 Lisa B. E. Shields
Lisa B. E. Shields Vasudeva G. Iyer
Vasudeva G. Iyer Yi Ping Zhang
Yi Ping Zhang Christopher B. Shields
Christopher B. Shields- 1Norton Neuroscience Institute, Norton Healthcare, Louisville, KY, United States
- 2Neurodiagnostic Center of Louisville, Louisville, KY, United States
- 3Department of Neurological Surgery, University of Louisville School of Medicine, Louisville, KY, United States
Objectives: Gunshot wounds of the upper extremities may cause permanent neurovascular injuries, leading to significant morbidity, chronic pain, functional loss, and disability. While there are many reports on the incidence and intraoperative findings in gunshot-related nerve injuries (GSNI) sustained during wars, there is a paucity of details pertaining to GSNI of the upper extremities in civilians. The goal of this paper is to provide the clinical, electrodiagnostic (EDX), and ultrasound (US) findings in 22 patients with GSNI of the upper extremities.
Methods: This is a retrospective study of patients referred for EDX studies to evaluate the presence of nerve injury after sustaining GSWs to the upper extremities. All patients underwent EDX studies, and 16 patients had US evaluations. Numerous metrics were documented including presenting symptoms, neurological abnormalities, EDX findings, and US features.
Results: The forearm was the most frequent location of injury (8 [36%] patients). The ulnar nerve was the most common injured nerve (10 [45%] patients), followed by the brachial plexus (7 [32%] patients). All patients complained of muscle weakness; the most frequently affected muscles were the first dorsal interosseous (FDI) (14 [64%] patients) and abductor pollicis brevis (APB) (11 [50%] patients). Muscle atrophy was noted in 19 (86%) patients, 15 of whom had atrophy of the FDI. Axonotmesis was the type of nerve injury in all patients based on EDX studies. Of the 16 patients who underwent US studies, a neuroma in continuity was noted in 4 (25%) patients and neurotmesis in 1 (6.2%) patient. Eleven (69%) patients had enlarged and/or hypoechoic nerves.
Conclusions: Axonotmesis of the ulnar nerve was the most common finding among patients sustaining gunshot injuries to the upper extremities. EDX and US studies provide valuable insight into the underlying pathophysiology and guidance for management of patients with GSNI of the upper extremities.
Introduction
According to the Centers for Disease Control and Prevention (CDC), more Americans died of gun-related injuries in 2021 than in any other year on record (1). Gun violence (unintentional, suicide, and homicide) is higher than motor vehicle accidents as the leading cause of trauma-related years of potential life lost (2). The burden of gun violence represents a dire public health issue that primarily affects the younger members of society (3). While gunshot wounds (GSWs) of the upper extremities are not commonly life threatening, they pose a high risk of long-term disability due to neurovascular injuries (4).
The mechanism of peripheral nerve injury caused by firearms involves either a direct transection of the nerve or indirect injury by producing thermal damage, shock waves, laceration secondary to fracture fragment displacement, or compression due to swelling or subacute scar formation (5–9). Traction injuries often spontaneously recover without surgical intervention, however, rupture and avulsion injuries usually require surgery and have a worse prognosis. Patients who undergo surgery within 6 months of the injuries usually have a better outcome (6, 7, 10–12). Additionally, vascular injury and fractures increase the risk of nerve injury after GSWs (9).
Firearm injuries of peripheral nerves can cause neuropraxia, axonotmesis, and/or neurotmesis (Table 1) (12). Low-velocity projectiles often damage nerves by direct impact leading to neuropraxia or axonotmesis, and patients usually have significant return of function within several months. High-velocity injuries are caused by shock waves or cavitation effects with ensuing stretching and compression often outside the path of the projectile and across longer nerve segments. Significant return of function is infrequent with high-velocity projectiles. Unlike the military, most of the gunshot injuries in a community setting inflict low-energy penetrating trauma (9).
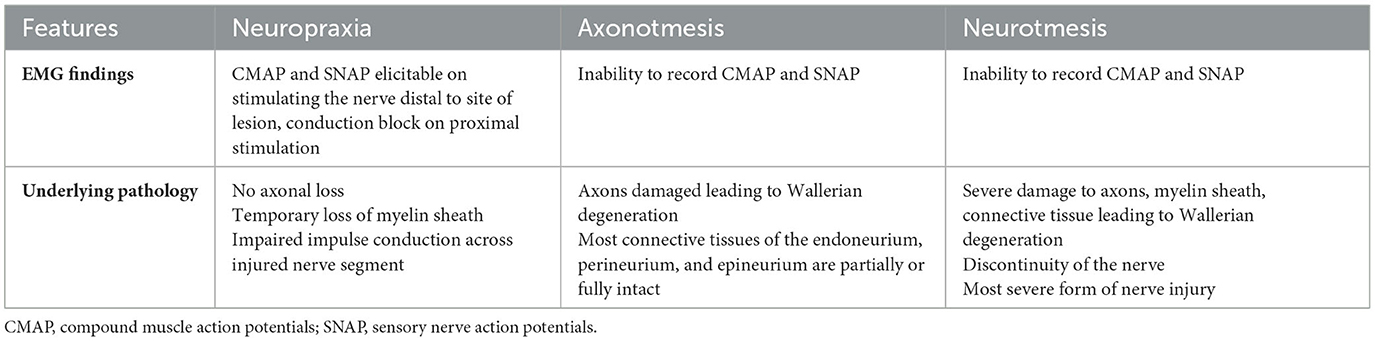
Table 1. Differentiating between neuropraxia, axonotmesis, and neurotmesis.
