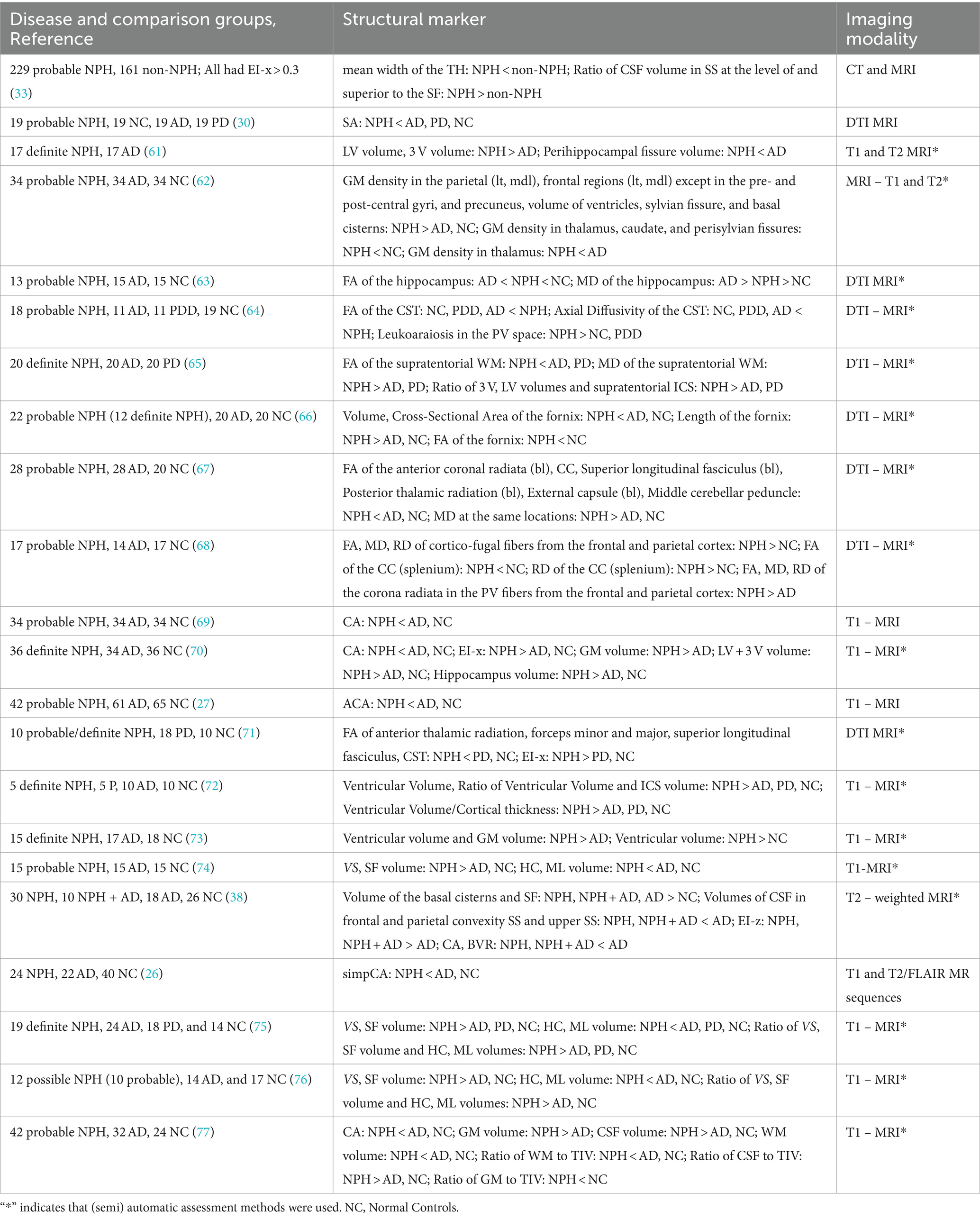
Table 4. Structural imaging markers for differentiation of NPH from AD and PD.
Alzheimer’s Dementia (AD) is best characterized by the abnormal presence of extracellular amyloid plaques and intracellular neurofibrillary tangles (NFT) of protein tau which leads to a loss of synapses and cell death (78). In the US, AD is prevalent among 6.5 million people (79). Studies have shown that amyloid beta plaques start accumulating in abnormal clumps called oligomers and fibrils in the early stages which is correlated to downstream accumulation of NFT (80). Activated microglia that are unable to keep up with debris clearance cause chronic inflammation and cell death leads to atrophy. In early stages, the medial temporal lobe involving hippocampus, entorhinal cortex, amygdala, and para-hippocampal cortex seem to be most affected along with global atrophy involving the frontal, temporal, and parietal lobes excluding the sensory-motor cortex and occipital regions. Basal ganglia regions like the caudate, putamen, pallidum, and nucleus accumbens also show atrophy (15). Clinical symptoms mainly include loss of memory, decreased executive function, language deficit, loss of vision, and gait instability (78). Diagnosis is based on physical exam, evaluation of patient history, memory, cognitive, and neurological functions along with radiographic imaging. Therapeutic solutions for AD like cholinesterase inhibitors are commonly used to alleviate symptoms. While there is no complete cure for the disease yet, a drug which was shown to remove amyloid plaque deposits in the brain was approved by the FDA and several others are being investigated (79).
The medical research community has directed significant efforts to solving the problem of accurately distinguishing between NPH and AD using neuroimaging markers, in the hope that patients with reversible dementia do not get sentenced to a hopeless diagnosis of AD and miss their chance at a better quality of life. Identifying the structural effects of NPH and AD accurately may also find application in predicting patients with poorer shunt outcomes in NPH patients with comorbid AD (81). Expectedly, MRI-based markers and methods have dominated and emerged successfully in this quest. The CSF flow void sign on T2-weighted MR sequences which appears in the cerebral aqueduct was one of the earlier signs of impaired CSF dynamics in NPH, and it was shown to classify it from AD (82). This was also substantiated quantitatively by demonstrating a higher aqueductal CSF flow rate in NPH as opposed to AD, using phase contrast MRI, a few years later (83). However, even though CSF hydrodynamics is impaired in NPH, there is also evidence that it may not provide distinction from AD (84).
Signs of structural integrity loss in specific anatomies affected by the NPH pathology have been promising in segregating AD pathology. Holodny et al. (61) identified the dilation of the peri-hippocampal fissure as a distinctive anatomical marker between NPH and AD, along with the LV and 3 V sizes, as seen on MRI. Potentially indirect effects of ventriculomegaly like the narrowing of the posterior cingulate sulcus as compared to the anterior part and a concave upper midbrain profile, apparent on MRI, was shown to be more likely in NPH as opposed to AD but it was not tested for its sensitivity in classifying NPH from AD (54). While these studies set a promising avenue, extracting features from these specific neuroanatomies on MRI and CT requires significant manual intervention and/or preprocessing in the form of region-of-interest definitions. GM density on T1 and T2 MRI was shown to be significantly higher in the precuneus, frontal and parietal regions (medially and laterally, except around the central sulcus potentially spared due to dilation from aging) when NPH was compared to AD and normal controls. When NPH was compared to normal controls, it was significantly lower in the thalamus, caudate, and perisylvian fissure, but only so in the thalamus when compared to AD. It also revealed the enlargement of the ventricles, SF, and basal cisterns in NPH versus AD and normal controls (62).
WM abnormality has gained importance as a structural marker in differentiating NPH from AD. A 2010 study argued for the use of DTI to detect microstructural integrity of WM in the hippocampus using fractional anisotropy (FA) and mean diffusivity (MD) as more sensitive measures in detecting NPH from AD, as opposed to its whole volume (63). FA and axial diffusivity values measured on DTI MRI at the CST, distention of which is thought to cause gait impairment in NPH, were shown to be highly sensitive in detecting probable NPH from AD, PD with Dementia, and healthy controls (64). In the same year, another study found that higher MD coupled with lower FA in the supratentorial WM of the brain was indicative of NPH versus AD and PD (65). The SA which captures the effect of distention of LVs on the forceps major of the CC (30) was also shown to differentiate between NPH and AD.
In a very insightful finding on DTI, it was demonstrated that the WM structure fornix had reduced volume and cross-sectional area in NPH patients but longer compared to AD and normal controls (66). The FA value in this structure was also lower in NPH as compared to normal controls. Revealing structural damage to the fornix due to LV enlargement, this finding illustrates the power of structural imaging to capture the degenerative effects of NPH on the brain. Kang et al. (67) provided a more anatomically localized insight into WM structural integrity by showing lower FA and higher MD bilaterally in the anterior corona radiata, posterior thalamic radiation, superior longitudinal fasciculus, and external capsule of NPH patients as opposed to AD patients, as well as in the CC and the middle cerebral peduncle. They showed the FA was lowered in the splenium of the CC and right external capsule in NPH patients with higher gait disturbance. Another study of WM integrity using DTI parameters like MD, FA, radial diffusivity (RD), and axial diffusivity showed a higher FA, RD, and MD in the corona radiata in periventricular fibers from the frontal and parietal cortices in NPH as compared to AD (68).
When attention is shifted to the structural degenerative markers that are seemingly similar in NPH and AD, ventriculomegaly emerges in the top spot. The CA has long been established as a direct marker that can capture if the ventricular enlargement is due to true hydrocephalus in NPH or a compensated enlargement due to atrophy in AD on MRI (69). This finding has been extensively validated, and even by more recent studies. The simpCA was also shown to be significantly lower in NPH as opposed to AD (26). Using manually annotated CA and EI-x measures on MRI images, an AUC of 0.96 was reported in distinguishing 36 definite NPH patients from 34 AD patients and 36 healthy controls (70). Even though a cut-off of 0.3 is usually recommended for the EI-x, it was found that a cut-off of 0.32 for the EI-x and 1000 for the CA maximized diagnostic accuracy, and the performance metrics were reported based on this classification. The EI-x cut-off of 0.3 has also been contested with a better proposal of age and sex specific values pointing to higher sensitivity (85). The anterior CA (ACA) was proposed and tested against the conventional CA, and EI-x on MRI scans in distinguishing NPH from AD and healthy controls (27). While it was significantly lower in NPH as compared to AD and healthy controls, it did not outperform the CA in diagnostic accuracy. A subsequent study of its association with gait impairment showed correlation with pre-surgery symptoms and post-operative improvement (86). Overall, we found that numerous distinctive features of NPH versus AD have been studied, but MRI is predominantly used as opposed to CT.
Parkinson’s disease (PD) is primarily diagnosed in a clinical setting through thorough examination of neurological symptoms that have motor manifestations like tremor, impairment of gait, arm-swing, balance, postural stability, and facial expression, and non-motor manifestations like impairment of behavior and cognition. Definitive diagnostic tests using blood, CSF, or imaging biomarkers do not currently exist (87). The manifestation of dementia in PD (PDD) patients (16) makes some patients more susceptible to misdiagnosis. There are reports that indicate that more than 15% of patients with PD may be misdiagnosed (88), with prominent misdiagnoses including AD (16). NPH may also be misdiagnosed as PD due to parkinsonism (89). Early diagnosis of this disease is challenged by the late manifestation of its defining motor symptoms, heterogeneity in clinical presentations, underlying mechanisms of its subtypes, age at onset, rate of progression, and response to treatment. This is also reflected in the heterogeneity of imaging features which correlate with symptomatic presentation (87).
