 Isaíra Almeida Pereira da Silva Nascimento1†
Isaíra Almeida Pereira da Silva Nascimento1† Kátia Cirilo Costa Nobrega1
Kátia Cirilo Costa Nobrega1 Bruno Rafael Antunes Souza2Isabela Carneiro Barone1Giovanna Checchio1Vitória Pereira Ponciano1Clara Greif Cerveira de Paula1Arieni Nunes Possani1Natália Cardoso Penha1
Bruno Rafael Antunes Souza2Isabela Carneiro Barone1Giovanna Checchio1Vitória Pereira Ponciano1Clara Greif Cerveira de Paula1Arieni Nunes Possani1Natália Cardoso Penha1 André Frazão Helene3
André Frazão Helene3 Antonio Carlos Roque4
Antonio Carlos Roque4 Rodolfo Savica5
Rodolfo Savica5 Maria Elisa Pimentel Piemonte1*†
Maria Elisa Pimentel Piemonte1*†- 1Department of Physical Therapy, Speech Therapy, and Occupational Therapy, Faculty of Medical Science, University of São Paulo, São Paulo, Brazil
- 2Department of Neuroscience and Behavior, Institute of Psychology, University of São Paulo, São Paulo, Brazil
- 3Department of Physiology, Institute of Biosciences, University of São Paulo, São Paulo, Brazil
- 4Department of Physics, School of Philosophy, Sciences, and Letters of Ribeirão Preto, University of São Paulo, Ribeirão Preto, Brazil
- 5Department of Neurology, Mayo Clinic, Rochester, MN, United States
Background: Parkinson’s disease (PD) is a degenerative neurological disorder that usually affects people over the age of 60. However, 10%–20% of patients have an early onset of PD (EOPD).
Objectives: To compare disability levels according to the World Health Organization Disability Assessment Schedule 2.0 (WHODAS-2) between people with EOPD and those with late-onset PD (LOPD).
Methods: We conducted a cross-sectional study with 95 EOPD patients (mean-age 44.51 ± 4.63, H&Y 1.93 ± 0.93) and 255 LOPD patients (mean-age 63.01 ± 7.99, H&Y 2.02 ± 0.95). Demographic information, clinical characteristics, cognitive evaluation by Telephone-Montreal-Cognitive-Assessment (T-MoCA), functionality self-evaluation by WHODAS-2 and the Unified-Parkinson’s-Disease-Rating-Scale (MDS-UPDRS), parts I and II, were documented for each patient by an individual remote interview.
Results: Analysis showed a statistically significant difference between EOPD and LOPD in two domains of WHODAS-2 only: cognition (Z-adjusted = 2.60; p-value adjusted <0.009) and activities of daily living related to work/school (Z-adjusted = 2.34; p-value adjusted <0.01). T-MoCA scores confirmed more impaired cognition capacity in LOPD (Z-adjusted = 2.42; p-value adjusted <0.01). The two groups had no significant differences in levodopa daily dosage, Hoehn and Yahr (H&Y) stages, disease time duration, and MDS-UPDRS I and II scores.
Conclusion: People living with EOPD face similar disability levels as those with LOPD, except for cognition, where LOPD patients exhibited higher levels of disability than EOPD and for work activities where the EOPD exhibited higher levels of disability than LODP. These results highlight the challenges faced by people with EOPD in interacting with society and living with the disease for a longer time. The WHODAS-2 can be a useful tool to assess disability and tailor interventions for people with PD of different age groups.
1. Introduction
Parkinson’s disease (PD) is the second most common neurodegenerative disorder after Alzheimer’s dementia (1). The disease onset is typically around 65 to 70 years of age (2), and the higher prevalence (2%) is found in people over the age of 70, defined as Late Onset of PD (LOPD) (3). However, Early Onset of PD (EOPD), defined as PD with age at onset after 21 years but before 50 years (4), also be observed, with an incidence between 0.29 and 3.3 per 100,000 persons-years (5, 6).
Given the effect of PD symptoms earlier in life, the interaction of symptoms with potentially more active roles in society, and the longer time-life living with the disease, people with EOPD face more challenges than those with LOPD. Rigidity, and dystonia have been found as more frequently presenting symptoms in EOPD (7, 8). In addition, the severity of the postural instability after a longer disease duration is higher in people with EOPD than in LOPD (9). Interestingly, regarding non-motor symptoms, the rate of depression was reported higher in patients with EOPD than in patients with LOPD (10), as well as worse emotional well-being and poorer quality of life, independent of depression status (11).
Besides the motor and non-motor aspects, people with EOPD face different social challenges than LOPD. Unemployed men with EOPD are twice more than what observed in the general population (12), and early retirement is also higher for people with EOPD (13). Finally, EOPD may present a challenge to relationships. Couples with EOPD reported higher marital discord scores than those with LOPD (14). Sexual dysfunction has been reported as more prevalent in EOPD than in the general population (15).
The interaction among the physical, mental, and social aspects may be behind the higher prevalence of suicidal ideas in people with EOPD than in LOPD (16). Despite these specific challenges, there is no standardized pharmacological and non-pharmacological therapeutic approach for EOPD. Better awareness about the EOPD disability will undoubtedly improve the management and care of these patients (17).
When it comes to controlling the severity of PD, objective measures based on motor tests have proven to be quite effective. However, it is crucial to understand that the impact of the disease cannot always be directly linked to motor impairments alone, even though there is a clear relationship (18). There seems to be a notable gap between how healthcare providers and patients view the health condition linked to Parkinson’s disease, according to a recent report by movement disorder specialists from around the world (19). The current preconized care model centered on the patient (20) emphasizes the significance of self-perception in assessing disability levels as the primary indicator of health conditions. This approach recognizes the significance of the patient’s own experience and perspective as the primary indicator of their health condition.
The World Health Organization Disability Assessment Schedule 2.0 (WHODAS-2) was developed to assess disability based on the International Classification of Functioning, Disability, and Health (ICF) (21). According to ICF, disability is described as “a difficulty in functioning at the body, person, or societal levels, in one or more life domains, as experienced by an individual with a health condition in interaction with contextual factors” (22). Although other tools have traditionally been used to measure disability, such as the Indexes of activities of daily living (ADL) and quality of life, none of them has been developed based on the ICF biopsychosocial conceptual model (21).
