
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
STUDY PROTOCOL article
Front. Neurol. , 02 November 2023
Sec. Experimental Therapeutics
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1255999
 Xiao-Yu Wang1,2†
Xiao-Yu Wang1,2† Wei Liu1,2†
Wei Liu1,2† Huan Li1,2
Huan Li1,2 Meng-Ying Rong1,2
Meng-Ying Rong1,2 Jing-Yu Li1,2
Jing-Yu Li1,2 Shao-Kang Wang1,2
Shao-Kang Wang1,2 Yu-Zheng Du1,2
Yu-Zheng Du1,2 Qi Zhao1,2*
Qi Zhao1,2*Introduction: The treatment and rehabilitation of stroke and its complications have become major global health issues. Acupuncture is widely used as a complementary and alternative treatment for stroke. Many clinical studies have evaluated the efficacy and safety of acupuncture, but the research results need to be more consistent. The quality of research based on previously published meta-analyzes is uneven, leading to unstable conclusions. This study aims to provide a comprehensive and systematic analysis of the efficacy of high-quality, randomized controlled trials (RCTs) based on blinded designs for treating stroke and its complications. It also aims to review the characteristics of blinded designs and the current use of sham/placebo acupuncture controls in treating stroke.
Methods and analysis: This study will be conducted under the reporting guidelines for systematic reviews and meta-analyzes. Randomized controlled trials using acupuncture as the primary measure for stroke will be searched in databases such as China National Knowledge Infrastructure (CNKI), Chongqing VIP (CQVIP), Wan-fang, PubMed, Embase, Cochrane Library, and Web of Science. To evaluate high-quality research based on a blind design, if the trial evaluates the efficacy of any acupuncture intervention by including a sham/placebo acupuncture control, it will be included. The primary outcome indicator will be the ability to perform daily activities. Secondary outcome indicators include evaluating quality of life and related functions in stroke-related sequelae. We will assess the quality of evidence, reporting quality, and risk of bias for the acupuncture intervention in the literature included in this study using the GRADE system, the STRICTA 2010 checklist, and ROB2.0, respectively. RevMan 5.4 software will be used to conduct the meta-analysis, and Stata 15.0 software will be used for sensitivity analysis and publication bias testing.
Discussion: By analyzing high-quality, well-designed, randomized controlled trials of acupuncture, the results of this study may contribute to a more objective and standardized evaluation of acupuncture efficacy in treating stroke and its complications.
Systematic review registration: PROSPERO, Identifier (CRD42023378930).
Stroke is the second leading cause of death and the primary cause of disability globally (1). Among neurological disorders, stroke ranks first in disability-adjusted life-years (DALY) in 21 Global Burden of Diseases (GBD) regions (2). Primary and secondary prevention, stroke units, acute treatment, and neurorehabilitation positively reduce the stroke incidence rate (1). However, the overall enhanced burden of stroke caused by the increasing prevalence of chronic stroke means that stroke is becoming a major global health problem (2, 3). According to estimates, there will be more than 70 million stroke survivors in 2030 (4). The complication of stroke mainly includes movement, sensory, epilepsy, cognitive, emotional, speech, swallowing, excretion, thromboembolism, fatigue, pain, fever, and cardiopulmonary dysfunctions. A cohort study discovered that stroke survivors often could not complete daily activities due to impairments such as hemiplegia, depression, aphasia, and cognition (5). Hence, the treatment and rehabilitation of stroke and stroke-related disabilities remains a significant problem to be solved in the coming decades.
Acupuncture is one of the oldest and most widespread treatments in traditional Chinese medicine. It has become the primary supplementary and alternative therapy recommended by the World Health Organization (WHO) due to its characteristics of being inexpensive and having less adverse effects (6). There is growing evidence to suggest that acupuncture affects the increment of blood perfusion in injured brain areas, reduction of the inflammatory reaction, stimulation of neuronal cell reorganization, and restoration of neural plasticity (7, 8). Additionally, acupuncture can facilitate the recovery of movements and emotional and cognitive function (9, 10) by widely activating various physiological pathways in the central and peripheral nervous systems (11, 12). This means that acupuncture is available for various stroke treatments and related disabilities.
