
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Neurol., 21 February 2024
Sec. Multiple Sclerosis and Neuroimmunology
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1341473
 Álvaro Cobo-Calvo1*
Álvaro Cobo-Calvo1* Rocío Gómez-Ballesteros2
Rocío Gómez-Ballesteros2 Aida Orviz3María Díaz Sánchez4Sabas Boyero5Marta Aguado-Valcarcel6María Sepúlveda7Pablo Rebollo8Paloma López-Laiz2
Aida Orviz3María Díaz Sánchez4Sabas Boyero5Marta Aguado-Valcarcel6María Sepúlveda7Pablo Rebollo8Paloma López-Laiz2 Jorge Maurino2
Jorge Maurino2 Nieves Téllez Lara9
Nieves Téllez Lara9Introduction and objective: Limited information is available on how neurologists make therapeutic decisions in neuromyelitis optica spectrum disorder (NMOSD), especially when new treatments with different mechanisms of action, administration, and safety profile are being approved. Decision-making can be complex under this uncertainty and may lead to therapeutic inertia (TI), which refers to lack of treatment initiation or intensification when therapeutic goals are not met. The study aim was to assess neurologists’ TI in NMOSD.
Methods: An online, cross-sectional study was conducted in collaboration with the Spanish Society of Neurology. Neurologists answered a survey composed of demographic characteristics, professional background, and behavioral traits. TI was defined as the lack of initiation or intensification with high-efficacy treatments when there is evidence of disease activity and was assessed through five NMOSD aquaporin-4 positive (AQP4+) simulated case scenarios. A multivariate logistic regression analysis was used to determine the association between neurologists’ characteristics and TI.
Results: A total of 78 neurologists were included (median interquartile range [IQR] age: 36.0 [29.0–46.0] years, 55.1% male, median [IQR] experience managing demyelinating conditions was 5.2 [3.0–11.1] years). The majority of participants were general neurologists (59.0%) attending a median (IQR) of 5.0 NMOSD patients (3.0–12.0) annually. Thirty participants (38.5%) were classified as having TI. Working in a low complexity hospital and giving high importance to patient’s tolerability/safety when choosing a treatment were predictors of TI.
Conclusion: TI is a common phenomenon among neurologists managing NMOSD AQP4+. Identifying TI and implementing specific intervention strategies may be critical to improving therapeutic decisions and patient care.
Neuromyelitis optica spectrum disorder (NMOSD) is a chronic and devastating autoimmune disease of the central nervous system characterized by inflammatory lesions mainly of the optic nerve and the spinal cord (1). Despite being considered as a rare disease (2), it is a serious condition, as permanent disability or even death are driven by relapses (3–5). Thus, the main therapeutic goal for patients with NMOSD is to reduce the frequency and severity of these episodes with the aim of avoiding long-term disability accumulation (6, 7).
Historically, NMOSD has been treated with off-label treatments, mainly immunosuppressants (ISTs), oral corticosteroids (OCs) or rituximab. However, in recent years, targeted high-efficacy therapies with a positive safety profile have been approved for its management (8). These new treatments have broadened the landscape of available options, but in turn may have complicated the decision-making process (9, 10). A consequence of this difficulty might be the presence of therapeutic inertia (TI) in decision-making, defined as the lack of treatment initiation or intensification when therapeutic goals are not met (11). In fact, TI has been shown to be present in more than half and up to 96% of treatment decisions in a demyelinating disease with multiple treatment choices such as multiple sclerosis (MS) (12). Several factors have been related to TI prevalence in MS, some influenced by neurologist’s professional experience, such as a lower volume of patients, not being an MS specialist, and fewer years of practice; and others by personality-related traits, namely an aversion to ambiguity and lower tolerance to uncertainty (13). However, what might be influencing TI is the complexity of decisions in MS due to the increasing availability of numerous different treatments and the limited training physicians receive in terms of decision-making processes and risk management in complex environments with multiple options and uncertainty (10). Furthermore, complicated treatment monitoring and fear of side effects have been related to TI as well (10, 14).
In a varying context in NMOSD aquaporin-4 positive (AQP4+) with a broadened therapeutic landscape, the lack of head-to-head trials to facilitate decisions, and no clear management guidelines, understanding the decision-making process and its contributors may be important to provide information on how these decisions are made and reach the best patient care approach. Thus, the aim of the present study was to assess the prevalence of TI and associated factors in the clinical decisions of neurologists caring for patients with NMOSD in Spain.
PREFERENCES-NMOSD was an online, non-interventional, cross-sectional, and exploratory study in collaboration with the Spanish Society of Neurology (SEN). From June 16th to September 27th, 2022, neurologists were invited to participate and proactively answered an online survey sent by email to provide details about their demographic characteristics, professional background, and behavioral traits. Being actively involved in the management of NMOSD patients at the time of the study was set as an inclusion criteria. The study was approved by the research ethics board of Hospital Universitario Clínico San Carlos, Madrid, Spain and performed in accordance with the 1964 Helsinki Declaration and its later amendments. All participants provided written informed consent.
We explored the prevalence of TI through five simulated NMOSD AQP4+ clinical practice case scenarios designed by the research team (Supplementary material). Treatment options for case scenarios were presented unbranded (Drug A-F) as in Table 1, mimicking the current available landscape of treatments for NMOSD. For its creation, we used the available scientific evidence of efficacy, safety, and route and frequency of administration from literature on clinical trials and off-label treatments (15–20).