A seminal study to assess the WHODAS-2 conceptual model and metric properties in a set of chronic and prevalent clinical conditions accounting for a broad scope of disability included people living with early, intermediate, and advanced PD stages among the 1,119 participants recruited in 7 European centers. The results showed very high reliability, good ability to discriminate among known groups, and adequate capacity to detect change over time, confirming that WHODAS-2 is adequate to evaluate disability in patients with chronic conditions, which may help to eliminate barriers to developing policies, giving excellent evidence of these populations’ need (21).
The results from a cross-sectional analytical study examining the metric properties WHODAS-2 short version, which included 168 PD patients with 69.6 mean age, demonstrated their suitable metric properties (23).
Regarding the complex interaction among the motor, mental and social aspects associated with disability level in people living with EOPD and being WHODAS-2, a common, international, and interdisciplinary instrument based on the biopsychosocial model, the present study aimed to investigate the disability level in people living with EOPD in comparison with people living with LOPD.
2. Materials and methods
2.1. Study design and participants
A cross-sectional study of 350 people with idiopathic PD was recruited for this study. The people were divided into the EOPD group (age of onset between 21 and 50 years, n = 95, mean age 44.51 ± 4.63, mean H&Y stage 1.93 ± 0.93) and LOPD group (age of onset >50 years, n = 255, mean age 63.01 ± 7.99, mean H&Y stage 2.02 ± 0.95; Figure 1). The eligibility criteria were (a) a diagnosis of idiopathic PD according to the diagnostic criteria of the UK Parkinson’s Disease Society Brain Bank (24), confirmed by a neurologist, and (b) ≥ 21 years old (4), and (c) being treated for PD in the 6 months preceding the commencement of the study and (d) have access to telephone or internet and agree to participate in the study. The non-eligibility criteria were (a) the presence of neurological disorders other than PD and (b) the presence of dementia, speech, and hearing disorders since interviews were conducted by phone calls or phone messages.
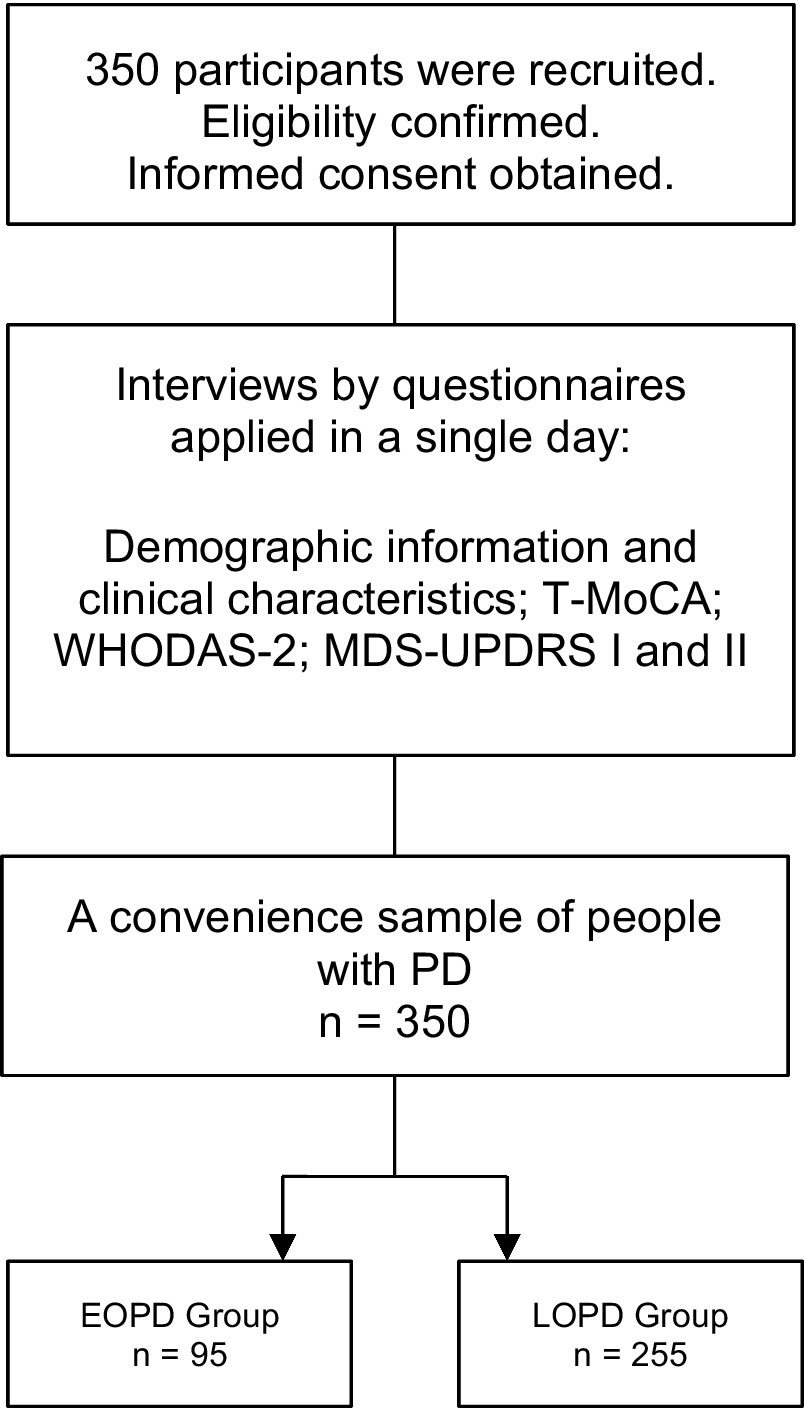
Figure 1. The schematic study designs. T-MoCA, Telephone-Montreal Cognitive Assessment; WHODAS-2, World Health Organization Disability Assessment Schedule 2; MDS-UPDRS, Movement Disorder Society—Unified Parkinson’s Disease Rating Scale; EOPD, Early-onset Parkinson’s disease; LOPD, Late-onset Parkinson’s disease.
To assess the cognitive status, we considered the ability of the participants to properly answer the first section of the study questionnaire about personal and socioeconomic information as clinical evidence of the minimal cognitive capacity to self-evaluate their health condition.