The current evidence has suggested that acupuncture, a complementary and alternative therapy, has been widely recognized to treat the various clusters of symptoms occurring during stroke rehabilitation (13–16). However, the uneven quality of randomized controlled trials (RCTs) makes it difficult to evaluate acupuncture efficacy (17–19) objectively. Some studies (20–22) provide insufficient evidence to support the beneficial effect of acupuncture for stroke treatment, which might be related to methodological deficiencies in the existing acupuncture studies. Double-blind RCTs are the most rigorous way to test medical hypotheses (23, 24). However, the rigorous double-blind design of acupuncture RCTs is generally difficult to achieve because of the particularity of acupuncture operations. Therefore, most clinical studies of acupuncture adopt a single-blind design. It is essential, thus, to evaluate acupuncture treatment of stroke-related diseases in high-quality RCTs based on a blinded design. Meanwhile, sham acupuncture control, a commonly used control method for evaluating the non-specific efficacy of acupuncture, helps to meet the basic requirements of blind design (25) and promotes more definitive and meaningful conclusions in acupuncture research.
High-quality, well-designed RCTs help improve the normative theoretical support and evidence of acupuncture treatment of stroke and its complications. This study aims to (1) estimate the efficacy of acupuncture treatment based on the blind design for stroke and stroke complications and (2) summarize the characteristics of the blind design of the current acupuncture treatment of stroke and the status quo of the control application of sham/placebo acupuncture.
The protocol of this study has been registered in the Prospective Register of Systematic Reviews (CRD42023378930). The results of this systematic review and meta-analysis will be followed by the Preferred Reporting Items for Systematic Reviews and Meta-Analyzes (PRISMA) reporting guidelines. The study selection is shown in Figure 1.
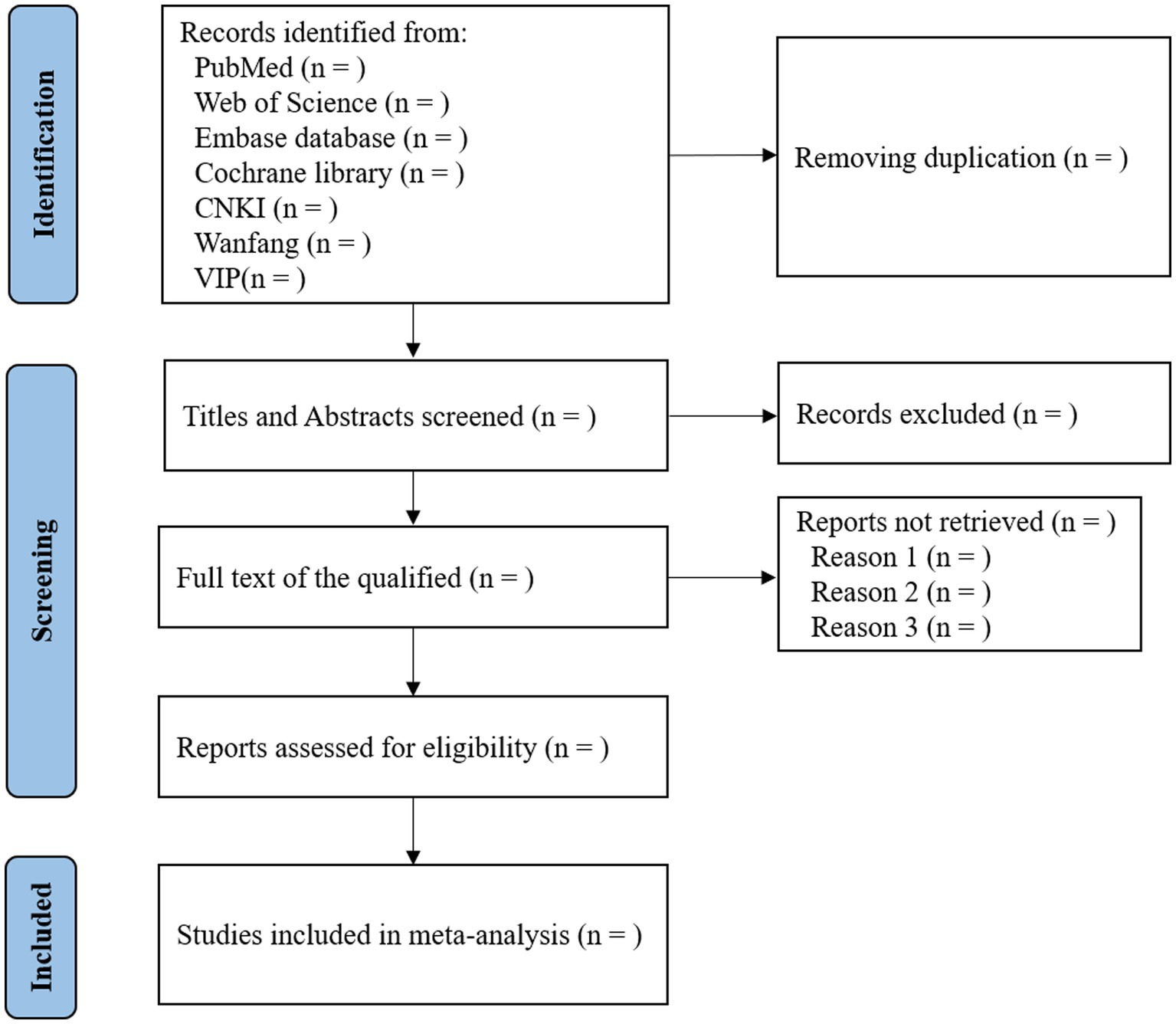
Figure 1. Flow diagram of the studies identified.
A comprehensive search of PubMed, Cochrane Library, Embase, Web of Science, China National Knowledge Infrastructure (CNKI), Chongqing VIP (CQVIP), and WanFang Data from 1 January 2000 to 31 August 2022, will be conducted to identify clinical trials of acupuncture in patients with stroke. Two of the authors (X-YW and WL) will perform the literature search. The association of free words and medical subject headings (MeSH) will be comprised of “stroke,” “cerebral infarction,” or “cerebral hemorrhage,” and MeSH terms “acupuncture” and “sham acupuncture,” or “placebo acupuncture,” or “non-acupoint acupuncture,” and “randomized controlled,” and not “animal.”