As a direct consequence of the fact that the source of this synucleinopathy is known to primarily affect the substantia nigra (SN) and basal ganglia, and its microscopic magnitude of origin, imaging markers from structural imaging which rely on the scatter of external radiation like CT and MRI are not recommended for assessment of PD. Rather, functional imaging markers that directly correlate with the function at cellular levels by reflecting the uptake of specific radioactive tracers are the most viable option for detection, especially in early stages. In support of this claim is an article from Dalaker et al. (90) who found that global markers like atrophy and white matter hyperintensities were not significantly distinct in early PD as compared to healthy controls. Recently, Bae et al. (91) reviewed the degenerative markers of the SN on advanced imaging techniques like Nigrosome and Neuromelanin Imaging (NMI) using high field MRI techniques, Quantitative Iron Mapping (QMI), and Single Photon Emission Computed Tomography (SPECT). They highlight studies which have shown highly sensitive classification of PD when iron deposition in the SN driven by dopaminergic cell loss is used as a biomarker. In support of high field and neuromelanin sensitive MRI is a review from 2019 by Prange et al. (92) and from 2016 by Pagano et al. (93) Near normal or diffuse cortical atrophy is associated with PD (94), which raises the possibility of no visible markers of degeneration on CT or MRI. We investigate this further by providing the following review of structural imaging markers in PD and those that can distinguish it from NPH on MRI and CT sequences.
The presence of parkinsonian symptoms is not an uncommon occurrence in NPH (95), with case reports that were made as early as 1983 (96) which also recognized that it did not negatively impact shunt outcome. A 1994 report presented insight into the pathophysiological mechanisms of co-occurring hydrocephalus and parkinsonism manifesting as impairment of the nigrostriatal or neural circuits traversing the cortex, striatum, pallidus, and thalamus (97). Their proximity to the enlarged ventricles may introduce mass effects and ischemic changes. According to Akiguchi et al. (89) WM lesions and parkinsonism symptoms (prevalent in 71% of patients) in NPH were reversed after shunt surgery. Given this, differentiating NPH from PD, with which it is so frequently mistaken, is of paramount importance.
DTI has been shown to distinguish between NPH and PD using FA measures at the forceps major and minor, anterior thalamic radiations, CST, and superior longitudinal fasciculus by Marumoto et al. (71). Interestingly, they also found that the EI-x was significantly higher in NPH as compared to PD (100% sensitivity). The anterior thalamic radiation FA measure demonstrated higher specificity as compared to the EI-x in distinguishing NPH from PD. Ventricular dilation and atrophy have been demonstrated in PD (greater at baseline in those with dementia) on MRI (98), so Marumoto et al.’s (71) finding of a higher EI-x in NPH versus PD may suggest that ventricular enlargement in PD may not be as high as NPH. Measures of WM structural deformation and integrity measured through DTI have also been shown to distinguish between NPH and PD. The SA introduced by Chan et al. (30) was significantly higher in NPH versus PD. Kanno et al. (65) found lower FA and higher MD in the supratentorial WM in NPH when compared to PD. Visual evaluation of periventricular WM demonstrated significantly higher leukoaraiosis in NPH when compared to PDD and healthy controls (64). There are a limited number of studies which have examined the structural differentiation between NPH and PD, which may be a general reflection of the fact that structural imaging markers are discouraged in the assessment of PD.
Burton et al. (16) demonstrated GM and overall volume loss in PD as compared to healthy controls localized to the bilateral temporal and occipital lobes, thalami, right putamen, caudate tail, and middle-inferior frontal gyri. A review from 2017 highlights the structural markers of PD on MRI, with notable volumetric changes seen in the basal ganglia, GM volume loss in the frontal lobe, cingulate, temporal gyri, hippocampus, and loss of cortical thickness in specific frontal and occipital areas as compared to controls (99). Adding to the nuance which can be picked up on structural imaging, a recent study using MRI scans showed a difference in the amount and pattern of GM and cortical atrophy between patients with PD-without-dementia and healthy controls (100). As expected, pronounced structural effects were found in more severe manifestations of the disease. With a comprehensive classification system that factored clinical, demographic, and symptomatic presentations to categorize patients into mild and moderate–severe groups, they found significant differences only between the moderate–severe group and the healthy controls. The CC volume in the mid-anterior and central regions were found to be reduced in PD patients on MRI as compared to healthy controls by Goldman et al. (101). Shape changes and volume loss in the putamen, and shape changes in the caudate were shown to distinguish between PD and healthy controls (102). In a first attempt of its kind, a study from 1985 found that the size of the CSF spaces was increased in patients with PD when compared to normal controls on CT scans (103). Asymmetric ventricular enlargement was reported in PD using MRI scans (104), and later verified on 17 PD patients (105). Longitudinal atrophy and ventricular enlargement measured on MRI has been reported even in PD patients with dementia (106). Amidst the discouragement of structural imaging in the assessment of PD, textural features derived from first and second order grayscale/intensity statistics on T1-MRI scans were shown to be significantly associated with clinical features of PD by a 2021 study (107). In this highly welcome development, they showed that changes in the nigrostriatal pathway in early stages of PD could be captured through structural images, which was supported by correlation with motor symptoms. With these insights into the structural degradation in PD as opposed to normal controls, there is a considerable knowledge pool of structural markers that may be tested for their differentiative capacities from NPH.
Early adopters of semi-automatic algorithms included an effort to extract volumetric ventricular sizes and cortical thickness for distinction of NPH from AD, PD, and normal controls using MRI, and advocated for the ratio of ventricular size and cortical thickness as a better feature to distinguish between definite NPH (n = 5), from the rest, especially as ventricular volumes in NPH and AD may overlap (72). This problem has also been countered by considering the distribution of (normalized) CSF volumes rather than using it as a global measure, as shown by many studies so far. Voxel-based morphometry (VBM) has long been established as a reliable computational tool in MRI studies to assess structural markers of NPH. Yamashita et al. (76) analyzed CSF distribution using VBM on MRI scans and showed significant distinction between NPH (n = 12 with 83% probable NPH and 17% definite NPH) when compared to AD and normal controls in terms of LV/SF volumes, and HC/ML volumes. In a measure that reflects DESH, their analysis also showed that the volume of CSF in the LV and SF areas as compared to that in the HC and ML areas was higher in NPH as compared to AD and normal controls. Subsequently, they showed similar trends in those features on a definite NPH cohort, and when it was compared to PD patients (75).
Ishii et al. (74) developed an automatic volumetric CSF segmentation method on T1-MRI, which provided localization into the SF, HC, and ML sulci, as well as the ventricular spaces. They demonstrated the validation of previously known findings that enlarged ventricles and SF, and tight HC sulci were evident in a group of 15 probable NPH patients as opposed to AD and healthy controls. In a more targeted and automatic effort to segment GM, WM, and CSF spaces on T1-MRI, ventricular and GM volume, and gender were found to distinguish shunt-responsive NPH from AD and normal controls (73). Ellingsen et al. (108) developed a segmentation and labeling software to compartmentalize the ventricular system (into lateral, third, and fourth), referred to as RUDOLPH on MRI at a time when limited or no efforts were made for automatic segmentation of highly deformed ventricles. Yamada et al.’s studies on indices characterizing CSF spaces for the optimal distinction of probable NPH from healthy controls (29), AD, and NPH-and-AD cohorts on T2-MRI (38) were also based on semi-quantitative approaches relying on automatic segmentation of brain tissue. In a recent study of CSF distribution, the normalized WM and CSF volumes derived using VBM, along with the CA were shown to provide improved distinction between probable NPH and AD using MRI sequences when compared to the CA alone (77).
Peterson et al. (55) used an automatic segmentation method on T1-MRI to quantify volume in deep subcortical GM structures and showed reduced volume of the caudate, putamen, thalamus, nucleus accumbens, hippocampus, and pallidum in 14 NPH patients as compared to 8 healthy controls. Efforts apart from volumetry have also been made to extract nuanced MRI-based features. Statistical parametric methods using MD histogram analysis from DTI images have also been shown to distinguish between probable NPH and AD/PD/normal controls with minimal manual intervention (109).
Linear and interpretable measures of ventriculomegaly have also been computationally assessed on MRI. Borzage et al. (7) developed an automated methodology to extract CA from MRI from the Open Access Series of Imaging Studies (OASIS) and Alzheimer’s Disease Neuroimaging Initiative (ADNI) databases. With a high ICC of 0.9 between the automated measure and expert annotations on 281 images and an innovative approach to coronal pitch correction for image standardization, they showed the utility of data-driven applications in objective evaluation of diagnostic standard features. CT based methods for automatic assessment of interpretable measures have been limited. An automated image-processing methodology to extract the EI-x from CT images reported a correlation coefficient of 0.983 between the automated measure and expert annotations among 44 subjects (12 NPH). However, they applied nonlinear registration for image standardization which would render the brain width as a constant and affect the measurement of the EI-x (110).
Deep learning-based methods have shown promise in the objective and automatic assessment of NPH using structural imaging modalities. Again, MRI dominates this field of investigation. To enable the automatic segmentation and parcellation of the ventricular system in patients with severe ventriculomegaly due to hydrocephalus, Shao et al. (111) developed a deep learning model named VParNet trained on MRI scans of NPH patients and healthy controls, which showed high agreement with expert annotations and outperformed state-of-the-art. However, they did not test the classification capacity of their model. Irie et al. (112) developed a 3D convolutional-ladder network, and showed that their model can distinguish between probable NPH (n = 23), AD, and controls with an accuracy, sensitivity, and specificity of about 90% using MRI scans. By showing regions like the periventricular spaces, hippocampus, and THof the LVs being highlighted in the activation maps sensed by the network on some successfully classified scans, they demonstrated agreement with previous neuroanatomical findings in their findings.
Deep learning methods to assess NPH on CT scans have also emerged recently. Considering an EI-x ≥ 0.32 to be an indicator of hydrocephalus, a transfer learning scheme was applied on a large dataset of CT scans to show a classification performance with AUC of 0.93, sensitivity of 93.6%, and specificity of 94.4% in distinguishing hydrocephalus from normal controls (113). Automated segmentation of CSF, subarachnoid, and cerebral spaces on non-contrast CT scans of 27 patients with possible NPH, integrated with indirectly inferred connectome data, was shown to be as effective as the EI-x for prediction with a specificity of 85% and sensitivity of 86% (114). Haber et al. (115) recently developed a convolutional neural network (CNN) which was able to classify patients with definite improvement post-surgery as identified by the 2nd edition of the Japanese guidelines from healthy controls using CT scans setting a promising precedent in the application of deep learning to CT scans in NPH assessment. Further studies are required to study the potential of deep learning in assessing imaging markers that can predict positive and objective shunt response in symptomatic NPH and distinguish it from its mimics.
TBI casts a pervasive shadow, affecting an estimated 27 to 69 million individuals globally each year, with each case carrying significant chronic consequences (116, 117) and pathophysiological connections to various neurodegenerative diseases including NPH, AD, and PD. Its impact can range from concussions and diffuse axonal injury (DAI) which are harder to detect on structural imaging to extra-axial and intracerebral lesions that appear prominently. While acute injury is easily identified on CT and treated surgically, detecting (and differentiating between) its chronic degenerative consequences including atrophy and hydrocephalus which is crucial for optimal management may be challenging.
Subdural hemorrhage (SDH) refers to bleeding that occurs in the subdural space of the brain. And chronic SDHs (cSDH) represent these lesions which may evolve bilaterally in patients with symmetric cranial vaults, but most frequently occur on the side with higher frontal or occipital convexity. They may also be seen at interhemispheric locations in some cases (118). Even though intracranial hypotension and defective coagulation can cause cSDH, mild trauma to the head remains the predominant cause (119). Rupturing bridging veins in the subdural space following trauma may cause hematomas with varying cellular and vascular compositions as they evolve (118). It mostly affects older patients and is diagnosed with CT even though MRI might be more sensitive in isodense cases. Cerebral atrophy has been shown to be a risk factor for cSDH using volumetric analysis of CT scans (120), as well as being a prominent chronic consequence of it (121). Progressive volume loss in cSDH, at rates higher than dementia, have also been reported using volumetric analysis of CT scans (122). While hydrocephalus is also reported to be a risk factor for the development of cSDH following a minor head injury (123), there has been no compelling investigation into its development post cSDH.