2.2. Recruitment
Participants were recruited by a non-probability sampling method from health units that offer care for PD. At first, through calls and/or telephone messages, we identified their eligibility. Subsequently, information about the study procedures was passed on, and they were invited to consent to participate.
This study was approved by the proper Ethics Committee and conducted in accordance with the Helsinki Declaration.
2.3. Study procedures
The participants were requested to specify their preferred day and time for the remote interview, considering the on-period of dopaminergic medication (40–120 min post the last intake). Additionally, the participants could decide whether to have family assistance during the interview. Then, the researchers applied the questionnaire in a single day, which included: 1—general information (i.e., age, sex/gender, race), 2—socioeconomic status, 3—information associated with PD, 4—information dosage of medication (25), 5—self-evaluation on functionality by World Health Organization Disability Assessment Schedule—WHODAS-2 (23), 6—self-evaluation on “non-motor aspects of daily life experiences” by MDS-UPDRS (Part I): (26), 7—self-evaluation on “motor experiences daily living” by—MDS-UPDRS (Part II) (26) and 8—evaluation of the global cognitive capacity by T-MoCA (27).
2.4. Instruments
2.4.1. WHODAS-2 (World Health Organization Disability Assessment Schedule 2.0)
It is a practical, generic assessment instrument that can measure health and disability at the population level or clinical practice based on the difficulties presented in the last 30 days. There are several different versions of World Health Organization Disability Assessment Schedule 2.0 (WHODAS-2), which differ in length and intended mode of administration. This study used the full version of 36 items through an interview.
WHODAS-2 captures the level of functioning in six domains of life (3): Domain 1: Cognition—understanding and communicating; Domain 2: Mobility—moving and getting around; Domain 3: Self-care—attending to one’s hygiene, dressing, eating, and staying alone; Domain 4: Getting along—interacting with other people; Domain 5: Life activities—domestic responsibilities, leisure, work, and school; Domain 6: Participation—joining in community activities, participating in society.
For all six domains, WHODAS-2 provides a profile and a summary measure of functioning and disability that is reliable and applicable across cultures in all adult populations. Each question is scored between 1 and 5. The higher the score, the worse the functionality of people.
2.4.2. T-MoCA (Telephone - Montreal Cognitive Assessment)
The Telephone - Montreal Cognitive Assessment (T-MoCA) is an adapted version of the MoCA 30 administered over the telephone with changes in the score. We used the MoCA items that did not require the use of a pencil and paper, or a visual stimulus were used for the T-MoCA, which has a maximum score of 22.
2.4.3. MDS-UPDRS (Movement Disorder Society—Unified Parkinson’s Disease Rating Scale)
It is a tool to measure the severity and progression of Parkinson’s disease based on the difficulties presented in the last 7 days. It consists of four parts: Part I (non-motor experiences of daily living), Part II (motor experiences of daily living), Part III (motor examination), and Part IV (motor complications). In this study, only parts I and II were used. Part I consists of 13 questions that assess the non-motor impact of PD on patients’ daily living experiences. Part II contains 20 questions that assess motor impact. Each question is scored between 0 and 4. The higher the score, the worse the severity and progression of PD.
2.5. Statistical analysis
Descriptive statistical analysis was used for the demographic and clinical data of the participants. Considering the normal age distribution, test T was used to compare the two groups (EOPD and LOPD).
Variables that did not exhibit a normal distribution, including WHODAS, MDS-UPDRS I and II, and T-MoCA, were analyzed using appropriate non-parametric tests.
To compare the stage, Kruskal-Wallis ANOVA (KW-ANOVA) was utilized with the H&Y stage (1, 2, and 3) considered as a factor. When statistically significant differences were observed, multiple comparisons of the average ranks for each pair of groups were applied by the Nemenyi post hoc test. To correct the multiple comparisons, the Bonferroni test was applied.
For onset comparison, the Mann–Whitney U-Test with continuing correction was utilized to compare the two groups (EOPD and LOPD). Normal z-values and value of p were adjusted for each comparison as a correction for the number of comparisons.
Finally, the Spearman Rank Order Correlation was used to test the correlation between MDS-UPDRS I-II and WHODAS-2 scores and between T-MoCA and WHODAS-2 domain cognitive scores.
Differences were considered statistically significant when the value of p was below 0.05. The statistical analyses were performed using Statistica Version 13 (TIBCO Software Inc. United States).
3. Results
The demographic and clinical participants’ features are demonstrated in Table 1. As expected, most of them are males, with a significant statistical difference in age between the groups. There were no statistically significant differences in levodopa daily dosage, H&Y stages, disease time duration, and MDS-UPDRS I and II scores.