Clinical examination alone cannot differentiate between neuropraxia, axonotmesis, and neurotmesis (7). EDX can differentiate between neuropraxia and axonotmesis 1–2 weeks after the injury but cannot distinguish neurotmesis from axonotmesis; US evaluation can make that distinction (13). Combining EDX and US can provide critical information in planning management of patients with nerve injuries. Prompt identification of nerve laceration is crucial as it requires surgical repair, while there is controversy about treatment for nerves with neuroma in continuity (7). A total of 70% of nerves in continuity regain function after 3–9 months of observation according to Pannell et al. (7).
We report 22 patients with GSWs of the upper extremities leading to nerve injuries and were referred for EDX studies. Sixteen (73%) patients also had US studies. The presenting symptoms, clinical and EDX findings, and US features of these patients are highlighted. The value of EDX and US studies in the evaluation of firearm wounds of the upper extremities as well as management of these type of injuries are discussed. We also describe the impact of the COVID-19 pandemic on the increased incidence of firearm injuries both nationally and among patients seen in our facility.
Methods
Study population and electrodiagnostic/ultrasound studies
This was a retrospective study under an Institutional Review Board (IRB)-approved protocol. Inclusion criteria included patients referred to our facility for EDX studies to evaluate for the presence of a nerve injury after sustaining a GSW to the upper extremities during the 8-year (2016–2023) period. The patients underwent clinical neurological examination followed by nerve conduction and EMG studies. The EDX studies were performed in our American Association of Neuromuscular and Electrodiagnostic Medicine (AANEM)-accredited facility using standard protocol of our laboratory (14). Patients in whom EDX studies did not show evidence for nerve injuries were excluded from the study. The US studies were conducted using the GE Logiq E system and 12–18 MHz probe (six patients were seen before the US machine was available to us). Short axis views at, proximal to, and distal to the injury were obtained to evaluate the cross-sectional area (CSA), fascicular pattern, and altered echogenicity (15). Long axis views were also studied. Several metrics were collected including the patients' gender and age, location of projectile entry, the specific nerve(s) injured, and the type of injury (neuropraxia, axonotmesis, or neurotmesis).
Ethical approval and informed consent
Informed consent was obtained from all patients. The IRB determined that our study was exempt according to 45 CFR 46.101(b) under Category 4. The IRB number is 22.1087.
Results
Clinical findings
A total of 22 patients sustained gunshot injuries of the upper extremities (Table 2). The mean age was 38 years (range: 14–68 years), and 19 (86%) patients were male. The left side was more commonly (13 [59%] patients) injured. A total of 21 (95%) patients had single projectile entry, while one (5%) had three entries of the same upper extremity. Another six (73%) patients sustained both the entry and exit wounds in the same upper extremity (Figures 1A–C, 2A). The forearm was the most frequent entry wound location (8 [36%] patients). The ulnar nerve was the most commonly injured nerve (10 [45%] patients), followed by the brachial plexus (seven [32%] patients). Nine (41%) patients suffered GSWs of the upper extremities prior to the COVID-19 pandemic, while there were 13 (59%) victims after the COVID-19 onset.
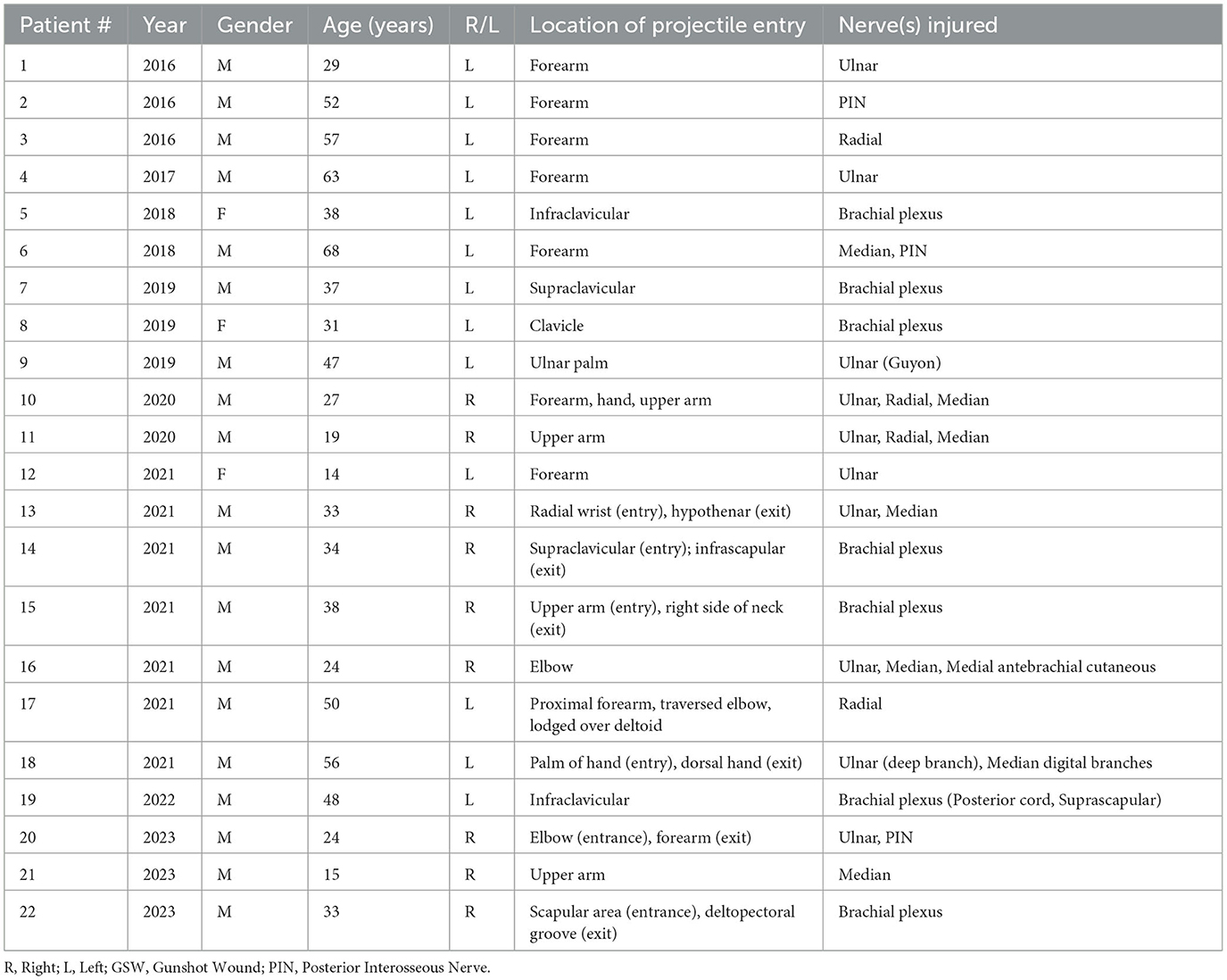
Table 2. Demographics of patients with gunshot-related nerve injuries to the upper extremities referred for EDX studies.