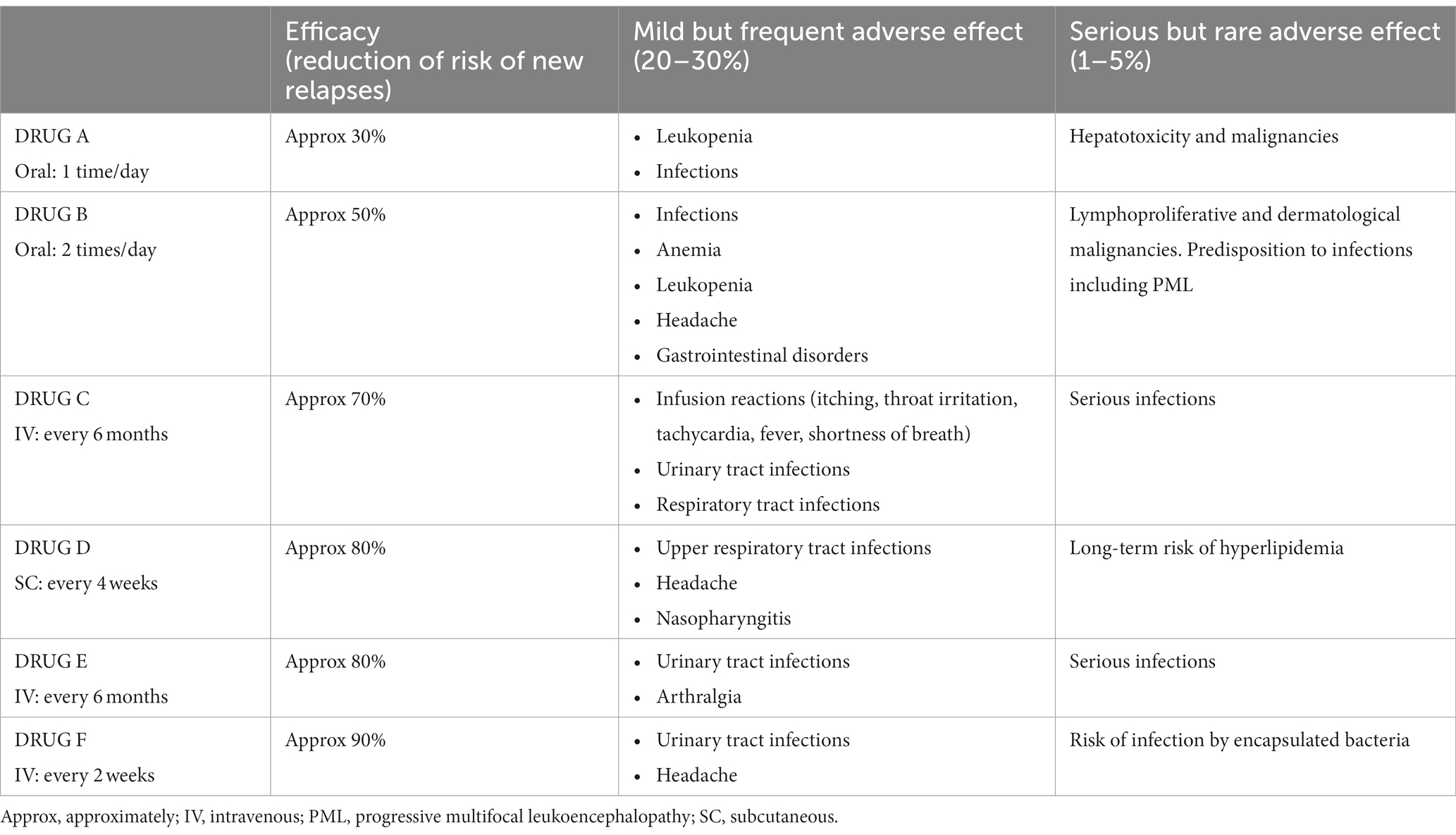
Table 1. Hypothetical treatments for case scenarios.
Due to the severity of NMOSD relapses and disability accumulation, we used a stricter definition of therapeutic inertia, described in our study as the lack of pursuit of high-efficacy treatments when there is evidence of disease activity (based on clinical course and neuroimaging markers) (21). For the same reason, we established the term therapeutic error (TE) for case scenarios where, despite evidence of disease activity, the decision was to deescalate to a lower efficacy treatment (cases 3 and 4). In our study, high-efficacy treatments were considered those having more than 70% of efficacy in reduction of risk of new relapses (22), that is, Drugs C- F in Table 1.
The Evidence-Based Practice Attitude Scale (EBPAS), Provider Decision Process Assessment Instrument (PDPAI), Jefferson Scale of Physician Empathy (JSPE), Regret Intensity Scale (RIS-10), General Risk Propensity Scale (GRiPS), and Reasons for Treatment Selection Questionnaire (RTSQ) were used to gather information on neurologists’ attitudes to innovation, decision-making comfort, empathy, care-related regret, risk attitude, and treatment decision, respectively.
The EBPAS is a validated questionnaire assessing the attitude toward the adoption of new treatments, interventions, and practices among healthcare professionals with 15 items divided into four subscales: Requirements, Appeal, Opening, and Divergence. Scores range from 0 (not at all) to 4 (to a very great extent), with higher scores indicating a more positive attitude toward innovation, except for Divergence (reversed) (23).
The PDPAI is a 12-item questionnaire measuring healthcare professional comfort regarding a medical decision. In our study, neurologists were asked to think about their contentment when making medical decisions in NMOSD. Each item is scored using a 5-point Likert scale ranging from 1 (strongly agree) to 5 (strongly disagree). Total score ranged from 12 to 60 as a result of adding each item response after reversing some of the items. Lower scores imply a better decision-making process (24).
The JSPE assesses physicians’ empathy using 20 items scored on a 7-point Likert scale that ranges from 1 (strongly disagree) to 7 (strongly agree). Total score ranged from 20 to 140 after adding each item and reversing some of them. Higher scores are associated with a higher degree of empathy (25).
The RIS-10 assesses the intensity of care-related regret at the time of measurement caused by a past decision or event occurring up to 5 years earlier. Items are scored using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), with higher scores indicating higher intensity of regret (26).
The GRiPS is an 8-item questionnaire measuring the attitude to risk. Each item is assessed on a 5-point Likert scale from 1 (strongly disagree) to 5 (strongly agree), with higher scores meaning higher risk-taking behavior (27).
The RTSQ evaluates the reasons leading to a treatment decision with 22 items, which are grouped in 5 categories based on knowledge of recent empirical findings (theoretical), personal experiences (experiential), patient tolerance (situational), anticipation about the course of a therapy, and patient preferences (interactional). Each item is scored using a 5-point Likert scale ranging from 0 (irrelevant) to 4 (decisive) (28).
Demographic and clinical characteristics were summarized using frequencies (percentages) and mean (standard deviations). TI was considered to be present if there was at least one incorrect response based on the definition, and this was used to calculate the sample prevalence of TI. TE was present when the participant selected the second answer (Switch to drug B) in case scenarios 3 and 4.
Neurologists’ demographic, professional, and behavioral characteristics were compared among groups with presence/absence of TI using independent t-test for continuous variables and Chi-square test for categorical variables. Values of p < 0.05 were considered significant.
Demographic, professional and behavioral factors associated with the presence of TI were analyzed using univariate (association of the dichotomous outcome variable – presence of TI – with one predictor factor) and multivariate logistic regressions. Variables with value of p less than 0.1 in the univariate analysis were included in the multivariate model. Categorical variables were considered significant in the univariate model when at least one of the categories resulted significant. All variables (except type of hospital) were included as continuous. Odds ratios with 95% confidence intervals were derived.