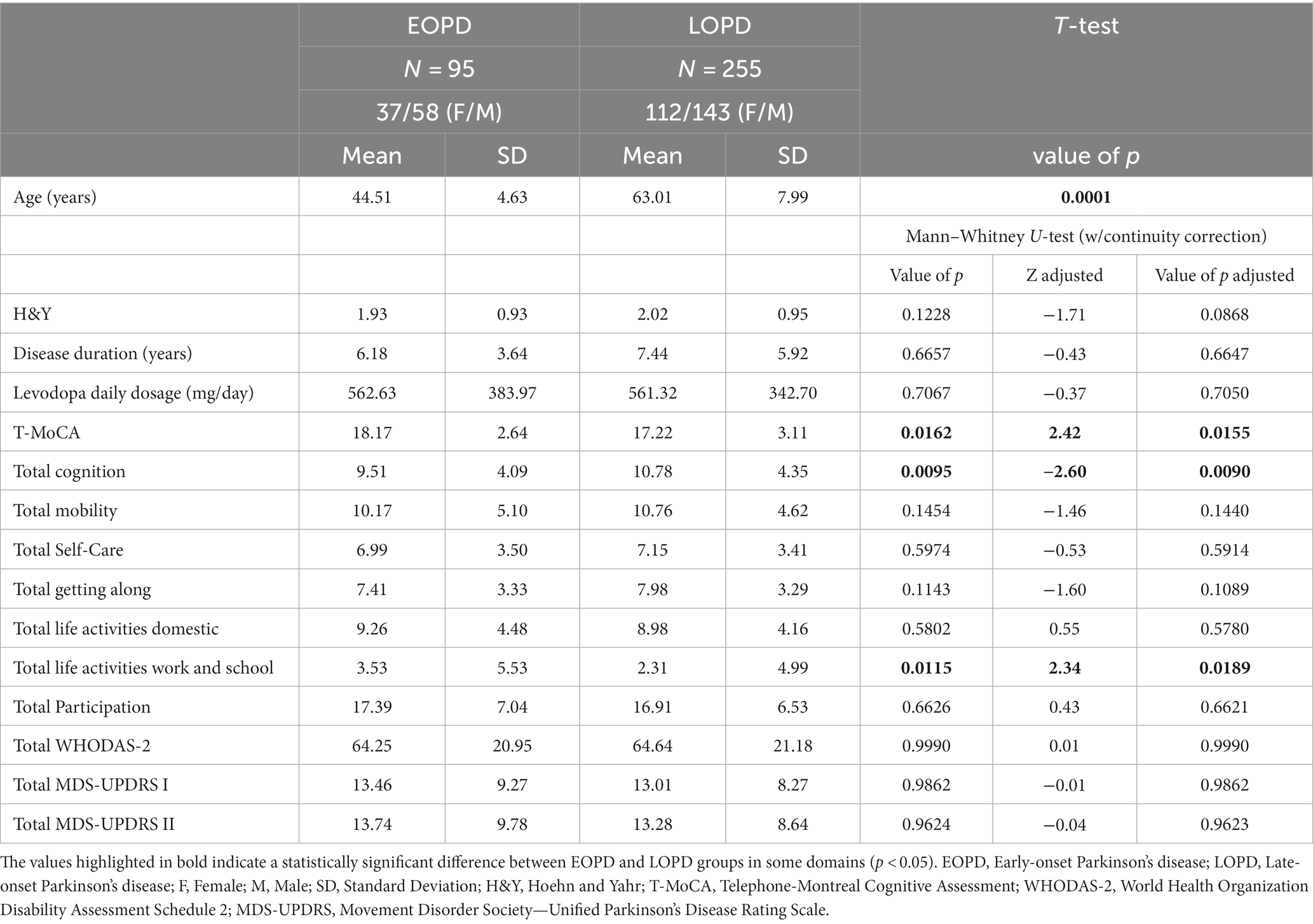
Table 1. Demographic and clinical characteristics of people with idiopathic PD.
Regarding the disease evolution, there was a significant H&Y stage effect for WHODAS-2, MDS-UPDRS I, and II total scores, as indicated in Table 2. The post-hoc test confirmed a significant difference between H&Y 3 and H&Y 1 and H&Y 2 for WHODAS-2, MDS-UPDRS I and II total scores, as also presented in Table 2. Additionally, there was a positive significant correlation between MDS-UPDRS I and II and WHODAS-2 scores (R = 0.61, value of p < 0.00001 and R = 0.65, value of p ≤ 0.00001, respectively).
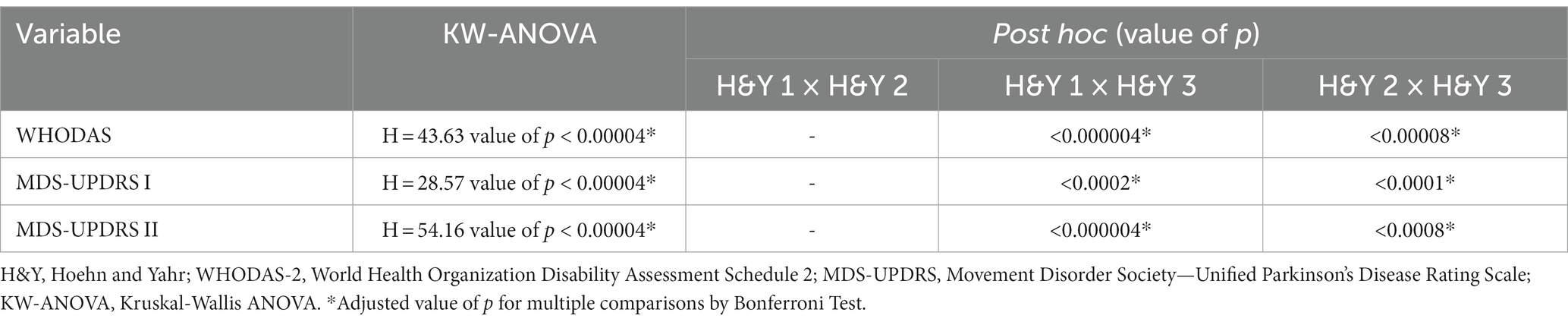
Table 2. Stages comparison.
Regarding the disease onset, there was a statistically significant difference between EOPD and LOPD groups in two domains of WHODAS-2 only: cognition (Table 1; Figure 2) and ADL associated with work/school (Table 1). Furthermore, the analysis of T-MoCA scores reinforced those participants from LOPD showed statistically significantly lower scores than participants from EOPD, which reflects a worse cognitive global performance (Table 1; Figure 3). Lastly, WHODAS-2 domain cognitive and T-MoCA scores were inversely and significantly correlated (R = −0.304, value of p < 0.0000001).