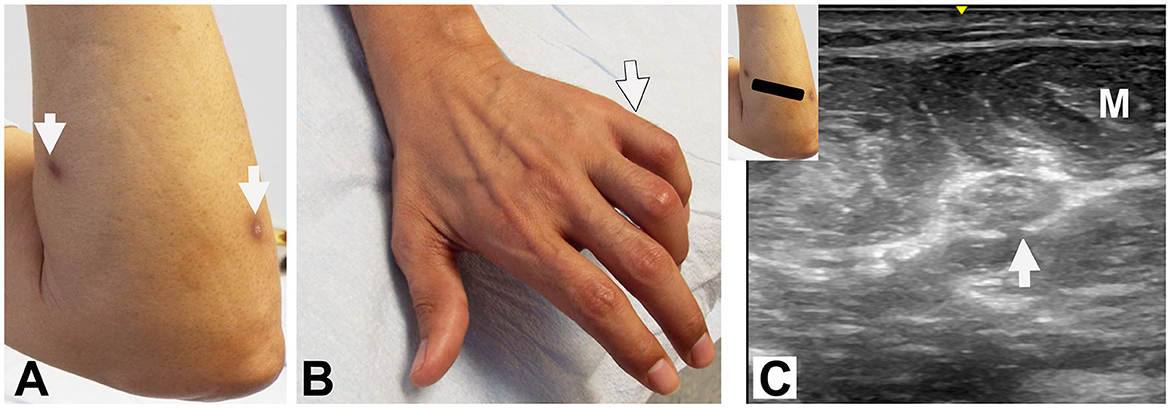
Figure 1. Patient #4: (A) Entry: dorsal proximal forearm (right arrow). Exit: ventral proximal forearm (left arrow). (B) Clawing of digits 4 and 5 (arrow). (C) Ultrasound: Short axis view at proximal forearm shows enlarged ulnar nerve (cross-sectional area 18mm2) (arrow) with loss of fascicular pattern. M: Flexor carpi ulnaris muscle.
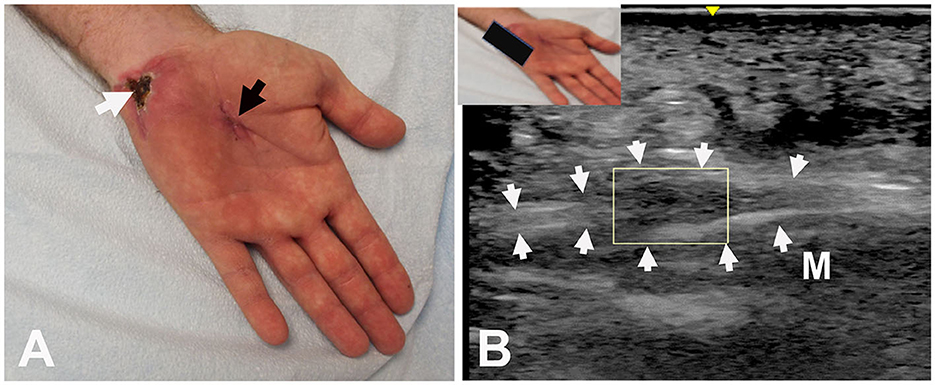
Figure 2. Patient #9: (A) Entry in palm (black arrow) and exit at base of hypothenar eminence (white arrow). (B) Ultrasound: Long axis view shows hypoechoic enlargement of the ulnar nerve (neuroma in continuity) (box). Arrows outline the ulnar nerve. M: Abductor digiti minimi muscle.
All patients experienced significant muscle weakness of the upper extremities following the gunshot injuries (Table 3). The most frequently affected muscles that caused decreased or absent muscle contraction were the first dorsal interosseous (FDI) (14 [64%] patients), abductor pollicis brevis (APB) (11 [50%] patients), and abductor digiti minimi (ADM) and extensor digitorum communis (EDC) (each 7 [32%] patients). Muscle atrophy (clinical observation) was noted in 19 (86%) patients, 15 of whom had atrophy of the FDI (Figures 3A–D). A total of 19 of the 22 patients showed sensory loss corresponding to the nerve injured.