A total of 1,400 neurologists were invited to participate through the Spanish Society of Neurology. Of those, 154 agreed to participate (11%), and 117 met selection criteria (8.4%). Finally, a total of 78 neurologists (5.6%) completed the therapeutic inertia assessment and were included in the study, representing a 13% of Spanish neurologists who potentially treat demyelinating conditions. The median [interquartile range (IQR)] age was 36.0 (29.0–46.0) years, 55.1% were male, and the median (IQR) time of experience managing demyelinating conditions was 5.2 (3.0–11.1) years. The majority of participants were general neurologists (59.0%) attending a median (IQR) of 5.0 (3.0–12.0) NMOSD patients annually. Demographic, professional, and other characteristics of the sample are shown in Table 2.
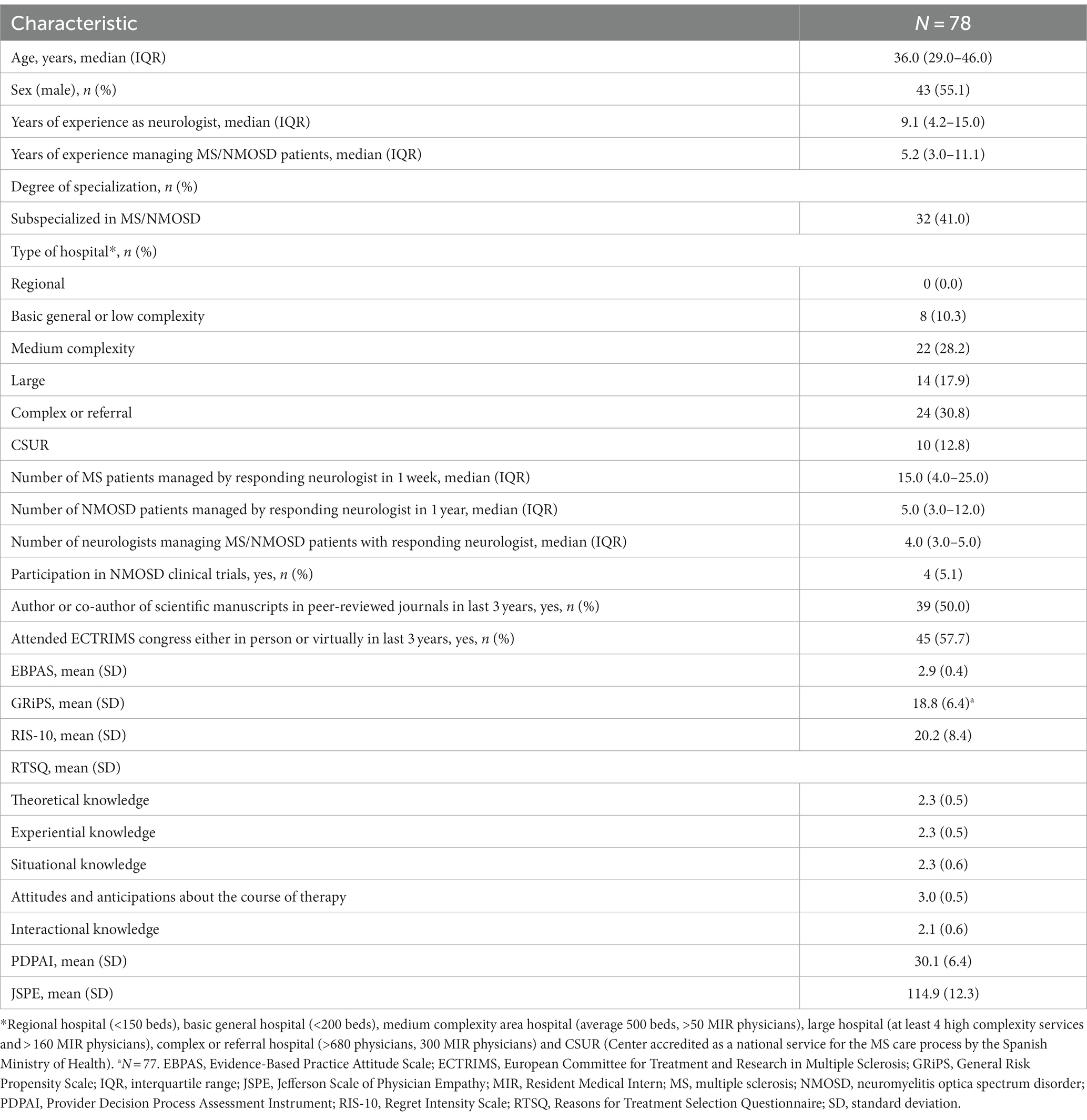
Table 2. Demographic and professional characteristics.
Thirty participants (38.5%) were classified as having TI in at least one of the presented case scenarios, and 10 participants (12.8%) in 2 or more responses (Table 3). Therapeutic error was found in seven participants (9%) in at least one of the case scenarios (cases 3 and 4). Using the classical definition of TI (not starting or escalating when therapeutic goals are not achieved) led to a similar percentage (32.1%, n = 25) of results.