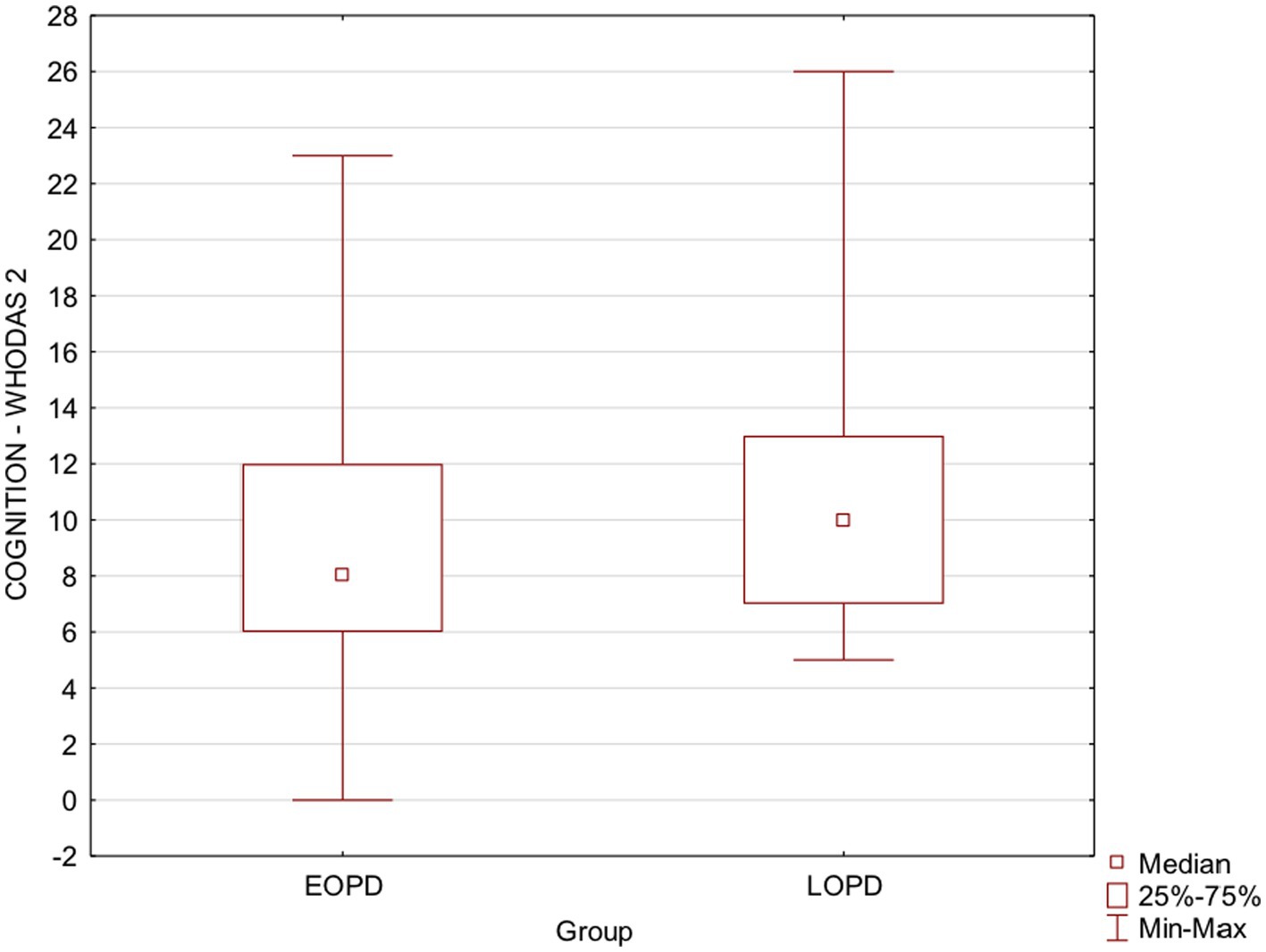
Figure 2. Box plots show EOPD and LOPD group Cognition-WHODAS 2 scores. Squares represent means, lines represent medians, and boxes show the interquartile range. Maximum and minimum scores are indicated by the upper and lower markers, respectively. EOPD, Early-onset Parkinson’s disease; LOPD, Late-onset Parkinson’s disease; WHODAS-2, World Health Organization Disability Assessment Schedule 2.
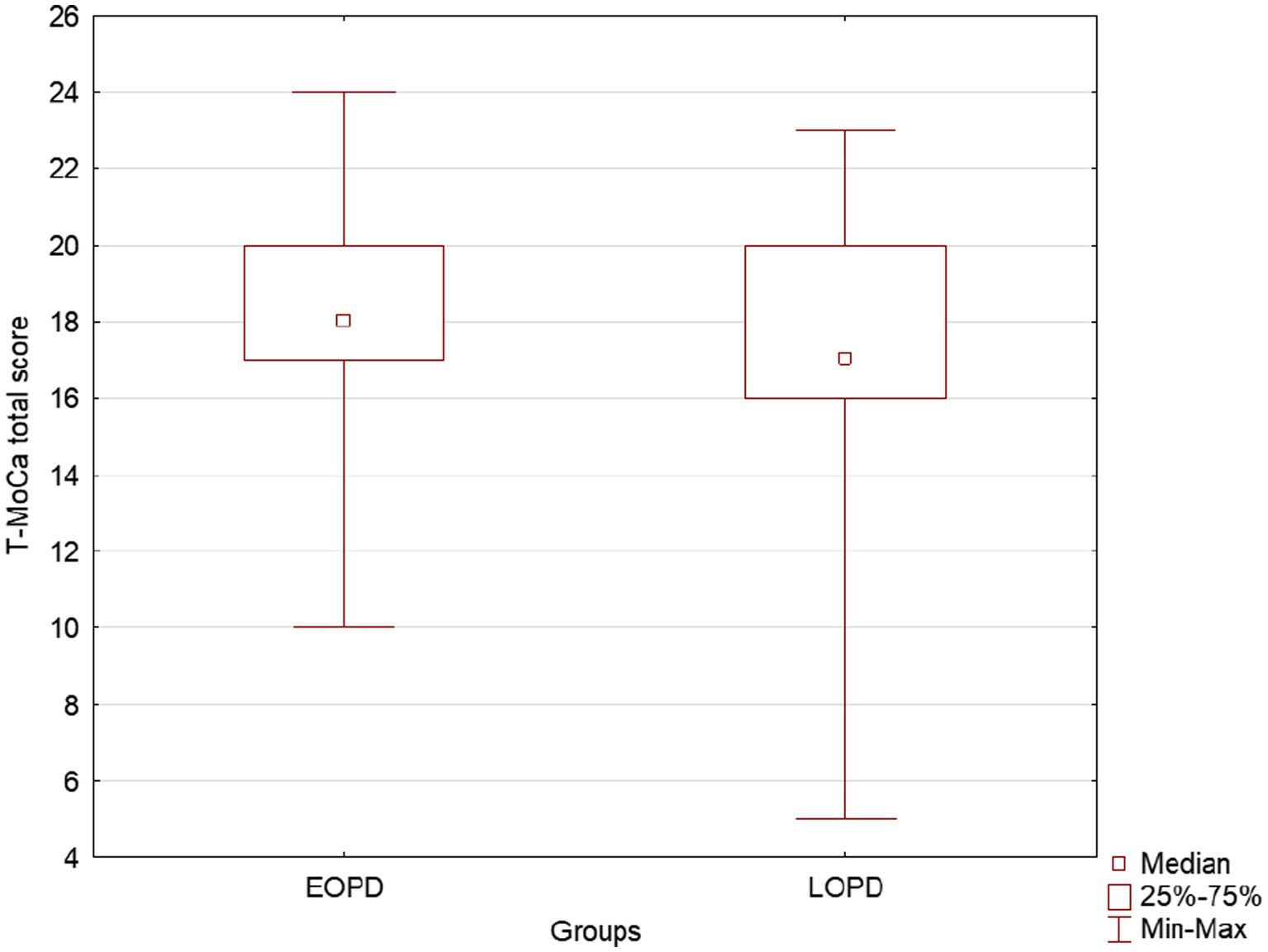
Figure 3. Box plots show EOPD and LOPD group T-MoCA total scores. Squares represent means, lines represent medians, and boxes show the interquartile range. Maximum and minimum scores are indicated by the upper and lower markers, respectively. EOPD, Early-onset Parkinson’s disease; LOPD, Late-onset Parkinson’s disease; T-MoCA, Telephone-Montreal Cognitive Assessment.
