 Alex S. Aguirre
Alex S. Aguirre Kenny Rojas
Kenny Rojas
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Neurol. , 06 September 2023
Sec. Pediatric Neurology
Volume 14 - 2023 | https://doi.org/10.3389/fneur.2023.1253515
Background: Pediatric casualties in war zones are a devastating consequence of armed conflicts, causing significant challenges for affected children, especially in the context of poor access to care. This study aimed to understand traumatic brain injuries (TBIs) in this high-risk population and to identify and provide information for the stakeholders, as well as to recognize severe long-term consequences and develop strategies to prevent them, thus minimizing their burden while aiding in the management of these cases.
Methods: We carried out a systematic literature review following PRISMA guidelines to identify publications discussing traumatic brain injuries in children in the context of war zones, and we analyzed all the collected data.
Results: Our study showed that head injuries were the most common casualty in war zones; male and female children were affected, and the mean age was 8–10 years. Most children were reported to be from Afghanistan, and blasts were the most common mechanism of injury. The mortality fluctuated from 3 to 47%.
Conclusion: There is a lack of evidence-based information regarding the characterization, approach, and management of children with TBI in conflict zones. While the world finds ways to live in peace, there is an urgency to research, train, and deploy enough specialists to these areas, if governments are serious about improving outcomes for this population.
Pediatric casualties in war zones are a devastating consequence of armed conflicts, causing significant physical, emotional, and cognitive challenges for affected children (1). War zones expose children to various forms of violence, such as being caught in crossfire or becoming victims of deliberate attacks, leading to head injuries that can result in severe head traumas such as traumatic brain injury (TBI). The consequences of pediatric TBIs in war zones are extensive, impacting not only the individual child but also their families and the community at large (2, 3).
War amplifies injuries due to the use of heavy artillery, explosive devices, and other weapons that cause substantial damage. The developing brains of children are particularly vulnerable, making them more susceptible to long-term cognitive and neurological impairments. The immediate effects of pediatric TBI in war zones can be life-threatening. Children may suffer from loss of consciousness, seizures, and respiratory difficulties, requiring urgent medical attention (4, 5).
Access to quality healthcare is often limited in war zones due to medical infrastructure destruction, lack of resources, and restricted movement. These challenges further exacerbate the difficulties in providing timely and appropriate care for children with TBIs. However, even when children with TBI receive initial medical care, the long-term consequences can be profound. Cognitive impairments, including memory deficits, attention problems, and executive functioning difficulties, are common. Emotional and behavioral changes, such as depression, anxiety, aggression, and impulsivity, may also arise due to the injury (1–3, 6).
These impairments can significantly affect a child's ability to learn, concentrate, and perform daily activities and their integration into society, leading to economic and public health burdens. Therefore, it is crucial that appropriate resources and research efforts are focused on comprehending the underlying mechanisms of TBIs in children in war zones. This understanding is essential for making accommodations considering the limited availability of specialized medical personnel, a shortage of rehabilitation facilities, and socioeconomic barriers that hinder comprehensive care (7). Our study aimed to clarify this topic, promoting awareness and prompting actions on this matter.
We carried out a systematic review using the PRISMA protocol. Figure 1 shows the results of the study using this protocol.
