
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CLINICAL TRIAL article
Front. Neurol. , 04 April 2024
Sec. Stroke
Volume 15 - 2024 | https://doi.org/10.3389/fneur.2024.1303402
This article is part of the Research Topic Novel approaches in diagnosis and management of ischemic edema in large vessel occlusion stroke - Volume II View all 8 articles
 Francisco Hernández-Bernal1,2†‡
Francisco Hernández-Bernal1,2†‡ Donner Estenoz-García3‡
Donner Estenoz-García3‡ Juan H. Gutiérrez-Ronquillo4‡
Juan H. Gutiérrez-Ronquillo4‡ Yenima Martín-Bauta1‡Karen Catasús-Álvarez1‡Mario Gutiérrez-Castillo4‡
Yenima Martín-Bauta1‡Karen Catasús-Álvarez1‡Mario Gutiérrez-Castillo4‡ Marbelys Guevara-Rodríguez4‡Aliuska Castro-Jeréz5‡Yoandra Fuentes-González5‡Yulemis Pinto-Cruz3‡Carmen Valenzuela-Silva6‡Verena L. Muzio-González1‡Héctor Pérez-Saad7‡
Marbelys Guevara-Rodríguez4‡Aliuska Castro-Jeréz5‡Yoandra Fuentes-González5‡Yulemis Pinto-Cruz3‡Carmen Valenzuela-Silva6‡Verena L. Muzio-González1‡Héctor Pérez-Saad7‡ Nelvys Subirós-Martínez7‡
Nelvys Subirós-Martínez7‡ Gerardo E. Guillén-Nieto8,9‡
Gerardo E. Guillén-Nieto8,9‡ Diana Garcia-del-Barco-Herrera7,9,*†‡ on behalf of the COURAGE (COmbined therapeUtic appRoAch durinG acute strokE) Research Group
Diana Garcia-del-Barco-Herrera7,9,*†‡ on behalf of the COURAGE (COmbined therapeUtic appRoAch durinG acute strokE) Research GroupObjective: This study tested the hypothesis that a neuroprotective combined therapy based on epidermal growth factor (EGF) and growth hormone-releasing hexapeptide (GHRP6) could be safe for acute ischemic stroke patients, admitting up to 30% of serious adverse events (SAE) with proven causality.
Methods: A multi-centric, randomized, open-label, controlled, phase I-II clinical trial with parallel groups was conducted (July 2017 to January 2018). Patients aged 18–80 years with a computed tomography-confirmed ischemic stroke and less than 12 h from the onset of symptoms were randomly assigned to the study groups I (75 μg rEGF + 3.5 mg GHRP6 i.v., n=10), II (75 μg rEGF + 5 mg GHRP6 i.v., n=10), or III (standard care control, n=16). Combined therapy was given BID for 7 days. The primary endpoint was safety over 6 months. Secondary endpoints included neurological (NIHSS) and functional [Barthel index and modified Rankin scale (mRS)] outcomes.
Results: The study population had a mean age of 66 ± 11 years, with 21 men (58.3%), a baseline median NIHSS score of 9 (95% CI: 8–11), and a mean time to treatment of 7.3 ± 2.8 h. Analyses were conducted on an intention-to-treat basis. SAEs were reported in 9 of 16 (56.2%) patients in the control group, 3 of 10 (30%) patients in Group I (odds ratio (OR): 0.33; 95% CI: 0.06–1.78), and 2 of 10 (20%) patients in Group II (OR: 0.19; 95% CI: 0.03–1.22); only two events in one patient in Group I were attributed to the intervention treatment. Compliance with the study hypothesis was greater than 0.90 in each group. Patients treated with EGF + GHRP6 had a favorable neurological and functional evolution at both 90 and 180 days, as evidenced by the inferential analysis of NIHSS, Barthel, and mRS and by their moderate to strong effect size. At 6 months, proportion analysis evidenced a higher survival rate for patients treated with the combined therapy. Ancillary analysis including merged treated groups and utility-weighted mRS also showed a benefit of this combined therapy.
Conclusion: EGF + GHRP6 therapy was safe. The functional benefits of treatment in this study supported a Phase III study.
Clinical Trial Registration: RPCEC00000214 of the Cuban Public Registry of Clinical Trials, Unique identifier: IG/CIGB-845I/IC/1601.
Ischemic stroke remains an important target for novel preventive and therapeutic strategies. It is estimated that 15 million people worldwide are affected by stroke every year, 5 million of them die and another 5 million of them suffer from long-term disability (1). The global population aged 65 years and over is growing faster than all other age groups, with a concomitant increase in stroke incidence (2). Furthermore, stroke among COVID-19 patients is associated with a significant risk of early mortality (3).
Currently, reperfusion therapy with thrombolytic drugs or endovascular thrombectomy represents the only approved therapeutic approach for acute stroke (4, 5). However, these approaches are associated with a narrow therapeutic window, increased risk of hemorrhagic transformation, and the high cost required to deliver these treatments (6), which limit their suitability for patients (~3%−6%), particularly in low-income countries (7). Moreover, despite treatment, recovery may be incomplete in a significant proportion of patients (8), as the vascular dynamics following recanalization do not invariably reduce tissue injury or reverse functional deficits (9, 10), and there remains scope for additional pharmacological-based neuroprotective interventions in addition to recanalization in acute ischemic stroke.
Considering the strong interdependence of elements in the neurovascular unit (11) and the limitations of neuron-protective strategies in clinical trials (12, 13), the scientific community has moved to combination strategies that seek to enhance endogenous mechanisms of neuroprotection (14). Combined therapies for stroke are likely to be more effective as they simultaneously target multiple levels of the ischemic pathophysiological cascade. However, few clinical trials have been published to date (2).
Molecules that trigger cytoprotective effects can be considered candidates for combined therapies (8). Particularly, a combined therapy based on epidermal growth factor (EGF) and growth hormone-releasing hexapeptide (GHRP6) has demonstrated benefit in preclinical contexts by activating pleiotropic endogenous mechanisms of survival and brain protection (15–19). Both molecules cross the blood-brain barrier (20–23), and their receptors are widely distributed in brain tissues (24, 25). EGF and GHRP6 share common properties such as anti-apoptotic (26, 27) and anti-excitotoxic effects (28, 29). In addition, both molecules have independent biological effects. Specifically, EGF promotes neurogenesis and remyelination (30), while GHRP6 induces endogenous neuroprotective factors such as growth hormone and insulin, like growth factor 1 (31).
Previous results of our group demonstrated the therapeutic benefits of this combination in animal models of multiple sclerosis (15), proximal axonopathy mimicking ALS, and focal and global ischemic stroke (16). Later, EGF+GHRP6 combined therapy improved both clinical and pathological aspects as it reduced neurological symptoms and brain infarct volume, preserving neuronal density (17). Additionally, EGF+GHRP6 combined therapy achieved similar results in a preclinical context when compared to therapeutic hypothermia (18). Moreover, both active ingredients exhibited a high safety profile in preclinical and clinical trials (32, 33).
Supported by these data, a phase I/II randomized clinical trial was designed to test the hypothesis that administration of a combined therapy based on rEGF and GHRP6 at two dose levels is safe for acute ischemic stroke (AIS) patients, admitting up to 30% of serious adverse events (SAE) in relation to proven causality. The therapeutic effect was assessed as a secondary endpoint. The current report has been written in compliance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines for randomized controlled trials (34, 35).
Growth hormone-releasing hexapeptide (GHRP6) (His-d-Trp-Ala-Trp-d-Phe-Lys-NH2) was synthesized by BCN peptide (Barcelona, Spain). Saccharomyces cerevisiae is the host organism that expresses recombinant epidermal growth factor (rEGF). Both ingredients were formulated separately in lyophilized preparation for intravenous administration at the facilities of the Center for Genetic Engineering and Biotechnology (Havana, Cuba).
EGF and GHRP6 were retained at 2–8°C at all times to guarantee the cold chain. Packages containing 14 kits, corresponding to the 14 administrations for each patient, were sent to the pharmacy of each clinical site. Trained personnel, under researcher supervision, carried out the preparation and administration of the study drugs.
This study was conducted according to the ethical principles of protection of participants in biomedical research stated in the Guidelines of Good Clinical Practice (CECMED 2000, Cuba) (36), the Guide of Good Clinical Practices of the International Conference on Harmonization (ICH E6) (37), and the Declaration of Helsinki (38).
The study protocol (Code: IG/CIGB-845I/IC/1601) was approved by the Ethics and Review Committee of every hospital involved in this trial and by the Cuban Center for State Control of Drugs, Medical Devices, and Equipment (CECMED, in Spanish). The Ethics and Review Committees also supervised the study execution, ensuring the protection of the rights, safety, and well-being of the participants involved in the study and verifying the progress of the clinical trial and the investigators' adherence to the protocol. This clinical trial was also registered at the Cuban Clinical Trial Public Registry No. RPCEC00000214 (https://rpcec.sld.cu/en/trials/RPCEC00000214-En).
Verbal and written informed consent was obtained from all patients or their legally authorized representatives regarding interventions, clinical assessments, and all features related to the current research (see below).
This was a multicenter, open-label, controlled, phase I/II clinical trial with centralized randomization and parallel groups. The primary endpoint was the assessment of the safety of two dose levels of EGF+GHRP6 combined therapy in patients with acute ischemic stroke, in addition to secondary endpoints of therapeutic effects.
The trial was performed in stroke units of 11 hospitals from eight provinces of Cuba from July 2017 to January 2018. The participating researchers were internists, neurologists, and emergency room physicians.
The sample size was estimated according to a specific method for pilot studies of transition therapies to estimate an upper limit to the related serious adverse event rate of 30% (39). Assuming a type I error of 0.05, a sample size of 10 subjects per group was estimated.
However, a protocol deviation occurred at the beginning of the study because a delay in enrollment and treatment procedures led to unmet therapeutic window criteria for the first six patients. Thus, it was decided to include them in the control group. On completion of the study, a total of 36 patients were included (Figure 1).