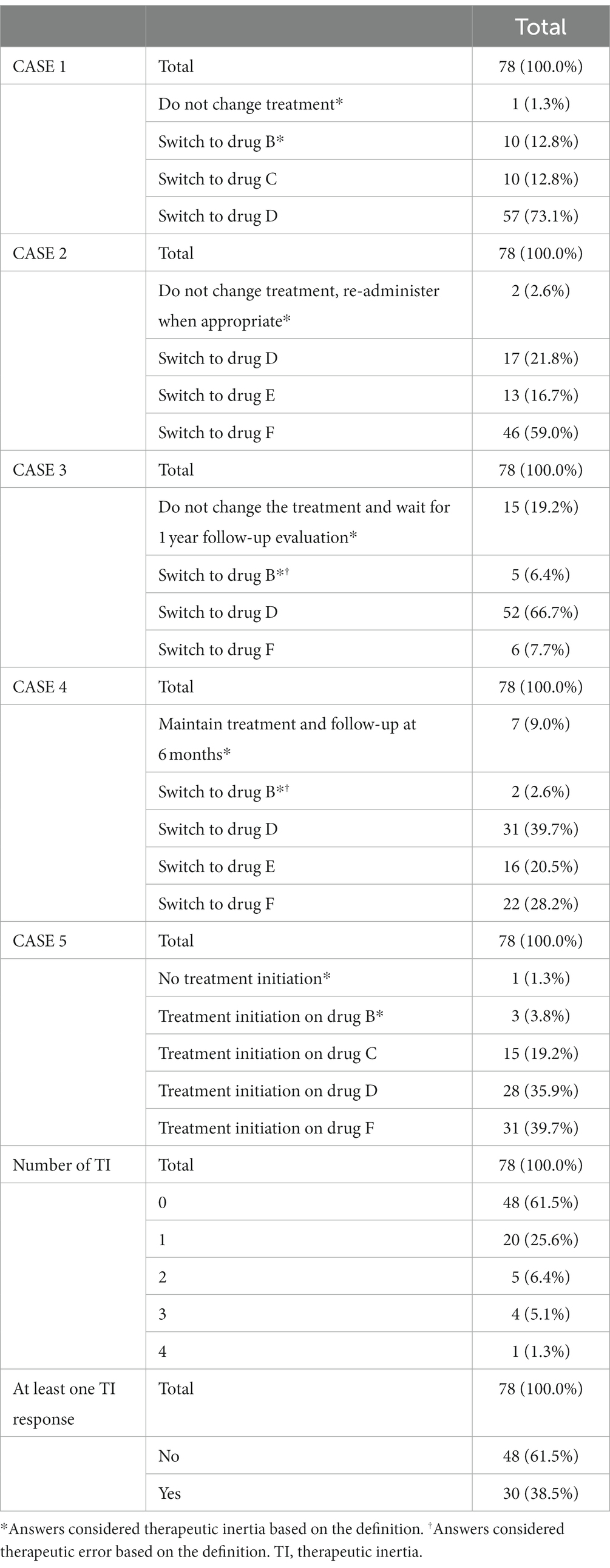
Table 3. Therapeutic inertia related to case scenarios.
Participants with TI showed a lower degree of empathy (JSPE scale; p = 0.0005) and perceived research-based interventions as not clinically useful and less important than clinical experience in the EBPAS scale (p = 0.0014). When choosing a treatment, neurologists with TI gave more importance to ease of use (RTSQ item 9; p = 0.0424), patient tolerability/safety (RTSQ item 5; p = 0.0057), or made the choice casually (RTSQ item 18; p = 0.0128), while giving lower importance to the existence of scientific evidence in favor of treatment in the RTSQ questionnaire (item 2; p = 0.0030) (Table 4).
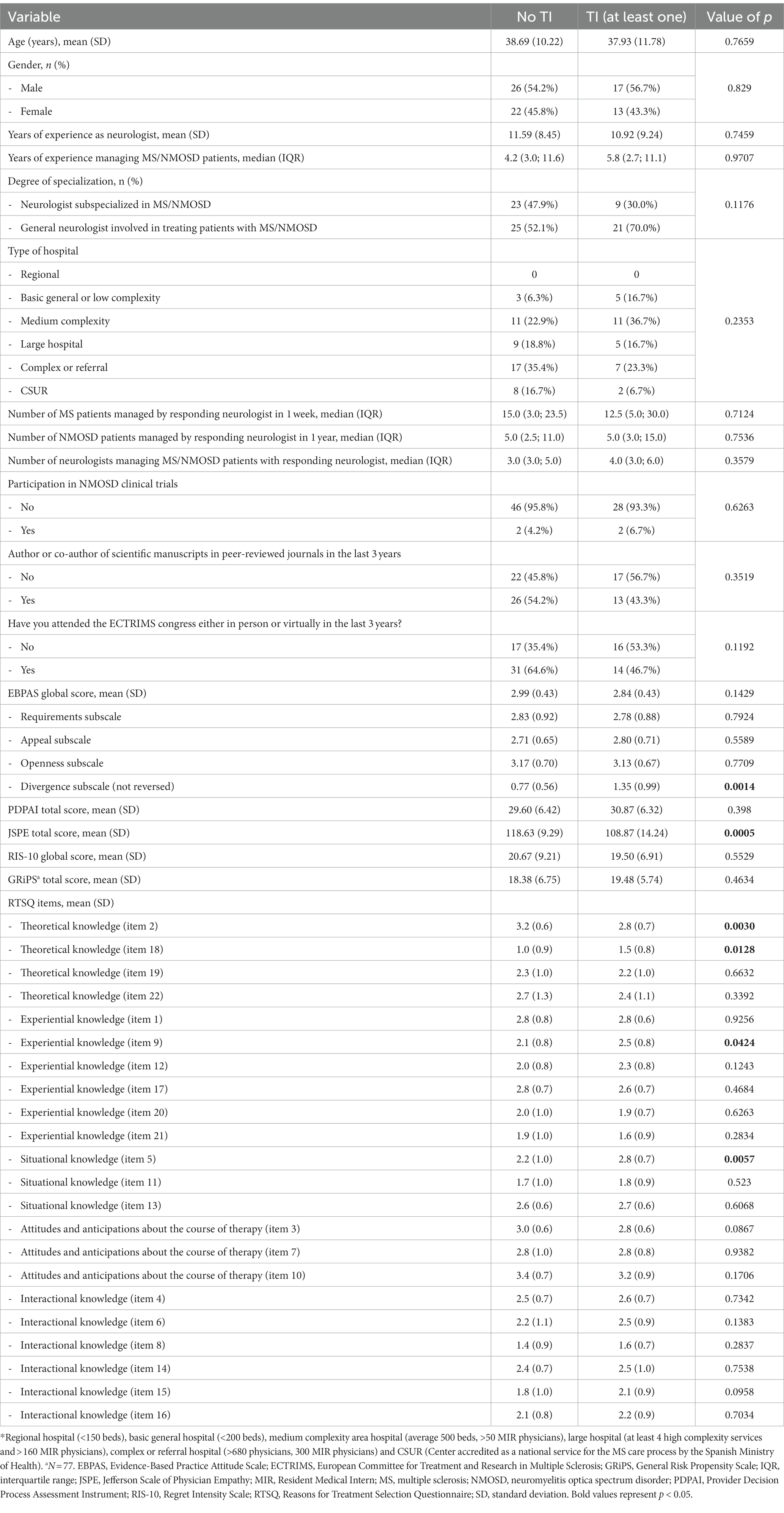
Table 4. Associations between demographic, professional and behavioral characteristics and therapeutic inertia (n = 78).