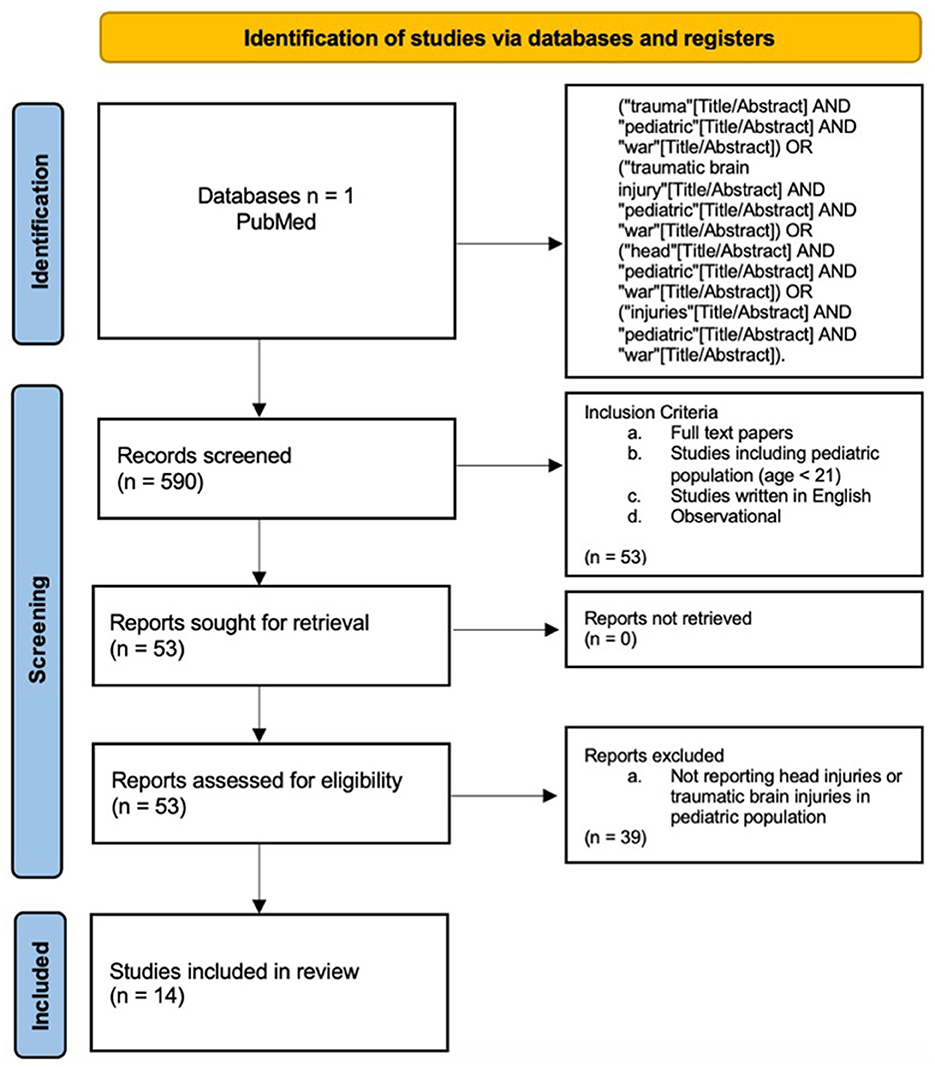
Figure 1. PRISMA protocol for this study. Identification, screening, and inclusion process.
We selected studies written in English. Animal studies and articles that did not fulfill the aims of our study were excluded. We only included studies about trauma in war zones that contain an analysis of traumatic brain injury and head injuries in pediatric patients. We gathered outcomes of the mechanism of injury, the characteristics of the trauma, and the main conclusions.
We used the PubMed database for this systematic literature review. The search was conducted between 10 March and 16 June 2023. We used an advanced search strategy with the following terms: (“trauma”[Title/Abstract] AND “pediatric”[Title/Abstract] AND “war”[Title/Abstract]) OR (“traumatic brain injury”[Title/Abstract] AND “pediatric”[Title/Abstract] AND “war”[Title/Abstract]) OR (“head”[Title/Abstract] AND “pediatric”[Title/Abstract] AND “war”[Title/Abstract]) OR (“injuries”[Title/Abstract] AND “pediatric”[Title/Abstract] AND “war”[Title/Abstract]).
We collected the following information from each article: the author/year, methods, number of participants, and study design. We also extracted the main results, including each study's outcome measures and main limitations. We analyzed the studies' primary and secondary goals and gathered the main conclusions from each study.