We will follow the PICO (population, intervention, comparison, and outcome) model to specify inclusion and exclusion criteria. We will include randomized clinical trials (RCT) in English or Chinese from 1 January 2000 to 31 August 2022.
Trials involving participants of any age, sex, duration, or degree of disease with stroke (infarctional or hemorrhagic) diagnosed with CT/MRI or clinical criteria will be eligible.
Interventions in the experiment group contain traditional acupuncture and electroacupuncture. We will exclude trials in which their intervention in the experiment group involved acupoint catgut embedding therapy, acupoint injection, acupoint application, cupping, moxibustion, and bloodletting therapy.
Trials will be considered eligible if they assess the efficacy of any acupuncture intervention by including a sham/placebo acupuncture control. To ensure that the acupuncture effect can be estimated, trials with the control group receiving co-interventions not provided to the experimental group will be excluded. It will not be excluded when the trial adopts a double-blind and double-simulated design. Specifically, placebo acupuncture refers to acupuncture control methods where the needle does not penetrate the skin and only causes minor irritation to the surface of the skin. Common placebo acupunctures include blunt-headed needles and telescopic needles/devices. Sham acupuncture, a type of penetrating sham acupuncture, refers to a needle superficially placed in a region close to but not a specific therapeutic acupoint. Common sham acupunctures mainly include non-points (i.e., locations that are not known points), minimal stimulation (i.e., needling superficially), or non-meridian points (i.e., points unrelated to this disease).
We will include studies that used at least one of these outcome indicators: The primary outcome indicator is the daily living ability (i.e., the Barthel Index, the Activities of Daily Living, and the modified Barthel index). The secondary outcome indicators are the score of neurological defection (i.e., the National Institute of Health Stroke Scale, the modified Rankin Scale, and the Chinese Stroke Scale), life quality (i.e., the World Health Organization Quality of Life (QQL), the Stroke Specific Quality of Life Scale), and all indicators that can be used to evaluate stroke-related complications (i.e., limb function, dysphagia, depression, and cognitive or sleep disorders), and adverse events. We will include the measures used more than three times cumulatively in the meta-analysis. If the included studies used more than one indicator of the same type, we would select according to the order used in the above examples.