In contrast, for ADL associated with work, the participants from EOPD group reported higher disability levels than LOPD. Additional analysis showed that 5% of participants from the LOPD group reported being “unemployed” against 11% from the EOPD group, 36% to be “employed” against 41% from the EOPD group, and 50% were “retired” against 28% from the EOPD group.
4. Discussion
Overcoming a neurodegenerative, progressive, and incurable disease such as PD is a complex challenge in any life cycle. Supposedly, managing the motor and non-motor symptoms and their social consequences is harder for younger people in the more active phase of life. In fact, the results from the current study showed a worse disability level and higher unemployment rate in people living with EOPD. However, the self-perception of disability levels related to mobility, self-care, getting along, life activities, and participation were similar for people living with EOPD and LOPD. In contrast, self-perception cognitive disability level was higher for people with LOPD than EOPD.
Several considerations can be made based on our results.
First, the WHODAS-2 was able to detect differences between clinical-severity groups: participants classified as intermediate disease stage (H&Y 3) reported worse disability scores than those with early disease stages (H&Y 1 and 2). Additionally, the disability levels according to WHODAS-2 were correlated with motor and non-motor aspects of daily living experiences according to MDS-UPDRS, considered golden standing for PD evaluation (26). The WHODAS-2, designed to cover disability, measures the restrictions on daily life activities and social participation (21), whereas MDS-MDS-UPDRS I and II address the impact of non-motor and motor symptoms on daily life activities (26). The moderate magnitude of the associations among the two instruments reflects how the WHODAS-2 and the MDS-UPDRS I and II measure different aspects of related concepts. Thus, WHODAS-2 may be used to complement the information obtained by MDS-UPDRS, offering a more comprehensive evaluation of the biopsychosocial impact of disease on patient functionality.
Second, despite some previous studies showing the slower disease evolution for early onset (28), our results showed a similar disability level according to WHODAS-2 and motor and non-motor aspects of daily living experiences according to MDS-UPDRS for both groups that reported the same disease duration. These findings show that people with early and late-onset PD experience similar disability levels in daily living after living with the disease for the same amount of time. The MDS-UPDRS Section II has been found to be a reliable tool for measuring disease progression, particularly in the early stages of the disease (29) and has stronger and more stable association with disease duration than other MDS-UPDRS sections (30). Sections I and II of the MDS-UPDRS also have established clinically important differences that can be used to judge the effectiveness of interventions (31). Therefore, self-reported experiences related to daily living can be considered a reliable tool to measure the severity and progression of PD. Based on this finding, it is plausible to suppose that the participants from EOPD could potentially experience higher disability levels when at the same age as LOPD participants. Further longitudinal studies are needed to investigate this issue. However, this reasonable supposition should be alert for specialized care improvement for people with EOPD.
Third, differences were found between the two groups for two WHODAS-2 domains: cognition and work/school activity. The disability level related to cognition was higher for LOPD participants. The decline in global cognitive capacity due to the aging process is well-known (32). The interaction between neurodegeneration associated with PD and aging processes may explain why younger people living for a similar time with PD have a smaller cognitive disability. Results from T-MoCA confirm the more preserved cognitive global capacity for EOPD participants than LOPD. However, T-MoCA was not able to show the difference between the disease stages regardless of the onset. In contrast, WHODAS-2 domain cognitive showed significantly higher disability levels for participants in the intermediate PD stage (H&Y 3) in comparison to initial PD stages (H&Y 1 and 2). This finding suggests that even before objective tests can detect cognitive decline, they can impact cognitive functionality. Then, cognitive intervention should be considered priority care for people with LOPD and be started even before the detectable objective impairments.
Finally, the higher disability levels in work activities for EOPD than LOPD was unsurprising. A previous study comparing people with EOPD with LOPD showed that, among those who retired, 97% of the patients with EOPD retired early vs. 73% of those with LOPD (14). Other studies have found that 54% of people with EOPD retire early, and 94% are likely to give up work within 10 years of disease onset (13). In the present study, 28% of participants reported being retired, even having less than 60 years of age. Another previous study showed that men aged 55 to 64 living with PD were twice as likely to be unemployed than the general population (12). In the present study, the percentage of unemployed was twice larger for EOPD than for LOPD participants (11 and 5%, respectively). Finally, 20% of people with EOPD reported being away from their jobs for health reasons. Further studies are needed to investigate the long-term socioeconomic impact of this population’s high unemployment level and early retirement. Thus, besides offering proper care to minimize the effects of motor and non-motor symptoms on work activities performance, it is crucial to improve the social support for this population as well as to promote a social policy to decrease the social stigma.