We used the Newcastle–Ottawa tool to perform the quality assessment in observational studies.
We found 14 clinical trials that specifically discussed pediatric traumatic brain injuries in war zones, along with other pediatric casualties in this context.
Table 1 presents the demographics of each study. Our findings show that 50% (7/14) of the studies report pediatric TBIs that occurred in Afghanistan. The total sum of all pediatric samples found in these studies is 14,624. The mean age falls between 8 and 10 years. The most prevalent mechanism of injury is blast related to explosive devices (57%), followed by ballistic injuries caused by gunshots (29%) and fragment injuries (14%). TBI accounts for one of the most commonly reported injuries in war zones.

Table 1. Population demographics and most common mechanism of the TBI.
Table 2 shows the outcomes and conclusions of the studies included in this systematic review. Our findings show that 64% (9/14) of the studies used the New Injury Severity Score or the Injury Severity Score (NISS or ISS) to report injuries. The range of mortality lies between 3.4 and 47%. Cuenca et al. report that most TBIs generate an unspecific pattern but suggest that neurosurgeons should be prepared for intracranial hemorrhages (18). Naaman et al. support this idea (19). On a different note, Cingoz et al. report that intraparenchymal bone fragments caused most TBIs in their study and suggest that surgical treatment should be established in all patients using a Glasgow Coma Scale (GCS) higher than 3 and a radiological indication (20). Finally, Klimo et al. and Maitland et al. emphasize that male patients die less than female patients, possibly due to the inequality of healthcare access for female patients in these regions (17, 21).

Table 2. Characteristics and outcomes.
Table 3 shows the quality assessment of the studies included in this systematic review.
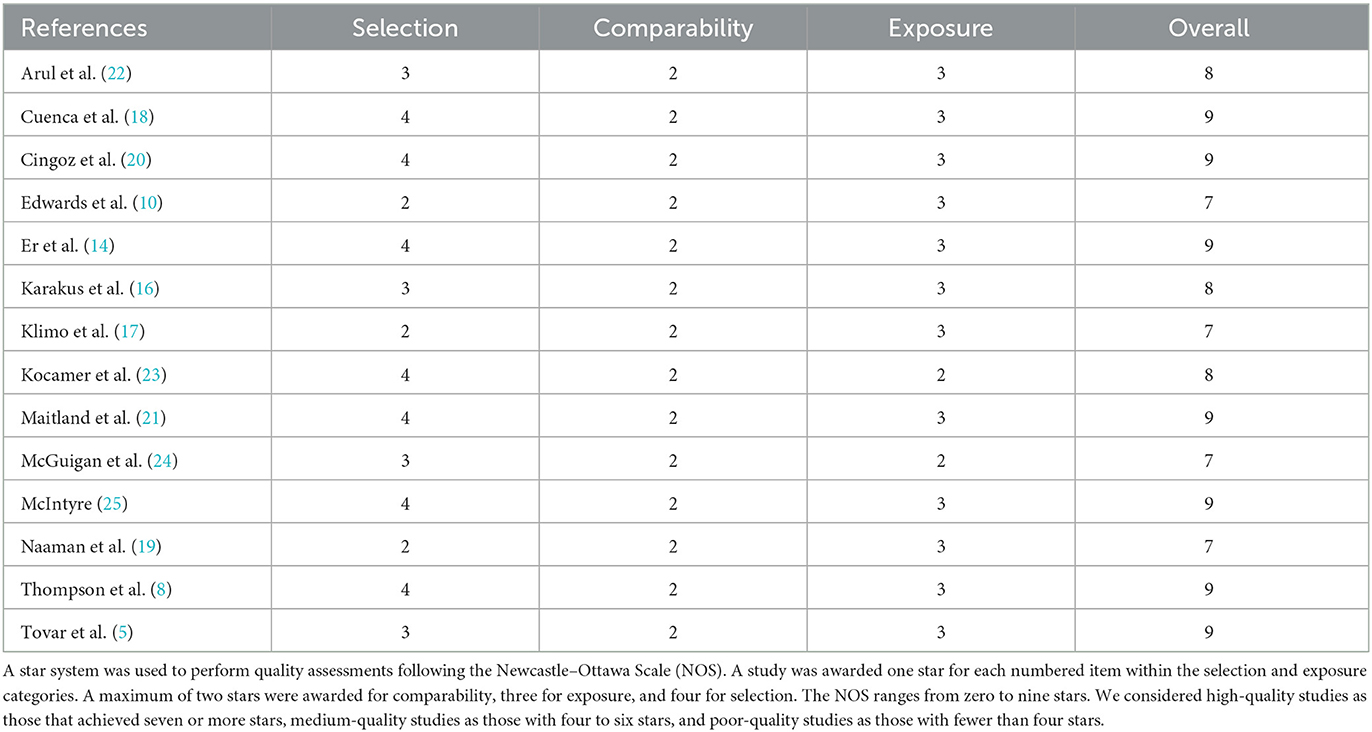
Table 3. Quality assessment.