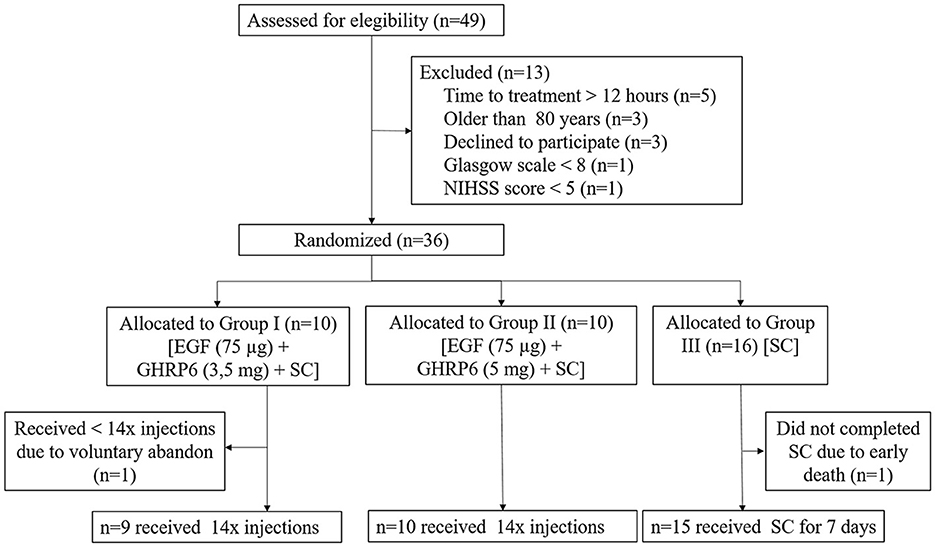
Figure 1. CONSORT flow diagram of the study. Allocation of patients and causes of non-compliance. A total of 36 patients were randomized and included in the final analysis. SC, standard care.
The randomization procedure was carried out through a randomized, centralized list based on three-subject blocks using the “2N” computer tool (University of Arkansas). After verbal consent was obtained, clinician researchers enrolled patients without previous knowledge of their group assignment and then phoned the central trial coordinator (HBF), who assigned the identification code and the study group. Subsequently, the study drugs were prescribed accordingly and requested at the hospital's pharmacy.
Patients assigned to the control group (n = 16) only received standard care for stroke in the acute phase, which did not include recanalization (40). Two other groups were treated with standard care plus EGF 75 μg + GHRP6 3.5 mg (Group I, n=10) or EGF 75 μg + GHRP6 5 mg (Group II, n=10). Dose selection was based on previous preclinical and clinical studies and two methods of dose extrapolation from rodents to humans, which considered body surface and body weight (41). Both substances were slowly injected intravenously twice a day, 12 h apart, and over the course of 7 days, with EGF being administered first.
Standard care for all groups included symptomatic control of comorbidities such as hypertension and diabetes. Patient stabilization, including airways, breathing, and circulation, was achieved through continued vital sign monitoring, hydration, and adequate oxygenation, among other measures included in the Cuban National Program of Care for patients with cerebrovascular disease (40). In the case of those with impaired consciousness or a large mass effect with midline displacement in the CT scan, 20% mannitol (0.25–0.5 g/kg) was administered every 4 h, and hyperventilation therapy was considered. Any concomitant medication was delivered according to the medical criteria. Recanalization interventions were not applied.
Treatment was completed in the hospital admission regime. Hospital discharge occurred at least 12–24 h after the last administration of the combined therapy.
Eligible participants were adults aged 18–80 years with a focal acute neurological defect caused by an acute ischemic stroke (a hemorrhagic event was excluded by computed tomography), with less than 12 h between the onset of symptoms and therapy initiation. Verbal consent was obtained from the patient or their legal representative. Once patients were stabilized, in the following days, they were asked for a written and signed consent form to continue participating.
Exclusion criteria were coma state (Glasgow scale less than 8), NIHSS scale score < 5 or > 20, a neurological defect explainable by a condition other than ischemic stroke, patients with quickly resolving neurological symptoms, severe and uncontrolled arterial hypertension (systolic > 185 mmHg or diastolic > 110 mmHg) or arterial hypotension (systolic < 95 mmHg) both unresponsive to standard treatment, seizures, and patients with a diagnosis of malignant neoplasms, pregnancy, puerperium, or mental disorders.
If a related serious adverse event rate higher than that allowed in the hypothesis (30%) with a high probability (> 0.90) occurred in the highest dose group of GHRP6 (5.0 mg), inclusion and treatment would be stopped in that specific group. If this phenomenon occurred in Group I (3.5 mg GHRP6), the clinical trial would be stopped. Safety and primary data were assessed and reviewed by an independent data monitoring committee consisting of a statistician, a clinician, an epidemiologist, and a neurologist. None of the treatment groups in the present study were closed.
As a phase I/II clinical trial, the primary endpoint was the safety of intravenously administered EGF+GHRP6 combined therapy in the setting of an acute stroke. Clinical adverse events [type, intensity, evolutionary outcome, and causal relationship (42)], vital signs, and electrocardiographic monitoring were recorded during the 7-day in-hospital stay and in outpatient visits at 1, 3, and 6 months after discharge. Patients were instructed to observe adverse events during the study period and report them to their attending physician.
Combined therapy was considered safe if not associated with an adverse event degree ≥ 3. The treating physicians determined causality at the time of the event based on their expertise and previously reported adverse events for each independent component, which was further reviewed by the data monitoring committee. Considering that both EGF and GHRP6 had previous clinical studies focused on other conditions, the expected adverse effects were mainly fever, shivering, and vomiting for the former (43), and sweating and bradycardia for the latter (32). The causes of death were registered based on clinical evidence and necropsy findings.
Secondary endpoints included neurological (National Institutes of Health Stroke Scale, NIHSS) and functional (modified Rankin scale (mRS) and Barthel index) outcomes at discharge, 3 and 6 months later, and survival 6 months after treatment. At the time of enrollment, patients were evaluated according to the NIHSS (44) to register baseline stroke severity. This scale assesses the degree of neurological deficit in 11 categories, wherein a normal function level without neurological deficit has a zero score and the maximum score is 42 points.
mRS, which is a simplified evaluation of functionality, was used at discharge and during the follow-up period (3 and 6 months). mRS values range from 0 (to indicate no residual symptoms) to 6 (to indicate death). The Barthel Index ranged from 0 to 100, wherein a 100 score indicates no deficit and a 0 score indicates complete dependence or death. Based on these assessments, ordinal and dichotomous data analyses were conducted. mRS ≤ 2 and Barthel index ≥ 85 were considered favorable outcomes (45, 46).
Hematological and biochemical assays were carried out at the beginning of the study, 72 h at hospital discharge, and 1, 3, and 6 months later. The Isotope Center (CENTIS) laboratories performed hormonal assays (for growth hormone (hGH), ACTH, aldosterone, cortisol, prolactin, and insulin), for which sera were collected at the beginning of the study, 72 h, at hospital discharge, and 1, 3, and 6 months later.
Before study initiation, a workshop took place to unify criteria with researchers involved in this trial. Trained personnel carried out visits and quality monitoring in 100% of the hospitals participating in the study to verify compliance with the Good Clinical Practices.
The primary objective was to establish that the intervention was safe, admitting up to 30% of serious adverse events with a proven causal relationship.
For the purposes of this study, a data entry system was created in OpenClinica software (www.openclinica.com), with Data Collecting Notebook (DCN) as a primary data source. After review and query resolution, information was double-entered for subsequent automatic comparisons and corrections until no differences between databases were found. After completion, databases were closed and exported for the corresponding statistical analyses; no modification of primary data was allowed. SPSS software version 26.0 and EPIDAT v. 4.1 were used for statistical analyses. All analyses were done on an intention-to-treat (ITT) basis.
Adverse events were reported as descriptive statistics. Recurrent events were counted as separate events. The effect size was calculated based on the odds ratio (OR) with a 95% CI. The probability of treatment-related serious adverse events was evaluated iteratively with a Bayesian algorithm, as well as the criterion for stopping due to an unacceptable related serious adverse event rate with Beta (0.5, 0.5) as a priori distribution (47).
Categorical data were compared using the χ2 and Fisher's exact tests. For quantitative variables, the mean and standard deviation, minimum and maximum values, and confidence intervals for the mean were determined. For group differences, ANOVA or the Kruskal-Wallis tests were used according to the variable's nature. In the cases of normal approximation, groups were compared using the Bayesian method for independent samples by means of the Bayes factor, assuming diffuse priors for unequal variance between groups (Rouder method) (48). When applicable, the effect size was reported as the mean difference with a 95% CI accompanied by the Hedges' g (49, 50). Deceased patients were given the highest possible score on the previously mentioned scales.
Survival of both treated groups vs. control was analyzed using a log-rank (Mantel-Cox) test and a Cox regression model using the hazard ratio and 95% CI as effect sizes.
Ancillary analyses included the ordinal assessment of mRS and the survival of merged treated groups. Spearman's correlation coefficients were calculated in order to assess the likeness between the EGF+GHRP6-treated groups. In addition, utility-weighted mRS (UW-mRS) (51) and quality-adjusted life-years (QALY) gained by the intervention were calculated (52). For UW-mRS data, the utility weights proposed by Chaisinanunkul N. et al. (51) (mRS 0–1.0; mRS 1–0.91; mRS 2–0.76; mRS 3–0.65; mRS 4–0.33; mRS 5–0; mRS 6–0) were adopted. To determine the exact QALYs, the utility value associated with a given state of health was multiplied by the specific time (3 and 6 months) lived in that state (52).
Of the 49 stroke patients screened for participation in the trial, 73.5% (n=36) fulfilled the inclusion criteria. The most common reasons for exclusion were time to treatment longer than 12 h, older than 80 years, and patients' will. In the present study, there was no closure of any treatment group.
A total of 36 patients were included in the study (Figure 1). One out of 36 patients (from Group I) voluntarily withdrew from the trial after receiving 7 of 14 scheduled injections. This withdrawal was not associated with any risk concerns.
The mean time elapsed from the onset of symptoms to the start of treatment was 7.3 ± 2.8 h overall. No ECG changes were noted in more than 50% of patients in each group. Acute cerebral infarcts had a CT scan-confirmed ischemic etiology at baseline in 100% of cases. Two patients had subsequent hemorrhagic transformations (one patient in Group I with a 6-month survival and one deceased patient in Group III). The most frequent infarct locations were the left parietal (11.1%), left temporal (8.3%), and left temporoparietal (8.3%) zones.
Demographic and baseline characteristics were similar between groups. The mean age was 66 ± 11 years, and 21 were men (58.3%). Other clinical characteristics were also similar between groups, based on comparable grades of infarct symptoms and signs according to the NIHSS scale (Table 1).