Studies lacking definite diagnoses or without full texts will be excluded. Our study will also exclude studies with issues such as missing data, incomplete data, or incorrect data expression. We will choose the most recent publication date for the article from the same research project.
Note-express 3.7.0 will be used to manage studies. Two assessors (X-YW and WL) will independently screen the titles and abstracts of potential candidate studies for a full-text review. In case of disagreements and discrepancies between the two assessors, a third member of our team (LH) will mediate.
We will extract the following characteristics from each selected study: country, sample size, mean age, percentage of female participants, diagnosis criteria, stroke duration, precise definition and duration of intervention, pseudo-acupuncture control type, doctor qualification, blinding, time points, and content of outcome assessment. If the reported method or data is missing or unclear, the assessors will contact the corresponding author to supplement or clarify the information. Any disagreements and discrepancies will be resolved through discussion by a third reviewer (HL).
This study will use the Grades of Recommendation, Assessment, Development, and Evaluation (GRADE) approach to evaluate the treatment outcomes of acupuncture and the quality of evidence for the leading outcome indicators of included studies. The GRADE approach involves five aspects, namely, limitation, inconsistency, indirectness, imprecision, and publication bias, and the quality of evidence is divided into high, moderate, low, and very low (26). This study will use the Standards for Reporting Interventions in Controlled Trials of Acupuncture (STRICTA) 2010 checklist to assess the detailed acupuncture treatment protocol for the included studies. The STRICTA list consists of six sections, including rationality of acupuncture treatment, details of the acupuncture, treatment protocol, other interventions, therapist background, and control or controlled interventions, divided into six entries and 17 secondary items. Two assessors (X-YW and WL) will independently assess the methodologic and reporting quality for each study using the GRADE approach and the STRICTA list, respectively. A panel with the other authors will solve all discrepancies and disagreements.
The Risk of Bias Tool (ROB2.0) will be used to assess the risk of bias of included RCTs, which consists of five dimensions of bias: randomization process, deviation from intended interventions, missing outcome data, outcome measures, and the selection of the reported results. We also assessed the risk of bias by two assessors (X-YW and WL).
We will use Begg’s and Egger’s tests to assess the publication bias of these trials and form the publication bias plot. When the number of included articles exceeds 10, the funnel plot will be used to analyze whether the study has publication bias.
All statistical analyzes will be performed using Review Manager, version 5.4, and Stata, version 15.0. We will test heterogeneity between outcomes of included studies using the I2 statistic. Statistically significant heterogeneity will be considered as a p-value of <0.10 and with I2 more than 50%. We will assess possible sources of heterogeneity through subgroup analysis. For the effect quantity analysis, odds ratios (ORs) will be expressed for binary outcomes (i.e., adverse effects) with 95% confidence intervals (CIs).
In contrast, for continuous outcomes (i.e., the daily living ability), the mean difference (MD) or the standardized mean difference (SMD) will be used. Given the character of the considerable clinical heterogeneity of acupuncture, we will anticipate potential heterogeneity between included studies. Therefore, the random-effects model will be used to pool effect sizes.
Patients will not be involved in the development of this systematic review protocol. The data for this systematic review will be collected from previously published studies.
This systematic review protocol does not require ethical approval because it does not include the private information/data of the participants. This article will be published in peer-reviewed journals.
To the best of our knowledge, this will be the first meta-analysis exploring the effectiveness of acupuncture treatment for stroke complications based on single-blind RCTs. The number of meta-analyzes on acupuncture for stroke complications is increasing, including post-stroke motor dysfunction (27, 28), cognitive impairment (29, 30), dysphagia (31), depression (32), and insomnia (33). Nevertheless, the results of existing meta-analyzes could have been made more stable and consistent, overcoming issues of low quality and high heterogeneity, by including RCTs. The lack of blind design and results that report according to consolidated standards are significant factors of quality and heterogeneity. Moreover, whether acupuncture is merely a placebo effect has been controversial for years (34–36). Therefore, in this study, we only included single- and double-blind RCTs to provide high-quality evidence for the effectiveness of acupuncture and summarize the characteristics of sham/placebo acupuncture designs. Meanwhile, the general characteristics, such as age, gender, disease classification, and disease duration, will also be discussed in our study. This study could provide evidence to assist in decision-making among patients, caregivers, and clinicians in treating patients who have stroke complications with acupuncture and as a foundation for future studies.