When evaluating neurologists’ characteristics predictive of TI, the binary regression univariate model found that working in a low complexity hospital (basic general hospital with less than 200 beds), perceiving research-based interventions as not clinically useful in the EBPAS scale, and showing a lower degree of empathy in the JSPE scale were associated to TI. Different items in the RTSQ scale were associated to TI as well, such as giving more importance to ease of use (item 9), patient tolerability/safety (item 5), or patient’s social factors (item 15) when choosing a treatment or making the choice casually (item 18), while giving lower importance to the existence of scientific evidence in favor of treatment (item 2). Finally, the multivariate analysis found that working in a low complexity hospital [OR = 104.394 (95% CI 1.67–999.99), p = 0.0276] and giving high importance to patient tolerability/safety when choosing a treatment [RTSQ item 5; OR = 32.04 (95% CI 3.25–315.57), p = 0.0030] were independently associated to the risk of TI.
Understanding the current treatment decision-making process in NMOSD is of significant relevance, as there are few consensus or management guidelines and new therapies have been approved for this condition in the last few years (6, 15, 29, 30). Due to the severity of relapses in this condition, which result in disability accumulation and can even lead to death (83% of patients with partial or no recovery from relapses and mortality rates vary from 3.3–25%) (3–5, 31, 32), we classified TI as not pursuing high-efficacy treatments when therapeutic goals are not met. We found that TI is a common phenomenon in the management of NMOSD patients, observed in more than one-third of participating neurologists. Factors associated with TI were working in a low complexity hospital and giving higher importance to patient tolerability/safety when choosing a treatment.
The management of patients with NMOSD has become more challenging with the approval of the first new therapies. Despite these advances in the last few years, there is little information on treatment decisions including new agents. In this study, we specifically assessed TI in NMOSD with unbranded treatments mimicking the available ones. Min et al. performed a clinical record review in six countries worldwide and found that relapses in NMOSD do not always lead to immediate initiation of maintenance therapy or a switch from off-label OC/ISTs to higher efficacy monoclonal antibodies (33). For newly diagnosed patients, they found that 47% did not receive maintenance treatment within 2 months of diagnosis for reasons such as disease stability, patient refusal and cost/access restrictions, being the severity of relapse a factor related to immediate treatment initiation (33). They also found that 32% of neurologists strongly agreed on initiating OC/IST as first-line therapy in patients with moderate-to-severe symptoms, and 38% agreed if symptoms were mild. When exploring treatment escalation, lack of efficacy, relapse severity and insufficient recovery from relapse drove 54% of all switches (33). However, almost half of the patients most recently seen by the participating neurologists had a relapse and did not change their treatment, mainly for reasons such as relapse mildness, patient stability, or receiving good treatment already (33). Furthermore, a proportion of 42.5% of patients were switched between different OC/ISTs when they had a relapse instead of escalating to a high-efficacy monoclonal antibody, even though half of those relapses were moderate-to-severe in nature (33). This would imply a similar-to-higher percentage of TI than in our study, although new agents were not available in all countries at the time of survey completion. Similar to our results, Thon et al. found that 40% of neuroimmunologists (n = 10/25) would switch none or up to 25% of their patients to one of the novel NMOSD treatments following a relapse (34). The authors hypothesized that the reasons behind this decision could be due to insurance and cost-related barriers (34). However, these factors did not apply in our study as treatments were unbranded and only efficacy/safety data was provided to respondents.
Another survey about treatment choices performed in Korea before new treatments’ approval found that ISTs were prescribed by 85% of the 27 participating neurologists as first-line therapies, and 70% of them would switch to rituximab as second-line therapy if there was a relapse (35). Participants treating a higher number of NMOSD patients annually were more likely to prescribe rituximab as second-line therapy (35). Similarly, a higher volume of patients managed by the responding neurologist has been associated with lower TI in other studies in MS, as well as more years of experience or being an MS specialist (12, 13). However, in our study, the only professional characteristic found as a predictor of TI was working in a low complexity hospital. Additionally, although we found a higher prevalence of TI among neurologists with a lower degree of empathy, and those who gave higher importance to treatment ease of use and their own experience rather than research or scientific evidence, the only predictor of TI in the multivariate analysis in this matter was giving higher importance to patient tolerability/safety when choosing a treatment. We hypothesized that all these factors could be strategies adopted by the respondent in an attempt to reduce the ambiguity and risk-aversion that has been related with TI in previous studies (13).
Uncertainty due to the limited experience with new agents and their differences, the rarity of the disease, the lack of clinical management guidelines including the increasing therapeutic options, together with long experience with off-label treatments, might be affecting the decision-making process (36), giving importance to relapse severity or lesion location as a driver of switches (33, 37). However, there is no clear consensus on how relapse severity is defined in clinical practice and current mildness does not necessary reflect the same in subsequent relapses, the prevention of all relapses being the therapeutic goal regardless of their severity (6, 7, 38, 39). In fact, patients describe disease stability as the absence of any relapse, since they focus on the impact relapses have on daily life and wellbeing (40, 41). Thus, the relapsing nature of the disease together with the importance of a patient-centered approach with shared decision-making should lead to a shift in the treatment paradigm to early use of high-efficacy therapies when treating this condition, as it is evolving in the MS field (42). This is a matter of importance in NMOSD due to the severity of relapses, poor recovery, and associated disability accumulation (5, 22, 39, 43). New therapeutic landscapes might facilitate reaching this ambition, as recent studies have shown an increase in the use of high-efficacy monoclonal antibodies with better outcomes at the expense of IST/OCs (7, 22, 44). However, as shown in this study, there is still a need to improve therapeutic decisions in order to reduce the prevalence of TI and its magnitude, as new highly effective therapies may be an advantage, but the choice between multiple options might lead to suboptimal decisions. For this reason, it could be helpful to implement continuous updated medical education and training with innovative therapeutic interventions that facilitate the decision-making process, with the aim to achieve better patient outcomes (45–47). As NMOSD is a rare disease, patients also could benefit from being treated at referral centers, where continuous training and a greater number of patients assisted is usually more common, thus providing the center with higher expertise and specialization.