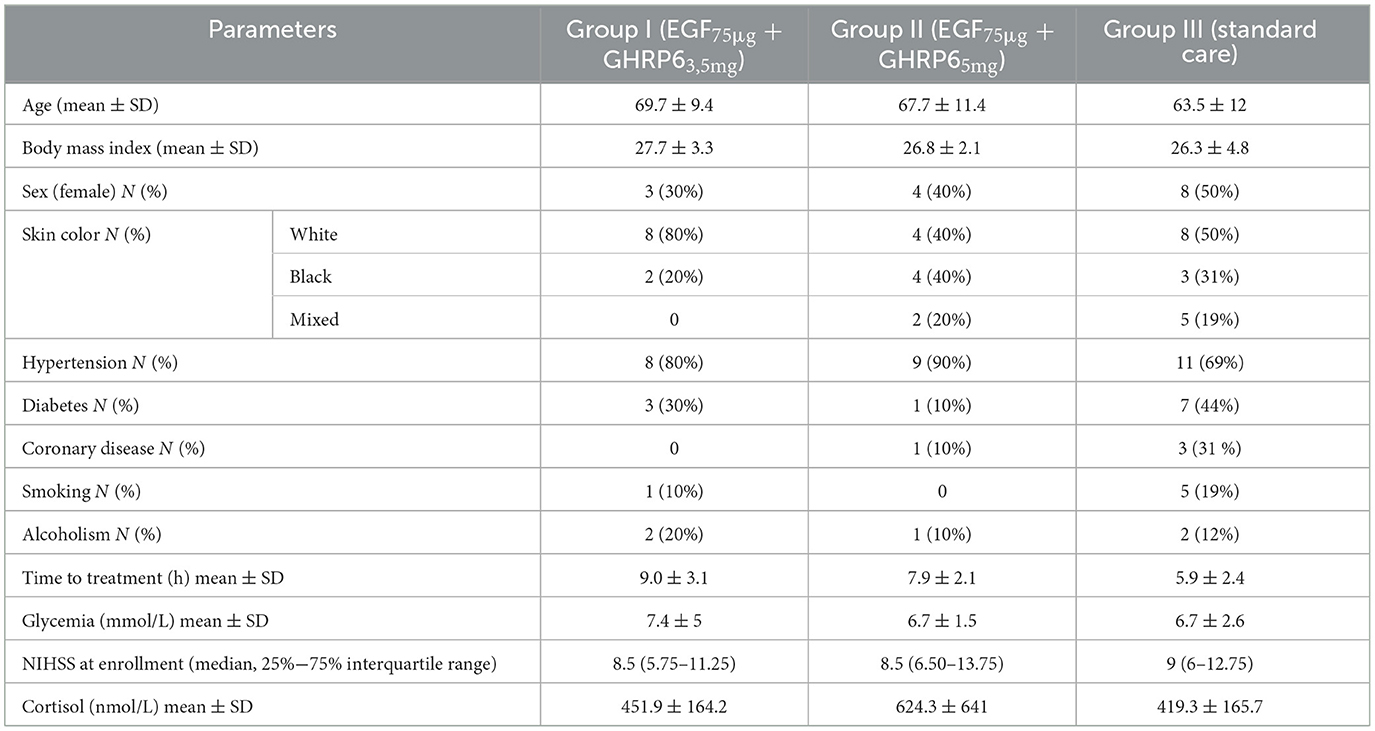
Table 1. Baseline characteristics of the patients.
In general, the laboratory parameters evaluated over time remained within the normal ranges; any variations had no clinical relevance. The hormonal profiles, in all cases, were similar between the three groups and were within the reference values for each hormone (data not shown).
The frequency of adverse events (AE) and serious AEs (SAEs) in the ITT population was similar among all groups (Table 2). In total, 23% of AE (in three and four patients in Groups I and II, respectively) had a probable or definite causal relationship with the intervention therapy. The intensity of these AEs was mainly mild or moderate (Table 3). Additionally, these AEs were completely solved.
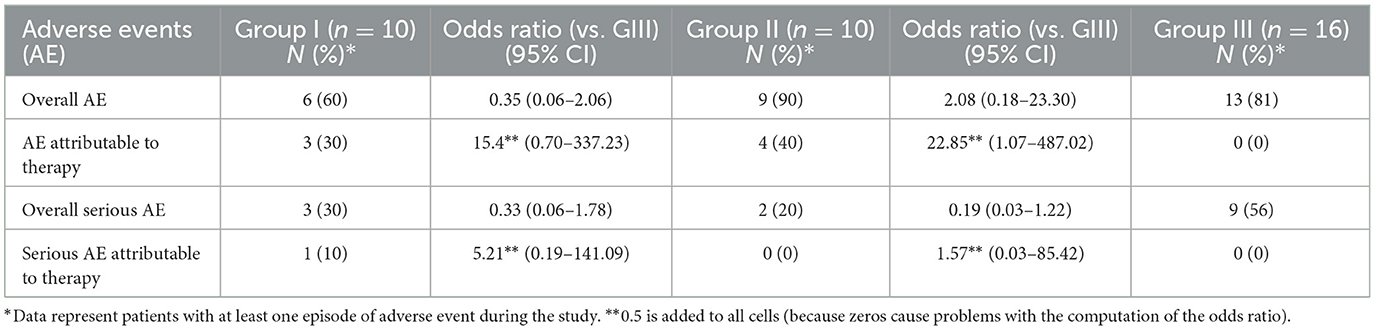
Table 2. Frequency of patients with serious and total adverse events.
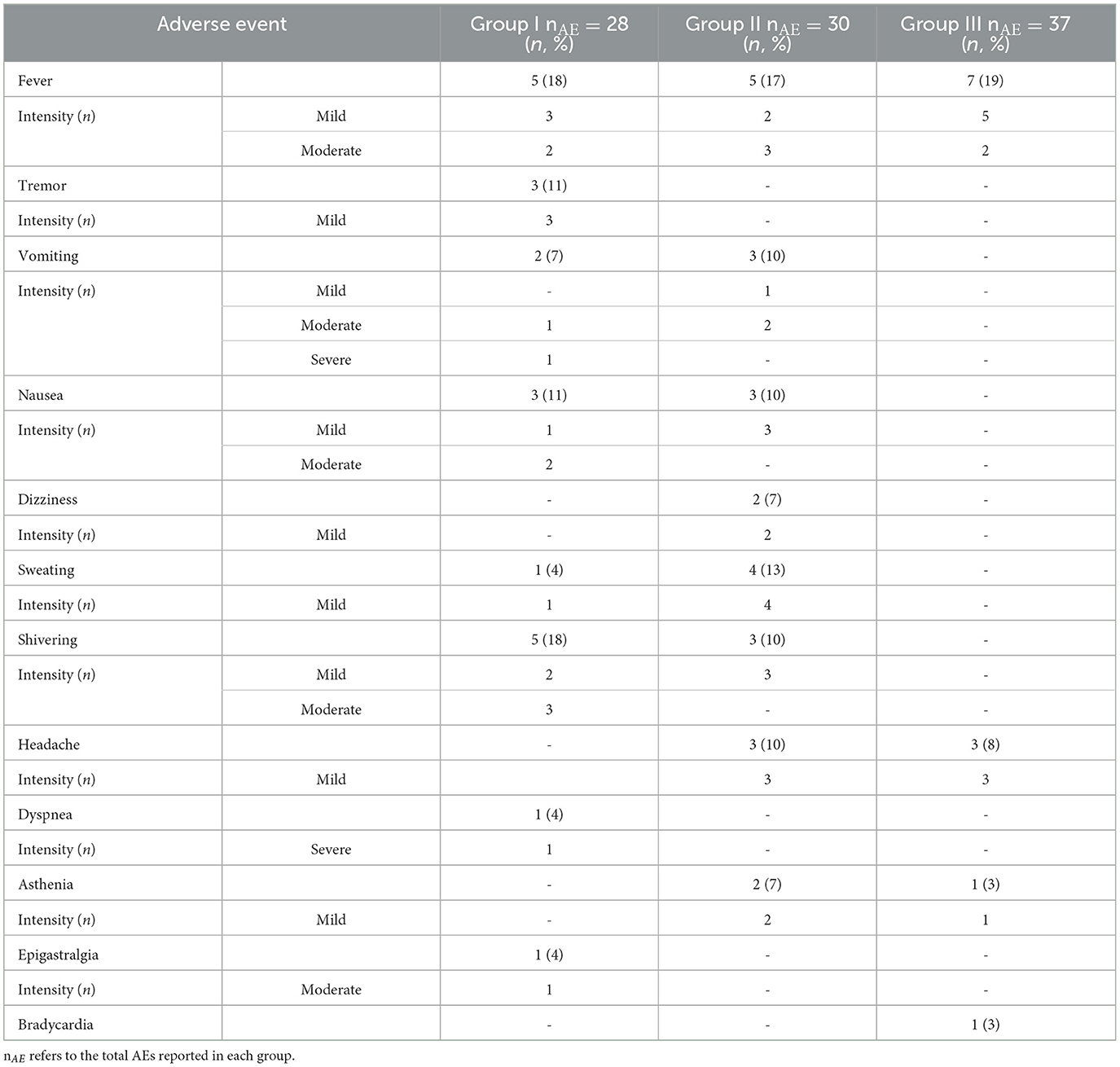
Table 3. Relevant expected adverse events in this study.
A total of 19 serious AEs were reported in 14 of 36 patients (three, two, and nine patients in Groups I, II, and III, respectively; see Table 2). In terms of causality with the interventional drug, only two serious AEs occurred in one patient in Group I (vomiting and dyspnea). In Group II, neither of the two SAEs (respiratory infection and brain reinfarction) reported (leading to death in both cases) had a causal relationship with the therapy under study. A higher probability of related AEs is detected in Group II with respect to Group III (lower limit of 95% CI for OR>1). No other significant association was detected (Table 2). The probability of confirming the study hypothesis (a limit to related serious adverse event rates lower than 30%) was greater than 0.90 in each group (globally greater than 0.99), with a related serious adverse event rate expected between 0 and 0.18 (95% CI).
The most relevant AEs with any causal relationship to investigational drugs are listed in Table 3. Bradycardia, which was one of the expected AEs associated with GHRP6, was not reported in any EGF+GHRP6-treated patients.
A total of seven deaths in Group III (control) and two deaths in Group II were reported. The lowest-dose group reported no mortality. Causes of mortality in Group III were arterial hypotension (1), bronchopneumonia (2), pulmonary embolism (1), acute pulmonary edema (1), respiratory distress (1), and brain edema (1). Deaths in Group II were due to respiratory infection and brain reinfarction. These were not associated with the interventional drugs.