Acupuncture dosage, a vital factor for heterogeneity, needs to be given more importance in meta-analyzes. Many acupuncture dosage factors, such as acupoint selection, treatment timing, manipulation technique, the background of an acupuncturist, and retention time, are essential for the acupuncture effect (37). In our study, the subgroup analysis will be conducted according to acupuncture dosage factors.
This study is also anticipated to have some limitations. First, different stroke complications and the stroke severity of the participants in included studies may lead to high potential heterogeneity and may decrease the reliability of the results. In addition, detailed information on acupuncture treatment, such as retention time and manipulation technique, may not be provided by clinical studies. The subgroup analysis on acupuncture dosage factors will be difficult to conduct with insufficient information. Finally, the number of single-blind RCTs on acupuncture treatment for stroke complications might need to be expanded to perform the analyzes.
Ethical approval was not required for the study involving humans in accordance with the local legislation and institutional requirements. Written informed consent to participate in this study was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and the institutional requirements.
X-YW: Conceptualization, Data curation, Formal analysis, Investigation, Software, Writing – original draft, Writing – review & editing. WL: Conceptualization, Data curation, Formal analysis, Investigation, Software, Writing – original draft, Writing – review & editing. HL: Data curation, Formal analysis, Writing – review & editing. M-YR: Data curation, Formal analysis, Writing – original draft. J-YL: Data curation, Formal analysis, Writing – original draft. S-KW: Data curation, Formal analysis, Writing – original draft. Y-ZD: Conceptualization, Writing – original draft. QZ: Conceptualization, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This trial was financially supported by the National Key R&D Program of China (2019YFC0840709). The funding source had no role in the study design, data collection, data analysis, interpretation, writing, or report publication.
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fneur.2023.1255999/full#supplementary-material
1. Katan, M , and Luft, A . Global Burden of Stroke. Semin Neurol. (2018) 38:208–11. doi: 10.1055/s-0038-1649503
2. GBD 2015 Neurological Disorders Collaborator Group . Global, regional, and national burden of neurological disorders during 1990-2015: a systematic analysis for the global burden of disease study 2015. Lancet Neurol. (2017) 16:877–97. doi: 10.1016/S1474-4422(17)30299-5
3. GBD 2016 Stroke Collaborators . Global, regional, and national burden of stroke, 1990-2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. (2019) 18:439–58. doi: 10.1016/S1474-4422(19)30034-1
4. Feigin, VL , Forouzanfar, MH , Krishnamurthi, R , Mensah, GA , Connor, M , Bennett, DA, et al. Global and regional burden of stroke during 1990-2010: findings from the global burden of disease study 2010. Lancet. (2014) 383:245–55. doi: 10.1016/s0140-6736(13)61953-4
5. Kelly-Hayes, M , Beiser, A , Kase, CS , Scaramucci, A , D'Agostino, RB , and Wolf, PA . The influence of gender and age on disability following ischemic stroke: the Framingham study. J Stroke Cerebrovasc Dis. (2003) 12:119–26. doi: 10.1016/S1052-3057(03)00042-9
6. World Health Organization . WHO global report on traditional and complementary medicine 2019. Geneva: World Health Organization (2019).