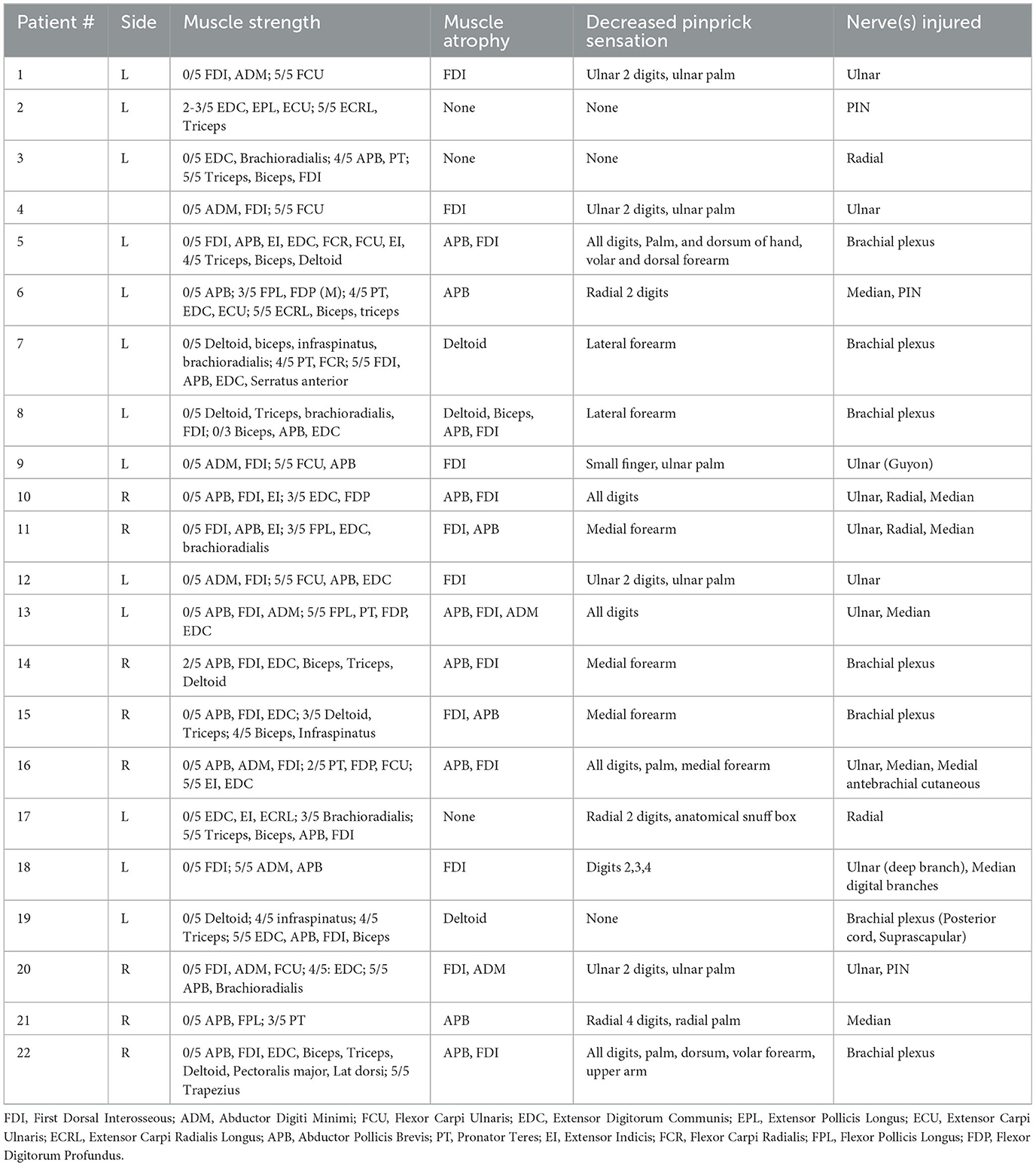
Table 3. Clinical findings of patients with gunshot-related nerve injuries to the upper extremities.
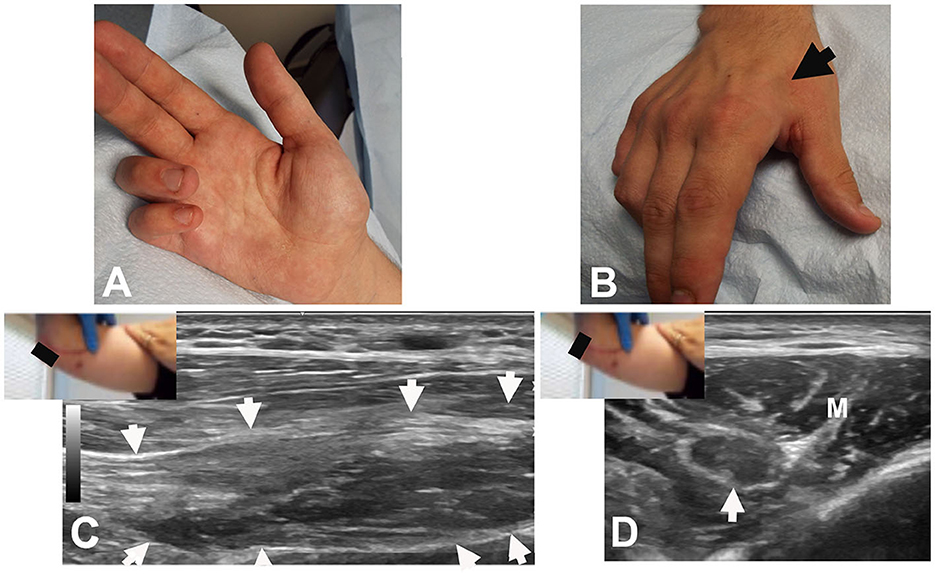
Figure 3. Patient #20: (A) Clawing of ulnar 2 digits of right hand. (B) Atrophy of FDI (arrow). (C) Long axis view at the elbow showing neuroma in continuity (arrows). The black rectangle denotes the position of the US probe. (D) Short axis view at the elbow showing the neuroma (arrow); the nerve is hypoechoic with epineural thickening. Note the transition from fascicular edema (on the left) to irregular echotexture (to the right). M: Flexor carpi ulnaris muscle.
Electrodiagnostic studies
Denervation of muscles as well as absence/decreased amplitude of compound muscle action potential (CMAP) and sensory nerve action potential (SNAP) suggested axonal injury in all patients. Distinction between axonotmesis and neurotmesis could not be made based on the EDX findings.