Subarachnoid hemorrhage (SAH), which refers to bleeding in the space between the arachnoid and pia mater of the brain, is associated with secondary hydrocephalus (124) and atrophy (125). NPH was shown to develop in 21% of patients within a month following SAH, and improvement was noted in 85% of patients who underwent shunt surgery (126). While SAHs can occur due to nontraumatic causes, it is also estimated to occur in 33–60% of patients with moderate to severe TBI (127). Dilation of the LVs, as assessed with linear measures such as the bicaudate index and dilation rate assessed as change in volume over time on CT (124), atrophy measured indirectly as the modified cella media index (mCMI) and normalized CSF volume on T1-MRI (32), and parenchymal volume loss assessed through volumetric methods (128) are known structural markers of nontraumatic/spontaneous SAH. Hydrocephalus also occurs in traumatic SAH (13, 129, 130) which are usually found in the sulci at the convexities (131). Tian et al. (129) found that it may be correlated with intraventricular bleeding, severity of injury, thickness, and location of the lesion. Overall, we found that there are limited efforts to characterize and differentiate between the structural markers of hydrocephalus and atrophy following traumatic SAH. The prominent features of atrophic and hydrocephalic degradation in cTBI are summarized in Table 5.
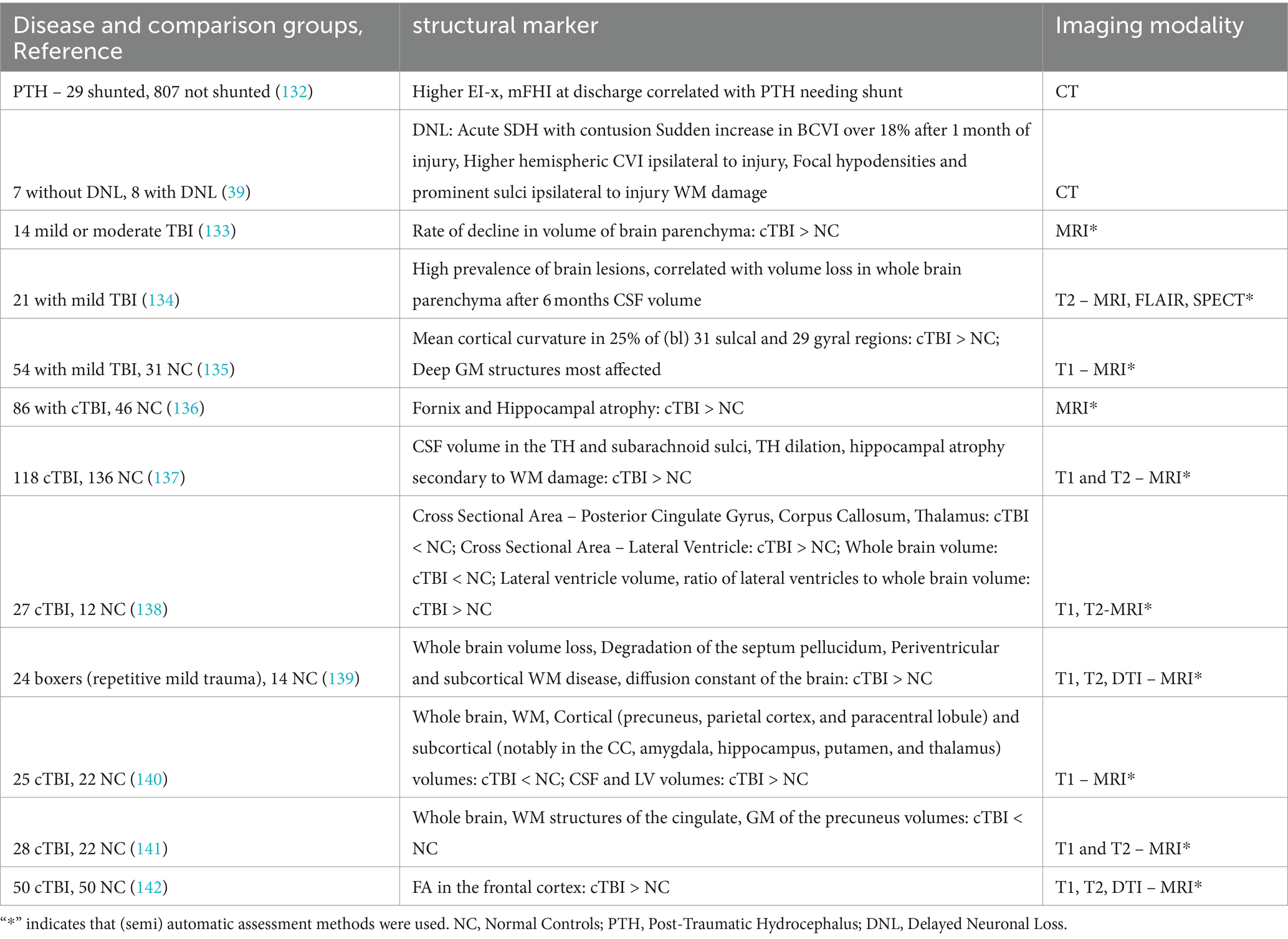
Table 5. Structural imaging markers of cTBI.
Hydrocephalus is known to be associated with TBI, irrespective of the presence of traumatic lesion (143). Therefore, it is pivotal to differentiate ventriculomegaly resulting from hydrocephalus and atrophy, as the former may be surgically treated. A call for this was made by Marmarou et al. (13) as early as 1996. In their study, 44% of patients with a severe head injury displayed ventriculomegaly (EI-x > 0.3), with 20% of them indicative of hydrocephalus as per CSF dynamics (monitored as intracranial pressure and CSF outflow resistance). Patients with an SAH showed a higher incidence of ventriculomegaly (80%) than those without (30.8%), and hydrocephalus was detected through CSF dynamics in both groups (50 and 9.1%, respectively). They described a methodology which combines the EI-x and CSF dynamics to classify patients as having high pressure hydrocephalus, NPH, or ventriculomegaly secondary to atrophy, and suggested shunting in the high pressure and normal pressure groups. The need for this distinction was reemphasized by Guyot and Michael (14) who also recognized that shunt-response was dependent on the distinction between symptomatic-hydrocephalic and atrophic ventriculomegaly (14), with the former group faring better.
A later study proposed a noninvasive selection criterion for shunt surgery in this group. 45% of patients with a severe TBI were found to have post-traumatic hydrocephalus, and it correlated with decreased perfusion in the temporal lobes, as seen on SPECT imaging 2–4 months after injury was found to improve post shunting (144). This imaging marker was dependent on functional imaging, but a valuable insight from this study is that even though hydrocephalus may develop within 3 months after injury, ventriculomegaly secondary to atrophy may not be seen until 6 months. This emphasizes the importance of longitudinal imaging to assess the nature of ventriculomegaly in chronic stages. In a recent finding and larger study (n = 836), the incidence of post-traumatic ventriculomegaly was found to be 46% in TBI patients (132). 3.5% of the patients in the study received shunts (post-traumatic hydrocephalus), with an improvement that was seen in 66%. The patients selected for shunting all displayed ventriculomegaly, but clinical decision based on symptoms was a predominant factor in their selection. Those with low pressure hydrocephalus had better outcomes, and the EI-x and modified frontal horn index (mFHI) were found to be higher in the acute phase for those who developed post-traumatic hydrocephalus.
In a study following patients with severe TBI, 88% displayed ventriculomegaly, and in 1–4 months after injury, a distinct atrophy/degradation termed as delayed neuronal loss (DNL) was observed in about 50% of patients through the bicaudate cerebroventricular index (BCVI) on CT scans. This measure progressed rapidly after 1 month of injury, indicating the sudden manifestation of DNL. Interestingly, acute SDH with contusion was the only contrasting finding between patients with DNL and those without it (39). Those patients’ CT findings also included the enlargement of the ipsilateral ventricle as measured by the hemispheric cerebroventricular index (CVI), a sudden appearance of a hypodense focal area ipsilateral to injury (confined to areas of the middle and anterior cerebral arteries) and WM damage as opposed to preserved cortical structures.
Whole brain atrophy has been an established marker of degradation in chronic TBI. Using analysis of MRI, it was found to occur post 11 months of injury and was correlated to loss of consciousness (133). In a prospective study of young patients with mild TBI, even though their neurocognitive profiles were normal, it was found that lesions on MRI (T2-weighted) were associated with whole brain atrophy 6 months post injury, emphasizing the essentiality of radiological follow-up in the post-traumatic course after an initial injury is detected (134). Another structural marker which was found to be distinct in mTBI was the mean cortical curvature of various bilateral cortical structures as measured on MRI. This feature is different from the global volumetric ones, in the aspect of quantifying region-specific pattern of atrophy (135).
Evidence of degradation in specific cortical and subcortical structures has also been abundantly described over the years. Another study which conducted MRI analysis of TBI subjects after 2 months of injury found atrophy in the hippocampus and fornix as opposed to controls (136). An MRI-based tissue specific and volumetric analysis of the temporal lobe structures including the SF, hippocampus, THs of the LVs, temporal gyrus and sulcus, and temporal WM stem, showed that CSF volume was increased (in the THs, subarachnoid sulci) which was more related to WM damage than GM in TBI as opposed to controls (137). They also found that the TH dilation was more related to WM damage than hippocampal atrophy.
At a time when it was thought that medial structures were not as affected from TBI as compared to the frontal and temporal regions (which are more susceptible to TBI insult), an MRI based study showed that the cross-sectional area of the posterior cingulate gyrus (PCG), CC, and thalamus was reduced, and that of the LVs was increased in TBI patients as opposed to controls. As WM from the frontal, temporal, and hippocampal areas connect with the PCG, the authors suggested that these localized structural markers may capture trans-neuronal damage in TBI. The total brain volume was decreased, and the LV volume, and the ratio of the latter to the former were increased (138). A diffusion weighted imaging study of boxers showed increased diffusion indicative of microstructural damage, and MRI analysis (T1/T2/DWI/FLAIR) indicated age-inappropriate volume loss, degradation of the septum pellucidum, periventricular and subcortical WM disease as compared to controls (139). About 8 months following a TBI with axonal injury, whole brain atrophy and increased CSF volumes, cortical (precuneus, parietal cortex, and paracentral lobule) and subcortical atrophy (notably in the amygdala, hippocampus, putamen, and thalamus) localized to specific regions were found by analyzing MRI (T1-weighted) scans using a semi-automated morphometric analysis (140). Post 12 months after mild TBI, global brain atrophy, loss in volume of specific WM structures of the cingulate and precuneal GM was detected using T1-MRI (141). Cortical abnormalities may also be detected using diffusion measures such as increased FA in mild TBI (142). While hydrocephalus and (GM, WM) atrophy are well studied structural consequences of cTBI, studies of structural markers that can characterize their interplay in producing an appearance of ventriculomegaly are lacking.