Multiple studies have demonstrated the vast consequences of war on children, from physical trauma to mental health problems (1, 6, 9, 11). Our study shows that TBIs in war zones have many mechanisms of injury that vary depending on the location and historical time. It is difficult to detail the characteristics of TBIs in every study, given that the scale used to represent the trauma is inconsistent and varies depending on the study. Additionally, most studies include “head trauma” or “head injury” as part of their TBI reports, even when the injuries range from minor bruises to injuries requiring neurosurgical consultation, making a detailed analysis of the TBIs difficult (5).
Our study focuses on all characteristics of TBIs; some data are provided by articles that failed to distinguish between pediatric and adult patient injuries but are good for understanding the background and characterization of TBIs in war. The most prevalent mechanism of injury is blast. Blast injuries usually cause more damage to the body than an isolated brain injury, which directly worsens the prognosis of the patients, increases the mortality of these cases, and raises concerns for bias in the collected data by making the reports unspecific information.
Blast injuries are linked directly to neurological effects due to the physical science behind them. Technically, explosive devices create shock waves with high-speed pressure changes that travel faster than sound. However, war explosions are more chaotic because they may involve multiple shock waves and reflections from surfaces. This causes various injuries from direct pressure effects on organs, flying objects that get thrown and hit people, and thermal effects. Electromagnetic disturbances may also be present, but their physiological impact is unclear (12).
Researchers are pivotal in advancing pediatric TBI understanding and treatment in war zones. Studies examining TBI's long-term outcomes, rehabilitation strategies, and psychosocial impact can guide evidence-based interventions.
Our study shows a range of mortality between 3.4 and 47%. However, each study's mean age and number of pediatric patients vary significantly. As mentioned earlier, the data are biased, causing marked variability. Nevertheless, it is evident that pediatric mortality is higher in war zones, especially when the children have a TBI associated with other lesions or when they have a TBI caused by war alone (17, 19–21). Pediatric population is more susceptible to dying from a TBI in war than an adult.
Most authors use the Abbreviated Injury Scale (AIS) or the ISS scale to report TBIs, while only three studies present GCS reports. Data analysis of these scales shows they are good for interpreting mortality and outcomes in patients with TBIs. While the AIS/ISS reports data concerning the physical and anatomical aspects of TBIs, GCS presents data from the functional and physiological aspects. There are no significant differences in the mortality reported from one scale to another, but it would be ideal for further studies to report on both anatomical and physiological scales (21, 23).
Some studies mentioned the difference between male and female children. However, this was not mentioned in light of any anatomical or physiological difference but in the context of culture. Some authors report that male injuries tend to be more commonly reported because of the geographical location of most wars (i.e., the middle east), where a male individual's life is more valuable than a female individual's (21). However, those reports may also be influenced by the historical role of men as house protectors; then, they would be more likely to be exposed to TBIs.