Ultrasound studies
Of the 16 patients who underwent US studies, a neuroma in continuity (Figures 2B, 3C) was observed in four (25%) patients (Table 4). Eleven (69%) patients had enlarged and/or hypoechoic nerves, often with large fascicles (Figure 4). One patient showed features of neurotmesis (Figure 5). Other findings included epineural and perineural thickening (hyperechoic appearance), loss of fascicular pattern and fascicular discontinuity (Table 4).
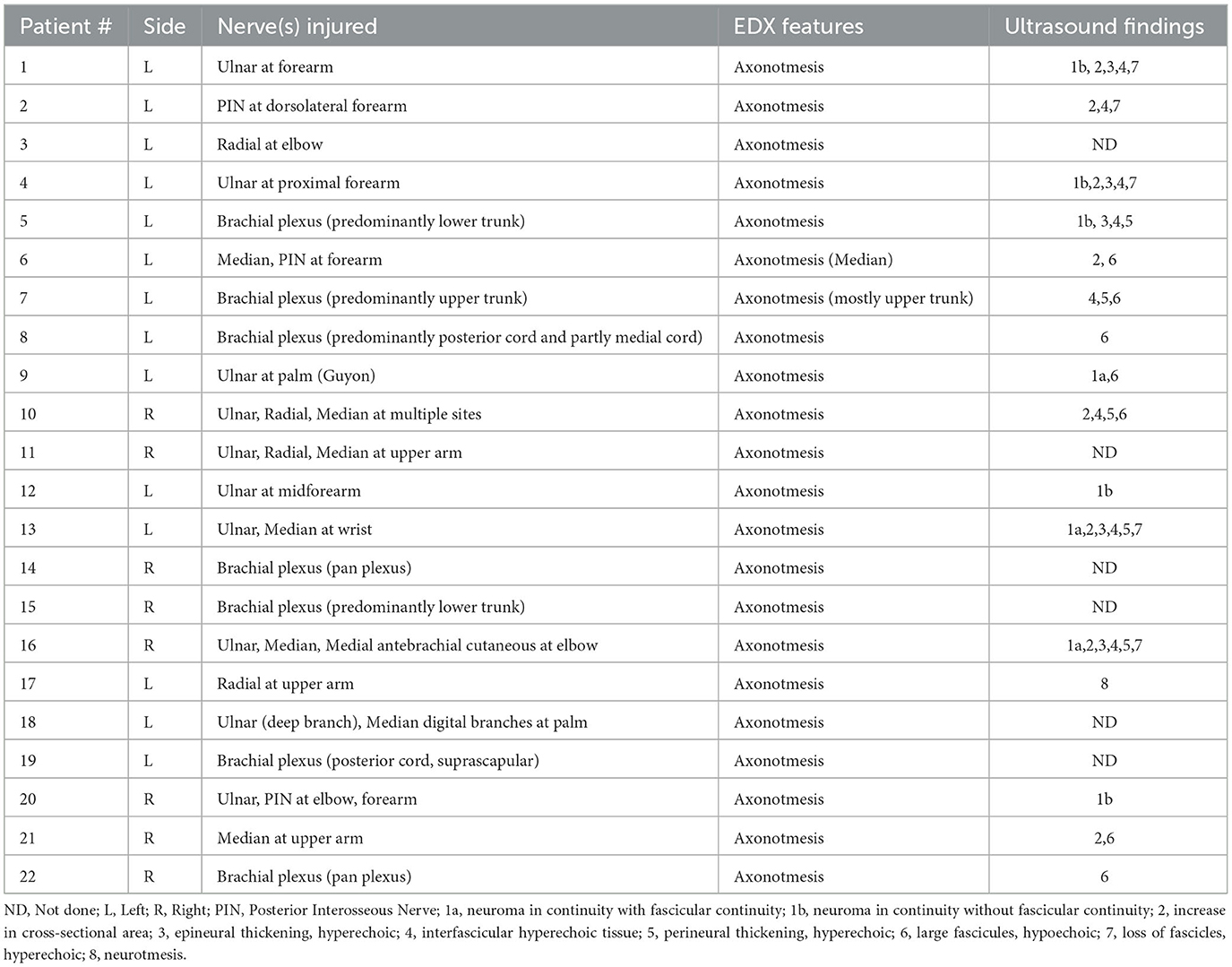
Table 4. Neurological and ultrasound findings of patients with gunshot-related nerve injuries of the upper extremities.
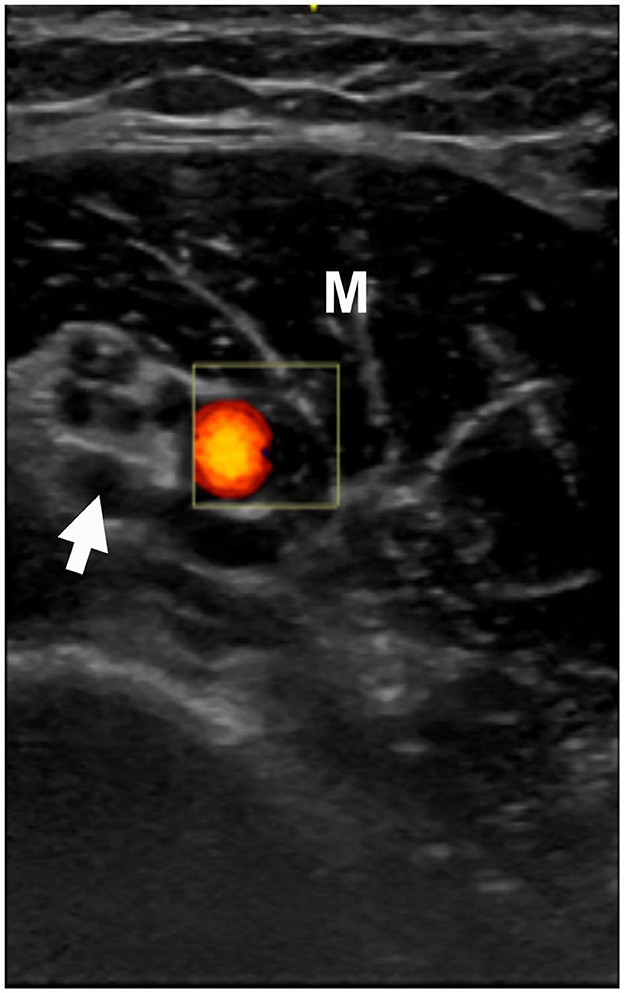
Figure 4. Patient #21: Ultrasound: short axis view at distal upper arm. Arrow points to the median nerve with hypoechoic enlarged fascicles and perineural thickening. The brachial artery is in orange color. M: Biceps muscle.