7. Wu, P , Mills, E , Moher, D , and Seely, D . Acupuncture in poststroke rehabilitation: a systematic review and meta-analysis of randomized trials. Stroke. (2010) 41:e171–9. doi: 10.1161/STROKEAHA.109.573576
8. Cao, BQ , Tan, F , Zhan, J , and Lai, PH . Mechanism underlying treatment of ischemic stroke using acupuncture: transmission and regulation. Neural Regen Res. (2021) 16:944–54. doi: 10.4103/1673-5374.297061
9. Chae, Y , Chang, DS , Lee, SH , Jung, WM , Lee, IS , Jackson, S, et al. Inserting needles into the body: a meta-analysis of brain activity associated with acupuncture needle stimulation. J Pain. (2013) 14:215–22. doi: 10.1016/j.jpain.2012.11.011
10. Zhang, Y , Zhang, H , Nierhaus, T , Pach, D , Witt, CM , and Yi, M . Default mode network as a neural substrate of acupuncture: evidence, Challenges and Strategy. Front Neurosci. (2019) 13:100. doi: 10.3389/fnins.2019.00100
11. Sun, HL , and Li, XM . Clinical study on treatment of cerebral apoplexy with penetration needling of scalp acupoints. Chinese Acupuncture Moxibustion. (2001) 21:275–8. doi: 10.13703/j.0255-2930.2001.05.012
12. Yang, A , Wu, HM , Tang, JL , Xu, L , Yang, M , and Liu, GJ . Acupuncture for stroke rehabilitation. Cochrane Database Syst Rev. (2016) 2016:CD004131. doi: 10.1002/14651858.CD004131.pub3
14. Panel, O , Khadilkar, A , Phillips, K , Jean, N , Lamothe, C , Milne, S, et al. Ottawa panel evidence-based clinical practice guidelines for post-stroke rehabilitation. Top Stroke Rehabil. (2006) 13:1–269. doi: 10.1310/3TKX-7XEC-2DTG-XQKH
15. Winstein, CJ , Stein, J , Arena, R , Bates, B , Cherney, LR , Cramer, SC, et al. Guidelines for adult stroke rehabilitation and recovery: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. (2016) 47:e98–e169. doi: 10.1161/STR.0000000000000098
16. Zhang, W , Lou, B , Li, J , Shi, W , Liu, X , Tang, J, et al. Clinical practice guidelines of Chinese medicine rehabilitation for ischemic stroke(cerebral infarction). Rehabil Med. (2021) 31:437–47. doi: 10.3724/SP.J.1329.2021.06001
17. Niu, JF , Zhao, XF , Hu, HT , Wang, JJ , Liu, YL , and Lu, DH . Should acupuncture, biofeedback, massage, qi gong, relaxation therapy, device-guided breathing, yoga, and tai chi be used to reduce blood pressure? Recommendations based on high-quality systematic reviews. Complement Ther Med. (2019) 42:322–31. doi: 10.1016/j.ctim.2018.10.017
18. Birch, S , and Robinson, N . Acupuncture as a post-stroke treatment option: a narrative review of clinical guideline recommendations. Phytomedicine. (2022) 104:154297. doi: 10.1016/j.phymed.2022.154297
19. Wang, L , Chi, X , Lyu, J , Xu, Z , Fu, G , Liu, Y, et al. An overview of the evidence to guide decision-making in acupuncture therapies for early recovery after acute ischemic stroke. Front Neurol. (2022) 13:1005819. doi: 10.3389/fneur.2022.1005819
20. Xin, Z , and Xue-TL, D-YK . GRADE in systematic reviews of acupuncture for stroke rehabilitation: recommendations based on high-quality evidence. Sci Rep. (2015) 5:16582. doi: 10.1038/srep16582
21. Wei, JJ , Yang, WT , Yin, SB , Wang, C , Wang, Y , and Zheng, GQ . The quality of reporting of randomized controlled trials of electroacupuncture for stroke. BMC Complement Altern Med. (2016) 16:512. doi: 10.1186/s12906-016-1497-y
22. Xu, M , Li, D , and Zhang, S . Acupuncture for acute stroke. Cochrane Database Syst Rev. (2018) 2018:CD003317. doi: 10.1002/14651858.CD003317.pub3
23. Kaptchuk, TJ . The double-blind, randomized, placebo-controlled trial: gold standard or golden calf? J Clin Epidemiol. (2001) 54:541–9. doi: 10.1016/s0895-4356(00)00347-4