Several limitations should be mentioned. First, the cross-sectional design did not allow us to assess changes or causal relationships in neurologists’ TI over time, as the study consisted of a single online survey. Furthermore, we acknowledge it would had been better to perform a prospective or two stage study with training implementation and subsequent measurement of results. Second, there could be potential selection bias in including people with a greater interest in collaborating or who are actively involved with the society. Third, case scenarios did not include all the details (e.g., MRI lesions) or all patient situations, such as adolescents or patients with concurrent autoimmune conditions, but they do contain the minimal information in order to make proper decisions and not develop cognitive fatigue, which could affect the results. Fourth, the study was only performed in Spain, and generalizability of results might not apply to other countries. However, country-specific factors that could affect decisions such as price or insurance cover were removed from the case scenarios. Fifth, we only explored TI in NMOSD AQP4+, without including seronegative patients, as new treatments are approved only in seropositive population. Future studies should be performed to fill these gaps.
In conclusion, TI was detected in 4 out of 10 participating neurologists when initiating or switching treatments in NMOSD AQP4+, a severe condition with accumulating disability led by potentially devastating relapses. This study uncovers the need to challenge the therapeutic status quo in NMOSD, pursuing high-efficacy treatments from the start, and developing specific intervention strategies to ensure optimal therapeutic decisions and patient care. Future longitudinal studies should investigate this matter and strategies to reduce TI in NMOSD, including patient perspectives.
Qualified researchers may request access to individual level data through the clinical study data request platform (https://vivli.org/). Further details on Roche’s criteria for eligible studies are available here (https://vivli.org/members/ourmembers/). For further details on Roche’s Global Policy on the Sharing of Clinical Information and how to request access to related clinical study documents, see here https://www.roche.com/innovation/process/clinical-trials/data-sharing.
The studies involving humans were approved by the research ethics board of Hospital Universitario Clínico San Carlos, Madrid, Spain. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
ÁC-C: Conceptualization, Data curation, Writing – original draft, Writing – review & editing. RG-B: Conceptualization, Writing – original draft, Writing – review & editing. AO: Data curation, Writing – review & editing. MD: Data curation, Writing – review & editing. SB: Data curation, Writing – review & editing. MA-V: Data curation, Writing – review & editing. MS: Data curation, Writing – review & editing. PR: Conceptualization, Writing – review & editing. PL-L: Conceptualization, Writing – review & editing. JM: Conceptualization, Writing – original draft, Writing – review & editing. NTL: Conceptualization, Data curation, Writing – original draft, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The study was funded by the Medical Department of Roche Farma Spain (SL43671). The funding source had no role in the design of this study, data analysis and interpretation, review and approval of the manuscript or the decision to submit for publication.
The authors are most grateful to the Spanish Society of Neurology (SEN) and all neurologists who participated in the PREFERENCES-NMOSD study. The authors also thank Laura Prieto del Val, PhD, of Evidenze Clinical Research for providing medical writing support.
ÁC-C has received a grant from Instituto de Salud Carlos III, Spain; JR19/00007. RG-B, PL-L, and JM are employees of Roche Pharma Spain. PR is an employee of IQVIA, Madrid. NTL received compensation for consulting services, advisory activities and speaking honoraria from Bayer Schering Pharma, Biogen Idec, MerckSerono, Novartis, Sanofi-Aventis, Teva Pharmaceuticals, Roche Pharma, and Bristol Myers Squibb. MS received speaking honoraria from Roche, Biogen, and UCB Pharma, and travel reimbursement from Biogen, Sanofi, Merck, and Roche for national and international meetings. AO received research grants, travel support or honoraria for speaking engagements from Almirall, Biogen, Bristol Myers Squibb, Merck, Mylan, Novartis, Roche, Sanofi-Genzyme, and Teva. MD received speaking honoraria from Roche, Biogen, Novartis, Sanofi, and Janssen; and travel reimbursement from Biogen for international meetings. SB received research grants, travel support or honoraria for speaking engagements from Biogen, Bristol Myers Squibb, Merck, Novartis, Roche, Sanofi-Genzyme, and Teva. MA-V received speaking honoraria from Roche, Biogen, Novartis, Sanofi, and Janssen.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2024.1341473/full#supplementary-material
1. Wingerchuk, DM, and Lucchinetti, CF. Neuromyelitis Optica Spectrum disorder. N Engl J Med. (2022) 387:631–9. doi: 10.1056/NEJMra1904655
2. Papp, V, Magyari, M, Aktas, O, Berger, T, Broadley, SA, Cabre, P, et al. Worldwide incidence and prevalence of Neuromyelitis Optica: a systematic review. Neurology. (2021) 96:59–77. doi: 10.1212/wnl.0000000000011153
3. Berthele, A, Levy, M, Wingerchuk, DM, Pittock, SJ, Shang, S, Kielhorn, A, et al. A single relapse induces worsening of disability and health-related quality of life in patients with neuromyelitis optica spectrum disorder. Front Neurol. (2023) 14:376. doi: 10.3389/fneur.2023.1099376
4. Du, Q, Shi, Z, Chen, H, Zhang, Y, Wang, J, Qiu, Y, et al. Mortality of neuromyelitis optica spectrum disorders in a Chinese population. Ann Clin Transl Neurol. (2021) 8:1471–9. doi: 10.1002/acn3.51404