Figure 5. Patient #17 sustained a radial nerve injury (neurotmesis) at the upper arm. Figure shows terminal neuromas in the proximal and the distal portions of the injured nerve. H, Humerus.
Discussion
COVID-19 and GSWs
According to the Morbidity and Mortality Weekly Report, the firearm homicide rate in the United States increased by approximately 35% during the COVID-19 pandemic (16, 17). Compared with 2019, the average number of weekly Emergency Department (ED) visits for firearm injuries was 27% higher in 2020, 36% higher in 2021, and 20% higher in 2022 based on data from the National Vital Statistics System (17). The highest rate was observed among individuals ages 15–24 years. Similarly, we observed a higher number of upper extremities GSW injuries following the COVID-19 initiation compared to before COVID-19 (13 vs. nine patients, respectively), with eight patients evaluated in 2021 alone. This finding of the largest number of cases in 2021 concurs with the substantial increase in ED visits for firearm injuries specifically in 2021 as reported by the National Vital Statistics System. In Risinger and colleagues' study (2011–2021) of the association between COVID-19 and gun violence in our same county, the years of potential life lost was higher for firearm fatalities than COVID-19 (3). These authors attributed the increase in gun violence during COVID-19 primarily due to stay-at-home orders and decreased access to mental health care. Additional psychodynamic factors include diminished security and safety (housing and financial insecurity, elevated exposure to violence, fear of illness, uncertainty about the future), and increased firearm purchases (17). Numerous measures have been proposed to address the risk of gunshot injuries, including enhancing community and street outreach programs, initiating implement hospital-based violence prevention programs, enriching community physical environments, encouraging secure storage of firearms, and boosting social and economic supports (17).
Common nerves injured
Previous studies have reported gunshot injuries of the upper extremities with consequent peripheral nerve injuries, specifically, brachial plexus (6, 18, 19), radial nerve (5, 10, 20), ulnar nerve (12, 21), or a combination of upper extremity nerves (7, 8, 11, 22–25). In Secer and colleagues' 40-year study of 2,106 patients with 2,210 peripheral nerve lesions of the upper and lower extremities caused by combat-related GSWs, the median nerve was the most frequently injured upper extremity nerve followed by the ulnar nerve, radial nerve, and brachial plexus (8). In Pannell and colleagues' study (2007–2014) of 41 patients (59 nerves) who sustained firearm injuries of the upper extremities, there was a 63% incidence of nerve dysfunction after upper extremity GSWs (7). A higher frequency of fractures, retained fragments, vascular injury, and compartment syndrome in patients with nerve palsies was noted (7). Additionally, patients with palsies were significantly more likely to have nerve lacerations intraoperatively. Of the 59 nerves studied, 37 palsies were identified, including 13 ulnar, 8 median, and 7 radial. Ten of the 37 (27%) palsies had lacerated nerves, whereas nerve lacerations were not observed in patients without palsies. Straszewski et al. studied GSWs of the upper extremities in an urban trauma center; among 126 injuries in 117 patients, 38 had a documented nerve deficit (9). The location of injury was 18 in the arm, 13 in the forearm, six in both the arm and forearm, and one in the hand. The most common nerve injured was the radial nerve, followed by the ulnar and median nerves. In patients with a GSW to the forearm, the most common nerve injured was the ulnar nerve. In our study the most frequent nerve injured was the ulnar nerve, and the site of projectile entry was three at the forearm, two at the elbow, two at the palm, one at the wrist, and one at the upper arm. Henriques et al.'s study also noted the high frequency of ulnar nerve involvement (21). It is possible that the superficial location of the nerve at the elbow and the forearm makes it more vulnerable to injury.
The brachial plexus was the second most common site of GSW in our series. The projectile entry location included supraclavicular, clavicular, and infraclavicular areas; in one patient the projectile entered in the upper arm and exited on the left side of neck. Most brachial plexus injuries are due to traction injuries caused by motor vehicle accidents, however, ~3–12% result from GSWs (6, 19).
The radial/PIN nerve was injured in six patients in our study; in three patients, additional nerves were injured. In Guo et al.'s study of patients who sustained a gunshot injury of the radial nerve, only 30% of firearm radial nerve injuries were associated with another nerve injury in the upper extremity (5).
EDX studies
EDX studies play a valuable role in the investigation of gunshot injuries by detecting nerve injuries and recovery. They localize the site of the lesion, identify the type and severity of the lesion, and provide prognostic details pre- and postoperatively (6, 19, 26). EDX studies are crucial in differentiating conduction bock from axonal injury; they are also useful in differentiating total from partial injuries and to detect reinnervation. Serial EMGs are beneficial in analyzing the progression of recovery by assessing the presence of volitionally-recruited motor units and the quantity of fibrillation potentials (19). An important limitation of EDX is its inability to distinguish total axonotmesis from neurotmesis; combining EDX and US studies can potentially circumvent this limitation and lead to prompt surgical repair without delay in cases of neurotmesis.