Our study has some limitations. The absence of a motor evaluation of the motor symptoms severely may be considered a limitation of the present study; therefore, we cannot necessarily explore and correlate motor function and self-perception of disability level in the two groups. However, the importance of our findings is still maintained since the self-perception of disability level is a relevant measure that can provide valuable insight into the personal experiences of those living with PD (30, 31). In addition, our study is based on a relatively small number of patients; therefore, a larger sample size is needed to confirm our findings. Also, socioeconomic, and social status may have a major role in our results; however, we do not have detailed data to potentially explore this additional important variable. Lastly, a potential recall bias can be evoked when the participants have been interviewed via phone, but it should be equally distributed among EOPD and LOPD; unfortunately, patients with cognitive decline may have more difficulties in the phone interview and we should be aware about this possible limitation as well.
Finally, the participants in the study were selected from diverse geographical areas, varying educational levels, socio-economic backgrounds, and different ages, genders, and disability levels. This confirms that our convenient non-probability sampling method was unbiased and representative. However, exclusion criteria based on the presence of dementia and/or speech problems prevented patients in advanced disease stages from being included in the study. As a result, the sample mostly comprised patients in mild to moderate stages (mostly H&Y 2), which may limit the generalizability of the findings to patients in more advanced stages of the disease. The study’s primary inclusion criteria were based on a diagnosis of idiopathic PD by a neurologist who may not be specialized in movement disorders. This may also be considered as a study limitation.
Further studies are needed to investigate the association between disability level according to WHODAS-2 and PD motor symptoms severity.
5. Conclusion
In our study, we observed similar global disability levels between people living with EOPD and LOPD, according to WHODAS-2, except in the cognition domain that was more impaired in people living with LOPD than EOPD, and in activities related to work that was more impaired in people living EOPD than LOPD, findings that can be partially explained by the productive cycle of life.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Ethics Committee of the General Hospital of the Faculty of Medicine of the University of São Paulo (#CAAE 19504619.5.0000.0065). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
IN: Conceptualization, Formal analysis, Investigation, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing. KN: Investigation, Project administration, Supervision, Writing – original draft. BS: Investigation, Project administration, Writing – original draft. IB: Investigation, Writing – original draft. GC: Investigation, Writing – original draft. VP: Investigation, Writing – original draft. CP: Investigation, Writing – original draft. AP: Investigation, Writing – original draft. NP: Investigation, Writing – original draft. AH: Writing – original draft, Writing – review & editing. AR: Writing – original draft, Writing – review & editing. RS: Writing – original draft, Writing – review & editing. MP: Conceptualization, Formal analysis, Investigation, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior—Brasil (CAPES)—Finance Code 001. This article was produced as part of the activities of FAPESP Research, Innovation, and Dissemination Center for Neuromathematics (grant #2013/07699-0, S. Paulo Research Foundation). AR was partially funded by Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) grant # 303359/2022-6.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Erkkinen, MG, Kim, MO, and Geschwind, MD. Clinical neurology and epidemiology of the major neurodegenerative diseases. Cold Spring Harb Perspect Biol. (2018) 10:a033118. doi: 10.1101/cshperspect.a033118
2. Ascherio, A, and Schwarzschild, MA. The epidemiology of Parkinson's disease: risk factors and prevention. Lancet Neurol. (2016) 15:1257–72. doi: 10.1016/S1474-4422(16)30230-7
3. Schrag, A, Ben-Shlomo, Y, and Quinn, NP. Cross sectional prevalence survey of idiopathic Parkinson's disease and parkinsonism in London. BMJ. (2000) 321:21–2. doi: 10.1136/bmj.321.7252.21
4. Mehanna, R, Smilowska, K, Fleisher, J, Post, B, Hatano, T, Pimentel Piemonte, ME, et al. International Parkinson and Movement Disorder Society task force on early onset Parkinson's disease. Age cutoff for early-onset Parkinson's disease: recommendations from the International Parkinson and Movement Disorder Society task force on early onset Parkinson's disease. Mov Disord Clin Pract. (2022) 9:869–78. doi: 10.1002/mdc3.13523
5. Ylikotila, P, Tiirikka, T, Moilanen, JS, Kääriäinen, H, Marttila, R, and Majamaa, K. Epidemiology of early-onset Parkinson's disease in Finland. Parkinsonism Relat Disord. (2015) 21:938–42. doi: 10.1016/j.parkreldis.2015.06.003
6. Camerucci, E, Stang, CD, Hajeb, M, Turcano, P, Mullan, AF, Martin, P, et al. Early-onset parkinsonism and early-onset Parkinson's disease: a population-based study (2010-2015). J Parkinsons Dis. (2021) 11:1197–207. doi: 10.3233/JPD-202464
7. Pagano, G, Ferrara, N, Brooks, DJ, and Pavese, N. Age at onset and Parkinson disease phenotype. Neurology. (2016) 86:1400–7. doi: 10.1212/WNL.0000000000002461
8. Wickremaratchi, MM, Knipe, MD, Sastry, BS, Morgan, E, Jones, A, Salmon, R, et al. The motor phenotype of Parkinson's disease in relation to age at onset. Mov Disord. (2011) 26:457–63. doi: 10.1002/mds.23469
9. Becker, D, Maric, A, Schreiner, SJ, Büchele, F, Baumann, CR, and Waldvogel, D. Onset of postural instability in Parkinson's disease depends on age rather than disease duration. Parkinsons Dis. (2022) 2022:6233835. doi: 10.1155/2022/6233835