Computational techniques like tensor-based morphometry (TBM) have been used on MRI (T1-weighted) scans to study localized volume loss in cTBI. WM structures including but not limited to the CC, subcortical structures like the caudate (middle and posterior) cingulate, thalamus, frontal and temporal neocortices, and the cerebellum, were shown to be affected after at-least 3 months of moderate–severe TBI as opposed to controls using this technology (145). Ventricular volume was also revealed to be enlarged. This pattern remained irrespective of the presence of macroscopic lesions. SIENA (146), an automated software for brain atrophy quantification on MRI was applied by Trivedi et al. (147), to show significantly higher brain volume decline in mild-to-severe TBI as opposed to normal controls. This software was also used to quantify longitudinal brain atrophy on MRI (T1-weighted) among severe TBI patients and revealed an association between higher rates of brain atrophy and injury severity, and that brain volume change was a better predictor of long-term functional outcome as compared to functional measures at 8 weeks post-injury (148). TBM revealed localized atrophy in the brain stem, thalamus, putamen, and WM structures like the cerebellar peduncles, internal and external capsules, CC, superior and inferior longitudinal fasciculus, and corona radiata as opposed to normal controls. A surface-based morphometry (SBM) study including DTI and high-resolution MRI revealed distinct cortical thinning, GM diffusivity, and loss of integrity in the pericortical WM in TBI patients (149). Developments in the use of computational tools for objective assessment of atrophy after mild TBI have also led to an FDA approved software. It was shown to reliably capture progressive volume loss, and demonstrated degradation in whole brain (parenchyma, CSF, WM), and regional (forebrain, cortical GM, cerebellum, brainstem) structures on T1-MRI as compared to normal controls (150). This tool was subsequently shown to be more sensitive to (progressive) atrophy and asymmetry detection than radiologist interpretations (151, 152). In a very interesting application of this tool to predict previous brain volumes based on current measures, the developers also showed that reliable estimates of brain volumes were obtained on normal subjects. And that TBI patients show rapid progression of cortical atrophy, as opposed to enlargement in the subcortical nuclei and infratentorial spaces, in the few months after injury. As in the case of distinguishing NPH from AD and PD, we found that computational methods to assess atrophy and hydrocephalus cTBI are predominantly MRI based, and deep learning based approaches are lacking.
There are abundant examinations into features that can classify between NPH and asymptomatic controls, but those that predict shunt response in symptomatic NPH have not been established. Imaging studies have typically focused on predicting probable NPH due to the apparently high clinical value. Therefore, prediction of tap-test/lumbar drain responses using structural neuroimaging markers as a non-invasive alternative for a preliminary assessment of shunt response is a well-studied topic. CSF space morphological features, characterizing the narrowing of the HC/ML sulci and higher SS, enlargement of the SF and lower SS, and vertical expansion of the LVs have been shown to be highly discriminative in predicting tap-test response. The EI-z and DESH capture them in a straightforward and interpretable manner, but the latter would benefit from a computational formulation. Benedetto et al. (35) proposed the SILVER index as a potential solution. However, localized measurements of SS require manual annotation which inevitably introduces observer variability and higher computational cost. Features characterizing GM and WM integrity have also been shown to correlate with tap-test response, but nonuniformity in scanner calibration, noise, and poor soft tissue resolution may impact such density-based measures on CT scans, which is additionally limited by the need for manual annotation on both CT and MRI scans for localized anatomical measurements.
While discriminating the tap-test response is important, the low sensitivity of the tap-test itself toward shunt response (153) suggests that features optimized to predict tap-test response might reflect or exaggerate the low sensitivity. The performance reports of imaging markers as predictors of shunt response in NPH have also been mixed. Features like the iNPH Radscale have shown prognostic value in discriminating shunt responsive from healthy individuals, but there is no compelling evidence that it can predict shunt response in symptomatic individuals. Additionally, response to shunting may depend upon many factors like post-surgery care, presence of comorbidities, physical therapy, shunt complications etc. which need to be considered in future studies. Optimizing the sensitivity of radiographic evaluation to predict NPH related signal whether it is possible, probable, or definite might enable higher screening and lower cases of underdiagnosis.
Addressing the high levels of misdiagnosis in NPH is also crucial to identify and treat patients with this reversible dementia. While features for the distinction of NPH from AD have been well established, we observe that there is a lack of neuroimaging studies to distinguish NPH from PD using structural imaging. Perhaps due to heavy reliance on levodopa response in patients with suspected PD or clinical symptoms. Clinicians and researchers alike must recognize that this is a suboptimal approach which may put true NPH patients at unnecessary risk due to levodopa side effects and delay treatment with shunt-surgery. We have identified features that are discriminative of PD from controls, which may be tested for their application of distinguishing NPH from it. We encourage researchers to explore computational approaches to fully explore the potential of structural imaging in distinguishing between NPH and PD. Shunt surgery is also capable of relieving post-traumatic hydrocephalus. But research is needed to test the potential of structural imaging markers in selecting patients for surgery, as it is riddled with the problem of distinguishing between atrophy and hydrocephalus following TBI. Unfortunately, in more than 20 years post Marmarou et al.’s (13) advocacy for the use of CSF dynamics in patient selection for shunting in post-traumatic hydrocephalus, an alternative solution with noninvasive markers has not been found.
It is also important to distinguish Long Standing Overt Ventriculomegaly in Adults (LOVA), which is a chronic form of hydrocephalus, from NPH. Most cases are thought to arise due to aqueductal stenosis and may have symptomatic overlap with NPH. Patients with LOVA may also see clinical improvement with shunt surgery (154, 155). It is crucial to differentiate it from NPH as it may be extremely sensitive to pressure variations, which needs to be considered while evaluating surgical treatment (endoscopic third ventriculostomy for LOVA versus ventriculoperitoneal shunt for NPH) options. Characteristic neuroimaging finds of LOVA include (third and lateral) ventriculomegaly, decreased prominence of cortical sulci, macrocephaly, and expansion of the sella turcica due to compensatory mechanisms (156). In cases where LOVA occurs with an open aqueduct, where it may be differentiated from Late Onset Idiopathic Aqueductal Stenosis (LIAS), it becomes more crucial to distinguish it from NPH due to their clinical and symptomatic overlap (157). ICP monitoring in LOVA patients was shown to correlate with patient conditions pre- and post-surgery (158), and CSF dynamics was recommended to differentiate them from NPH patients (159). A noninvasive and accurate diagnostic score consisting of clinical features like age, presence/absence of the Hakim triad, headache, nausea/vomit, and neuroradiological features (evaluated on MRI) like the head circumference, EI-x, 3 V width, DESH, sellar bone distortion with the bulging of the 3 V floor was proposed recently by Palandri et al. (157) which was shown to classify probable NPH patients from LOVA and LIAS patients with a high AUC of 0.97, sensitivity of 95.1%, and specificity of 90.6%. Higher values of this diagnostic score correlates with higher EI-x, 3 V width, head circumference, 3 V floor bulging, and lower prominence of DESH which incorporates distinctive neuroradiological findings in LOVA as opposed to NPH. More research is needed to identify imaging markers which can differentiate shunt-responsive NPH from LOVA/LIAS.
Even though the most prominent structural impact of NPH except for WM abnormality can be visualized on CT, most research studies lean toward MRI. We identify some CT based markers which have shown good predictive performance, and further encourage researchers to not only adapt MRI-based features to CT studies, but also develop CT-specific features for this application. CT-imaging biomarkers, as affordable, timely, and accessible diagnostic solutions, with fewer contraindications than MRI may offer a hopeful prospect. Even though MRI is the preferred mode of structural imaging due to its higher soft tissue resolution as opposed to CT, the development of computational tools to extract volumetric, intensity, and texture-based CT-features may reveal the potential in characterizing structural degeneration in NPH and its differential diagnosis from AD and PD. CT is the preferred mode of evaluation for acute TBI, but the distinction between atrophy and hydrocephalus in cTBI is still heavily studied only on MRI. Advances in computational tools, particularly in machine (deep) learning and image processing, may hold the key to discovering novel CT-based markers, and objectively extracting diagnostic standard markers for these conditions.
A popular choice in semi-automatic image processing methods is to integrate domain knowledge through the volumetric characterization of brain regions that are known to be affected. While this has been successful on MRI, obtaining pixel-level ground-truth for segmentation on CT is not only expensive, but difficult to create by visual inspection. Moreover, brain regions are impacted differently in different neuropathologies and developing individual segmentation-based approaches to capture them, and their interactions can be challenging and quickly add complexity. Architectures from CNN models with the inherent capacity to learn feature representations at increasing levels of abstraction, residual networks that utilize skip connections to solve the problem of vanishing gradients in deep architectures, and the U-Net and its variants that optimally integrate local and contextual features have been limited in the assessment of NPH, and mostly on MRI. The potential of such models in solving other problems such as differentiation of (shunt-responsive) NPH from AD/PD, and atrophy/hydrocephalus in cTBI on CT scans should be tested.
Our article has a few limitations. It is a narrative review. Even though the search strategy was methodical, it was not exhaustive in terms of databases as we only included PubMed. We did not conduct a dedicated search for articles pertaining to computational methods which have been reviewed in this paper, but they were isolated from the search described in the “Search Methodology” section.
Better recognition of (normal pressure) hydrocephalus is paramount for the timely management of patients with potentially reversible dementia or brain injury. Despite a plethora of knowledge on the discriminative anatomical markers of NPH, only a few like the EI-x, CA, and DESH have notably been included in diagnostic guidelines. While prediction of tap-test/shunt response may offer most assistance to clinicians, discriminating hydrocephalic pathology from irreversible atrophy is necessary to identify patients who may be surgically treated. Anatomical markers that can accurately predict shunt surgical response in symptomatic NPH are yet to be reliably established, which may be complicated by amount of pathological progression prior to surgery, comorbidities, and post-surgical care. Longitudinal evaluation of anatomical markers correlated with symptomatic progression before and after surgery may shed light on expected recovery and planning treatment options. Additionally, there is a clear under-utilization of CT based markers in distinguishing NPH from AD, and an overall lack of studies assessing its structural differentiation from PD. Investigations into the distinction of the chronic effects of TBI, namely atrophy and (normal pressure) hydrocephalus, using structural imaging markers is also a crucially unaddressed area which may help to identify patients whose symptoms may be alleviated with shunt placement. Computational tools like image processing may help with objective measurement of features that are correlated with NPH pathology on CT; and advances in deep learning may also highlight explainable features with potential for accurate diagnosis. In emergency settings, smaller community care centers, and hospitals that may not have access to advanced imaging and the expertise to assess them, automatic methods for assessing CT scans for the accurate detection of NPH or post-traumatic hydrocephalus may be of immense value in recognizing patients with reversible symptoms. Through this effort, we urge researchers to untangle the web connecting these neurodegenerative conditions, offering hope to millions, and potentially preventing countless more from stumbling down the treacherous path of structural neurodegeneration.