5. Jarius, S, Ruprecht, K, Wildemann, B, Kuempfel, T, Ringelstein, M, Geis, C, et al. Contrasting disease patterns in seropositive and seronegative neuromyelitis optica: a multicentre study of 175 patients. J Neuroinflammation. (2012) 9:14. doi: 10.1186/1742-2094-9-14
6. Paul, F, Marignier, R, Palace, J, Arrambide, G, Asgari, N, Bennett, JL, et al. International Delphi consensus on the management of AQP4-IgG+ NMOSD: recommendations for Eculizumab, Inebilizumab, and Satralizumab. Neurol Neuroimmunol Neuroinflamm. (2023) 10:124. doi: 10.1212/nxi.0000000000200124
7. Wingerchuk, DM, Weinshenker, BG, McCormick, D, Barron, S, Simone, L, and Jarzylo, L. Aligning payer and provider strategies with the latest evidence to optimize clinical outcomes for patients with neuromyelitis optica spectrum disorder. J Manag Care Spec Pharm. (2022) 28:S3–s27. doi: 10.18553/jmcp.2022.28.12-a.s1
8. Held, F, Klein, AK, and Berthele, A. Drug treatment of Neuromyelitis Optica Spectrum disorders: out with the old, in with the new? Immunotargets Ther. (2021) 10:87–101. doi: 10.2147/itt.S287652
9. Dennison, JB, Sazhin, D, and Smith, DV. Decision neuroscience and neuroeconomics: recent progress and ongoing challenges. Wiley Interdiscip Rev Cogn Sci. (2022) 13:e1589. doi: 10.1002/wcs.1589
10. Saposnik, G, and Montalban, X. Therapeutic inertia in the new landscape of multiple sclerosis care. Front Neurol. (2018) 9:174. doi: 10.3389/fneur.2018.00174
11. Saposnik, G, Sempere, AP, Raptis, R, Prefasi, D, Selchen, D, and Maurino, J. Decision making under uncertainty, therapeutic inertia, and physicians' risk preferences in the management of multiple sclerosis (DIScUTIR MS). BMC Neurol. (2016) 16:58. doi: 10.1186/s12883-016-0577-4
12. Almusalam, N, Oh, J, Terzaghi, M, Maurino, J, Bakdache, F, Montoya, A, et al. Comparison of physician therapeutic inertia for Management of Patients with Multiple Sclerosis in Canada, Argentina, Chile, and Spain. JAMA Netw Open. (2019) 2:e197093. doi: 10.1001/jamanetworkopen.2019.7093
13. Saposnik, G, Sempere, AP, Prefasi, D, Selchen, D, Ruff, CC, Maurino, J, et al. Decision-making in multiple sclerosis: the role of aversion to ambiguity for therapeutic inertia among neurologists (DIScUTIR MS). Front Neurol. (2017) 8:65. doi: 10.3389/fneur.2017.00065
14. Mata-Cases, M, Franch-Nadal, J, Gratacòs, M, and Mauricio, D. Therapeutic inertia: still a long way to go that cannot be postponed. Diabetes Spectr. (2020) 33:50–7. doi: 10.2337/ds19-0018
15. Levy, M, Fujihara, K, and Palace, J. New therapies for neuromyelitis optica spectrum disorder. Lancet Neurol. (2021) 20:60–7. doi: 10.1016/s1474-4422(20)30392-6
16. Tugizova, M, Vlahovic, L, Tomczak, A, Wetzel, NS, and Han, MH. New therapeutic landscape in Neuromyelitis Optica. Curr Treat Options Neurol. (2021) 23:13. doi: 10.1007/s11940-021-00667-3
17. Yamamura, T, Kleiter, I, Fujihara, K, Palace, J, Greenberg, B, Zakrzewska-Pniewska, B, et al. Trial of Satralizumab in Neuromyelitis Optica Spectrum disorder. N Engl J Med. (2019) 381:2114–24. doi: 10.1056/NEJMoa1901747
18. Traboulsee, A, Greenberg, BM, Bennett, JL, Szczechowski, L, Fox, E, Shkrobot, S, et al. Safety and efficacy of satralizumab monotherapy in neuromyelitis optica spectrum disorder: a randomised, double-blind, multicentre, placebo-controlled phase 3 trial. Lancet Neurol. (2020) 19:402–12. doi: 10.1016/s1474-4422(20)30078-8
19. Cree, BAC, Bennett, JL, Kim, HJ, Weinshenker, BG, Pittock, SJ, Wingerchuk, DM, et al. Inebilizumab for the treatment of neuromyelitis optica spectrum disorder (N-MOmentum): a double-blind, randomised placebo-controlled phase 2/3 trial. Lancet. (2019) 394:1352–63. doi: 10.1016/s0140-6736(19)31817-3
20. Pittock, SJ, Berthele, A, Fujihara, K, Kim, HJ, Levy, M, Palace, J, et al. Eculizumab in Aquaporin-4-positive Neuromyelitis Optica Spectrum disorder. N Engl J Med. (2019) 381:614–25. doi: 10.1056/NEJMoa1900866
21. Knapp, RK, Hardtstock, F, Wilke, T, Maywald, U, Deiters, B, Schneider, S, et al. Evaluating the economic burden of relapses in Neuromyelitis Optica Spectrum disorder: a real-world analysis using German claims data. Neurol Ther. (2022) 11:247–63. doi: 10.1007/s40120-021-00311-x
22. Moog, TM, Smith, AD, Burgess, KW, McCreary, M, and Okuda, DT. High-efficacy therapies reduce clinical and radiological events more effectively than traditional treatments in neuromyelitis optica spectrum disorder. J Neurol. (2023) 270:3595–602. doi: 10.1007/s00415-023-11710-5
23. Santesson, AHE, Bäckström, M, Holmberg, R, Perrin, S, and Jarbin, H. Confirmatory factor analysis of the evidence-based practice attitude scale (EBPAS) in a large and representative Swedish sample: is the use of the total scale and subscale scores justified? BMC Med Res Methodol. (2020) 20:254. doi: 10.1186/s12874-020-01126-4
24. Dolan, JG. A method for evaluating health care providers' decision making: the provider decision process assessment instrument. Med Decis Mak. (1999) 19:38–41. doi: 10.1177/0272989x9901900105
25. Hojat, M, DeSantis, J, Shannon, SC, Mortensen, LH, Speicher, MR, Bragan, L, et al. The Jefferson scale of empathy: a nationwide study of measurement properties, underlying components, latent variable structure, and national norms in medical students. Adv Health Sci Educ Theory Pract. (2018) 23:899–920. doi: 10.1007/s10459-018-9839-9
26. Courvoisier, DS, Cullati, S, Haller, CS, Schmidt, RE, Haller, G, Agoritsas, T, et al. Validation of a 10-item care-related regret intensity scale (RIS-10) for health care professionals. Med Care. (2013) 51:285–91. doi: 10.1097/MLR.0b013e318280f02c
27. Zhang, DC, Highhouse, S, and Nye, CD. Development and validation of the general risk propensity scale (GRiPS). J Behav Decis Mak. (2019) 32:152–67. doi: 10.1002/bdm.2102