The only study that analyzed the treatment costs per case was conducted by Karakus et al., which noted that the value could be as high as 69,556 Turkish Liras, equivalent to 6.1 minimum wages per month in Turkey (16). Other studies have also analyzed the costs and financial burden of non-fatal TBIs in the United States, which in 2016 were 40.6 billion US dollars (26).
War conflicts profoundly impact children's mental health, both during and after the conflicts. War experiences can leave deep psychological scars on young minds, often leading to long-lasting emotional, behavioral, and developmental issues. Understanding and addressing the mental health needs of children affected by war are crucial for their wellbeing and future prospects.
During war conflicts, children are exposed to a range of traumatic events such as violence, displacement, loss of loved ones, destruction of homes, and separation from their families. These experiences can lead to acute stress reactions, including fear, anxiety, depression, and post-traumatic stress disorders (PTSDs). Witnessing or experiencing violence can disrupt a child's normal brain development and have lifelong consequences.
Children in war-affected areas often lack access to essential resources and services, including mental healthcare. The destruction of healthcare infrastructure, limited availability of trained professionals, and societal stigma surrounding mental health exacerbate the challenges faced by these children. As a result, many suffer in silence, without the support they need to recover and rebuild their lives.
Even after the conflict ends, the effects of war on children's mental health can persist. They may continue to experience symptoms of trauma, depression, anxiety, and other mental health disorders. Additionally, the loss of education, disrupted social networks, and economic instability can further hinder their psychological wellbeing.
Additionally, children with TBIs suffer from severe physical consequences. These injuries can range from immediate life-threatening conditions to long-term impairments. Common physical consequences include motor impairments, sensory deficits, speech and language difficulties, cognitive impairments, and an increased risk of seizures and epilepsy (11, 13).
All these factors create an environment to develop chaos by increasing the pediatric risk of abuse and neglect due to limited access to basic needs and care. This is closely linked to more direct effects, such as toxic environmental exposures and the increased incidence of infectious diseases (13, 15).
Addressing pediatric TBIs in war zones requires a multidisciplinary team. Efforts to solve the problem should focus on reducing armed conflicts and protecting children's rights during times of war. International humanitarian organizations and governments must work together to implement policies and interventions prioritizing children's safety and wellbeing, including strict regulations on using explosive weapons in populated areas.
Furthermore, healthcare infrastructure is critical in war-torn regions. Building and equipping medical facilities, training healthcare professionals in TBI management, and ensuring essential medical supplies are crucial steps. International aid organizations and governments should collaborate to provide financial support and technical expertise to strengthen healthcare systems. This, of course, should include a specific focus on pediatric TBI care.
Finally, rehabilitation services must also be expanded and tailored to meet the unique needs of children with TBI in war zones, including specialized rehabilitation centers, mobile clinics, and community-based programs that reach children in remote and conflict-affected areas. Additionally, psychosocial support services for both children and their families should be integrated into the rehabilitation process to address the emotional and social challenges of TBIs.
As mentioned before, the major limitation of this systematic review is the analysis of biased data. However, it is important to note that it would be impossible to collect unbiased data in scenarios such as war. Additionally, the report we generated from the collected data provides a good understanding of pediatric TBIs in war zones, allowing stakeholders to develop better plans for chaotic events such as this one.