SKS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. JD: Conceptualization, Methodology, Project administration, Writing – original draft. RG: Conceptualization, Methodology, Writing – review & editing. SC: Investigation, Writing – original draft. RK: Methodology, Project administration, Resources, Supervision, Writing – review & editing. US: Conceptualization, Investigation, Methodology, Project administration, Resources, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. We thank the MN State Office of Higher Education for supporting this review.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kiefer, M, and Unterberg, A. The differential diagnosis and treatment of Normal-pressure hydrocephalus. Dtsch Arztebl Int. (2012) 109:15–25. quiz 26. doi: 10.3238/arztebl.2012.0015
2. Krauss, JK, and Halve, B. Normal pressure hydrocephalus: survey on contemporary diagnostic algorithms and therapeutic decision-making in clinical practice. Acta Neurochir. (2004) 146:379–88. doi: 10.1007/s00701-004-0234-3
3. Tisell, M, Höglund, M, and Wikkelsø, C. National and regional incidence of surgery for adult hydrocephalus in Sweden. Acta Neurol Scand. (2005) 112:72–5. doi: 10.1111/j.1600-0404.2005.00451.x
4. Klassen, BT, and Ahlskog, JE. Normal pressure hydrocephalus: how often does the diagnosis hold water? Neurology. (2011) 77:1119–25. doi: 10.1212/WNL.0b013e31822f02f5
5. Andersson, J, Rosell, M, Kockum, K, Lilja-Lund, O, Söderström, L, and Laurell, K. Prevalence of idiopathic normal pressure hydrocephalus: a prospective, population-based study. PLoS One. (2019) 14:e0217705. doi: 10.1371/journal.pone.0217705
6. Oike, R, Inoue, Y, Matsuzawa, K, and Sorimachi, T. Screening for idiopathic normal pressure hydrocephalus in the elderly after falls. Clin Neurol Neurosurg. (2021) 205:106635. doi: 10.1016/j.clineuro.2021.106635
7. Borzage, M, Saunders, A, Hughes, J, McComb, JG, Blüml, S, and King, KS. The first examination of diagnostic performance of automated measurement of the callosal angle in 1856 elderly patients and volunteers indicates that 12.4% of exams met the criteria for possible normal pressure hydrocephalus. AJNR Am J Neuroradiol. (2021) 42:1942–8. doi: 10.3174/ajnr.A7294
8. Hydrocephalus Association. (2022). What is normal pressure hydrocephalus (NPH)? Available at: https://www.hydroassoc.org/about-normal-pressure-hydrocephalus/ (Accessed July 4, 2022)
9. Feigin, VL, Vos, T, Nichols, E, Owolabi, MO, Carroll, WM, Dichgans, M, et al. The global burden of neurological disorders: translating evidence into policy. Lancet Neurol. (2020) 19:255–65. doi: 10.1016/S1474-4422(19)30411-9
10. Gavrilov, GV, Gaydar, BV, Svistov, DV, Korovin, AE, Samarcev, IN, Churilov, LP, et al. Idiopathic normal pressure hydrocephalus (Hakim-Adams syndrome): clinical symptoms, diagnosis, and treatment. Psychiatr Danub. (2019) 31:737–44.
11. Sahuquillo, J, and Poca, MA. To shunt or not to shunt patients with idiopathic Normal pressure hydrocephalus? A reappraisal of an old question. J Clin Med. (2020) 9:4120. doi: 10.3390/jcm9124120
12. Adams, R, Fisher, C, Hakim, S, Ojemann, R, and Sweet, W. Symptomatic occult hydrocephalus with Normal cerebrospinal-fluid pressure. N Engl J Med. (1965) 273:117–26. doi: 10.1056/NEJM196507152730301
13. Marmarou, A, Abd-Elfattah Foda, MA, Bandoh, K, Yoshihara, M, Yamamoto, T, Tsuji, O, et al. Posttraumatic ventriculomegaly: hydrocephalus or atrophy? A new approach for diagnosis using CSF dynamics. J Neurosurg. (1996) 85:1026–35. doi: 10.3171/jns.1996.85.6.1026
14. Guyot, LL, and Michael, DB. Post-traumatic hydrocephalus. Neurol Res. (2000) 22:25–8. doi: 10.1080/01616412.2000.11741034
15. Risacher, SL, and Saykin, AJ. Neuroimaging biomarkers of neurodegenerative diseases and dementia. Semin Neurol. (2013) 33:386–416. doi: 10.1055/s-0033-1359312
16. Burton, EJ, McKeith, IG, Burn, DJ, Williams, ED, and O'Brien, JT. Cerebral atrophy in Parkinson's disease with and without dementia: a comparison with Alzheimer's disease, dementia with Lewy bodies and controls. Brain. (2004) 127:791–800. doi: 10.1093/brain/awh088
17. Das, JM, and Biagioni, MC. Normal pressure hydrocephalus. In: StatPearls. Treasure Island, FL: StatPearls Publishing (2024).
18. Sheridan, PL, Solomont, J, Kowall, N, and Hausdorff, JM. Influence of executive function on locomotor function: divided attention increases gait variability in Alzheimer's disease. J Am Geriatr Soc. (2003) 51:1633–7. doi: 10.1046/j.1532-5415.2003.51516.x
19. Váradi, C . Clinical features of Parkinson's disease: the evolution of critical symptoms. Biology. (2020) 9:103. doi: 10.3390/biology9050103
20. Aarsland, D, Andersen, K, Larsen, JP, Lolk, A, and Kragh-Sørensen, P. Prevalence and characteristics of dementia in Parkinson disease: an 8-year prospective study. Arch Neurol. (2003) 60:387–92. doi: 10.1001/archneur.60.3.387
21. Dever, A, Powell, D, Graham, L, Mason, R, Das, J, Marshall, SJ, et al. Gait impairment in traumatic brain injury: a systematic review. Sensors. (2022) 22:1480. doi: 10.3390/s22041480
22. Barman, A, Chatterjee, A, and Bhide, R. Cognitive impairment and rehabilitation strategies after traumatic brain injury. Indian J Psychol Med. (2016) 38:172–81. doi: 10.4103/0253-7176.183086
23. Pyrgelis, E-S, Velonakis, G, Papageorgiou, SG, Stefanis, L, Kapaki, E, and Constantinides, VC. Imaging markers for Normal pressure hydrocephalus: an overview. Biomedicines. (2023) 11:1265. doi: 10.3390/biomedicines11051265
24. Yin, R, Wen, J, and Wei, J. Progression in neuroimaging of Normal pressure hydrocephalus. Front Neurol. (2021) 12:700269. doi: 10.3389/fneur.2021.700269
25. Damasceno, BP . Neuroimaging in normal pressure hydrocephalus. Dement Neuropsychol. (2015) 9:350–5. doi: 10.1590/1980-57642015DN94000350
26. Cagnin, A, Simioni, M, Tagliapietra, M, Citton, V, Pompanin, S, Della Puppa, A, et al. A simplified callosal angle measure best differentiates idiopathic-Normal pressure hydrocephalus from neurodegenerative dementia. J Alzheimers Dis. (2015) 46:1033–8. doi: 10.3233/JAD-150107
27. Mantovani, P, Albini-Riccioli, L, Giannini, G, Milletti, D, Sorenson, TJ, Stanzani-Maserati, M, et al. Anterior callosal angle: a new marker of idiopathic normal pressure hydrocephalus? World Neurosurg. (2020) 139:e548–52. doi: 10.1016/j.wneu.2020.04.085
28. Huh, PW, Yoo, DS, Cho, KS, Park, CK, Kang, SG, Park, YS, et al. Diagnostic method for differentiating external hydrocephalus from simple subdural hygroma. J Neurosurg. (2006) 105:65–70. doi: 10.3171/jns.2006.105.1.65
29. Yamada, S, Ishikawa, M, and Yamamoto, K. Optimal diagnostic indices for idiopathic Normal pressure hydrocephalus based on the 3D quantitative volumetric analysis for the cerebral ventricle and subarachnoid space. AJNR Am J Neuroradiol. (2015) 36:2262–9. doi: 10.3174/ajnr.A4440
30. Chan, LL, Chen, R, Li, H, Lee, AJY, Go, WY, Lee, W, et al. The splenial angle: a novel radiological index for idiopathic normal pressure hydrocephalus. Eur Radiol. (2021) 31:9086–97. doi: 10.1007/s00330-021-07871-4
31. Ryska, P, Slezak, O, Eklund, A, Malm, J, Salzer, J, and Zizka, J. Radiological markers of idiopathic normal pressure hydrocephalus: relative comparison of their diagnostic performance. J Neurol Sci. (2020) 408:116581. doi: 10.1016/j.jns.2019.116581
32. Bendel, P, Koivisto, T, Aikiä, M, Niskanen, E, Könönen, M, Hänninen, T, et al. Atrophic enlargement of CSF volume after subarachnoid hemorrhage: correlation with neuropsychological outcome. AJNR Am J Neuroradiol. (2010) 31:370–6. doi: 10.3174/ajnr.A1804
33. Kojoukhova, M, Koivisto, AM, Korhonen, R, Remes, AM, Vanninen, R, Soininen, H, et al. Feasibility of radiological markers in idiopathic Normal pressure hydrocephalus. Acta Neurochir. (2015) 157:1709–19. doi: 10.1007/s00701-015-2503-8
34. Hashimoto, M, Ishikawa, M, Mori, E, and Kuwana, N. Study of INPH on neurological improvement (SINPHONI). Diagnosis of idiopathic normal pressure hydrocephalus is supported by MRI-based scheme: a prospective cohort study. Cerebrospinal Fluid Res. (2010) 7:18. doi: 10.1186/1743-8454-7-18
35. Benedetto, N, Gambacciani, C, Aquila, F, Di Carlo, DT, Morganti, R, and Perrini, P. A new quantitative method to assess disproportionately enlarged subarachnoid space (DESH) in patients with possible idiopathic normal pressure hydrocephalus: the SILVER index. Clin Neurol Neurosurg. (2017) 158:27–32. doi: 10.1016/j.clineuro.2017.04.015
36. He, W, Fang, X, Wang, X, Gao, P, Gao, X, Zhou, X, et al. A new index for assessing cerebral ventricular volume in idiopathic Normal-pressure hydrocephalus: a comparison with Evans’ index. Neuroradiology. (2020) 62:661–7. doi: 10.1007/s00234-020-02361-8
37. Kockum, K, Lilja-Lund, O, Larsson, EM, Rosell, M, Söderström, L, Virhammar, J, et al. The idiopathic normal-pressure hydrocephalus Radscale: a radiological scale for structured evaluation. Eur J Neurol. (2018) 25:569–76. doi: 10.1111/ene.13555
38. Yamada, S, Ishikawa, M, and Yamamoto, K. Comparison of CSF distribution between idiopathic Normal pressure hydrocephalus and Alzheimer disease. AJNR Am J Neuroradiol. (2016) 37:1249–55. doi: 10.3174/ajnr.A4695
39. Shiozaki, T, Akai, H, Taneda, M, Hayakata, T, Aoki, M, Oda, J, et al. Delayed hemispheric neuronal loss in severely head-injured patients. J Neurotrauma. (2001) 18:665–74. doi: 10.1089/089771501750357618
40. Jaraj, D, Rabiei, K, Marlow, T, Jensen, C, Skoog, I, and Wikkelsø, C. Prevalence of idiopathic Normal-pressure hydrocephalus. Neurology. (2014) 82:1449–54. doi: 10.1212/WNL.0000000000000342
41. Skalický, P, Mládek, A, Vlasák, A, De Lacy, P, Beneš, V, and Bradáč, O. Normal pressure hydrocephalus-an overview of pathophysiological mechanisms and diagnostic procedures. Neurosurg Rev. (2020) 43:1451–64. doi: 10.1007/s10143-019-01201-5