The increased stroke severity over time in the control group, observed in Figure 2, was consistent with the worst possible score assigned to dead patients. This fact was influenced equally in all groups and in both neurological and functional assessment tools.
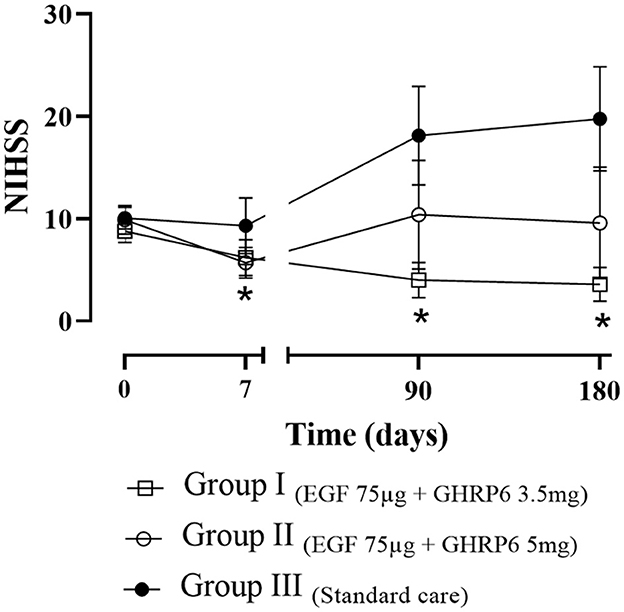
Figure 2. Functional recovery of patients assessed by NIHSS. The data depict the mean ± SEM. Bayesian analysis: * indicates differences vs. the baseline score. Dead patients receive the worst possible score.
ITT analysis showed a reduction in neurological deficit at 90 and 180 days in patients receiving EGF 75 μg + GHRP6 3.5 mg (Group I) compared to baseline NIHSS score. This reduction is also observed regarding Group III at the same assessment times (probabilities of difference greater than 0.95). In Group II, a reduction in the NIHSS score was recorded only at discharge compared to baseline (Figure 2).
As a measure of changes over the entire period, the areas under the individual curves (AUC) were calculated. The Bayes Factor1 − 0 in favor of the difference between Group I and Group III was 2.14 (p = 0.031), indicating sufficient evidence to reject the equality hypothesis.
Dichotomized analyses of the mRS scale and Barthel index showed an improved functional outcome in EGF+GHRP6-treated groups vs. Group III (control) at 90 days and 180 days, respectively. Notably, this benefit was seen at both ends of the scale (Figure 3).
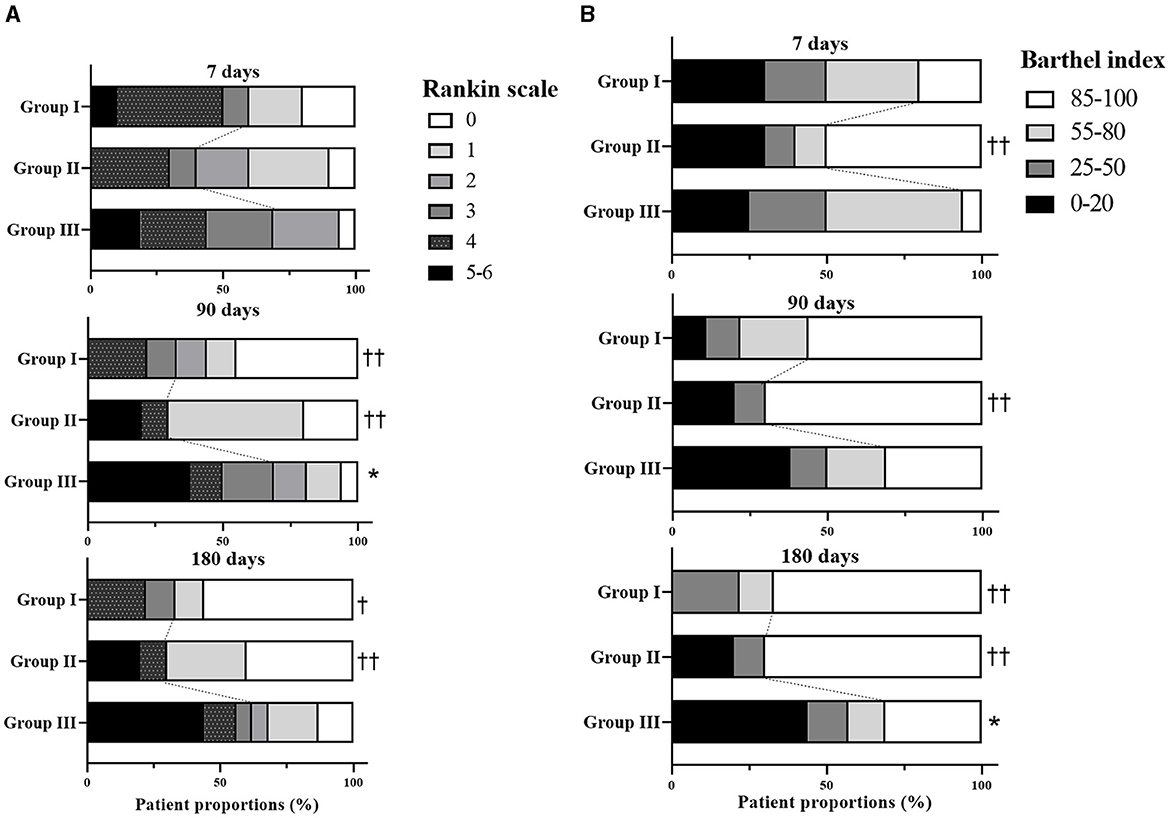
Figure 3. Clinical outcomes in the ITT population: modified Rankin scale (A) and Barthel index (B) at discharge (7 days), 3 and 6 months after stroke onset. * indicates significant differences between Group III and the EGF+GHRP6-treated groups, according to χ2 test (p < 0.05). ††indicates probabilities of difference with respect to Group III >0.95; †probabilities of difference >0.90, based on Bayesian analysis. Dashed lines demarcate the boundaries between the strata considered favorable (0–2 for the Rankin scale and ≥ 85 for the Barthel index) and not favorable. Dead patients received the worst possible score.
Effect size analysis based on mean difference and Hedges' g for NIHSS and mRS scores showed a strong effect in Group I from 90 to 180 days. Barthel index analysis indicated a moderate effect in both EGF+GHRP6-treated groups (Table 4).
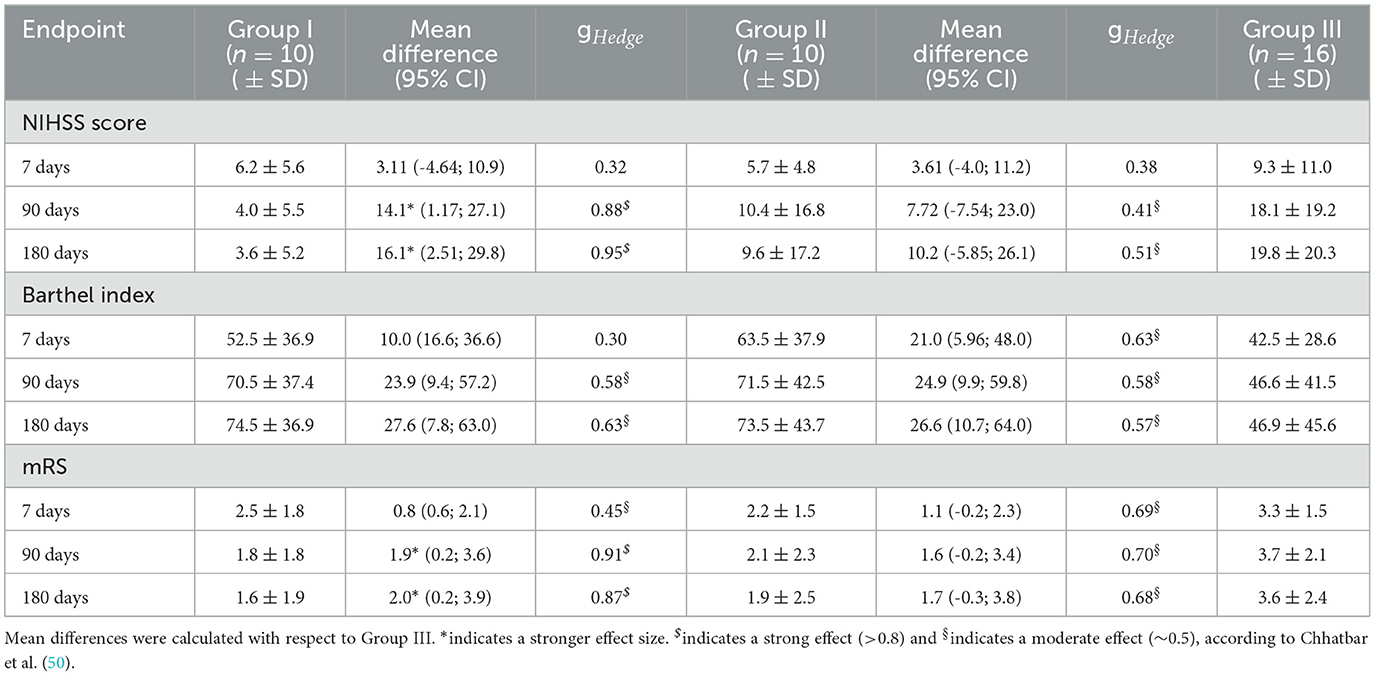
Table 4. Summary of the effect size of neurological and functional outcomes.
At 6 months, proportion analysis evidenced a higher survival of patients treated with the combined therapy (Figure 4A). At this time, Group I treated with EGF 75 μg + GHRP6 3.5 mg showed the highest overall survival (HR=0; p = 0.02). Group II (EGF 75 μg + GHRP6 5 mg) achieved an HR of 0.42 (95% CI: 0.111–1.597) at the end of the study. However, the log-rank test showed no statistical differences (Figure 4B).