24. Ferrante di Ruffano, L , Dinnes, J , Sitch, AJ , Hyde, C , and Deeks, JJ . Test-treatment RCTs are susceptible to bias: a review of the methodological quality of randomized trials that evaluate diagnostic tests. BMC Med Res Methodol. (2017) 17:35. doi: 10.1186/s12874-016-0287-z
25. White, AR , Filshie, J , and Cummings, TM . International acupuncture research forum. Clinical trials of acupuncture: consensus recommendations for optimal treatment, sham controls and blinding. Complement Ther Med. (2001) 9:237–45. doi: 10.1054/ctim.2001.0489
26. Yoshida, M , Kinoshita, Y , Watanabe, M , and Sugano, K . JSGE clinical practice guidelines 2014: standards, methods, and process of developing the guidelines. J Gastroenterol. (2015) 50:4–10. doi: 10.1007/s00535-014-1016-1
27. Lv, Q , Xu, G , Pan, Y , Liu, T , Liu, X , Miao, L, et al. Effect of acupuncture on neuroplasticity of stroke patients with motor dysfunction: a Meta-analysis of fMRI studies. Neural Plast. (2021) 2021:8841720–10. doi: 10.1155/2021/8841720
28. Liu, S , Zhang, CS , Cai, Y , Guo, X , Zhang, AL , Xue, CC, et al. Acupuncture for post-stroke shoulder-hand syndrome: a systematic review and Meta-analysis. Front Neurol. (2019) 10:433. doi: 10.3389/fneur.2019.00433
29. Kuang, X , Fan, W , Hu, J , Wu, L , Yi, W , Lu, L, et al. Acupuncture for post-stroke cognitive impairment: a systematic review and meta-analysis. Acupunct Med. (2021) 39:577–88. doi: 10.1177/09645284211009542
30. Liu, W , Rao, C , Du, YZ , Zhang, LL , and Yang, JP . The effectiveness and safety of manual acupuncture therapy in patients with Poststroke cognitive impairment: a Meta-analysis. Neural Plast. (2020) 2020:1–15. doi: 10.1155/2020/8890521
31. Lu, Y , Chen, Y , Huang, D , and Li, J . Efficacy of acupuncture for dysphagia after stroke: a systematic review and meta-analysis. Ann Palliat Med. (2021) 10:3410–22. doi: 10.21037/apm-21-499
32. Liu, R , Zhang, K , Tong, QY , Cui, GW , Ma, W , and Shen, WD . Acupuncture for post-stroke depression: a systematic review and meta-analysis. BMC Complement Med Ther. (2021) 21:109. doi: 10.1186/s12906-021-03277-3
33. Lee, SH , and Lim, SM . Acupuncture for insomnia after stroke: a systematic review and meta-analysis. BMC Complement Altern Med. (2016) 16:228. doi: 10.1186/s12906-016-1220-z
34. Kim, TH , Lee, MS , and Lee, H . Sham acupuncture is not just a placebo. J Acupunct Meridian Stud. (2022) 15:333–5. doi: 10.51507/j.jams.2022.15.6.333
35. McGeeney, BE . Acupuncture is all placebo and here is why. Headache. (2015) 55:465–9. doi: 10.1111/head.12524
36. Wu, XK , Stener-Victorin, E , Kuang, HY , Ma, HL , Gao, JS , Xie, LZ, et al. Effect of acupuncture and clomiphene in Chinese women with polycystic ovary syndrome: a randomized clinical trial. JAMA. (2017) 317:2502–14. doi: 10.1001/jama.2017.7217
Keywords: stroke, stroke complications, acupuncture, blind design, sham acupuncture
Citation: Wang X-Y, Liu W, Li H, Rong M-Y, Li J-Y, Wang S-K, Du Y-Z and Zhao Q (2023) Effectiveness of acupuncture treatment for stroke and stroke complications: a protocol for meta-analysis and systematic review based on randomized, single-blind, controlled trials. Front. Neurol. 14:1255999. doi: 10.3389/fneur.2023.1255999
Edited by:
Narayanaswamy Venketasubramanian, Raffles Hospital, SingaporeReviewed by:
António Moreira, Instituto Politécnico de Santarém-ESDRM, PortugalCopyright © 2023 Wang, Liu, Li, Rong, Li, Wang, Du and Zhao. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Qi Zhao, aG91aGFvd2VuMkAxNjMuY29t
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.