42. Relkir, N, Marmarou, A, Klinge, P, Bergsneider, M, and Black, PM. Diagnosing idiopathic normal-pressure hydrocephalus. Neurosurgery. (2005) 57:S2–4. doi: 10.1227/01.NEU.0000168185.29659.C5
43. Nakajima, M, Yamada, S, Miyajima, M, Ishii, K, Kuriyama, N, Kazui, H, et al. Research committee of idiopathic normal pressure hydrocephalus. Guidelines for Management of Idiopathic Normal Pressure Hydrocephalus (third edition): endorsed by the Japanese Society of Normal Pressure Hydrocephalus. Neurol Med Chir. (2021) 61:63–97. doi: 10.2176/nmc.st.2020-0292
44. Fasano, A, Espay, AJ, Tang-Wai, DF, Wikkelsö, C, and Krauss, JK. Gaps, controversies, and proposed roadmap for research in Normal pressure hydrocephalus. Mov Disord. (2020) 35:1945–54. doi: 10.1002/mds.28251
45. Giordan, E, Palandri, G, Lanzino, G, Murad, MH, and Elder, BD. Outcomes and complications of different surgical treatments for idiopathic normal pressure hydrocephalus: a systematic review and meta-analysis. J Neurosurg. (2019) 131:1024–36. doi: 10.3171/2018.5.JNS1875
46. Andrén, K, Wikkelsø, C, Tisell, M, and Hellström, P. Natural course of idiopathic normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry. (2014) 85:806–10. doi: 10.1136/jnnp-2013-306117
47. Kotagal, V, Walkowiak, E, and Heth, JA. Serious adverse events following Normal pressure hydrocephalus surgery. Clin Neurol Neurosurg. (2018) 170:113–5. doi: 10.1016/j.clineuro.2018.05.008
48. Isaacs, AM, Williams, MA, and Hamilton, MG. Current update on treatment strategies for idiopathic normal pressure hydrocephalus. Curr Treat Options Neurol. (2019) 21:65. doi: 10.1007/s11940-019-0604-z
49. Sasaki, M, Honda, S, Yuasa, T, Iwamura, A, Shibata, E, and Ohba, H. Narrow CSF space at high convexity and high midline areas in idiopathic normal pressure hydrocephalus detected by axial and coronal MRI. Neuroradiology. (2008) 50:117–22. doi: 10.1007/s00234-007-0318-x
50. Kockum, K, Virhammar, J, Riklund, K, Söderström, L, Larsson, EM, and Laurell, K. Diagnostic accuracy of the iNPH Radscale in idiopathic normal pressure hydrocephalus. PLoS One. (2020) 15:e0232275. doi: 10.1371/journal.pone.0232275
51. Sohn, GM, Bae, MJ, Park, J, and Kim, SE. Semi-quantitative analysis of periventricular gray-white matter ratio on CT in patients with idiopathic Normal pressure hydrocephalus. J Clin Neurosci. (2022) 101:16–20. doi: 10.1016/j.jocn.2022.04.036
52. Lv, M, Yang, X, Zhou, X, Chen, J, Wei, H, Du, D, et al. Gray matter volume of cerebellum associated with idiopathic Normal pressure hydrocephalus: a cross-sectional analysis. Front Neurol. (2022) 13:922199. doi: 10.3389/fneur.2022.922199
53. Golomb, J, de Leon, MJ, George, AE, Kluger, A, Convit, A, Rusinek, H, et al. Hippocampal atrophy correlates with severe cognitive impairment in elderly patients with suspected normal pressure hydrocephalus. J Neurol Neurosurg Psychiatry. (1994) 57:590–3. doi: 10.1136/jnnp.57.5.590
54. Adachi, M, Kawanami, T, Ohshima, F, and Kato, T. Upper midbrain profile sign and cingulate sulcus sign: MRI findings on sagittal images in idiopathic normal-pressure hydrocephalus, Alzheimer's disease, and progressive supranuclear palsy. Radiat Med. (2006) 24:568–72. doi: 10.1007/s11604-006-0074-6
55. Peterson, KA, Mole, TB, Keong, NCH, DeVito, EE, Savulich, G, Pickard, JD, et al. Structural correlates of cognitive impairment in normal pressure hydrocephalus. Acta Neurol Scand. (2019) 139:305–12. doi: 10.1111/ane.13052
56. Agerskov, S, Wallin, M, Hellström, P, Ziegelitz, D, Wikkelsö, C, and Tullberg, M. Absence of disproportionately enlarged subarachnoid space hydrocephalus, a sharp callosal angle, or other morphologic MRI markers should not be used to exclude patients with idiopathic Normal pressure hydrocephalus from shunt surgery. AJNR Am J Neuroradiol. (2019) 40:74–9. doi: 10.3174/ajnr.A5910
57. Kockum, K, Virhammar, J, Riklund, K, Söderström, L, Larsson, EM, and Laurell, K. Standardized image evaluation in patients with idiopathic normal pressure hydrocephalus: consistency and reproducibility. Neuroradiology. (2019) 61:1397–406. doi: 10.1007/s00234-019-02273-2
58. Carlsen, JF, Backlund, ADL, Mardal, CA, Taudorf, S, Holst, AV, Munch, TN, et al. Can shunt response in patients with idiopathic Normal pressure hydrocephalus be predicted from preoperative brain imaging? A retrospective study of the diagnostic use of the Normal pressure hydrocephalus Radscale in 119 patients. AJNR Am J Neuroradiol. (2022) 43:223–9. doi: 10.3174/ajnr.A7378
59. Mataró, M, Poca, MA, Matarín, M, Sahuquillo, J, Sebastián, N, and Junqué, C. Corpus callosum functioning in patients with Normal pressure hydrocephalus before and after surgery. J Neurol. (2006) 253:625–30. doi: 10.1007/s00415-005-0073-z
60. Yamamoto, D, Kazui, H, Wada, T, Nomura, K, Sugiyama, H, Shimizu, Y, et al. Association between milder brain deformation before a shunt operation and improvement in cognition and gait in idiopathic Normal pressure hydrocephalus. Dement Geriatr Cogn Disord. (2013) 35:197–207. doi: 10.1159/000347147
61. Holodny, AI, Waxman, R, George, AE, Rusinek, H, Kalnin, AJ, and de Leon, M. MR differential diagnosis of Normal-pressure hydrocephalus and Alzheimer disease: significance of Perihippocampal fissures. Am J Neuroradiol. (1998) 19:813–9.
62. Ishii, K, Kawaguchi, T, Shimada, K, Ohkawa, S, Miyamoto, N, Kanda, T, et al. Voxel-based analysis of gray matter and CSF space in idiopathic normal pressure hydrocephalus. Dement Geriatr Cogn Disord. (2008) 25:329–35. doi: 10.1159/000119521
63. Hong, YJ, Yoon, B, Shim, YS, Cho, AH, Lim, SC, Ahn, KJ, et al. Differences in microstructural alterations of the hippocampus in Alzheimer disease and idiopathic normal pressure hydrocephalus: a diffusion tensor imaging study. AJNR Am J Neuroradiol. (2010) 31:1867–72. doi: 10.3174/ajnr.A2207
64. Hattori, T, Yuasa, T, Aoki, S, Sato, R, Sawaura, H, Mori, T, et al. Altered microstructure in corticospinal tract in idiopathic normal pressure hydrocephalus: comparison with Alzheimer disease and Parkinson disease with dementia. AJNR Am J Neuroradiol. (2011) 32:1681–7. doi: 10.3174/ajnr.A2570
65. Kanno, S, Abe, N, Saito, M, Takagi, M, Nishio, Y, Hayashi, A, et al. White matter involvement in idiopathic normal pressure hydrocephalus: a voxel-based diffusion tensor imaging study. J Neurol. (2011) 258:1949–57. doi: 10.1007/s00415-011-6038-5
66. Hattori, T, Sato, R, Aoki, S, Yuasa, T, and Mizusawa, H. Different patterns of fornix damage in idiopathic normal pressure hydrocephalus and Alzheimer disease. AJNR Am J Neuroradiol. (2012) 33:274–9. doi: 10.3174/ajnr.A2780
67. Kang, K, Choi, W, Yoon, U, Lee, JM, and Lee, HW. Abnormal white matter integrity in elderly patients with idiopathic Normal-pressure hydrocephalus: a tract-based spatial statistics study. Eur Neurol. (2016) 75:96–103. doi: 10.1159/000443206
68. Hořínek, D, Štěpán-Buksakowska, I, Szabó, N, Erickson, BJ, Tóth, E, Šulc, V, et al. Difference in white matter microstructure in differential diagnosis of normal pressure hydrocephalus and Alzheimer's disease. Clin Neurol Neurosurg. (2016) 140:52–9. doi: 10.1016/j.clineuro.2015.11.010
69. Ishii, K, Kanda, T, Harada, A, Miyamoto, N, Kawaguchi, T, Shimada, K, et al. Clinical impact of the callosal angle in the diagnosis of idiopathic normal pressure hydrocephalus. Eur Radiol. (2008) 18:2678–83. doi: 10.1007/s00330-008-1044-4
70. Miskin, N, Patel, H, Franceschi, AM, Ades-Aron, B, Le, A, Damadian, BE, et al. Diagnosis of normal-pressure hydrocephalus: use of traditional measures in the era of volumetric MR imaging. Radiology. (2017) 285:197–205. doi: 10.1148/radiol.2017161216
71. Marumoto, K, Koyama, T, Hosomi, M, Kodama, N, Miyake, H, and Domen, K. Diffusion tensor imaging in elderly patients with idiopathic normal pressure hydrocephalus or Parkinson's disease: diagnosis of gait abnormalities. Fluids Barriers CNS. (2012) 9:20. doi: 10.1186/2045-8118-9-20
72. Moore, DW, Kovanlikaya, I, Heier, LA, Raj, A, Huang, C, Chu, KW, et al. A pilot study of quantitative MRI measurements of ventricular volume and cortical atrophy for the differential diagnosis of normal pressure hydrocephalus. Neurol Res Int. (2012) 2012:718150. doi: 10.1155/2012/718150
73. Serulle, Y, Rusinek, H, Kirov, II, Milch, H, Fieremans, E, Baxter, AB, et al. Differentiating shunt-responsive normal pressure hydrocephalus from Alzheimer disease and normal aging: pilot study using automated MRI brain tissue segmentation. J Neurol. (2014) 261:1994–2002. doi: 10.1007/s00415-014-7454-0
74. Ishii, K, Soma, T, Shimada, K, Oda, H, Terashima, A, and Kawasaki, R. Automatic volumetry of the cerebrospinal fluid space in idiopathic normal pressure hydrocephalus. Dement Geriatr Cogn Dis Extra. (2013) 3:489–96. doi: 10.1159/000357329
75. Yamashita, F, Sasaki, M, Saito, M, Mori, E, Kawaguchi, A, Kudo, K, et al. Voxel-based morphometry of disproportionate cerebrospinal fluid space distribution for the differential diagnosis of idiopathic normal pressure hydrocephalus. J Neuroimaging. (2014) 24:359–65. doi: 10.1111/jon.12049
76. Yamashita, F, Sasaki, M, Takahashi, S, Matsuda, H, Kudo, K, Narumi, S, et al. Detection of changes in cerebrospinal fluid space in idiopathic normal pressure hydrocephalus using voxel-based morphometry. Neuroradiology. (2010) 52:381–6. doi: 10.1007/s00234-009-0610-z
77. Li, H, Liu, C, Tai, H, Wei, Y, Shen, T, Yang, Q, et al. Comparison of cerebrospinal fluid space between probable normal pressure hydrocephalus and Alzheimer's disease. Front Aging Neurosci. (2023) 15:1241237. doi: 10.3389/fnagi.2023.1241237.6
78. Soria Lopez, JA, González, HM, and Léger, GC. Alzheimer's disease. Handb Clin Neurol. (2019) 167:231–55. doi: 10.1016/B978-0-12-804766-8.00013-3
79. Alzheimer’s Association. (2022). Alzheimer’s disease facts and figures [fact sheet]. Available at: https://www.alz.org/media/Documents/alzheimers-facts-and-figures.pdf.(Accessed February 01, 2024).