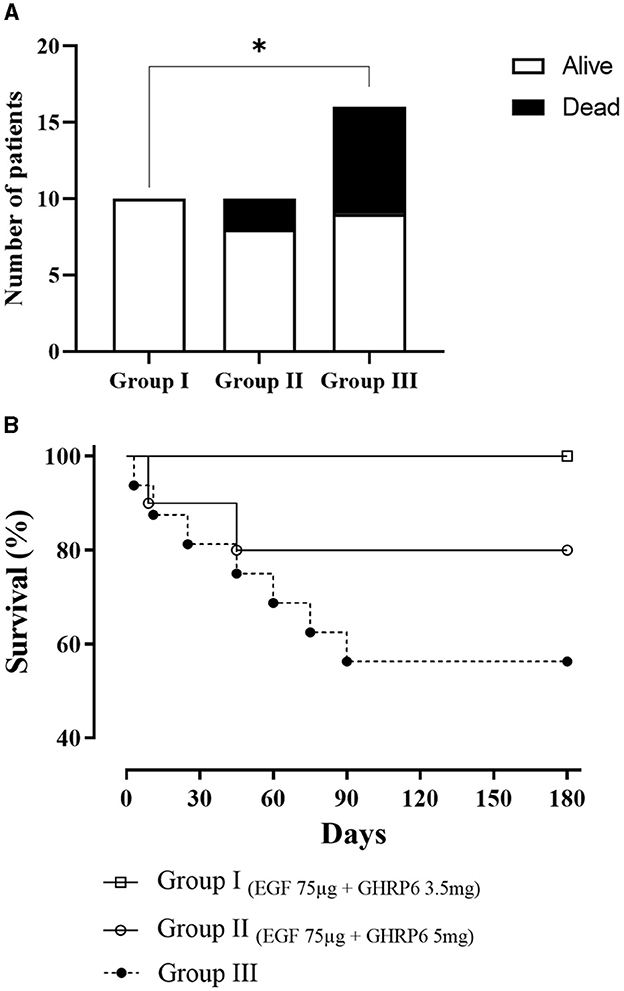
Figure 4. Survival of experimental groups analyzed by (A) χ2 test at 6 months (*p = 0.03) and (B) Kaplan-Meier curves and log-rank test (p = 0.053).
An analysis of weight-based dosing revealed significant differences between the mean dosages of both groups (p < 0.0001, t-test). Additionally, the relationship between dosing and mRS showed a probability of differences between Group I and Group II less than 0.6, with symmetrical confidence intervals around 0, suggesting similarity between both treated groups (data not shown).
Thus, for an additional purpose in terms of therapeutic effects, an ordinal analysis of mRS was conducted, in which merged treated groups showed a significant reduction of disability at 90 and 180 days vs. control (p = 0.01). This evidence was also confirmed using the AUC calculation, wherein the difference between the global change and the control group was in favor of the merged treated groups (Bayes Factor1 − 0 =1.44, p = 0.046). Regarding effect size, a mRS mean difference of 2 was associated with a Hedges' g equivalent to 0.821 (95% CI: 0.13–1.50) (Figure 5A). Survival assessment showed a significant reduction of mortality risk in the merged treated groups against Group III (p = 0.024) with a hazard ratio (HR) of 0.21 (95% CI: 0.06–0.82) at the end of the study (Figure 5B). Additionally, mRS of merged treated groups at 180 days positively correlated to time to treatment (r=0.55, 95% CI: 0.12–0.80, p = 0.01).
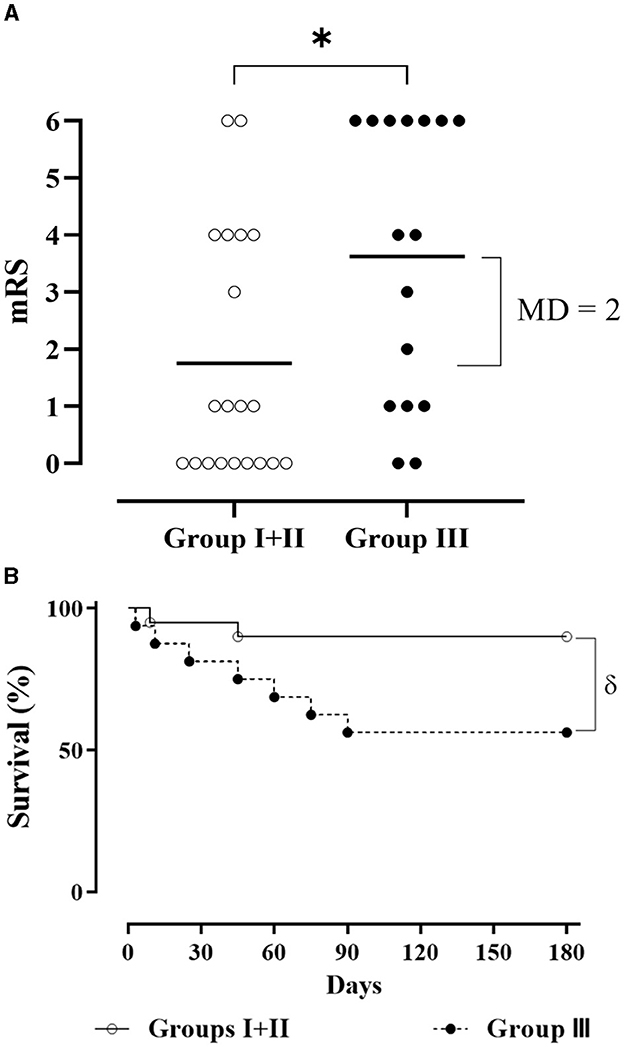
Figure 5. (A) mRS score of EGF+GHRP6-treated patients (Groups I and II; empty circle) and Group III (filled circle) at 180 days (*: p = 0.015, according to the Mann-Whitney U test). MD, mean difference. (B) Survival Kaplan-Meier curves in groups analyzed [δ: p = 0.024, HR 0.21 (95% CI: 0.06–0.82) according to log-rank test].
Adopting a patient-centered approach by using utility-weighted mRS, a higher utility mean was demonstrated for merged treated groups when compared to Group III. This effect was evident at 3 months and continued until the last assessment (Table 5).
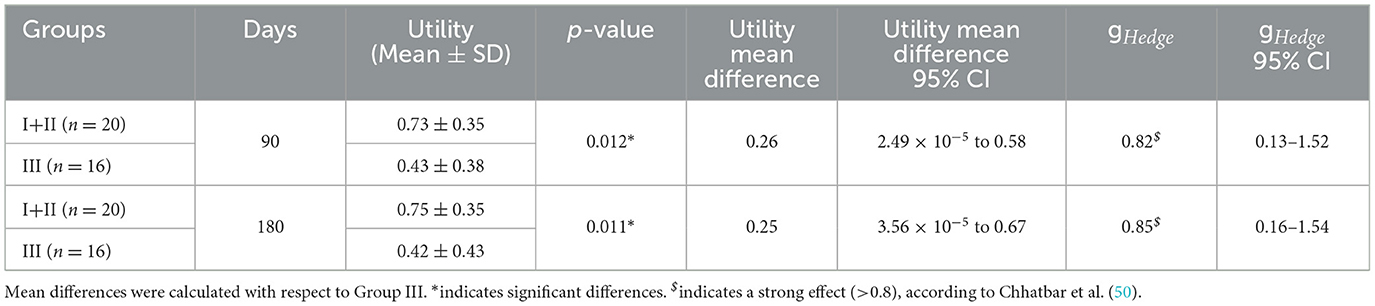
Table 5. Measures of effect size using utility-weight analysis of the mRS.
The phrase “combination therapy” for stroke usually refers to the use of recanalization approaches along with other therapeutics (13). Few published studies have combined pure neuroprotective drugs under the combined therapy concept (2). Indeed, generally, the use of agents with clear neuroprotective effects appears under the expression of “adjuvant therapy” (53). Our proposal, based on the combination of two pharmacological components with neuroprotective properties, represents a “combination therapy” that does not target the re-opening of the occluded vessel but the protection of remaining viable cells and the strengthening of endogenous regenerative and plasticity mechanisms that might enhance functional recovery. The promising results of this trial showed that EGF+GHRP6 combined therapy is safe. Although not powered for efficacy, this study revealed a significantly better outcome for EGF+GHRP6-treated patients relative to the clinical endpoints of stroke.
The Courage study population had typical risk factors for stroke (54), including older participants, high body mass index, and hypertension. The groups were well balanced with respect to these risk factors and admission stroke scores (Table 1, Figure 2). This baseline balance guarantees the reliability of the results (55).
In this study, the positive and significant correlation between time to treatment and mRS suggests that earlier intervention with EGF+GHRP6 may decrease disability 6 months after the onset of symptoms. This finding is also consistent with our pre-clinical studies (19). Although the immediate intervention is likely to enhance the therapeutic effects, we anticipate that components of this combination therapy will also target later secondary events, promoting survival of the neurovascular unit and activating endogenous neuroprotective pathways, which would predict a longer-lasting effect (56, 57).
The Courage trial based on intravenous delivery of EGF+GHRP6 for acute ischemic stroke was successful in terms of the prespecified primary endpoint concerning safety (Tables 2, 3), confirmed by less than 30% of serious AEs with a causal relationship to treatment, as stated in the hypothesis. Although some AEs, known to be elicited by EGF and GHRP6, were reported, the lack of statistical significance of the relative risks associated with total and serious AEs (Table 2) supports the expected safety profile for this therapeutic approach. At the end of the study, the ethical committees and the independent data monitoring committee issued a favorable assessment in terms of the safety of the therapeutic combination under investigation, endorsing the continuity of the clinical development of the project.
The association between increased survival and combined therapy detected in the prespecified analyses (Figure 4A) is further demonstrated when the two treatment groups are merged (Figure 5B). The hazard ratio indicates a 79% decreased risk of death in patients who received the combined therapy. The survival outcome of this study was consistent with the robust preclinical evidence obtained in animal models of acute focal and global brain ischemia (17, 18). This suggests local and systemic cytoprotection induced by EGF+GHRP6 that eventually preserves organs and systems vulnerable to dysautonomies typical of stroke (58–60).
The additional beneficial effect on functional assessments at 90 and 180 days, as evidenced by dichotomous (Figure 3) and ordinal analyses of merged treated groups (Figure 5A), further supports the likely therapeutic effects of this combination therapy.
Considering that examination of the full range of scores has statistical superiority vs. dichotomous analysis (61), ordinal approaches were also performed along with their associated effect size (mean differences and Hedges' g) (Table 4). Our results were consistent across dichotomous and ordinal approaches. The inclusion of effect size analysis not only implies compliance with the CONSORT guidelines (35) but also overcomes the limitations of sample size (62). The moderate to strong effect size of EGF+GHRP6 in the reduction of both stroke severity and resulting disability in treated patients provides additional evidence in favor of this therapeutic approach. Furthermore, the effect size of the mRS at 90 days, which is maintained until 180 days, confirms that the ordinal form of the 3-month mRS correlates better with long-term outcomes (63).