We found a lack of evidence-based information concerning the approach and management of children with TBIs in conflict zones, primarily due to the absence of a clear consensus on their characteristics. Our findings reveal that head injuries were the most frequently identified type of injury, often caused by blasts. The majority of affected children were reported to be from Afghanistan, with both male and female children impacted, and their average age falling between 8 and 10 years. Mortality rates varied significantly from 4 to 47%, depending on the conflict, indicating substantial diversity. In light of these findings, it is evident that as the world seeks pathways to global peace, there is an urgent need to conduct research, provide training, and deploy specialists to these regions if governments are genuinely committed to enhancing outcomes for this vulnerable population. These conclusions should serve as a catalyst for potential recommendations aimed at medical professionals, legislators, and stakeholders, urging them to ensure timely treatment and rehabilitation services for pediatric patients based on this compelling evidence.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
AA: Data curation, Formal analysis, Investigation, Methodology, Resources, Visualization, Writing—original draft, Writing—review and editing. KR: Formal analysis, Validation, Visualization, Writing—review and editing. AT: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Resources, Validation, Visualization, Writing—original draft, Writing—review and editing.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Wild H, Stewart BT, LeBoa C, Stave CD, Wren SM. Pediatric casualties in contemporary armed conflict: a systematic review to inform standardized reporting. Injury. (2021) 52:1748–56. doi: 10.1016/j.injury.2021.04.055
2. Haverkamp FJC, van Gennip L, Muhrbeck M, Veen H, Wladis A, Tan ECTH. Global surgery for paediatric casualties in armed conflict. World J Emerg Surg. (2019) 14:55. doi: 10.1186/s13017-019-0275-9
3. Samara M, Hammuda S, Vostanis P, El-Khodary B, Al-Dewik N. Children's prolonged exposure to the toxic stress of war trauma in the Middle East. Br Med J. (2020) 371:m3155. doi: 10.1136/bmj.m3155
4. Shi X, Edwards MJ. Pediatric wartime injuries in Afghanistan and Iraq: what have we learned? US Army Med Dep J. (2016) 153–6.
5. Tovar MA, Pilkington RA, Goodwin T, Root JM. Pediatric blast trauma: a systematic review and meta-analysis of factors associated with mortality and description of injury profiles. Prehosp Disaster Med. (2022) 37:492–501. doi: 10.1017/S1049023X22000747
6. Goldson E. The effect of war on children. Child Abuse Negl. (1996) 20:809–19. doi: 10.1016/0145-2134(96)00069-5
7. Bürgin D, Anagnostopoulos D, Vitiello B, Sukale T, Schmid M, Fegert JM. Impact of war and forced displacement on children's mental health-multilevel, needs-oriented, and trauma-informed approaches. Eur Child Adolesc Psychiatry. (2022) 31:845–53. doi: 10.1007/s00787-022-01974-z
8. Thompson DC, Crooks RJ, Clasper JC, Lupu A, Stapley SA, Cloke DJ. The pattern of paediatric blast injury in Afghanistan. Br Med J Mil Health. (2020) 166:151–5. doi: 10.1136/jramc-2017-000795
9. Ludvigsson JF, Loboda A. Systematic review of health and disease in Ukrainian children highlights poor child health and challenges for those treating refugees. Acta Paediatr. (2022) 111:1341–53. doi: 10.1111/apa.16370
10. Edwards MJ, Lustik M, Eichelberger MR, Elster E, Azarow K, Coppola C. Blast injury in children: an analysis from Afghanistan and Iraq, 2002-2010. J Trauma Acute Care Surg. (2012) 73:1278–83. doi: 10.1097/TA.0b013e318270d3ee