80. Querfurth, HW, and LaFerla, FM. Alzheimer's disease. N Engl J Med. (2010) 362:329–44. doi: 10.1056/NEJMra0909142
81. Hamilton, R, Patel, S, Lee, EB, Jackson, EM, Lopinto, J, Arnold, SE, et al. Lack of shunt response in suspected idiopathic normal pressure hydrocephalus with Alzheimer disease pathology. Ann Neurol. (2010) 68:535–40. doi: 10.1002/ana.22015
82. Jack, CR Jr, Mokri, B, Laws, ER Jr, Houser, OW, Baker, HL Jr, and Petersen, RC. MR findings in normal-pressure hydrocephalus: significance and comparison with other forms of dementia. J Comput Assist Tomogr. (1987) 11:923–31. doi: 10.1097/00004728-198711000-00001
83. Luetmer, PH, Huston, J, Friedman, JA, Dixon, GR, Petersen, RC, Jack, CR, et al. Measurement of cerebrospinal fluid flow at the cerebral aqueduct by use of phase-contrast magnetic resonance imaging: technique validation and utility in diagnosing idiopathic normal pressure hydrocephalus. Neurosurgery. (2002) 50:534–43; discussion: 543–4. doi: 10.1097/00006123-200203000-00020
84. Bateman, GA, and Loiselle, AM. Can MR measurement of intracranial hydrodynamics and compliance differentiate which patient with idiopathic normal pressure hydrocephalus will improve following shunt insertion? Acta Neurochir. (2007) 149:455–62. doi: 10.1007/s00701-007-1142-0
85. Brix, MK, Westman, E, Simmons, A, Ringstad, GA, Eide, PK, Wagner-Larsen, K, et al. The Evans' index revisited: new cut-off levels for use in radiological assessment of ventricular enlargement in the elderly. Eur J Radiol. (2017) 95:28–32. doi: 10.1016/j.ejrad.2017.07.013
86. Mantovani, P, Giannini, G, Milletti, D, Cevoli, S, Valsecchi, N, Gramegna, LL, et al. Anterior callosal angle correlates with gait impairment and fall risk in iNPH patients. Acta Neurochir. (2021) 163:759–66. doi: 10.1007/s00701-020-04699-7
87. Rizek, P, Kumar, N, and Jog, MS. An update on the diagnosis and treatment of Parkinson disease. CMAJ. (2016) 188:1157–65. doi: 10.1503/cmaj.151179
88. Rizzo, G, Copetti, M, Arcuti, S, Martino, D, Fontana, A, and Logroscino, G. Accuracy of clinical diagnosis of Parkinson disease: a systematic review and meta-analysis. Neurology. (2016) 86:566–76. doi: 10.1212/WNL.0000000000002350
89. Akiguchi, I, Ishii, M, Watanabe, Y, Watanabe, T, Kawasaki, T, Yagi, H, et al. Shunt-responsive parkinsonism and reversible white matter lesions in patients with idiopathic NPH. J Neurol. (2008) 255:1392–9. doi: 10.1007/s00415-008-0928-1
90. Dalaker, TO, Larsen, JP, Bergsland, N, Beyer, MK, Alves, G, Dwyer, MG, et al. Brain atrophy and white matter hyperintensities in early Parkinson's disease (a). Mov Disord. (2009) 24:2233–41. doi: 10.1002/mds.22754
91. Bae, YJ, Kim, JM, Sohn, CH, Choi, JH, Choi, BS, Song, YS, et al. Imaging the substantia nigra in Parkinson disease and other parkinsonian syndromes. Radiology. (2021) 300:260–78. doi: 10.1148/radiol.2021203341
92. Prange, S, Metereau, E, and Thobois, S. Structural imaging in Parkinson’s disease: new developments. Curr Neurol Neurosci Rep. (2019) 19:50–13. doi: 10.1007/s11910-019-0964-5
93. Pagano, G, Niccolini, F, and Politis, M. Imaging in Parkinson's disease. Clin Med. (2016) 16:371–5. doi: 10.7861/clinmedicine.16-4-371
94. Broski, SM, Hunt, CH, Johnson, GB, Morreale, RF, Lowe, VJ, and Peller, PJ. Structural and functional imaging in parkinsonian syndromes. Radiographics. (2014) 34:1273–92. doi: 10.1148/rg.345140009
95. Molde, K, Söderström, L, and Laurell, K. Parkinsonian symptoms in normal pressure hydrocephalus: a population-based study. J Neurol. (2017) 264:2141–8. doi: 10.1007/s00415-017-8598-5
96. Lobo Antunes, J, Fahn, S, and Cote, L. Normal pressure hydrocephalus and Parkinson's disease. J Neural Transm Suppl. (1983) 19:225–31.
97. Curran, T, and Lang, AE. Parkinsonian syndromes associated with hydrocephalus: case reports, a review of the literature, and pathophysiological hypotheses. Mov Disord. (1994) 9:508–20. doi: 10.1002/mds.870090503
98. Camicioli, R, Sabino, J, Gee, M, Bouchard, T, Fisher, N, Hanstock, C, et al. Ventricular dilatation and brain atrophy in patients with Parkinson’s disease with incipient dementia. Mov Disord. (2011) 26:1443–50. doi: 10.1002/mds.23700
99. Saeed, U, Compagnone, J, Aviv, RI, Strafella, AP, Black, SE, Lang, AE, et al. Imaging biomarkers in Parkinson's disease and parkinsonian syndromes: current and emerging concepts. Transl Neurodegener. (2017) 6:8. doi: 10.1186/s40035-017-0076-6
100. Filippi, M, Sarasso, E, Piramide, N, Stojkovic, T, Stankovic, I, Basaia, S, et al. Progressive brain atrophy and clinical evolution in Parkinson's disease. Neuroimage Clin. (2020) 28:102374. doi: 10.1016/j.nicl.2020.102374
101. Goldman, JG, Bledsoe, IO, Merkitch, D, Dinh, V, Bernard, B, and Stebbins, GT. Corpus callosal atrophy and associations with cognitive impairment in Parkinson disease. Neurology. (2017) 88:1265–72. doi: 10.1212/WNL.0000000000003764
102. Nemmi, F, Sabatini, U, Rascol, O, and Péran, P. Parkinson's disease and local atrophy in subcortical nuclei: insight from shape analysis. Neurobiol Aging. (2015) 36:424–33. doi: 10.1016/j.neurobiolaging.2014.07.010
103. Steiner, I, Gomori, JM, and Melamed, E. Features of brain atrophy in Parkinson’s disease – a CT scan study. Neuroradiology. (1985) 27:158–60. doi: 10.1007/BF00343788
104. Huang, X, Lee, YZ, McKeown, M, Gerig, G, Gu, H, Lin, W, et al. Asymmetrical ventricular enlargement in Parkinson's disease. Mov Disord. (2007) 22:1657–60. doi: 10.1002/mds.21626
105. Lewis, MM, Smith, AB, Styner, M, Gu, H, Poole, R, Zhu, H, et al. Asymmetrical lateral ventricular enlargement in Parkinson's disease. Eur J Neurol. (2009) 16:475–81. doi: 10.1111/j.1468-1331.2008.02430.x
106. Mak, E, Su, L, Williams, GB, Firbank, MJ, Lawson, RA, Yarnall, AJ, et al. Longitudinal whole-brain atrophy and ventricular enlargement in nondemented Parkinson's disease. Neurobiol Aging. (2017) 55:78–90. doi: 10.1016/j.neurobiolaging.2017.03.012
107. Betrouni, N, Moreau, C, Rolland, A-S, Carrière, N, Chupin, M, Kuchcinski, G, et al. Texture-based markers from structural imaging correlate with motor handicap in Parkinson’s disease. Sci Rep. (2021) 11:2724–4. doi: 10.1038/s41598-021-81209-4
108. Ellingsen, LM, Roy, S, Carass, A, Blitz, AM, Pham, DL, and Prince, JL. Segmentation and labeling of the ventricular system in normal pressure hydrocephalus using patch-based tissue classification and multi-atlas labeling. Proc SPIE Int Soc Opt Eng. (2016) 9784:97840G. doi: 10.1117/12.2216511
109. Ivkovic, M, Liu, B, Ahmed, F, Moore, D, Huang, C, Raj, A, et al. Differential diagnosis of normal pressure hydrocephalus by MRI mean diffusivity histogram analysis. AJNR Am J Neuroradiol. (2013) 34:1168–74. doi: 10.3174/ajnr.A3368
110. Takahashi, N, Kinoshita, T, Ohmura, T, Matsuyama, E, and Toyoshima, H. Automated method to compute Evans index for diagnosis of idiopathic normal pressure hydrocephalus on brain CT images In:. Medical imaging 2017: Computer-aided diagnosis, vol. 10134. Washington, DC: SPIE (2017). 600–6.
111. Shao, M, Han, S, Carass, A, Li, X, Blitz, AM, Shin, J, et al. Brain ventricle parcellation using a deep neural network: application to patients with ventriculomegaly. Neuroimage Clin. (2019) 23:101871. doi: 10.1016/j.nicl.2019.101871
112. Irie, R, Otsuka, Y, Hagiwara, A, Kamagata, K, Kamiya, K, Suzuki, M, et al. A novel deep learning approach with a 3D convolutional ladder network for differential diagnosis of idiopathic Normal pressure hydrocephalus and Alzheimer's disease. Magn Reson Med Sci. (2020) 19:351–8. doi: 10.2463/mrms.mp.2019-0106
113. Duan, W, Zhang, J, Zhang, L, Lin, Z, Chen, Y, Hao, X, et al. Evaluation of an artificial intelligent hydrocephalus diagnosis model based on transfer learning. Medicine. (2020) 99:e21229. doi: 10.1097/MD.0000000000021229
114. Zhang, A, Khan, A, Majeti, S, Pham, J, Nguyen, C, and Tran, P. Automated Segmentation and Connectivity Analysis for Normal Pressure Hydrocephalus. BME Front. (2022).
115. Haber, MA, Biondetti, GP, Gauriau, R, Comeau, DS, Chin, JK, Bizzo, BC, et al. Detection of idiopathic normal pressure hydrocephalus on head CT using a deep convolutional neural network. Neural Comput Applic. (2023) 35:9907–15. doi: 10.1007/s00521-023-08225-5
116. GBD 2016 Traumatic Brain Injury and Spinal Cord Injury Collaborators. Global, regional, and national burden of traumatic brain injury and spinal cord injury, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:56–87. doi: 10.1016/S1474-4422(18)30415-0
117. Dewan, MC, Rattani, A, Gupta, S, Baticulon, RE, Hung, YC, Punchak, M, et al. Estimating the global incidence of traumatic brain injury. J Neurosurg. (2018) 130:1080–97. doi: 10.3171/2017.10.JNS17352
118. Yadav, YR, Parihar, V, Namdev, H, and Bajaj, J. Chronic subdural hematoma. Asian. J Neurosurg. (2016) 11:330–42. doi: 10.4103/1793-5482.145102
119. Ou, Y, Yu, X, Liu, X, Jing, Q, Liu, B, and Liu, W. A comparative study of chronic subdural hematoma in patients with and without head trauma: a retrospective cross sectional study. Front Neurol. (2020) 11:588242. doi: 10.3389/fneur.2020.588242
120. Yang, AI, Balser, DS, Mikheev, A, Offen, S, Huang, JH, Babb, J, et al. Cerebral atrophy is associated with development of chronic subdural haematoma. Brain Inj. (2012) 26:1731–6. doi: 10.3109/02699052.2012.698364
121. Tomita, H, Tone, O, and Ito, U. Hemispheric cerebral atrophy after traumatic extra-axial hematoma in adults. Neurol Med Chir. (1997) 37:819–24. doi: 10.2176/nmc.37.819
122. Bin Zahid, A, Balser, D, Thomas, R, Mahan, MY, Hubbard, ME, and Samadani, U. Increase in brain atrophy after subdural hematoma to rates greater than associated with dementia. J Neurosurg. (2018) 129:1579–87. doi: 10.3171/2017.8.JNS17477
123. Tseng, JH, Tseng, MY, Liu, AJ, Lin, WH, Hu, HY, and Hsiao, SH. Risk factors for chronic subdural hematoma after a minor head injury in the elderly: a population-based study. Biomed Res Int. (2014) 2014:218646. doi: 10.1155/2014/218646
124. Chen, S, Luo, J, Reis, C, Manaenko, A, and Zhang, J. Hydrocephalus after subarachnoid hemorrhage: pathophysiology, diagnosis, and treatment. Biomed Res Int. (2017) 2017:8584753–8. doi: 10.1155/2017/8584753
125. Tam, AK, Kapadia, A, Ilodigwe, D, Li, Z, Schweizer, TA, and Macdonald, RL. Impact of global cerebral atrophy on clinical outcome after subarachnoid hemorrhage. J Neurosurg. (2013) 119:198–206. doi: 10.3171/2013.3.JNS121950
126. Fujita, K, Kusunoki, T, Noda, M, Hirayama, A, Tamaki, N, and Matsumoto, S. Normal pressure hydrocephalus (NPH) following subarachnoid hemorrhage (SAH)-clinical consideration of CT and development of hydrocephalus after SAH (author's transl). No To Shinkei. (1981) 33:845–51.