Taking into account that a statistically significant difference is not necessarily translated into a meaningful difference for both patients and clinicians, minimal clinically important differences (MCID) are a better point of reference than the traditional use of statistical significance (64). MCIDs for the NIHSS and mRS scales are 2 points (65) and 1 point (66), respectively. For the Barthel index, an MCID of 1.85 has been reported for a 15-point Likert-type scale (64). By analogy, this may be translated into an MCID of 12.3 change score for the 100-point Barthel index. In this study, the mean differences of NIHSS, Barthel index, and mRS exceeded their respective MCID in the subacute and chronic post-stroke phases (Table 4), showing enhanced outcomes in those patients receiving EGF+GHRP6 therapy. These significant score changes for the three assessment tools are an important finding of this trial as evidence of a real impact on patient perception beyond possible measurement errors (64). The largest MCIDs have such strong evidence that they have been considered the defining criteria for superior clinical trials (67).
In stroke, as in other disabling diseases, the most widely accepted patient-centered outcome measure is utility in terms of the desirability of a specific health outcome to the patient (68). In this study, the effect size of EGF+GHRP6 based on utility-weighted (UW) mRS was relatively large at 3 months and maintained until the last evaluation of the trial (6 months). The analysis of UW-mRS has been a strong recommendation of the Stroke Therapy Academic Industry Roundtable (STAIR) in stroke clinical trials (52), to rate disability outcomes with greater accuracy than unweighted approaches to mRS analysis (69).
An additional feature of UW-mRS is the ability to generate QALYs gained or lost by an intervention or treatment (52). If the current data were reproduced in a study designed for efficacy purposes, our therapeutic approach would confer 0.06 QALYs for every 6 months of survival. The concurrent inclusion of clinically interpretable and reliable mRS along with a contextually appropriate health utility scale allowed us to characterize favorable and meaningful differences in the patient's quality of life (70).
The EGF+GHRP6 combined therapy for stroke was designed to activate a cascade of endogenous neuroprotection mechanisms, including regeneration of adult neural stem cells and repair in the penumbra zone (26–31, 57, 71, 72). The activation of these pathways could explain the clinical (neurological, functional, and survival) outcomes evidenced in this study, which had been previously demonstrated in stroke animal models (17–19). The events induced by both active agents in this combined therapy have a scope that transcends beyond the acute phase of brain infarction (57, 71, 73, 74). The control of infarct core expansion also systemically influences the autonomous functioning of cardiovascular systems, usually affected by stroke (58–60).
The study was limited by a low sample size and a non-blinded design. This could lead to overestimated treatment effects from subjective measures (75). Another important limitation of this study was that imaging could only be used for diagnosis, specifically to rule out the presence of hemorrhagic stroke, and not as an evolutionary parameter together with the clinical outcomes. Additionally, standard therapy did not include thrombolysis, as this treatment is not currently widely available in Cuba for stroke therapy.
Furthermore, the exclusion of patients with NIHSS < 5 and > 20 rendered a more clinically homogeneous population, although the inclusion of only moderately affected patients (median stroke severity of 9) could reduce the discriminative power and the possibility of showing a beneficial effect of any therapy under study, as noted by Ehrenreich et al. (46).
In conclusion, EGF+GHRP6-based therapy is biologically plausible as a therapeutic intervention, given that both serum levels of EGF and insulin-like growth factor-1 (IGF-1) (as the main effect induced by GHRP6) were substantially lower in stroke patients and are determinant factors of ischemic stroke outcomes (76, 77). Thus, this combined therapy could also be considered as a replacement therapy.
For the purposes of stroke interventions, the neuroprotective properties of EGF and GHRP6, in addition to the molecular and cellular events they trigger, suggest a long-term effect, possibly generating trophic effects both in compromised tissue of the ischemic penumbra and in cells with regenerative potential. Intervention with EGF+GHRP6 demonstrates that the treatment is safe and provides encouraging evidence of therapeutic effects. These data provide support for the design of a large pivotal trial, ideally in combination with thrombolytic therapy.
Effective neuroprotective therapies remain an unmet clinical and social need, especially for patients not tributary to recanalization options. Advantageously, neuroprotective therapies with a high safety profile could always be combined with recanalization alternatives and even be used in subacute or chronic periods along with and after rehabilitation therapies.
This trial has demonstrated the safety of this combination therapy, and although underpowered, the data demonstrate robust evidence of therapeutic effects, both with respect to functional outcome and survival.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by the Ethic and Review Committee and /or institutional review board of every hospital or clinical sites as follow: Dr. Antonio Luaces Iraola Castro Hospital, Camilo Cienfuegos Hospital, Carlos Manuel de Céspedes Hospital, Celia Sánchez Manduley Hospital, Mártires del 4 de Abril Hospital, Juan Bruno Zayas Hospital, Agostinho Neto Hospital, Dr. Ernesto Guevara Hospital, and Faustino Pérez Hospital. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
FH-B: Conceptualization, Formal analysis, Methodology, Writing – review & editing, Project administration, Supervision. DE-G: Data curation, Investigation, Writing – review & editing. JG-R: Data curation, Investigation, Writing – review & editing. YM-B: Data curation, Resources, Supervision, Writing – review & editing. KC-Á: Data curation, Resources, Supervision, Writing – review & editing. MG-C: Data curation, Investigation, Writing – review & editing. MG-R: Data curation, Investigation, Writing – review & editing. AC-J: Data curation, Investigation, Writing – review & editing. YF-G: Data curation, Investigation, Writing – review & editing. YP-C: Data curation, Investigation, Writing – review & editing. CV-S: Formal analysis, Writing – review & editing. VM-G: Project administration, Resources, Writing – review & editing. HP-S: Conceptualization, Methodology, Writing – review & editing. NS-M: Conceptualization, Formal analysis, Visualization, Writing – original draft, Writing – review & editing. GG-N: Conceptualization, Formal analysis, Resources, Writing – review & editing. DG-d-B-H: Conceptualization, Formal analysis, Methodology, Visualization, Writing – original draft, Writing – review & editing.
Jorge L. Alonso Freire, Liliana Renté Cantillo, Rogelio Creagh Bandera, Ilietys Borroto Carpio, Héctor Santana Milian, Amaury del Puerto Cruz, Javier J. García Sacarías, Milagro Rodríguez Rosell, José L. Rodríguez Reynoso, Elio Llerena Rodríguez, Grettel Melo Suárez, Elizeth García Iglesias, Marel Alonso Abad, Laurina Hernández Turiño, Idania Baladrón Castrillo, María M. Ríos Cabrera, Ketty Cruz Chirino, Marisol Cruz Díaz, Misleydis Camejo Alemán, Yelién Martín Fadragas, Lourdes M. Basanta Marrero, Milagro Rodríguez González, Ahmed Ruiz Moré, Alina M. Alonso Ruiz, Nelson Rojas Sierra, Anisbel Rodríguez López, Erisdania Esquivel Ferrer, Carmen Remón Chávez, Yoska Castro Jeréz, Virginia Robledo Cabrera, Odalis Mora Barbán, Silvia Vázquez Labrada, Danay Duharte Sarmiñón, Yaritza Alvarado Rey, Adanais González Flores, Ledis Garbey Delás, Yirsa Luna Negret, Tamara Hudson Megret, Mayda Cisnero Rubalcaba, Adelina S. Ferrer Fernández, Idalmis Quevedo Palomo, Yadileydi Elias Oquendo, Dimitri Dueñas Valdivia, Alexis Suárez Quesada, Camelia Valhuerdi, Enrique Rodríguez, Cecilia Sayoux, Niurka Arteaga, Amelia González, Olaida Valdivia, Marta Pérez, Herminia Rodríguez, Indira Brito, Evelin Rangel, Maylín Ortiz, Yamila Espinosa, Yaila Ramírez, Marelis Pantoja, Caridad Guerra, Ana Santana, Salustina Sánchez, Carlos Casas, Norma Mora, Yoelis Copello, Melitza Pupo, Karen Alí, María C. López, Pilar Laborí, Elizabeth Lobaina, Jorge R. Góngora, Yomaidis Araujo, José A. Martínez, Raúl Domínguez, Mae Pupo, Tatiana Marañón, Yadira Hidalgo Boza, Tania González López, and Silvia Barcelona Pérez.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors are thankful for the medical and non-medical staff from the several clinical sites where the Courage study was conducted (enlisted below). However, our greatest gratitude is to all the patients and their families for their valuable contribution in accepting to participate in this trial. The authors wish to thank Dr. Orla Hardiman, Dr. Jorge Berlanga, and Dr. Rosa Maria Coro for their critical review of the manuscript. On the other hand, the authors wish to acknowledge the usefulness of the CONSORT guidelines as an invaluable tool to write this manuscript in a clearer and more objective way.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Roy-O'Reilly M, McCullough LD. Sex differences in stroke: the contribution of coagulation. Exp Neurol. (2014) 259:16–27. doi: 10.1016/j.expneurol.2014.02.011