11. Cuenca CM, Borgman MA, Dengler BA, Schauer SG. Incidence of post-traumatic seizures in children during combat operations in Afghanistan and Iraq. Injury. (2022) 53:3297–300. doi: 10.1016/j.injury.2022.07.013
12. Hicks RR, Fertig SJ, Desrocher RE, Koroshetz WJ, Pancrazio JJ. Neurological effects of blast injury. J Trauma. (2010) 68:1257–63. doi: 10.1097/TA.0b013e3181d8956d
13. Kadir A, Shenoda S, Goldhagen J. Effects of armed conflict on child health and development: a systematic review. PLoS ONE. (2019) 14:e0210071. doi: 10.1371/journal.pone.0210071
14. Er E, Çorbacioglu SK, Güler S, Aslan S, Seviner M, Aksel G, et al. Analyses of demographical and injury characteristics of adult and pediatric patients injured in Syrian civil war. Am J Emerg Med. (2017) 35:82–6. doi: 10.1016/j.ajem.2016.10.008
15. Kaya OM, Serarslan G, Dirican E. Evaluation of clinical and demographic characteristics of Turkish and Syrian pediatric cutaneous Leishmaniasis patients from Hatay, Turkey after the Syrian civil war. Postepy Dermatol Alergol. (2020) 37:229–33. doi: 10.5114/ada.2018.79729
16. Karakus A, Yengil E, Akkucuk S, Cevik C, Zeren C, Uruc V. The reflection of the Syrian civil war to emergency department and assessment of hospital costs. Ulus Travma Acil Cerrahi Derg. (2013) 19:429–33. doi: 10.5505/tjtes.2013.78910
17. Klimo P, Ragel BT, Jones GM, McCafferty R. Severe pediatric head injury during the Iraq and Afghanistan conflicts. Neurosurgery. (2015) 77:1–7. doi: 10.1227/NEU.0000000000000743
18. Cuenca CM, Clarke EE, Dengler BA, Borgman MA, Schauer SG. An analysis of intracranial hemorrhage in wartime pediatric casualties. World Neurosurg. (2021) 154:e729–33. doi: 10.1016/j.wneu.2021.07.128
19. Naaman O, Yulevich A, Sweed Y. Syria civil war pediatric casualties treated at a single medical center. J Pediatr Surg. (2020) 55:523–9. doi: 10.1016/j.jpedsurg.2019.02.022
20. Cingoz ID, Kaya I, Sahin MC, Vural M. Pediatric cranial injuries: the Syrian civil war. Childs Nerv Syst. (2022) 38:1743–9. doi: 10.1007/s00381-022-05556-x
21. Maitland L, Middleton L, Veen H, Harrison DJ, Baden J, Hettiaratchy S. Analysis of 983 civilian blast and ballistic casualties and the generation of a template of injury burden: an observational study. eClinicalMedicine. (2022) 54:101676. doi: 10.1016/j.eclinm.2022.101676
22. Arul GS, Reynolds J, Di Russo S, Scott A, Bree S, Templeton P, et al. Paediatric admissions to the British military hospital at Camp Bastion, Afghanistan. Ann R Coll Surg Engl. (2012) 94:52–7. doi: 10.1308/003588412X13171221499027
23. Kocamer Simşek B, Dokur M, Uysal E, Çaliker N, Gökçe N, Deniz IK, et al. Characteristics of the injuries of Syrian refugees sustained during the civil war. Ulus Travma Acil Cerrahi Derg. (2017) 23:199–206. doi: 10.5505/tjtes.2016.95525
24. McGuigan R, Spinella PC, Beekley A, Sebesta J, Perkins J, Grathwohl K, et al. Pediatric trauma. Experience of a combat support hospital in Iraq. J Pediatr Surg. (2007) 42:207–10. doi: 10.1016/j.jpedsurg.2006.09.020
25. McIntyre J. Syrian Civil War: a systematic review of trauma casualty epidemiology. Br Med J Mil Health. (2020) 166:261–5. doi: 10.1136/jramc-2019-001304
Keywords: war, children, conflict, brain, injury
Citation: Aguirre AS, Rojas K and Torres AR (2023) Pediatric traumatic brain injuries in war zones: a systematic literature review. Front. Neurol. 14:1253515. doi: 10.3389/fneur.2023.1253515
Received: 05 July 2023; Accepted: 11 August 2023;
Published: 06 September 2023.
Edited by:
Kette D. Valente, University of São Paulo, BrazilReviewed by:
Rodrigo Ramos-Zúñiga, University of Guadalajara, MexicoCopyright © 2023 Aguirre, Rojas and Torres. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alcy R. Torres, YXJ0b3JyZXNAYnUuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.