127. Griswold, DP, Fernandez, L, and Rubiano, AM. Traumatic subarachnoid hemorrhage: a scoping review. J Neurotrauma. (2022) 39:35–48. doi: 10.1089/neu.2021.0007
128. Gama Lobo, G, and Fragata, I. Long-term global and focal cerebral atrophy in perimesencephalic subarachnoid hemorrhage-a case-control study. Neuroradiology. (2022) 64:669–74. doi: 10.1007/s00234-021-02804-w
129. Tian, HL, Xu, T, Hu, J, Cui, YH, Chen, H, and Zhou, LF. Risk factors related to hydrocephalus after traumatic subarachnoid hemorrhage. Surg Neurol. (2008) 69:241–6. doi: 10.1016/j.surneu.2007.02.032
130. Chen, KH, Lee, CP, Yang, YH, Yang, YH, Chen, CM, Lu, ML, et al. Incidence of hydrocephalus in traumatic brain injury: a nationwide population-based cohort study. Medicine. (2019) 98:e17568. doi: 10.1097/MD.0000000000017568
131. Kim, J, and Lee, SJ. Traumatic subarachnoid hemorrhage resulting from posterior communicating artery rupture. Int Med Case Rep J. (2020) 13:237–41. doi: 10.2147/IMCRJ.S254160
132. Wettervik, S, Lewén, A, and Enblad, P. Post-traumatic hydrocephalus-incidence, risk factors, treatment, and clinical outcome. Br J Neurosurg. (2022) 36:400–6. doi: 10.1080/02688697.2021.1967289
133. MacKenzie, JD, Siddiqi, F, Babb, JS, Bagley, LJ, Mannon, LJ, Sinson, GP, et al. Brain atrophy in mild or moderate traumatic brain injury: a longitudinal quantitative analysis. AJNR Am J Neuroradiol. (2002) 23:1509–15.
134. Hofman, PA, Stapert, SZ, van Kroonenburgh, MJ, Jolles, J, de Kruijk, J, and Wilmink, JT. MR imaging, single-photon emission CT, and neurocognitive performance after mild traumatic brain injury. AJNR Am J Neuroradiol. (2001) 22:441–9.
135. King, JB, Lopez-Larson, MP, and Yurgelun-Todd, DA. Mean cortical curvature reflects cytoarchitecture restructuring in mild traumatic brain injury. Neuroimage Clin. (2016) 11:81–9. doi: 10.1016/j.nicl.2016.01.003
136. Tate, DF, and Bigler, ED. Fornix and hippocampal atrophy in traumatic brain injury. Learn Mem. (2000) 7:442–6. doi: 10.1101/lm.33000
137. Bigler, ED, Anderson, CV, and Blatter, DD. Temporal lobe morphology in normal aging and traumatic brain injury. AJNR Am J Neuroradiol. (2002) 23:255–66.
138. Yount, R, Raschke, KA, Biru, M, Tate, DF, Miller, MJ, Abildskov, T, et al. Traumatic brain injury and atrophy of the cingulate gyrus. J Neuropsychiatry Clin Neurosci. (2002) 14:416–23. doi: 10.1176/jnp.14.4.416
139. Zhang, L, Ravdin, LD, Relkin, N, Zimmerman, RD, Jordan, B, Lathan, WE, et al. Increased diffusion in the brain of professional boxers: a preclinical sign of traumatic brain injury? AJNR Am J Neuroradiol. (2003) 24:52–7.
140. Warner, MA, Youn, TS, Davis, T, Chandra, A, Marquez de la Plata, C, Moore, C, et al. Regionally selective atrophy after traumatic axonal injury. Arch Neurol. (2010) 67:1336–44. doi: 10.1001/archneurol.2010.149
141. Zhou, Y, Kierans, A, Kenul, D, Ge, Y, Rath, J, Reaume, J, et al. Mild traumatic brain injury: longitudinal regional brain volume changes. Radiology. (2013) 267:880–90. doi: 10.1148/radiol.13122542
142. Ling, JM, Klimaj, S, Toulouse, T, and Mayer, AR. A prospective study of gray matter abnormalities in mild traumatic brain injury. Neurology. (2013) 81:2121–7. doi: 10.1212/01.wnl.0000437302.36064.b1
143. Poca, MA, Sahuquillo, J, Mataró, M, Benejam, B, Arikan, F, and Báguena, M. Ventricular enlargement after moderate or severe head injury: a frequent and neglected problem. J Neurotrauma. (2005) 22:1303–10. doi: 10.1089/neu.2005.22.1303
144. Mazzini, L, Campini, R, Angelino, E, Rognone, F, Pastore, I, and Oliveri, G. Posttraumatic hydrocephalus: a clinical, neuroradiologic, and neuropsychologic assessment of long-term outcome. Arch Phys Med Rehabil. (2003) 84:1637–41. doi: 10.1053/S0003-9993(03)00314-9
145. Kim, J, Avants, B, Patel, S, Whyte, J, Coslett, BH, Pluta, J, et al. Structural consequences of diffuse traumatic brain injury: a large deformation tensor-based morphometry study. NeuroImage. (2008) 39:1014–26. doi: 10.1016/j.neuroimage.2007.10.005
146. Smith, SM, De Stefano, N, Jenkinson, M, and Matthews, PM. Normalized accurate measurement of longitudinal brain change. J Comput Assist Tomogr. (2001) 25:466–75. doi: 10.1097/00004728-200105000-00022
147. Trivedi, MA, Ward, MA, Hess, TM, Gale, SD, Dempsey, RJ, Rowley, HA, et al. Longitudinal changes in global brain volume between 79 and 409 days after traumatic brain injury: relationship with duration of coma. J Neurotrauma. (2007) 24:766–71. doi: 10.1089/neu.2006.0205
148. Sidaros, A, Skimminge, A, Liptrot, MG, Sidaros, K, Engberg, AW, Herning, M, et al. Long-term global and regional brain volume changes following severe traumatic brain injury: a longitudinal study with clinical correlates. NeuroImage. (2009) 44:1–8. doi: 10.1016/j.neuroimage.2008.08.030
149. Turken, AU, Herron, TJ, Kang, X, O'Connor, LE, Sorenson, DJ, Baldo, JV, et al. Multimodal surface-based morphometry reveals diffuse cortical atrophy in traumatic brain injury. BMC Med Imaging. (2009) 9:20. doi: 10.1186/1471-2342-9-20
150. Ross, DE, Ochs, AL, Seabaugh, JM, DeMark, MF, Shrader, CR, Marwitz, JH, et al. Progressive brain atrophy in patients with chronic neuropsychiatric symptoms after mild traumatic brain injury: a preliminary study. Brain Inj. (2012) 26:1500–9. doi: 10.3109/02699052.2012.694570
151. Ross, DE, Ochs, AL, Seabaugh, JM, and Shrader, CR. Alzheimer's disease neuroimaging initiative. Man versus machine: comparison of radiologists' interpretations and neuro quant® volumetric analyses of brain MRIs in patients with traumatic brain injury. J Neuropsychiatry Clin Neurosci. (2013) 25:32–9. doi: 10.1176/appi.neuropsych.11120377
152. Ross, DE, Ochs, AL, DeSmit, ME, and Seabaugh, JM. Havranek MD Alzheimer’s disease neuroimaging initiative. Man versus machine part 2: comparison of Radiologists' interpretations and neuro quant measures of brain asymmetry and progressive atrophy in patients with traumatic brain injury. J Neuropsychiatry Clin Neurosci. (2015) 27:147–52. doi: 10.1176/appi.neuropsych.13040088
153. Marmarou, A, Bergsneider, M, Klinge, P, Relkin, N, and Black, PM. The value of supplemental prognostic tests for the preoperative assessment of idiopathic normal-pressure hydrocephalus. Neurosurgery. (2005) 57:S2-17–28. doi: 10.1227/01.NEU.0000168184.01002.60
154. Kiefer, M, Eymann, R, Steudel, WI, and Strowitzki, M. Gravitational shunt management of long-standing overt ventriculomegaly in adult (LOVA) hydrocephalus. J Clin Neurosci. (2005) 12:21–6. doi: 10.1016/j.jocn.2004.02.022
155. Ved, R, Leach, P, and Patel, C. Surgical treatment of long-standing overt ventriculomegaly in adults (LOVA). Acta Neurochir. (2017) 159:71–9. doi: 10.1007/s00701-016-2998-7
156. Oi, S, Shimoda, M, Shibata, M, Honda, Y, Togo, K, Shinoda, M, et al. Pathophysiology of long-standing overt ventriculomegaly in adults. J Neurosurg. (2000) 92:933–40. doi: 10.3171/jns.2000.92.6.0933
157. Palandri, G, Carretta, A, La Corte, E, Giannini, G, Martinoni, M, Mantovani, P, et al. Open-aqueduct LOVA, LIAS, iNPH: a comparative clinical-radiological study exploring the "grey zone" between different forms of chronic adulthood hydrocephalus. Acta Neurochir. (2022) 164:1777–88. doi: 10.1007/s00701-022-05215-9
158. Horcajadas Almansa, Á, Cordero Tous, N, Román Cutillas, A, Jorques Infante, A, Saura Rojas, E, Iáñez Velasco, B, et al. Utilidad de la monitorización de la presión intracraneal en pacientes con ventriculomegalia marcada de larga evolución [Usefulness of continuous intracranial pressure monitoring in long-standing overt ventriculomegaly in adults]. Neurocirugia. (2015) 26:64–72. doi: 10.1016/j.neucir.2014.07.002
Keywords: normal pressure hydrocephalus, Alzheimer’s dementia, Parkinson’s disease, chronic traumatic brain injury, structural imaging, computational methods
Citation: Kadaba Sridhar S, Dysterheft Robb J, Gupta R, Cheong S, Kuang R and Samadani U (2024) Structural neuroimaging markers of normal pressure hydrocephalus versus Alzheimer’s dementia and Parkinson’s disease, and hydrocephalus versus atrophy in chronic TBI—a narrative review. Front. Neurol. 15:1347200. doi: 10.3389/fneur.2024.1347200
Edited by:
Alba Scerrati, University of Ferrara, ItalyReviewed by:
Giulia Giannini, University of Bologna, ItalyCopyright © 2024 Kadaba Sridhar, Dysterheft Robb, Gupta, Cheong, Kuang and Samadani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Uzma Samadani, dXNhbWFkYW5AdW1uLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.