2. Paul S, Candelario-Jalil E. Emerging neuroprotective strategies for the treatment of ischemic stroke: an overview of clinical and preclinical studies. Exp Neurol. (2021) 335:113518. doi: 10.1016/j.expneurol.2020.113518
3. Ramos-Araque ME, Siegler JE, Ribo M, Requena M, Lopez C, de Lera M, et al. Stroke etiologies in patients with COVID-19: the SVIN COVID-19 multinational registry. BMC Neurol. (2021) 21:43. doi: 10.1186/s12883-021-02075-1
4. Aguiar de Sousa D, von Martial R, Abilleira S, Gattringer T, Kobayashi A, Gallofré M, et al. Access to and delivery of acute ischaemic stroke treatments: a survey of national scientific societies and stroke experts in 44 European countries. Eur Stroke J. (2019) 4:13–28. doi: 10.1177/2396987318786023
5. Yang P, Zhang Y, Zhang L, Zhang Y, Treurniet KM, Chen W, et al. Endovascular thrombectomy with or without intravenous alteplase in acute stroke. New Engl J Med. (2020) 382:1981–93. doi: 10.1056/NEJMoa2001123
6. Neuhaus AA, Couch Y, Hadley G, Buchan AM. Neuroprotection in stroke: the importance of collaboration and reproducibility. Brain. (2017) 140:2079–92. doi: 10.1093/brain/awx126
7. Saini V, Guada L, Yavagal DR. Global epidemiology of stroke and access to acute ischemic stroke interventions. Neurology. (2021) 97:S6–S16. doi: 10.1212/WNL.0000000000012781
8. Zhao L-R, Willing A. Enhancing endogenous capacity to repair a stroke-damaged brain: an evolving field for stroke research. Prog Neurobiol. (2018) 163:5–26. doi: 10.1016/j.pneurobio.2018.01.004
9. Konduri P, van Voorst H, Bucker A, van Kranendonk K, Boers A, Treurniet K, et al. Posttreatment ischemic lesion evolution is associated with reduced favorable functional outcome in patients with stroke. Stroke. (2021) 52:3523–31. doi: 10.1161/STROKEAHA.120.032331
10. Xiong XY, Liu L, Yang QW. Refocusing neuroprotection in cerebral reperfusion era: new challenges and strategies. Front Neurol. (2018) 9:249. doi: 10.3389/fneur.2018.00249
11. Wang L, Xiong X, Zhang L, Shen J. Neurovascular unit: a critical role in ischemic stroke. CNS Neurosci Ther. (2021) 27:7–16. doi: 10.1111/cns.13561
12. del Zoppo GJ. The neurovascular unit in the setting of stroke. J Intern Med. (2010) 267:156–71. doi: 10.1111/j.1365-2796.2009.02199.x
13. Chamorro Á, Lo EH, Renú A, van Leyen K, Lyden PD. The future of neuroprotection in stroke. J Neurol Neurosurg Psychiatr. (2021) 92:129–35. doi: 10.1136/jnnp-2020-324283
14. Marmolejo-Martínez-Artesero S, Casas C, Romeo-Guitart D. Endogenous mechanisms of neuroprotection: to boost or not to be. Cells. (2021) 10:370. doi: 10.3390/cells10020370
15. del Barco DG, Montero E, Coro-Antich RM, Brown E, Suarez-Alba J, Lopez L, et al. Coadministration of epidermal growth factor and growth hormone releasing peptide-6 improves clinical recovery in experimental autoimmune encephalitis. Restor Neurol Neurosci. (2011) 29: 243–52. doi: 10.3233/RNN-2011-0595
16. Del Barco DG, Perez-Saad H, Rodriguez V, Marin J, Falcon V, Martin J, et al. Therapeutic effect of the combined use of growth hormone releasing peptide-6 and epidermal growth factor in an axonopathy model. Neurotox Res. (2011) 19:195–209. doi: 10.1007/s12640-010-9160-8
17. Garcia Del Barco-Herrera D, Martinez NS, Coro-Antich RM, Machado JM, Alba JS, Salgueiro SR, et al. Epidermal growth factor and growth hormone-releasing peptide-6: combined therapeutic approach in experimental stroke. Restor Neurol Neurosci. (2013) 31:213–23. doi: 10.3233/RNN-120262
18. Subiros N, Perez-Saad H, Aldana L, Gibson CL, Borgnakke WS, Garcia-Del-Barco D. Neuroprotective effect of epidermal growth factor plus growth hormone-releasing peptide-6 resembles hypothermia in experimental stroke. Neurol Res. (2016) 38:950–8. doi: 10.1080/01616412.2016.1235249
19. Subiros N, Perez-Saad HM, Berlanga JA, Aldana L, Garcia-Illera G, Gibson CL, et al. Assessment of dose-effect and therapeutic time window in preclinical studies of rhEGF and GHRP-6 coadministration for stroke therapy. Neurol Res. (2016) 38:187–95. doi: 10.1179/1743132815Y.0000000089
20. Yang S, Jin H, Zhao ZG. Epidermal growth factor treatment has protective effects on the integrity of the blood-brain barrier against cerebral ischemia injury in bEnd3 cells. Exp Ther Med. (2019) 17:2397–402. doi: 10.3892/etm.2019.7186
21. Pan W, Kastin AJ. Entry of EGF into brain is rapid and saturable. Peptides. (1999) 20:1091–8. doi: 10.1016/S0196-9781(99)00094-7
22. Kumarnsit E, Johnstone LE, Leng G. Actions of neuropeptide Y and growth hormone secretagogues in the arcuate nucleus and ventromedial hypothalamic nucleus. Eur J Neurosci. (2003) 17:937–44. doi: 10.1046/j.1460-9568.2003.02521.x
23. Dickson SL, Leng G, Dyball REJ, Smith RG. Central actions of peptide and non-peptide growth hormone secretagogues in the rat. Neuroendocrinology. (1995) 61:36–43. doi: 10.1159/000126825
24. Guan X-M, Yu H, Palyha OC, McKee KK, Feighner SD, Sirinathsinghji DJ, et al. Distribution of mRNA encoding the growth hormone secretagogue receptor in brain and peripheral tissues. Mol brain Res. (1997) 48:23–9. doi: 10.1016/S0169-328X(97)00071-5
25. Novak U, Walker F, Kaye A. Expression of EGFR-family proteins in the brain: role in development, health and disease. J Clin Neurosci. (2001) 8:106–11. doi: 10.1054/jocn.2000.0799
26. Niidome T, Morimoto N, Iijima S, Akaike A, Kihara T, Sugimoto H. Mechanisms of cell death of neural progenitor cells caused by trophic support deprivation. Eur J Pharmacol. (2006) 548:1–8. doi: 10.1016/j.ejphar.2006.07.052
27. Delgado-Rubin A, Chowen JA, Argente J, Frago LM. Growth hormone-releasing peptide 6 protection of hypothalamic neurons from glutamate excitotoxicity is caspase independent and not mediated by insulin-like growth factor I. Eur J Neurosci. (2009) 29:2115–24. doi: 10.1111/j.1460-9568.2009.06770.x
28. Casper D, Blum M. Epidermal growth factor and basic fibroblast growth factor protect dopaminergic neurons from glutamate toxicity in culture. J Neurochem. (1995) 65:1016–26. doi: 10.1046/j.1471-4159.1995.65031016.x
29. Delgado-Rubín de Célix A, Chowen JA, Argente J, Frago LM. Growth hormone releasing peptide-6 acts as a survival factor in glutamate-induced excitotoxicity. J Neurochem. (2006) 99:839–49. doi: 10.1111/j.1471-4159.2006.04122.x
30. Scalabrino G. Epidermal growth factor in the CNS: a beguiling journey from integrated cell biology to multiple sclerosis. An extensive translational overview. Cell Mol Neurobiolgy. (2020) 21:1–26. doi: 10.1007/s10571-020-00989-x
31. Frago L. M., Chowen J. A. Basic Physiology of the Growth Hormone/Insulin-Like Growth Factor Axis. In: Varela-Nieto I, Chowen J, , editors. The Growth Hormone/Insulin-Like Growth Factor Axis During Development. Boston, MA: Springer (2005). p. 1–25.
32. Cabrales A, Gil J, Fernandez E, Valenzuela C, Hernandez F, Garcia I, et al. Pharmacokinetic study of growth hormone-releasing peptide 6 (GHRP-6) in nine male healthy volunteers. Eur J Pharm Sci. (2013) 48:40–6. doi: 10.1016/j.ejps.2012.10.006
33. Palomino A, Hernandez-Bernal F, Haedo W, Franco S, Mas J, Fernández J, et al. A multicenter, randomized, double-blind clinical trial examining the effect of oral human recombinant epidermal growth factor on the healing of duodenal ulcers. Scand J Gastroenterol. (2000) 35:1016–22. doi: 10.1080/003655200451126
34. Ioannidis JP, Evans SJ, Gøtzsche PC, O'Neill RT, Altman DG, Schulz K, et al. Better reporting of harms in randomized trials: an extension of the CONSORT statement. Annal Int Med. (2004) 141:781–8. doi: 10.7326/0003-4819-141-10-200411160-00009
35. Moher D, Hopewell S, Schulz KF, Montori V, Gøtzsche PC, Devereaux PJ, et al. CONSORT 2010 Explanation and Elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. (2010) 340:c869. doi: 10.1136/bmj.c869
36. CECMED. Center for state control on the quality of medicines. Good clinical practices in Cuba. MINSAP Resol. (2000) 165:48.
37. Dixon JR. The international conference on harmonization good clinical practice guideline. Q Assurance. (1999) 6:65–74. doi: 10.1080/105294199277860
38. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. (2013) 310:2191–4. doi: 10.1001/jama.2013.281053
39. Carter RE, Woolson RF. Statistical design considerations for pilot studies transitioning therapies from the bench to the bedside. J Transl Med. (2004) 2:1–3. doi: 10.1186/1479-5876-2-37
40. Buergo-Zuaznábar MA, Fernández-Concepción O, Pérez-Nellar J, Lara-Fernández G, Maya-Entenza C, Pando-Cabrera A. Guías de práctica clínica para las enfermedades cerebrovasculares. Medisur. (2007) 5:20. Available online at: https://www.redalyc.org/articulo.oa?id=180020185002
41. Sharma V, McNeill JH. To scale or not to scale: the principles of dose extrapolation. Br J Pharmacol. (2009) 157:907–21. doi: 10.1111/j.1476-5381.2009.00267.x
42. Naranjo C., Shear N., Busto U. Adverse drug reactions. In: Kalant H, Roschlau W, , editors. Principles of Medical Pharmacology, 6th Edn. New York, NY: Oxford University Press (1998). p. 791–800.