In this series, the findings suggested axonotmesis in all patients. The EDX studies were performed in most patients 3 months after injury (ranging from 2 months to 12 months). Injuries of the brachial plexus were partial and involved trunks/cords.
Ultrasound study
An MRI is the gold standard for imaging nerve injuries of the upper extremities due to its multiplanar images and high-contrast resolution in soft tissues (6). However, this modality may be contraindicated in GSWs due to the presence of metal fragments which may shift, generate heat, and may cause imaging artifact. The readily available and cost-effective US may be a more useful technique to detail the anatomy of the injury without being limited by metal fragments. US also detects both nerve and vascular injury as well as the presence of neuroma formation and nerve structural integrity following firearm injuries (6, 27). In Fagan and colleagues' study of 17 patients who sustained a GSW of the upper or lower extremities and subsequently underwent neuromuscular US, all patients had either a nerve transection or neuroma in continuity of a major upper or lower extremity nerve at the site of the GSW (27). A total of 13 (76%) patients had significant morphological changes in distal segments of the injured nerve, and 12 (71%) had changes in other nearby distal nerves. Enlarged nerve cross-sectional area, enlarged fascicles, and hypoechogenicity were also frequently observed. These authors surmised that ballistic trauma of firearm injuries can result in concussive damage that disrupts the normal architecture of distal nerves (27). In Nwawka and colleagues' case series of 3 patients who sustained brachial plexus injuries due to firearms, the US revealed nerve abnormalities that complemented the EDX and intraoperative findings (6). Two of these patients experienced nerve transection of the median and ulnar nerves detected by US, one of whom also had a radial nerve transection. In this series four patients with brachial plexus injury showed hypoechoic enlarged trunks, perineural thickening and hyperechoic scar tissue surrounding the neural structures. Of the 16 patients who underwent US in the present study, a neuroma in continuity was observed in four patients, while 11 patients had enlarged and/or hypoechoic nerves. In one patient neurotmesis was noted (Table 4).
Among the advantages of US in comparison to MRI, dynamic evaluation can be useful for confirming neurotmesis and monitoring the recovery process. Additionally, US may detect compression by a hematoma and entrapment by scar tissue formation (28, 29).
Strengths and limitations
The strength of our study is the use of both EDX and US studies in evaluating a large cohort of gunshot-related nerve injuries of the upper extremities in a non-combat setting. This allowed us to correlate the clinical examination findings with the EDX and US features in these patients. Limitations of our study include its retrospective nature and lack of follow-up of patients after their EDX evaluation which has precluded our ability to assess the long-term outcome. Additional limitations include the lack of measuring the cross-sectional area of the different nerves using comparative scanning, the lack of color/power Doppler assessment of the pathological peripheral nerves, and the lack of sonographic follow-up.
Conclusion
Physicians should be cognizant of the potential for nerve injuries following GSWs and look for the clinical signs, diagnostic of injury to specific nerves. EDX and US studies should be utilized to determine the location and the type of nerve injury so that appropriate management can be initiated promptly.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by University of Louisville Institutional Review Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
LS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review and editing. VI: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review and editing. YZ: Resources, Software, Visualization, Writing – review and editing. CS: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – review and editing.
Funding
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Gramlich J. What the data says about gun deaths in the U.S. (2023). Available online at: https://pewresearch.org/short-reads/2023/04/26/what-the-data-says-about-gun-deaths-in-the-u-s/ (accessed December 20, 2023).
2. Klein J, Prabhakaran K, Latifi R, Rhee P. Firearms: the leading cause of years of potential life lost. Trauma Surg Acute Care Open. (2022) 7:e000766. doi: 10.1136/tsaco-2021-000766
3. Risinger WB, Pera SJ, Bhutiani N, Ruther M, Harbrecht BG, Smith JW et al. A new pandemic and an old epidemic: the impact of COVID-19 and gun violence as measured by years of potential life lost in a US city. Surgery. (2022) 172:1555–62. doi: 10.1016/j.surg.2022.06.040
4. Stein JS, Strauss E. Gunshot wounds to the upper extremity. Evaluation and management of vascular injuries. Orthop Clin North Am. (1995) 26:29–35. doi: 10.1016/S0030-5898(20)31965-9
5. Guo Y, Chiou-Tan FY. Radial nerve injuries from gunshot wounds and other trauma: comparison of electrodiagnostic findings. Am J Phys Med Rehabil. (2002) 81:207–11. doi: 10.1097/00002060-200203000-00009
6. Nwawka OK, Casaletto E, Wolfe SW, Feinberg JH. Ultrasound imaging of brachial plexus trauma in gunshot injury. Muscle Nerve. (2019) 59:707–11. doi: 10.1002/mus.26461
7. Pannell WC, Heckmann N, Alluri RK, Sivasundaram L, Stevanovic M, Ghiassi A. Predictors of nerve injury after gunshot wounds to the upper extremity. Hand (N Y). (2017) 12:501–6. doi: 10.1177/1558944716675294
8. Secer HI, Daneyemez M, Tehli O, Gonul E, Izci Y. The clinical, electrophysiologic, and surgical characteristics of peripheral nerve injuries caused by gunshot wounds in adults: a 40-year experience. Surg Neurol. (2008) 69:143–52. doi: 10.1016/j.surneu.2007.01.032
9. Straszewski AJ, Schultz K, Dickherber JL, Dahm JS, Wolf JM, Strelzow JA. Gunshot-related upper extremity nerve injuries at a level 1 trauma center. J Hand Surg Am. (2022) 47:88. doi: 10.1016/j.jhsa.2021.03.020
10. Akhavan-Sigari R, Mielke D, Farhadi A, Rohde V. Study of radial nerve injury caused by gunshot wounds and explosive injuries among Iraqi soldiers. Open Access Maced J Med Sci. (2018) 6:1622–6. doi: 10.3889/oamjms.2018.346
11. Ergen TJ, Ipaktchi K, Leversedge FJ, Lauder A. Nerve injury to the upper extremity after a gunshot wound; a systematic review. In: 2022 American Association for Hand Surgery Annual Meeting. January 11-15, 2022. Beverly, MA: American Association for Handy Surgery. Available online at: https://meeting.handsurgery.org/program/2022/HSEP116.cgi (accessed December 20, 2023).