28. Linden, M, Pyrkosch, L, Dittmann, RW, and Czekalla, J. Why do physicians switch from one antipsychotic agent to another? The "physician drug stereotype". J Clin Psychopharmacol. (2006) 26:225–31. doi: 10.1097/01.jcp.0000219917.88810.55
29. Jarius, S, Aktas, O, Ayzenberg, I, Bellmann-Strobl, J, Berthele, A, Giglhuber, K, et al. Update on the diagnosis and treatment of neuromyelits optica spectrum disorders (NMOSD) - revised recommendations of the Neuromyelitis Optica study group (NEMOS). Part I: diagnosis and differential diagnosis. J Neurol. (2023) 270:3341–68. doi: 10.1007/s00415-023-11634-0
30. Kümpfel, T, Giglhuber, K, Aktas, O, Ayzenberg, I, Bellmann-Strobl, J, Häußler, V, et al. Update on the diagnosis and treatment of neuromyelitis optica spectrum disorders (NMOSD) – revised recommendations of the Neuromyelitis Optica study group (NEMOS). Part II: attack therapy and long-term management. J Neurol. (2023) 271:141–76. doi: 10.1007/s00415-023-11910-z
31. Banerjee, A, Ng, J, Coleman, J, Ospina, JP, Mealy, M, and Levy, M. Outcomes from acute attacks of neuromyelitis optica spectrum disorder correlate with severity of attack, age and delay to treatment. Mult Scler Relat Disord. (2019) 28:60–3. doi: 10.1016/j.msard.2018.12.010
32. Carnero Contentti, E, Lopez, PA, Pettinicchi, JP, Criniti, J, Pappolla, A, Miguez, J, et al. Mortality of neuromyelitis optica spectrum disorder patients in an Argentinean population: a study from the RelevarEM registry. Mult Scler J Exp Transl Clin. (2023) 9:5444. doi: 10.1177/20552173231205444
33. Min, JH, Capobianco, M, Welsh, C, Lobo, P, deFiebre, G, Lana-Peixoto, M, et al. Understanding treatment decisions in Neuromyelitis Optica Spectrum disorder: a global clinical record review with patient interviews. Neurol Ther. (2023) 12:619–33. doi: 10.1007/s40120-022-00431-y
34. Thon, JM, Sharkus, R, Thakkar, R, Hunter, K, Siegler, JE, and Thon, OR. Utilization of FDA approved treatments for neuromyelitis optica spectrum disorder in clinical practice: a survey study of academic neuroimmunologists. Mult Scler Relat Disord. (2023) 80:105076. doi: 10.1016/j.msard.2023.105076
35. Lee, HL, Kim, SH, Seok, JM, Kim, BJ, Kim, HJ, and Kim, BJ. Results of a survey on diagnostic procedures and treatment choices for Neuromyelitis Optica Spectrum disorder in Korea: beyond the context of current clinical guidelines. J Clin Neurol. (2022) 18:207–13. doi: 10.3988/jcn.2022.18.2.207
36. Saposnik, G. Applying behavioral economics and Neuroeconomics to medical education and clinical care. Can J Neurol Sci. (2019) 46:35–7. doi: 10.1017/cjn.2018.371
37. Gholizadeh, S, Exuzides, A, Lewis, KE, Palmer, C, Waltz, M, Rose, JW, et al. Clinical and epidemiological correlates of treatment change in patients with NMOSD: insights from the CIRCLES cohort. J Neurol. (2023) 270:2048–58. doi: 10.1007/s00415-022-11529-6
38. Kessler, RA, Mealy, MA, and Levy, M. Treatment of Neuromyelitis Optica Spectrum disorder: acute, preventive, and symptomatic. Curr Treat Options Neurol. (2016) 18:2. doi: 10.1007/s11940-015-0387-9
39. Ma, X, Kermode, AG, Hu, X, and Qiu, W. Risk of relapse in patients with neuromyelitis optica spectrum disorder: recognition and preventive strategy. Mult Scler Relat Disord. (2020) 46:102522. doi: 10.1016/j.msard.2020.102522
40. Capobianco, M, Ringelstein, M, Welsh, C, Lobo, P, deFiebre, G, Lana-Peixoto, M, et al. Characterization of disease severity and stability in NMOSD: a global clinical record review with patient interviews. Neurol Ther. (2023) 12:635–50. doi: 10.1007/s40120-022-00432-x
41. Meca-Lallana, JE, Gómez-Ballesteros, R, Pérez-Miralles, F, Forero, L, Sepúlveda, M, Calles, C, et al. Impact of Neuromyelitis Optica Spectrum disorder on quality of life from the Patients' perspective: an observational cross-sectional study. Neurol Ther. (2022) 11:1101–16. doi: 10.1007/s40120-022-00356-6
42. Hartung, HP, Meuth, SG, and Thompson, AJ. Paradigm shifts: early initiation of high-efficacy disease-modifying treatment in multiple sclerosis. Mult Scler. (2021) 27:1473–6. doi: 10.1177/13524585211033190
43. Park, SY, Kwon, YN, Kim, S, Kim, SH, Kim, JK, Kim, JS, et al. Early rituximab treatment reduces long-term disability in aquaporin-4 antibody-positive neuromyelitis optica spectrum. J Neurol Neurosurg Psychiatry. (2023) 94:800–5. doi: 10.1136/jnnp-2022-330714
44. Richter, D, Bartig, D, Tönges, L, Kümpfel, T, Schwake, C, Gold, R, et al. Inpatient care of neuromyelitis optica spectrum disorder in Germany: Nationwide analysis from 2010 to 2021. Mult Scler J Exp Transl Clin. (2023) 9:84433. doi: 10.1177/20552173231184433
45. Lewinski, AA, Jazowski, SA, Goldstein, KM, Whitney, C, Bosworth, HB, and Zullig, LL. Intensifying approaches to address clinical inertia among cardiovascular disease risk factors: a narrative review. Patient Educ Couns. (2022) 105:3381–8. doi: 10.1016/j.pec.2022.08.005
46. Saposnik, G, Tobler, PN, Caceres, F, Terzaghi, MA, Ruff, C, Maurino, J, et al. Usability of an educational intervention to overcome therapeutic inertia in multiple sclerosis care. Front Neurol. (2018) 9:522. doi: 10.3389/fneur.2018.00522
Keywords: neuromyelitis optica, therapeutic inertia, severe disease, shared decision-making, high-efficacy treatments
Citation: Cobo-Calvo &, Gómez-Ballesteros R, Orviz A, Díaz Sánchez M, Boyero S, Aguado-Valcarcel M, Sepúlveda M, Rebollo P, López-Laiz P, Maurino J and Téllez Lara N (2024) Therapeutic inertia in the management of neuromyelitis optica spectrum disorder. Front. Neurol. 15:1341473. doi: 10.3389/fneur.2024.1341473
Edited by:
Edgar Carnero Contentti, Hospital Aleman, ArgentinaReviewed by:
Friedemann Paul, Charité University Medicine Berlin, GermanyCopyright © 2024 Cobo-Calvo, Gómez-Ballesteros, Orviz, Díaz Sánchez, Boyero, Aguado-Valcarcel, Sepúlveda, Rebollo, López-Laiz, Maurino and Téllez Lara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Álvaro Cobo-Calvo, YWNvYm9AY2VtLWNhdC5vcmc=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.