43. Fernández-Montequín JI, Betancourt BY, Leyva-Gonzalez G, Mola EL, Galán-Naranjo K, Ramírez-Navas M, et al. Intralesional administration of epidermal growth factor-based formulation (Heberprot-P) in chronic diabetic foot ulcer: treatment up to complete wound closure. Int Wound J. (2009) 6:67–72. doi: 10.1111/j.1742-481X.2008.00561.x
44. Spilker J, Kongable G, Barch C, Braimah J, Bratina P, Daley S, et al. Using the NIH Stroke Scale to assess stroke patients. J Neurosci Nurs. (1997) 29:384–93. doi: 10.1097/01376517-199712000-00008
45. Lai S-M, Duncan PW. Stroke recovery profile and the Modified Rankin assessment. Neuroepidemiology. (2001) 20:26–30. doi: 10.1159/000054754
46. Ehrenreich H, Hasselblatt M, Dembowski C, Cepek L, Lewczuk P, Stiefel M, et al. Erythropoietin therapy for acute stroke is both safe and beneficial. Mol Med. (2002) 8:495–505. doi: 10.1007/BF03402029
47. Thall PF, Estey EH. A Bayesian strategy for screening cancer treatments prior to phase II clinical evaluation. Stat Med. (1993) 12:1197–211. doi: 10.1002/sim.4780121303
48. Johnson VE. Bayes factors based on test statistics. J Royal Stat Soc Series B. (2005) 67:689–701. doi: 10.1111/j.1467-9868.2005.00521.x
49. Lenhard W, Lenhard A. Computation of effect sizes. Psychometrica. (2016). doi: 10.13140/RG.2.2.17823.92329
50. Chhatbar PY, Ramakrishnan V, Kautz S, George MS, Adams RJ, Feng W. Transcranial direct current stimulation post-stroke upper extremity motor recovery studies exhibit a dose–response relationship. Brain Stimul. (2016) 9:16–26. doi: 10.1016/j.brs.2015.09.002
51. Chaisinanunkul N, Adeoye O, Lewis R, Grotta J, Broderick J, Jovin T, et al. Adopting a patient-centered approach to primary outcome analysis of acute stroke trials using a utility-weighted modified rankin scale. Stroke. (2015) 46:2238–43. doi: 10.1161/STROKEAHA.114.008547
52. Broderick JP, Adeoye O, Elm J. Evolution of the modified Rankin scale and its use in future stroke trials. Stroke. (2017) 48:2007–12. doi: 10.1161/STROKEAHA.117.017866
53. Zhang L, Zhang ZG, Chopp M. The neurovascular unit and combination treatment strategies for stroke. Trends Pharmacol Sci. (2012) 33:415–22. doi: 10.1016/j.tips.2012.04.006
54. Dearborn J. L., Gottesman R. F. Hypertension: The Major Risk Factor for Stroke. In: Seshadri S, Debette S, , editors. Risk Factors for Cerebrovascular Disease and Stroke. Oxford: Oxford University Press (2016), p. 155–79.
55. Alper BS, Foster G, Thabane L, Rae-Grant A, Malone-Moses M, Manheimer E. Thrombolysis with alteplase 3-45 hours after acute ischaemic stroke: trial reanalysis adjusted for baseline imbalances. BMJ Evid Based Med. (2020) 25:168–71. doi: 10.1136/bmjebm-2020-111386
56. Johansson I, Destefanis S, Aberg ND, Åberg MA, Blomgren K, Zhu C, et al. Proliferative and protective effects of growth hormone secretagogues on adult rat hippocampal progenitor cells. Endocrinology. (2008) 149:2191–9. doi: 10.1210/en.2007-0733
57. Romano R, Bucci C. Role of EGFR in the nervous system. Cells. (2020) 9:1887. doi: 10.3390/cells9081887
58. Nayani S, Sreedharan SE, Namboodiri N, Sarma PS, Sylaja P. Autonomic dysfunction in first ever ischemic stroke: prevalence, predictors and short term neurovascular outcome. Clin Neurol Neurosurg. (2016) 150:54–8. doi: 10.1016/j.clineuro.2016.08.022
59. Jimenez-Ruiz A, Racosta JM, Kimpinski K, Hilz MJ, Sposato LA. Cardiovascular autonomic dysfunction after stroke. Neurol Sci. (2021) 42:1751–8. doi: 10.1007/s10072-021-05128-y
60. Constantinescu V, Arsenescu-Georgescu C, Matei D, Moscalu M, Corciova C, Cuciureanu D. Heart rate variability analysis and cardiac dysautonomia in ischemic stroke patients. Clin Neurol Neurosurg. (2019) 186:105528. doi: 10.1016/j.clineuro.2019.105528
61. Ganesh A, Luengo-Fernandez R, Pendlebury ST, Rothwell PM, Study OV. Weights for ordinal analyses of the modified Rankin Scale in stroke trials: a population-based cohort study. EClinicalMedicine. (2020) 23:100415. doi: 10.1016/j.eclinm.2020.100415
62. Sullivan GM, Feinn R. Using effect size—or why the P value is not enough. J Grad Med Educ. (2012) 4:279–82. doi: 10.4300/JGME-D-12-00156.1
63. Ganesh A, Luengo-Fernandez R, Wharton RM, Rothwell PM. Ordinal vs dichotomous analyses of modified Rankin Scale, 5-year outcome, and cost of stroke. Neurology. (2018) 91:e1951–e60. doi: 10.1212/WNL.0000000000006554
64. Hsieh Y-W, Wang C-H, Wu S-C, Chen P-C, Sheu C-F, Hsieh C-L. Establishing the minimal clinically important difference of the Barthel Index in stroke patients. Neurorehabil Neural Repair. (2007) 21:233–8. doi: 10.1177/1545968306294729
65. Ma Y, Deng K, Liu J, Ma B, Mei F, Hui W, et al. The add-on effects of Danhong injection among patients with ischemic stroke receiving Western medicines: A systematic review and meta-analysis. Front Pharmacol. (2022) 13:937639. doi: 10.3389/fphar.2022.937369
66. Narayan Arya K, Verma R, Garg R. Estimating the minimal clinically important difference of an upper extremity recovery measure in subacute stroke patients. Top Stroke Rehabil. (2011) 18:599–610. doi: 10.1310/tsr18s01-599
67. Cranston JS, Kaplan BD, Saver JL. Minimal clinically important difference for safe and simple novel acute ischemic stroke therapies. Stroke. (2017) 48:2946–51. doi: 10.1161/STROKEAHA.117.017496
68. Feeny D. A utility approach to the assessment of health-related quality of life. Med Care. (2000) 38:II151–II4. doi: 10.1097/00005650-200009002-00022
69. Tokunboh I, Sung EM, Chatfield F, Gaines N, Nour M, Starkman S, et al. Improving Visualization Methods of Utility-Weighted Disability Outcomes for Stroke Trials. Frontiers in Neurology (2022) 998. doi: 10.3389/fneur.2022.875350
70. Rebchuk A.D., O'Neill Z.R., Szefer E.K., Hill M.D., Field T.S. Health utility weighting of the modified Rankin scale: a systematic review and meta-analysis. JAMA network open (2020) 3: e203767-e. doi: 10.1001/jamanetworkopen.2020.3767
71. Chan SJ, Love C, Spector M, Cool SM, Nurcombe V, Lo EH. Endogenous regeneration: Engineering growth factors for stroke. Neurochem Int. (2017) 107:57–65. doi: 10.1016/j.neuint.2017.03.024
72. Aguirre A, Dupree JL, Mangin J, Gallo V. A functional role for EGFR signaling in myelination and remyelination. Nat Neurosci. (2007) 10:990–1002. doi: 10.1038/nn1938
73. Xin W-Q, Wei W, Pan Y-L, Cui B-L, Yang X-Y, Bähr M, et al. Modulating poststroke inflammatory mechanisms: novel aspects of mesenchymal stem cells, extracellular vesicles and microglia. World J Stem Cells. (2021) 13:1030. doi: 10.4252/wjsc.v13.i8.1030
74. Dhir N, Medhi B, Prakash A, Goyal MK, Modi M, Mohindra S. Pre-clinical to clinical translational failures and current status of clinical trials in stroke therapy: A brief review. Curr Neuropharmacol. (2020) 18:596–612. doi: 10.2174/1570159X18666200114160844
75. Hróbjartsson A, Emanuelsson F, Skou Thomsen AS, Hilden J, Brorson S. Bias due to lack of patient blinding in clinical trials. A systematic review of trials randomizing patients to blind and nonblind sub-studies. Int J Epidemiol. (2014) 43:1272–83. doi: 10.1093/ije/dyu115
76. Øverberg LT, Lugg EF, Gaarder M, Langhammer B, Thommessen B, Rønning OM, et al. Plasma levels of BDNF and EGF are reduced in acute stroke patients. Heliyon. (2022) 12:e09661. doi: 10.1016/j.heliyon.2022.e09661
Keywords: ischemic stroke, brain ischemia, epidermal growth factor, growth hormone-releasing hexapeptide, clinical trial, combination drug therapy, neuroprotection, effect size
Citation: Hernández-Bernal F, Estenoz-García D, Gutiérrez-Ronquillo JH, Martín-Bauta Y, Catasús-Álvarez K, Gutiérrez-Castillo M, Guevara-Rodríguez M, Castro-Jeréz A, Fuentes-González Y, Pinto-Cruz Y, Valenzuela-Silva C, Muzio-González VL, Pérez-Saad H, Subirós-Martínez N, Guillén-Nieto GE and Garcia-del-Barco-Herrera D (2024) Combination therapy of Epidermal Growth Factor and Growth Hormone-Releasing Hexapeptide in acute ischemic stroke: a phase I/II non-blinded, randomized clinical trial. Front. Neurol. 15:1303402. doi: 10.3389/fneur.2024.1303402
Received: 27 September 2023; Accepted: 14 March 2024;
Published: 04 April 2024.
Edited by:
Gabriel Broocks, University of Hamburg, GermanyReviewed by:
Nora Ramdani, University Medical Center Hamburg-Eppendorf, GermanyCopyright © 2024 Hernández-Bernal, Estenoz-García, Gutiérrez-Ronquillo, Martín-Bauta, Catasús-Álvarez, Gutiérrez-Castillo, Guevara-Rodríguez, Castro-Jeréz, Fuentes-González, Pinto-Cruz, Valenzuela-Silva, Muzio-González, Pérez-Saad, Subirós-Martínez, Guillén-Nieto and Garcia-del-Barco-Herrera. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Diana Garcia-del-Barco-Herrera, ZGlhbmEuZ2FyY2lhQGNpZ2IuZWR1LmN1
‡ORCID: Francisco Hernández-Bernal orcid.org/0000-0002-1857-4219
Donner Estenoz-García orcid.org/0000-0002-6834-7348
Juan H. Gutiérrez-Ronquillo orcid.org/0000-0001-7089-1281
Yenima Martín-Bauta orcid.org/0000-0002-8673-9425
Karen Catasús-Álvarez orcid.org/0000-0001-8349-4111
Mario Gutiérrez-Castillo orcid.org/0000-0003-1733-0914
Marbelys Guevara-Rodríguez orcid.org/0000-0001-8860-3479
Aliuska Castro-Jeréz orcid.org/0000-0002-4411-8137
Yoandra Fuentes-González orcid.org/0000-0002-1634-3118
Yulemis Pinto-Cruz orcid.org/0000-0002-1805-4029
Carmen Valenzuela-Silva orcid.org/0000-0002-1082-2089
Verena L. Muzio-González orcid.org/0000-0001-8595-9170
Héctor Pérez-Saad orcid.org/0000-0003-1133-4308
Nelvys Subirós-Martínez orcid.org/0000-0002-4024-7759
Gerardo E. Guillén-Nieto orcid.org/0000-0003-3098-0970
Diana Garcia-del-Barco-Herrera orcid.org/0000-0003-3654-490x
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.