10. Mehanna, R, Moore, S, Hou, JG, Sarwar, AI, and Lai, EC. Comparing clinical features of young onset, middle onset and late onset Parkinson's disease. Parkinsonism Relat Disord. (2014) 20:530–4. doi: 10.1016/j.parkreldis.2014.02.013
11. Knipe, MD, Wickremaratchi, MM, Wyatt-Haines, E, Morris, HR, and Ben-Shlomo, Y. Quality of life in young- compared with late-onset Parkinson's disease. Mov Disord. (2011) 26:2011–8. doi: 10.1002/mds.23763
12. Murphy, R, Tubridy, N, Kevelighan, H, and O'Riordan, S. Parkinson's disease: how is employment affected? Ir J Med Sci. (2013) 182:415–9. doi: 10.1007/s11845-013-0902-5
13. Schrag, A, and Banks, P. Time of loss of employment in Parkinson's disease. Mov Disord. (2006) 21:1839–43. doi: 10.1002/mds.21030
14. Schrag, A, Hovris, A, Morley, D, Quinn, N, and Jahanshahi, M. Young- versus older-onset Parkinson's disease: impact of disease and psychosocial consequences. Mov Disord. (2003) 18:1250–6. doi: 10.1002/mds.10527
15. Vela-Desojo, L, Urso, D, Kurtis-Urra, M, García-Ruiz, PJ, Pérez-Fernández, E, Lopez-Valdes, E, et al. Sexual dysfunction in early-onset Parkinson's disease: a cross-sectional, Multicenter Study. J Parkinsons Dis. (2020) 10:1621–9. doi: 10.3233/JPD-202066
16. Ou, R, Wei, Q, Hou, Y, Zhang, L, Liu, K, Kong, X, et al. Suicidal ideation in early-onset Parkinson's disease. J Neurol. (2021) 268:1876–84. doi: 10.1007/s00415-020-10333-4
17. Riboldi, GM, Frattini, E, Monfrini, E, Frucht, SJ, and Di Fonzo, A. A practical approach to early-onset parkinsonism. J Parkinsons Dis. (2022) 12:1–26. doi: 10.3233/JPD-212815
18. Cools, CI, de Vries, NM, and Bloem, BR. Happiness: a novel outcome in Parkinson studies? J Parkinsons Dis. (2020) 10:1261–6. doi: 10.3233/JPD-201999
19. Bhidayasiri, R, Panyakaew, P, Trenkwalder, C, Jeon, B, Hattori, N, Jagota, P, et al. Delivering patient-centered care in Parkinson's disease: challenges and consensus from an international panel. Parkinsonism Relat Disord. (2020) 72:82–7. doi: 10.1016/j.parkreldis.2020.02.013
20. van der Eijk, M, Nijhuis, FA, Faber, MJ, and Bloem, BR. Moving from physician-centered care towards patient-centered care for Parkinson's disease patients. Parkinsonism Relat Disord. (2013) 19:923–7. doi: 10.1016/j.parkreldis.2013.04.022
21. Garin, O, Ayuso-Mateos, JL, Almansa, J, Nieto, M, Chatterji, S, Vilagut, G, et al. MHADIE consortium. Validation of the "World Health Organization disability assessment schedule, WHODAS-2" in patients with chronic diseases. Health Qual Life Outcomes. (2010) 8:51. doi: 10.1186/1477-7525-8-51
22. World Health Organization (WHO). International classification of functioning, disability and health: ICF. Geneva: WHO Library Cataloguing-in-Publication Data (2000).
23. Serrano-Dueñas, M, Serrano, M, Mafla, D, and Martínez-Martín, P. Evaluation of the metric properties of the WHODAS 2.0, WHODAS-S, and RADS in the assessment of disability in parkinsonian patients. Clin Neurol Neurosurg. (2020) 194:105872. doi: 10.1016/j.clineuro.2020.105872
24. Hoehn, MM, and Yahr, MD. Parkinsonism: onset, progression and mortality. Neurology. (1967) 17:427–42. doi: 10.1212/wnl.17.5.427
25. Tomlinson, CL, Stowe, R, Patel, S, Rick, C, Gray, R, and Clarke, CE. Systematic review of levodopa dose equivalency reporting in Parkinson's disease. Mov Disord. (2010) 25:2649–53. doi: 10.1002/mds.23429
26. Goetz, CG, Tilley, BC, Shaftman, SR, Stebbins, GT, Fahn, S, Martinez-Martin, P, et al. Movement Disorder Society UPDRS revision task force. Movement Disorder Society-sponsored revision of the unified Parkinson's disease rating scale (MDS-UPDRS): scale presentation and clinimetric testing results. Mov Disord. (2008) 23:2129–70. doi: 10.1002/mds.22340
27. Katz, MJ, Wang, C, Nester, CO, Derby, CA, Zimmerman, ME, Lipton, RB, et al. T-MoCA: a valid phone screen for cognitive impairment in diverse community samples. Alzheimers Dement. (2021) 13:e12144. doi: 10.1002/dad2.12144
28. Mehanna, R, and Jankovic, J. Young-onset Parkinson's disease: its unique features and their impact on quality of life. Parkinsonism Relat Disord. (2019) 65:39–48. doi: 10.1016/j.parkreldis.2019.06.001
29. Parashos, SA, Elm, J, Boyd, JT, Chou, KL, Dai, L, Mari, Z, et al. Validation of an ambulatory capacity measure in Parkinson disease: a construct derived from the unified Parkinson's disease rating scale. J Parkinsons Dis. (2015) 5:67–73. doi: 10.3233/JPD-140405
30. Harrison, MB, Wylie, SA, Frysinger, RC, Patrie, JT, Huss, DS, Currie, LJ, et al. UPDRS activity of daily living score as a marker of Parkinson's disease progression. Mov Disord. (2009) 24:224–30. doi: 10.1002/mds.22335
31. Horváth, K, Aschermann, Z, Kovács, M, Makkos, A, Harmat, M, Janszky, J, et al. Minimal clinically important differences for the experiences of daily living parts of movement disorder society-sponsored unified Parkinson's disease rating scale. Mov Disord. (2017) 32:789–93. doi: 10.1002/mds.26960
Keywords: Parkinson’s disease, early onset, disability, cognition, WHODAS-2
Citation: Nascimento IAPdS, Nobrega KCC, Souza BRA, Barone IC, Checchio G, Ponciano VP, de Paula CGC, Possani AN, Penha NC, Helene AF, Roque AC, Savica R and Piemonte MEP (2023) Comparison of disability level between Early and Late Onset Parkinson’s Disease using WHODAS 2. Front. Neurol. 14:1281537. doi: 10.3389/fneur.2023.1281537
Edited by:
Wolfgang H. Jost, Parkinson-Klinik Ortenau GmbH & Co KG, GermanyReviewed by:
Mayela Rodríguez-Violante, Manuel Velasco Suárez National Institute of Neurology and Neurosurgery, MexicoAdeel Ali Memon, West Virginia University, United States
Copyright © 2023 Nascimento, Nobrega, Souza, Barone, Checchio, Ponciano, de Paula, Possani, Penha, Helene, Roque, Savica and Piemonte. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Maria Elisa Pimentel Piemonte, ZWxpc2FwcEB1c3AuYnI=
†These authors have contributed equally to this work and share first authorship