12. Secer HI, Daneyemez M, Gonul E, Izci Y. Surgical repair of ulnar nerve lesions caused by gunshot and shrapnel: results in 407 lesions. J Neurosurg. (2007) 107:776–83. doi: 10.3171/JNS-07/10/0776
13. Iyer VG. Role of ultrasound in the EMG lab. Open Access J Neurol Neurosurg. (2021) 15:555910. doi: 10.19080/OAJNN.2021.15.555910
14. Iyer VG. Understanding nerve conduction and electromyographic studies. Hand Clin. (1993) 9:273–87. doi: 10.1016/S0749-0712(21)00968-9
15. Walker FO. and Cartwright, MS. Ultrasound of focal neuropathies Neuromuscular Ultrasound. Amsterdom: Elsevier. (2011). doi: 10.1016/B978-1-4377-1527-9.10005-1
16. Kegler SR, Simon TR, Zwald ML, Chen MS, Mercy JA, Jones CM et al. Vital signs: changes in firearm homicide and suicide rates - United States, 2019-2020. MMWR Morb Mortal Wkly Rep. (2022) 71:656–63. doi: 10.15585/mmwr.mm7119e1
17. Zwald ML, Van Dyke ME, Chen MS, Radhakrishnan L, Holland KM, Simon TR et al. Emergency department visits for firearm injuries before and during the COVID-19 pandemic - United States, January 2019-December 2022. MMWR Morb Mortal Wkly Rep. (2023) 72:333–7. doi: 10.15585/mmwr.mm7213a2
18. Kim DH, Murovic JA, Tiel RL, Kline DG. Penetrating injuries due to gunshot wounds involving the brachial plexus. Neurosurg Focus. (2004) 16:E3. doi: 10.3171/foc.2004.16.5.4
19. Park HR, Lee GS, Kim IS, Chang JC. Brachial plexus injury in adults. The Nerve. (2017) 3:1–11. doi: 10.21129/nerve.2017.3.1.1
20. Nikica D, Marijan C, Denis G, Zeljko R, Anela D, Egol K. Shotgun injury to the arm: a staged protocol for upper limb salvage. Mil Med. (2010) 175:206–11. doi: 10.7205/MILMED-D-09-00064
21. Henriques VM, Torrao FJL, Rosa LAN, Sanches GE, Guedes F. Surgery as an effective therapy for ulnar nerve neuropathic pain caused by gunshot wounds: a retrospective case series. World Neurosurg. (2023) 173:e207–17. doi: 10.1016/j.wneu.2023.02.033
22. Bercik MJ, Kingsbery J, Ilyas AM. Peripheral nerve injuries following gunshot fracture of the humerus. Orthopedics. (2012) 35:e349–52. doi: 10.3928/01477447-20120222-18
23. Duncan J, Kettelkamp DB. Low-velocity gunshot wounds of the hand. Arch Surg. (1974) 109:395–7. doi: 10.1001/archsurg.1974.01360030047012
24. Elstrom JA, Pankovich AM, Egwele R. Extra-articular low-velocity gunshot fractures of the radius and ulna. J Bone Joint Surg Am. (1978) 60:335–41. doi: 10.2106/00004623-197860030-00010
25. Pereira C, Boyd JB, Olsavsky A, Gelfand M, Putnam B. Outcomes of complex gunshot wounds to the hand and wrist: a 10-year level I urban trauma center experience. Ann Plast Surg. (2012) 68:374–7. doi: 10.1097/SAP.0b013e31823d2ca1
26. Kamble N, Shukla D, Bhat D. Peripheral nerve injuries: electrophysiology for the neurosurgeon. Neurol India. (2019) 67:1419–22. doi: 10.4103/0028-3886.273626
27. Fagan P, Geiger C, Preston D. Morphological changes on neuromuscular ultrasound in nerves distal to gunshot injuries. Neurology. (2023) 100:P14–8.003. doi: 10.1212/WNL.0000000000202943
28. Cocco G, Ricci V, Corvino A, Pacini P, Boccatonda A, Nanka O et al. Ultrasound imaging of the sciatic nerve. Ultraschall Med. (2023) 44:e263–73. doi: 10.1055/a-2095-2842
Keywords: neurology, gunshot, upper extremity, electrodiagnostic studies, ultrasound, COVID-19
Citation: Shields LBE, Iyer VG, Zhang YP and Shields CB (2024) Gunshot-related nerve injuries of the upper extremities: clinical, electromyographic, and ultrasound features in 22 patients. Front. Neurol. 14:1333763. doi: 10.3389/fneur.2023.1333763
Received: 06 November 2023; Accepted: 27 December 2023;
Published: 11 January 2024.
Edited by:
Sabrina Ravaglia, Neurological Institute Foundation Casimiro Mondino (IRCCS), ItalyReviewed by:
Vincenzo Ricci, Luigi Sacco Hospital, ItalyGiovanna Squintani, Unità di Allergia, Azienda Ospedaliera Universitaria Integrata Verona, Italy
Copyright © 2024 Shields, Iyer, Zhang and Shields. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Christopher B. Shields, Y2JzaGllbGRzMUBnbWFpbC5jb20=